

Abstract
Background
Cam morphology is thought to originate near puberty and reflects a response of the peripheral aspect of the proximal femoral physis to increased local load. Participation in particular sports activities has been associated with cam morphology in contemporary patient populations; however, it is unclear whether cam is a recent phenomenon. There are limited data regarding the frequency of its occurrence and the general deviations in femoral anatomy in different historical populations. Such information may help to understand the possible influence of lifestyle and diet on cam morphology.
Questions/purposes
The purpose of this study was to evaluate femoral morphology in three historical populations. We asked: (1) Was cam morphology present in the three study populations, did those populations differ, and were there differences between sexes? (2) Were there differences in neck-shaft angle, version, or inclination between and among the examined populations?
Methods
We examined 204 adult femurs from the Neolithic population from Iran (n = 37, 3000 BC to 1631 BC), medieval population from Poland (n = 135, 10th to 13th centuries), and contemporary Australian aborigines (n = 32, early 20th century), provided by the Open Research Scan Archive, Museum of the First Piasts at Lednica and the University of Wrocław, respectively. All three human populations represent different chronologic periods and lifestyles. All bones were scanned using CT and then measured on their three-dimensional (3-D) reconstructions in selected planes. Cam impingement was defined as an alpha angle > 55° measured on the inclination view. To evaluate the differences in anatomy between populations, we measured the true neck-shaft angle on the true AP view, apparent neck-shaft angle on the apparent AP view, the version angle on the version view, and the inclination angle on the inclination view. The prevalence of cam morphology and other anatomic parameters were compared among groups using chi-square test, one-way ANOVA with post hoc Tukey test, and paired t-test.
Results
Cam morphology was present in 5% of the Neolithic population from Iran, in 7% of the medieval population from Poland, and 3% of the contemporary Australian aborigine femurs (OR Neolithic population from Iran/the medieval population from Poland 0.7 [95% CI 0.2 to 3.4]; p = 0.67; OR Neolithic population from Iran/contemporary Australian aborigines 1.8 [95% CI 0.2 to 20.5]; p = 0.65; OR the medieval population from Poland/contemporary Australian aborigines 2.5 [95% CI 0.3 to 20.1]; p = 0.40). There were differences in the presence of cam morphology between the sexes in the medieval population from Poland with both femurs (females: 1% [1 of 76]; males: 15% [9 of 59]; p = 0.002). There was a difference in true neck-shaft angle between the Neolithic population from Iran (121° ± 6°) and contemporary Australian aborigines (131° ± 5°; mean difference 10° [95% CI 7° to 13°]; p < 0.001) and between the medieval population from Poland (124° ± 5°) and the contemporary Australian aborigines (mean difference 7° [95% CI 5° to 9°]; p < 0.001). Apparent neck-shaft angle differed between the Neolithic population from Iran (126° ± 6°) and the contemporary Australian aborigines (134° ± 5°; mean difference 8° [95% CI 6° to 11°]; p < 0.001), and between the medieval population from Poland (126° ± 6°) and the contemporary Australian aborigines (mean difference 9° [95% CI 7° to 11°]; p < 0.001). Moreover, we observed a difference in the version angle between the Neolithic population from Iran (19° ± 7°) and the medieval population from Poland (12° ± 9°; mean difference 7° [95% CI 4° to 10°]; p < 0.001] and in the inclination angle between aforementioned groups (18° ± 7° versus 11° ± 8°; mean difference 7° [95% CI 5° to 10°]; p < 0.001).
Conclusion
This study found that cam morphology existed in historical populations at rates comparable with a contemporary population.
Clinical Relevance
The presence of cam morphology in historical populations suggests that cam morphology can develop outside of the intense sports activity seen in modern adolescents. Further study will help elucidate the etiology of cam morphology, which may be useful in the development of preventive strategies.
Introduction
Femoroacetabular impingement is a dynamic process related to abnormal, iterative contact between the rim of the acetabulum and the junction between the femoral head and neck. The most common type of femoroacetabular impingement comes from an aspherical prominence at the proximal femur known as cam morphology. Cam is a recognized cause of hip pain in young adults and has been correlated with the development of osteoarthritis [20, 26]. Studies have suggested that cam morphology originates near puberty and reflects a response of the peripheral aspect of the proximal femoral physis to increased local load [16, 17]. Accordingly, cam morphology has been correlated with multiple sports activities, including soccer, hockey, football, volleyball, and track and field [16].
