

ABSTRACT
Rhabdomyolysis (RML) is a pathological entity characterized by symptoms of myalgia, weakness and dark urine (which is often not present) resulting in respiratory failure and altered mental status. Laboratory testing for myoglobinuria is pathognomonic but so often not present during the time of testing that serum creatine kinase should always be sent when the diagnosis is suspected. Kidney injury from RML progresses through multiform pathways resulting in acute tubular necrosis. Early treatment (ideally<6 hoursfrom onset) is needed with volume expansion of all non-overloaded patients along with avoidance of nephrotoxins. There is insufficient data to recommend any specific fluid. The mortality rate ranges from 10% to up to 50% with severe AKI, so high index of suspicion and screening should be in care plan of seriously ill patients at risk for RML.
Keywords: Rhabdomyolysis, pathophysiology, acute kidney injury, treatment
INTRODUCTION
Rhabdomyolysis (RML, lysis of skeletal muscle cells) is a pathological syndrome of acute or subacute onset in which a patient develops localized or generalized myalgia and weakness, associated with a rapid rise in the serum creatine kinase (CK) level, the extent of which will depend upon the timing of analysis with respect to the acute event.1 A systematic review on the definition of RML recommends these clinical symptoms combined with a CK cut-off value of >1000 IU/L or CK > 5 times upper limit of normal (ULN) as mild RML.1 Additionally, measured myoglobinuria and acute kidney injury (AKI) indicate a severe RML1. The above definition holds true after exclusion of elevated CK due to other aetiologies like myocardial infarction,2 status epilepticus,3 or a chronic neuromuscular disease.4 The coexistence of RML in these aetiologies is also a possibility with acute elevation of CK.1
RML has been documented in historic times. The Old Testament refers to a plague suffered by Israelites after consumption of quails during their exodus from Egypt.5 AKI characterized by dark red urine and oliguria from quail poisoning (and resultant Coturnism) has been reported from Greece in the past.6,7 In contemporary era, the first cases of traumatic RML with renal failure were reported during Messina earthquake in 1908 and then, subsequently in the World War I.8 However, the first detailed report of RML and AKI was by Bywaters et al. who described four war victims from the Battle of Britain in 1940.9 The same author identified myoglobin in the urine of air-raid traumatic crush injuries.10 Non-traumatic myoglobinuria was initially reported by Koenigsberg Haff in erstwhile province of East Prussia and then later from Sweden.11 It was, however, until the 1960’s when other causes like heat injury,12 and a metabolic myopathy predisposing to acute renal failure were recognized.13,14
The true incidence of RML is unknown since it is frequently oligo-symptomatic or asymptomatic. Approximately 26,000 cases of rhabdomyolysis are reported annually in the United States.15 African Americans, males, obese patients, patients younger than ten years of age, and patients older than 60 years old all have a higher incidence of RML.16 The percentage of patients developing AKI varies from 13% to approximately 50%, depending on clinical and organizational setting.17 In those with severe RML, the incidence of AKI goes up to 81% with 26% needing kidney replacement therapies.18 Mortality from RML is 10%, which increases in the setting of AKI and reaches 50% in AKI stage 3.19,20
AETIOLOGY
The etiology of RML varies according to the age group, geographical variation and the timing in relation to the analysis. Traumatic causes are more common in the developing countries, while drug abuse is the most frequent cause in the Western world.21 Infections and congenital diseases are largely responsible for pediatric RML, while drugs and trauma are the most common causes in adults (up to 80% of cases).22 The list of causes of RML is exhaustive and is beyond the scope of this article, however, broad categories have been covered in figure 1.
Figure 1.
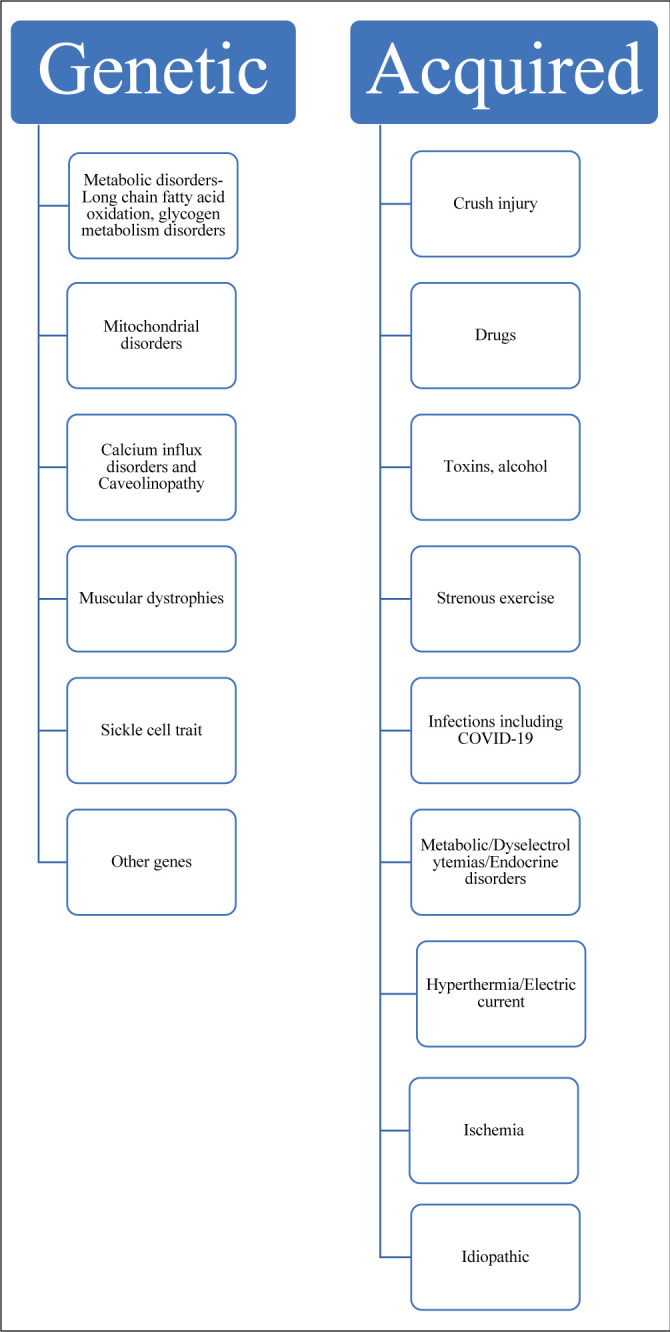
Causes of rhabdomyolysis
Recently, RML has been reported in cases of coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The first case was a report of a COVID-19 patient from Wuhan, China, who developed RML during hospitalization.23 Second patient was an octogenarian who initially presented with RML and was subsequently diagnosed as COVID-19.24 A recent review reported nine patients (all adult males) with COVID-19 related myositis/RML, of which three passed red cells in urine and one had cola colored urine.25 The postulated mechanisms include excessive immune response and cytokine storm, direct viral invasion and circulating viral muscle toxins.26
PATHOPHYSIOLOGY
The disorders causing RML result in mechanical stress on the cell, which in turn leads to cellular membrane injury, hypoxiaand the release of degradative enzymes, ATP depletion and the generation of oxidative free radicals.27 This results in persistent contraction of the myofibers and an inflammatory cascade causing cell death. Injured muscles sequester up to 10-12 liters of fluid in a few days culminating in a compartment syndrome.28,29 (figure 2)
Figure 2.
