

Abstract
PURPOSE:
The effectiveness of immune checkpoint inhibitors (ICIs) is limited in pancreatic ductal adenocarcinoma (PDAC). We conducted a phase I study to evaluate the safety of ICI with stereotactic body radiation therapy (SBRT) in patients with metastatic PDAC.
PATIENTS AND METHODS:
Patients enrolled must have received at least one line of prior systemic chemotherapy for metastatic disease. Cohort A1 and A2 received durvalumab every 2 weeks plus either 8Gy in one fraction of SBRT on day 1 or 25Gy in 5 fractions on day −3 to +1. Cohort B1 and B2 received durvalumab plus tremelimumab every 4 weeks and either 8Gy in one fraction of SBRT on day 1 or 25Gy in 5 fractions on day −3 to +1. ICIs were continued until unacceptable toxicity or disease progression. The primary objective was the safety and feasibility of treatment. Objective response was assessed in lesions not subjected to SBRT.
RESULTS:
Fifty-nine patients were enrolled and 39 were evaluable for efficacy. No dose limiting toxicities were seen. The most common adverse event was lymphopenia. Two patients achieved a partial response (one confirmed and the other unconfirmed). The overall response rate was 5.1%. Median PFS and OS was 1.7 months (95% CI 0.8–2.0 months) and 3.3 months (95% CI 1.2–6.6 months) in cohort A1; 2.5 months (95% CI 0.1–3.7 months) and 9.0 months (95% CI 0.5–18.4 months) in A2; 0.9 months (95% CI 0.7–2.1 months) and 2.1 months (95% CI 1.1–4.3 months) in B1; and 2.3 months (95% CI 1.9–3.4 months) and 4.2 months (95% CI 2.9–9.3 months) in B2.
CONCLUSION:
The combination of ICI and SBRT has an acceptable safety profile and demonstrates a modest treatment benefit in patients with metastatic PDAC.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) affects over 55,000 people in the United States each year and is projected to become the second leading cause of cancer related deaths by 2030[1]. The 5-year survival rate remains at 7%, which is the lowest amongst other cancers[1, 2]. The management of PDAC has traditionally focused on systemic treatment with few effective chemotherapies[3–5] as a minority of patients present with potentially resectable disease. In the first line setting for advanced disease, FOLFIRINOX improved the median overall survival (OS) to 11.1 months compared to 6.8 months with gemcitabine monotherapy[6]. Gemcitabine and nab-paclitaxel resulted in a median OS of 8.5 months compared to 6.7 months with gemcitabine alone [7].
Immune checkpoint inhibitors (ICIs) have shown clinical benefit and are FDA approved in multiple tumor types [8–13]. However, they have demonstrated limited response in PDAC patients treated with monotherapy[9, 14, 15] with the exception of patients with mismatch repair deficiency who achieved an objective response rate of 62%[16]. Combination checkpoint blockade was shown to have modest activity in in a phase II trial where 65 patients with refractory metastatic PDAC received either durvalumab (a PD-L1 inhibitor) alone or durvalumab with tremilimumab (a CTLA-4 inhibitor), resulting in a median OS of 3.6 months versus 3.1 months, respectively. In addition, there was one confirmed partial response in the combination arm[17].
Radiation is used in the management of all stages of pancreatic cancer. Several studies have documented an increase in peripheral antitumor immunity following radiation [18–20]. The underlying mechanism is not completely understood but appears to be associated with radiation-induced cell death that results in the exposure of tumor antigens, subsequently increasing the pool of intracellular peptides for cross-presentation[21] and encouraging radiation-killed cells to function as a vaccine in situ[22]. In addition, radiation is able to reprogram and remodel the tumor stromal microenviroment that is against the immune evasion mechanisms of cancer[23]. Therefore, it is suggested that combined radiation with immune checkpoint blockade offers better local tumor regression and systemic control[24]. However, emerging data that suggests that dose escalation enhances tumor response and outcomes when radiation is used in a definitive or adjuvant manner for locally advanced disease, but there is a lack of clinical data to inform dose selection in the setting of treating metastatic pancreatic cancer with checkpoint blockade or other forms of immunotherapy. The current trial assessed the safety and efficacy of combining checkpoint blockade (durvalumab +/− tremilimumab) and two common dose schedules for treating tumors with stereotactic body radiation therapy (SBRT) in patients with metastatic pancreatic cancer as second line therapy.
Methods
Patient Population
Eligible patients (18 years or older) with pathologically confirmed PDAC as defined by the Laboratory of Pathology at the National Cancer Institute (NCI) were enrolled in this single center study. Patients must have had disease that was not amenable to potentially curative resection. Primary in-situ (or locally-recurrent) tumor must have been present and, in the opinion of radiation oncology, be amenable to radiation therapy as planned in the protocol. Each case was discussed at the institution’s tumor board with a multidisciplinary team. All patients were evaluated by a radiation oncologist to determine eligibility for the protocol-mandated SBRT. Patients must have had at least 1 measurable metastatic lesion by RECIST v1.1 criteria that was followed during treatment but was not radiated. Patients must have received at least one line of prior systemic chemotherapy for metastatic disease. Additional eligibility criteria included: Eastern Cooperative Oncology Group (ECOG) performance status score 0–1; adequate organ and marrow function and no history of chronic or active autoimmune disease or inflammatory bowel disease. This trail was conducted in accordance with the Declaration of Helsinki after approval by the NCI Institutional Review Board. All patients provided written informed consent. The ClinicalTrials.gov identifier was: NCT02311361. Patients who met the eligibility criteria were enrolled onto the study.
Study Design
This was a pilot phase 1, two-cohort, four-arm, open-label clinical trial with a two arm extension cohort conducted at the NCI between March 2015 to August 2019. The trial consisted of two cohorts, denoted as cohort A and B. Patients in cohort A received durvalumab 10 mg/kg every 2 weeks which was continued for a total of 12 months or until progressive disease (PD) was confirmed by immune-related response criteria. Patients in cohort B received durvalumab 1500 mg and tremelimumab 75 mg every 4 weeks for 4 doses, followed by 1500 mg durvalumab monthly for up to 8 months (9 doses total). Each cohort included 2 separate radiation dose levels (DLs) which differed by the quantity of radiation: DL1 (denoted A1 and B1 for each cohort) comprised of 8Gy in 1 fraction (Total = 8 Gy, 8Gy × 1) at Day 1; DL2 (denoted A2 and B2 for each cohort) comprised of 25Gy in 5 fractions over 5 days (5Gy × 5, Day −3 to Day +1). The cohorts were enrolled sequentially, for example, patients in cohort A finished before the first patient in cohort B was enrolled. Imaging studies were performed by contrast-enhanced CT scans every 8 weeks. Mandatory baseline and Day 29 tumor biopsies were obtained in all patients based on the evaluation of risk at the multidisciplinary GI tumor board. Each arm was originally intended to be evaluated in a pilot fashion, focusing on safety and preliminary efficacy, with a goal of 10 evaluable patients per arm. Arm B2 was expanded to allow up to 20 evaluable patients, and the other arms were allowed to accrue additional patients in case inevaluable patients were identified.
