

Abstract
Alzheimer's disease has been one of the major concerns recently. Around 45 million people are suffering from this disease. Alzheimer's is a degenerative brain disease with an unspecified cause and pathogenesis which primarily affects older people. The main cause of Alzheimer's disease is Dementia, which progressively damages the brain cells. People lost their thinking ability, reading ability, and many more from this disease. A machine learning system can reduce this problem by predicting the disease. The main aim is to recognize Dementia among various patients. This paper represents the result and analysis regarding detecting Dementia from various machine learning models. The Open Access Series of Imaging Studies (OASIS) dataset has been used for the development of the system. The dataset is small, but it has some significant values. The dataset has been analyzed and applied in several machine learning models. Support vector machine, logistic regression, decision tree, and random forest have been used for prediction. First, the system has been run without fine-tuning and then with fine-tuning. Comparing the results, it is found that the support vector machine provides the best results among the models. It has the best accuracy in detecting Dementia among numerous patients. The system is simple and can easily help people by detecting Dementia among them.
1. Introduction
Machine learning (ML) is defined as the study of computer programs that leverage algorithms and statistical models to learn through inference and patterns without being explicitly programmed [1]. ML algorithms learn over experience and improve automatically. It finds techniques, trains models, and uses the learned approach to determine the output automatically [2]. Machine learning systems can also adjust themselves to a changing environment.
A model is a machine learning system that has been trained to identify specific types of patterns using an algorithm in a machine learning system [3]. That means it processes the data and finds out the hidden structures in a dataset [4]. The feature extraction and the known answers of a dataset determine the formula that relies upon the input and output functions and applies it to new data to predict the response [5]. Hence, the model's algorithm uses a collection of data for training and builds a way to predict the output and saves that procedure for future purposes.
A support vector machine (SVM) is a supervised machine learning model that uses classification algorithms for two-group classification problems. Support vector machine is a fast and dependable classification algorithm that performs very well with a limited amount of data to analyze [6]. SVMs are a group of similar supervised learning techniques that are used for classification and regression problems [7].
The logistic regression model is the appropriate regression analysis. Logistic regression is predictive regression analysis [8]. To classify data and to illustrate the relationship between one dependent binary variable and one or more independent nominal, ordinal, interval, or ratio-level variables, logistic regression is used [9].
In a machine learning system, a decision tree algorithm partitions the data into subsets. A decision tree's purpose is to sum up the training data in the smallest tree possible [10]. The decision tree is a supervised classification method that carries out a split test in its internal node and forecasts an example target class in its leaf node [11]. Decision tree algorithms are used to classify the characteristics to be evaluated at any node to specify the “best” splitting [12]. Decision trees are commonly used in classification problems because of their versatility and consistency.
The random forest is a supervised learning algorithm. Random forest is a versatile, easy-to-use machine learning algorithm that provides, most of the time, a fantastic result even without hyperparameter tuning [13]. Its simple design and variety are also some of the most used algorithms [14].
SVM can be applied to nonlinear problems, whereas logistic regression can only work with linear ones. SVM operates outliers better, as it derives maximum margin solution. Decision trees are better at dealing with collinearity than logistic regression. For categorical values, decision trees outperform logistic regression. A random forest is a set of decision trees that are randomly generated, and the expected output is chosen by the forest's majority vote. Decision trees are less reliable and accurate than random forest. SVM solves nonlinear issues using kernel methods, whereas decision trees apply hyperrectangles in input space to solve the problem. For a classification problem, SVM performs better than random forest [15].
Machine learning models are now widely used in medical diagnosis [16–19]. This paper compares different machine learning performances to diagnose Alzheimer's syndrome. Alzheimer's syndrome is an inherited, irreversible brain condition that steadily affects the ability to perform the necessary things, memory, and reasoning skills [20]. A massive proportion of neurons stop working in Alzheimer's disease, losing synaptic connections [21]. Alzheimer's diseases are infrequent in people aged between their 30s and mid-60s [22]. Symptoms can include a shift in sleep habits, depression, anxiety, and difficulties doing basic tasks such as reading or writing and aggressive actions, and poor decision-making also happened in Alzheimer's disease [23]. Alzheimer's disease and initial changes in the brain begin 10–20 years before the onset of symptoms [24]. It progressively leads to memory damage and decreases thinking abilities [25]. The leading cause of this disease is Dementia. A report shows that around 40–50 million people worldwide are suffering from Dementia, and this number will be increased to around 131.5 million by 2050 [26]. Approximately 70% of people who have Dementia are from low-income countries; see Figure 1.
Figure 1.
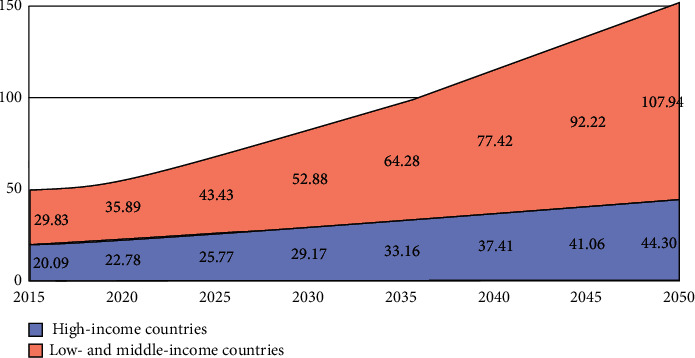
Number of people with Dementia in millions [27].