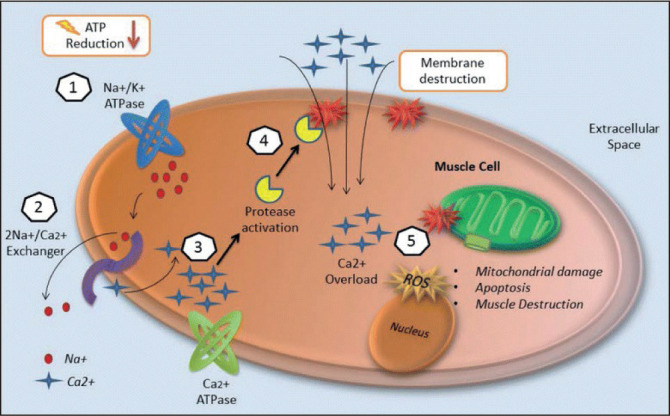
Injury mechanisms of rhabdomyolysis.1 Energy (ATP) depletion inhibits Na+/K+ ATPase function, thus increasing intracellular sodium.2 The 2Na+/Ca2+ exchanger increases intracellular calcium.3 Ca2+ ATPase is not able to pump out intracellular calcium due to energy depletion.4 Intracellular calcium activates proteases such as phospholipase 2 (PLA2), which destroy structural components of the cell membrane, allowing the entrance of more calcium.5 Calcium overload disrupts mitochondrial integrity and induces apoptosis leading to muscle cell necrosis. (Adapted from Chavez et al: Beyond muscle destruction: a systematic review of rhabdomyolysis for clinical practice. Crit Care Lond Engl. 2016 Jun 15;20(1):135. Open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).27
The destruction of approximately 100 g of muscle tissue is capable of inducing RML.30,31 The intracellular metabolites (potassium, phosphates and urate) and intracellular proteins (myoglobin, CK, aldolase, lactate dehydrogenase, aspartate aminotransferase, and nucleic acids) are released in the extracellular space and circulation. The release of excessive myoglobin into the plasma overwhelms the capacity of the binding proteins (mainly haptoglobin). Myoglobin then gets filtered across the glomerulus, causing tubular damage. The pathophysiology of AKI in rhabdomyolysis is likely to be multifactorial, including vasoconstriction, hypovolemia, direct myoglobin toxicity and intraluminal cast formation.21,29 Myoglobin can exert a direct cytotoxic effect through the enhancement of local oxidative stress in the tubular cells.30,32 The high rates of generation and urinary excretion of uric acid further contribute to tubular obstruction by uric acid casts. The precipitation of these casts is amplified in acidic urine. The free iron released from degradation of intratubular myoglobin catalyzes free radical production and further enhances ischemic damage.29,33.34 A recent study showed that heme-activated platelets released from necrotic muscle cells during RML promoted AKI.35 Alkaline conditions prevent this effect by stabilizing the reactive ferryl-myoglobin complex.36 Disseminated intravascular coagulation (DIC) and renal arteriolar constriction also occurs.17,22 The transient prerenal phase, if not treated early progresses to persistent AKI, which is almost always, due to acute tubular necrosis.21 (figure 3)
Figure 3.
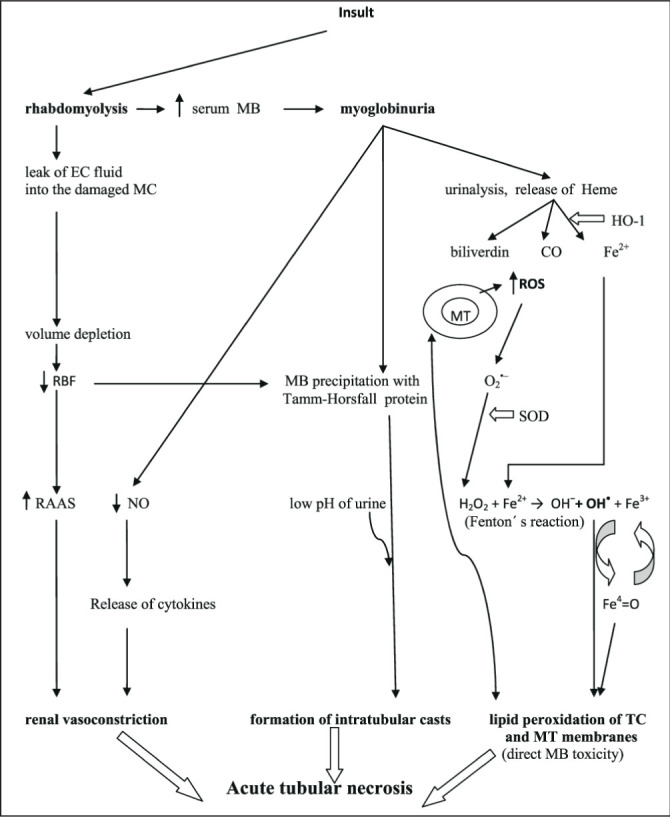
Pathophysiology of rhabdomyolysis-induced acute kidney injury. CO, carbon monoxide; EC, extracellular; Fe 2+ , ferrous iron; Fe 3+, ferric iron; Fe4 = O, ferryl iron; HO-1, heme oxygenase-1; H2O2, hydrogen peroxide; MB, myoglobin; MC, muscle cell; MT, mitochondria; NO, nitric oxide; OH-, hydroxyl anion; O2-, superoxide radical; OH*, hydroxyl radical, RAAS, renin-angiotensin-aldosterone system; RBF, renal blood flow; ROS, reactive oxygen species; SOD, superoxide dismutase; TC, tubular cell. (Adapted from: Petejova et al : Acute kidney injury due to rhabdomyolysis and renal replacement therapy: a critical review. Crit Care Lond Engl. 2014 May 28;18(3):224. Open access article distributed under the terms of the Creative Commons Attribution License. (http://creativecommons.org/licenses/by/2.0)32
CLINICAL FEATURES
There is a wide variation in the clinical presentation of RML.37 The ‘classic’ triad of symptoms includes muscle pain (23% of patients), weakness (12% of patients) and dark urine (Coca-cola colored or tea-colored, 10% of patients).1,19,38 Because of the relatively quick renal clearance of myoglobin, this dark urine often lasts for a short duration, and may be overlooked by both patients and clinicians.