To evaluate the relationship between cam morphology and modern lifestyles, Moats et al. [14] compared a population from more than 1000 years ago with a population from approximately 100 years ago and found cam morphology only in the latter population. The authors were unsure whether this represented differences in activity, diet, or other factors. To our knowledge, no other study of ancient populations has reproduced Moats et al.’s [14] findings in a different cohort. Interestingly, a recent radiologic evaluation of a single specimen by Zurmühle et al. [27] found that cam morphology existed as early as 5000 years ago. Nevertheless, the case report by Zurmühle et al. [27] might have overemphasized the presence of cam morphology in ancient populations. Of note, there are secondary causes of cam morphology such as a subtle slip, noted to occur in 12% of patients with cam morphology who underwent surgery in the study by Albers et al. [1], and it is potentially challenging to differentiate in an osteologic specimen without cartilage. Given this, it is difficult to make conclusions about whether primary cam existed historically based on a single specimen. Such information could help determine whether cam morphology is a recent phenomenon associated primarily with sports-related contemporary activities or if a more extensive range of lifestyles might also lead to cam morphology.
The purpose of this study was to evaluate femoral morphology in three populations (Neolithic population from Iran, Medieval population from Poland, and contemporary Australian aborigines). We asked: (1) Was cam morphology present in the three study populations, did those populations differ, and were there differences between sexes? (2) Were there differences in neck-shaft angle, version, or inclination between and among the examined populations?
Materials and Methods
Population Groups
The analyzed bones consisted of 204 femurs from adult individuals from three human populations representing different chronologic periods and lifestyles. The first group (the Neolithic population from Iran) is derived from the archaeological site of Tepe Hissar in Iran and is dated to the Neolithic period (3000 BC to 1631 BC). Due to the poor preservation of skeletons, only 18 left and 19 right femurs from 37 adult individuals were selected for this research. According to archaeological and anthropological data, the subsistence economy of this Neolithic population from Iran was mainly based on agriculture and animal husbandry [2]. In turn, the isotopic data show that the society at Tepe Hissar had a stable social structure and adequate food resources across all periods [2]. However, the lifestyle and diet of this population is still being investigated, and the femurs were shared by the Open Research Scan Archive. The second group (medieval population from Poland) came from a medieval site in Ostrów Lednicki, Poland, which was occupied from the 10th to the 13th centuries [5]. Within this group, 135 adult femurs, which belonged to 38 females (38 left and 38 right femurs) and 33 males (29 left and 30 right femurs), were available for the current study. Inhabitants of this settlement complex relied mainly on agriculture and partly on breeding domestic animals such as pigs, goats, chickens [12, 19]. This was a homogeneous population in terms of socioeconomic structure, with a division of labor wherein females were responsible for raising children, weaving, helping in the harvest, and breeding animals in turn, with male activities focused on lowing, harvesting, and building operations [12]. The femurs of the medieval population from Poland were shared by the Museum of the First Piasts at Lednica. The third population (contemporary Australian aborigines) consisted of 32 individuals of contemporary aborigines who occupied West and South Australia at the beginning of the 20th century [11]. The number of femora of contemporary Australian aborigines was very limited; 32 adult femurs that belonged to 14 females and 18 males were selected for this research. These femurs were shared by the University of Wrocław.
The femoral measurements used in this study required very good preservation of the bone, especially the femoral head, lateral and medial condyles, and lesser and greater trochanters, as these anatomical features are necessary to correctly measure the alignment of the femur. As a result of taphonomic processes, the articular surfaces degrade over time; nevertheless, the osteological material used in this research included well-preserved femurs of most individuals from all three populations.
Primary and Secondary Study Outcomes
Our primary study goal was to determine whether the cam morphology was present in the three studied populations, did those populations differ, and were there differences between sexes within the particular populations. To achieve this, we searched for the existence of cam morphology defined as alpha angle > 55o measured on the inclination view.
Our secondary study goal was to assess whether there were differences in the proximal femoral anatomy among the three populations. To answer this question, we analyzed multiple parameters: the true neck-shaft angle on the true AP view, the neck-shaft angle on the apparent AP view, the version angle on the version view, and the inclination angle on the inclination view. This allowed us to assess whether trends in proximal femoral anatomy in our populations matched those previously reported in the evidence.
Morphologic and Image Analysis
The sex and approximate age of the individuals from the medieval population from Poland and the contemporary Australian aborigines were assessed using morphologic features of the skull and pelvis [4] (see Table 1; Supplemental Digital Content 1, http://links.lww.com/CORR/A552). In the Neolithic population from Iran, all individuals were classified as having an unknown sex because there was a lack of bones other than femurs that could be assessed. All femurs analyzed in this study had no observable pathologic changes such as fractures, osteophytes, or porosity.