Dementia is the failure of brain function, understanding, recognizing, thinking, and behavioral skills to such a level that an individual faces problems in everyday life and behaviors [28]. Few people with Dementia are unable to deal with their emotions, and their personalities can be changed [29]. From the mildest stage, Dementia varies in severity [30]. It mainly affects older people. No cure is available other than treatment [31].
There is little data available on Alzheimer's patients in Bangladesh. According to the WHO data published in 2017, Alzheimer's or Dementia deaths in Bangladesh reached 9,917 or 1.26% of the total deaths, which was the last data found in this aspect that ranks Bangladesh number 152 globally [32]. In Bangladesh, the awareness about Alzheimer's is now in the primary stage. Therefore, impacted patients and families are regularly experiencing various issues [33]. The fund for researching Alzheimer's is limited. A lower-middle-income country like Bangladesh is not yet prepared for the management of Alzheimer's [34]. Besides that, almost one-fifth of the Bangladeshi adult population is overweight, according to a global study [35], which is the leading risk factor for Alzheimer's. Therefore, there are more chances of occurrences of Alzheimer's [36]. To give a treatment for this disease, physicians tend to test individuals for Alzheimer's disease by obtaining a medical and family history and psychiatric history from the point of view of specialists such as neurologists, neuropsychologists, geriatricians, and geriatric psychiatrists [37].
Studies show that the situation may improve if people can detect Alzheimer's disease early by taking therapy at the initial stage [38]. For this, they have to predict the progress of the disease accurately from mild condition to Dementia. Machine learning technology can help to predict accurately early Alzheimer's disease. There are many machine learning systems, but they give inconsistent and inaccurate predictions. They also have overfitting and underfitting issues. Therefore, a model has been developed by us which can indicate Alzheimer's disease early, using machine learning to support medical technicians. It will verify and show if anyone has Alzheimer's disease or not.
The remainder of the paper is organized as follows: Section 2 discusses methods and methodology, and Section 3 provides the results and analysis. Finally, in Section 4, the conclusion of the presented work is provided.
2. Methods and Methodology
In this section, all methods and materials, the dataset feature's description, block diagram, flow diagram, and evaluation matrices of the system are discussed.
2.1. Dataset
The main goal of the system is to predict Dementia in different patients based on various attributes. The longitudinal Magnetic Resonance Imaging (MRI) data from OASIS [39] has been used for the development of the system. The OASIS dataset has a dimension of 373 rows x 15 columns, which is relatively small in the field of machine learning. Table 1 shows eight different attributes: gender (M/F), person's age (age), years of education (EDUC), socioeconomic status (SSE), mini-mental state examination (MMSE), estimated total intracranial volume (eTIV), normalized whole brain volume (nWBV), and Atlas scaling factor (ASF) have been considered for the final outcome. For range values, a standardization method has been applied for scaling the dataset. A standard score is the number of standard deviations by which the value of a raw score is above or below the mean value of what is being observed or measured. The formula is as follows: z = (x − μ)/σ. Here, µ is the mean, and σ is the standard deviation.
Table 1.
OASIS dataset of proposed machine learning system.
| Subject ID | MRI ID | Group | Visit | MR delay | M/F | Hand | Age | EDUC | SES | MMSE | CDR | eTIV | nWBV | ASF |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OSA2_0001 | OSA2_0001_MR1 | Nondemented | 1 | 0 | M | R | 87 | 14 | 2.0 | 27.0 | 0.0 | 1987 | 0.696 | 0.883 |
| OSA2_0001 | OSA2_0001_MR2 | Nondemented | 2 | 457 | M | R | 88 | 14 | 2.0 | 30.0 | 0.0 | 2004 | 0.681 | 0.876 |
| OSA2_0002 | OSA2_0001_MR1 | Demented | 1 | 0 | M | R | 75 | 12 | NaN | 23.0 | 0.5 | 1678 | 0.736 | 1.046 |
| OSA2_0002 | OSA2_0001_MR2 | Demented | 2 | 560 | M | R | 76 | 12 | NaN | 28.0 | 0.5 | 1738 | 0.713 | 1.010 |
| OSA2_0002 | OSA2_0001_MR | Demented | 3 | 1895 | M | R | 80 | 12 | NaN | 22.0 | 0.5 | 1698 | 0.701 | 1.034 |
Table 2 shows the eight features of the dataset which have been considered for the proposed model to predict Alzheimer's disease and the description of the features. Most of the features are numerical. Group, hand, and M/F are categorical. All of these terms describe the patient's condition and aid in determining the stage of Dementia using the ML system.
Table 2.
Dataset description of proposed machine learning system.
| Features | Description |
|---|---|
| M/F | Gender |
| Age | Person's age |
| EDUC | Years of education |
| SES | Socioeconomic status |
| MMSE | Mini-mental state examination |
| eTIV | Estimated total intracranial volume |
| nWBV | Normalized whole brain volume |
| ASF | Atlas scaling factor |
2.2. Block Diagram
Figure 2 shows the block diagram of the machine learning system. The OASIS dataset has been used in the system, which contains all the attributes and values. First, the dataset has been analyzed by us for any categorical values, and there are several categorical values present in the dataset. Among them, gender and group attribute columns are converted into numeric values 0 and 1. The correlation between attributes has been checked by us using the “correlation matrix” function based on group attributes and plotted to understand them better. Gender, SES, and ASF showed a closer correlation with the group attribute. After that, the dataset is checked for any null or missing values. SES and MMSE columns have 19 and 2 missing values, respectively. As mentioned earlier, the SES feature has a close correlation with the target attribute. For that reason, the missing values of those rows were not deleted. Instead, the median value is used to fill in those missing values for both features.