The clinical manifestations can be classified as musculoskeletal signs, general manifestations and complications. The muscle pain, weakness, swelling, tenderness and contracture may involve specific groups of muscles or may be generalized. The most frequently involved muscle groups are the calves and the lower back. The muscles can be tender and swollen, and there can be skin changes indicating pressure necrosis. However, these classic features are seen in less than 10% of the patients.39 Systemic circulation of intracellular muscle components can yield additional non-specific symptoms like malaise, fever, tachycardia, nausea or vomiting.37
Cardiovascular symptoms may stem from the associated electrolyte abnormalities (i.e., potassium, calcium, phosphate) and may range from arrhythmias to cardiac arrest.40 Patients may be hypoventilating if RML was drug-induced or due to trauma or hyperventilating due to pain if they are awake and agitated.27 Respiratory failure and acute respiratory distress syndrome may occur in some patients.21 Hepatic dysfunction secondary to proteases released from muscle injury is seen in 25% of patients with RML.41 AKI and DIC (thought to be due to activation of clotting cascade thromboplastin released during muscle injury) are late complications, developing 12–72 hours after the acute insult.42 AKI as a complication of RML is quite common, representing about 7 to 10% of all cases of acute kidney injury in the United States.43 The course of AKI is typically initial oliguria followed by polyuria in 1-3 weeks after the primary insult, however, some cases may non-oilguric from the beginning.31 Another complication is metabolic acidosis as a result of uremia and lactic acidosis from ischemia. A non-anion gap acidosis may also occur from release of sulfur-containing proteins in large amounts overwhelming kidney excretion.44
LABORATORY WORK UP
Serum creatine kinase
Serum CK concentration, mainly the CK-MM subtype, is the most sensitive indicator of damage to muscles. The normal plasma CK level varies between 45 to 260 U/L.45 Serum CK begins to rise approximately 2 to 12 hours after the onset of muscle injury, peaks within 24 to 72 hours, and then declines at the relatively constant rate of 39% of the previous day’s value.46 (figure 4) A CK cut-off value of >1000 IU/L or CK > 5 times upper limit of normal (ULN) in correct clinical context could diagnose mild RML.1 An exception to these criteria is statin-related RML where it is defined as CK elevation >10 times ULN with evidence of renal impairment and muscle symptoms or CK > 50 times ULN.47 The concentration of CK is directly proportional to the extent of muscle injury. A persistently elevated CK level suggests continuing muscle injury or development of a compartment syndrome.48 Whether increased levels of CK point to an increased risk of subsequent AKI, and/or need of kidney replacement therapy is unclear as CK is only a surrogate marker of myoglobin nephrotoxicity.49,50,51 Rarely, total CK may be factitiously low in RML. Running the sample in dilution should be considered if the low values do not correlate with the diagnosis.52
Figure 4.
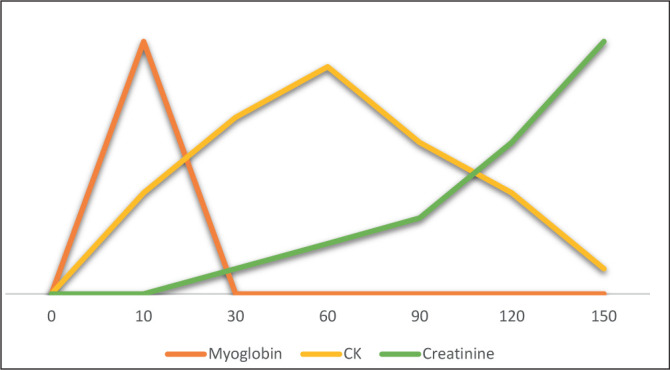
Time course (in hours; y-axis) of serum myoglobin, CK, and creatinine with respect to the insult. CK, creatine kinase.
Serum and urine myoglobin
Myoglobin is normally bound to plasma globulins, and has a rapid renal clearance with a half-life of 2-3 hours. A small quantity of filtered myoglobin (0.01-5%) is normally excreted with urine. The normal concentration of myoglobin in the serum is below 5.7nmol/L (100 μg/L) and in urine below 0.57nmol/L (10 μg/L). After the occurrence of muscle damage, the circulating myoglobin levels exceed the plasma protein binding capacity, reach the glomeruli and are eventually excreted in the urine. Before the urine becomes discoloured (dirty-brown) by myoglobin, the level of myoglobin in the urine must exceed 57000 nmol/L (100 mg/ dl). In RML, the level of myoglobin in the serum increases within 1–3 h, reaches its peak in 8–12 h, and then returns to normal within 24 h after the onset of the injury. (figure 4) Thus, the detection of myoglobin in the blood or urine is pathognomonic for the diagnosis of RML, provided that it is made in the initial phases of the syndrome (i.e., within the first 24 h).42 A systematic review showed that myoglobinuria is detected in 17% of the patients with RML.1
The practical applicability of serum and urine myoglobin in the diagnosis of RML has several caveats.42 Firstly, serum myoglobin usually increases before a rise in CK and drops more rapidly than does the decline in CK. Moreover, myoglobinuria may not be visible or may resolve early in the course of RML. These facts make this parameter less sensitive and therefore should not be relied upon to rule out the diagnosis of RML. Secondly, myoglobinuria is detected by urine dipstick tests (orthotolidine), which also react with the globin fragment of haemoglobin. Thus, in the presence of red blood cells or haemolysis, the specificity of this test is limited. False negative (heme-negative dipstick) results may occur in the presence of high specific gravity, ascorbic acid, or high nitrite concentration.53 Radioimmunoassay is more sensitive and specific than dipstick.54 However, this test is often not readily available, and it may take more than 24 hours to obtain results.
Urine myoglobin analysis is also affected by sample timing, glomerular filtration rate (GFR), and urine flow rate.55 Urine myoglobin concentration may be falsely low if the collection represents a mixture of urine filtered after the injury with preinjury urine from the bladder or if filtered myoglobin excretion is limited because of kidney dysfunction.21 Alternatively, the presence of urine myoglobin may indicate good renal function in that the kidneys are still able to excrete the high plasma myoglobin load.55
Other relevant laboratory findings
In 45% of the cases of RML, the urine dipstick can be found to be positive for the presence of protein. Proteinuria is due to the release of myoglobin and other proteins by the disrupted muscle cells. In the microscopic examination of urine, red blood cells are relatively few (<5 per high-power field).46 There could be detection of coarse granular red-brown myoglobin casts. The fractional excretion of sodium may remain low even in the later course of the disease, reflecting primarily tubular obstruction rather than tubular necrosis.21
Creatine released in large quantities from the muscles gets converted into creatinine in the circulation. Some of the studies have suggested a higher ratio of serum creatinine/ blood urea nitrogen in RML.56 At the later stages of RML, the proteins released by the dead muscle cells are catabolized, thereby increasing the production of urea and thus the urea/ creatinine ratio returns to normal.57 Hyperkalemia is the most life-threatening electrolyte abnormality in RML. Its mechanisms include efflux from intracellular to extracellular compartment, hyper-catabolism, inadequate excretion in AKI and iatrogenic (blood transfusions).58 Hypocalcaemia is also common in RML from influx of plasma calcium into injured muscles, calcium-phosphate precipitation in muscles, calcitriol suppression from hyperphosphatemia and parathyroid hormone resistance.21,36 Upon complete cellular necrosis, the calcium initially entrapped in the cytoplasm of muscle cells is released back into the plasma. This, in combination with the secondary hyperparathyroidism that develops due to early hypocalcaemia and high levels of vitamin D (produced in great quantities by the glomerular cells), leads to the late manifestation of hypercalcemia.46 Furthermore, inorganic and organic phosphoric components are dissolved and large amounts of inorganic phosphorus are released into the plasma, leading to hyperphosphatemia.46 Hyperuricemia is seen as a result of purines derived from nucleic acids of damaged myocytes.46 The elevation in aspartate transaminase and lactate dehydrogenase is quite common in RML.59 Rarely, features of DIC including thrombocytopenia, increased fibrinogen degradation products (FDP), and extended prothrombin time (PT) are present.46
Muscle biopsy
A muscle biopsy is usually not required. For a diagnostic evaluation of muscle structure in select cases, biopsy is best deferred until at least 3 months after symptom resolution.60 The histopathological findings include loss of cross striations and nuclei (necrosis and fragmentation of muscle fibers) with the absence of inflammatory cells.61,62
Kidney biopsy
Similarly, renal biopsy is not required to make the diagnosis of RML. The characteristic biopsy feature is acute tubular injury with globular red-brown casts which are positive for myoglobin by immunohistochemistry.63,64 (figure 5)
Figure 5.