The incidence of cam morphology was assessed by measuring the alpha angle in the inclination view. An angle > 55° was considered indicative of the cam morphology, based on previous anatomical studies [15, 17] and with the goal of setting a more stringent value than > 50° as used by Moats et al. [14]. Moreover, we measured the true neck-shaft angle on the true AP view, the neck-shaft angle on the apparent AP view, the version angle on the version view, and the inclination angle on the inclination view to evaluate the differences in anatomy between populations. These four parameters are most commonly used to describe the overall femur morphology. Although apparent and true neck-shaft angles are similar and mathematically related, as are version and inclination, we decided to measure all four parameters for completeness and potential future comparison to our data.
The bones were scanned using 32-slice CT (Siemens SOMATOM Sensation) in the same craniocaudal position, with the femur resting on the posterior aspect of the medial and lateral femoral condyles distally and the posterior aspect of the greater trochanter proximally, using a standard protocol (0.625 mm3 х 0.625 mm3 х 0.625 mm3 cubic voxels) [12]. For each bone, a 3-D reconstruction was prepared using InVesalius software (version 3.1.1; Centro de Tecnologia da Informação Renato Archer). The 3-D reconstruction for each femur was then set in four basic positions (two AP and two axial views) that were captured and used for measuring the following parameters: First, the apparent AP view was obtained while looking down at the femur from the front, which rested on the virtual surface on the greater trochanter and femoral condyles (Fig. 1A). Second, the true AP view was obtained by starting with the apparent AP view and then rotating the femur on the axis of the shaft such that the femoral neck was horizontal and in a plane parallel to the virtual surface (Fig. 1B). Third, the version view was obtained by starting with the apparent AP view, and then it was switched to an orthogonal axial viewpoint looking at the femur from cephalad and viewing down the femoral shaft (parallel to the femoral shaft) (Fig. 1C). Finally, the inclination view was obtained by starting with the version view and then abducting the femur such that the femoral neck was set perpendicular to the viewpoint (Fig. 1D). The inclination view mirrors the special MRI view described by Nötzli et al. [21].
Fig. 1.
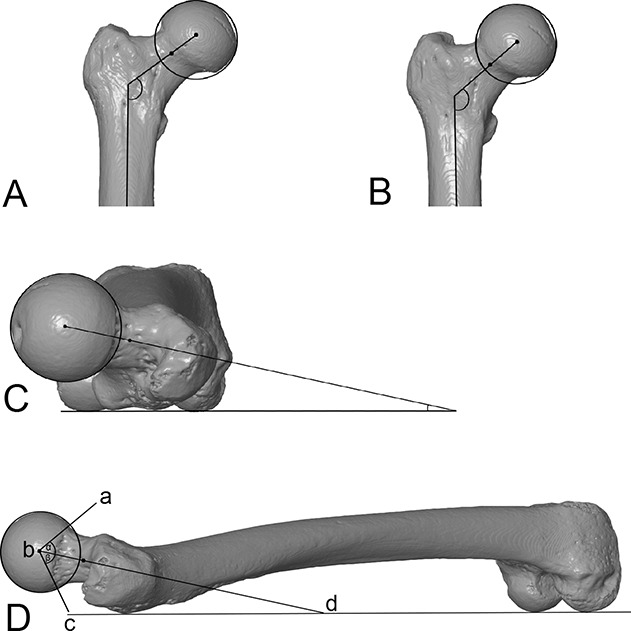
A-D This figure shows the femoral measurements: (A) the true neck-shaft angle measured on the true AP view, (B) the apparent neck-shaft angle measured on the apparent AP view, (C) the version angle measured on the version view, and (D) the inclination angle (defined between line b-c and the bottom horizontal line connecting the posterior aspects of the greater trochanter and distal femoral condyles) and the alpha angle (defined between points a, b, and c) measured on the inclination view.
Finally, the following parameters were measured in these views using ImageJ software (National Institutes of Health and the Laboratory for Optical and Computational Instrumentation) [24]: First, the apparent neck-shaft angle was measured on the apparent AP view. The angle is formed by the crossing of two lines: the femoral neck axis line passing through the center of the best-fit circle of the femoral head and the center of the narrowest part of the femoral neck, and the long axis of the femoral shaft (Fig. 1B). Second, the true neck-shaft angle was measured on the true AP view. This angle is formed by the crossing of the femoral neck axis and the long axis of the femoral shaft (Fig. 1A). Third, the version angle was measured on the version view. The angle is formed by the femoral neck axis and a line parallel to the posterior aspect of the femoral condyles (Fig. 1C). Fourth, the inclination angle was measured on the inclination view. The angle is formed by the femoral neck axis and a line parallel to the posterior aspect of the femoral condyles (Fig. 1D). Finally, the alpha angle was measured on the inclination view. The angle is formed by a line representing the femoral neck axis and a line from the center of the femoral head to the point at which the femoral head-neck junction exits the best-fit circle of the femur’s head (Fig. 1D). We did not note any cases where the femoral head was not in line with the axis of the neck.
