

Key Points
Question
What is the global prevalence of young-onset dementia?
Findings
In this systematic review, a total of 95 studies were included, of which 74 studies with 2 760 379 unique patients were included in the meta-analysis; the global age-standardized prevalence of young-onset dementia was 119.0 per 100 000 population aged 30 to 64 years. Estimates increased from 1.1 per 100 000 population aged 30 to 34 years to 77.4 per 100 000 population aged 60 to 64 years.
Meaning
These prevalence estimates show the importance of young-onset dementia worldwide; policy makers could use this information to organize sufficient health care for young people living with dementia.
Abstract
Importance
Reliable prevalence estimates are lacking for young-onset dementia (YOD), in which symptoms of dementia start before the age of 65 years. Such estimates are needed for policy makers to organize appropriate health care.
Objective
To determine the global prevalence of YOD.
Data Sources
The PubMed, Embase, CINAHL, and PsycInfo databases were systematically searched for population-based studies on the prevalence of YOD published between January 1, 1990, and March 31, 2020.
Study Selection
Studies containing data on the prevalence of dementia in individuals younger than 65 years were screened by 2 researchers for inclusion in a systematic review and meta-analysis.
Data Extraction and Synthesis
Prevalence estimates on 5-year age bands, from 30 to 34 years to 60 to 64 years, were extracted. Random-effects meta-analyses were conducted to pool prevalence estimates. Results were age standardized for the World Standard Population. Heterogeneity was assessed by subgroup analyses for sex, dementia subtype, study design, and economic status based on the World Bank classification and by meta-regression.
Main Outcomes and Measures
Prevalence estimates of YOD for 5-year age bands.
Results
A total of 95 unique studies were included in this systematic review, of which 74 with 2 760 379 unique patients were also included in 5-year age band meta-analyses. Studies were mostly conducted in Europe and in older groups in Asia, North America, and Oceania. Age-standardized prevalence estimates increased from 1.1 per 100 000 population in the group aged 30 to 34 years to 77.4 per 100 000 population in the group aged 60 to 64 years. This gives an overall global age-standardized prevalence of 119.0 per 100 000 population in the age range of 30 to 64 years, corresponding to 3.9 million people aged 30 to 64 years living with YOD in the world. Subgroup analyses showed prevalence between men and women to be similar (crude estimates for men, 216.5 per 100 000 population; for women, 293.1 per 100 000 population), whereas prevalence was lower in high-income countries (crude estimate, 663.9 per 100 000 population) compared with upper–middle-income (crude estimate, 1873.6 per 100 000 population) and lower–middle-income (crude estimate, 764.2 per 100 000 population) countries. Meta-regression showed that age range (P < .001), sample size (P < .001), and study methodology (P = .02) significantly influenced heterogeneity between studies.
Conclusions and Relevance
This systematic review and meta-analysis found an age-standardized prevalence of YOD of 119.0 per 100 000 population, although estimates of the prevalence in low-income countries and younger age ranges remain scarce. These results should help policy makers organize sufficient health care for this subgroup of individuals with dementia.
Study Registration
PROSPERO CRD42019119288
This systematic review and meta-analysis assesses the global prevalence of young-onset dementia.
Introduction
Young-onset dementia (YOD) refers to onset of dementia before the age of 65 years.1 Young-onset dementia affects partnerships, parenthood, social life, and occupational functioning2 and causes considerable caregiver burden and delayed access to appropriate care owing to misdiagnosis.3,4,5,6
Dementia is generally perceived as a condition that affects older adults, with prevalence estimates of late-onset dementia (LOD) increasing exponentially with age.7 Approximately 45 million people live with LOD worldwide.8 The focus on LOD may marginalize the importance of dementia in younger people.9 Exact figures on the burden of YOD are needed to determine the necessary budget and set priorities by policy makers.
Harvey et al10 and Ikejima et al11 have authored the most referenced studies on the prevalence of YOD, reporting estimates from 42.3 to 54.0 per 100 000 population. People with YOD were identified retrospectively with a register-based approach, so underreporting was likely. Three systematic reviews exist on the prevalence of YOD12,13,14; however, each included only a limited number of studies, concentrated on a specific diagnosis, or reviewed non–population-based studies.
Our primary goal was to assess the global prevalence of YOD using all available data on the prevalence of YOD. We also compared prevalence estimates between different subgroups of sex, age, causes, study design, and countries’ economic status.
Methods
Search Strategy and Selection Criteria
This systematic review and meta-analysis followed the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines.15 We searched literature in PubMed, Embase, CINAHL, and PsycInfo for observational population-based prospective, retrospective, or cross-sectional studies on the prevalence or incidence of YOD (eMethods 1 in the Supplement). Studies were searched from January 1, 1990, to March 31, 2020, without language restrictions. The study is part of the larger PRECODE (Prevalence Recognition and Care Pathways in Young Onset Dementia) project.
