

Abstract
Pandemics pose new and difficult challenges. Risks associated with the spread of pandemics generate intense speculation in Western media. Taking the 2014–2015 Ebola outbreak as a case study, the article critically analyses how the risk of contagion in the US, Europe, and the UK has been constructed in UK media and policy discourse. Drawing on the importance of media framing in shaping a given problem definition, causal interpretation and treatment recommendation, the article critically assesses the impacts of the British newspaper framing of Ebola, questioning the rationale of a UK domestic political response based on containment and border screenings. The article also takes a comparative angle, engaging with constructions of previous pandemics. Underscoring the importance of a sociological analysis of these framings, the article critically reflects on the role of media communication in reproducing certain topoi, which reduce the scope for open public debate around best responses to a pandemic emergency.
Keywords: contagion, Ebola, frame analysis, infectious disease, media coverage, outbreak, pandemics, preparedness, risk communication, security
Introduction
Pandemics pose new and difficult challenges, not least in relation to mapping and controlling contagion beyond the immediate locations of disease outbreak. The recent unfolding of the Ebola crisis, the 2002–2003 SARS pandemic and the 2009 H1N1 flu epidemic illustrate some of the implications and added complexities of increased connectivity.
Risks associated with the spread of pandemics generate intense and high-profile speculation in Western media. Taking the recent Ebola outbreak as a case study, the article critically analyses how the risk of pandemic contagion in the US, Europe, and the UK has been constructed in UK media and policy discourse. Drawing on the importance of media framing in shaping a given problem definition, causal interpretation and treatment recommendation (Entman, 1993), the article critically discusses the impacts of the dominant framings circulating in national media coverage in 2014. While social media analysis promises interesting insights into detection of crises and rapid communication in an emergency, national newspaper coverage continues to be central to the framing of public and policy debates on security and health emergencies (Dry and Leach, 2010). Against the chronology of the Ebola outbreak and its rapid unfolding in 2014–2015, this article takes a novel and original approach by mapping the development of different frames in the media against the backdrop of the policy actions taken in the UK. First, a significant contribution of this article is thus to theorise the evolution and succession of framings that appeared in the UK press, culminating in the media re-framing of a humanitarian health crisis into a threat to security primarily.
Second, the article also calls into question the rationale of a UK domestic political response based on containment, which was instantiated through entry screening at UK ports of entry, despite little clinical evidence of their efficacy and sensitivity. The significance of my findings is thus to query the robustness of this response by exploring the interaction between media and policy and arguing that the policy response may have received legitimation through the dominant media coverage of events.
Third, the implications of the findings presented here extend beyond the Ebola outbreak case study. The article also takes a comparative angle, and engages with research on the construction of previous pandemics, critically unpacking some of the main commonalities and differences that emerge in relation to previous outbreak events. As pandemic threats, and particularly the next influenza pandemic, are predicted to be both impending and unavoidable, the significance of this article is also to critically reflect on the role of mainstream media communication both in the event of the next pandemic emergency and in the phase of preparedness planning that is currently ongoing (ahead of the next pandemic). Mainstream media, as the UK Ebola coverage shows, can reproduce certain unhelpful topoi, which become problematic as they may reduce the scope for open public debate around best responses to infectious disease – for example, by narrowly focusing response efforts and resources on (unrealistic) containment of disease outside of the UK borders.
Pandemic risk and preparedness
Global pandemics are increasingly seen as among the most serious threats that contemporary Western societies may have to face (Davis, 2005; Elbe, 2010; Fidler, 2004; McInnes et al., 2014; Sipress, 2009). Under the aegis of the World Health Organization (WHO), various mechanisms for surveillance and cooperation have been established – most notably the Global Outbreak Alert and Response Network (GOARN) in 2000.1 The recent reform of the International Health Regulations (IHR; WHO, 2005) was also accomplished to tighten global surveillance. Plans to respond to future pandemics have been formulated by 109 countries (Scoones, 2010), generating a wide set of protocols to inform best practice and rapid mitigation in a bio-emergency crisis of this type. In some cases, such preparations are pursued under the remit of enhancing resilience to biological risk (for instance, see Elbe (2010: 67–98) for a discussion of the Bush Administration’s BioShield Programme). Thus, they are considered alongside the threat of terrorist attacks, such as contamination of key infrastructure (including water reservoirs) or the direct exposure of citizens to lethal agents, as in the notorious anthrax attacks in the US. In the UK, the National Security Strategy considers an influenza pandemic ‘an example of a natural threat, classified as a tier one risk to the UK’ (Public Health England, 2014b: 11; HM Government, 2010). This is the most serious category of risk which the register acknowledges.
The sense of imminence and foreboding associated with pandemic threats is starkly in contrast with the post-war narrative of modernisation, whose optimism, peaking in the 1960s and 1970s, had consigned infectious disease to the history books. A new era of anti-viral medication, vaccine, and antibiotic research promised then much progress against all known infectious diseases (Abraham, 2007; Dry and Leach, 2010). The advent of the HIV/AIDS epidemic in the early 1980s shook the global scientific community out of its complacency, as it became obvious then that novel and lethal infectious diseases were still emerging. Even when they were not spreading as silently and widely as HIV/AIDS did, novel lethal communicable diseases like Ebola and other fatal haemorrhagic fevers had been observed to occur intermittently since the mid-1970s in parts of Africa. Other diseases, though not novel, were suddenly re-emerging in variants resistant to known antibiotic treatment (Abraham, 2007; Dry and Leach, 2010). However, it was probably only with the advent of the severe acute respiratory syndrome (SARS) in 2003–2004 that our understanding of pandemic risk in the West was revolutionised (Abraham, 2007). SARS demonstrated how a disease outbreak in a location in China could travel fast and infect victims in a matter of hours in some of the most highly developed and industrialised cities on the map, from Singapore and Hong Kong to Toronto, causing havoc and spreading panic. SARS was a novel disease diffusing via the extensive mobility of citizens around the globe and illustrating what a 21st century ‘plague’ would look like in a highly interconnected world (Abraham, 2007). Despite much panic and loss of life (approximately 800 deaths globally), thanks to the rapid and coordinated interventions taken during SARS, and in no little measure thanks to its mode of transmission, which could be arrested though stringent traditional methods of viral infection isolation and quarantine, the outbreak was very rapidly contained. However, as those involved in flu pandemic preparedness continue to highlight, in the likely event of a future type A influenza pandemic (not unlike the 1918 Spanish Flu) a much more apocalyptic death toll would be likely to materialise, resulting in the death of tens of millions of citizens globally (Davis, 2005; Sipress, 2009).