Figure 2.
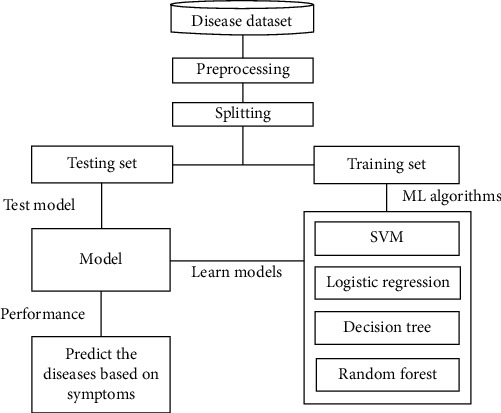
Block diagram.
Next, the features have been assigned to make the prediction, and the target value has been set so that the model can predict. Then, the dataset was split for training-validation and testing. Random sampling has been used for the split, but this creates an imbalance between training and testing split. So, stratified sampling has been applied with a training-validation size of 80% and a testing size of 20%. After that, standardization has been applied to do the scaling of the features. Furthermore, some histograms and scatterplot visualization have been done on the training split to understand the scenario better. Then the training of this system began. All of the models have been implemented using the scikit-learn library.
2.3. Flowchart Diagram
2.3.1. SVM Flowchart
Figure 3 shows the flow diagram of the whole SVM model. First, the support vector machine has been implemented without any fine-tuning. Without fine-tuning, SVM takes regularization parameter C as 1, and, for the kernel, it uses the radial basis function (RBF). After that, the grid search has been applied to fine-tune the model. Then, different regularization parameters have been taken for the parameter combinations, such as values C, gamma values, and four types of kernels: the RBF, linear, poly, and sigmoid kernel. Also, 5-fold cross-validation has been applied to evaluate all possible combinations. Then, the model was trained again, and there was a significant improvement. The confusion matrix has been calculated based on this version.
Figure 3.
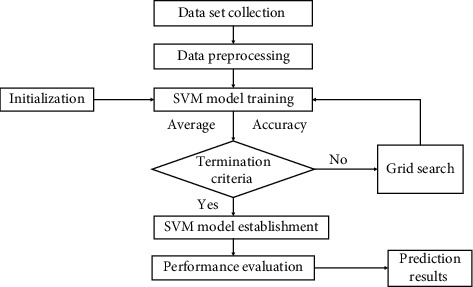
Flowchart of SVM.
2.3.2. Logistic Regression Flowchart
Figure 4 shows the flow diagram of the whole logistic regression model. The same approach has been applied with the logistic regression model, just like the SVM. It determines the independent and dependent variables. It uses the sigmoid function for predicting probabilities and making decision boundaries. The only difference is that the l2 penalty and different regularization parameter values C have been used for the fine-tuning.
Figure 4.
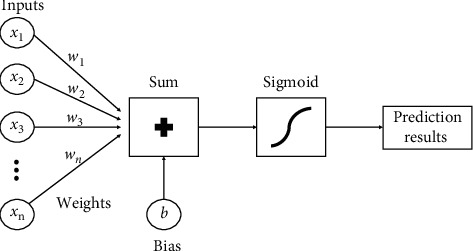
Flowchart of logistic regression.
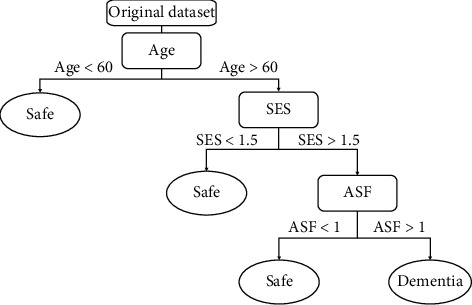
2.3.3. Decision Tree Flowchart
Figure 5 shows the flow diagram of the whole decision tree model. In the decision tree model, the same approach is followed. The model has been trained without fine-tuning and then used the grid search to find the best parameter values to fine-tune the model. Here, the Gini criterion has been considered a fixed value to evaluate the tree's quality and choose a range of 1 to 10 to evaluate the depth of the tree. It decides every node and goes more in depth. After analyzing all the nodes' choices, it predicts the results for the best solution.
Figure 5.
Flowchart of decision tree.
2.3.4. Random Forest Flowchart
Figure 6 shows the flow diagram of the whole random forest model. It is a collection of some decision trees. The process is the same as the decision tree. It preprocesses the data and selects some random samples from the dataset for training. For every selected sample, it forms a decision tree. First, the random forest model has been trained without fine-tuning. Then, just like the SVM, grid search has been used with 5-fold cross-validation and different parameter combinations such as the number of trees in the random forest (n_estimators), what function to use for the number of features to consider at every split, levels in the tree, and method of selecting samples for training each tree. To measure the quality of the tree, the Gini criterion has been used. The entropy criterion has also been tried in the model, but Gini criterion provides better accuracy.