Studies were eligible for inclusion in the prevalence report if they included individuals younger than 65 years. Cohort studies on demographic subpopulations (eg, certain age ranges, women only, ethnic minority populations) and population-based hospital, primary care, and insurance registry studies were included. Cohort studies restricted to specific patient groups at risk for developing YOD (eg, patients with Down syndrome or HIV) or to residents of care homes were excluded. Dementia diagnosis had to be set according to accepted criteria (ie, International Classifications of Diseases and Diagnostic and Statistical Manual of Mental Disorders [Third Edition] to Diagnostic and Statistical Manual of Mental Disorders [Fifth Edition]) or its subtypes (ie, National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association [NINCDS-ADRDA], National Institute of Neurological Disorders and Stroke–Association Internationale pour la Recherche et l’Enseignement en Neuroscience [NINDS-AIREN]) or, in case criteria were not specified, studies had to report a diagnosis by a clinician. Studies relying on mortality data or death certificates were excluded because of expected misclassification bias due to underreporting.
Two researchers (S.H. and K.P.) independently screened both abstracts and eligible full texts. Disagreements were resolved by discussion, if needed, with a third researcher (S.K.). The Cohen κ for interrater agreement was substantial (0.67).16 For cohorts with multiple publications, we chose the most complete data set (ie, largest sample, most relevant age range). Reference lists of included articles and reviews were checked for additional studies. Authors were contacted at least twice in case of missing data or to verify eligibility for inclusion.
Statistical Analysis
One researcher (S.H.) extracted study characteristics and outcome estimates using a uniform data extraction sheet (eMethods 2 in the Supplement) with cross-checking by a second researcher (K.P.). We used the risk of bias tool for quality assessments (eMethods 3 in the Supplement).17 When checklist items were not reported or unclear, they were qualified as high risk.
Whenever possible, prevalence estimates were meta-analyzed using a generalized linear mixed-model random-effects meta-analysis (Metafor package in R, version 3.3.6 [R Program for Statistical Computing]).18 Studies that did not report both the number of cases and sample size or studies investigating specific subpopulations only (eg, ethnic minorities) were not included in the meta-analysis.
First, crude meta-analyses were performed for all types of dementia and the subtypes Alzheimer disease (AD), vascular dementia (VaD), and frontotemporal dementia (FTD). A study was considered as covering all types of dementia if it reported 1 overall prevalence estimate for all causes and subtypes of dementia.
Because studies included different age ranges, we estimated age-specific prevalence by 5-year age bands. Next, because pooling into a single estimate would apply the same weight to each age group, we age-standardized estimates by the World Standard Population of 2000 to 2025,19 the United States Standard Population of 2000,20 and the European Standard Population of 2011 to 202021 using direct standardization.
Subgroup analyses were performed based on sex, study methodology (cohort vs register-based studies), and economic status of countries. The latter was based on a country’s gross national income per capita following the World Bank classification22 (eTable 1 in the Supplement).
Meta-regression according to DerSimonian and Laird23 assessed the mitigation of between-study differences in sample size, age ranges, diagnostic criteria, economic status, and study methodology. Analyses were run for each covariate separately, followed by multivariable analyses of significant covariates.
Heterogeneity was assessed using the I2 statistic, showing the proportion of the total variance in pooled estimates that is explained by variation between studies. Funnel plots were visually inspected to account for small studies. P <.05 from 2-sided hypothesis testing was considered statistically significant in all analyses.
Results
We found 11 422 articles after removing duplicates, and 95 studies were eligible for inclusion (eFigure 1 in the Supplement),10,11,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116 for a total of 2 760 379 participants in the 5-year age band meta-analyses. The study characteristics are described in Table 1 and eTable 2 in the Supplement. The quality of the studies was adequate (Table 1 and eTable 2 in the Supplement), but studies differed on methodology and data reporting. External validity was deemed problematic in some studies in which the study population did not represent the target population or in which nonparticipation was high. Incomplete reporting also lowered quality assessments.
Table 1. Characteristics of the Included Studiesa.