The media and pandemics
The SARS pandemic and subsequent avian flu scares have generated intense media coverage (for instance, see Abraham, 2007 on SARS; Scoones, 2010 on the 2009 H1N1 flu). The role of the Internet and social media alongside that of mainstream press outlets cannot be underestimated, as international mechanisms of surveillance regulated by the WHO are now open to receive alerts from these new media, alongside communication issued from official channels (Dry, 2010). This is also in recognition of the role played by Internet communication in raising the alarm during the SARS outbreak (Fidler, 2004). The Chinese authorities initially sought to silence any official news coverage of a serious and ill-understood outbreak within China’s territories, as well as any news of its lethality and speculations about its possible causes or potential to spread further (Fidler, 2004). The initial mishandling of the SARS crisis allowed the disease to spread undetected to Hong Kong, Singapore, Canada and Vietnam, as well as to other destinations (Fidler, 2004). As Fidler (2004) explains, the alarm about the presence of a lethal disease in China was sounded through personal email communication, by a retired medical professional who courageously took the risk of disobeying state censure.
These events have since prompted revisions within the IHR (WHO, 2005) changing the way surveillance is collected (i.e. from a wider set of sources, including informal ones), and introducing new duties for nation states to promptly report outbreaks to the international community (Dry, 2010; Fidler, 2004; WHO, 2005).
Novel modes of operationalising data gathering from tweets, blogs, and other social media micro-post sources are also being tested with a view to detect in near-to-real-time the emergence of a crisis, with the aim of increasing situation awareness. This can involve sentiment analysis (Schulz et al., 2013), through semantic text mining analysis of the data collected, particularly focusing on certain keywords being used and their prevalence. These media are being studied also for their potential to guide intervention in the event of failure of formal assistance networks (Yang et al., 2009) and to communicate health and emergency messages to various publics (for instance, see Sastry and Lovari’s (2017) analysis of facebook posts by Centers for Disease Control and Prevention (CDC) and WHO).
Nonetheless, newspaper media coverage (in print or online), especially that produced through national channels in the West, continues to remain central to the framing of public and policy debates there on national security and health emergencies, like pandemics (Dry and Leach, 2010; Stephenson and Jamieson, 2009; Wald, 2008). As such it remains of great relevance to analysts interested in the debates and the policy-making connected to pandemic threats.2 As I argue below, mainstream media coverage of pandemics is intent on reproducing unhelpful topoi, which may reduce the scope for open public debate around best responses to a serious infectious disease outbreak – for example, by narrowly targeting response and resources around (unrealistic) efforts to contain disease outside UK borders.
Methodology and data collection
A wide range of disciplines have conceptualised the notion of framing, seeing frames as cognitive schemata through which we perceive, organise, and communicate experiences or as conscious devices used strategically for casting ‘events’ in a certain light, defining ‘the issues’ that we ought to attend to, and prioritising some interventions and responses over other possible ones (Pieri, 2009). Hence, some frame analyses explore the intentions of frame producers, others focus on the frames recovered by the analysts, while others still pay attention to frames as they may be perceived, resisted, or even re-worked by various audiences. The approach to Frame Analysis that I adopt is prevalent in media studies (Kitzinger, 2007) and indebted to the work of Robert Entman (2007), who highlights that framing can generally be used to perform four distinct but often interrelated functions – problem definition, causal analysis, expression of moral judgement, and promoting a remedy. Entman’s definition of framing is widely used in media analysis (Halfpenny et al., 2009) and it states that
[t]o frame is to select some aspects of a perceived reality and make them more salient in a communicating text, in such a way as to promote a particular problem definition, causal interpretation, moral evaluation, and/or treatment recommendation. (Entman, 1993: 52)
Drawing on Entman, I conducted an analysis of British newspaper coverage to identify the dominant frames circulated via UK mainstream media into the public arena about the threat posed by Ebola. The results of my analysis, presented below, reveal how risks were configured in the coverage and how these narratives enabled certain judgements to be made about how best to tackle the threat posed by Ebola. As I discuss in the article, for example, in relation to hospital preparedness, powerful framings can at times be resisted and even reframed by different actors (also see Pieri, 2009). Nonetheless, dominant framings can also contribute to legitimise the implementation of policy interventions, for example, the ineffective UK border screening against Ebola.
The article takes a novel and original approach by seeking to map the development of different frames in the media against the backdrop of the policy actions taken in the UK, so as to explore the interaction between media and policy. For this reason, while all articles mentioning Ebola were retrieved, their analysis was organised in consecutive chronological snapshots along the milestones of the Ebola crisis development, as set out in the official expert review of the outbreak and the lessons learnt, which was conducted for the UK Parliament (House of Commons, 2016b).
To access electronically the UK coverage of the recent Ebola crisis (2014–2015), I used the online LexisNexis archive.3 My sampling protocol involved searching and analysing coverage on Ebola from all UK national newspapers for the period 2014–2015, using a range of recall keywords (e.g. Ebola and pandemic or epidemic) and structuring both the searches and the analysis around a chronology of the unfolding of the pandemic. The chronology of events appeared in the report entitled ‘Ebola: responses to a public health emergency’ (House of Commons, 2016b) and presents the unfolding of the crisis along the following milestones:
First case (later believed to have) occurred in December 2013 in Guinea;
First formal diagnosis (and declaration of outbreak) of Ebola in March 2014;
Disease first spreads to Liberia in late March;
Disease appearing to subside in May;
First cases reported in Sierra Leone in late May;
337 reported dead by June (deadliest Ebola epidemic in history);
WHO declaration that the epidemic is a Public Health Emergency of International Concern on 7 August;
UK Department of International Development: frontline response arrangements in July, scaled up in August, after WHO declaration, and in September; British Military personnel involvement; creation of six Ebola treatment centres (after the UN request for UK leadership in containment in Sierra Leone);
Pandemic peaks in November 2014, then declines;
Liberia declared Ebola-free on 9 May 2015; sporadic cases in June and July declared Ebola-free again in September 2015; more sporadic cases in late November declared Ebola-free on 14 January 2016;
Sierra Leone declared Ebola-free on 7 November 2015;
Guinea declared Ebola-free on 29 December 2015.
