

Abstract
Background and aims
The Apo B/A1 ratio is a major factor that predicts future cardiovascular outcomes. However, it is unclear whether the apolipoprotein B (Apo B)/apolipoprotein A1 (Apo A1) is a better predictor of future outcome than the total cholesterol (TC)/HDL-C ratio or lipoprotein (a) (Lp (a)) after the percutaneous coronary intervention (PCI). Therefore, we performed this study to evaluate the impact of the Apo B/A1 ratio on the patients who achieved LDL-C below 70 mg/dL one year after PCI.
Methods
We included 448 PCI patients whose LDL-C levels were below 70 mg/dL at follow-up. The Apo B/A1 ratio, TC/HDL-C ratio, and Lp (a) levels were measured at the time of PCI and follow-up, and decreases in these parameters between baseline and follow-up were assessed as potential markers to predict major cardiovascular adverse events (MACEs).
Results
During a median follow-up period of 38.0 months, 115 MACEs were recorded. The tertile with the lowest decrease in the Apo B/A1 ratio (≤ 0.146) showed a lower MACE survival rate compared to the other tertiles. There were no differences in MACE survival rates for the TC/HDL-C ratio or Lp (a) levels.
Conclusions
The Apo B/A1 ratio had better predictive accuracy for clinical outcomes compared to the TC/HDL-C ratio and Lp (a) level. A lower decrease in the Apo B/A1 ratio may be a residual risk factor for MACEs in patients who have reached LDL-C levels below 70 mg/dL after PCI.
Introduction
The 2018 American Heart Association (AHA)/American College of Cardiology (ACC) guideline strongly suggests that low-density lipoprotein cholesterol (LDL-C) should be maintained below 70 mg/dL in patients with clinical atherosclerotic cardiovascular disease by using statins to achieve 50% or greater reduction [1]. However, the residual cardiovascular risk factor is not clear in patients whose LDL-C levels are maintained below 70 mg/dL after percutaneous coronary intervention (PCI).
The apolipoprotein B (Apo B) is the main component of very low-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL), low-density lipoproteins (LDL) and lipoprotein (a) (Lp(a)); while Apolipoprotein A1 (Apo A1) is the main apolipoprotein incorporated into high‐density lipoprotein (HDL). Therefore, the Apo B/A1 ratio reflects the cholesterol balance between atherogenic and anti-atherogenic lipoprotein particles [2, 3]. Lp(a) is a low-density lipoprotein like particle with Apo B-100, linked by a disulfide bond to apolipoprotein (a). Lp(a) has enhanced atherogenic and thrombogenic properties and has been identified as an independent risk factor for cardiovascular disease [4]. Total cholesterol (TC)/high-density lipoprotein cholesterol (HDL-C) ratio has been reported as a risk indicator with greater predictive value than isolated parameters, particularly LDL [5]. In previous studies, high Apo B/A1 ratios, TC/HDL-C ratios, and Lp (a) levels have been associated with cardiovascular disease [2–4, 6–16]. However, it is unclear whether the Apo B/A1 ratio is similar to or better than the TC/HDL-C ratio or Lp (a) levels as a clinical predictor in patients who have achieved the recommended target level of LDL-C after PCI. Therefore, for the first time, we investigated the impact of Apo B/A1 ratios on clinical outcomes for patients who achieved LDL-C levels below 70 mg/dL 1 to 3 years after PCI with drug eluting stents (DES).
Materials and methods
Study population and data collection
The study population was selected from the PCI registry at the Daegu Catholic Medical Center (Daegu, Korea). Between October 2005 and February 2018, 1,361 patients underwent their first PCI with DES and began statin therapy. Among the 1,361 patients, we investigated 487 patients whose LDL-C was below 70 mg/dL between 1 and 3 years after the PCI. Of 487 patients, we excluded 18 patients who had an estimated glomerular filtration rate below 30 mL/min/1.73 m2 and 21 patients who used lipid lowering agents other than statins. The inclusion and exclusion criteria for the study are shown in a flow diagram (Fig 1).
Fig 1. Enrollment flow chart for analysis.
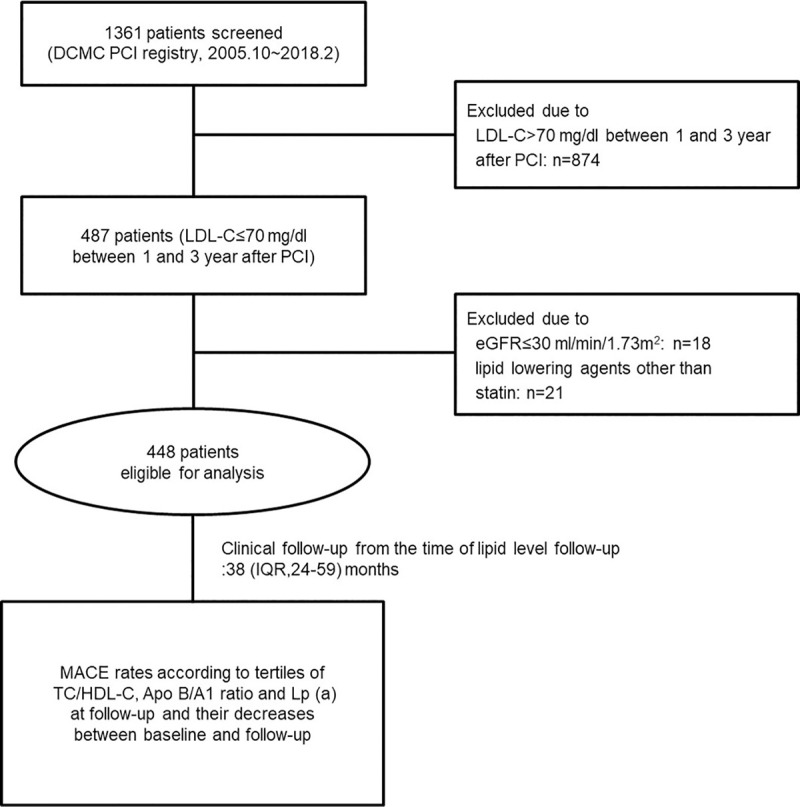
Apo A1; apolipoprotein A1, Apo B; apolipoprotein B, DCMC; Daegu catholic medical center, eGFR; estimated glomerular filtration rate, HDL-C; high-density lipoprotein cholesterol, LDL-C; low-density lipoprotein cholesterol, Lp (a); lipoprotein (a), MACE; major cardiovascular adverse event, PCI; percutaneous coronary intervention, TC; total cholesterol.