| Characteristic | Dementia type | |||
|---|---|---|---|---|
| All (n = 81) | AD (n = 20) | VaD (n = 13) | FTD (n = 12) | |
| Study period | ||||
| Before 1990 | 4 | 0 | 0 | 0 |
| 1990-1999 | 12 | 8 | 5 | 2 |
| 2000-2009 | 27 | 6 | 4 | 6 |
| 2010-2019 | 19 | 3 | 2 | 3 |
| Unknown | 19 | 3 | 2 | 1 |
| Age range, y | ||||
| <30-64 | 7 | 2 | 1 | 2 |
| 30-64 | 3 | 3 | 3 | 4 |
| 40-59 | 1 | 1 | 0 | 0 |
| 40-64 | 6 | 1 | 1 | 1 |
| 45-64 | 3 | 0 | 0 | 0 |
| 50-59 | 7 | 3 | 1 | 5 |
| 50-64 | 6 | 1 | 1 | 0 |
| 55-64 | 9 | 4 | 3 | 0 |
| 60-64 | 39 | 5 | 3 | 0 |
| Sample size | ||||
| <500 | 26 | 1 | 0 | 0 |
| 500-1000 | 9 | 3 | 2 | 0 |
| 1000-2000 | 8 | 2 | 2 | 0 |
| >2000 | 27 | 14 | 9 | 12 |
| Unknownb | 11 | 0 | 0 | 0 |
| Diagnostic criteria | ||||
| ICD | 12 | 1 | 0 | 0 |
| DSM-III to DSM-5 | 43 | 9 | 6 | 4 |
| NINCDS-ARDRA | 1 | 3 | 0 | 0 |
| NINDS-AIREN | 0 | 0 | 1 | 0 |
| Combination of above | 15 | 7 | 6 | 3 |
| Otherc | 10 | 0 | 0 | 5 |
| Design | ||||
| Cohort | ||||
| Cross-sectional | 57 | 10 | 7 | 0 |
| Prospective | 3 | 0 | 0 | 0 |
| Register-based | 21 | 10 | 6 | 12 |
| Mean quality assessment (range)d | 8.1 (4-10) | 8.4 (8-10) | 8.0 (7-10) | 7.9 (7-9) |
| World Bank classification | ||||
| High-income | 46 | 10 | 7 | 12 |
| Upper–middle-income | 18 | 7 | 4 | 0 |
| Lower–middle-income | 16 | 3 | 2 | 0 |
| Low-income | 1 | 0 | 0 | 0 |
| Continent | ||||
| Europe | 27 | 8 | 5 | 9 |
| Asia | 33 | 9 | 5 | 2 |
| North America | 7 | 0 | 0 | 0 |
| South America | 6 | 1 | 1 | 0 |
| Africa | 4 | 1 | 1 | 0 |
| Oceania | 4 | 1 | 1 | 1 |
Abbreviations: AD, Alzheimer disease; DSM-III, Diagnostic and Statistical Manual of Mental Disorders (Third Edition); DSM-5, Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition); FTD, frontotemporal dementia; ICD, International Classification of Diseases; NINCDS-ADRDA, National Institute of Neurological and Communicative Disorders and Stroke–Alzheimer’s Disease and Related Disorders Association; NINDS-AIREN, National Institute of Neurological Disorders and Stroke–Association Internationale pour la Recherche et l’Enseignement en Neurosciences; VaD, vascular dementia.
Unless indicated otherwise, data are presented as number of studies. Studies may be reported multiple times if they are included in multiple meta-analyses (all types, AD, VaD, FTD).
Studies with unknown sample size (and number of cases) were not eligible for meta-analyses.
Other diagnostic criteria were subtype specific (eg, Neary and McKahnn criteria for FTD).
Scores range from 4 to 10, with higher scores indicating higher-quality assessment of the studies.
The Figure shows where the included studies were conducted. Although studies from many countries were included, information on ethnicity was insufficient. Studies in the age range of 30 to 59 years were mainly performed among White populations and only 5 were performed in Asian populations (1 in a population aged 30-49 years11 and 4 in populations aged 50-59 years46,59,65,108). Hence, no subgroup analyses on ethnicity could be performed.
Figure. World Map of Included Studies.
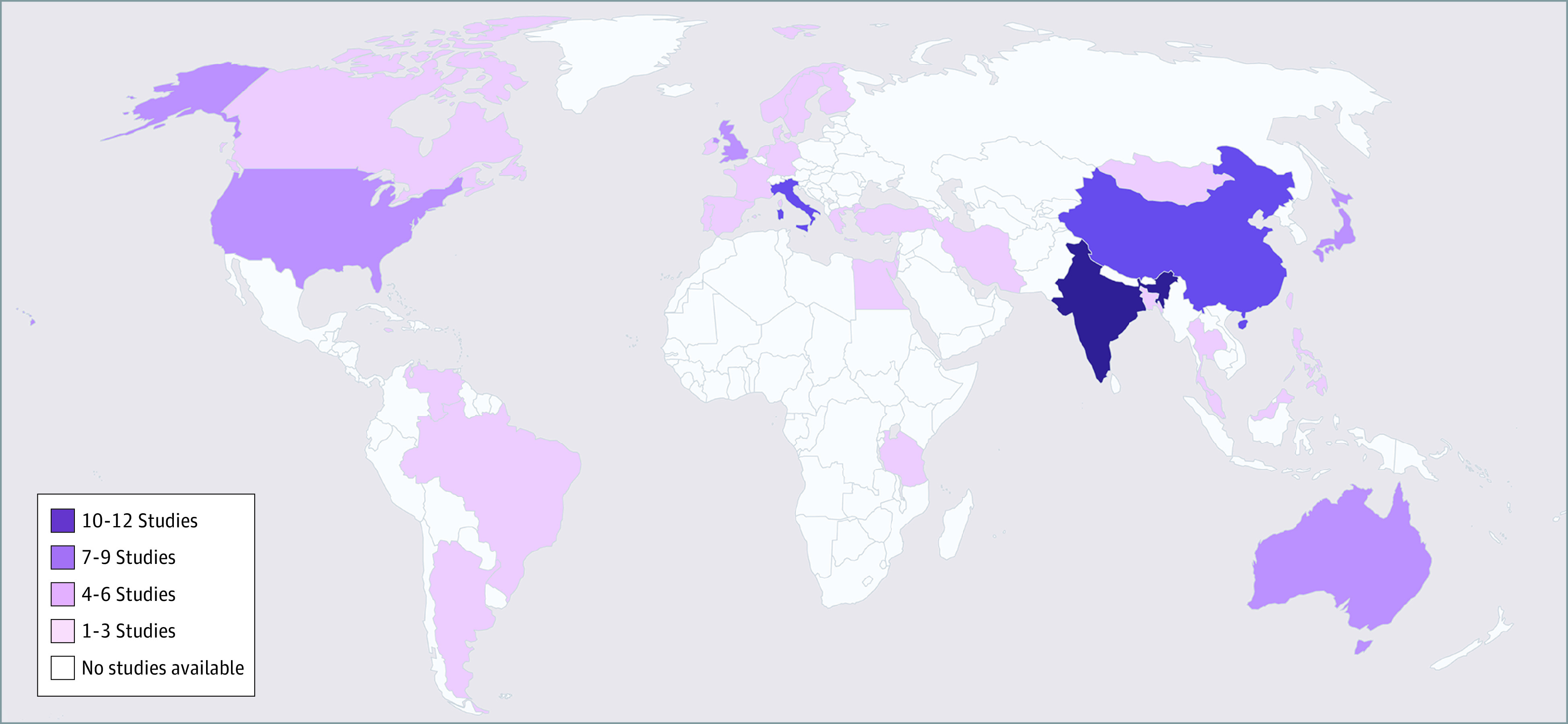