SBRT
Patients were simulated supine with the addition of a 4D CT if appropriate. In some cases, a stereotactic immobilization device with oral contrast was used, and/or oral and IV contrast was delivered for the simulation if deemed necessary by the treating radiation oncologist. Target lesions for radiation were primary or recurrent pancreatic lesions. If there was no pancreatic lesion present or in the opinion of the radiation oncologist, there was a more amenable lesion outside of the pancreas, this was designated as the target lesion. Treatment was delivered at the discretion of the radiation oncologist. Localization was verified with pretreatment imaging prior to every fraction. The gross tumor volume (GTV) was defined based on imaging in a treatment planning CT scan and optionally based on the treatment planning 4D CT, with which an additional margin of up to 3 mm that was added as needed to accommodate respiratory motion of the target within an interval target volume (ITV). A 2–5 mm expansion of the GTV was used to generate the planning target volume (PTV). Conformal radiation doses were delivered with megavoltage external beam radiation with beam energies of 6MV or higher. For Cohorts A1 and B1 treatment was delivered in 8Gy as a single fraction. For Cohorts A2 and B2 treatment was delivered in 25Gy in 5 fractions. Selection of the radiation schedule to be employed was based on technical and clinical factors and after discussion with and at the discretion of the radiation oncologist.
Safety
All adverse events (AEs), including clinically significant abnormal findings on laboratory evaluations, regardless of severity, were followed until satisfactory resolution. All safety events were reported according to the NCI Common Terminology Criteria for Adverse Events v4.0. The safety population was defined as all patients who received at least one dose of ICI or SBRT. Given that the primary aim of the study was to assess safety of ICI in combination with SBRT, the evaluation period of DLTs was extended for 6 weeks following completion of radiation.
Assessments of Efficacy and Statistical Analysis of Clinical Results
The primary objective was to determine the safety and tolerability of the combination of ICI with SBRT in patients with metastatic PDAC. Secondary objectives were overall response rate (ORR), progression free survival (PFS) and overall survival (OS). Objective response was assessed by Response Evaluation Criteria in Solid Tumors (RECIST, version 1.1) in lesions not subjected to SBRT. Only those patients who had measurable disease present at baseline, had received at least one cycle of therapy and had their disease re-evaluated were considered evaluable for response using RECIST v1.1. PFS and OS were calculated by the Kaplan-Meier method and reported along with 95% confidence intervals (CI). The significance of the difference between two Kaplan-Meier curves was determined by a log-rank test. PFS was defined as the time from the first treatment included in the protocol until the first documented progression of disease or death. OS was defined as the time between the initiation of protocol therapy and date of death or last follow-up. The definition of complete response (CR), partial response (PR), stable disease (SD) and PD was defined as reported previously [25]. Statistical analysis was performed using SAS Version 9.4 (SAS Institute, Cary NC).
Tumor Sample Analysis
Biopsied tumor tissue was processed for the analysis of immune cell infiltration. After fixation with formalin and embedded in paraffin, tumor slides were stained with hematoxylin and eosin, anti-CD3, anti-CD8 and anti-MHC-1. The stained slides were scanned (Hamamatsu Nano Zoomer XR) and analyzed with an automated image analysis software (QuPath 2.0). The percentage of total positive pixels (corresponding to 3, 3-diaminobenzidine chromogen saturation) in areas of tumor was analyzed between samples collected at pre- and post-treatment time points.
Statistical Analysis of Immune Correlative Data
Paired t tests were used to assess differences in cell frequencies between samples, and a Wilcoxon signed rank test was used when the paired difference was not normally distributed. Results are reported without adjustment for multiple testing. Statistical analysis was performed using Prism software (GraphPad).
Results
Patient Characteristics
Between March 2015 and January 2019, fifty-nine patients were enrolled and received treatment with durvalumab and SBRT 8 Gy in one fraction (Cohort A1; N=14), durvalumab and SBRT 25 Gy in 5 fractions (Cohort A2; N=10), durvalumab/tremelimumab and SBRT 8 Gy in one fraction (Cohort B1; N=19), and durvalumab/tremelimumab and SBRT 25 Gy in 5 fractions (Cohort B2; N=16). One patient withdrew before receiving any treatment in Cohort A2. The demographic and disease characteristics of the patients at baseline are shown in Table 1. The median age of the population was 61.0 years (range 43–85). All enrolled patients had good performance status with ECOG 0 (39%) or 1 (61%). Seventy-five percent of patients had received at least 2 prior lines of chemotherapy before enrolling onto this trial.
Table 1:
Baseline Characteristics
| Cohort A1 8Gy x1 +Durva (N=14) |
Cohort A2 5Gy x5 +Durva (N=10) |
Cohort C1 8Gy x1 +Durva/Treme (N=19) |
Cohort C2 5Gy × 5 +Durva/Trem (N=16) |
|
|---|---|---|---|---|
| Age | ||||
| Median | 62.0 | 61.5 | 60.0 | 60.5 |
| Range | 43–80 | 48–77 | 43–85 | 44–79 |
| Sex -- no. (%) | ||||
| Female | 7 (50) | 5 (50) | 9 (47) | 1 (6) |
| Male | 7 (50) | 5 (50) | 10 (53) | 15 (94) |
| Ethnicity -- no.(%) | ||||
| Asian | 1 (7) | 0 (0) | 0 (0) | 0 (0) |
| Black | 2 (14) | 0 (0) | 3 (16) | 4 (25) |
| White | 11 (79) | 10 (100) | 16 (84) | 12 (75) |
| ECOG -- no/ (%) | ||||
| 0 | 5 (36) | 2 (20) | 6 (32) | 10 (63) |
| 1 | 9 (64) | 8 (80) | 13 (68) | 6 (38) |
| Pancreatic tumor location at diagnosis -- no. (%) | ||||
| Head | 4 (29) | 3 (30) | 13 (68) | 9 (58) |
| Body | 6 (43) | 3 (30) | 2 (11) | 5 (31) |
| Tail | 4 (29) | 4(40) | 4 (21) | 1 (6) |
| Unknown | 0 (0) | 0(0) | 0 (0) | 1 (6) |
| Metastasis at diagnosis -- no. (%) | 12 (86) | 8 (80) | 12 (63) | 13 (81) |
| Previous therapy -- no. (%) | ||||
| Radiation therapy | 0 (0) | 0 (0) | 8 (42) | 1 (6) |
| Chemotherapy | 14 (100) | 10 (100) | 19 (100) | 16 (100) |
| Whipple procedure | 2 (14) | 2 (20) | 6 (32) | 3 (19) |
| Biliary stent | 0 (0) | 0 (0) | 1 (5) | 1 (6) |
| Previous chemotherapy -- no (%) | ||||
| 1 line | 4 (29) | 2 (20) | 3 (16) | 6 (38) |
| 2 lines | 4 (29) | 4 (40) | 6 (32) | 2 (13) |
| ≥3 lines | 6 (43) | 4 (40) | 10 (53) | 8 (50) |
| Site of disease at enrollment -- no. (%) | ||||
| Pancreas | 14 (86) | 8 (80) | 14 (58) | 13 (75) |
| Surgical bed | 2 (14) | 2 (20) | 3 (16) | 1 (6) |
| Liver | 9 (64) | 4 (40) | 7 (37) | 10 (63) |
| Lung | 3 (21) | 2 (20) | 3 (16) | 5 (31) |
| Peritoneum | 1 (7) | 1 (10) | 3 (16) | 2 (13) |
| No. of metastatic sites at enrollment -- no. (%) | ||||
| 1 | 6 (43) | 7 (70) | 9 (47) | 10 (63) |
