

Abstract
Background:
CrossFit is an increasingly popular, rapidly growing exercise regimen. Few studies have evaluated CrossFit-associated musculoskeletal injuries on a large scale. This study explores such injuries and associated risk factors in detail.
Objective:
To identify the most common musculoskeletal injuries endured during CrossFit training among athletes at different levels of expertise.
Design:
Survey-based retrospective cross-sectional study.
Setting:
Distribution at CrossFit gyms in the United States and internationally. Also published on active online forums.
Participants:
A total of 885 former and current CrossFit athletes.
Methods:
Institutional review board-approved 33-question Web-based survey focused on CrossFit injuries and associated risk factors. Survey submissions were accepted for a period of 6 months.
Main outcome measurements:
Specific injuries with associated workouts, risk factors that affected injury including (1) basic demographics, (2) regional differences in reported injuries, (3) training intensity, and (4) expertise level at time of injury.
Results:
Of the 885 respondents, 295 (33.3%) were injured. The most common injuries involved the back (95/295, 32.2%) and shoulder (61/295, 20.7%). The most common exercises that caused injury were squats (65/295, 22.0%) and deadlifts (53/295, 18.0%). Advanced-level (64/295, 21.7%) athletes were more significantly injured than beginner-level (40/295, 13.6%) athletes. International participants were 2.2 times more likely than domestic US participants to suffer injury. Individuals with 3+ years of CrossFit experience were 3.3 times more likely to be injured than those with 2 or less years of experience. Participants who trained for 11+ h/week were significantly more likely to be injured than those who trained less than or equal to 10 h/week.
Conclusions:
As CrossFit becomes more popular, it is important to monitor the safety of its practitioners. Further studies are needed to explore how to lower this injury prevalence of 33.3%. Areas to focus on include factors that have caused the regional (international vs US states) differences, level of expertise/experience differences (advanced level vs intermediate and beginner levels), and stretching routine modifications.
Keywords: CrossFit, Injury, Muscles, Athletes, weight-lifting
Introduction
CrossFit is one of the most popular and rapidly growing exercise regimens in the world. With more than 13 000 active CrossFit gyms (or boxes), the workouts of the day are commonly practiced by hundreds of thousands of people daily. CrossFit incorporates a physical exercise philosophy, a competitive fitness sport, peer-supporting atmosphere, and to some, a lifestyle. CrossFit workouts include elements from high-intensity interval training, Olympic-style weightlifting, plyometrics, powerlifting, gymnastics, calisthenics, cross training, cardiovascular training, and other exercise routines. 1 CrossFit has 2 unique advantages, that is, it can be done in almost any environment, as well as the aforementioned box, by using the terrain and natural resources to fit almost any clientele, including military personnel (O’Hara et al, 2012) 2 . The second being the overall structure yet variation it offers, one can understand the allure of CrossFit. These high-intensity exercises are conducted in a repetitive fashion with emphasis on minimal “recovery” time. In addition, the founders of CrossFit suggest that their program increases the body’s neuroendocrine response. The combination of high-intensity training, short resting interval between each sets and increased heart rate leads to the initiation of the release of insulin and human-like growth hormones, which in turn is associated with an increase in skeletal muscle tissue growth and muscular strength levels (O’Hara et al, 2012) 2 .
CrossFit attracts participants from a widespread distribution of ages and physical condition. At the rate at which CrossFit has gained its popularity over the last 2 decades, it has not allowed the community to really slow down and asses any possible health risks involved. The risk of injury in CrossFit training has been controversial since its foundation in the early 2000s. While CrossFit Inc. encourages safe technique with proper coaching as well as scaling workouts to prevent injuries, only a handful of studies have been compiled testing the possible injury outcomes compared to other modalities of exercise and training.
A sizable percentage of the studies that take a look at CrossFit and possible injury outcomes are included in the systematic review compiled by Meyer et al. 1 Rhabdomyolysis has been a small aspect that has been touched upon but has shown no incidence in relatively minute sample sizes. 3 There is also a lack of large studies with the understanding and information of other musculoskeletal (MSK) injuries including, but not limited to: muscle strains, stress fractures, ligament injuries, tendinopathies, delayed onset muscle soreness, and more. In the limited studies that have evaluated CrossFit training, the injury rate is noted to be similar to that reported in the literature for sports such as Olympic weightlifting, powerlifting, and gymnastics, and lower than competitive contact sports such as rugby union and rugby league. Shoulder and spine injuries predominate. 3 This relation is also noted in the systematic review by Meyer et al, 1 but goes further to display that males were more likely to be injured and that supervision of a trainer decreased overall injury incidence.
Unlike other training programs, there are no predefined weights or repetition (reps) schedules that participants follow. Instead, there is an emphasis on completing as many reps as possible within a narrow window of time with weight levels deemed appropriate by the participant. At the beginner level, the emphasis is on establishing motor skills and competency to build the structural strength that will allow handling of more advanced movement patterns 4 as well as reducing the risk of future injury within their first year. 5 Furthermore, there is a great deal of customization to individual training schedules. Athletes who train are not obligated to adhere to a specific routine. Exercise regimens are individually tailored to each athlete, and the risk of injury from these exercise combinations can vary from case to case.