The femora were digitally reconstructed and positioned, and images were recorded in the four basic views by one researcher (AMK). Then, the femoral measurements were performed by two orthopaedic surgeons (BJM, ŁW) experienced in the femoral parameters used in this study.
Ethical Approval
Ethical approval for this study was waived by Bioethics Committee at Poznan University of Medical Sciences.
Statistical Analysis
To calculate the interobserver error, two independent researchers (ŁW, BJM) performed the measurements for 20 randomly selected femurs. The intraobserver error was estimated for one researcher (BJM), who repeated the femoral measurements after 1 month. The level of technical measurement error was calculated using the intraclass correlation coefficient, with values less than 0.40, between 0.40 and 0.59, between 0.60 and 0.74, and greater than 0.75 indicating poor, moderate, good, and excellent reliability, respectively [23]. The intraclass correlation coefficient values demonstrated good-to-excellent reliability of measurements between and within researchers (Table 1).
Table 1.
Intraclass correlation coefficient values for each femur measurement
| Measurement | Interobserver reliability | Intraobserver reliability |
| True NSA | 0.962 | 0.927 |
| Apparent NSA | 0.921 | 0.854 |
| Version angle | 0.984 | 0.969 |
| Inclination angle | 0.995 | 0.991 |
| Alpha angle | 0.853 | 0.727 |
NSA = neck-shaft angle.
The data were tested for normality and homogeneity of variances using the Shapiro-Wilk test and or the Levene test, respectively. The femoral measurements fulfilled the criteria for normality and homogeneity of variances, and parametric tests were used for further statistical analysis. Differences in the presence of cam morphology between populations and sexes were analyzed using a chi-square test. We used one-way ANOVA with a post hoc Tukey test to analyze which of the femoral parameters differed among the three populations. To examine differences in the measurements between sides of the body, we performed a paired t-test only for individuals with both the left and right femur preserved. Because of many comparisons, the significance level of the chi-square test, ANOVA, and a post hoc Tukey test was corrected using a Bonferroni correction by dividing the p value cutoff (0.05) by the number of tests. All statistical analyses were performed using R software (version 4.0.3, The R Foundation).
Results
Frequency of Cam Morphology in Three Populations
Cam morphology was present in all three study populations, but there were no differences in terms of its frequency (5% [2 of 37], 7% [10 of 135], and 3% [1 of 32], respectively; OR (Neolithic population from Iran/medieval population from Poland 0.7 [95% CI 0.2 to 3.4]; p = 0.67; OR (Neolithic population from Iran/contemporary Australian aborigines 1.8 [95% CI 0.2 to 20.5]; p = 0.65; OR (medieval population from Poland/contemporary Australian aborigines 2.5 [95% CI 0.3 to 20.1]; p = 0.40) (Fig. 2).
Fig. 2.
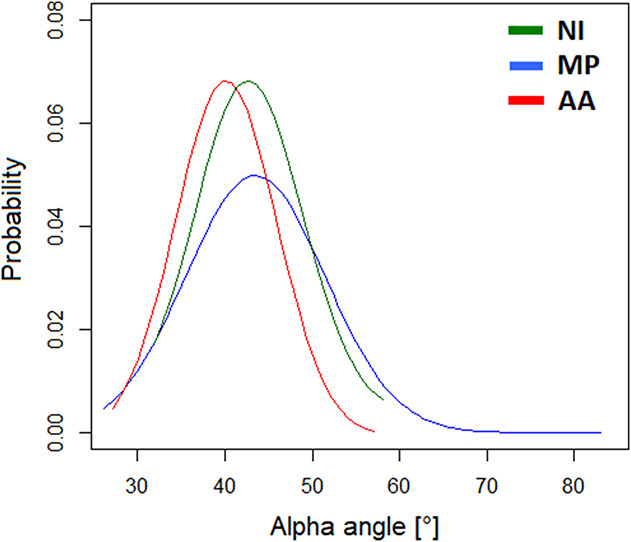
This graph shows the probability of the alpha angles in the Neolithic population from Iran (NI), the medieval population from Poland (MP), and the Australian aborigines (AA). A color image accompanies the online version of this article.
There were differences in the presence of cam morphology between the sexes only in the medieval population from Poland (Table 2). In males it was present in 15% (9 of 59) of femora, while in females in 1% (1 of 76) of femora (p = 0.002).
Table 2.