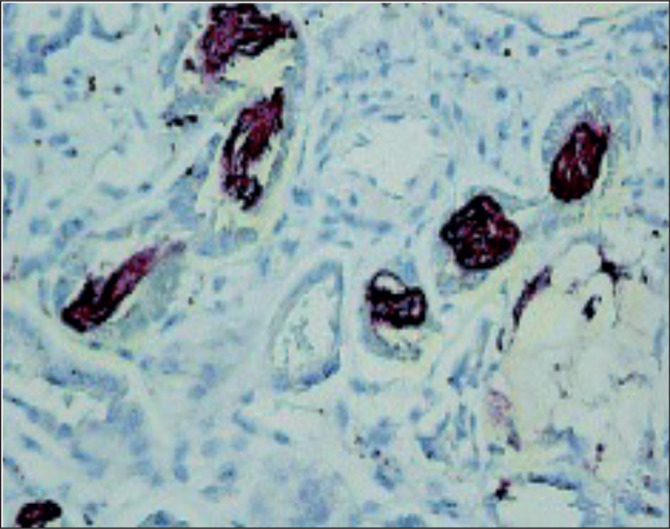
Kidney biopsy showing positive immunoperoxidase staining for myoglobin pigmented casts in a young female with heavy cocaine use and acute kidney injury. (Modified from Mansoor et al : Systematic review of nephrotoxicity of drugs of abuse, 2005-2016. BMC Nephrol [Internet]. 2017 Dec 29 [cited 2020 Apr 30];18. Open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).64
Imaging
RML is a clinical diagnosis with supporting serum/urine tests. However, in cases of uncertainness, ultrasound, computerized tomography, magnetic resonance imaging and skeletal-scintigraphy provide supporting clues in diagnosing RML.65 MRI seems to be more sensitive than CT or US (sensitivity 100%, 62%, 42% respectively).66 Though these imaging modalities are non-specific; their help in localization is found useful when fasciotomy is being contemplated.
Investigating exertional RML
The risk of exertional RML is increased up to 11-fold in those with prior heat injuries and more than 50% of patients with exertional RML have a history of heat cramps or heat exhaustion.67 Risk factors for greater increase in CK postexercise include low premorbid physical fitness, males, African ethnicity, dehydration and high intensity prolonged weight bearing exercises.68 A higher pre-disease CK and lower coenzyme CoQ10, specifically CK:CoQ10 ratio, is associated with risk of exertional RML in African Americans.69 Further work up should be considered in patients with no history of heat exposure, or who have exertional RML. The acronym “RHABDO” has been suggested as an aide-memoire. (table 1)70 Identifying genetic disorders presenting as RML is a diagnostic dilemma due to their rarity and marked heterogeneity, needing a high degree of clinical suspicion. Even presence of an identifiable trigger does not necessarily exclude an underlying genetic cause. Whole exome/genome sequencing and next generation sequencing may identify new genetic aetiologies of RML.71,72
Table 1.
Selection of patients for screening of a genetic disorder as a cause of exertional rhabdomyolysis. CK, creatine kinase; ULN, upper limit of normal. (Adapted from Scalo et al: Exertional rhabdomyolysis: physiological response or manifestation of an underlying myopathy? BMJ Open Sport Exerc Med. 2016;2(1):e000151. Open access article distributed under the terms of the Creative Commons Attribution Non-Commercial (CC BY-NC 4.0) License. (http://creativecommons.org/licenses/by-nc/4.0/)70
| R | Recurrent episodes of exertional rhabdomyolysis |
| H | HyperCKaemia persists 8 weeks after the event |
| A | Accustomed physical exercise |
| B | Blood CK >50 x ULN (>10 000 ULN in female Caucasian patients) |
| D | Drugs/medications/supplements and other exogenous and endogenous factors cannot sufficiently explain the rhabdomyolysis severity |
| O | Other family members affected/Other exertional symptoms (cramps, myalgia) |
In episodic RML in children and young adults, apart from detailed history (including a family history of consanguinity), a thorough search for muscle-energy correlation is mandated.22 The major fuel source (glycogen/fatty acids/ amino acids) depends on intensity and duration of activity. A metabolic myopathy from a defect in any one fuel source is likely to present during or immediately post activity most dependent on that fuel source.73 For example, long chain fatty acids are metabolized to acyl-CoA during fasting or prolonged low intensity exercise. Symptoms in lipidoses typically occur after 24-48 hours of exercise, when glycogen stores are exhausted. On the contrary, glycogenoses manifests as premature fatigue/myalgia within minutes of moderate to high intensity exercise, when defective anaerobic glycolysis results in failure of energy production. A reduction in exercise intensity resolves myalgia and the ability to begin exercising again after 6-10 minutes, without recurrence of symptoms (second wind phenomenon) is classical of McArdle disease, an autosomal recessive glycogen storage disorder.73,74 These investigations are likely unnecessary in patients with COVID-19 as this is a described provoking factor.
TREATMENT
The management of RML is targeted towards prevention of AKI. Any nephrotoxic medication should be discontinued. British guidelines recommend that adult and paediatric patients identified as being at risk of developing AKI due to RML, and who are not volume overloaded, should receive prompt intravenous volume expansion in order to achieve a high urinary flow rate.75 Recent Danish guidelines for prevention of RML induced AKI also suggest using early rather than late fluid resuscitation.76 The underlying principle is maintenance of a satisfactory urine output with fluid administration.
Other agents like mannitol were thought to be useful. It increases renal blood flow and GFR, acts like osmotic diuretic preventing obstructive myoglobin casts and scavenges free radicals. In addition, loop diuretics increase tubular flow and decrease precipitation of myoglobin. The evidence of benefit with these agents is not convincing in studies reported.77,78 The guidelines suggest against the use of loop (or any other) diuretics or mannitol to prevent AKI.76
The evidence for specific type of fluid which confers the greatest benefit is of low quality. There is a weak recommendation to suggest using crystalloids rather than colloids. A recent meta-analysis of twenty-seven studies demonstrated no evidence which supported a preferred fluid type.79 Historically, alkalinisation of the urine aiming for a urinary pH > 6.5 to mitigate intra-tubular precipitation of myoglobin has been the practice.36 However, the guidelines suggest against the routine use of alkalinisation with sodium bicarbonate (low quality of evidence).76 The primary role for sodium bicarbonate is simply to treat metabolic acidemia if present. Intravenous fluids should be initiated as soon as possible, preferably within the first 6 hours after muscle injury, at a rate that maintains a urine output in adults of 300 mL/h.79 Clinical judgment should be exercised in deciding when to stop fluid. If oliguric AKI develops and patient is a positive fluid balance, then administering additional fluids would be harmful.
The guidelines also suggest against the use of antioxidants or routine use of kidney replacement therapy as compared to none in prevention of RML induced AKI.76 However, no recommendations/suggestions could be provided on continuous kidney replacement therapy (CKRT) vs intermittent hemodialysis (IHD), filtration vs diffusion or low vs high cut-off membranes for AKI prevention.76
Prediction for Kidney failure or mortality
An admission prognostic score by McMahon et al. is likely to be useful in emergency room for risk stratification in RML.80 It includes age, sex, type of injury, and clinical laboratory parameters. In a retrospective observational study, a score of at least 6 was more sensitive (86% vs 83%) and specific (68% vs 55%) than peak CK of 5000U/L in predicting AKI requiring dialysis.81 Another risk score formula predicting AKI in patients with severe RML applied laboratory values related to the extent of muscle injury (CK levels, metabolic acidosis) and the general condition prior to the index event (hypoalbuminemia and decreased PT).82 A retrospective analysis of patients who were hospitalized for RML with admission CK > 1000U/L and serum creatinine of < 115 umol/L (1.3 mg/dL) were found not to be at risk for developing AKI if treated promptly with fluids, regardless of their initial CK levels.83 Another recent large, multicenter, retrospective study of 387 patients reported that invasive ventilation and severity of RML, including myoglobin level, are associated with the risk of stage 2–3 AKI. The long-term fall in estimated glomerular filtration rate (eGFR) correlated to serum phosphate and myoglobin (>8000U/L) at admission.18 These scoring assessments assist clinicians to identify patients who are at high risk of developing AKI so that they could be triaged for aggressive medical management. Furthermore, the transition from AKI to CKD in such patients would have future prognostic considerations.