It is the goal of this study to compile more data about MSK injuries from CrossFit athletes. Obtaining a better understanding of common injuries and potential risks of CrossFit, we can reduce the risk of injury or better serve our active athlete population who participate in CrossFit. While the number one priority being the individual client’s or athlete’s well-being, the economics revolving injuries in CrossFit must also be taken into consideration. Injuries during military training cost the US Army alone, $125 million yearly for disability compensation. 6 As CrossFit becomes more prevalent as a training modality in US military training systems, we must further the conversation around its possible pros and cons. Bergeron and colleagues 7 when assessing cost-effectiveness, claimed that “there is an apparent disproportionate musculoskeletal injury risk from these demanding programs, particularly for novices, resulting in lost duty time, medical treatment, and extensive rehabilitation.” Later in this article, there may be some contrary evidence, specifically to the assumption Bergeron makes on the risk CrossFit incurs onto novice participants. In order to cut down on CrossFit injuries and costs, we must take an empiric approach. We hope this article adds another puzzle piece to this growing topic, in the attempt to protect athletes and consumers.
Methods
The study was initiated with the creation of a 33-question Web-based survey that was thoroughly reviewed and approved for distribution by the institutional review board in 2016. The survey was securely created on an online survey website, and distributed at numerous gyms across the country (NY, NJ, CA, TX, FL, OH, WA, AZ, MI, NC, PA) and internationally (United Kingdom, Canada, and Australia), as well as published on active online forums (Reddit.com [CrossFit subreddit], Bodybuilding.com, MuscleandStrength.com, and ShapeFit.com) for a period of 6 months. The study was structured as a retrospective cross-sectional study with a special emphasis on analyzing the various factors influencing a CrossFit participant’s likelihood of injury.
Basic demographics such as age and gender were collected early in the survey. Specific factors that could affect the likelihood of injury secondary to CrossFit were then addressed. A primary data point in the survey was the individual’s CrossFit experience level: “Beginner” defined as recently initiated solo training but not at a competitive level, “Intermediate” defined as a group-training multiple times per week but not at a competitive level, and “Advanced” defined as capable of competing in CrossFit games. Other factors assessed included training hours per week, injury type, causative exercise, site of training (state and/or country), instruction regarding proper form and technique, stretching before and between workouts, treatment of injury, injury recurrence, and impact of injury on future CrossFit sessions. Later in the survey, injured participants were able to select from a list of factors that they felt may have contributed to the suffered injury only and during CrossFit sessions. Finally, consent was obtained to use participant data for research purposes.
Participants from the 50 US states and District of Columbia (DC) were pooled into one subgroup. All participants from outside of the 50 US states and DC were pooled into a separate international subgroup with Puerto Rico included. The data were analyzed by creating chi-squares from which odds ratios (ORs) and respective 95% confidence intervals (CIs) were obtained. A threshold of P value less than .05 was used to determine statistical significance.
Results
Our survey drew a total of 885 respondents from 40 different states in the United States, Puerto Rico, and 13 other countries. The number of injured participants was 295 (33.3%), whereas the number of noninjured participants was 590 (66.7%). The most common injury sustained among our participants was back injury (95/295, 32.2%) followed by shoulder injury (61/295, 20.7%) as shown in Figure 1. The most common exercise that caused the injury was squats (65/295, 22.0%) followed by deadlifts (53/295, 18.0%) as shown in Figure 2. The average age of participants was 29 years with a gender distribution of 589 (66.6%) male and 296 (33.4%) female. Of the injured participants, 198 (67.1%) were male and 97 (32.9%) were female. Injury prevalence among male was 198/589 (33.6%) and among female was 97/296 (32.8%). There was no statistical significance in injury prevalence between male and female CrossFit participants in our study (OR: 1.04, 95% CI: .77-1.40, P = .80).
Figure 1.
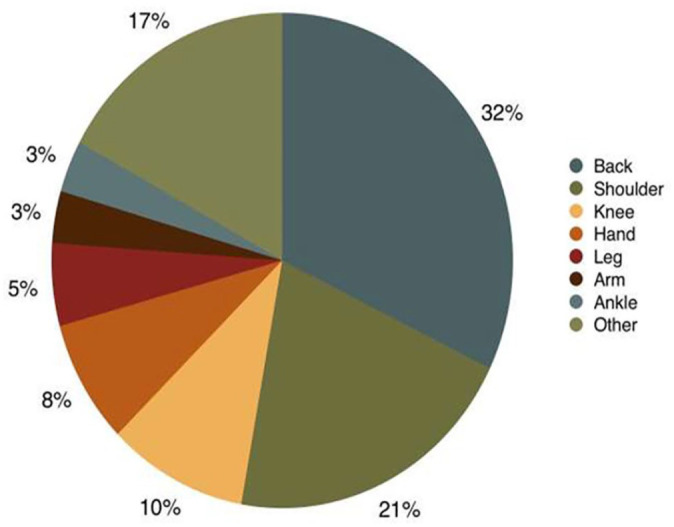
Injury distribution by type.