We included 448 patients in our study and evaluated the lipid profiles of these patients at the time of the PCI (baseline) and follow-up. The lipid profiles included measurements of Lp (a), TG, TC, LDL-C, HDL-C, Apo B, and Apo A1. Patients were classified into tertiles based on the Apo B/A1 and TC/HDL-C ratios and Lp (a) levels at follow-up and the differences in these parameters between baseline and follow-up. The primary endpoint was major adverse cardiovascular events (MACEs), which were defined as cardiac death, non-fatal myocardial infarction (MI), any coronary revascularization, and ischemic stroke. MI was defined by the third universal definition [17]. Clinical follow-up began at the time of the lipid profile follow-up. MACE rates were compared according to the tertile classification described above. Prescribed statins were evaluated at baseline and follow-up and classified according to statin intensity based on the ACC guideline [1]. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki. The Institutional Review Board at our center approved the study and waived the requirement for patient informed consent because of the study’s retrospective nature (CR20224L).
PCI procedure and statin usage
The type of stent selected for each patient was at the discretion of the physician at the time of the PCI. Patients were treated with first (n = 54) or second (n = 394) generation DES. First-generation DES eluted sirolimus (Cypher) or paclitaxel (Taxus), whereas second-generation DES eluted agents other than sirolimus or paclitaxel. DES implantation was performed using conventional techniques. Unfractionated heparin was administered as an initial IV bolus of 100 IU/kg body weight, with additional heparin administered during the procedure to achieve an activated clotting time of 250 to 300 s. Dual oral antiplatelet therapy (100 mg aspirin and 75 mg clopidogrel, 180 mg ticagrelor, or 10 mg prasugrel) was recommended to all patients for at least 12 months after DES implantation. Each of the 448 patients was discharged with a statin prescription after the PCI, and the type of statin selected was at the discretion of the physician.
Statistical analysis
Data were expressed as the number (%), mean ± standard deviation, or median with interquartile range (IQR). Categorical data were compared by the chi-square test or Fisher’s exact test. Continuous variables were compared using a Student’s t-test when normally distributed and Kruskal-Wallis H test when non-normally distributed. Event-free survival was analyzed using Kaplan-Meier survival curves and compared using the log-rank test between different groups. Univariate Cox proportional hazards regression was performed to identify potential independent predictors for MACE. Age, sex and variables achieving a p-value less than 0.10 in the univariate analysis were entered in the multivariate analysis to determine the independent predictors for MACE. In the regression models, the Apo B/A1 and TC/HDL-C ratios, Lp (a) levels, and their differences between baseline and follow-up were analyzed as categorical variables and the distributions were divided into tertiles. Diagnostic accuracy of decreases in TC/HDL-C, Lp (a), Apo B/A1 ratio and LDL-C on a continuous scale in the prediction of MACE was estimated as the area under the curve (AUC) from receiver operating characteristic (ROC) curves. Univariate analysis using logistic regression was performed to identify independent predictors of the tertile showing the lowest decrease in the Apo B/A1 ratio. Age, sex and variables achieving a p-value less than 0.10 were entered in the multivariate analysis. A p-value less than 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 20.0.0 (IBM, Armonk, NY, USA).
Results
Of the 448 patients, the mean age was 63.5 ± 10.7 years, 72.5% were men, and 49.1% were diabetic patients. After the PCI, 229 patients were discharged with a high-intensity statin dose (20 mg rosuvastatin, n = 81; 40 mg atorvastatin, n = 148) and 219 patients were discharged with a moderate intensity statin dose (5 mg rosuvastatin, n = 1; 10 mg rosuvastatin, n = 39; 10 mg atorvastatin, n = 72; 20 mg atorvastatin, n = 66; 2 mg pitavastatin, n = 36; 4 mg pitavastatin, n = 3; 20 mg simvastatin, n = 1; 40 mg pravastatin, n = 1). At the time of lipid profile follow-up, 190 patients were using a high-intensity statin dose (20 mg rosuvastatin, n = 65; 40 mg atorvastatin, n = 125) and 258 patients were taking a moderate intensity statin dose (5 mg rosuvastatin, n = 14; 10 mg rosuvastatin, n = 53; 10 mg atorvastatin, n = 76; 20 mg atorvastatin, n = 58; 2 mg pitavastatin, n = 49; 4 mg pitavastatin, n = 5; 20 mg simvastatin, n = 1; 40 mg pravastatin, n = 2). The median duration from index PCI to lipid profile follow-up was 14.0 months (interquartile range: 12.0–22.0 months). The median duration of clinical follow-up was 38.0 months (interquartile range: 24.0–59.0 months).
Characteristics according to tertiles for the decrease in Apo B/A1 ratio
The clinical characteristics of the patients stratified by tertiles for the decrease in Apo B/A1 ratios between the PCI and lipid profile follow-up are displayed in Table 1. The proportion of hypertensive and male patients was highest in tertile 1 and tertile 3, respectively. At the time of both PCI and lipid profile follow-up, the incidence of high-intensity statin use was the lowest in tertile 1 and highest in tertile 3. In lipid profile evaluation, significant differences between tertiles were observed for TC, LDL-C, Apo B, HDL-C, Apo A1, and the Apo B/A1 ratio at the time of PCI. At the time of lipid profile follow-up, significant differences between tertiles were observed for HDL-C, Apo B, Apo A1, and the Apo B/A1 ratio. However, there were no significant differences for TC, TG, LDL-C, or Lp (a) among the three groups.