Following this chronology, I identified a series of snapshots, whose start and end dates coincided with some of the key milestones, and collected articles accordingly. For instance, I initially took a snapshot spanning from 1 January 2014 (the first case of Ebola was retrospectively dated as occurring in late December 2013) to 1 May 2014. This snapshot was sampled to explore how risk was initially framed upon news of the outbreak and how its pandemic potential was constructed at this stage, since by then the disease had spread across countries. I focused on UK coverage from inception of reporting on Ebola in January to the subsequent peaking of the crisis and its decline, and through critical engagement with the coverage I aim to show how these dominant framings interlock with the UK policy interventions that were being formulated and acted upon to tackle the crisis. In this article, I specifically focus on the 2014 UK coverage from the inception of Ebola (January 2014) to the implementation of the UK border screening measure (14 October 2014).4
Dominant media framings of Ebola
The dominant frames were recovered by qualitative textual analysis, and each qualitative dataset (i.e. each consecutive snapshot of coverage) was read and annotated for frame analysis, through an inductive process of iterative identification, consolidation, and revision of emerging and recurrent themes and their grouping together to form larger frames (Halfpenny et al., 2009; Kitzinger, 2007; Mason, 2006). While largely qualitative, my analysis was also assisted by WordSmith software, which allowed me to compute and visualise concordances, or the lexical items5 that collocate with the lexical items of interest to me – for example, ‘Ebola’, ‘pandemic’, ‘epidemic’ – in these articles. I was able to observe which words (nouns, adjectives, verbs, and other semantic particles) appeared immediately next or nearby my keywords of interest, as illustrated in Figure 1.
Figure 1.

A concordance search output on WordSmith.
Using WordSmith, I also looked at frequency lists (the most frequent items/words recurring in the articles collected – for example, ‘crisis’, ‘threat’, ‘risk’) and explored clusters (larger units of lexical items/words which occurred together a number of times in these articles), for example see Figure 2.
Figure 2.
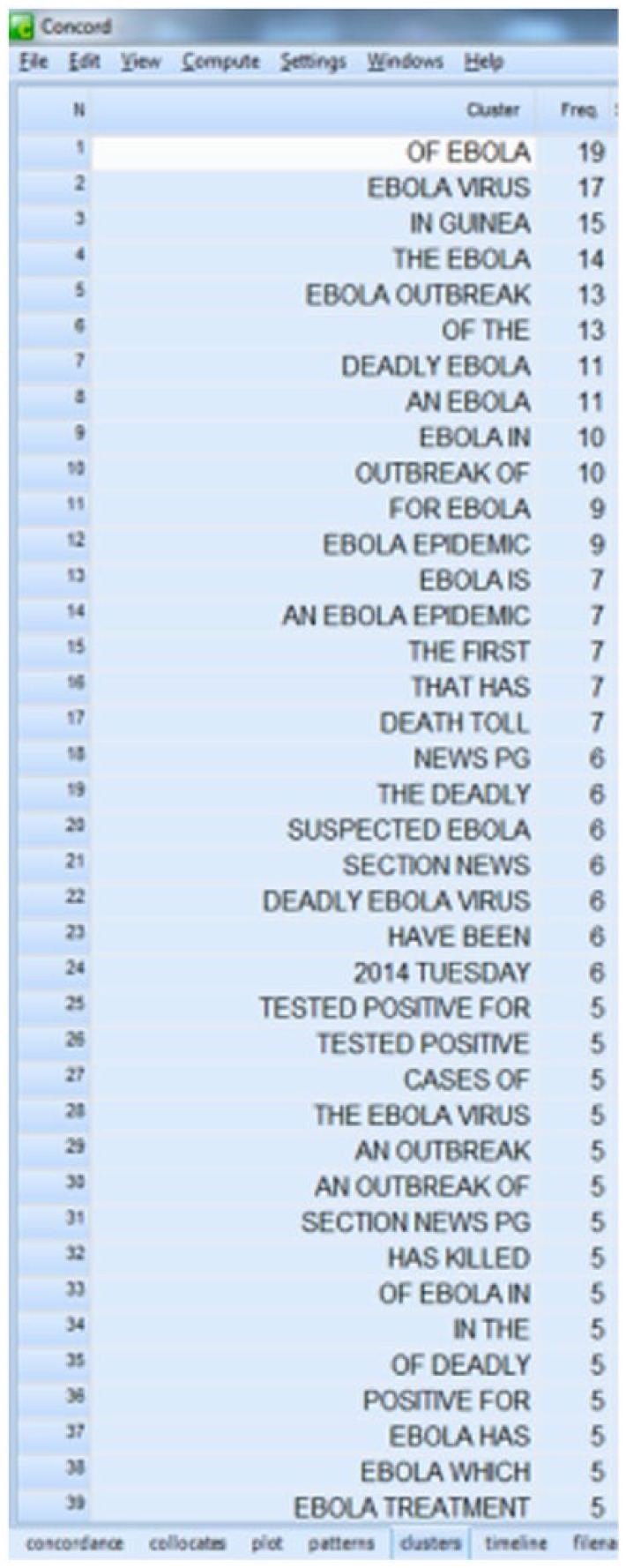
A cluster search output on WordSmith.
Frames are presented in chronological order below, so as to display their permanence or evolution over time, and to allow their mapping against the development of British policy response.
A localised African crisis
Initially, the Ebola crisis was framed as a localised African crisis. The 31 articles which I retrieved in the initial snapshot (1 January–1 May 2014) variously reported on the outbreak, its death toll, and the transmission to bordering countries.
After recovering the initial framing of the crisis, I analysed the subsequent snapshot, which spanned from 1 May to 15 June 2014. The UK coverage in this period was extremely sparse, and one can hardly speak of a dominant framing, given that only five articles mentioned Ebola and the epidemic/pandemic. This is strangely at odds with the progression of infection and the increasingly wide reach of the epidemic across countries. However, it reinforces a point often made, that not all pandemics are ‘equal’ in the attention that they receive by the media in the West. The latter is a corollary of the bigger point – deaths are also not considered equal, and the attention they receive depends on where they occur (Abraham, 2007). Diseases that threaten (to spread to) the West receive greater attention, which often also matches the more substantial investments which countries in the Global North are prepared to make to respond to these threats.