Treatment of Myoglobinuric AKI
The basic principles of treatment of such patients remain same: adequate nutrition, management of metabolic complications and kidney replacement therapy (KRT) if overt renal failure develops. Dialysis is indicated when uremic encephalopathy, deteriorating kidney function, uncontrolled hyperkalemia, metabolic acidosis, and fluid overload occur due to RML and AKI. KRT modes include CKRT and intermittent KRT. Conventional IHD does not remove myoglobin effectively owing to the size of the protein and is therefore usually mandated by renal indications.
Myoglobin which is compatible with convective removal, can be transported to the filtrate by continuous hemofiltration and hemodiafiltration.84,85,86 Compared with IHD and peritoneal dialysis, CKRT is better able to maintain stable haemodynamic and homeostasis status, and remove myoglobin and inflammatory mediators.87 CKRT may therefore, theoretically, be a better choice for blood purification than intermittent KRT in the management of RML. Selected case reports have shown promising results in both pediatric and adult population.88,89 In a Cochrane systematic review, the authors were unable to conclude whether or not CKRT is a safe and effective option to treat people with RML.90
High cut-off and medium cut-off dialyzers have also been found to be useful in myoglobin elimination, though, the clinical benefits of such treatment strategies have yet to be established.91,92,93 Other extracorporeal therapies like plasmapheresis has been shown to have no favorable effect on outcomes or on the myoglobin burden of the kidneys.94,95
CONCLUSION
The clinical features of RML are highly varied and the timing of testing is important. While the classic triad of myalgias, weakness and dark urine still holds it is rarely present and the ephemeral nature of urine myoglobin and the multiple possibilities for false negatives (especially in the current era of using ascorbic acid supplementation in critical illness) make this an insensitive test as well. It requires a high index of suspicion and careful history taking to suggest RML and serum CK is the most sensitive laboratory test likely to result in the crucial early window for volume expansion to ensure dilution of the urine the reduce the risk of renal impairment. The mechanisms of renal injury are as varied as the causes of RML but the essential elements are oxidative stress (and myoglobin toxicity), mechanical injury from cast formation and vasoconstriction/ hypoperfusion.
While the classic approach has been avoiding nephrotoxins and early alkaline fluids (sodium bicarbonate) to achieve alkalization of the urine to decrease precipitation, there is no good quality evidence to support this or any specific fluid to achieve expansion in non-overloaded patients. Multiple predictive models are available but if a patient does progress to renal injury this should be managed as with acute tubular necrosis of any cause.
Footnotes
Provenance: Externally peer reviewed
UMJ is an open access publication of the Ulster Medical Society (http://www.ums.ac.uk).
REFERENCES
- 1.Stahl K, Rastelli E, Schoser B. A systematic review on the definition of rhabdomyolysis. J Neurol. 2020;267(4):877–82. doi: 10.1007/s00415-019-09185-4. [DOI] [PubMed] [Google Scholar]
- 2.Navin TR, Hager WD. Creatine kinase MB isoenzyme in the evaluation of myocardial infarction. Curr Probl Cardiol. 1979;3(12):1–32. doi: 10.1016/0146-2806(79)90010-0. [DOI] [PubMed] [Google Scholar]
- 3.Nass RD, Sassen R, Elger CE, Surges R. The role of postictal laboratory blood analyses in the diagnosis and prognosis of seizures. Seizure. 2017;47:51–65. doi: 10.1016/j.seizure.2017.02.013. [DOI] [PubMed] [Google Scholar]
- 4.Tarnopolsky MA. Myopathies Related to Glycogen Metabolism Disorders. Neurotherapeutics. 2018;15(4):915–27. doi: 10.1007/s13311-018-00684-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rutecki GW, Ognibene AJ, Geib JD. Rhabdomyolysis in antiquity. From ancient descriptions to scientific explication. Pharos Alpha Omega Alpha-Honor Med Soc. 1998;61(2):18–22. [PubMed] [Google Scholar]
- 6.Billis AG, Kastanakis S, Giamarellou H, Daikos GK. Acute renal failure after a meal of quail. Lancet. 1971;2(7726):702. doi: 10.1016/s0140-6736(71)92264-1. [DOI] [PubMed] [Google Scholar]
- 7.Basile C. [Rhabdomyolysis: have you considered food poisoning from quails?] G Ital Nejrol. 2020 Apr 9;37(2) Italian. [PubMed] [Google Scholar]
- 8.Bisaccia C, De Santo NG, De Santo LS. Antonino D’Antona (18421913) was the first in describing the crush syndrome with renal failure following the Messina earthquake of December 28, 1908. G Ital Nejrol. 2016;33(Suppl 660):33.S66.10. PMID: 26913878. [PubMed] [Google Scholar]
- 9.Bywaters EG, Beall D. Crush Injuries with Impairment of Renal Function. Br Med J. 1941;1(4185):427–32. doi: 10.1136/bmj.1.4185.427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bywaters EG, Delory GE, Rimington C, Smiles J. Myohaemoglobin in the urine of air raid casualties with crushing injury. Biochem J. 1941;35(10-11):1164–8. doi: 10.1042/bj0351164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Berlin R. Haff disease in Sweden. Acta Med Scand. 1948;129(6):560–72. doi: 10.1111/j.0954-6820.1948.tb09326.x. [DOI] [PubMed] [Google Scholar]
- 12.Vertel RM, Knochel JP. Acute renal failure due to heat injury. An analysis of ten cases associated with a high incidence of myoglobinuria. Am J Med. 1967;43(3):435–51. doi: 10.1016/0002-9343(67)90196-9. [DOI] [PubMed] [Google Scholar]
- 13.Rowland LP, Penn AS. Myoglobinuria. Med Clin North Am. 1972;56(6):1233–56. doi: 10.1016/s0025-7125(16)32319-7. [DOI] [PubMed] [Google Scholar]
- 14.Grunfeld JP, Ganeval D, Chanard J, Fardeau M, Dreyfus JC. Acute renal failure in McArdle’s disease. Report of two cases. N Engl J Med. 1972;286(23):1237–41. doi: 10.1056/NEJM197206082862304. [DOI] [PubMed] [Google Scholar]
- 15.Graves EJ, Gillum BS. Detailed diagnoses and procedures, National Hospital Discharge Survey, 1995. Vital Health Stat 13. 1997;(130):1–146. [PubMed] [Google Scholar]