Figure 2.
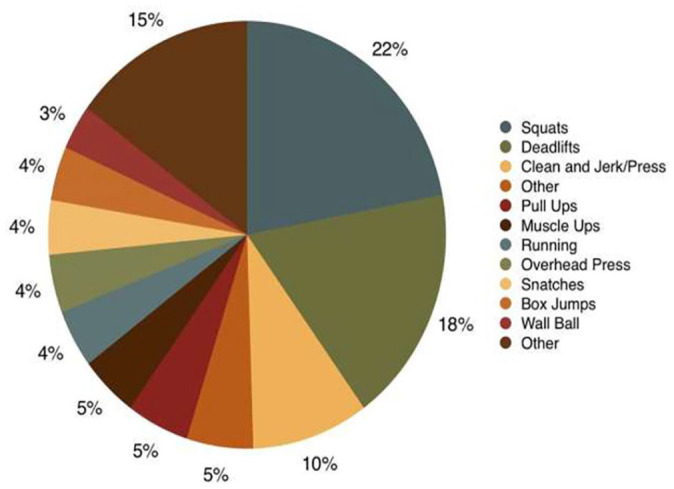
Exercise associated with injury.
Of our 885 subjects, 240 (27.1%) identified as beginner-level participants, 537 identified as intermediate (60.7%), and 108 (12.2%) identified as advanced. When stratifying injured CrossFit participants by level of athleticism, as is shown in Table 1, beginners composed 40/295 (13.6%), intermediates 191/295 (64.7%), and advanced 64/295 (21.7%). Injury prevalence for beginner participants was 40/240 (16.7%), for intermediate 191/537 (35.6%), and for advanced 64/108 (59.3%). For noninjured participants, beginners accounted for 200/590 (33.9%), intermediates 346/590 (58.6%), and advanced 44/590 (7.5%). Our results showed that advanced-level athletes were significantly more likely to be injured than intermediate-level athletes (OR: 2.63, 95% CI: 1.73-4.02, P < .0001). Advanced-level athletes were also more significantly injured than beginner athletes (OR: 7.27, 95% CI: 4.36-12.14, P < .0001). Finally, intermediate-level athletes were significantly more likely to be injured than their beginner-level counterparts (OR: 2.76, 95% CI: 1.88-4.05, P < .0001). When participants were geographically stratified into “50 US states + District of Columbia” and “International + Puerto Rico” subgroups, as is shown in Table 2, the international subgroup was 2.2 times more likely than domestic US participants to suffer injury (OR: 2.21, 95% CI: 1.38-3.54, P = .0009). Stratified by athleticism, international intermediate-level athletes were 2.6 times more likely than US intermediate-level athletes to suffer injury (OR: 2.55, 95% CI: 1.40-4.64, P = .002). Beginner-and advanced-level international athletes were not significantly more likely than US beginner-and advanced-level athletes to suffer injury.
Table 1.
Injury prevalence by level of athleticism.
| Injured (%) | Not injured (%) | |
|---|---|---|
| Beginner | 40 (16.7) | 200 (83.3) |
| Intermediate | 191 (35.6) | 346 (64.4) |
| Advanced | 64 (59.3) | 44 (40.7) |
| Odds ratio for injury prevalence among different level athletes | ||
| Statistical significance | ||
| Beginner vs intermediate | OR: .36 (95% CI: .25-.53), P < .0001 | |
| Beginner vs advanced | OR: .14 (95% CI: .08-.23), P < .0001 | |
| Intermediate vs beginner | OR: 2.76 (95% CI: 1.88-4.05), P < .0001 | |
| Intermediate vs advanced | OR: .38 (95% CI: .25-.58), P < .0001 | |
| Advanced vs beginner | OR: 7.27 (95% CI: 4.36-12.14), P < .0001 | |
| Advanced vs intermediate | OR: 2.63 (95% CI: 1.73-4.02), P < .0001 | |
Abbreviations: CI, confidence interval; OR, odds ratio.
Table 2.
Injury prevalence by geography and athleticism.
| Injured (%) | Not injured (%) | ||
|---|---|---|---|
| 50 US States + District of Columbia | Beginner | 34 (15.4) | 187 (84.6) |
| Intermediate | 164 (33.5) | 325 (66.5) | |
| Advanced | 58 (59.2) | 40 (40.8) | |
| International + Puerto Rico | Beginner | 6 (31.6) | 13 (68.4) |
| Intermediate | 27 (56.2) | 21 (43.8) | |
| Advanced | 6 (60.0) | 4 (40.0) | |
| Odds ratio for injury prevalence among international vs US CrossFit participants | |||
| Statistical significance | |||
| All international vs US participants | OR: 2.21 (95% CI: 1.38-3.54), P = .0009 | ||
| Beginner-level international vs US participants | OR: 2.54 (95% CI: .90-7.14), P = .08 | ||
| Intermediate-level international vs US participants | OR: 2.55 (95% CI: 1.40-4.64), P = .002 | ||
| Advanced-level international vs US participants | OR: 1.03 (95% CI: .27-3.90), P = .96 | ||
Abbreviations: CI, confidence interval; OR, odds ratio.