Table 1. Characteristics of individuals stratified by tertiles of Apo B/A1 ratio decrease.
| Variables | Total patients (n = 448) | Tertile 1 of Apo B/A1 ratio decrease ≤0.146 (n = 149) | Tertile 2 of Apo B/A1 ratio decrease 0.146–0.346 (n = 150) | Tertile 3 of Apo B/A1 ratio decrease >0.346 (n = 149) | p-value |
|---|---|---|---|---|---|
| Clinical characteristics | |||||
| Age, years | 63.5 ± 10.7 | 64.4 ± 10.4 | 63.7 ± 10.3 | 62.4 ± 11.3 | 0.238 |
| Male | 325 (72.4) | 101 (67.8) | 103 (68.7) | 121 (81.2) | 0.015 |
| Diabetes | 220 (49.0) | 77 (51.7) | 74 (49.3) | 69 (46.3) | 0.649 |
| Hypertension | 242 (53.9) | 95 (63.8) | 77 (51.3) | 70 (47.0) | 0.011 |
| Smoking | 199 (44.3) | 69 (46.3) | 57 (38.0) | 73 (49.0) | 0.137 |
| MI at index PCI | 261 (58.1) | 83 (55.7) | 84 (56.0) | 94 (63.1) | 0.343 |
| eGFR, (ml/min/1.73 m2) | 85.2 ± 19.1 | 84.8 ± 19.4 | 84.2 ± 19.7 | 86.6 ± 18.2 | 0.523 |
| BMI (kg/m2) | 23.6 ± 3.15 | 23.6 ± 3.57 | 23.7 ± 3.05 | 23.6 ± 2.81 | 0.886 |
| EF (%) | 56.1 ± 11.3 | 56.1 ± 11.4 | 56.2 ± 11.7 | 56.0 ± 10.8 | 0.989 |
| Beta blocker | 386 (86.0) | 125 (83.9) | 128 (85.3) | 133 (89.3) | 0.381 |
| ACEi or ARB | 390 (86.9) | 128 (85.9) | 128 (85.3) | 134 (89.9) | 0.435 |
| CCB | 66 (14.7) | 24 (16.1) | 22 (14.7) | 20 (13.4) | 0.807 |
| High intensity statin at index PCI | 229 (51.0) | 60 (40.3) | 71 (47.3) | 98 (65.8) | <0.001 |
| High intensity statin at lipid follow-up | 190 (42.4) | 53 (35.6) | 57 (38.0) | 80 (53.7) | 0.003 |
| Procedural characteristics | |||||
| Multi vessel disease | 218 (48.6) | 77 (51.7) | 71 (47.3) | 70 (47.0) | 0.665 |
| Type b2/c lesions | 230 (51.2) | 71 (47.7) | 86 (57.3) | 73 (49.0) | 0.192 |
| PCI on LAD lesion | 301 (67.0) | 92 (61.7) | 109 (72.7) | 100 (67.1) | 0.132 |
| Lipid profile at index PCI | |||||
| TC (mg/dL) | 169.8 ± 35.9 | 151.4 ± 32.4 | 171.1 ± 33.6 | 186.8 ± 32.9 | <0.001 |
| TG (mg/dL) | 157.0 ± 117.1 | 153.4 ± 125.8 | 159.3 ± 124.0 | 158.4 ± 100.7 | 0.898 |
| HDL-C (mg/dL) | 43.9 ± 12.1 | 47.1 ± 14.3 | 44.9 ± 11.5 | 39.6 ± 8.75 | <0.001 |
| LDL-C (mg/dL) | 103.0 ± 31.9 | 82.0 ± 24.1 | 102.5 ± 28.5 | 124.6 ± 27.7 | <0.001 |
| Lp(a) (mg/dL) | 25.5 ± 26.7 | 27.1 ± 28.9 | 24.6 ± 26.0 | 25.0 ± 25.3 | 0.681 |
| Apo B (mg/dL) | 88.2 ± 23.6 | 70.9 ± 17.8 | 85.7 ± 17.4 | 107.9 ± 19.0 | <0.001 |
| Apo A1 (mg/dL) | 124.1 ± 26.5 | 132.9 ± 28.0 | 127.7 ± 26.4 | 111.8 ± 19.5 | <0.001 |
| Apo B/A1 ratio | 0.740 ± 0.249 | 0.549 ± 0.155 | 0.685 ± 0.138 | 0.985 ± 0.209 | <0.001 |
| Lipid profile at follow-up | |||||
| TC (mg/dL) | 113.5 ± 18.0 | 115.0 ± 19.6 | 114.0 ± 18.7 | 111.5 ± 15.4 | 0.231 |
| TG (mg/dL) | 113.6 ± 73.4 | 123.3 ± 86.3 | 110.6 ± 68.3 | 107.1 ± 63.1 | 0.134 |
| HDL-C (mg/dL) | 44.7 ± 13.1 | 42.6 ± 14.7 | 46.5 ± 13.0 | 44.9 ± 11.1 | 0.036 |
| LDL-C (mg/dL) | 56.0 ± 10.6 | 57.1 ± 9.5 | 55.6 ± 11.3 | 55.4 ± 10.9 | 0.295 |
| Lp(a) (mg/dL) | 25.7 ± 26.8 | 28.0 ± 26.8 | 25.2 ± 26.5 | 23.9 ± 27.2 | 0.406 |
| Apo B (mg/dL) | 57.9 ± 12.2 | 60.6 ± 12.6 | 56.3 ± 12.8 | 56.8 ± 10.7 | 0.003 |
| Apo A1 (mg/dL) | 125.8 ± 27.0 | 120.4 ± 29.6 | 130.9 ± 25.6 | 125.9 ± 24.6 | 0.003 |
| Apo B/A1 ratio | 0.485 ± 0.166 | 0.543 ± 0.217 | 0.447 ± 0.135 | 0.465 ± 0.113 | <0.001 |
Data are given as mean ± SD, or as number (%). ACEi; angiotensin converting enzyme inhibitor, Apo A1; apolipoprotein A1, Apo B; apolipoprotein B, ARB; angiotensin receptor blocker, BMI; body mass index, CCB; calcium channel blocker, DES; drug-eluting stent, EF; ejection fraction, eGFR; estimated glomerular filtration rate, HDL-C; high-density lipoprotein cholesterol, LAD; left anterior descending artery, LDL-C; low-density lipoprotein cholesterol, Lp(a); lipoprotein (a), PCI; percutaneous coronary intervention, TC; total cholesterol, TG; triglyceride.