Femurs with cam morphology in studied populations
| Value | Left | p value | Right | p value | Total | p value |
| Neolithic population from Iran (n = 37) | ||||||
| Unknown sex | 6 (1 of 18) | 5 (1 of 19) | 5 (2 of 37) | |||
| Medieval population from Poland (n = 135) | ||||||
| Females | 3 (1 of 38) | 0.19 | 0 (0 of 38) | < 0.001 | 1 (1 of 76) | 0.002 |
| Males | 10 (3 of 29) | 20 (6 of 30) | 15 (9 of 59) | |||
| Australian aborigines (n = 32) | ||||||
| Females | 0 (0 of 5) | 0.46 | 0 (0 of 9) | 0 (0 of 14) | 0.37 | |
| Males | 10 (1 of 10) | 0 (0 of 8) | 6 (1 of 18) | |||
Data presented as % (n).
Differences in Other Femoral Measurements Among the Study Populations
The apparent neck-shaft angle was larger in the contemporary Australian aborigines than in the Neolithic population from Iran (134° ± 5° versus 126° ± 6°, mean difference 8° [95% CI 6° to 11°; p < 0.001), and in the contemporary Australian aborigines than in the medieval population from Poland (134° ± 5° versus 126° ± 6°, mean difference 9° [95% CI 7° to 11°]; p < 0.001) (Table 3). The true neck-shaft angle was larger in the contemporary Australian aborigines than in the Neolithic population from Iran (131° ± 5° versus 121° ± 6°, mean difference 10° [95% CI 7° to 13°]; p < 0.001) and in the contemporary Australian aborigines than in the medieval population from Poland (131° ± 5° versus 124° ± 5°, mean difference 7° [95% CI 5° to 9°]; p < 0.001). The version angle was larger in the Neolithic population from Iran than in the medieval population from Poland (19° ± 7° versus 12° ± 9°, mean difference 7° [95% CI 4° to 10°]; p < 0.001). The inclination angle was larger in the Neolithic population from Iran than in the medieval population from Poland (18° ± 7° versus 11° ± 8°, mean difference 7° [95% CI 5° to 10°]; p < 0.001) (Table 3).
Table 3.
Descriptive statistics (in degrees) and post hoc Tukey test results of femur measurement comparisons between populations
| Parameter | Neolithic population from Iran (n = 37) | Medieval population from Poland (n = 135) | Australian aborigines (n = 32) | ||||||
| Mean ± SD | Mean difference vs Australian aborigines (95% CI) | p value for Neolithic population from Iran vs Australian aborigines | Mean ± SD | Mean difference vs Neolithic population from Iran (95% CI) | p value for medieval population from Poland vs Neolithic population from Iran | Mean ± SD | Mean difference vs medieval population from Poland (95% CI) | p value for Australian aborigines vs medieval population from Poland | |
| True NSA | 121 ± 6 | 10 (7-13) | < 0.001 | 124 ± 5 | 3 (1-5) | 0.01 | 131 ± 5 | 7 (5-9) | < 0.001 |
| Apparent NSA | 126 ± 6 | 8 (6-11) | < 0.001 | 126 ± 6 | 0 (-2 to 3) | 0.94 | 134 ± 5 | 9 (7-11) | < 0.001 |
| Version angle | 19 ± 7 | 4 (0-8) | 0.09 | 12 ± 9 | 7 (4-10) | < 0.001 | 15 ± 10 | 3 (0-6) | 0.19 |
| Inclination angle | 18 ± 7 | 6 (3-9) | 0.01 | 11 ± 8 | 7 (5-10) | < 0.001 | 12 ± 8 | 1 (-2 to 4) | 0.40 |
| Alpha angle | 44 ± 6 | 4 (1-7) | 0.19 | 44 ± 8 | 0 (-3 to 3) | 0.99 | 40 ± 6 | 4 (1-6) | 0.09 |
NSA = neck-shaft angle.
There were no differences in the alpha angle measurements between the three populations (Fig. 2) with the numbers available (Table 3). Moreover, there were no differences in femoral parameters between sides of the body (see Table 2; Supplemental Digital Content 2, http://links.lww.com/CORR/A553).
Discussion
This study was designed to address the reported inconsistencies regarding cam morphology in historical populations. Moats et al. [14] found no cam morphology in the population from 1000 years ago, while a single specimen studied by Zurmühle et al. [27] suggests that it existed as early as 5000 years ago. Given that it is difficult to make conclusions about whether primary cam existed historically based on a single specimen, our purpose was to search for evidence of cam morphology in the Neolithic population from Iran, the medieval population from Poland, and the contemporary Australian aborigine population. Moreover, we evaluated the difference in occurrence by sex and the difference in proximal femoral anatomy between these groups. Our assessment found cam morphology in all groups, with no difference in prevalence among the three populations and no differences in the alpha angle values between the three populations. This demonstrates that cam morphology is not a purely modern phenomenon. In addition, an increase in the proportions of males versus females with cam morphology was noted in the medieval population from Poland. Our findings of a higher neck-shaft angle (both true and apparent) in a population in a warmer climate (the contemporary Australian aborigines) and higher femoral version in a more ancient population (the Neolithic population from Iran) highlight the environmental influence on skeletal development. Overall, this study suggests that activities other than sports can put an adolescent proximal femur at risk for cam morphology.