Of the studies excluded from the meta-analysis, several investigated specific ethnic subpopulations. Smith et al,60 Radford et al,97 and Li et al87 investigated Australian Indigenous people, in whom prevalence was higher compared with the non-Indigenous population. Raina et al,58,69 Parlevliet et al,103 and Nielsen et al74 investigated ethnic minority groups in different countries and found higher prevalence compared with the general population. Liu et al,31 Bartoloni et al,83 and Phanthumchinda et al26 reported a higher prevalence in people with a low socioeconomic status or poor housing conditions.
Overall Prevalence of YOD
Eighty-one studies10,11,24,25,26,27,28,29,31,32,33,34,35,36,37,38,39,40,42,43,45,46,47,50,52,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,74,75,76,78,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,97,98,99,100,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116 reported prevalence estimates on all types of YOD (Table 1). Of these, 21 studies were excluded from meta-analyses: 11 studies26,31,58,60,69,74,83,84,87,97,103 reported solely on specific ethnic subpopulations, and 10 studies35,45,54,88,91,104,105,107,116 lacked numerator or denominator data. The number of eligible studies ranged from 4 in the age band 30 to 34 years10,11,93,113 to 45 in the age band 60 to 64 years.10,11,24,25,27,33,34,37,39,42,43,46,50,56,57,59,62,63,65,66,67,70,71,75,78,80,82,85,92,93,94,95,98,99,106,108,109,110,111,113,115 Pooled analyses within 5-year age bands showed an increased prevalence with age (eFigure 2 in the Supplement and Table 2). Age-standardized prevalence estimates increased from 1.1 per 100 000 population in the group aged 30 to 34 years to 77.4 per 100 000 population in the group aged 60 to 64 years. The global age-standardized prevalence was 119.0 per 100 000 population in the maximum age span of 30 to 64 years, 159.4 per 100 000 population in Europe, and 114.7 per 100 000 population in the US. This corresponds to an absolute number of 3.9 million people living with YOD worldwide, of whom 0.5 million live in Europe and 200 000 live in the US.
Table 2. Age-Standardized Prevalence Estimates for 5-Year Age Bands per 100 000 Population.
| Age range, ya | Dementia type | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | AD | VaD | FTD | |||||||||
| WSP | ESP | USP | WSP | ESP | USP | WSP | ESP | USP | WSP | ESP | USP | |
| 30-34 | 1.1 | 0.8 | 0.9 | NA | NA | NA | 0.2 | 0.2 | 0.2 | 0.02 | 0.01 | 0.02 |
| 35-39 | 1.0 | 0.9 | 1.1 | 0.1 | 0.1 | 0.1 | 0.6 | 0.5 | 0.6 | 0.02 | 0.01 | 0.02 |
| 40-44 | 3.8 | 3.5 | 4.3 | 0.1 | 0.1 | 0.1 | 0.8 | 0.73 | 0.9 | 0.1 | 0.04 | 0.1 |
| 45-49 | 6.3 | 6.4 | 6.8 | 0.1 | 0.1 | 0.1 | 0.4 | 0.4 | 0.5 | 0.3 | 0.3 | 0.3 |
| 50-54 | 10.0 | 11.1 | 10.6 | 1.5 | 1.7 | 1.6 | 1.1 | 1.3 | 1.2 | 0.2 | 0.3 | 0.3 |
| 55-59 | 19.2 | 24.3 | 18.5 | 6.9 | 8.8 | 6.7 | 2.9 | 3.6 | 2.7 | 1.0 | 1.3 | 1.0 |
| 60-64 | 77.4 | 112.4 | 72.6 | 24.8 | 36.0 | 23.3 | 8.9 | 12.9 | 8.3 | 0.7 | 1.0 | 0.6 |
| All | 119.0 | 159.4 | 114.7 | 41.1 | 54.1 | 31.8 | 14.9 | 19.5 | 14.3 | 2.3 | 2.9 | 2.3 |
Abbreviations: AD, Alzheimer disease; ESP, European Standard Population; FTD, frontotemporal dementia; USP, United States Standard Population; VaD, vascular dementia; WSP, World Standard Population.