Nonetheless, the dearth of coverage in this period is also at odds with the UK Government’s actions over the same time frame. The Government was following closely the outbreak at the time, beginning to invest in tackling it in June and July, including by planning a military operation to deliver aid in Sierra Leone (House of Commons, 2016b).
Not only is the coverage almost negligible, it is also departing from the previously dominant (localised) health crisis frame. Of the three articles which appeared on The Telegraph, two were in the market news section, reporting on UK mining interests in the area, namely the effects of unfolding events on share prices, and the evacuation of UK miners from affected areas. The third relayed the inflammatory comments made by right-wing French politician Le Pen, who suggested Ebola might help solve overpopulation issues in Africa and alleviating Europe’s migration problems. A fourth article appeared in The Guardian, reporting the health messages circulated locally by way of song to communicate basic protection measures. It thus related more closely to the health emergency framing seen previously. The fifth article appeared in The Times and again reported the comments by Le Pen.
A regional crisis
Following the Ebola crisis chronology, the snapshot I analysed next spanned from 16 to 30 June 2014, a time when the Ebola infection was reaching horrific proportions and resulting in an unprecedented death toll. A total of 15 articles appeared in the UK national newspapers. The dominant framing in this coverage constructs the outbreak as the worst epidemic, and as an ‘out of control’ crisis, but still frames the threat as regional. The following excerpt, from a 23 June article in The Independent, exemplifies this dominant frame:
[…] the number of cases continues to mount in what is now the worst recorded outbreak of the deadly disease in history.
Health ministers from 11 African nations will meet in Ghana next week for an emergency summit on Ebola, which has killed hundreds in Guinea, Sierra Leone and Liberia and now threatens to spread across borders into neighbouring countries including Ivory Coast and Mali. While the threat to the wider world is considered to be low, health authorities are remaining vigilant. (Cooper, 2014, my emphasis)
This framing dominates national newspaper coverage throughout the summer, even in August, when the WHO officially declares the crisis to be a Public Health Emergency of International Concern, allowing the much delayed allocation of more substantive aid and expertise (House of Commons, 2016a).
A global security threat
In September 2014, the framing in the UK national coverage changes dramatically. The turning point is a speech delivered by US president Obama at the Atlanta headquarters of the Centers for Disease Control and Prevention, in which he reframes Ebola as a global security threat. In his speech, reported by Reuters on 16 September 2014 (Mason and Harding Giahyue, 2014), what had previously been seen as primarily a health emergency is now reconstructed as a security concern. The reframing extends the reach of the threat, as Ebola is now seen as a risk to the Global North too:
This is an epidemic that is not just a threat to regional security. It’s a potential threat to global security, if these countries break down, if their economies break down, if people panic. That has profound effects on all of us. (Mason and Harding Giahyue, 2014)
As Elbe (2010) notes, global health security has become an international policy imperative over the last couple of decades, a phenomena that only intensified after the 9/11 security attack. In the domain of pandemic preparedness, he argues that this results in a greater push towards establishing international mechanism for disease surveillance, as well as for sharing laboratory samples. Fidler (2004) too claims that the governance of diseases with pandemic potential has become globalised and that this considerably extends the influence of the international medical expert community. However, Elbe (2010; see also Scoones, 2010) warns that the prioritisation of health security, particularly in relation to pandemic risk (and bioterrorism), is spearheaded by the West and often read by other countries and by non-governmental organisations as pursuing primarily the interest of the Global North.
Not only do pandemics get prioritised over endemic diseases already prevalent in the Global South, but the very means used to pursue this type of global health security engender further tensions. Commercialisation of pharmaceuticals is an example of the tensions that arise. The WHO freely shares with the pharmaceutical industry the virus samples collected by countries like Thailand or Vietnam, enabling their proprietorial commercial exploitation by multinationals. These are often companies with headquarters in the Global North and targeting their products to the affluent Global North markets. No benefits, such as intellectual property or access to drug stockpiling, arise for the countries that collect and freely share the disease data with the WHO in the first place. Such countries are now beginning to withdraw from their WHO duties to report and share clinical and laboratory data (Davis, 2005; Elbe, 2010).
Another negative consequence of the securitisation of a pandemic health crisis is that it can lead to a militarisation and politicisation of the crisis (Elbe, 2010). The UK had responded to the WHO August declaration about the status of the Ebola emergency by increasing its commitment to intervene in the frontline in Sierra Leone. While the UK response (like that of the international community at large) was severely delayed (House of Commons, 2016a), it did engage approximately 1300 military personnel, along with 200 Department for International Development surge staff, 150 NHS volunteers, and over 100 specialists from Public Health England (2016a: 9).
It was one of the objectives of a later review to establish whether this military engagement had been wise, or whether it might have been more fruitful to engage further medical and NGO personnel instead (House of Commons, 2016b). The point remains contentious (House of Commons, 2015b: 15). An expert witness to the enquiry, Dr Johnson, director of the King’s Sierra Leone Partnership, expressed concerns about the efficacy of the large military contingent deployed:
[b]ecause of a large military presence there, potentially it over-militarised some of the responses, because the assets available were almost entirely military ones that were not necessarily specialists in public health or epidemiology. (House of Commons, 2015b: 13)
Appraising the British response more generally, Dr Johnson judged it to have been ‘a bit deaf and blind as a result of its lack of public health specialists at senior level that could help interpret what was going on’ (House of Commons, 2015b: 13).
In parallel with these obvious policy implications linked to the Ebola crisis being conceived as a global security concern, the latter framing successfully permeates the media coverage from 16 September onwards (as well as the policy debate) and catalyses a further transformation in the way the crisis is understood, giving rise to specific understandings of how it needs to be tackled.
Outbreak
While the risk of contracting Ebola in the UK remained at the time incredibly low, the reframing of the crisis as a security threat activated in the media a related framing of pandemic disease that has characterised the coverage of previous pandemics too, including SARS and various Avian Flu scares. The frame is known as an outbreak narrative. It constructs the pandemic crisis by seeing it as originating on the ‘outside’, that is, outside the borders of the West. This framing is consistent (i.e. does not disrupt or require a re-framing of issues) with the previous UK media framing of the Ebola crisis as a localised African crisis, which characterised the newspaper coverage of Ebola from inception of UK reporting till the speech by Obama in September 2014. Dry and Leach (2010: 14) in their analysis of the policy framings prevalent in avian pandemic emergencies argue that the outbreak narrative is triggered by a dominant framing of pandemic risk that identifies the system and goals to be global – that is, affecting the global population and seeking to protect/reduce its mortality. In the case of the recent Ebola crisis, as seen via the lenses of its UK coverage, this shift towards a global construction of the risk posed by Ebola occurs on the occasion of the speech made by Obama. Dry and Leach (2010) also note that the outbreak narrative is invariably accompanied by a construction of the disease as dynamic, fast emerging, and rapidly spreading. Unsurprisingly, they conclude that this construction leaves only a limited set of responses open – namely, targeting of at-source control and eradication of the disease, as opposed to envisaging it as an endemic disease likely to re-occur periodically and therefore requiring a rather different set of responses and management strategies.