| 2 | 5 (21) | 0 (0) | 2 (11) | 4 (25) |
| 3 | 1 (7) | 1 (10) | 2 (11) | 0 (0) |
| Level of CA 19-9 at enrollment-- no. (%) | ||||
| Normal (0–34.9 U/ml) | 0 (0) | 2 (20) | 2 (11) | 2 (13) |
| ULN to ≤59× ULN | 3 (21) | 5 (50) | 10 (53) | 5 (31) |
| >59× ULN | 11 (79) | 3 (30) | 7 (37) | 10 (63) |
| CA 19-9 (U/ml) at enrollment | ||||
| Median | 5067.5 | 853.1 | 1349.0 | 5880.5 |
| Range | 175.5–97560 | 29.3–57040 | 0.6–536100 | 2.3–49800 |
Abbreviation: Durva: Durvalumab; Treme: Tremelimumab; ECOG: Eastern Cooperative Oncology Group
Treatment
The median number of treatment cycles was 4 (range, 1 to 6) in cohort A1, 5 (range, 4 to 10) in cohort A2, 2 (range, 1 to 4) in cohort B1 and 2 (range, 1–12) in cohort B2. The median duration of treatment was 53 days (range, 21 to 84) in cohort A1, 77 days (range, 62 to 141) in cohort A2, 28 days (range, 14 to 152) in cohort B1 and 69 days (range, 29–496) in cohort B2. All patients received ICI treatment except two patients who only received SBRT because of rapid clinical decline secondary to complications of their disease. This included one patient from cohort A2 and one from cohort B1. All patients received radiation to an extracranial (abdominal or thoracic) site of metastatic disease. The majority of patients received SBRT to the primary pancreatic tumor site or recurrent disease site in the surgical bed (75%) (Table 2). SBRT of liver metastasis was done in 20% of patients.
Table 2:
SBRT Sites
| SBRT location – no. (%) | Cohort A1 8Gy × 1 +Durva (N=14) |
Cohort A2 5Gy × 5 +Durva (N=10) |
Cohort B1 8Gy × 1 +Durva/Treme (N=19) |
Cohort B2 5Gy × 5 +Durva/Trem (N=16) |
|---|---|---|---|---|
| Pancreas | 14 (100) | 8 (80) | 9 (47) | 13 (81) |
| Liver | 0 (0) | 1 (10) | 9 (47) | 2 (13) |
| Peritoneum lesions | 0 (0) | 1 (10) | 1 (5) | 1 (6) |
Abbreviation: SBRT: stereotactic body radiation therapy; Durva: Durvalumab; Treme: Tremelimumab
Safety
Treatment-related toxicities are summarized in Table 3. The safety population consisted of 58 evaluable patients. All patients experienced at least one treatment related AE, with the majority being grade 1–2 (81.5%) where medical intervention was not required. AEs of grade 3 or 4 were reported in 1 of 14 patients (lymphopenia, 7.1%) in cohort A1, 3 of 9 patients (lymphopenia, 33.3%) in cohort A2, 4 of 19 patients (lymphopenia and elevated amylase, 21.1%) in cohort B1, and 10 of 16 (lymphopenia, anemia, dehydration, diarrhea, hyperthyroidism, nausea and vomiting, 62.5%) in cohort B2. Grade 4 events were reported in 1 patient in cohort B1 and 2 patients in the cohort B2. All grade 4 AEs were lymphopenia. The most commonly occurring treatment-related AEs were lymphopenia, anemia, fatigue, thrombocytopenia, nausea, pruritus, elevated aspartate aminotransferase, diarrhea, hyponatremia, hypoalbuminemia, leukopenia, vomiting, skin rashes and fever. No DLT was encountered. No patient died of AEs. Fifty-one patients (83.6%) died during follow up because of disease progression.
Table 3:
Common Treatment Related Adverse Events With at Least 5% Incidence in Study Population
| Adverse Events | No.(%) of patients (N=58) | Cohort A1 (N=14) | Cohort A2 (N=10) | Cohort B1 (N=19) | Cohort B2 (N=16) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Grade 1–2 | Grade 3–4 | Grade 1–2 | Grade 3–4 | Grade 1–2 | Grade 3–4 | Grade 1–2 | Grade 3–4 | ||
| Lymphocyte count decreased | 38 (65.5) | 6 | 1 | 5 | 3 | 7 | 3 | 6 | 7 |
| Anemia | 20 (34.5) | 3 | 2 | 6 | 6 | 3 | |||
| Fatigue | 10 (17.2) | 1 | 2 | 7 | |||||
| Platelet count decreased | 10 (17.2) | 2 | 2 | 6 | |||||
| Rash | 9 (15.5) | 3 | 3 | 3 | |||||
| Nausea | 7 (12.1) | 1 | 3 | 2 | 1 | ||||
| Pruritus | 7 (12.1) | 2 | 3 | 2 | |||||
| AST increased | 6 (10.3) | 1 | 1 | 4 | |||||
| Vomiting | 6 (10.3) | 1 | 2 | 3 | |||||
| White blood cell decreased | 6 (10.3) | 1 | 2 | 1 | 2 | ||||
| Hypoalbuminemia | 6 (10.3) | 6 | |||||||
| Hyponatremia | 6 (10.3) | 1 | 3 | 2 | |||||
| Diarrhea | 5 (8.6) | 1 | 3 | 2 | |||||
| Fever | 5 (8.6) | 1 | 1 | 1 | 2 | ||||
| Anorexia | 4 (6.9) | 1 | 3 | ||||||
| Neutrophil count decreased | 3 (5.2) | 2 | 1 | ||||||
| Hypothyroidism | 3 (5.2) | 1 | 1 | 1 | |||||
Efficacy
A total of 39 patients had lesions that were evaluable for response (excluding the areas treated with SBRT), including 9 patients from cohort A1, 7 patients from cohort A2, 9 patients from cohort B1 and 14 patients from cohort B2. Efficacy data for the study population are shown in Fig 1A (radiologic response) and Fig 1B (quality and duration of objective responses). The data cut-off date of analysis was August 1, 2019. One patient achieved an unconfirmed partial response in Cohort A1 which lasted less than 2 months. He was a 63 year-old white male initially presenting with epigastric pain and diagnosed with moderately differentiated pancreatic ductal adenocarcinoma in the body and tail. He underwent a Whipple procedure and received adjuvant gemcitabine. He was susequently found to have a rising CA 19-9 and PET-avid lesions in the surgical bed and a left supraclavicular lymph node after the completion of adjuvant chemotherapy. The left supraclavicular lymph node was biopsied and confirmed metastatic PDAC. His cancer progressed through FOLFIRINOX, radiation and gemcitabine/nab-paclitaxel. His tumor had a KRAS codon 12 mutation and his disease was located in the surgical bed, liver and supraclavicular lymph node. After three dose of durvalumab, he developed severe abdominal pain. CT imaging indicated a partial response, but the patient decided to withdraw from the clinical trial. He then began treatment with liposomal irinotecan with 5-FU. He subsequently developed a bowel obstruction and had an ostomy procedure. Before he passed away, he received mitomycin treatment. One patient achieved a confirmed partial response in cohort B2 lasting over 16.5 months. This was 58 year-old black male who was diagnosed with metastatic PDAC with lung and liver involvement. He was previously treated FOLFIRINOX and gemcitatbine/nab-paclitaxel. His tumor was KRAS and CDKN2A mutated. He received four cycles of durvalumab/ tremelimumab followed by nine cycles of durvalumab alone. His 8-week restaging indicated a partial response and this response lasted until the planned 9-cycle of durvalumab treatment finished. He subsequently developed gastric outlet obstruction secondary to the pancreas mass and underwent a loop gastrojejunostomy. He was also found to have enlarged lung lesions that he had video-assisted thoracoscopic surgery. However, his condition declined rapidly and he passed while on home hospice. There were 14 patients with stable disease across the 4 treatment arms (Figure 1). Median time of stable disease was 2.0 months (range from 1.9–2.8 months) in cohort A1; 3.8 months (range from 2.2–4.7 months) in cohort A2; 4.5 months (range from 4.0–5.1 months) in cohort B1; and 3.5 months (range from 1.9 to 13.5 months) in cohort B2. The response was not associated with radiation site (Supplemental Table S1).