Those participants with 1 to 5 years of weightlifting experience comprised the largest segment of our injured respondents (147/295, 49.8%). This subgroup also comprised the largest of our noninjured group (313/590, 53.1%). However, injury prevalence steadily increased with years of weightlifting experience, with our most experienced weightlifters (>15 years) most commonly injured (24/48, 50.0%) and our least experienced (<1 year) least injured (37/141, 26.2%). Participants with more than 6 years of weightlifting experience were 1.45 times more likely to be injured than those with 5 or less years of experience (OR: 1.45, 95% CI: 1.08-1.95, P = .013). Similar trends were observed when analyzing our CrossFit athlete participants.
Our respondents who had 1 to 2 years of CrossFit experience comprised the largest of our injured group (95/295, 32.2%), and those with less than 1 year of CrossFit experience were most represented in the noninjured group (313/590, 53.1%), as is shown in Table 3. Similar to our findings in weightlifters, a direct relationship was observed between years of CrossFit experience and overall injury prevalence, as those with 5 or more years of experience had the highest prevalence, 68/108 (63.0%), and those with less than 1 year of experience had the lowest prevalence of injury, 55/368 (14.9%). Individuals with more than 3 years of CrossFit experience were 3.3 times more likely to be injured than those with 2 or less years of experience (OR: 3.26, 95% CI: 2.42-4.39, P < .0001).
Table 3.
Injury prevalence by years of CrossFit experience.
| Years of experience | Injured (%) | Not injured (%) |
|---|---|---|
| <1 | 55 (14.9) | 313 (85.1) |
| 1-2 | 95 (40.1) | 142 (59.9) |
| 3-4 | 77 (44.8) | 95 (55.2) |
| 5 or more | 68 (63.0) | 40 (37.0) |
| Odds ratio for injury prevalence by years of CrossFit experience | ||
| Years of experience | Statistical significance | |
| ⩾3 | OR: 3.26 (95% CI: 2.42-4.39), P < .0001 | |
| 0-2 | ||
Abbreviations: CI, confidence interval; OR, odds ratio.
Participants with 4 to 6 h/week of CrossFit training comprised the largest of our injured group (122/295, 41.4%), while this same group was most represented in our noninjured group (285/590, 48.3%), as is shown in Table 4. Our results indicate that injury prevalence consistently increased with length of CrossFit training time, as our longest trainers (>15 h/week) were most often injured (9/15, 60.0%) and our shortest trainers (0-3 h/week) were least often injured (65/205, 31.7%). Our participants who trained for more than 11 h/week were significantly more likely to be injured than those who trained less than or equal to 10 h/week (OR: 2.27, 95% CI: 1.35-3.82, P = .002).
Table 4.
Injury prevalence by length of CrossFit training time.
| Number of hours per week | Injured (%) | Not injured (%) |
|---|---|---|
| 0-3 | 65 (31.7) | 140 (68.3) |
| 4-6 | 122 (30.0) | 285 (70.0) |
| 7-10 | 76 (36.0) | 135 (64.0) |
| 11-15 | 23 (48.9) | 24 (51.1) |
| >15 | 9 (60.0) | 6 (40.0) |
| Odds ratio for injury prevalence by length of CrossFit training time | ||
| Number of hours per week | Statistical significance | |
| ⩾11 | OR: 2.27 (95% CI: 1.35-3.82), P = .002 | |
| 0-10 | ||
Abbreviations: CI, confidence interval; OR, odds ratio.
Of the 885 participants, 691 (78.1%) reported stretching before beginning exercises, while 205 (23.2%) reported stretching between exercises. Among those who were injured, the injury prevalence among those who stretched before exercises (246/295, 83.4%) was higher than that among those who did not stretch before exercises (49/295, 16.6%), as is shown in Table 5, and this difference was statistically significant (OR: 1.64, 95% CI: 1.14-2.34, P = .007). The injury prevalence among those who stretched between exercises (67/295, 22.7%) was lower than among those who did not stretch between exercises (228/295, 77.3%), and this difference was not statistically significant (OR: .96, 95% CI: .69-1.34, P = .82).
Table 5.
Impact of stretching on injury.
| Injured (%) | Not injured (%) | |
|---|---|---|
| Stretching before exercises | 246 (35.6) | 445 (64.4) |
| Not stretching before exercises | 49 (25.3) | 145 (74.7) |
| Odds ratio for injury prevalence in stretching vs not stretching before exercises | OR: 1.64, 95% CI: 1.14-2.34, P = .007 | |
| Stretching between exercises | 67 (32.7) | 138 (67.3) |
| Not stretching between exercises | 228 (33.5) | 452 (66.5) |
| Odds ratio for injury prevalence in stretching vs not stretching between exercises | OR: .96, 95% CI: .69-1.34, P = .82 | |
Abbreviations: CI, confidence interval; OR, odds ratio.