The lipoprotein ratios and cardiovascular events
During the clinical follow-up, MACEs occurred in 115 patients. Kaplan-Meier curves of MACE survival rates by tertiles for the TC/HDL-C and Apo B/A1 ratios at lipid profile follow-up are summarized in Fig 2A and 2B, respectively. There were no significant differences in MACE survival rates between the tertiles for the TC/HDL-C ratio at lipid profile follow-up (Fig 2A). However, for the Apo B/A1 ratio at lipid profile follow-up, tertile 3 showed a significantly lower MACE survival rate compared to tertile 1 and tended to have a lower MACE survival rate compared to tertile 2 (Fig 2B). Kaplan-Meier curves of MACE survival rates by tertiles for decreases in TC/HDL-C and Apo B/A1 ratios that were observed between PCI and follow-up are summarized in Fig 2C and 2D, respectively. There were no significant differences in MACE survival rates between tertiles for the TC/HDL-C ratio decrease (Fig 2C). However, for the decrease in Apo B/A1 ratio, tertile 1 showed significantly lower MACE survival rate compared to tertile 2 and 3 (Fig 2D).
Fig 2.
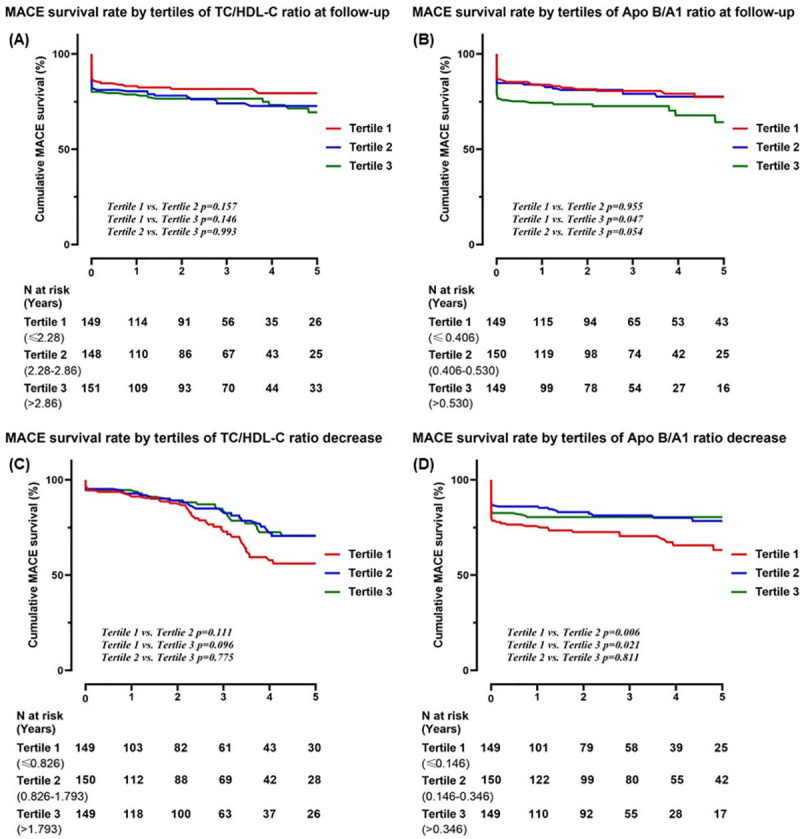
Kaplan-Meier curves of MACE survival rate by tertile of TC/HDL-C ratio at follow-up (A). Kaplan-Meier curves of MACE survival rate by tertile of Apo B/A1 ratio at follow-up (B). Kaplan-Meier curves of MACE survival rate by tertile of TC/HDL-C ratio decrease (C). Kaplan-Meier curves of MACE survival rate by tertile of Apo B/A1 ratio decrease (D). Apo A1; apolipoprotein A1, Apo B; apolipoprotein B, HDL-C; high-density lipoprotein cholesterol, MACE; major cardiovascular adverse event, TC; total cholesterol.
Kaplan-Meier curves of MACE survival rates by tertiles for Lp (a) at PCI and follow-up are summarized in Fig 3A and 3B, respectively. Kaplan-Meier curves of MACE survival rate by tertiles for decreases in Lp (a) levels between PCI and follow-up are summarized in Fig 3C. There were no significant differences in MACE survival rate among tertiles for Lp (a) levels at the time of PCI, follow-up, or for decreased Lp (a) levels between PCI and follow-up.
Fig 3.

Kaplan-Meier curves of MACE survival rate by tertile of Lp (a) at index PCI (A). Kaplan-Meier curves of MACE survival rate by tertile of Lp (a) at follow-up (B). Kaplan-Meier curves of MACE survival rate by tertile of Lp (a) decrease (C). Lp (a); lipoprotein (a), MACE; major cardiovascular adverse event, PCI; percutaneous coronary intervention.