Figure 1:
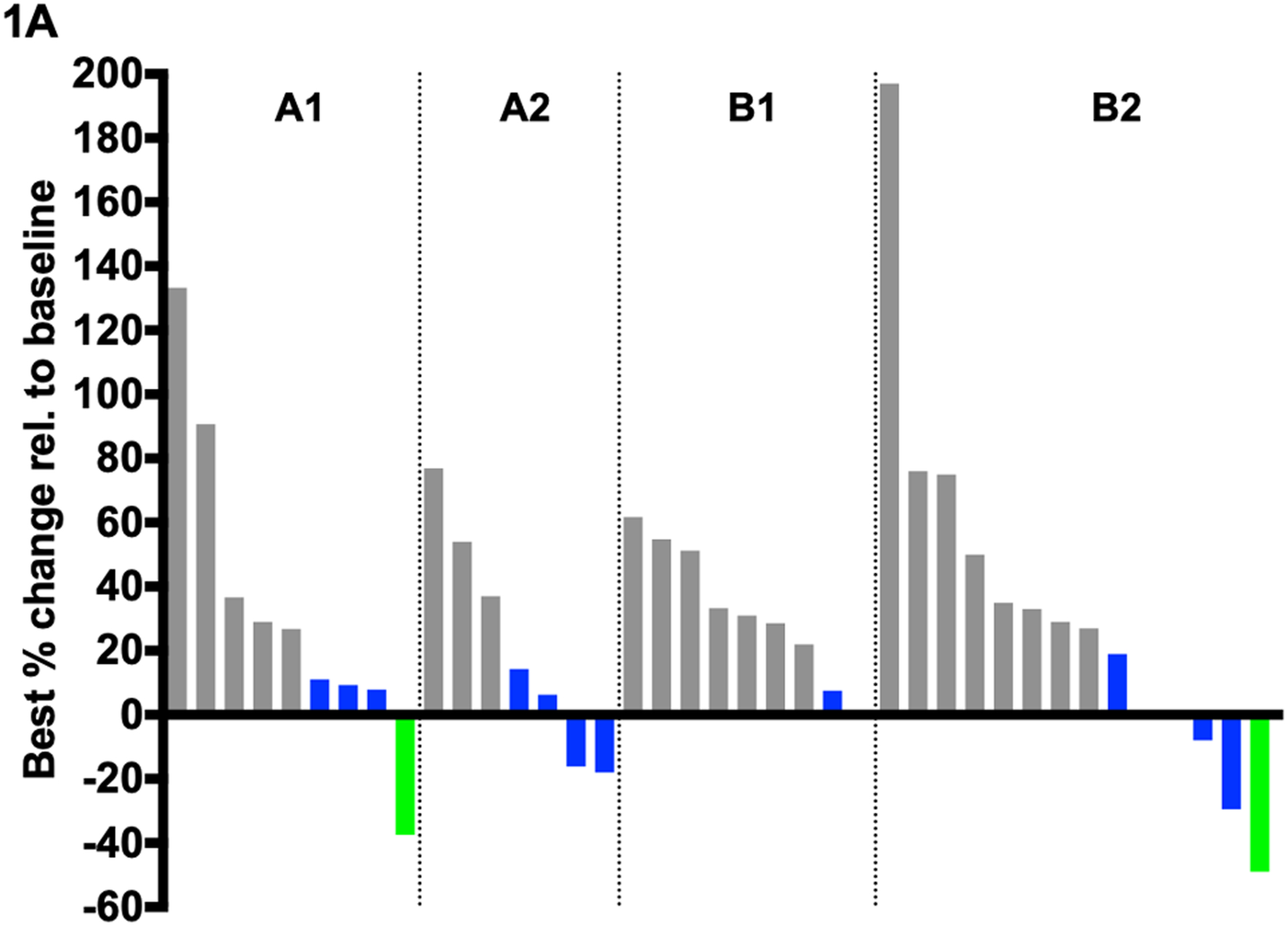
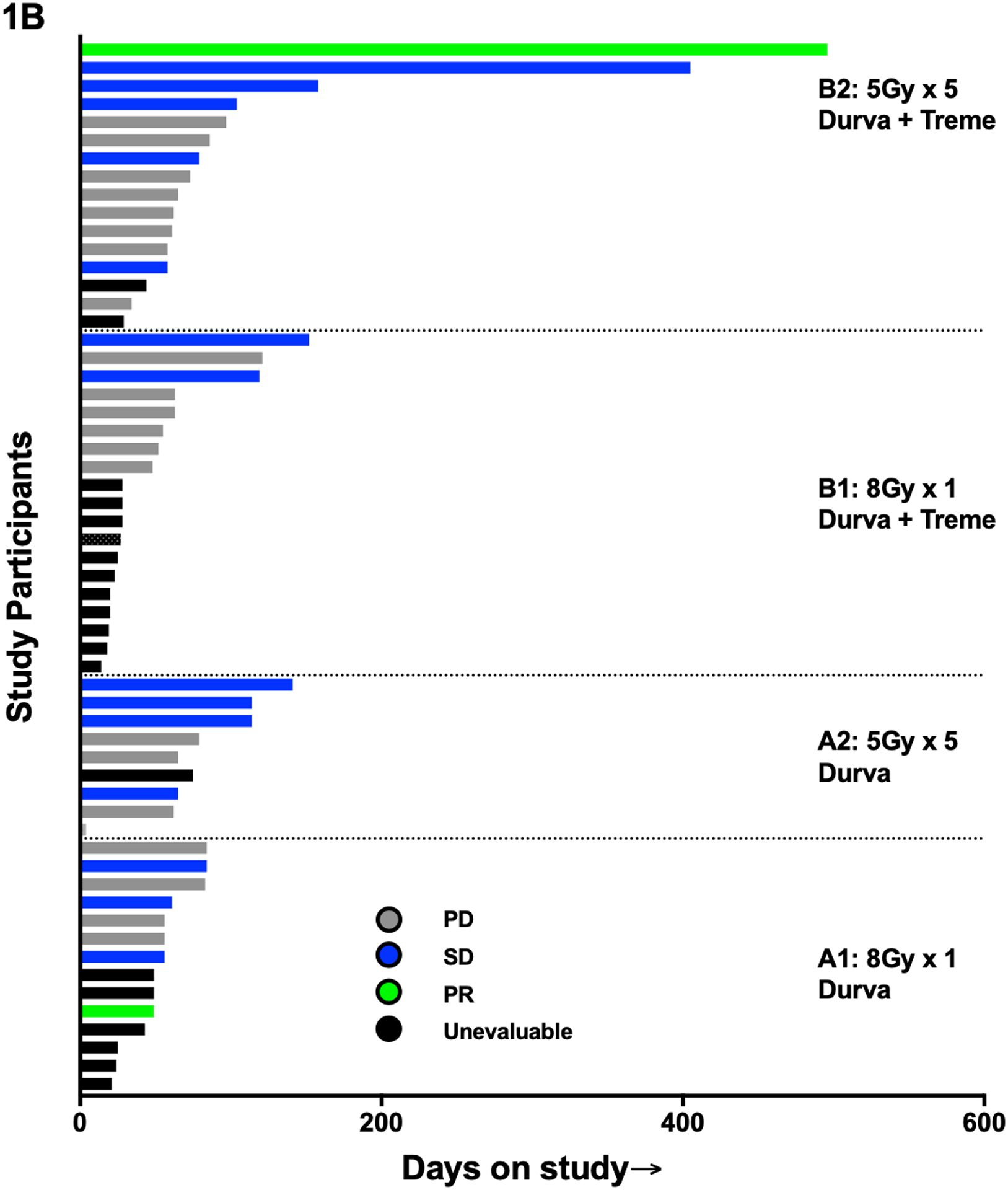
Efficacy data of study population. Durva, durvalumab; Treme, tremelimumab; PR, partial response; SD, stable disease; PD, progression disease; 8Gy × 1, 8Gy in one fraction; 5Gy × 5, 25Gy in 5 fractions.
There were 58 patients total included for survival analysis. One patient in cohort A2 was not included in PFS and OS analyses since this patient withdrew after enrollment and did not receive any treatment. Median PFS and OS was 1.7 months (95% CI 0.8–2.0 months) and 3.3 months (95% CI 1.2–6.6 months) in cohort A1; 