Limitations
Our study is limited by a relatively small number of femora from each of the three study populations. This was because of the scarcity of such historical collections and the need for femoral specimens that were intact at the proximal and distal ends. This limited our comparative analysis. Furthermore, the populations were from different regions of the world, which influenced their relative lifestyles and genetic backgrounds. On the other hand, our analysis of historical populations allowed us to investigate whether cam morphology was present in older populations before it was present in contemporary populations. We attempted to maximize our data by obtaining 3-D reconstructions to measure each specimen. We were also limited in our lack of sex data in the Neolithic population from Iran. Although differences in femoral condylar shape have been described between males and females [7], there is enough overlap between sexes that we could not use such data to discriminate the sex of each individual. Finally, although each population’s general physical activities (agricultural or a hunter-gatherer society) are known, the individual lifestyle of each person was not known, and with the small cohort sizes, these details may have an important effect on femur morphology, such as changes in version arising from different sitting positions. However, prehistoric and historic populations were much more homogeneous in terms of lifestyle than modern populations were, and this effect was likely small [12].
Frequency of Cam Morphology in Three Populations
Our results demonstrate that cam morphology can occur in populations spanning from 100 years to 5000 years ago (Fig. 3). Moats et al. [14] found different results in 249 femora in 175 individuals from approximately 1000 years ago; these people had lower alpha angle values than an osteological collection in Cleveland, OH, USA, from 100 years ago did, with mean alpha angles of 35° versus 46°, respectively. Notably, there were no cases of cam morphology in the older population, defined as an alpha angle greater than 50°. Our study, in contrast, found cam morphology in multiple collections, with the differences potentially due to activity, dietary, or genetic differences.
Fig. 3.
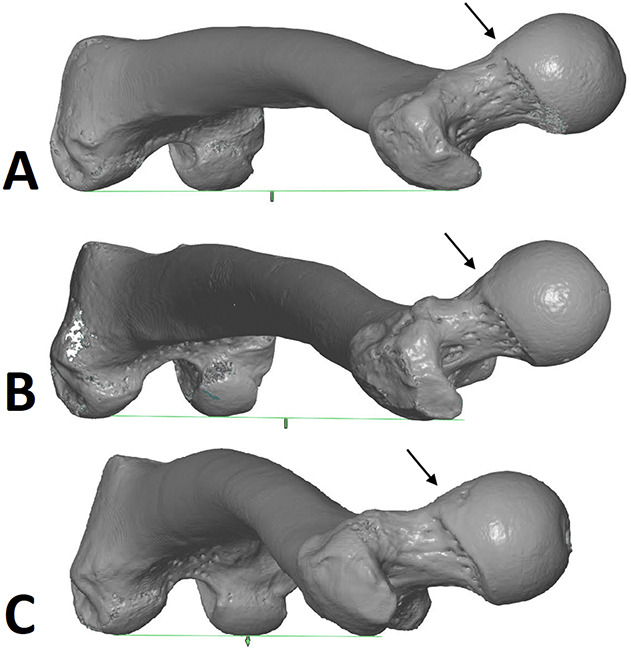
A-C These images show examples of bones with cam morphology among (A) the Neolithic population from Iran, (B) the Australian aboriginal people, and (C) the medieval population from Poland. Arrows indicate the area of cam morphology.
We found higher alpha angles and a higher prevalence of cam morphology in males than in females only in the medieval group. The increased prevalence in males is well reported among contemporary patient populations [13, 16, 22]. With the theory that cam morphology develops around the time of puberty because the proximal femoral physis forms extra bone to stabilize a relatively weak physis, it is often postulated that males have a higher proportion of cam morphology than females because of increased activity levels [16]. However, females are susceptible to increases in the alpha angle approximately 2 years earlier than males [17], at an age when overall activity levels and sports participation are less intense, which may also explain sex-based differences.
The biological diversity of human populations may have also played a role in the prevalence of cam morphology in this study. Mosler et al. [18] compared professional male soccer players from Qatar and found similar incidences of cam morphology among Arabic, Persian, white, and Black athletes, but a lower incidence in East Asians. Gollwitzer et al. [9] used CT scans and found the highest alpha angles in white people (61°), lower values in Black people (56°), and the lowest values in people of Asian heritage (51°). Van Houcke et al. [25] reported higher alpha angles in white individuals than in Chinese individuals.