Figure 6.

Flowchart of random forest.
2.4. Evaluation Matrices
Figure 7 shows the diagram of the confusion matrix. The confusion matrix is a performance evaluator for the classification models of machine learning. To evaluate the performance of all the developed models, the confusion matrix has been used. The confusion matrix represents how many times our models predict correctly and how many times they predict incorrectly. It categorized the correctly predicted values as true positives and true negatives and also categorized the wrongly predicted values as false positives and false negatives. After organizing all the predicted values in the matrix, the model's performance has been measured through accuracy, precision-recall trade-off, and AUC.
Figure 7.
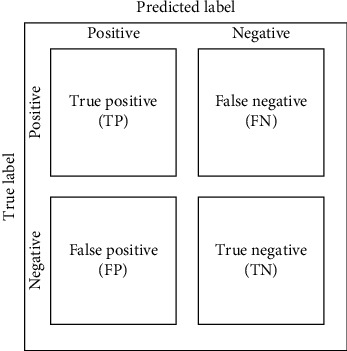
Diagram of confusion matrix.
3. Results and Analysis
The models' functions, model predictions, analysis, and final results are discussed in this section.
3.1. Data Visualization
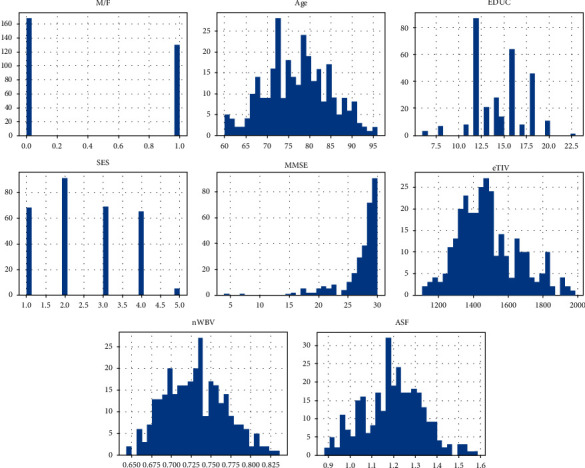
3.1.1. Histogram
Figure 8 shows the histogram of the training and validation set. Histogram portrays the ratios of the dataset. From the M/F plot, it has been observed that the male-female ratio in the dataset is 60% to 40%. All patients' age in the dataset is 60+ years. The majority of SES is 2, and MMSE is 30. Most of the patients' education years are 12.5. Also, the eTIV, nWBV, and ASF are relatively high.
Figure 8.
Histogram of training and validation set.
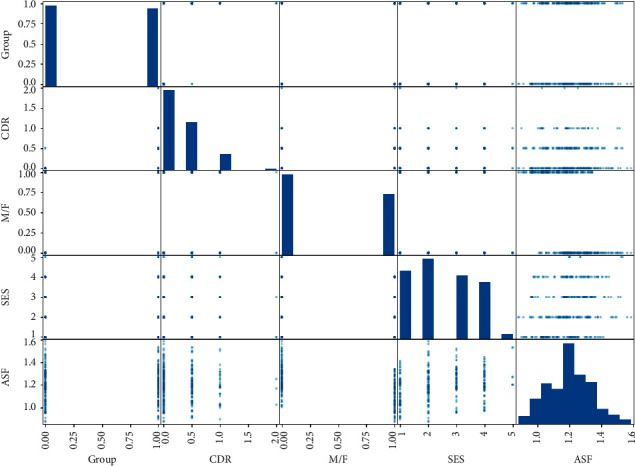
3.1.2. Correlation Matrix
Figure 9 shows the correlation matrix of the features in the dataset. The correlation matrix indicates how features are interrelated with each other. The group is the main target feature for detecting Dementia. If the value of the group is greater than 0.5, the patients have Dementia. From the correlation matrix, it has been observed that the higher the value of ASF and SES, the more the chances of getting Dementia. It is also observed that males have more chance of getting Dementia than females.
Figure 9.
Correlation matrix.
3.2. Model
3.2.1. SVM Model
Figure 10 shows the SVM model's prediction before fine-tuning. The predicted result is shown in the confusion matrix, and the model's calculated performance has also been demonstrated. The number of correct predictions is 56, and the number of wrong predictions is 19. It has 85% training accuracy and 74% testing accuracy. It also possesses 59% test recall and 74% test AUC.
Figure 10.
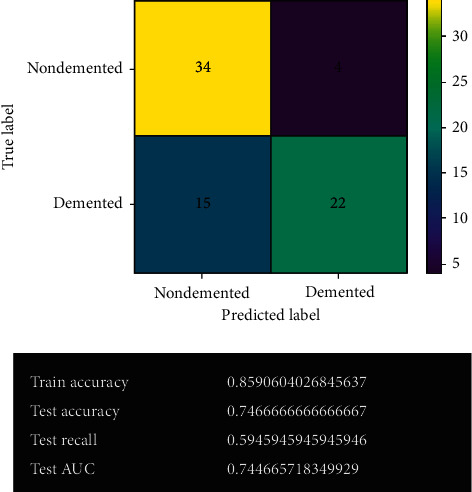
SVM model.