2.5 months (95% CI 0.1–3.7 months) and 9.0 months (95% CI 0.5–18.4 months) in A2; 0.9 months (95% CI 0.7–2.1 months) and 2.1 months (95% CI 1.1–4.3 months) in B1; and 2.3 months (95% CI 1.9–3.4 months) and 4.2 months (95% CI 2.9–9.3 months) in B2 (Figure 2). No disease-specific subset analyses were performed given the small number of patients.
Figure 2:
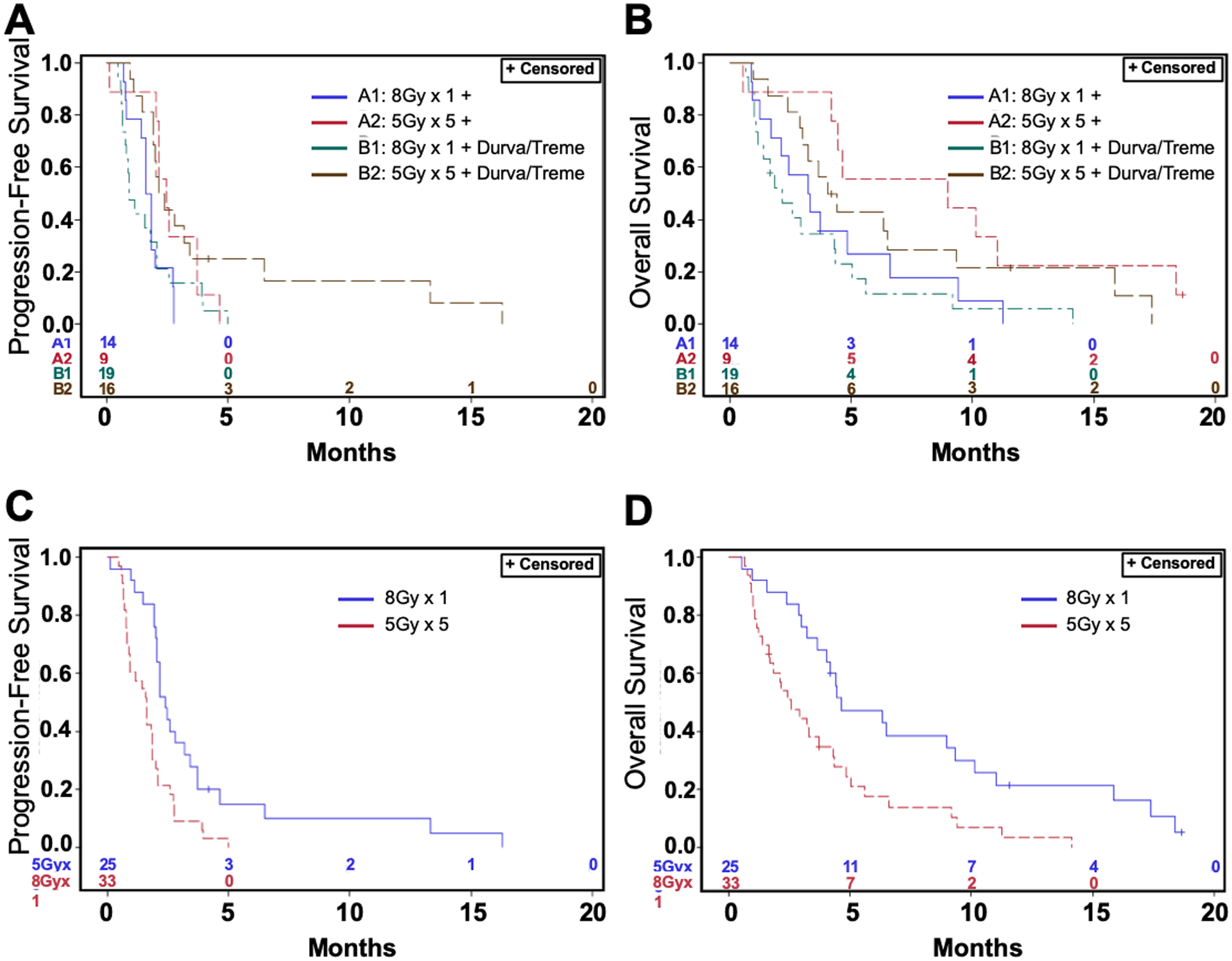
Progression-free and overall survival curves for each of the 4 arms and combined according to radiation dosage. Durva, durvalumab; Treme, tremelimumab; 8Gy × 1, 8Gy in one fraction; 5Gy × 5, 25Gy in 5 fractions.