Differences in Other Femoral Measurements Among the Study Populations
Research shows a consistent connection between an increase in the true neck-shaft angle and decrease in human mobility and activity level [3, 8]. However, in the current study, both the apparent and true neck-shaft angle were higher in the hunter-gatherer Australian aborigines than in the two agricultural groups from Poland and Iran. The warmer climate in Australia may account for these findings. A higher neck-shaft angle (both true and apparent) has been reported in people living in warmer climates, with the theory that colder climates are associated with heavier and stockier body types with a correspondingly lower neck-shaft angle [8]. The time period may have also had an effect, with Moats et al. [14] finding a lower neck-shaft angle in their ancient population than in their modern population. Ethnic differences may also have an effect, because lower neck-shaft angles have been reported in the hips of Chinese individuals than in Black and white people [6].
The Neolithic population from Iran had higher femoral version and femoral neck inclination than the other two groups. Moats et al. [14] also found higher femoral version in their ancient population. This may relate to lifestyle habits such as sitting and squatting patterns. Femoral version seems to have less ethnic variation, with Koerner et al. [10] reporting no differences between and among Black, white, and Hispanic populations in the United States. Overall, our results for true and apparent neck-shaft angle, version, and inclination fit reasonably with previous reports, supporting the validity of our data set.
Conclusion
This study demonstrates that cam morphology was present at comparable rates in historical populations and is not a purely modern phenomenon. This shifts our understanding of cam morphology etiology, demonstrating that modern intensive sports participation in adolescents is not the only cause of cam morphology. Additional research on the etiology of cam morphology is needed to better understand this highly prevalent condition and develop preventive strategies.
Supplementary Material
Acknowledgments
We thank Anna Wrzesińska MSc from the Museum of the First Piasts at Lednica, Wioletta Nowaczewska PhD from the University of Wrocław, and the Open Research Scan Archive for allowing us to use the skeletal material. We also thank Szymon Stelting from the Poznań University of Life Sciences for technical support in scanning the osteologic material.
Footnotes
The institution of one or more of the authors (AMK) has received, during the study period, funding from the National Science Center in Poland (grant number 2015/19/N/NZ8/00177).
One of the authors (AMK) has received, during the study period, a scholarship at the Musee de l’Homme from the Polish National Agency for Academic Exchange, which allowed for the conduct of this research.
Each author certifies that neither he nor she, nor any members of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Ethical approval for this study was waived by Bioethics Committee at Poznan University of Medical Sciences.
This work was performed at the Department of Paediatric Orthopaedics and Traumatology of Poznan University of Medical Sciences, Poznan, Poland, and at the Department of Zoology, Poznań University of Life Sciences, Poznan, Poland.
Contributor Information
Anna Maria Kubicka, Email: amkkubicka@gmail.com.
Marek Jóźwiak, Email: jozwiakmp@gmail.com.
Raymond W. Liu, Email: lukaswoz@wp.pl.
References
- 1.Albers CE, Steppacher SD, Haefeli PC, et al. Twelve percent of hips with a primary cam deformity exhibit a slip-like morphology resembling sequelae of slipped capital femoral epiphysis. Clin Orthop Relat Res . 2015;473:1212-1223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Afshar Z., Millard A, Roberts C, Gröcke. The evolution of diet during the 5th to 2nd millennium BCE for the population buried at Tepe Hissar, north-eastern Central Iranian Plateau: the stable isotope evidence. J Archaeol Science Reports. 2019;27:101983. [Google Scholar]
- 3.Anderson JY, Trinkaus E. Patterns of sexual bilateral and interpopulational variation in human femoral neck-shaft angles. J Anat. 1998;192:279-285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Buikstra JE, Ubelaker DH. Standards for data collection from human skeletal remains. Arkansas Archeological Survey Research Series No. 44. Am J Hum Biol. 1995;7:672. [Google Scholar]
- 5.Ćwirko-Godycki M. Early medieval burial ground on the Lednicki Promontory. Materiali I Prace Antropologiczne. 1956;11:1-56. [Google Scholar]