The rates for individual MACE are summarized in Table 2 according to tertiles based on the decrease in the Apo B/A1 ratios between the PCI and follow-up. The overall MACE, any revascularization, and cardiac death rates were significantly higher in tertile 1 than in tertile 2 and 3. The rates for individual MACE according to TC/HDL-C ratio, Apo B/A1 ratio, Lp(a), and their decreases are summarized in S1–S3 Tables, respectively. We also performed analysis to evaluate whether or not the achievement of LDL lowering of more than 50% from baseline was associated with improved outcomes. As a result, the group in which LDL-C decreased by more than 50% showed a significantly lower incidence of MACE compared to the group in which LDL-C decreased by less than 50% (MACE rate: 21.2% vs 30.2%, p = 0.012). The rates for individual MACE according to % reduction of LDL-C is summarized in S4 Table.
Table 2. Clinical adverse events stratified by tertiles of Apo B/A1 ratio decrease.
| Variables | Tertile of Apo B/A1 ratio decrease | p-value | ||
|---|---|---|---|---|
| Tertile 1 ≤0.146 (n = 149) | Tertile 2 0.146–0.346 (n = 150) | Tertile 3 >0.346 (n = 149) | ||
| MACE | 51 (34.2) | 33 (22.0) | 31 (20.8) | 0.010 |
| Any revascularization | 47 (31.5) | 33 (22.0) | 30 (20.1) | 0.039 |
| Nonfatal-MI | 5 (3.4) | 4 (2.7) | 5 (3.4) | 0.854 |
| Ischemic stroke | 7 (4.7) | 3 (2.0) | 1 (0.7) | 0.132 |
| Cardiac death | 5 (3.4) | 1 (0) | 1 (0.7) | 0.033 |
Data are given as number (%) Apo A1; apolipoprotein A1, Apo B; apolipoprotein B, MACE; major cardiovascular adverse event (cardiac death, non-fatal myocardial infarction, any coronary revascularization and ischemic stroke), MI; myocardial infarction.
Independent predictors of MACEs and lower decrease in the Apo B/A1 ratio
According to multivariate analysis using Cox proportional hazards regression, the rate of MACE was independently increased by multi-vessel disease at the time of PCI and the lowest tertile for the decrease in the Apo B/A1 ratio (Table 3).
Table 3. Independent predictors for MACEs.
| Variable | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-value | HR | 95% CI | p-value | |
| Age | 1.007 | 0.989–1.025 | 0.435 | 1.005 | 0.986–1.025 | 0.622 |
| Male | 0.961 | 0.641–1.440 | 0.846 | 1.020 | 0.655–1.587 | 0.932 |
| Diabetes | 0.917 | 0.636–1.323 | 0.644 | |||
| Hypertension | 1.059 | 0.732–1.531 | 0.762 | |||
| Smoking hx | 0.959 | 0.664–1.386 | 0.825 | |||
| BMI | 1.021 | 0.964–1.081 | 0.473 | |||
| Ejection fraction | 0.993 | 0.978–1.009 | 0.416 | |||
| Multi vessel disease at index PCI | 1.583 | 1.092–2.295 | 0.015 | 1.529 | 1.053–2.221 | 0.026 |
| Type b2/c lesion at index PCI | 0.959 | 0.665–1.383 | 0.823 | |||
| Highest tertile of Apo B/ A1 ratio at lipid follow-up | 1.513 | 1.035–2.210 | 0.032 | 1.107 | 0.752–1.630 | 0.607 |
| Highest tertile of Lp (a) at lipid follow-up | 0.889 | 0.601–1.316 | 0.557 | |||
| Highest tertile of TC/HDL-C ratio at lipid follow-up | 1.168 | 0.801–1.702 | 0.421 | |||
| Lowest tertile of Apo B/A1 ratio decrease | 1.708 | 1.181–2.469 | 0.004 | 1.644 | 1.004–2.689 | 0.048 |
| Lowest tertile of Lp (a) decrease | 0.996 | 0.680–1.459 | 0.983 | |||
| Lowest tertile of TC/HDL-C ratio decrease | 1.430 | 0.986–1.430 | 0.059 | 1.049 | 0.642–1.712 | 0.850 |
| Non-high intensity statin at index PCI | 0.933 | 0.632–1.378 | 0.729 | |||
| Non-high intensity statin at lipid follow-up | 0.721 | 0.490–1.062 | 0.098 | 0.731 | 0.485–1.101 | 0.134 |
| ACE inhibitor/ARB | 0.773 | 0.467–1.278 | 0.315 | |||
| Beta blocker | 0.742 | 0.462–1.193 | 0.218 | |||
| CCB | 1.409 | 0.885–2.244 | 0.148 | |||
| First-generation DES | 0.597 | 0.323–1.102 | 0.099 | 0.671 | 0.354–1.274 | 0.223 |
ACE; angiotensin-converting enzyme, Apo A1; apolipoprotein A1, Apo B; apolipoprotein B, ARB; angiotensin receptor antagonist, BMI; body mass index, CCB; calcium channel blocker, CI; confidence interval, DES; drug-eluting stent, HR; hazard ratio, Lp (a); lipoprotein (a), MACEs; major cardiovascular adverse events, PCI; percutaneous coronary intervention.
According to the ROC analyses, the best predictive value for MACEs was Apo B/A1 ratio decrease ≤0.1633 ([AUC] = 0.575 p = 0.017, sensitivity 46.96%, specificity 69.37%). The AUC for Apo B/A1 ratio decrease was larger than that of TC/HDL-C ratio decrease, Lp (a) decrease and LDL-C decrease. (TC/HDL-C decrease: [AUC] = 0.560, p = 0.056, Lp (a) decrease: [AUC] = 0.485, p = 0.620, LDL-C decrease: [AUC] = 0.556, p = 0.072) In multivariate analysis using logistic regression, the lowest tertile of LDL-C (≤ 87.6 mg/dL) and use of non-high-intensity statins at the time of PCI were the independent predictors of the lowest tertile for the decrease in the Apo B/A1 ratio (Table 4).