Immune Correlatives
Tumor samples were obtained from five patients at baseline (pre-treatment) and day 29 (i.e. after SBRT plus ICI treatment) during the treatment course, including 2 SD, 2 PD and one PR from Cohort B2 that were analyzed for immune cell. Paired sample analyses demonstrated an increase in CD3 and CD8 positive cells for individual patients (Figure 3A and 3B), however, this was not statistically significant and independent of response to treatment. All samples tested had positive MHC-1 staining (Supplemental Figure S1).
Figure 3:
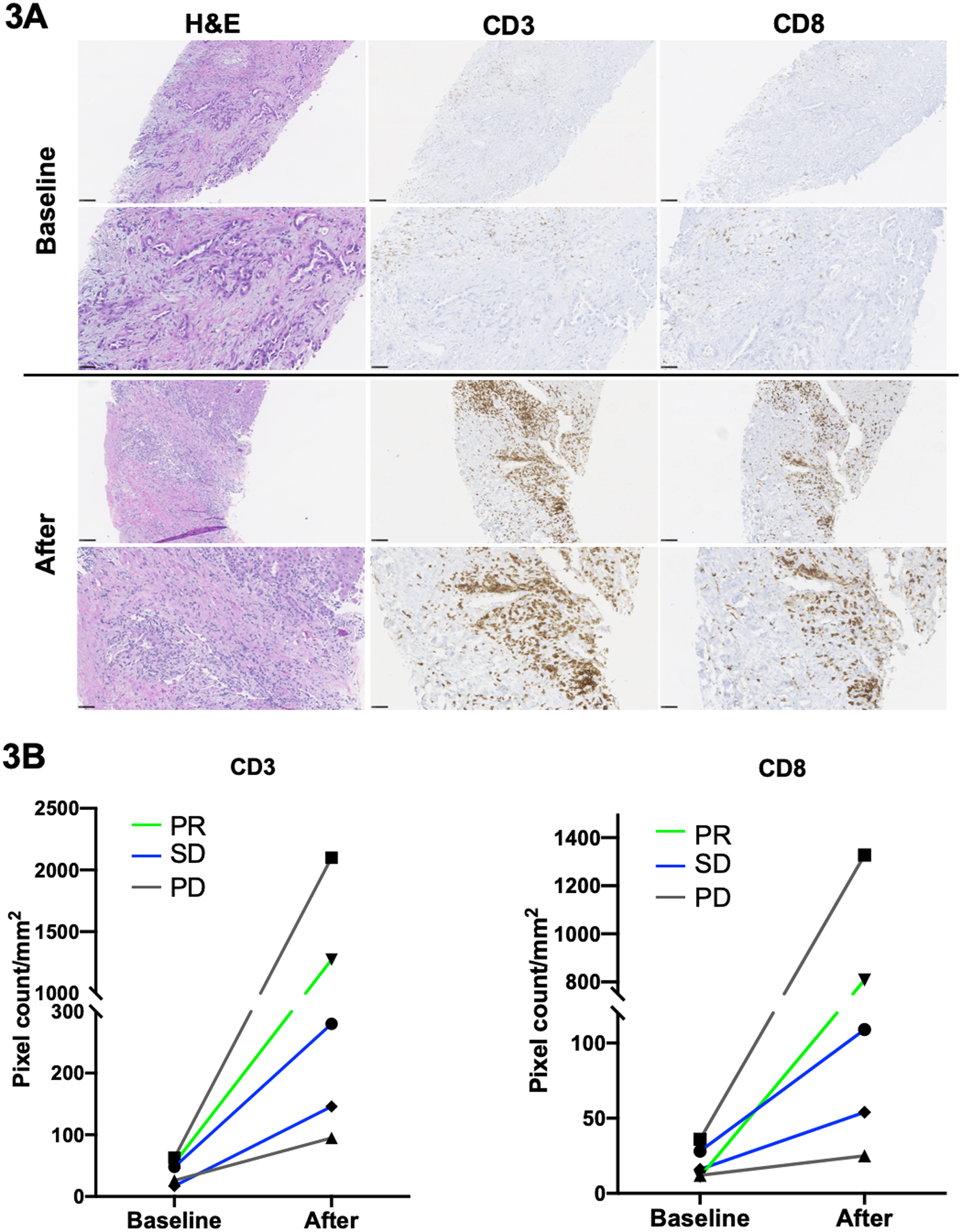
Immune cell infiltration studies. A: Representative H&E staining and intratumoral CD3+/CD8+ Tcell infiltration tested by immunohistochemistry from biopsied tumor samples at baseline (upper panel) and day 29 (after treatment, lower panel). Scale bar: 20 X and 40 X respectively. B: Changes of quantitative pixel count/mm2 of positive immunohistochemical staining of CD3 (left panel)/CD8 (right panel) immune cell tumor infiltration from baseline to after treatment. PR, partial response; SD, stable disease; PD, progression disease.
Discussion
During the past two decades, little progress has been made in improving the treatment of patients with metastatic PDAC despite extensive investigation of immune and targeted therapies[17, 26–28]. To our knowledge, the present phase I study is the first prospective report of safety and efficacy of combining ICI with SBRT in metastatic PDAC.
The safety profile of ICI plus SBRT was favorable and manageable. Only two patients from cohort B2 experienced grade 3 diarrhea with biopsy-confirmed autoimmune colitis and both were managed appropriately with no long term effects. The most common toxicities observed, regardless of grade, were cytopenias, transaminitis, rash, diarrhea, fever, fatigue, nausea and vomiting. The frequency of AEs in general was higher in cohort B2, likely related to the intensity of treatment. Similarly, the occurrence of grade 3 or 4 lymphopenia was higher in cohort B2 compared to the other cohorts. This may indicate that dual ICI combined with low fraction dosing has a stronger immunomodulating effect. No toxicity-related deaths were observed.
Of the 39 evaluable patients for efficacy analysis, there was 1 confirmed PR and 14 SD as best response which corresponds to a disease control rate of 41.0% and an objective response rate (ORR) of 2.6%. These results demonstrate similar clinical outcome compared to previous reports of no response with ICI monotherapy [14, 15, 26] or a 1.5% ORR with dual ICI in advanced PDAC[17]. Historically, second-line chemotherapy resulted in a median PFS of 1.8–3.1 months and OS of 4.5–10.1 months, depending on the regimen used [29–35]. In a phase II trial comparing durvalumab alone versus durvalumab plus tremelimumab in patients with advanced PDAC, the median PFS in both arms was 1.5 months and median OS was 3.6 months with durvalumab alone versus 3.1 months with the combination[17]. The median PFS and OS in our study was 2.0 and 3.7 months, respectively. The median PFS of all 4 arms were relatively close. However, the median OS was 3.3 months in cohort A1, 9.0 months in cohort A2, 2.1 months in cohort B1 and 4.2 months in cohort B2. In addition, over 75% of participants had progressive disease on at least two prior lines of chemotherapy. Although the study was not powered to conclude the benefit of ICI plus SBRT in advanced PDAC, our data indicates a potential new treatment strategy using SBRT to promote enhanced antitumor effects of ICI, which requires further follow-up studies.