However, the outbreak framing produces other consequences too, I argue, by focusing attention so intensely, even obsessively, on the issue of contagion. It results in privileging as the only viable and reasonable solutions those strategies that are heavily focused on geographical containment, reinforcing an unhelpful fortress mentality. It helps trigger, I suggest below, a fortressing of borders via entry screening for instance, even if this measure is acknowledged by the WHO (2014a, 2014b) to be unnecessary and unhelpful.
Frenzy and panic over contagion
The UK media coverage post 16 September 2014 is centrally concerned with stories of frenzy and panic over contagion in the West. It is also exponentially increasing in volume. In the month between 16 September and 16 October, 824 articles on the Ebola pandemic/epidemic appear in the UK national papers, whereas in the month preceding 16 September (but following the WHO’s declaration that Ebola was now an emergency of international concern) there were 225 articles on the topic. Initially, this coverage focuses on a series of incidents that take place in the US, following reports of the death of the first patient diagnosed with Ebola on US soil. This type of coverage intensifies after the first case of infection occurs in the US – the nurse who delivered medical care to the Ebola patient becomes infected. Infection of a second nurse from the same team is reported shortly afterwards. The US incidents are emblematic of the climate of fear that was spreading and that was being amplified through media coverage too. The UK coverage includes accounts of US children being pulled out of their schools (The Mail, 2014) in Texas for fear of contagion. Other US stories appearing in the UK coverage report the cording off of the hospital in which the first US patient had been treated. They also describe how the second nurse was cleared to travel by plane (within the US) in the days that followed her tendering of the Ebola patient who died, amplifying concerns that the disease could imminently spread in the US via transport networks. Despite official reassurances that the risk to the UK remained low (and reports of similar reassurances by the US Government about the US), following the first case of contagion occurring within the EU, panic over contagion continued to dominate the way in which the Ebola crisis was framed in the UK newspapers. On 7 October, the UK newspapers announced that a health worker in Spain had been infected with Ebola after treating a sick missionary repatriated from an Ebola-affected area. Much of the initial framing of these events centred on the supposedly shambolic and inadequate safety protocols adopted by the Spanish medical institution in which infection occurred, therefore reinforcing a narrative of fortressing and containment of the disease outside the UK borders. The media framing suggested that standards and protocols in Spain were inadequate:
it emerged that a catalogue of errors led to [the nurse] not being isolated in a specialised unit until six days after she showed signs of the illness and after she had sought medical advice three times.
[…] she may have touched her face while removing the protective suit, an error that she was not aware of at the time.
[…] She was then transported in an ambulance by paramedics not dressed in protective clothing to the emergency department of the Alcorcón hospital […] after reportedly waiting some time in a busy waiting room […] the patient was left in an improvised isolation area. (The Telegraph, 8 October 2014)
The message implicitly conveyed was that in Britain standards were more advanced and guidelines scrupulously followed, and that therefore the same failures would never have occurred, a message also reinforced through the reporting on 11 October 2014 that a UK-based exercise had been conducted to test the preparedness of UK health services and simulate other contingency arrangements, including a meeting of the COBRA emergency committee. The coverage contains details of other arrangements that ostensibly are being reported to reassure the public, for instance about the four hospital facilities ready to tackle a potential infection on UK soil, should the numbers of infected patients become high (The Mirror, 2014). Some of this coverage (and especially its headlines6), however, exacerbate the framing of frenzy and panic. The same Mirror article that reports the hospital preparedness plans runs with the following headline:
Four NHS hospitals on standby for mass UK outbreak of killer disease: In addition to London’s Royal Free Hospital, units in Liverpool, Sheffield and Newcastle will provide ‘surge capacity’ in the event of a mass outbreak. (8 October 2014)
Panic and frenzy about impending UK contagion continue to frame stories in the media. The coverage begins to undermine the Government’s reassurances about UK preparedness and to question the soundness of the medical protocols in place, even as it continues to report these official messages. A series of suspected Ebola cases, poorly handled by UK hospitals, result in panic in wards and among medical staff. While the patients were ultimately found not to have been infected with Ebola, the incidents raised doubts about the level of UK readiness in dealing with contagion on UK soil:
[headline:]Ebola UK: NHS staff ‘panicked’ after suspected Ebola cases
NHS wards were left reeling after two suspected cases of Ebola walked into unprepared A&E departments over the weekend. Staff at London’s University Hospital Lewisham are said to have panicked […]
Meanwhile, an Ebola scare shut down Coventry’s main walk-in centre on Saturday […]
An unnamed source […] described the reaction on Saturday night as ‘farcical’ and alleged the London hospital was ill-prepared to deal with Ebola cases. (The Independent, 13 October 2014)
Despite previous official reassurances that no border screening was going to be put in place and that screening would not have been effective (a message diffused also by the WHO, alongside Public Health England and the UK Government), on 10 October it was suddenly announced that UK border screening would start on 14 October. It would be carried out at key UK ports of entry. Posters, like that which appeared at Manchester Airport (below), advised passengers on the procedure to follow, if they started displaying Ebola-like symptoms after having travelled from one of the affected areas (Figure 3).
Figure 3.

Poster displayed at UK ports of entry (Public Health England, 2014a).