Table 4. Independent predictors for lowest tertile of Apo B/A1 ratio decrease.
| Variable | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-value | OR | 95% CI | p-value | |
| Age | 1.013 | 0.994–1.032 | 0.183 | 0.988 | 0.966–1.012 | 0.328 |
| Male | 0.705 | 0.457–1.085 | 0.112 | 0.676 | 0.395–1.157 | 0.153 |
| Diabetes | 1.167 | 0.787–1.729 | 0.442 | |||
| Hypertension | 1.819 | 1.125–2.724 | 0.004 | 1.531 | 0.959–2.444 | 0.075 |
| Smoking hx | 1.121 | 0.755–1.664 | 0.570 | |||
| BMI | 0.987 | 0.927–1.051 | 0.692 | |||
| Lowest tertile of LDL-C at index PCI | 7.982 | 5.113–12.461 | <0.001 | 9.132 | 5.659–14.738 | <0.001 |
| Non-high intensity statin at index PCI | 1.928 | 1.293–2.875 | 0.001 | 2.458 | 1.195–5.056 | 0.015 |
| Non-high intensity statin at lipid profile follow up | 1.532 | 1.021–2.297 | 0.039 | 0.928 | 0.446–1.929 | 0.840 |
| ACE inhibitor/ARB | 0.861 | 0.484–1.531 | 0.610 | |||
| Beta blocker | 0.758 | 0.436–1.319 | 0.327 | |||
| CCB | 1.175 | 0.681–2.026 | 0.562 | |||
ACE; angiotensin-converting enzyme, Apo A1; apolipoprotein A1, Apo B; apolipoprotein B, ARB; angiotensin receptor antagonist, BMI; body mass index, CCB; calcium channel blocker, CI; confidence interval, LDL-C; low-density lipoprotein cholesterol, OR; odds ratio, PCI; percutaneous coronary intervention.
Discussion
The Apo B/A1 ratio is an indicator of the balance between atherogenic and atheroprotective cholesterol transport. High Apo B/A1 ratios have been associated with poor cardiovascular outcomes, including cardiac death, MI, and ischemic stroke [2, 6–12]. The Apo B/A1 ratio has been shown to predict cardiovascular risk more accurately than the TC/HDL-C ratio [2, 6]. The primary findings of our study are as follows: 1) the Apo B/A1 ratio demonstrated a greater predictive accuracy for clinical outcomes compared with the TC/HDL-C ratio and Lp (a) levels in patients who reached the target LDL-C level of ≤ 70 mg/dL 1 to 3 years after PCI. Particularly, we showed for the first time that a decrease in the Apo B/A1 ratio over time was a better clinical predictor than the absolute value of the Apo B/A1 ratio at follow-up in patients who achieved the target level of LDL-C after PCI. 2) The risk factors that predicted the lowest decrease in the Apo B/A1 ratio were low LDL-C levels and use of non-high-intensity statins after the PCI.
Previous studies have reported that high Lp (a) levels may be associated with a poor prognosis after PCI [4, 15, 16]. Contrary to previous studies, in our study, neither Lp (a) at PCI, Lp (a) at lipid follow-up, and Lp (a) decrease were suitable for predicting future clinical outcomes after PCI. Unlike our research, previous studies did not evaluate patients whose LDL-C levels fell below 70 mg/dL after PCI and statin use. In the present study, the mean LDL-C level of lipid profile follow-up was extremely low, 56.0 ± 10.6 mg/dL. Schmidt et al. [12] have reported that for subjects in the lowest LDL tertile, the risk of having a plaque in the femoral artery was three times greater for subjects in the highest Apo B/A1 tertile compared to subjects in the lowest Apo B/A1 tertile. Given these results, it seems that the Apo B/A1 ratio has a better prognosis prediction than Lp(a) for patients who have succeeded in lowering LDL-C level to below 70 mg/dL after PCI.
The results of a meta-analysis demonstrated that the percentage reduction of LDL-C is more important for secondary prevention than for the achievement of a target LDL-C level [18]. European guidelines have suggested lowering the LDL-C level to a specific target while achieving a ≥ 50% reduction in LDL-C for very high-risk patients [19]. The idea is to avoid insufficient lipid-lowering therapy in patients with atherosclerotic cardiovascular disease and a low baseline LDL-C level. In these patients, lowering the LDL-C level to <70 mg/dL (but without a ≥ 50% reduction) using low- or moderate-intensity statins may deny them the potential outcome benefit that could be obtained if they were treated with high-intensity statins [20]. In our study, which was conducted on patients whose LDL-C remained low below 70 after PCI, the LDL-C reduction group of 50% or more showed significantly better results than the LDL-C reduction group of 50% or less. These results emphasize the use of high-intensity statins regardless of baseline LDL-C level in patients undergoing PCI. We also demonstrated that decrease in the Apo B/A1 ratio over time was a better clinical predictor than the absolute value of the Apo B/A1 ratio. In our study, the AUC for Apo B/A1 ratio decrease was larger than that of LDL-C decrease. This observation indicates that the Apo B/A1 ratio decrease may give additional information in predicting cardiovascular risk, beyond that of LDL-cholesterol decrease.