Of the participants who sustained an injury, 165 (55.9%) stopped training once the injury occurred, 198 (67.1%) received treatment for their injury, and 95 (32.2%) had a recurrence of their initial injury.
Discussion
Our survey-based retrospective cross-sectional study found the injury prevalence among CrossFit athletes to be 33.3%. In a similar retrospective survey of participants in a CrossFit program, the injury incidence was of 74%. 3 This study likely suffered from significant surveillance bias, as the survey was only distributed on online CrossFit forums, whereas our survey was completed online, but also by participants at numerous gyms across the country and internationally. A third study surveyed participants who suffered an injury within 6 months of completing the survey and found an injury rate of 19%. 8 The primary difference between this study and our own was that our model did not restrict responses to injuries suffered within a set time period of completing the survey, allowing us to include participants with prior injuries who may have recovered and since returned to CrossFit.
Of the 885 participants surveyed, a total of 295 (33.3%) reported experiencing an injury during CrossFit training. While the participants were not asked to provide exact diagnoses, the location of injury was prompted. Of the 295 injured participants, 32.2% suffered from back injuries and 20.7% suffered from shoulder injuries. Other studies have shown similar results that the back and shoulders have been the most commonly injured during the exercise regime within a 12-month period. 5 Of the total injured participants, 22% reported that injuries occurred during squats, 18% during deadlifts, and 9.5% during the clean and jerk/press. It is a well-known fact that the lower back is at an increased risk of injury during exercises like weighted squats, deadlifts, and clean and snatch repetitions. With the high-intensity and fast-pace associated with CrossFit routines, loss of form can occur, causing excess stress to be placed on the thoracic and lumbar spine, which would increase risk of injury. In addition, many researchers like Weisenthal et al 8 have demonstrated that classic powerlifting movements such as squats and deadlifts have an enormous impact on lower back injuries, whereas Olympic lifts in CrossFit are the most common causes of shoulder injuries. Athletes need to be educated about the risk of placing increased stress on the lower back when doing these exercises and encouraged to maintain proper lumbar curvature to avoid injury. 8 In addition, shoulder injuries, also referred to as “CrossFit shoulder,” are more likely during low squat snatch position exercises. Poor form can result in hyperflexion, internal rotation, and abduction of the shoulder. 3 Lack of proper technique places extreme forces on the joint and surrounding musculature resulting in injury. The study by Everhart et al 9 goes in depth about the types of treatments received for these CrossFit injuries and notes that 76% of injured subjects received physical therapy, 37.5% underwent advanced imaging such as magnetic resonance imaging, 15.8% received injections, and 15.8% underwent surgery.
The effects of stretching on injury prevention in sports have long been debated within the medical literature, and findings have varied depending on the type of stretch and intensity of the sport. It is generally agreed, however, that sports with high-intensity stretch-shortening cycles require a high storage capacity for potential energy and therefore need more compliant muscle-tendon units. 10 More compliant muscle-tendon units are better equipped for the rapid transfer of maximal energy during physical activity and are less likely to injure from forces applied. As CrossFit is considered a high-intensity and fast-paced workout, the need for optimally compliant muscle-tendon units cannot be overstated. We briefly explored how stretching may be associated with injuries in CrossFit athletes and found that, of the injured participants, 246/295 (83.3%) stretched before exercises and 67/295 (22.7%) stretched between exercises.
We were unable to specify in the questionnaire the type of stretching that the survey participants used before and during exercises. Some of the different types include static, dynamic, and proprioceptive neuromuscular facilitation stretching. A few studies have demonstrated that static stretching can cause a statistically significant reduction of musculotendinous and ligament injuries specifically. 11 Dynamic stretching has been found to help elevate core body temperature and increase nerve conduction velocity and muscle compliance, which accelerates energy production. This increase in muscle compliance can theoretically decrease the susceptibility to injury during activity. However, further studies are required to determine if dynamic stretching will produce a significant reduction in injury prevalence. More data are needed on the type of stretching CrossFit athletes currently use to formulate optimal evidence-based stretch recommendations that can be incorporated into their workouts. Another area to explore further is the utility to stretching between exercises. Current literature does not have sufficient data on the effect of interexercise stretching, and its impact on injury reduction or prevention. Owing to the rapid and consecutive circuit-like nature of CrossFit, it is not clear whether stretching between sets will provide a benefit without interrupting the structure of the workout.
Of our injured participants, advanced-level athletes (n = 108) were 2.63 times (P < .0001) more likely to be injured than intermediate-level athletes (n = 537) and 7.27 times more likely (P < .0001) to be injured than beginner-level participants (n = 240). These results are consistent with the findings from a cross-sectional study of injuries sustained during an extreme conditioning program (ECP) such as CrossFit, in which experienced athletes who participated in the ECP for at least 6 months were 4.4 times more likely to have sustained an injury (42% vs 14%, P < .05) than inexperienced athletes who had less than 6 months of ECP training. 12 Figure 3 shows the clear-positive correlation between injury prevalence and years of CrossFit experience. Our finding corroborates previous studies findings in which,
the proportion of injuries was dependent on how long a participant had participated in CrossFit training. Those with 3 years of experience reported more injuries (43.1%) compared with those with 1 to 3 years (38.8%) and those with less than 1 year (18.0%) of experience. 5
Figure 3.