Much more stringent and effective exit screening was in place at all ports of exit from Ebola-affected countries (EU/WHO, 2014). Entry screening, however, is much less effective, with a number of studies casting doubt on such measures as self-completion health questionnaires, alongside temperature scanning and testing itself (Priest et al., 2013). The efficacy of entry screening technologies, such as thermal scanners, has been questioned by empirical studies and by expert enquiries (Cowling et al., 2010; House of Commons, 2016b). At the UK Parliamentary Committee hearing set up to review lessons learnt from the 2014–2015 Ebola outbreak, Professor Griffin, former Chair of the Advisory Committee on Dangerous Pathogens, discussed the measures introduced in UK airports and ports of entry in 2014. He stated that ‘there was little clinical evidence that the screening involved, in terms of body temperature, would be either sensitive or helpful’, concluding that medically it was ‘an incredibly blunt and insensitive tool’ (House of Commons, 2016b: 27). His expert opinion was supported by that of Dr Jeremy Farrar, Director of the Wellcome Trust, who also testified in front of the same Committee that he did not think screening ‘was epidemiologically and scientifically justified’ (House of Commons, 2016b: 27), adding that
I also accept that policies need to take evidence into account but sometimes have to do things where there are other pressures […] (House of Commons, 2015a: 40)
When pressed on his view as to why the Government had reversed policy and imposed the screening, he stated:
I am not a politician, but sometimes there is a need for politicians to act and be seen to be acting. It was a public statement of how concerned the country was about the outbreak. I do not think that it was epidemiologically and scientifically justified. (House of Commons, 2015a: 40)
The House of Commons (2016b) report concludes that ‘many of [the] witnesses believed that the scientific evidence and rationale for introducing screening was missing’ (p. 27). These expert statements and the recommendation of the WHO (2014a, 2014b) highlight that the reason behind its introduction was not its efficacy in achieving containment. Entry screening was introduced merely as a way of being seen to actively respond to growing public anxieties about the risk of contagion in the UK. As shown, such public fears were heavily circulated, even amplified, in the media.
The screening measure, thus, needs to be understood chiefly as a public relation (PR) exercise, rather than as a realistic attempt to contain the spread of Ebola – let alone an effective strategy to respond to the crisis more widely. Two months later, in December 2014, the screening at Heathrow airport proved ineffective in stopping a UK nurse infected with Ebola on her return from Sierra Leone, the first case of undetected Ebola to reach UK soil. The details of her story and court cases7 emerged only later on, after the Ebola crisis had come to an end. It is beyond the scope of this article to consider the delayed coverage of her case, as the focus of this article is the relationship between the dominant media framing of the threat as circulated in the national UK coverage and the measures implemented in the UK to respond to that threat while the crisis was ongoing.8 The screening proved ineffective because the nurse had lowered her body temperature by taking paracetamol beforehand, as well as through a series of mistakes in recording her temperature made by those tasked with carrying out the screening. It later emerged from an inquest that some passengers were left to take and/or record their own body temperature and that in other cases temperatures were recorded incorrectly by screening personnel.
The UK media coverage has arguably played a key role in suggesting impending danger, by mobilising and amplifying fear, for instance by suggesting that other national containment measures (such as hospitalisation to isolate infected patients) were insufficient and that contagion was going to reach and spread in the UK imminently. Ironically, the UK national newspapers also remained critical of the new border screening measure. This is in no small part due to the fact that the screening remained largely voluntary (in various cases passengers would have had to self-identify as coming from an Ebola-affected area), and to the very public U-turn made by the Government in openly rejecting the need for screening first, only to then suddenly sanction its introduction as necessary.
The House of Commons report on the lessons learnt from Ebola reflects also on the Government’s communication during the Ebola crisis judging it to be generally good, balanced and accurate, both in relation to the health messages and the (low) risk posed by the possibility of infection in the UK (House of Commons, 2016b). However, in its final recommendations the report also registers that
It is disappointing, however, that [the Government] failed to explain clearly its rationale for going against guidance from both the World Health Organisation and Public Health England by introducing entry screening for Ebola at UK ports. […] We recommend that the evidential basis for – and the purpose of – the intervention is made explicit […] especially if it goes against established guidance from trusted advisory bodies. (House of Commons, 2016b: 38)
Unfortunately, The Government’s response to the report did not address the issue (UK Department of Health, 2016).
Among the evidence submitted to the House of Commons, the Science Media Centre (2015) also lamented that, in the pursuit of a single unified public health message, the Government was nervous about independent expert voices commenting on events, and excluded such experts from its media briefing, effectively leaving them entirely out of the loop on the development of events and response strategies. The same body also recommended that the Government took a different approach to uncertainty in the future, acknowledging openly the areas where uncertainty exists (including any uncertainty around best mitigation strategy to implement in the UK), rather than denying uncertainty and refusing to answer the questions posed by media and independent experts alike (Science Media Centre, 2015).
Conclusion
Global pandemics pose new and difficult challenges and are increasingly seen as among the most serious threats that contemporary Western societies may have to face. They are predicted to be both impending and unavoidable. The threat of pandemics periodically generates intense media coverage. Despite the growing role played by social media, including its potential to improve situation awareness, newspaper media coverage (in print or online) remains central to the framing of public and policy debates on national security and pandemics in the West.
As argued through the mapping of the Ebola crisis and its framing in the newspaper coverage in the UK, not all pandemics are equal, nor are all resulting deaths treated in the same way (Abraham, 2007). The Ebola coverage in the UK was sparse at best, particularly in the first 6 months of reporting. It is striking to compare it to the frantic media attention and volume of coverage generated by SARS (Abraham, 2007) and also by other pandemic flu scares (Scoones, 2010). This is despite the fact that the Ebola pandemic resulted in over 11,000 deaths by December 2015 and about 28,500 confirmed cases of infection (WHO, 2015). By contrast, SARS produced around 774 fatalities and resulted in approximately 8000 cases of infection.
Through the case study of Ebola and the UK national newspaper coverage, I have argued that Western media framing of risk of contagion is key to the manner in which a crisis can be perceived as a major pandemic or a localised (and remote) epidemic, and discussed the consequences of these different framings, both in terms of understanding of the phenomenon, but also in the material implications for the kinds of interventions deployed and believed to be most appropriate.
Commentators have found that some pandemics are discussed through a war framing (see Abraham, 2007 for SARS and Scoones and Forster 2010 for avian flu), whereby the medics engaged in responding to the crisis are viewed as an army, and the drugs deployed constructed as weapons. There was not any evidence of the same occurring in the case of the recent Ebola crisis. However, its re-framing, from a (localised) health and humanitarian emergency to a global security concern, transformed the way in which the crisis was configured and responded to.
