

Abstract
We present a case of a single coronary artery system arising from the right sinus of Valsalva found to have an obstructive mid-vessel lesion with functional evidence of ischemia on stress testing. She was treated with a first-generation Cypher (Cordis, Johnson & Johnson, Hialeah, Florida) drug-eluting stent and remains asymptomatic at 14-year follow-up. (Level of Difficulty: Intermediate.)
Key Words: drug-eluting stent, single coronary artery
Abbreviations and Acronyms: DES, drug-eluting stent(s); RCA, right coronary artery; RSoV, right sinus of Valsalva; SCA, single coronary artery; SCD, sudden cardiac death; TIMI, Thrombolysis In Myocardial Infarction
Graphical abstract
We present a case of a single coronary artery system arising from the right sinus of Valsalva found to have an obstructive mid-vessel lesion…
We present a case report of a single coronary artery (SCA) originating from the right sinus of Valsalva (RSoV) treated with first-generation Cypher (Cordis, Johnson & Johnson, Hialeah, Florida) drug-eluting stent (DES) implantation.
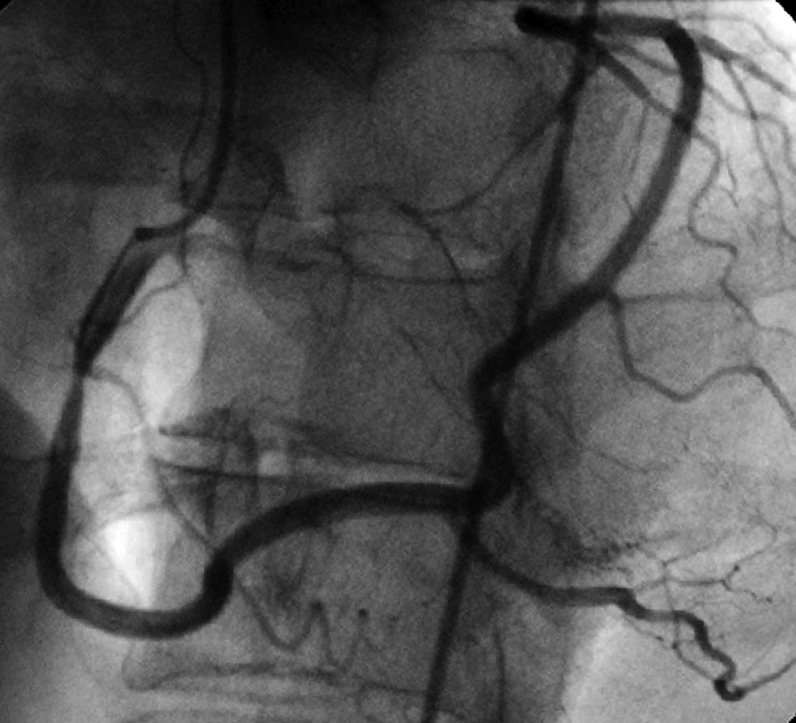
A 61-year-old woman with hypertension and hypercholesterolemia originally presented with lifestyle-limiting fixed threshold class 3 exertional angina on reasonable medical therapy including beta blocker, angiotensin converting enzyme inhibitor, nitrate, statin, and aspirin. She had an early positive exercise treadmill test for ischemia, demonstrating marked down sloping ST-segment depression and T-wave inversion in the inferolateral leads, with reproduction of limiting exertional angina at 4 min of Bruce protocol (high-risk Duke Treadmill Score). Coronary angiography performed October 2004 demonstrated a 70% eccentric focal mid stenosis of a single coronary artery originating from the RSoV (Figure 1). She underwent successful direct Cypher DES implantation, using temporary transvenous pacer support, yielding an excellent result (Figure 2). Repeat coronary angiography performed December 2004 for recurrent chest pain demonstrated a widely patent DES in the mid RCA with 0% residual and normal Thrombolysis In Myocardial Infarction (TIMI) flow grade 3 distal (Figure 3). The patient remains on dual antiplatelet therapy and aggressive lipid management. She continues to remain asymptomatic, with no events or additional procedures at her last follow-up visit in January 2019.
Figure 1.

Right Coronary Artery Giving Origin to the Entire Coronary Vasculature
Figure 2.

Post-Right Coronary Artery Stenting
Figure 3.

Subsequent Angiogram
SCA is a very rare congenital coronary anomaly, occurring in 0.031% of patients undergoing routine coronary angiography; these variants are classically characterized by the Lipton Classification 1, 2. Coronary anomalies with an interarterial course can be associated with myocardial infarction and sudden cardiac death (SCD), especially during exercise-induced great-vessel dilation, resulting in coronary compression (3). Nevertheless, this case demonstrated no interarterial course (Lipton R1), suggesting a more benign prognosis regarding the direct SCA consequences (3). However, these anomalies are less benign with coexisting atherosclerotic disease as SCAs predispose these patients to more diffuse/global myocardial injury—especially with main trunk stenoses—possibly leading to concomitant heart failure, cardiogenic shock, and SCD. These conditions are further exacerbated by the inability of SCAs to develop effective collaterals, which is otherwise possible with separate origins of the left and right coronary circulation. Therefore, SCA may inherently possess a worse prognosis upon restenosis of a DES compared with typical coronary anatomy.
There is lack of evidence to guide treatment of atherosclerotic lesions in patients with SCA. Percutaneous coronary intervention was used in this case because of the favorable lesion location and morphology (American College of Cardiology, type A). If we extrapolate data from left main coronary artery stenosis trials, coronary artery bypass surgery may be a superior or equivalent option, depending upon lesion location and morphology.
Footnotes
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
References
- 1.Turkmen S., Yolcu M., Sertcelik A., Ipek E., Dokumaci B., Batyraliev T. Single coronary artery incidence in 215,140 patients undergoing coronary angiography. Folia Morphol (Warsz) 2014;73:469–474. doi: 10.5603/FM.2014.0070. [DOI] [PubMed] [Google Scholar]
- 2.Lipton M.J., Barry W.H., Obrez I., Silverman J.F., Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979;130:39–47. doi: 10.1148/130.1.39. [DOI] [PubMed] [Google Scholar]
- 3.Elbadawi A., Baig B., Elgendy I.Y. Single coronary artery anomaly: a case report and review of literature. Cardiol Ther. 2018;7:119–123. doi: 10.1007/s40119-018-0103-4. [DOI] [PMC free article] [PubMed] [Google Scholar]