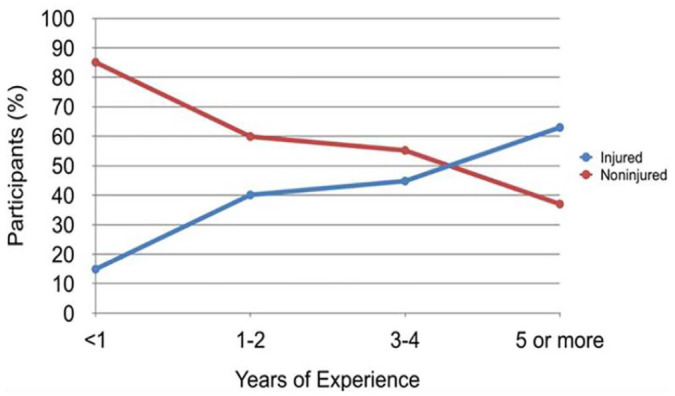
Injury prevalence by years of CrossFit experience.
To explore causative factors for this positive correlation, participants were asked if they were given appropriate instruction for the exercise that caused the injury and 271 (91.9%) answered “yes.” In addition, when asked what injured participants attributed their injury to, the largest percentage, 99 (33.6%), chose “training beyond capacity” and the next largest percentage, 84 (28.5%), chose “negligence.” In fact, a recent study by Elkin et al 13 noted that CrossFit participants were 1.3 times more likely to suffer injuries and 1.86 times more likely to seek medical attention when compared to traditional weightlifters. They postulate that this increase in injury rate seen in CrossFit participants is related to the intensity in which exercises are being performed and less to the types of exercises executed. These data make the case that CrossFit personnel have sufficiently instructed participants in specific CrossFit workouts, and the onus may fall on the participants to take further initiative to ensure personal safety during the high-risk exercise regimens, especially a few years into their training. However, coaches are still advised to pay close attention to athletes when they train, as this may significantly decrease the injury rate (P = 0.028). 8 Figure 4 shows the prevalence of injury among participants relative to the numbers of hours per week training. Here too, there is a clear positive correlation between injury prevalence and higher hours per week of training. This finding may also be supported by the fact that most injured participants attributed their injury to training beyond capacity and negligence. However, previous studies have also found dissimilar data to ours suggesting that those who get injured more often have in common 3 variables—participants are new (within their first year), engage in CrossFit less than 3 days a week, and engage in less than 3 workouts/week. 5 Minghelli et al 14 found that participants of CrossFit who trained twice or less than a week had a 3.24 greater probability of injury than those who exercised more. Furthermore, unlike Feito et al’s study and many others, this is the first retrospective study that not only contains a sample of 885 worldwide subjects but also compares them individually as an international subgroup and in relation to subjects practicing CrossFit within the United States.
Figure 4.
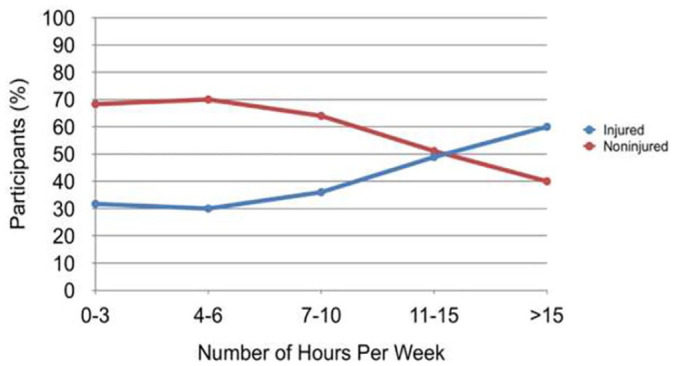
Injury prevalence by length of CrossFit training time.
When stratifying the group’s participants by geographic distribution, the data provide some further insight into the possible influence of an area’s CrossFit training culture on the likelihood of injury, depending on level of expertise. Across both US and international subgroups, intermediate-level athletes constituted the majority of injured participants. However, our stratified analysis found injury prevalence to be highest in advanced-level athletes, especially in the United States, next highest in intermediate-level athletes, and lowest in beginner-level athletes. Why are our advanced-level athletes consistently more often injured? We postulate that this is because these athletes may be compromising appropriate technique, as they exercise at increased intensities with fewer rest intervals. Further studies are necessary to more closely evaluate these interrelated factors and to better understand this higher injury prevalence at the advanced level. Regardless, trainers should be encouraged to be more attentive to advanced-level athletes and monitor for signs of fatigue for injury prevention. In fact, the study by Weisenthal et al 8 noted that the presence of a trainer/coach had a decreasing effect on the injury rate in both the male and female.