3.2.2. SVM Model after Fine-Tuning
Figure 11 shows the SVM model's prediction after fine-tuning. After fine-tuning, the obtained result has improved quite significantly. The SVM model gives 69 correct predictions and only 6 wrong predictions with 92% accuracy. For classification problems, SVM always provides the best accuracy among other models. It gives the best true negative results in the system. It also possesses 91% of both test recall and test AUC. No overfitting or underfitting issues have been observed from the model.
Figure 11.
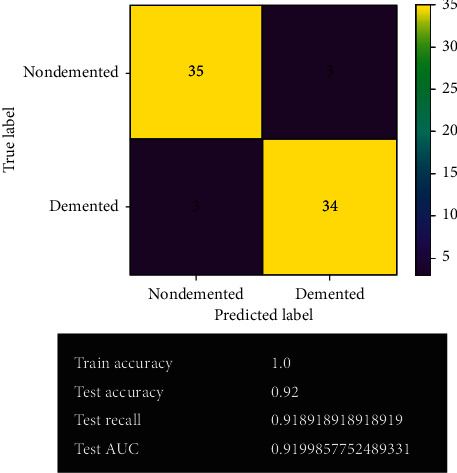
SVM model after fine-tuning.
3.2.3. Logistic Regression Model
Figure 12 shows the logistic regression model's prediction before fine-tuning. The confusion matrix shows the actual predicted values using this model. The model gives 56 correct predictions and 19 wrong predictions with 74.7% accuracy. It has given the same accuracy as before fine-tuning by the SVM model. It also holds 70% test recall and 74% test AUC.
Figure 12.
Logistic regression model.
3.2.4. Logistic Regression Model after Fine-Tuning
Figure 13 shows the logistic regression model's prediction after fine-tuning. After fine-tuning, the logistic regression model remained the same. The model's results have not changed. It gives the same correct and wrong predictions as before with 74.7% accuracy. No overfitting issue has been detected in the model.
Figure 13.
Logistic regression model after fine-tuning.
3.2.5. Decision Tree Model
Figure 14 shows the decision tree model's prediction before fine-tuning. The decision tree model gives 56 correct predictions and 19 wrong predictions, the same as the logistic regression model. It offers 100% training accuracy and 72% testing accuracy. It also provides 67% test recall and 71% test AUC.
Figure 14.
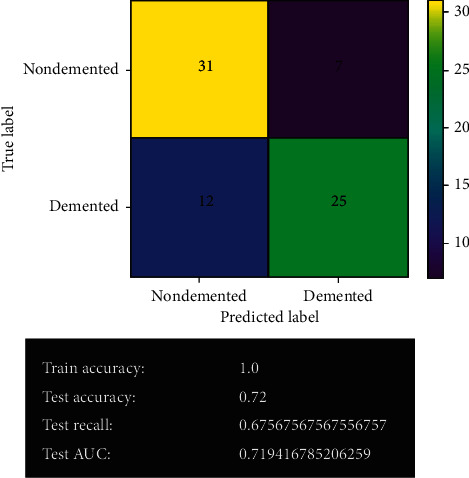
Decision tree model.
3.2.6. Decision Tree Model after Fine-Tuning
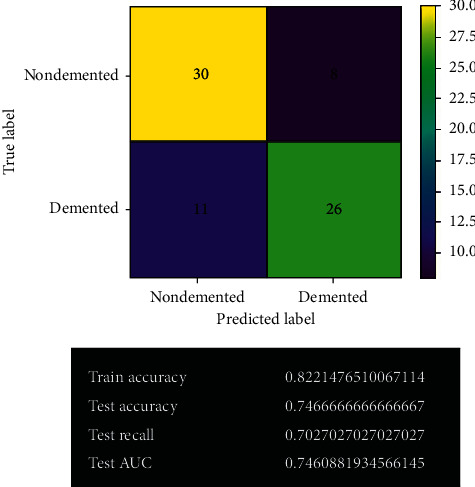
Figure 15 shows the decision tree model's prediction after fine-tuning. After fine-tuning, the decision tree model has improved quite a lot. It gives 60 correct predictions and 15 wrong predictions with 80% accuracy. It also gives the best true positive results in the system. The least overfitting issue has been experienced in the model.
Figure 15.

Decision tree model after fine-tuning.
3.2.7. Random Forest Model
Figure 16 shows the random forest model's prediction before fine-tuning. The random forest model gives 61 correct predictions and 14 wrong predictions. It offers 100% accuracy in training and 81% accuracy in test validation. It also gives 70% recall and 81% AUC on validation.
Figure 16.
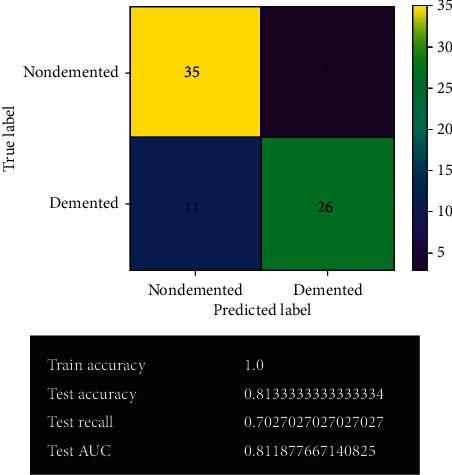
Random forest model.
