

Abstract
The hyoid bone fracture has traditionally been attributed to strangulation and hanging. Although rare, ensuing its vague presentation, hyoid bone fracture is oftentimes overlooked and missed, leading to delayed complications. Herein, we are reporting an overlooked hyoid bone fracture in a man who attempted suicide by strangulating himself, whereby Valsalva manoeuvre performed during bedside flexible nasopharyngolaryngoscopy revealed the fractured segment. As the patient was stable and asymptomatic, he was successfully managed conservatively. We would like to highlight the awareness of the Valsalva manoeuvre, which could elicit hyoid bone fracture as missing or overlooking the fracture may lead to devastating complications which may ensue, such as respiratory distress.
Keywords: ear, nose and throat/otolaryngology, emergency medicine, trauma
Background
The hyoid bone is a U-shaped bone located in the anterior midline of the neck and is a constituent of the laryngeal framework. Fracture of this bone has been reported with an incidence of 0.002% of all bone fractures.1 The rarity of fracture of the hyoid bone is owing to its secure location, as the bone is well defended anatomically by the projected mandible anterolaterally and cervical spine posteriorly. Nevertheless, strangulation, as well as hanging, has been the leading cause of hyoid bone fracture.2 Diagnosing isolated hyoid bone fracture has been a conundrum for the attending physicians as a result of the vague presentation and lack of classical clinical findings. Hence, radiological investigations, notably CT, have been regarded as the gold standard to diagnose isolated hyoid bone fracture. We report that a simple bedside technique of performing Valsalva manoeuvre during flexible nasopharyngolaryngoscopy (FNPLS) enables detection of hyoid bone fracture in stable patients.
Case presentation
A previously healthy 30-year-old man presented with a 1-day history of dysphagia and throat discomfort following a failed suicide attempt by strangulating himself using his belt. According to the patient, he attempted suicide, owing to financial constraints and family problems. The patient tried to strangulate himself using his belt three times. The patient passed out following the third attempt and was rushed to the hospital by his peers. The patient regained consciousness on the way to the emergency department. He reported throat discomfort and difficulty, and pain on swallowing. Otherwise, there was no shortness of breath or stridor, no hoarseness, no choking or gasping episodes.
On examination, the patient was comfortable under room air, not in respiratory distress and with stable vital signs. He was able to speak in complete sentences, with no change of voice or stridor. There were no bruises or any strangulation marks noted over the neck. Palpation of the neck revealed minimal tenderness over the left side with no palpable swelling, crepitation or step deformity. Laryngeal crepitus and the laryngeal framework appeared intact. FNPLS performed with Valsalva manoeuvre at bedside showed bony projection at the left lateral pharyngeal wall (figure 1). There were no other signs of haematoma, supraglottic and glottic structures were intact, and bilateral vocal cords were mobile.
Figure 1.

Flexible nasopharyngolaryngoscopy showing bony prominence at the left lateral pharyngeal wall.
Investigations
CT neck revealed fracture at the left body of the hyoid bone (figure 2) with air trapping noted over the valleculae region with no other deformities or injuries. Routine blood investigations, arterial blood gas and chest radiograph were unremarkable. Neck circumference was monitored every shift during the admission to look for signs of delayed haematoma or swelling.
Figure 2.
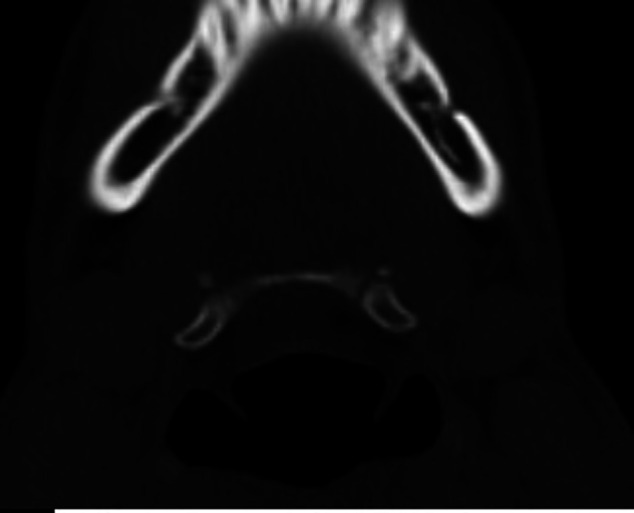
CT scan of the left hyoid bone fracture.
Treatment
The patient was referred to the psychiatry team and was admitted for observation. The hyoid bone fracture was treated conservatively as the patient was asymptomatic. Repeated FNPLS revealed normal findings and the absence of bony projection over the lateral pharyngeal wall.
Outcome and follow-up
The patient’s symptoms completely recovered after 3 days. The patient was allowed to go home with a 1-week follow-up, which he defaulted.
Discussion
Hyoid bone anatomically is located in a ‘safe zone’ owing to its protection by the mandible and cervical spine, in addition to its ability to move in all directions. The hyoid bone serves as an attachment site for both suprahyoid and infrahyoid muscles, which take part in both respiration and swallowing process. Hyoid bone fracture is traditionally associated with injuries of the surrounding structures, notably the mandible, cervical spine, larynx and pharynx. Nevertheless, the hyoid bone is susceptible to injury or trauma, especially when the neck is hyperextended3 as this places the bone in a vulnerable position as it loses its anatomical protection, resulting in an isolated hyoid bone fracture. The isolated hyoid fracture can be organised into three types. The first type is inward compression fracture with outer periosteal tears, and the second is an anteroposterior compression fracture with an inner periosteal tear. The third type is avulsion fracture, which is the most dangerous type.4
Habitually, patients with the isolated hyoid bone fracture may present with symptoms ranging from neck pain, which is more pronounced during coughing or straining, odynophagia and dysphagia, to more severe obstructive symptoms, such as shortness of breath and stridor, which may require emergent airway intervention. Additionally, there is also potential intraoral bleeding resulting from the injury to soft tissue caused by the mobile bony fragments.