Furthermore, the distribution of injury seen internationally among beginner-, intermediate-, and advanced-level athletes are consistent with that seen in the United States, with intermediate-level competitors accounting for the most frequent injuries. However, there appears to be a significantly greater overall injury prevalence among international CrossFit participants as compared to those from the United States (50.6% vs 31.7%), and the former group is 2.2 times more likely to be injured than the latter (OR: 2.21, 95% CI: 1.38-3.54, P = .0009). When accounting for level of athleticism, international intermediate-level athletes were 2.6 times more likely than US intermediate-level athletes to suffer injury (OR: 2.55, 95% CI: 1.40-4.64, P = .002). Beginner- and advanced-level international athletes were not significantly more likely than their US beginner- and advanced-level counterparts to suffer injury. This finding is however likely attributable to the low number of international participants in the study. The overall increased prevalence of injury internationally could be explained by a decreased emphasis on proper form, less education on the dangers of overexertion, or an inadequate number of trainers or ancillary staff at these locations. Previous international studies have investigated injury incidence rate of CrossFit athletes: 22.6% of participants in a Portuguese study were found to be injured over a 6-month period. 14 Meanwhile, a 39.9% injury incidence was noted in a retrospective study conducted in Italy, 15 as well as 56.1% in a Dutch study 16 and 31% among Brazilian CrossFit 17 athletes. Such a varying degree of injury incidence rates internationally potentially indicates that the different experiences of CrossFit training around the world, from coaching to technique to overall culture, may deviate significantly from country to country. While CrossFit is generally considered an overall safe training modality, 5 the findings certainly warrant further investigation elucidating geographic variations among international populations, especially given the stark increased risk of injury among intermediate-level athletes internationally. Italian athletes who attended a training course of “basic CrossFit movements” “with particular attention to mechanism” prior to the onset of CrossFit training, On-Ramp, were noted to have significantly less injuries. In addition, our study on the relationship between stretching prior to exercises and injuries experienced, although limited as explained above, calls for further investigation into a better-structured CrossFit training regimen. Standardization of a specific exercise regimen may be beneficial in reducing injuries potentiated by CrossFit training.
Study Limitations
There are a few limitations to our study. As participants were not required to mention how long ago the injury was incurred, recall bias could have influenced the number or type of reported risk factors. To further add to a potential recall bias, the study was conducted via a retrospective cross-sectional questionnaire, where participants could have recalled information incorrectly and therefore skew the data. While the best way to correct recall bias is to decrease the time from injury to reporting in the case of CrossFit, we could not intervene in time because it was a retrospective study, and the injuries could have been from years prior. Furthermore, there may be a degree of self-selection bias, as athletes who were injured from CrossFit may have been more predisposed to complete our survey. Although there were participants from 40 US states, Puerto Rico, and 13 other countries, some states and countries are overrepresented because of more participants and popularity of these training programs in those respective geographical areas. Our definitions of beginner-, intermediate-, and advanced-level athletes were not on the basis of time spent training in CrossFit but rather on the basis of experience, using the assumption that the normal trajectory of training is from the individual setting to groups, and ultimately to professional competition. This approach does not account for participants who may have hastily transitioned to group-training or even qualified for CrossFit games without adequate beginner-level training, a practice that could reasonably increase risk for injury. In addition, this study does not report an injury rate (injuries/1000 h of training) as some of the other studies do. Therefore, we must be cautious when comparing injury prevalence and incidence with the results of others. A final limitation is that athletes reported 1 injury/survey response, so while most may have reported their most significant injury, this may not have been the case across all participants.
Conclusion
CrossFit has become one of the most prevalent exercise regimens since the 2000s, increasing in popularity in the last 5 years. For this reason, it is extremely important to study the relationship between CrossFit-specific exercises and injury prevalence, with the goal of creating a safer (individually based) training program. Our study demonstrates that about one-third (33.3%) of the 885 participants experienced an injury during their training, with the lower back and shoulder being the most common sites of injury. Workouts that incurred the most injuries were squats, deadlifts, and clean and jerks. Our findings suggest that participants at more advanced levels of training, specifically with 3+ years of experience, those training 11+ h/week, and those training internationally outside of the United States were significantly more susceptible to CrossFit-related MSK injuries.
Further studies are necessary to explore means by which this injury prevalence can be reduced, especially in the specific groups listed above. The regional variation in injury prevalence is worth exploring further. There is always a certain degree of variation from gym to gym however the international participants, especially those at intermediate levels of training, reported significantly greater number of injuries than their intermediate-level counterparts in the United States. Further studies are also necessary to more closely evaluate why advanced-level athletes, especially in the US states are reporting more injuries than the intermediate-level and beginner-level athletes. Advanced-level athletes may be compromising appropriate technique, as they exercise at increased intensities with fewer rest intervals, especially a few years into their training. The fact that a vast majority of subjects picked “training beyond capacity” and “negligence” as the cause of their injury supports the aforementioned assumption. They may require more attention from trainers than previously anticipated. Another area that can be further explored is the type of stretching the athletes used (static stretching, dynamic stretching, or both) so better evidence-based recommendations can be introduced to incorporate during CrossFit routines. Hopefully, this study will spur further research on novel CrossFit exercise regimens to decrease the prevalence of injury and improve quality of life.