In our study, 74.6% patients received SBRT to the primary pancreatic tumor site or recurrent lesions in the surgical bed of the pancreas. We did not plan to compare the outcome of SBRT to different sites in this analysis, and do not have sufficient power in this study to draw clear conclusions about this. Previous studies in other tumor types have demonstrated potential differences in the effectiveness of the immune response triggered by radiation, citing differences based on the location and size of the irradiated target[36], targeting of deeper tumors (vs tumors in superficial organs)[37], transient bacteremia as a result of abdominal irradiation[38] and fractionated dosing[39] [40]. We observed no effect on response rates or survival based on location of radiation (i.e. primary pancreatic lesion vs metastatic site).
PDAC is characterized by a low tumor mutational burden (TMB), ranging from 10 to 60 encoded neoantigens [41], and a median TMB of 1.8 mutations/Mb with only 1% of patients reaching TMB > 20 mutations/Mb[42]. Prior studies have shown that higher TMB tumors express increased numbers of neoantigens leading to increased immune surveillance[43], similar to whats seen in microsatellite instability (MSI) tumors, and contributes to the response to ICI. Because the protocol was opened before the finding of the relationship between MSI and response to immunotherapy, microsatellite status was not routinely checked. However, none of responders were MSI-high when checked retrospectively. In PDAC, it is questionable if SBRT can trigger immune responses that are strong enough to enhance the immunomodulating effects of ICI. A recent publication found that increased serum interferon-β after radiation and early dynamic changes of circulatory T cell clones were the strongest response predictiors in non-small-cell lung cancer[44]. Although an increased CD8 positive T cell infiltration was seen in day 29 biopsy samples that were evaluable in Cohort B2, this did not correlate to improved response. Defects in MHC class 1 has been implicated as the mechanism of immune escape and commonly found in solid tumor[45]. However, all samples tested showed MHC-1 positive regardless the response status to the combination treatment. We are currently studying systemic and local immune responses with samples we collected during the study.
The median OS of SBRT 8Gy-in-one-fraction arm combined from both Cohort A1 and B1 (durvalumab monotherapy or durvalumab plus tremelimumab) was 2.6 months vs 4.7 months in the SBRT 25Gy-in-5- fraction arm combined from both Cohort A2 and B2 (p=0.0042). This difference may indicate the effectiveness of fraction dosing over single-dose regimens in terms of mounting an immune response. As shown previously, DNA exonuclease Trex1 is induced by higher dose with single fraction and results in attenuated immunogenicity upon radiation[39]. This was also suggested in a previous report of metastatic melanoma treated with ipilimumab and radiation which demonstrated a significant association between immune response and multiple-fraction regimens[40]. In our study, all participants received ICI immediately after the completion of SBRT (Day 1 of all arms). The optimal sequencing of ICI and radiation is still unclear with limited data currently available[40, 46].
The main limitation of this trial was the relatively small patient population and slow accrual rate which could have resulted in imbalances between the treatment arms. Patients were also treated with a variety of chemotherapeutic agents prior to enrollment which could potentially influence the pre-treatment or baseline immune response. However, the primary aim of this study was to evaluate the safety and tolerability of combining ICI with SBRT in metastatic PDAC which was shown to be tolerated in multiple combinations between the four treatment arms. Nevertheless, in our study, over 70% patients underwent at least 2 lines of chemotherapy before enrollment and maintained an ECOG performance status between 0–1 as required to participate the trial. This may indicate that this patient population had more slow growing tumor rather than more commonly aggressive PDAC, though most of patients were heavily pretreated prior to the enrollment. It is unknown if this interferes with the efficacy of combination therapy in the trial.
In conclusion, the combination of ICI with SBRT has an acceptable safety profile and demonstrates a modest treatment benefit in metastatic PDAC. Future prospective studies to better define the dose and sequence of ICI and radiation treatment would provide additional information.
Supplementary Material
Translational Relevance.
The poor prognosis of metastatic pancreatic ductal adenocarcinoma treated with conventional chemotherapy demands the need for novel therapies. Although immunotherapy has been shown to result in durable responses in multiple tumor types with a favorable toxicity profile, the effectiveness of immunotherapy is limited in metastatic pancreatic ductal adenocarcinoma. In this phase I study, we investigated the tolerability and clinical impact of immune checkpoint inhibitor in combination with stereotactic body radiation therapy in patients with metastatic pancreatic ductal adenocarcinoma. We showed that the combination of immune checkpoint inhibitor with stereotactic body radiation therapy was well tolerated and found modest clinical activity in patients with metastatic pancreatic ductal adenocarcinoma. Notably, paired sample analyses demonstrated an increase in CD3 and CD8 positive cells for individual patients, although this was independent of response to treatment. These findings highlight the need for optimization of immunotherapeutic strategies in metastatic pancreatic ductal adenocarcinoma.
Acknowledgments
This research was supported by the Intramural Research Program of the NIH, National Cancer Institute, Center for Cancer Research and a Cooperative Research and Development Agreement between NCI and AstraZeneca. TFG is supported by the Intramural Research Program of the NIH, NCI (ZIA BC 011343).
Footnotes
Conflict of Interest
The authors who have taken part in this study declared that they do not have anything to disclose regarding funding or conflict of interest with respect to this manuscript.