- 16.Stanley M, Adigun R. Rhabdomyolysis. StatPearls [Internet] Treasure Island, Florida: StatPearls Publishing LLC; 2020. [[cited 2020 Apr 24]]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK448168/ [Last accessed April 2021] [Google Scholar]
- 17.Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009;361(1):62–72. doi: 10.1056/NEJMra0801327. [DOI] [PubMed] [Google Scholar]
- 18.French Intensive Care Renal Network (F.I.R.N) Candela N, Silva S, Georges B, Cartery C, Robert T, et al. Short- and long-term renal outcomes following severe rhabdomyolysis: a French multicenter retrospective study of 387 patients. Ann Intensive Care. 2020;10(1):27. doi: 10.1186/s13613-020-0645-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gabow PA, Kaehny WD, Kelleher SP. The spectrum of rhabdomyolysis. Medicine (Baltimore) 1982;61(3):141–52. doi: 10.1097/00005792-198205000-00002. [DOI] [PubMed] [Google Scholar]
- 20.McKenna MC, Kelly M, Boran G, Lavin P. Spectrum of rhabdomyolysis in an acute hospital. Ir J Med Sci. 2019;188(4):1423–6. doi: 10.1007/s11845-019-01968-y. [DOI] [PubMed] [Google Scholar]
- 21.Sever MŞ, Vanholder R. Acute kidney injury in polytrauma and rhabdomyolysis [Internet] In: Turner N, et al., editors. Oxford Textbook of Clinical Nephrology. Section 11. Chapter 252. Oxford: Oxford University Press; [[cited 2020 Apr 26]]. Available from: https://oxfordmedicine.com/view/10.1093/med/9780199592548.001.0001/med-9780199592548-chapter-252 [Last accessed April 2021] [Google Scholar]
- 22.Elsayed EF, Reilly RF. Rhabdomyolysis: a review, with emphasis on the pediatric population. Pediatr Nephrol. 2010;25(1):7–18. doi: 10.1007/s00467-009-1223-9. [DOI] [PubMed] [Google Scholar]
- 23.Jin M, Tong Q. Rhabdomyolysis as Potential Late Complication Associated with COVID-19. Emerg Inject Dis. 2020;26(7):1618–20. doi: 10.3201/eid2607.200445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Suwanwongse K, Shabarek N K S, N S. Rhabdomyolysis as a Presentation of 2019 Novel Coronavirus Disease. [[cited 2020 Apr 26]];Cureus. [Internet] 2020 Apr 6;12(4):e7561. doi: 10.7759/cureus.7561. Available from: https://www.cureus.com/articles/30228-rhabdomyolysis-as-a-presentation-of-2019-novel-coronavirus-disease. [Last accessed April 2021.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Paliwal VK, Garg RK, Gupta A, Tejan N. Neuromuscular presentations in patients with COVID-19. Neurol Sci. 2020:1–18. doi: 10.1007/s10072-020-04708-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chong WH, Saha BK. Relationship between severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the etiology of acute kidney injury (aki) Am J Med Sci. 2020;41(11):3039–56. doi: 10.1016/j.amjms.2020.10.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chavez LO, Leon M, Einav S, Varon J. Beyond muscle destruction: a systematic review of rhabdomyolysis for clinical practice. Crit Care Lond Engl. 2016;20(1):135. doi: 10.1186/s13054-016-1314-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gonzalez D. Crush syndrome. Crit Care Med. 2005;33(1 Suppl):S34–41. doi: 10.1097/01.ccm.0000151065.13564.6f. [DOI] [PubMed] [Google Scholar]
- 29.Zager RA. Rhabdomyolysis and myohemoglobinuric acute renal failure. Kidney Int. 1996;49(2):314–26. doi: 10.1038/ki.1996.48. [DOI] [PubMed] [Google Scholar]
- 30.Hendgen-Cotta UB, Flogel U, Kelm M, Rassaf T. Unmasking the Janus face of myoglobin in health and disease. J Exp Biol. 2010;213(Pt 16):2734–40. doi: 10.1242/jeb.041178. [DOI] [PubMed] [Google Scholar]
- 31.Sever MS. Rhabdomyolysis. Acta ClinBelg. 2007;62(Suppl 2):375–9. doi: 10.1179/acb.2007.084. [DOI] [PubMed] [Google Scholar]
- 32.Petejova N, Martinek A. Acute kidney injury due to rhabdomyolysis and renal replacement therapy: a critical review. Crit Care Lond Engl. 2014;18(3):224. doi: 10.1186/cc13897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Holt S, Moore K. Pathogenesis of renal failure in rhabdomyolysis: the role of myoglobin. Exp Nephrol. 2000;8(2):72–6. doi: 10.1159/000020651. [DOI] [PubMed] [Google Scholar]
- 34.Boutaud O, Roberts LJ. Mechanism-Based Therapeutic Approaches to Rhabdomyolysis-Induced Renal Failure. Free Radic Biol Med. 2011;51(5):1062–7. doi: 10.1016/j.freeradbiomed.2010.10.704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Okubo K, Kurosawa M, Kamiya M, Urano Y, Suzuki A, Yamamoto K, et al. Macrophage extracellular trap formation promoted by platelet activation is a key mediator of rhabdomyolysis-induced acute kidney injury. Nat Med. 2018;24(2):232–8. doi: 10.1038/nm.4462. [DOI] [PubMed] [Google Scholar]
- 36.Vanholder R, Sever MS, Erek E, Lameire N. Rhabdomyolysis. J Am Soc Nephrol JASN. 2000;11(8):1553–61. doi: 10.1681/ASN.V1181553. [DOI] [PubMed] [Google Scholar]
- 37.Sauret JM, Marinides G, Wang GK. Rhabdomyolysis. Am Fam Physician. 2002;65(5):907–12. [PubMed] [Google Scholar]
- 38.Cervellin G, Comelli I, Lippi G. Rhabdomyolysis: historical background, clinical, diagnostic and therapeutic features. Clin Chem Lab Med. 2010;48(6):749–56. doi: 10.1515/CCLM.2010.151. [DOI] [PubMed] [Google Scholar]
- 39.Huerta-Alardin AL, Varon J, Marik PE. Bench-to-bedside review: Rhabdomyolysis -- an overview for clinicians. Crit Care. 2005;9(2):158–69. doi: 10.1186/cc2978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lane R, Phillips M. Rhabdomyolysis. BMJ. 2003;327(7407):115–6. doi: 10.1136/bmj.327.7407.115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Akmal M, Massry SG. Reversible hepatic dysfunction associated with rhabdomyolysis. Am J Nephrol. 1990;10(1):49–52. doi: 10.1159/000168053. [DOI] [PubMed] [Google Scholar]
- 42.Khan FY. Rhabdomyolysis: a review of the literature. Neth J Med. 2009;67(9):272–83. [PubMed] [Google Scholar]
- 43.Bagley WH, Yang H, Shah KH. Rhabdomyolysis. Intern Emerg Med. 2007;2(3):210–8. doi: 10.1007/s11739-007-0060-8. [DOI] [PubMed] [Google Scholar]
- 44.Khan FY. Rhabdomyolysis: a review of the literature. Neth J Med. 2009;67(9):272–83. [PubMed] [Google Scholar]
- 45.Slater MS, Mullins RJ. Rhabdomyolysis and myoglobinuric renal failure in trauma and surgical patients: a review. J Am Coll Surg. 1998;186(6):693–716. doi: 10.1016/s1072-7515(98)00089-1. [DOI] [PubMed] [Google Scholar]