Cho et al. [21] demonstrated that patients with low LDL-C level (< 70 mg/dL) at the time of acute MI showed the poorest clinical outcomes, which may be attributable to less statin use. Lee et al [22] also investigated the clinical outcomes of statin therapy in patients with acute MI whose LDL-C levels were <70mg/dl, and found that statin therapy was associated with improved clinical outcome compared to no statin therapy. However, the authors did not suggest an underlying mechanism for linking low LDL levels and less or no statin use to poor outcome. The present study demonstrated the independent predictors of the lowest decrease in Apo B/A1 ratios were the lowest LDL-C (≤ 87.6 mg/dL) and use of non-high-intensity statin after PCI, and a lower decrease in Apo B/A1 ratio led to poor clinical outcomes.
It has been reported that the decrease in the Apo B/A1 ratio varies depending on the type and intensity of statin or addition of ezetimibe. Patients who used high-intensity statins or added ezetimibe had a more reduced Apo B/A1 ratio than those who used non-high-intensity statins [23, 24]. Tani et al. [25] demonstrated that the decrease in the Apo B/A1 ratio in response to statin therapy is a simple predictor of coronary atherosclerotic regression. If the decrease of the Apo B/A1 ratio is not sufficient even when LDL-C reaches the target level, high intensity or combination of ezetimibe should be considered for the coronary plaque regression. Currently, target lipid levels are set mainly for LDL-C to improve outcomes after PCI; however, there are no clear target levels for other lipids, especially in patients who met the current LDL-C target level after PCI [1]. Although the best predictive value for MACEs was Apo B/A1 ratio decrease ≤0.1633 in our study, large-scale studies on target Apo B/A1 ratio decrease level should be conducted in the future. The results of our study suggest the need to pay close attention to the reduction of the Apo B/A1 ratio, even if the LDL-C criteria are met after PCI, and stricter lipid profile criteria should be applied to patients with low LDL-C levels at the time of the first PCI than patients with high LDL-C levels.
Our study had several limitations. First, because of the retrospective nature of this study, there were differences in duration for lipid and clinical follow-up for each patient. However, this study was conducted with patients who had good treatment compliance and arrived at the target LDL-C 1 to 3 year after statin use, and the clinical follow-up duration (median 38.0 months) was long enough to assess the effects of the decrease in the Apo B/A1 ratio. Second, this study was a single-center study and was conducted with a relatively small number of patients. Third, since the type of statins could be changed during clinical follow-up at the discretion of the physician, it was difficult to evaluate the effects of these statin changes on the lipid profiles and future clinical outcomes.
Conclusions
The Apo B/A1 ratio had greater predictive accuracy for clinical outcomes compared with the TC/HDL-C ratio and Lp (a) after PCI. A lower decrease in the Apo B/A1 ratio over time can be a residual risk factor of MACE in patients who have reached LDL-C levels below 70 mg/dL after PCI.
Supporting information
(DOCX)
(DOCX)
(DOCX)
(DOCX)
Data Availability
All relevant data are within the manuscript and its S1–S4 Tables.
Funding Statement
This work was supported by research grant from Daegu Catholic University Medical Center.
References
- 1.Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. 2019;139(25):e1082–e143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tian M, Li R, Shan Z, Wang DW, Jiang J, Cui G. Comparison of Apolipoprotein B/A1 ratio, Framingham risk score and TC/HDL-c for predicting clinical outcomes in patients undergoing percutaneous coronary intervention. Lipids Health Dis. 2019;18(1):202. doi: 10.1186/s12944-019-1144-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ljungberg J, Holmgren A, Bergdahl IA, Hultdin J, Norberg M, Näslund U, et al. Lipoprotein(a) and the Apolipoprotein B/A1 Ratio Independently Associate With Surgery for Aortic Stenosis Only in Patients With Concomitant Coronary Artery Disease. Journal of the American Heart Association.6(12):e007160. doi: 10.1161/JAHA.117.007160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Suwa S, Ogita M, Miyauchi K, Sonoda T, Konishi H, Tsuboi S, et al. Impact of Lipoprotein (a) on Long-Term Outcomes in Patients with Coronary Artery Disease Treated with Statin After a First Percutaneous Coronary Intervention. Journal of atherosclerosis and thrombosis. 2017;24(11):1125–31. doi: 10.5551/jat.38794 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Millán J, Pintó X, Muñoz A, Zúñiga M, Rubiés-Prat J, Pallardo LF, et al. Lipoprotein ratios: Physiological significance and clinical usefulness in cardiovascular prevention. Vasc Health Risk Manag. 2009;5:757–65. [PMC free article] [PubMed] [Google Scholar]
- 6.Walldius G, Jungner I, Holme I, Aastveit AH, Kolar W, Steiner E. High apolipoprotein B, low apolipoprotein A-I, and improvement in the prediction of fatal myocardial infarction (AMORIS study): a prospective study. Lancet (London, England). 2001;358(9298):2026–33. [DOI] [PubMed] [Google Scholar]
- 7.McQueen MJ, Hawken S, Wang X, Ounpuu S, Sniderman A, Probstfield J, et al. Lipids, lipoproteins, and apolipoproteins as risk markers of myocardial infarction in 52 countries (the INTERHEART study): a case-control study. Lancet (London, England). 2008;372(9634):224–33. [DOI] [PubMed] [Google Scholar]