During the physical examination, the presence of bruises, swelling or tenderness corresponding to the location of the hyoid bone may be a tell-tale sign of its injury. Parallel to that, a number of patients may exhibit suffocation or choking following tongue protrusion, dysphonia, inability to rotate the neck, as well as the presence of subcutaneous emphysema on palpation. As a part of the assessment, bedside FNPLS can be performed to assess the upper airway as well as to look for the presence of injuries, such as haematoma, bony prominence or exposed laryngeal cartilages. However, it is noteworthy that several techniques performed previously to visualise difficult areas, such as post-cricoid and pyriform fossa, such as Valsalva manoeuvre, can aid in visualising bony fragments.5 6 Valsalva manoeuvre creates a positive pressure within the pharynx, resulting in the mobile hyoid segment pushing against the lateral pharyngeal wall into the airway, as seen in our patient. Spielmann et al previously described two cases with normal radiographical findings, which revealed hyoid bone fracture through nasal Valsalva manouever.7
CT neck is regarded as the gold standard imaging in detecting the presence of isolated hyoid bone fracture due to its high accuracy.8 In the same vein, CT enables other concurrent injuries, such as haematoma and cervical spine pathology, to be detected. In a medical setting where CT is not available, a neck radiograph should be performed for the laryngeal framework and the integrity of the airway to be assessed.
Hyoid bone fracture has been traditionally treated conservatively unless the patient presents with acute airway obstruction. Close observation is mandatory in all hyoid bone fracture cases as oedema may be progressive, and acute airway obstruction oftentimes develops rapidly. Serial bedside FNPLS can help assess the airway if indicated. Conservative management of hyoid bone fracture has been reported to include observation for 24–72 hours, liquid or semisolid diet, insertion of the nasogastric or orogastric tube, along with medication, including analgesics and antibiotics. If surgery is deemed necessary, it can vary from neck exploration, fracture stabilisation and tracheostomy for severe cases.9
Learning points.
Hyoid bone fracture is an uncommon clinical entity generally caused by blunt trauma injuries, such as strangulation or hanging. Although rare, isolated hyoid bone fracture poses catastrophic airway complications.
Isolated hyoid bone fracture is very challenging to diagnose and difficult to identify clinically. Valsalva manoeuvre enables the fractured part to be visualised in the airway during flexible nasopharyngolaryngoscopy, which is suggestive of hyoid bone fracture.
A patient with an isolated hyoid bone fracture may present with diverse symptoms, including neck pain, dyspnoea and even bleeding. Careful and complete clinical examination is compulsory in every case with suspected hyoid bone injury. A flexible laryngoscope is an excellent bedside assessment tool.
Footnotes
Contributors: MH: Writing, drafting and literature review. JS: Editing and literature review. PN: Editing.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer-reviewed.
Ethics statements
Patient consent for publication
Obtained.
References
- 1.Dalati T. Isolated hyoid bone fracture. review of an unusual entity. Int J Oral Maxillofac Surg 2005;34:449–52. 10.1016/j.ijom.2004.09.004 [DOI] [PubMed] [Google Scholar]
- 2.Kuo L-C, Lin H-L, Chen C-W, et al. Traumatic hyoid bone fracture in patient wearing a helmet: a case report. Am J Emerg Med 2008;26:251.e1–251.e2. 10.1016/j.ajem.2007.04.015 [DOI] [PubMed] [Google Scholar]
- 3.Chowdhury R, Crocco AG, El-Hakim H. An isolated hyoid fracture secondary to sport injury. A case report and review of literature. Int J Pediatr Otorhinolaryngol 2005;69:411–4. 10.1016/j.ijporl.2004.10.003 [DOI] [PubMed] [Google Scholar]
- 4.Weintraub CM. Fractures of the hyoid bone. Med Leg J 1961;29:209–16. 10.1177/002581726102900405 [DOI] [PubMed] [Google Scholar]
- 5.Hillel AD, Schwartz AN. Trumpet maneuver for visual and CT examination of the pyriform sinus and retrocricoid area. Head Neck 1989;11:231–6. 10.1002/hed.2880110307 [DOI] [PubMed] [Google Scholar]
- 6.Purser S, Antippa P. Maneuver to assist examination of the hypopharynx. Head Neck 1995;17:389–93. 10.1002/hed.2880170505 [DOI] [PubMed] [Google Scholar]
- 7.Spielmann PM, Hathorn IF, Clarke JKV, et al. Hyoid bone fracture identified only with nasal Valsalva manoeuvre. J Laryngol Otol 2010;124:431–2. 10.1017/S0022215109992106 [DOI] [PubMed] [Google Scholar]
- 8.Erdoğan MO, Koşargelir M, Yorulmaz R, et al. [Isolated hyoid bone fracture due to blunt trauma: case report]. Ulus Travma Acil Cerrahi Derg 2013;19:282–4. 10.5505/tjtes.2013.64436 [DOI] [PubMed] [Google Scholar]
- 9.Ramchand T, Choudhry OJ, Shukla PA, et al. Management of hyoid bone fractures: a systematic review. Otolaryngol Head Neck Surg 2012;147:204–8. 10.1177/0194599812451409 [DOI] [PubMed] [Google Scholar]