Footnotes
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Note: Abstract presented at the Association of Academic Physiatrists Annual Meeting 2017.
Author Contributions: All authors contributed to the collection of data, analysis and writing of the manuscript.
ORCID iD: Alex John  https://orcid.org/0000-0002-7335-0859
https://orcid.org/0000-0002-7335-0859
References
- 1. Meyer J, Zuniga J, Morrison J. The benefits and risks of CrossFit: a systematic review. Workplace Health Saf. 2017;65:612-618. doi: 10.1177/2165079916685568. [DOI] [PubMed] [Google Scholar]
- 2. O’Hara RB, Serres J, Traver KL, Wright B, Vojta C, Eveland E. The influence of nontraditional training modalities on physical performance: review of the literature. Aviat Space Environ Med. 2012;83:985-990. doi:10.3357/ASEM.3376.2012. [DOI] [PubMed] [Google Scholar]
- 3. Hak PT, Hodzovic E, Hickey B. The nature and prevalence of injury during CrossFit training. J Strength Cond Res. 2013; [Epub ahead of print]doi:10.1519/JSC.0000000000000318 [DOI] [PubMed] [Google Scholar]
- 4. Campi M. How to injury proof your CrossFit. Breaking Muscle, June 19, 2018. http://breakingmuscle.com/functional-fitness/how-to-injury-proof-your-crossfit. Accessed November 17, 2017
- 5. Feito Y, Burrows EK, Tabb LP. A 4-year analysis of the incidence of injuries among CrossFit-trained participants. Orthop J Sports Med. 2018;6:2325967118803100. doi: 10.1177/2325967118803100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Poston WSC, Haddock CK, Heinrich KM, Jahnke SA, Jitnarin N, Batchelor DB. Is high-intensity functional training (HIFT)/CrossFit safe for military fitness training? Mil Med. 2016;181:627-637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bergeron MF, Nindl BC, Deuster PA, et al. Consortium for Health and Military Performance and American College of Sports Medicine consensus paper on extreme conditioning programs in military personnel. Curr Sports Med Rep. 2011;10:383-389. doi: 10.1249/JSR.0b013e318237bf8a. [DOI] [PubMed] [Google Scholar]
- 8. Weisenthal BM, Beck CA, Maloney MD, DeHaven KE, Giordano BD. Injury rate and patterns among CrossFit athletes. Orthop J Sports Med. 2014;2:2325967114531177. doi: 10.1177/2325967114531177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Everhart J, Kirven J, France T, Hidden K, Vasileff W. Rates and treatments of CrossFit-related injuries at a single hospital system. Curr Orthopaed Prac. 2019;30:347-352. [Google Scholar]
- 10. Witvrouw E, Nele M, Lieven D, et al. Stretching and injury prevention. Sports Med. 2004;34(7):443-449. doi:10.2165/00007256-200434070-00003. [DOI] [PubMed] [Google Scholar]
- 11. Small K, Mc Naughton L, Matthews M. A systematic review into the efficacy of static stretching as part of a warm-up for the prevention of exercise-related injury. Res Sports Med. 2008;16:213-231. doi: 10.1080/15438620802310784. [DOI] [PubMed] [Google Scholar]
- 12. Aune K, Powers J. Injuries in an extreme conditioning program. Sports Health. 2017;9:52-58. doi: 10.1177/1941738116674895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Elkin JL, Kammerman JS, Kunselman AR, Gallo RA. Likelihood of injury and medical care between CrossFit and traditional weightlifting participants. Orthop J Sports Med. 2019;7:2325967119843348. doi: 10.1177/2325967119843348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Minghelli B, Vicente P. Musculoskeletal injuries in Portuguese CrossFit practitioners. J Sports Med Phys Fitness. 2019;59:1213-1220. doi: 10.23736/S0022-4707.19.09367-8. [DOI] [PubMed] [Google Scholar]
- 15. Tafuri S, Salatino G, Napoletano P, Monno A, Notarnicola A. The risk of injuries among CrossFit athletes: an Italian observational retrospective survey. J Sports Med Phys Fitness. 2019;59:1544-1550. doi: 10.23736/S0022-4707.18.09240. [DOI] [PubMed] [Google Scholar]
- 16. Mehrab M, de Vos RJ, Kraan GA, Mathijssen NMC. Injury incidence and patterns among Dutch CrossFit athletes. Orthop J Sports Med. 2017;5:2325967117745263. doi: 10.1177/2325967117745263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Sprey JW, Ferreira T, de Lima MV, Duarte A, Jr, Jorge PB, Santili C. An epidemiological profile of CrossFit athletes in Brazil. Orthop J Sports Med. 2016;4:2325967116663706. doi: 10.1177/2325967116663706. [DOI] [PMC free article] [PubMed] [Google Scholar]