- 8.Zhan X, Chen Y, Yan C, Liu S, Deng L, Yang Y, et al. Apolipoprotein B/apolipoprotein A1 ratio and mortality among incident peritoneal dialysis patients. Lipids in Health and Disease. 2018;17(1):117. doi: 10.1186/s12944-018-0771-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kostapanos MS, Christogiannis LG, Bika E, Bairaktari ET, Goudevenos JA, Elisaf MS, et al. Apolipoprotein B-to-A1 ratio as a predictor of acute ischemic nonembolic stroke in elderly subjects. Journal of stroke and cerebrovascular diseases: the official journal of National Stroke Association. 2010;19(6):497–502. doi: 10.1016/j.jstrokecerebrovasdis.2009.09.010 [DOI] [PubMed] [Google Scholar]
- 10.Dong H, Chen W, Wang X, Pi F, Wu Y, Pang S, et al. Apolipoprotein A1, B levels, and their ratio and the risk of a first stroke: a meta-analysis and case-control study. Metabolic brain disease. 2015;30(6):1319–30. doi: 10.1007/s11011-015-9732-7 [DOI] [PubMed] [Google Scholar]
- 11.Emoto T, Sawada T, Morimoto N, Tenjin T, Wakimoto T, Ikeda F, et al. The apolipoprotein B/A1 ratio is associated with reactive oxygen metabolites and endothelial dysfunction in statin-treated patients with coronary artery disease. Journal of atherosclerosis and thrombosis. 2013;20(7):623–9. doi: 10.5551/jat.16824 [DOI] [PubMed] [Google Scholar]
- 12.Schmidt C, Fagerberg B. ApoB/apoA-I ratio is related to femoral artery plaques in 64-year-old women also in cases with low LDL cholesterol. Atherosclerosis. 2008;196(2):817–22. doi: 10.1016/j.atherosclerosis.2007.01.017 [DOI] [PubMed] [Google Scholar]
- 13.Calling S, Johansson SE, Wolff M, Sundquist J, Sundquist K. The ratio of total cholesterol to high density lipoprotein cholesterol and myocardial infarction in Women’s health in the Lund area (WHILA): a 17-year follow-up cohort study. BMC cardiovascular disorders. 2019;19(1):239. doi: 10.1186/s12872-019-1228-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Holman RR, Coleman RL, Shine BS, Stevens RJ. Non-HDL cholesterol is less informative than the total-to-HDL cholesterol ratio in predicting cardiovascular risk in type 2 diabetes. Diabetes care. 2005;28(7):1796–7. doi: 10.2337/diacare.28.7.1796 [DOI] [PubMed] [Google Scholar]
- 15.Konishi H, Miyauchi K, Kasai T, Tsuboi S, Ogita M, Naito R, et al. Impact of lipoprotein(a) as residual risk on long-term outcomes in patients after percutaneous coronary intervention. The American journal of cardiology. 2015;115(2):157–60. doi: 10.1016/j.amjcard.2014.10.015 [DOI] [PubMed] [Google Scholar]
- 16.Kwon S, Lee B, Hong B-K, Kim J-Y, Choi E-Y, Sung J, et al. Prognostic significance of elevated lipoprotein(a) in coronary artery revascularization patients. International journal of cardiology. 2013;167:1990–4. doi: 10.1016/j.ijcard.2012.05.007 [DOI] [PubMed] [Google Scholar]
- 17.Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. Third universal definition of myocardial infarction. Journal of the American College of Cardiology. 2012;60(16):1581–98. doi: 10.1016/j.jacc.2012.08.001 [DOI] [PubMed] [Google Scholar]
- 18.Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet (London, England). 2010;376(9753):1670–81. doi: 10.1016/S0140-6736(10)61350-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). European Heart Journal. 2020;41(1):111–88. doi: 10.1093/eurheartj/ehz455 [DOI] [PubMed] [Google Scholar]
- 20.Lee SH. We can do much better than what we did FAU. Korean J Intern Med. 2020;35(3):547–549. doi: 10.3904/kjim.2020.130 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cho KH, Jeong MH, Ahn Y, Kim YJ, Chae SC, Hong TJ, et al. Low-density lipoprotein cholesterol level in patients with acute myocardial infarction having percutaneous coronary intervention (the cholesterol paradox). The American journal of cardiology. 2010;106(8):1061–8. doi: 10.1016/j.amjcard.2010.06.009 [DOI] [PubMed] [Google Scholar]
- 22.Lee KH, Jeong MH, Kim HM, Ahn Y, Kim JH, Chae SC, et al. Benefit of Early Statin Therapy in Patients With Acute Myocardial Infarction Who Have Extremely Low Low-Density Lipoprotein Cholesterol. Journal of the American College of Cardiology. 2011;58(16):1664–71. doi: 10.1016/j.jacc.2011.05.057 [DOI] [PubMed] [Google Scholar]
- 23.Jones PH, Hunninghake DB, Ferdinand KC, Stein EA, Gold A, Caplan RJ, et al. Effects of rosuvastatin versus atorvastatin, simvastatin, and pravastatin on non-high-density lipoprotein cholesterol, apolipoproteins, and lipid ratios in patients with hypercholesterolemia: additional results from the STELLAR trial. Clinical therapeutics. 2004;26(9):1388–99. doi: 10.1016/j.clinthera.2004.09.006 [DOI] [PubMed] [Google Scholar]
- 24.Hong SJ, Jeong HS, Ahn JC, Cha D-H, Won KH, Kim W, et al. A Phase III, Multicenter, Randomized, Double-blind, Active Comparator Clinical Trial to Compare the Efficacy and Safety of Combination Therapy With Ezetimibe and Rosuvastatin Versus Rosuvastatin Monotherapy in Patients With Hypercholesterolemia: I-ROSETTE (Ildong Rosuvastatin & Ezetimibe for Hypercholesterolemia) Randomized Controlled Trial. Clinical therapeutics. 2018;40(2):226–41.e4. doi: 10.1016/j.clinthera.2017.12.018 [DOI] [PubMed] [Google Scholar]
- 25.Tani S, Nagao K, Anazawa T, Kawamata H, Furuya S, Takahashi H, et al. Relation of change in apolipoprotein B/apolipoprotein A-I ratio to coronary plaque regression after Pravastatin treatment in patients with coronary artery disease. The American journal of cardiology. 2010;105(2):144–8. doi: 10.1016/j.amjcard.2009.08.670 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX)
(DOCX)
(DOCX)
(DOCX)
Data Availability Statement
All relevant data are within the manuscript and its S1–S4 Tables.