For AD, the total is in the age range 35 to 64 years; for all other types of dementia, the total is in the age range 30 to 64 years.
Heterogeneity between studies was substantial (I2 > 90%). Subgroup analyses were performed by sex, World Bank classification, and study methodology (eTable 3 in the Supplement). For sex, data were available for 5-year age bands from 50 years onward, showing generally a similar prevalence for men and women (eg, for 50-54 years, 67.2 vs 81.2 per 100 000 population). For analyses based on World Bank classification, data from high-income countries were available for all age ranges, from upper–middle-income countries for 60 to 64 years of age, and from lower–middle-income countries for 50 to 64 years of age. No data were available for low-income countries. In the age band of 60 to 64 years, prevalence was highest in upper–middle-income countries (1873.6 per 100 000 population), followed by lower–middle-income countries (764.2 per 100 000 population) and high-income countries (663.9 per 100 000 population). Regarding study methodology, register-based studies were conducted across all age ranges, whereas cohort studies were only conducted for groups aged 50 to 64 years. Comparing the prevalence estimates in these later age bands, cohort studies reported higher prevalences (eg, 60-64 years, 1135.5 vs 302.1 per 100 000 population).
Both univariable and multivariable meta-regression were performed on crude estimates (Table 3). In multivariable meta-regression, age range, sample size, and study methodology significantly accounted for between-study differences in prevalence estimates, with an R2 of 85.9%. Prevalence estimates increased for studies with a higher mean age and studies with a smaller sample size.
Table 3. Meta-Regression Analysis of Study Characteristics in Univariable (Crude) and Multivariable Analyses and Interactions Between Characteristics.
| Crude analysis | Multivariable analysis | |||
|---|---|---|---|---|
| Coefficient (95% CI) | P value | Coefficient (95% CI) | P value | |
| Age range, y | ||||
| <30-64 | 1 [Reference] | NA | 1 [Reference] | NA |
| 30-64 | 0.3 (−0.5 to 1.1) | .43 | 0.2 (−0.5 to 0.8) | .63 |
| 40-64 | 1.6 (0.7 to 2.5) | <.001 | 1.3 (0.5 to 2.1) | .001 |
| 45-64 | 1.4 (0.7 to 2.1) | <.001 | 1.2 (0.7 to 1.8) | <.001 |
| 50-64 | 1.6 (0.7 to 2.4) | <.001 | 1.9 (1.1 to 2.8) | <.001 |
| 55-64 | 2.6 (1.9 to 3.2) | <.001 | 1.9 (1.1 to 2.7) | <.001 |
| 60-64 | 3.5 (2.9 to 4.1) | <.001 | 2.3 (1.6 to 3.0) | <.001 |
| Sample size | ||||
| 0-499 | 1 [Reference] | NA | 1 [Reference] | NA |
| 500-999 | −0.3 (−1.4 to 0.7) | .56 | −0.3 (−0.8 to 0.3) | .35 |
| 1000-1999 | 0.5 (−0.5 to 1.4) | .34 | 0.4 (−0.1 to 0.9) | .09 |
| 2000-4999 | −1.6 (−2.7 to −0.6) | .002 | −1.4 (−2.1 to −0.8) | <.001 |
| ≥5000 | −2.4 (−3.2 to −1.6) | <.001 | −2.0 (−2.8 to −1.2) | <.001 |
| Study methodology | ||||
| Cohort | 1 [Reference] | NA | 1 [Reference] | NA |
| Register-based | −1.9 (−2.6 to −1.1) | <.001 | 0.9 (0.2 to 1.5) | .02 |
| Diagnostic criteria | ||||
| Other | 1 [Reference] | NA | NA | NA |
| ICD | −1.2 (−2.9 to 0.5) | .15 | NA | NA |
Abbreviations: ICD, International Classification of Diseases; NA, not applicable.
Alzheimer Disease
Twenty studies10,11,30,33,37,41,44,47,51,53,55,72,73,81,85,93,95,101,108,113 reported on the prevalence of AD. The number of studies eligible for meta-analyses ranged from 3 (age group, 35-39 years)11,93,113 to 14 (age group, 60-64 years)10,11,25,30,37,44,53,73,85,93,95,101,108,113 (eTable 3 in the Supplement). The age-standardized prevalence was 41.1 per 100 000 population worldwide, 54.1 per 100 000 population in Europe, and 31.8 per 100 000 population in the US (Table 2). eTable 3 and the eResults in the Supplement show results of subgroup analyses by sex, World Bank Classification, and study methodology.
Vascular Dementia
All 13 studies on the prevalence of VaD10,11,33,37,40,47,51,55,85,93,95,108,113 were eligible for inclusion in the meta-analysis. The number of studies eligible for meta-analyses ranged from 3 (age group, 30-34 years)11,93,113 to 7 (age group, 60-64 years).10,11,37,85,93,95,108,113 The age-standardized prevalence of VaD was 14.9 per 100 000 population worldwide, 19.5 per 100 000 population in Europe, and 14.3 per 100 000 population in the US (Table 2). The results of subgroup analyses are presented in eTable 3 and the eResults in the Supplement.