3.2.8. Random Forest Model after Fine-Tuning
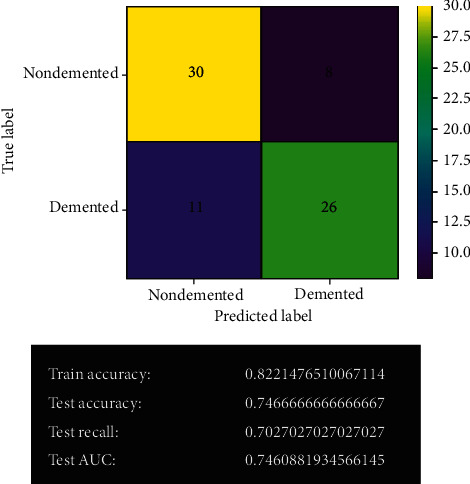
Figure 17 shows the random forest model's prediction after fine-tuning. After fine-tuning, the accuracy of the random forest model decreases. It gives 60 correct predictions and 15 wrong predictions with 80% accuracy. Actually, it has quite similar result to the previous one. Too many overfitting issues have been found in the model.
Figure 17.
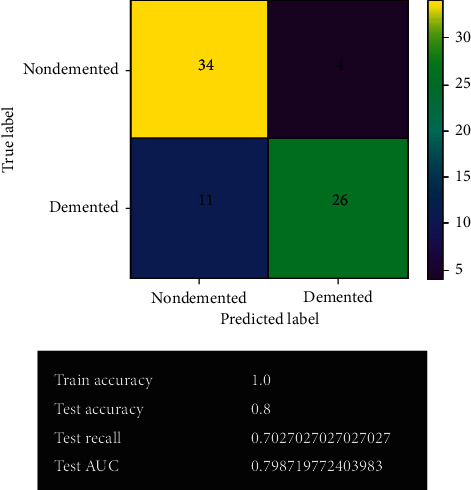
Random forest model after fine-tuning.
3.3. Model Comparison
3.3.1. ROC and AUC
Figure 18 shows the plotting of receiver operating characteristic (ROC) and comparison of AUC. Since this is a classification problem, the evaluation metrics used in this system were as follows: accuracy, recall, area under the curve (AUC), and confusion matrix. After compiling the results from all the models, it is evident that support vector machine (SVM), more specifically support vector classifier, gave the best overall result in all metrics. However, the decision tree classifier gave the best true positive result. For fine-tuning, grid search has been used in the models. So, the results obtained are the best possible result for the particular dataset. Some overfitting has been noticed in decision tree and random forest models.
Figure 18.
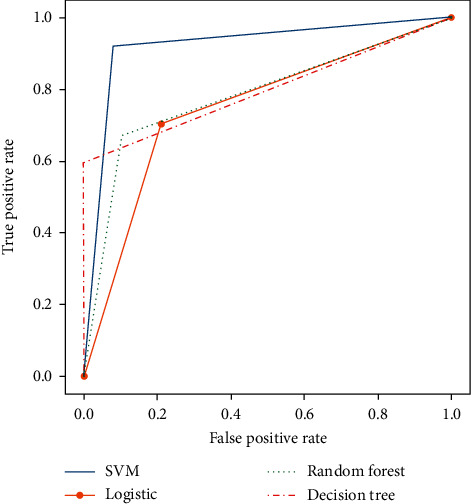
Plotting of ROC and comparison of AUC.
3.3.2. Comparison Table
Table 3 shows the comparison table of the models. The table clearly indicates that SVM is the best model among the other models in the system. It has better accuracy, recall, area under the curve, and F1 score.
Table 3.
Comparison table of models.
| Model | Accuracy (%) | Recall (%) | Precision (%) | AUC (%) | F1 score |
|---|---|---|---|---|---|
| SVM | 92.0 | 91.9 | 91.9 | 91.9 | 91.9% |
| Logistic regression | 74.7 | 70.3 | 76.5 | 74.6 | 73%.3 |
| Decision tree | 80.0 | 59.4 | 100 | 79.7 | 74.5% |
| Random forest | 81.3 | 70.3 | 84.4 | 81.2 | 76.7% |
4. Conclusion
The main aim of the system is to predict Alzheimer's disease. For predicting Alzheimer's disease or Dementia in adult patients, the “MRI and Alzheimer's” dataset has been used, which has been provided by the Open Access Series of Imaging Studies (OASIS) project. The dataset has been visualized and filled in the missing values. Data has been preprocessed by removing some unnecessary features. The values were standardized to make sure that they easily fit in the ML models. Then the dataset has been used to train SVM, logistic regression, decision tree, and random forest models. For evaluation metrics, accuracy, recall, AUC, and confusion matrix have been used. To improve the system result, the grid search method has been used to fine-tune all developed models. For this particular dataset, the system got the best result using SVM. A more complex model like the random forest classifier suffered from an overfitting issue. For deployment, the SVM model has been used for the best results among all the models. In the future, the system models could be improved by using a larger dataset and more ML models such as AdaBoost, KNN, Majority Voting, and Bagging. This will increase reliability and enhance the performance of the system. The ML system can help the general public get an idea about the possibility of Dementia in adult patients by simply inputting MRI data. Hopefully, it will help patients to get early treatment for Dementia and improve their life.