- 46.Giannoglou GD, Chatzizisis YS, Misirli G. The syndrome of rhabdomyolysis: Pathophysiology and diagnosis. Eur J Intern Med. 2007;18(2):90–100. doi: 10.1016/j.ejim.2006.09.020. [DOI] [PubMed] [Google Scholar]
- 47.Alfirevic A, Neely D, Armitage J, Chinoy H, Cooper RG, Laaksonen R, et al. Phenotype standardization for statin-induced myotoxicity. Clin Pharmacol Ther. 2014;96(4):470–6. doi: 10.1038/clpt.2014.121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Minnema BJ, Neligan PC, Quraishi NA, Fehlings MG, Prakash S. A case of occult compartment syndrome and nonresolving rhabdomyolysis. J Gen Intern Med. 2008;23(6):871–4. doi: 10.1007/s11606-008-0569-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Baeza-Trinidad R, Brea-Hernando A, Morera-Rodriguez S, Brito-Diaz Y, Sanchez-Hernandez S, El Bikri L, et al. Creatinine as predictor value of mortality and acute kidney injury in rhabdomyolysis. Intern Med J. 2015;45(11):1173–8. doi: 10.1111/imj.12815. [DOI] [PubMed] [Google Scholar]
- 50.de Meijer AR, Fikkers BG, de Keijzer MH, van Engelen BGM, Drenth JPH. Serum creatine kinase as predictor of clinical course in rhabdomyolysis: a 5-year intensive care survey. Intensive Care Med. 2003;29(7):1121–5. doi: 10.1007/s00134-003-1800-5. [DOI] [PubMed] [Google Scholar]
- 51.Safari S, Yousefifard M, Hashemi B, Baratloo A, Forouzanfar MM, Rahmati F, et al. The value of serum creatine kinase in predicting the risk of rhabdomyolysis-induced acute kidney injury: a systematic review and meta-analysis. Clin Exp Nephrol. 2016;20(2):153–61. doi: 10.1007/s10157-015-1204-1. [DOI] [PubMed] [Google Scholar]
- 52.Nanda SK, Dinakaran A, Ray L. Is dilution important: Factitious Total Creatine Kinase in case of Rhabdomyolysis? J Clin Diagn Res. 2016;10(10):BD01–2. doi: 10.7860/JCDR/2016/22338.8738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Cervellin G, Comelli I, Benatti M, Sanchis-Gomar F, Bassi A, Lippi G. Non-traumatic rhabdomyolysis: Background, laboratory features, and acute clinical management. Clin Biochem. 2017;50(12):656–62. doi: 10.1016/j.clinbiochem.2017.02.016. [DOI] [PubMed] [Google Scholar]
- 54.Roxin L-E, Venge P, Friman Gor, Hallgren R. Radioimmunoassays of human myoglobin in serum and urine. Scand J Clin Lab Invest. 1979;39(1):37–46. doi: 10.3109/00365517909104937. [DOI] [PubMed] [Google Scholar]
- 55.Rodrtguez-Capote K, Balion CM, Hill SA, Cleve R, Yang L, El Sharif A. Utility of urine myoglobin for the prediction of acute renal failure in patients with suspected rhabdomyolysis: a systematic review. Clin Chem. 2009;55(12):2190–7. doi: 10.1373/clinchem.2009.128546. [DOI] [PubMed] [Google Scholar]
- 56.Grossman RA, Hamilton RW, Morse BM, Penn AS, Goldberg M. Nontraumatic rhabdomyolysis and acute renal failure. N Engl J Med. 1974;291(16):807–11. doi: 10.1056/NEJM197410172911601. [DOI] [PubMed] [Google Scholar]
- 57.Russell TA. Acute renal failure related to rhabdomyolysis: pathophysiology, diagnosis, and collaborative management. Nephrol Nurs J. 2000;27(6):567–75. quiz 576-7. [PubMed] [Google Scholar]
- 58.Lindner A, Zierz S. [Rhabdomyolysis and myoglobinuria] Nervenarzt. 2003;74(6):505–15. doi: 10.1007/s00115-003-1518-1. German. [DOI] [PubMed] [Google Scholar]
- 59.Poels PJ, Gabreels FJ. Rhabdomyolysis: a review of the literature. Clin Neurol Neurosurg. 1993;95(3):175–92. doi: 10.1016/0303-8467(93)90122-w. [DOI] [PubMed] [Google Scholar]
- 60.Warren JD, Blumbergs PC, Thompson PD. Rhabdomyolysis: a review. Muscle Nerve. 2002;25(3):332–47. doi: 10.1002/mus.10053. [DOI] [PubMed] [Google Scholar]
- 61.Hino I, Akama H, Furuya T, Ueda H, Taniguchi A, Hara M, et al. Pravastatin-induced rhabdomyolysis in a patient with mixed connective tissue disease. Arthritis Rheum. 1996;39(7):1259–60. doi: 10.1002/art.1780390730. [DOI] [PubMed] [Google Scholar]
- 62.Savage DC, Forbes M, Pearce GW. Idiopathic rhabdomyolysis. Arch Dis Child. 1971;46(249):594–607. doi: 10.1136/adc.46.249.594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Liapis H, Boils C, Hennigar R, Silva F. Myoglobin casts in renal biopsies: immunohistochemistry and morphologic spectrum. Hum Pathol. 2016;54:25–30. doi: 10.1016/j.humpath.2016.02.026. [DOI] [PubMed] [Google Scholar]
- 64.Mansoor K, Kheetan M, Shahnawaz S, Shapiro AP, Patton-Tackett E, Dial L, et al. Systematic review of nephrotoxicity of drugs of abuse, 2005-2016. [[cited 2020 May 1]];BMC Nephrol [Internet] 2017 Dec 29;:18. doi: 10.1186/s12882-017-0794-0. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5747941/ [Last accessed April 2021] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Keltz E, Khan FY, Mann G. Rhabdomyolysis. The role of diagnostic and prognostic factors. Muscles Ligaments Tendons J. 2014;3(4):303–12. [PMC free article] [PubMed] [Google Scholar]
- 66.Lamminen AE, Hekali PE, Tiula E, Suramo I, Korhola OA. Acute rhabdomyolysis: evaluation with magnetic resonance imaging compared with computed tomography and ultrasonography. Br J Radiol. 1989;62(736):326–30. doi: 10.1259/0007-1285-62-736-326. [DOI] [PubMed] [Google Scholar]
- 67.Hill OT, Wahi MM, Carter R, Kay AB, McKinnon CJ, Wallace RF. Rhabdomyolysis in the US Active Duty Army, 2004-2006. Med Sci Sports Exerc. 2012;44(3):442–9. doi: 10.1249/MSS.0b013e3182312745. [DOI] [PubMed] [Google Scholar]
- 68.Clarkson PM, Kearns AK, Rouzier P, Rubin R, Thompson PD. Serum creatine kinase levels and renal function measures in exertional muscle damage. Med Sci Sports Exerc. 2006;38(4):623–7. doi: 10.1249/01.mss.0000210192.49210.fc. [DOI] [PubMed] [Google Scholar]
- 69.Prince LK, Abbott KC, Lee JJ, Oliver DK, Olson SW. Creatine Kinase, Coenzyme Q10, Race, and Risk of Rhabdomyolysis. Am J Kidney Dis Off J Natl Kidney Found. 2015;66(3):541–2. doi: 10.1053/j.ajkd.2015.04.045. [DOI] [PubMed] [Google Scholar]