Frontotemporal Dementia
All 12 studies on the prevalence of FTD10,11,40,47,48,49,72,77,79,93,96,113 were included in the meta-analysis. The number of studies eligible for meta-analyses ranged from 3 (age group, 30-34 years)11,49,93 to 5 (age group, 60-64 years).10,11,49,93,113 The age-standardized FTD prevalence for the group aged 30 to 64 years was 2.3 per 100 000 population worldwide, 2.9 per 100 000 population in Europe, and 2.3 per 100 000 population in the US (Table 2).
Other Types
Only 4 studies11,33,47,106 reported data on dementia with Lewy bodies and Parkinson disease dementia, but these studies were too diverse for pooling in a meta-analysis (eTable 4 in the Supplement). Three studies on alcohol-related dementia47,93,113 reported prevalence estimates from 4.9 to 16.3 per 100 000 for 30 to 64 years of age. All were conducted in high-income countries and used the register-based study design. No meta-analysis was conducted.
Discussion
Based on 95 population-based studies, the global age-standardized prevalence in individuals aged 30 to 64 years was 119.0 per 100 000 population. Using the United Nations world population of 2019,117 this projects to 3.9 million people aged 30 to 64 years living with YOD worldwide. Age-standardized prevalence was lower in the US than in Europe, similar in women and men, highest in upper–middle-income countries, and highest for AD, followed by VaD and FTD. Register-based studies reported lower prevalence estimates than cohort studies.
The observed prevalence is higher than earlier estimates from Harvey et al10 (54.0 per 100 000 population in 2003) and Ikejima et al11 (42.3 per 100 000 population in 2009). Both of these studies were retrospective register-based studies that reported lower estimates compared with the cohort studies in our meta-analysis and are therefore likely to be underestimations.
Analysis of 5-year age bands showed a large increase in prevalence in the group aged 60 to 64 years, except for FTD. Estimates for this age band are comparable with another systematic review by Prince et al,7 who reported on dementia prevalence for 60 years and older. They estimated 48.1 million people older than 60 years with dementia in 2020, when we estimated 3.9 million people had YOD. This neatly conceptualizes YOD prevalence in the overall dementia prevalence. Our findings fit the general observation that prevalence of dementia increases exponentially from 60 years of age onward. However, the sharp increase between groups aged 55 to 59 and 60 to 64 years could be partially explained by the scarcity of studies in younger bands and their reliance on register data. Therefore, the prevalence in the younger bands might be an underestimation. On the other hand, a clear definition of YOD is lacking, and our cutoff at 65 years of age remains arbitrary.1 Given the profound delay in diagnosis, with a mean delay of 4.4 years between initial symptoms and diagnosis,5,6 the true YOD prevalence is probably also higher in older bands. According to the World Alzheimer Report, only one-third to one-half of the people living with dementia receive a routine clinical diagnosis.118 Hence, the reported estimates should be seen as a lower boundary of the true YOD prevalence.
The overall prevalence in this review was highest for AD, followed by VaD and FTD. However, in the lower age ranges, until 50 years of age, VaD prevalence is highest, and FTD prevalence is higher than AD prevalence. However, these analyses were based on few studies, so interpreting these prevalence estimates with caution is warranted. We found a relatively low overall prevalence for FTD compared with the total YOD prevalence. However, all studies on FTD were register based and were conducted in high-income countries. Furthermore, FTD is frequently underdiagnosed or misdiagnosed.5,6 Because no pathological data were available, this is also most likely an underestimation. In addition, prevalence of FTD peaked at 55 to 59 years of age. Studies investigating FTD characteristics report the same peak at age of onset,119 probably owing to the high genetic component in this subtype of dementia at this age.120
The higher AD prevalence is in line with the findings of Harvey et al,10 although Ikejima et al11 found a higher prevalence of VaD followed by AD. Clinical diagnoses of subtypes of dementia are subject to a lack of precision, and they might not always represent the pure AD or vascular pathology.121 Furthermore, the included studies differed with regard to study protocols and diagnostic criteria for AD and VaD. Because diagnosing dementia subtypes depends on diagnostic criteria, available measurement tools, and clinician expertise, no certainty about the subtypes can be applied without pathological information.
For this review, only the subtypes AD, VaD, and FTD had sufficient data to be analyzed separately. However, to better understand the prevalence, health care needs, and underlying causes of YOD, research on all subtypes of YOD is needed.
Although there were interstudy differences in prevalence for men and women, we observed similar prevalence for both sexes. For dementia subtypes, we only had sufficient information on AD, again finding similar prevalence estimates. More research on putative sex differences in the prevalence of YOD subtypes is still necessary.
We age standardized for the World Standard Population, European Standard Population, and United States Standard Population. The reported difference in prevalence estimates among them is owing to a difference in the age structure of the populations, rather than a difference in the risk of YOD. Because the prevalence of YOD increases with age, prevalence of YOD is higher in the older European Standard Population than the younger World Standard Population and United States Standard Population. Unfortunately, we lacked data for age standardization for other parts of the world.