Acknowledgments
The authors would like to acknowledge the support from Taif University Researchers Supporting Project (no. TURSP-2020/73), Taif University, Taif, Saudi Arabia.
Data Availability
The data used to support the findings of this study are freely available at https://www.kaggle.com/jboysen/mri-and-alzheimers?select=oasis_longitudinal.csv.
Conflicts of Interest
The authors declare that they have no conflicts of interest to report regarding the present study.
References
- 1.Simon A., Deo M., Selvam V., Babu R. An overview of machine learning and its applications. International Journal of Electrical Sciences & Engineering. 2016;1:22–24. [Google Scholar]
- 2.Alzubi J., Nayyar A., Kumar A. Machine learning from theory to algorithms: an overview. Journal of Physics: Conference Series. 2018;1142 doi: 10.1088/1742-6596/1142/1/012012.012012 [DOI] [Google Scholar]
- 3.Çelik Ö. A research on machine learning methods and its applications. Journal of Educational Technology and Online Learning. 2018;1 doi: 10.31681/jetol.457046. [DOI] [Google Scholar]
- 4.Attaran M., Deb P. Machine learning: the new “big thing” for competitive advantage. International Journal of Knowledge Engineering and Data Mining. 2018;5(4):277–305. doi: 10.1504/ijkedm.2018.095523. [DOI] [Google Scholar]
- 5.Schmidt J., Marques M., Botti S., Marques M. Recent advances and applications of machine learning in solid-state materials science. Npj Computational Materials. 2019;5(83) doi: 10.1038/s41524-019-0221-0. [DOI] [Google Scholar]
- 6.Masud M., Eldin Rashed A. E., Hossain M. S. Convolutional neural network-based models for diagnosis of breast cancer. Neural Computing and Applications. 2020 doi: 10.1007/s00521-020-05394-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hsu C. W., Lin C. J. A comparison of methods for multiclass support vector machines. IEEE Transactions on Neural Networks. 2002;13(2):415–425. doi: 10.1109/72.991427. [DOI] [PubMed] [Google Scholar]
- 8.Peng C.-Y. J., Lee K. L., Ingersoll G. M. An introduction to logistic regression analysis and reporting. The Journal of Educational Research. 2002;96(1):3–14. doi: 10.1080/00220670209598786. [DOI] [Google Scholar]
- 9.Boateng E. Y., Abaye D. A. A review of the logistic regression model with emphasis on medical research. Journal of Data Analysis and Information Processing. 2019;7(4):190–207. doi: 10.4236/jdaip.2019.74012. [DOI] [Google Scholar]
- 10.Wang L.-M., Li X.-L., Cao C.-H., Yuan S.-M. Combining decision tree and Naive Bayes for classification. Knowledge-Based Systems. 2006;19(7):511–515. doi: 10.1016/j.knosys.2005.10.013. [DOI] [Google Scholar]
- 11.Aitkenhead M. J. A co-evolving decision tree classification method. Expert Systems with Applications. 2008;34(1):18–25. doi: 10.1016/j.eswa.2006.08.008. [DOI] [Google Scholar]
- 12.Patel H. H., Prajapati P. Study and analysis of decision tree based classification algorithms. International Journal of Computer Science and Engineering. 2018;6(10):74–78. doi: 10.26438/ijcse/v6i10.7478. [DOI] [Google Scholar]
- 13.Biau G. Analysis of a random forests model. Journal of Machine Learning Research. 2012;13:1063–1095. [Google Scholar]
- 14.Ali J., Khan R., Ahmad N., Maqsood I. Random forests and decision trees. International Journal of Computer Science Issues (IJCSI) 2012;9 [Google Scholar]
- 15.Chen W., Xie X., Wang J., et al. A comparative study of logistic model tree, random forest, and classification and regression tree models for spatial prediction of landslide susceptibility. Catena. 2017;151(1):147–160. doi: 10.1016/j.catena.2016.11.032. [DOI] [Google Scholar]
- 16.Tayal A., Gupta J., Solanki A., et al. DL-CNN-based approach with image processing techniques for diagnosis of retinal diseases. Multimedia Systems. 2021 doi: 10.1007/s00530-021-00769-7. [DOI] [Google Scholar]
- 17.Masud M., Sikder N., Nahid A.-A., Bairagi A. K., AlZain M. A. A machine learning approach to diagnosing lung and colon cancer using a deep learning-based classification framework. Sensors. 2021;21(3):p. 748. doi: 10.3390/s21030748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Masud M., Alhumyani H., Alshamrani S. S., et al. Leveraging deep learning techniques for malaria parasite detection using mobile application. Wireless Communications and Mobile Computing. 2020;2020:15. doi: 10.1155/2020/8895429.8895429 [DOI] [Google Scholar]
- 19.Masud M., Kumar Bairagi A., Al Nahid A., et al. A pneumonia diagnosis scheme based on hybrid features extracted from chest radiographs using an ensemble learning algorithm. Journal of Healthcare Engineering. 2021;2021:11. doi: 10.1155/2021/8862089.8862089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fiest K. M., Roberts J. I., Maxwell C. J., et al. The prevalence and incidence of dementia due to alzheimer’s disease: a systematic review and meta-analysis. The Canadian Journal of Neurological Sciences/Journal Canadien des Sciences Neurologiques. 2016;43(S1):S51–S82. doi: 10.1017/cjn.2016.36. [DOI] [PubMed] [Google Scholar]