References
- 1.Rahib L, Smith BD, Aizenberg R et al. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014; 74: 2913–2921. [DOI] [PubMed] [Google Scholar]
- 2.Ilic M, Ilic I. Epidemiology of pancreatic cancer. World J Gastroenterol 2016; 22: 9694–9705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Conroy T, Hammel P, Hebbar M et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N Engl J Med 2018; 379: 2395–2406. [DOI] [PubMed] [Google Scholar]
- 4.Neoptolemos JP, Palmer DH, Ghaneh P et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet 2017; 389: 1011–1024. [DOI] [PubMed] [Google Scholar]
- 5.Oettle H, Neuhaus P, Hochhaus A et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. JAMA 2013; 310: 1473–1481. [DOI] [PubMed] [Google Scholar]
- 6.Conroy T, Desseigne F, Ychou M et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364: 1817–1825. [DOI] [PubMed] [Google Scholar]
- 7.Von Hoff DD, Ervin T, Arena FP et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 2013; 369: 1691–1703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Borghaei H, Paz-Ares L, Horn L et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N Engl J Med 2015; 373: 1627–1639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brahmer J, Reckamp KL, Baas P et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N Engl J Med 2015; 373: 123–135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Brahmer JR, Drake CG, Wollner I et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol 2010; 28: 3167–3175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cha E, Klinger M, Hou Y et al. Improved survival with T cell clonotype stability after anti-CTLA-4 treatment in cancer patients. Sci Transl Med 2014; 6: 238ra270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Motzer RJ, Escudier B, McDermott DF et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N Engl J Med 2015; 373: 1803–1813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Weber JS, D’Angelo SP, Minor D et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol 2015; 16: 375–384. [DOI] [PubMed] [Google Scholar]
- 14.Patnaik A, Kang SP, Rasco D et al. Phase I Study of Pembrolizumab (MK-3475; Anti-PD-1 Monoclonal Antibody) in Patients with Advanced Solid Tumors. Clin Cancer Res 2015; 21: 4286–4293. [DOI] [PubMed] [Google Scholar]
- 15.Royal RE, Levy C, Turner K et al. Phase 2 trial of single agent Ipilimumab (anti-CTLA-4) for locally advanced or metastatic pancreatic adenocarcinoma. J Immunother 2010; 33: 828–833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Le DT, Uram JN, Wang H et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med 2015; 372: 2509–2520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.O’Reilly EM, Oh DY, Dhani N et al. Durvalumab With or Without Tremelimumab for Patients With Metastatic Pancreatic Ductal Adenocarcinoma: A Phase 2 Randomized Clinical Trial. JAMA Oncol 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Blanquicett C, Saif MW, Buchsbaum DJ et al. Antitumor efficacy of capecitabine and celecoxib in irradiated and lead-shielded, contralateral human BxPC-3 pancreatic cancer xenografts: clinical implications of abscopal effects. Clin Cancer Res 2005; 11: 8773–8781. [DOI] [PubMed] [Google Scholar]
- 19.Demaria S, Ng B, Devitt ML et al. Ionizing radiation inhibition of distant untreated tumors (abscopal effect) is immune mediated. Int J Radiat Oncol Biol Phys 2004; 58: 862–870. [DOI] [PubMed] [Google Scholar]
- 20.Lee Y, Auh SL, Wang Y et al. Therapeutic effects of ablative radiation on local tumor require CD8+ T cells: changing strategies for cancer treatment. Blood 2009; 114: 589–595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Reits EA, Hodge JW, Herberts CA et al. Radiation modulates the peptide repertoire, enhances MHC class I expression, and induces successful antitumor immunotherapy. J Exp Med 2006; 203: 1259–1271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zhang H, Liu L, Yu D et al. An in situ autologous tumor vaccination with combined radiation therapy and TLR9 agonist therapy. PLoS One 2012; 7: e38111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Valkenburg KC, de Groot AE, Pienta KJ. Targeting the tumour stroma to improve cancer therapy. Nat Rev Clin Oncol 2018; 15: 366–381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bernstein MB, Krishnan S, Hodge JW, Chang JY. Immunotherapy and stereotactic ablative radiotherapy (ISABR): a curative approach? Nat Rev Clin Oncol 2016; 13: 516–524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Xie C, Duffy AG, Mabry-Hrones D et al. Tremelimumab in Combination With Microwave Ablation in Patients With Refractory Biliary Tract Cancer. Hepatology 2019; 69: 2048–2060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Brahmer JR, Tykodi SS, Chow LQ et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med 2012; 366: 2455–2465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Le DT, Durham JN, Smith KN et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017; 357: 409–413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Neoptolemos JP, Kleeff J, Michl P et al. Therapeutic developments in pancreatic cancer: current and future perspectives. Nat Rev Gastroenterol Hepatol 2018; 15: 333–348. [DOI] [PubMed] [Google Scholar]
- 29.Sonbol MB, Firwana B, Wang Z et al. Second-line treatment in patients with pancreatic ductal adenocarcinoma: A meta-analysis. Cancer 2017; 123: 4680–4686. [DOI] [PubMed] [Google Scholar]
- 30.Oettle H, Riess H, Stieler JM et al. Second-line oxaliplatin, folinic acid, and fluorouracil versus folinic acid and fluorouracil alone for gemcitabine-refractory pancreatic cancer: outcomes from the CONKO-003 trial. J Clin Oncol 2014; 32: 2423–2429. [DOI] [PubMed] [Google Scholar]
- 31.Gill S, Ko YJ, Cripps C et al. PANCREOX: A Randomized Phase III Study of Fluorouracil/Leucovorin With or Without Oxaliplatin for Second-Line Advanced Pancreatic Cancer in Patients Who Have Received Gemcitabine-Based Chemotherapy. J Clin Oncol 2016; 34: 3914–3920. [DOI] [PubMed] [Google Scholar]
- 32.Kim JH, Lee SC, Oh SY et al. Attenuated FOLFIRINOX in the salvage treatment of gemcitabine-refractory advanced pancreatic cancer: a phase II study. Cancer Commun (Lond) 2018; 38: 32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ishikawa T, Kawashima H, Ohno E et al. Randomized Phase II Study of Consecutive-Day versus Alternate-Day Treatment with S-1 as Second-Line Chemotherapy in Advanced Pancreatic Cancer. Oncology 2019; 96: 1–7. [DOI] [PubMed] [Google Scholar]
- 34.Katopodis O, Polyzos A, Kentepozidis N et al. Second-line chemotherapy with capecitabine (Xeloda) and docetaxel (Taxotere) in previously treated, unresectable adenocarcinoma of pancreas: the final results of a phase II trial. Cancer Chemother Pharmacol 2011; 67: 361–368. [DOI] [PubMed] [Google Scholar]
- 35.Ettrich TJ, Perkhofer L, von Wichert G et al. DocOx (AIO-PK0106): a phase II trial of docetaxel and oxaliplatin as a second line systemic therapy in patients with advanced pancreatic ductal adenocarcinoma. BMC Cancer 2016; 16: 21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Demaria S, Formenti SC. Can abscopal effects of local radiotherapy be predicted by modeling T cell trafficking? J Immunother Cancer 2016; 4: 29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Yovino S, Kleinberg L, Grossman SA et al. The etiology of treatment-related lymphopenia in patients with malignant gliomas: modeling radiation dose to circulating lymphocytes explains clinical observations and suggests methods of modifying the impact of radiation on immune cells. Cancer Invest 2013; 31: 140–144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Paulos CM, Wrzesinski C, Kaiser A et al. Microbial translocation augments the function of adoptively transferred self/tumor-specific CD8+ T cells via TLR4 signaling. J Clin Invest 2007; 117: 2197–2204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Vanpouille-Box C, Alard A, Aryankalayil MJ et al. DNA exonuclease Trex1 regulates radiotherapy-induced tumour immunogenicity. Nat Commun 2017; 8: 15618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Chandra RA, Wilhite TJ, Balboni TA et al. A systematic evaluation of abscopal responses following radiotherapy in patients with metastatic melanoma treated with ipilimumab. Oncoimmunology 2015; 4: e1046028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Yarchoan M, Hopkins A, Jaffee EM. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N Engl J Med 2017; 377: 2500–2501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Chalmers ZR, Connelly CF, Fabrizio D et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med 2017; 9: 34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Schumacher TN, Schreiber RD. Neoantigens in cancer immunotherapy. Science 2015; 348: 69–74. [DOI] [PubMed] [Google Scholar]
- 44.Formenti SC, Rudqvist NP, Golden E et al. Radiotherapy induces responses of lung cancer to CTLA-4 blockade. Nat Med 2018; 24: 1845–1851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Garrido F, Cabrera T, Aptsiauri N. “Hard” and “soft” lesions underlying the HLA class I alterations in cancer cells: implications for immunotherapy. Int J Cancer 2010; 127: 249–256. [DOI] [PubMed] [Google Scholar]
- 46.Kiess AP, Wolchok JD, Barker CA et al. Stereotactic radiosurgery for melanoma brain metastases in patients receiving ipilimumab: safety profile and efficacy of combined treatment. Int J Radiat Oncol Biol Phys 2015; 92: 368–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.