Heterogeneity between studies was high, with many subgroup analyses showing I2 > 90%. Previous systematic reviews on prevalence studies found similar results.122 In addition, research has shown an association between high sample sizes and increased I2 heterogeneity, because study-specific confidence intervals become very narrow.123 Hence, it should not be seen as an absolute measure of heterogeneity. Meta-regression showed heterogeneity in prevalence estimates was partly explained by variability in included age ranges, sample sizes, and study methodology. Several differences between study designs might explain this heterogeneity. Population-based cohort studies adopt an active case finding with standardized protocols, leading to more accurate case finding; however, such studies are expensive and time consuming. Therefore, sample sizes of these studies are often relatively small, making them less suitable for studying rare diseases, such as YOD. Register-based studies are a cost-effective alternative but use passive case finding and are prone to misclassification bias and underreporting by relying on routine data (eg, primary, secondary, or tertiary care, insurance claims, or death certificates).124,125 However, the register-based studies in this review included young age bands and rarer causes of dementia. This can therefore be considered a strength of these register-based studies for prevalence estimates.126 We found no cohort studies reporting prevalence of dementia younger than 50 years; therefore, evidence of YOD prevalence in lower age ranges is based solely on register-based studies.
Finally, studies from high-income countries reported a lower prevalence, but they were more often register-based studies compared with studies from upper–middle- and lower–middle-income countries. Because insufficient data on ethnicity were available, we were unable to study ethnic differences. Future research is therefore needed to focus on possible differences in YOD prevalence between ethnic groups.
Strengths and Limitations
There are considerable strengths to this study. First, our inclusive search strategy without language restrictions led to the inclusion of 95 eligible articles, resulting in the largest review in this field, to our knowledge. More than 100 researchers were contacted to provide data for the meta-analysis. Nevertheless, not all requested data were available to us. Furthermore, in the meta-analyses, we did not pool across all age ranges in a single step. This would lead to an overestimation, given the overrepresentation of the later age ranges, especially 60 to 64 years of age. Therefore, we used 5-year age bands and direct standardization, leading to overall prevalence estimates for 30 to 64 years of age.
This study has some limitations that should be addressed in future studies. Studies from Africa and low-income countries were underrepresented; therefore, their estimates are lacking. In addition, 41 of the 95 included studies only reported on the age band 60 to 64 years. Consequently, crude prevalence estimates are most likely biased upward. Estimates of the 5-year age bands resulted in more conservative estimates, but fewer articles could be included in these analyses owing to a lack of information. Ideally, future studies on the prevalence of dementia will cover the full adult age range. In addition, meta-regression was only possible on the crude estimates because not all studies reported age-specific prevalence estimates.
In the meta-analyses of 5-year age bands, some of the sample sizes were small. However, post hoc analyses restricted to larger studies showed only slight changes in prevalence estimates in the 60- to 64-year age band. All studies were included because the studies with smaller sample sizes were often cohort studies, which are more accurate than register-based studies when investigating prevalence.
Subgroup analyses based on the World Bank classification were performed because analyses on ethnicity were not possible. The classification was chosen because it correlated with a given country’s quality of life measures, including educational level and mortality rates.127
Because YOD prevalence was not the main focus of most studies but was integrated into studies of total dementia prevalence, this led to reporting often being suboptimal for the purpose of this review (eg, no prevalence by sex and age ranges). Other between-study differences related to information sources (eg, primary care or hospital registers), methods for case ascertainment, and diagnostic criteria. Dementia diagnosis was sometimes poorly defined and not always reported properly.
In addition, the meta-analyses were performed on proportions. Because the prevalence was often near zero, data were transformed with generalized linear mixed models based on the logit transformation, because this eliminates misleading results that can occur when using other popular methods such as Freeman-Tukey double arcsine or normal logit transformation.128
Conclusions
In conclusion, monitoring the prevalence of YOD is essential to adequately plan and organize health services. Based on the available literature, this systematic review and meta-analysis estimated the age-standardized prevalence to be 119.0 per 100 000 population globally. Although this is higher than previously thought, it is probably an underestimation owing to lack of high-quality data. This should raise awareness for policy makers and health care professionals to organize more and better care for this subgroup of individuals with dementia. To yield more accurate and comparable prevalence estimates in the future, efforts should be made to conduct more cohort studies and to standardize procedures and reporting of prevalence studies. In addition, more data are needed from low-income countries as well as studies that include younger age ranges.