The article discussed the draconian measures put in place and the militarisation of the crisis. It problematised a recurrent and Western centric framing of pandemic risk along the lines of an outbreak narrative, arguing that this shift produced a strong and misguided focus on obsessive fear of contagion spreading to the West (the US, Europe, and the UK) and an unhelpful focus on ineffective border control containment strategies.
The security framing also gave way in the media to panic narratives, and this resulted in a concern with finding someone to blame (e.g. Spanish hospitals with poor containment standards, various UK hospitals with the same issues, the nurses who treated patients returning to the West with the infection). What is more, this framing of events also may have motivated, I have suggested, the implementation of ineffective measures at UK airports and ports of entry, focusing on entry screening, which was scientifically unfounded and deployed merely as a PR exercise and against expert advice.
There are many lessons that can be drawn from the case study of Ebola. First, the role of (traditional) media coverage continues to matter and needs to be scrutinised more closely, given that the emergence and reproduction of certain topoi is likely to directly affect the understanding of the risk at hand, both in public debates and in policy ones. It is also likely to contribute to the identification of best responses and the setting of priorities about how to respond nationally and internationally (and to which degree of involvement) to a pandemic emergency. Moreover, while some framings are more stable or recurrent than others (e.g. the outbreak narrative), others vary from pandemic to pandemic or shift even throughout the course of the same crisis. These dominant media framings are also likely to leave certain legacies or dependency paths that affect the preparedness planning that precedes a future pandemic event, making their timely and close investigation even more pressing.
Acknowledgments
I wish to thank the anonymous reviewers for their comments and constructive criticism and the editors. I also wish to thank Professor Alan Warde for his comments on an earlier version of this paper.
Author biography
Elisa Pieri is a sociologist at the University of Manchester. Her current research investigates how cities in the West securitise against the risk of global pandemics (Simon Fellowship, 2016–2019). Her interdisciplinary research explores the process of securitisation, governance under conditions of uncertainty and the biopolitical ramifications of security. Her previous work investigated the governance of emergent technologies and their social, ethical, policy and practice implications. She also researched policy controversies, and public and media debates. Her funded research projects have investigated a range of topics, including GM food and crops, medical and behavioural genomics, biometrics, urban securitisation and the built environment.
http://www.who.int/ihr/alert_and_response/outbreak-network/en/ (accessed 24 April 2018).
Analyses of social media also begin to yield interesting insights into ideology and narrative formation, as showcased by Sastry and Lovari (2017).
http://www.lexisnexis.co.uk/en-uk/home.page (accessed 24 April 2018).
Looking at his time frame involved retrieving over 1000 articles – of various lengths, from short, one paragraph news articles to full editorials – via LexisNexis.
A lexical item is a basic unit of language, one of the basic elements of a language’s lexicon. It can be a word but also a part of a word, it can be a verb, noun, adjective, or a particle. Here, I am using it interchangeably with the lay term ‘word’ for simplicity’s sake, but the two terms are not synonymous in linguistics.
The media also respond to their inherent logics of newsworthiness, and headlines in alarmist tones attract readers’ attention.
It later became apparent that the nurse was being accused of hiding her body temperature and possible Ebola infection before and through the entry screening, potentially allowing the disease to spread in the UK. The nurse admitted herself to a hospital in Glasgow.
The (delayed) media framing of the incident displayed the tendency towards scapegoating the nurse. This is consistent with an outbreak narrative (Dry and Leach, 2010), in which certain risky individuals, including super-spreaders and socially marginalised groups, come to be stigmatised and blamed for the spread of the pandemic.
Funding: This research was supported by a Simon Fellowship award (2016–2019), held at the University of Manchester, UK.
ORCID iD: Elisa Pieri  https://orcid.org/0000-0001-5477-5539
https://orcid.org/0000-0001-5477-5539
References
- Abraham T. (2007) Twenty-First Century Plague: The Story of SARS. Baltimore, MD: John Hopkins University Press. [Google Scholar]
- Cooper C. (2014) Ebola epidemic is a threat to global health. Independent, 28 June, pp. 13. [Google Scholar]
- Cowling B, Lau L, Wu P, et al. (2010) Entry screening to delay local transmission of 2009 pandemic influenza A (H1N1). BMC Infectious Diseases 10(82). Available at: https://bmcinfectdis.biomedcentral.com/track/pdf/10.1186/1471-2334-10-82 (accessed 7 November 2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis M. (2005) The Monster at Our Door: The Global Threat of Avian Flu. New York: The New Press. [Google Scholar]
- Dry S. (2010) New rules for health? Epidemics and the International Health Regulations. In: Dry S, Leach M. (eds) Epidemics: Science, Governance and Social Justice. London: Earthscan, pp. 23–42. [Google Scholar]
- Dry S, Leach M. (eds) (2010) Epidemics: Science, Governance and Social Justice. London: Earthscan. [Google Scholar]
- Elbe S. (2010) Security and Global Health. Cambridge: Polity Press. [Google Scholar]
- Entman R. (1993) Framing: Toward clarification of a fractured paradigm. Journal of Communication 43(4): 51–58. [Google Scholar]
- Entman R. (2007) Framing bias: Media in the distribution of power. Journal of Communication 57: 163–173. [Google Scholar]
- EU/WHO (2014) EU/WHO mission to review the exit screening measures at international airports in Conarky, Freetown and Monrovia. Summary technical report, EU and WHO, Brussels and Geneva, 15 December. [Google Scholar]
- Fidler D. (2004) SARS, Governance and the Globalization of Disease. New York: Palgrave Macmillan. [Google Scholar]
- Halfpenny P, Lin Y, Pieri E. (2009) Using text mining for frame analysis of media content. JISC E-Infrastructure Programme, JISC Final Report, NCESS, Manchester, August. [Google Scholar]
- HM Government (2010) A Strong Britain in an Age of Uncertainty: The National Security Strategy. London: The Stationary Office. [Google Scholar]
- House of Commons (2015. a). Science and Technology Committee. Oral Evidence: Science in Emergencies: UK Lessons from Ebola, HC 469. 20 October 2015. Available on http://www.parliament.uk/business/committees/committees-a-z/commons-select/science-and-technology-committee/inquiries/parliament-2015/science-in-emergencies/publications/ (accessed 12 October 2016).
- House of Commons (2015. b). Science and Technology Committee. Oral Evidence: Science in Emergencies: UK Lessons from Ebola, HC 469. 24 November 2015. Available on http://data.parliament.uk/writtenevidence/committeeevidence.svc/evidencedocument/science-and-technology-committee/science-in-emergencies/oral/25242.html (accessed 4 October 2016).