- 21.Rubenstein E., Hartley S., Bishop L. Epidemiology of dementia and alzheimer disease in individuals with down syndrome. JAMA Neurology. 2020;77(2):p. 262. doi: 10.1001/jamaneurol.2019.3666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Brookmeyer R., Johnson E., Ziegler-Graham K., Arrighi H. M. Forecasting the global burden of Alzheimer’s disease. Alzheimer’s and Dementia. 2007;3(3):186–191. doi: 10.1016/j.jalz.2007.04.381. [DOI] [PubMed] [Google Scholar]
- 23.Reitz C., Brayne C., Mayeux R. Epidemiology of alzheimer disease. Nature Reviews Neurology. 2011;7(3):137–152. doi: 10.1038/nrneurol.2011.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sims I. M. 2009 Alzheimer’s disease facts and figures. Alzheimer’s and Dementia. 2009;5(3):234–270. doi: 10.1016/j.jalz.2009.03.001. [DOI] [PubMed] [Google Scholar]
- 25.Mendez M. F., Underwood K. L., Zander B. A., Mastri A. R., Sung J. H., Frey W. H. Risk factors in Alzheimer’s disease: a clinicopathologic study. Neurology. 1992;42(4):p. 770. doi: 10.1212/WNL.42.4.770. [DOI] [PubMed] [Google Scholar]
- 26.International A. D., Wimo A., Ali G. C., et al. World Alzheimer Report 2015. London, UK: Alzheimer’s Disease International (ADI); 2015. https://www.alzint.org/resource/world-alzheimer-report-2015/ [Google Scholar]
- 27.International A. D. ADI-Dementia Statistics. London, UK: Alzheimer’s Disease International (ADI); 2015. https://www.alzint.org/about/dementia-facts-figures/dementia-statistics/ [Google Scholar]
- 28.Prince M., Bryce R., Albanese E., Wimo A., Ribeiro W., Ferri C. P. The global prevalence of dementia: a systematic review and metaanalysis. Alzheimer’s and Dementia. 2013;9(1):63–75. doi: 10.1016/j.jalz.2012.11.007. [DOI] [PubMed] [Google Scholar]
- 29.Livingston G., Sommerlad A., Orgeta V., et al. Dementia prevention, intervention, and care. The Lancet. 2017;390(10113):2673–2734. doi: 10.1016/S0140-6736(17)31363-6. [DOI] [PubMed] [Google Scholar]
- 30.Wu Y. T., Beiser A., Breteler M. M. B., et al. The changing prevalence and incidence of dementia over time-current evidence. Nature Reviews Neurology. 2017;13(6):327–339. doi: 10.1038/nrneurol.2017.63. [DOI] [PubMed] [Google Scholar]
- 31.Etters L., Goodall D., Harrison B. Caregiver burden among dementia patient caregivers: a review of the literature. Journal of the American Academy of Nurse Practitioners. 2008;20(8):423–428. doi: 10.1111/j.1745-7599.2008.00342.x. [DOI] [PubMed] [Google Scholar]
- 32.Roy N., Hassan A. M., Alom R., Rajib M. H. R., Mamun K. A. A. The situation of Alzheimer’s disease in Bangladesh: facilities, expertise, and awareness among general people. Journal of Neurological Disorders. 2020;8(7) [Google Scholar]
- 33.Taha D. S. World Alzheimer’s Day: Forgetting Dementia in Bangladesh. London, UK: Help Age International; 2014. https://www.helpage.org/blogs/dr-samnun-taha-23771/world-alzheimers-day-forgetting-dementia-in-bangladesh-770/ [Google Scholar]
- 34.Rahman A., Salam F., Islam M., et al. Alzheimer’s disease-an update. Bangladesh Journal of Neuroscience. 2013;28(1):52–58. doi: 10.3329/bjn.v28i1.17193. [DOI] [Google Scholar]
- 35.Rahman M. R., Tajmim A., Ali M., Sharif M. Overview and current status of Alzheimer’s disease in Bangladesh. Journal of Alzheimer’s Disease Reports. 2017;1(1):27–42. doi: 10.3233/adr-170012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kadir D. S. Chronicles of Alzheimer’s disease: a medicinal & therapeutic overview in Bangladeshi aspect. Journal of Pharmaceutical Research International. 2019;30(5):1–12. doi: 10.9734/jpri/2019/v30i530282. [DOI] [Google Scholar]
- 37.Kalaria R. N., Maestre G. E., Arizaga R., et al. Alzheimer’s disease and vascular dementia in developing countries: prevalence, management, and risk factors. The Lancet Neurology. 2008;7(9):812–826. doi: 10.1016/s1474-4422(08)70169-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bou M. C., Minguillón C., Gramunt N., Molinuevo J. L. Alzheimer’s disease prevention: from risk factors to early intervention. Alzheimer’s Research & Therapy. 2017;9:p. 71. doi: 10.1186/s13195-017-0297-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.The OASIS brains datasets. 2016, https://www.kaggle.com/jboysen/mri-and-alzheimers?select=oasis_longitudinal.csv.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used to support the findings of this study are freely available at https://www.kaggle.com/jboysen/mri-and-alzheimers?select=oasis_longitudinal.csv.