- 70.Scalco RS, Snoeck M, Quinlivan R, Treves S, Laforet P, Jungbluth H, et al. Exertional rhabdomyolysis: physiological response or manifestation of an underlying myopathy? BMJ Open Sport Exerc Med. 2016;2(1):e000151. doi: 10.1136/bmjsem-2016-000151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Sambuughin N, Mungunsukh O, Ren M, Capacchione JF, Horkayne-Szakaly I, Chuang K, et al. Pathogenic and rare deleterious variants in multiple genes suggest oligogenic inheritance in recurrent exertional rhabdomyolysis. Mol Genet Metab Rep. 2018;16:76–81. doi: 10.1016/j.ymgmr.2018.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Wu L, Brady L, Shoffner J, Tarnopolsky MA. Next-Generation sequencing to diagnose muscular dystrophy, rhabdomyolysis, and hyperCKemia. Can J Neurol Sci J Can Sci Neurol. 2018;45(3):262–8. doi: 10.1017/cjn.2017.286. [DOI] [PubMed] [Google Scholar]
- 73.Chan EK, Kornberg AJ, Ryan MM. A diagnostic approach to recurrent myalgia and rhabdomyolysis in children. Arch Dis Child. 2015;100(8):793–7. doi: 10.1136/archdischild-2014-307663. [DOI] [PubMed] [Google Scholar]
- 74.Scalco RS, Gardiner AR, Pitceathly RD, Zanoteli E, Becker J, Holton JL, et al. Rhabdomyolysis: a genetic perspective. [[cited 2020 May 2]];Orphanet J Rare Dis [Internet] 2015 May 2;:10–15. doi: 10.1186/s13023-015-0264-3. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4522153/ [Last accessed April 2021] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kanagasunderam S, Ashley C, Bhojani S, Caldwell A, Ellam T, Kaur A, et al. Clinical Practice Guideline Acute Kidney Injury (AKI) London: The Renal Association; 2019. [[cited 2020 May 2]]. Available from: https://renal.org/health-professionals/guidelines/guidelines-commentaries. [Last accessed April 2021] [Google Scholar]
- 76.Michelsen J, Cordtz J, Liboriussen L, Behzadi MT, Ibsen M, Damholt MB, et al. Prevention of rhabdomyolysis-induced acute kidney injury -A DASAIM/DSIT clinical practice guideline. Acta Anaesthesiol Scand. 2019;63(5):576–86. doi: 10.1111/aas.13308. [DOI] [PubMed] [Google Scholar]
- 77.Eneas JF, Schoenfeld PY, Humphreys MH. The effect of infusion of mannitol-sodium bicarbonate on the clinical course of myoglobinuria. Arch Intern Med. 1979;139(7):801–5. [PubMed] [Google Scholar]
- 78.Atef MR, Nadjatfi I, Boroumand B, Rastegar A. Acute renal failure in earthquake victims in Iran: epidemiology and management. Q J Med. 1994;87(1):35–40. [PubMed] [Google Scholar]
- 79.Scharman EJ, Troutman WG. Prevention of kidney injury following rhabdomyolysis: a systematic review. Ann Pharmacother. 2013;47(1):90–105. doi: 10.1345/aph.1R215. [DOI] [PubMed] [Google Scholar]
- 80.McMahon GM, Zeng X, Waikar SS. A risk prediction score for kidney failure or mortality in rhabdomyolysis. JAMA Intern Med. 2013;173(19):1821–8. doi: 10.1001/jamainternmed.2013.9774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Simpson JP, Taylor A, Sudhan N, Menon DK, Lavinio A. Rhabdomyolysis and acute kidney injury: creatine kinase as a prognostic marker and validation of the McMahon Score in a 10-year cohort. Eur J Anaesthesiol. 2016;33(12):906–12. doi: 10.1097/EJA.0000000000000490. [DOI] [PubMed] [Google Scholar]
- 82.Rodriguez E, Soler MJ, Rap O, Barrios C, Orfila MA, Pascual J. Risk Factors for Acute Kidney Injury in Severe Rhabdomyolysis. [[cited 2020 May 1]];PLoS ONE [Internet] 2013 8(12):e82992. doi: 10.1371/journal.pone.0082992. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3867454/ [Last accessed April 2021] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Manis T, George-Varghese B, Kashani J. Rhabdomyolysis - Go big or go home. Am J Emerg Med. 2019;37(12):2194–6. doi: 10.1016/j.ajem.2019.03.024. [DOI] [PubMed] [Google Scholar]
- 84.Ronco C. Extracorporeal therapies in acute rhabdomyolysis and myoglobin clearance. Crit Care. 2005;9(2):141–2. doi: 10.1186/cc3055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Bastani B, Frenchie D. Significant myoglobin removal during continuous veno-venous haemofiltration using F80 membrane. Nephrol Dial Transplant. 1997;12(9):2035–6. [PubMed] [Google Scholar]
- 86.Amyot SL, Leblanc M, Thibeault Y, Geadah D, Cardinal J. Myoglobin clearance and removal during continuous venovenous hemofiltration. Intensive Care Med. 1999;25(10):1169–72. doi: 10.1007/s001340051031. [DOI] [PubMed] [Google Scholar]
- 87.Baldwin I, Naka T, Koch B, Fealy N, Bellomo R. A pilot randomised controlled comparison of continuous veno-venous haemofiltration and extended daily dialysis with filtration: effect on small solutes and acid-base balance. Intensive Care Med. 2007;33(5):830–5. doi: 10.1007/s00134-007-0596-0. [DOI] [PubMed] [Google Scholar]
- 88.Padiyar S, Deokar A, Birajdar S, Walawalkar A, Doshi H. Cytosorb for management of acute kidney injury due to rhabdomyolysis in a child. Indian Pediatr. 2019;56(11):974–6. [PubMed] [Google Scholar]
- 89.Dilken O, Ince C, van der Hoven B, Thijsse S, Ormskerk P, de Geus HRH. Successful reduction of creatine kinase and myoglobin levels in severe rhabdomyolysis using Extracorporeal Blood Purification (CytoSorb®) Blood Purif. 2020;49(6):743–7. doi: 10.1159/000505899. [DOI] [PubMed] [Google Scholar]
- 90.Zeng X, Zhang L, Wu T, Fu P. Continuous renal replacement therapy (CRRT) for rhabdomyolysis. Cochrane Database Syst Rev. 2014;(6):CD008566. doi: 10.1002/14651858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Premru V, Kovac J, Buturovic-Ponikvar J, Ponikvar R. High cut-off membrane hemodiafiltration in myoglobinuric acute renal failure: a case series. Ther Apher Dial. 2011;15(3):287–91. doi: 10.1111/j.1744-9987.2011.00953.x. [DOI] [PubMed] [Google Scholar]
- 92.Albert C, Haase M, Bellomo R, Mertens PR. High cut-off and high-flux membrane haemodialysis in a patient with rhabdomyolysis-associated acute kidney injury. Crit Care Resusc. 2012;14(2):159–62. [PubMed] [Google Scholar]
- 93.Belmouaz M, Bauwens M, Hauet T, Bossard V, Jamet P, Joly F, et al. Comparison of the removal of uraemic toxins with medium cut-off and high-flux dialysers: a randomized clinical trial. Nephrol Dial Transplant. 2020;35(2):328–35. doi: 10.1093/ndt/gfz189. [DOI] [PubMed] [Google Scholar]
- 94.Szpirt WM. Plasmapheresis is notjustified in treatment of rhabdomyolysis and acute renal failure. J Cardiovasc Surg (Torino) 1997;38(5):557. [PubMed] [Google Scholar]
- 95.Cornelissen JJ, Haanstra W, Haarman HJ, Derksen RH. Plasma exchange in rhabdomyolysis. Intensive Care Med. 1989;15(8):528–9. doi: 10.1007/BF00273565. [DOI] [PubMed] [Google Scholar]