- House of Commons (2016. a) Ebola: Responses to a public health emergency. International Development Committee, Second Report of Session 2015-16, January 2016. London: The Stationary Office. [Google Scholar]
- House of Commons (2016. b) Science in emergencies: UK lessons from Ebola. Science and Technology Committee. Second Report of Session 2015-16. London: The Stationary Office. [Google Scholar]
- Kitzinger J. (2007) Framing and frame analysis. In: Devereux E. (ed.) Media Studies: Key Issues and Debates. London: SAGE, pp. 134–161. [Google Scholar]
- McInnes C, Kamradt-Scott A, Lee K, et al. (2014) The Transformation of Global Health Governance. Basingstoke: Palgrave Macmillan. [Google Scholar]
- Mason J. (2006) Mixing methods in a qualitatively driven way. Qualitative Research 6(1): 9–25. [Google Scholar]
- Mason J, Harding Giahyue J. (2014) Citing security threat, Obama expands U.S. role fighting Ebola. Reuters, 16 September. Available at: https://www.reuters.com/article/us-health-ebola-obama/citing-security-threat-obama-expands-u-s-role-fighting-ebola-idUSKBN0HB08S20140916
- Pieri E. (2009) ID cards: A snapshot of the debate in the UK Press. Project report, NCeSS, Manchester, April. Available at: https://danishbiometrics.files.wordpress.com/2009/08/pieri_idcards_full_report.pdf (accessed 28 June 2018).
- Priest P, Jennings L, Duncan A, et al. (2013) Effectiveness of border screening for detecting influenza in arriving airline travelers. American Journal of Public Health 103(8): 1412–1415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Public Health England (2014. a) Ebola: Returning from West Africa A3 Poster. London: The Crown. [Google Scholar]
- Public Health England (2014. b) Global Health Strategy: 2014-2019. London: The Crown. [Google Scholar]
- Sastry S, Lovari A. (2017) Communicating the ontological narrative of Ebola: An emerging disease in the time of ‘Epidemic 2.0’. Health Communication 32(3): 329–338. [DOI] [PubMed] [Google Scholar]
- Schulz A, Thanh T, Paulheim H, et al. (2013) A fine-grained sentiment analysis approach for detecting crisis related microposts. In: Proceedings of the10th international ISCRAM conference 2013 (ed Comes T, Fiedrich F, Fortier S, et al.), Baden, 12–15 May. [Google Scholar]
- Science Media Centre (2015) Written evidence submitted by the science media centre (EME0009). Evidence submitted to the House of Commons Select Committee on Science in Emergencies: UK Lessons from Ebola Inquiry, September. Available at: http://data.parliament.uk/writtenevidence/committeeevidence.svc/evidencedocument/science-and-technology-committee/science-in-emergencies/written/21019.html (accessed 6 November 2018).
- Scoones I. (ed.) (2010) Avian Influenza: Science, Policy and Politics. London: Earthscan. [Google Scholar]
- Scoones I, Foster P. (2010) Unpacking the international response to avian influenza: actors, networks and narratives. In: Scoones I. (ed) Avian Influenza: Science, Policy and Politics. London: Earthscan, pp. 19–64. [Google Scholar]
- Sipress A. (2009) The Fatal Strain: On the Trail of Avian Flu and the Coming Pandemic. New York: Penguin. [Google Scholar]
- Stephenson N, Jamieson M. (2009) Securitising health: Australian newspaper coverage of pandemic influenza. Sociology of Health and Illness 4: 525–539. [DOI] [PubMed] [Google Scholar]
- The Independent (2014) Ebola UK: NHS staff ‘panicked’ after suspected Ebola cases. The Independent, 13 October. Available at: https://www.independent.co.uk/life-style/health-and-families/health-news/ebola-uk-nhs-staff-panicked-after-suspected-ebola-cases-9791492.html
- The Mail (2014) One hundred exposed to Ebola in Texas as panicked parents pull children from local schools and neighbor describes how infected man was ‘throwing up all over the place’. The Mail, 2 October. Available at: https://catholic4lifeblog.wordpress.com/2014/10/02/one-hundred-exposed-to-ebola-in-texas-as-panicked-parents-pull-children-from-local-schools/
- The Mirror (2014) Four NHS hospitals on standby for mass UK outbreak of killer disease: In addition to London’s Royal Free Hospital, units in Liverpool, Sheffield and Newcastle will provide ‘surge capacity’ in the event of a mass outbreak. The Mirror, 8 October. Available at: https://www.mirror.co.uk/news/uk-news/ebola-crisis-four-nhs-hospitals-4399174
- The Telegraph (2014) Spanish nurse with Ebola ‘says her fever was ignored for six days’: Spanish nurse with Ebola ‘was fobbed off with paracetamol’ as it emerges she likely caught the virus when she touched her face with a contaminated glove. The Telegraph, 8 October 2014. Available at: https://www.telegraph.co.uk/news/worldnews/ebola/11150114/Spanish-nurse-with-Ebola-says-her-fever-was-ignored-for-six-days.html
- UK Department of Health (2016) Government Response to the House of Commons Science and Technology Committee 2nd Report of Session 2015-16: Science in Emergencies: UK Lessons from Ebola. London: The Crown. [Google Scholar]
- Wald P. (2008) Contagious: Cultures, Carriers, and the Outbreak Narrative. Durham, NC: Duke University Press. [Google Scholar]
- World Health Organisation (WHO) (2005) International Health Regulations. Geneva: WHO. [Google Scholar]
- World Health Organisation (WHO) (2014. a) Statement on travel and transport in relation to Ebola virus disease outbreak. WHO, Geneva, 18 August. [Google Scholar]
- World Health Organisation (WHO) (2014. b) Technical Note for Ebola Virus Disease Preparedness Planning for Entry Screening at Airports, Ports and Land Crossings. Geneva: WHO. [Google Scholar]
- World Health Organisation (WHO) (2015) Ebola situation reports. WHO, Geneva, December. [Google Scholar]
- Yang C, Yang J, Luo X, et al. (2009) Use of mobile phones in an emergency reporting system for infectious disease surveillance after the Sichuan earthquake in China. Bulletin of the World Health Organization 87: 619–623. [DOI] [PMC free article] [PubMed] [Google Scholar]