- 6.Edwards K, Leyland KM, Sanchez-Santos MT, et al. Differences between race and sex in measures of hip morphology: a population-based comparative study. Osteoarthritis Cartilage. 2020;28:189-200. [DOI] [PubMed] [Google Scholar]
- 7.Gillespie RJ, Levine A, Fitzgerald SJ, et al. Gender differences in the anatomy of the distal femur. J Bone Joint Surg Br. 2011;93:357-363. [DOI] [PubMed] [Google Scholar]
- 8.Gilligan I, Chandraphak S, Mahakkanukrauh P. Femoral neck-shaft angle in humans: variation relating to climate, clothing, lifestyle, sex, age and side. J Anat. 2013;223:133-151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gollwitzer H, Suren C, Strüwind C, et al. The natural alpha angle of the femoral head-neck junction: a cross-sectional CT study in 1312 femurs. Bone Joint J. 2018;100:570-578. [DOI] [PubMed] [Google Scholar]
- 10.Koerner JD, Patel NM, Yoon RS, Sirkin MS, Reilly MC, Liporace FA. Femoral version of the general population: does "normal" vary by gender or ethnicity? J Orthop Trauma. 2013;27:308-311. [DOI] [PubMed] [Google Scholar]
- 11.Kruczkiewicz E. Ossa Australica. Materiali I Prace Antropologiczne. 1962;58:1-93. [Google Scholar]
- 12.Kubicka AM, Lubiatowski P, Długosz JD, Romanowski L, Piontek J. Directional asymmetry of upper limbs in a medieval population from Poland: a combination of linear and geometric morphometrics. Am J Hum Biol. 2016;28:817-824. [DOI] [PubMed] [Google Scholar]
- 13.Laborie LB, Lehmann TG, Engesæter IØ, Eastwood DM, Engesæter LB, Rosendahl K. Prevalence of radiographic findings thought to be associated with femoroacetabular impingement in a population-based cohort of 2081 healthy young adults. Radiology. 2011;260:494-502. [DOI] [PubMed] [Google Scholar]
- 14.Moats AR, Badrinath R, Spurlock LB, Cooperman D. The antiquity of the cam deformity: a comparison of proximal femoral morphology between early and modern humans. J Bone Joint Surg Am. 2015;97:1297-1304. [DOI] [PubMed] [Google Scholar]
- 15.Morris W, Fowers C, Yuh R, Gebhart J, Salata M, Liu R. Decreasing pelvic incidence is associated with greater risk of cam morphology. Bone Joint Res . 2016;5:387-392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Morris WZ, Li RT, Liu RW, Salata MJ, Voos JE. Origin of cam morphology in femoroacetabular impingement. Am J Sports Med. 2018;46:478-486. [DOI] [PubMed] [Google Scholar]
- 17.Morris WZ, Weinberg DS, Gebhart JJ, Cooperman DR, Liu RW. Capital femoral growth plate extension predicts cam morphology in a longitudinal radiographic study. J Bone Joint Surg Am. 2016;98:805-812. [DOI] [PubMed] [Google Scholar]
- 18.Mosler AB, Crossley KM, Waarsing JH, et al. Ethnic differences in bony hip morphology in a cohort of 445 professional male soccer players. Am J Sports Med. 2016;44:2967-2974. [DOI] [PubMed] [Google Scholar]
- 19.Myszka A, Kubicka AM, Tomczyk T. The mechanical hypothesis of septal aperture formation tested in an early medieval population from Ostrów Lednicki (Poland). J Anat. 2019;234:368-375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nelson AE, Stiller JL, Shi XA, et al. Measures of hip morphology are related to development of worsening radiographic hip osteoarthritis over 6 to 13 year follow-up: the Johnston County Osteoarthritis Project. Osteoarthritis Cartilage. 2016;24:443-450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002;84:556-560. [DOI] [PubMed] [Google Scholar]
- 22.Raveendran R, Stiller JL, Alvarez C, et al. Population-based prevalence of multiple radiographically-defined hip morphologies: the Johnston County Osteoarthritis Project. Osteoarthritis Cartilage. 2018;26:54-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Schlager A, Ahlqvist K, Rasmussen-Barr E, et al. Inter- and intra-rater reliability for measurement of range of motion in joints included in three hypermobility assessment methods. BMC Musculoskelet Disord. 2018;19:376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Schneider CA, Rasband WS, Eliceiri KW. NIH Image to ImageJ: 25 years of image analysis. Nat Methods. 2012;9:671-675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Van Houcke J, Yau WP, Yan CH, et al. Prevalence of radiographic parameters predisposing to femoroacetabular impingement in young asymptomatic Chinese and white subjects. J Bone Joint Surg Am. 2015;97:310-317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Weinberg DS, Williamson DF, Millis MB, Liu RW. Decreased and increased relative acetabular volume predict the development of osteoarthritis of the hip: an osteological review of 1090 hips. Bone Joint J. 2017;99:432-439. [DOI] [PubMed] [Google Scholar]
- 27.Zurmühle CA, Milella M, Steppacher SD, Hanke MS, Albers CE, Tannast M. ArtiFacts: femoroacetabular impingement-a new pathology? Clin Orthop Relat Res. 2017;475:973-980. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.