eMethods 1. Search Strategy for PubMed
eMethods 2. Data Extraction Sheet
eMethods 3. Quality Assessment Tool
eTable 1. World Bank Classification
eTable 2. Detailed Information on Studies Included in the Review
eTable 3. Results Data Analyses of Subgroups
eTable 4. Prevalence of Dementia With Lewy Bodies/Parkinson Disease Dementia in the 4 Eligible Studies
eFigure 1. Flowchart of Included and Excluded Studies
eFigure 2. Forest Plot 5-Year Age Bands for All-Type YOD
eResults. Subgroup Analyses Within Subtypes of Dementia
References
- 1.Koopmans R, Rosness T. Young onset dementia—what does the name imply? Int Psychogeriatr. 2014;26(12):1931-1933. doi: 10.1017/S1041610214001574 [DOI] [PubMed] [Google Scholar]
- 2.Jefferies K, Agrawal N. Early-onset dementia. Adv Psychiatr Treatment. 2009;15(5):380-388. doi: 10.1192/apt.bp.107.004572 [DOI] [Google Scholar]
- 3.van Vliet D, de Vugt ME, Bakker C, Koopmans RTCM, Verhey FRJ. Impact of early onset dementia on caregivers: a review. Int J Geriatr Psychiatry. 2010;25(11):1091-1100. doi: 10.1002/gps.2439 [DOI] [PubMed] [Google Scholar]
- 4.Mendez MF. The accurate diagnosis of early-onset dementia. Int J Psychiatry Med. 2006;36(4):401-412. doi: 10.2190/Q6J4-R143-P630-KW41 [DOI] [PubMed] [Google Scholar]
- 5.van Vliet D, de Vugt ME, Bakker C, et al. Time to diagnosis in young-onset dementia as compared with late-onset dementia. Psychol Med. 2013;43(2):423-432. doi: 10.1017/S0033291712001122 [DOI] [PubMed] [Google Scholar]
- 6.Draper B, Cations M, White F, et al. Time to diagnosis in young-onset dementia and its determinants: the INSPIRED study. Int J Geriatr Psychiatry. 2016;31(11):1217-1224. doi: 10.1002/gps.4430 [DOI] [PubMed] [Google Scholar]
- 7.Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP. The global prevalence of dementia: a systematic review and metaanalysis. Alzheimers Dement. 2013;9(1):63-75.e2. doi: 10.1016/j.jalz.2012.11.007 [DOI] [PubMed] [Google Scholar]
- 8.Nichols E, Szoeke CEI, Vollset SE, et al. ; GBD 2016 Dementia Collaborators . Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(1):88-106. doi: 10.1016/S1474-4422(18)30403-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rossor MN, Fox NC, Mummery CJ, Schott JM, Warren JD. The diagnosis of young-onset dementia. Lancet Neurol. 2010;9(8):793-806. doi: 10.1016/S1474-4422(10)70159-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Harvey RJ, Skelton-Robinson M, Rossor MN. The prevalence and causes of dementia in people under the age of 65 years. J Neurol Neurosurg Psychiatry. 2003;74(9):1206-1209. doi: 10.1136/jnnp.74.9.1206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ikejima C, Yasuno F, Mizukami K, Sasaki M, Tanimukai S, Asada T. Prevalence and causes of early-onset dementia in Japan: a population-based study. Stroke. 2009;40(8):2709-2714. doi: 10.1161/STROKEAHA.108.542308 [DOI] [PubMed] [Google Scholar]
- 12.Lambert MA, Bickel H, Prince M, et al. Estimating the burden of early onset dementia: systematic review of disease prevalence. Eur J Neurol. 2014;21(4):563-569. doi: 10.1111/ene.12325 [DOI] [PubMed] [Google Scholar]
- 13.Vieira RT, Caixeta L, Machado S, et al. Epidemiology of early-onset dementia: a review of the literature. Clin Pract Epidemiol Ment Health. 2013;9:88-95. doi: 10.2174/1745017901309010088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zhu X-C, Tan L, Wang H-F, et al. Rate of early onset Alzheimer’s disease: a systematic review and meta-analysis. Ann Transl Med. 2015;3(3):38. doi: 10.3978/j.issn.2305-5839.2015.01.19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting: Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012. doi: 10.1001/jama.283.15.2008 [DOI] [PubMed] [Google Scholar]
- 16.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. doi: 10.2307/2529310 [DOI] [PubMed] [Google Scholar]
- 17.Hoy D, Brooks P, Woolf A, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. 2012;65(9):934-939. doi: 10.1016/j.jclinepi.2011.11.014 [DOI] [PubMed] [Google Scholar]
- 18.Viechtbauer W.Conducting meta-analyses in R with the metafor package. J Stat Software. 2010;36(3):1-48. doi:10.18637/jss.v036.i03 doi: 10.18637/jss.v036.i03 [DOI] [Google Scholar]
- 19.Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. Age standardization of rates: a new WHO standard. GPE Discussion Paper Series No. 31. World Health Organization; 2001;9(10). Accessed May 21, 2020. https://www.who.int/healthinfo/paper31.pdf
- 20.Klein RJ, Schoenborn CA. Age adjustment using the 2000 projected US population. Healthy People 2000 Stat Notes.2001;(20):1-9. [PubMed] [Google Scholar]
- 21.Commission E.Revision of the European Standard Population—Report of Eurostat's Task Force 2013 edition. November 7, 2013. Accessed May 21, 2020. https://ec.europa.eu/eurostat/web/products-manuals-and-guidelines/-/KS-RA-13-028
- 22.World Bank . World Bank Country and Lending Groups 2020. 2019. Accessed March 6, 2020. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
- 23.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177-188. doi: 10.1016/0197-2456(86)90046-2 [DOI] [PubMed] [Google Scholar]
- 24.Rocca WA, Bonaiuto S, Lippi A, et al. Prevalence of clinically diagnosed Alzheimer’s disease and other dementing disorders: a door-to-door survey in Appignano, Macerata Province, Italy. Neurology. 1990;40(4):626-631. doi: 10.1212/WNL.40.4.626 [DOI] [PubMed] [Google Scholar]
- 25.Beard CM, Kokmen E, Offord K, Kurland LT. Is the prevalence of dementia changing? Neurology. 1991;41(12):1911-1914. doi: 10.1212/WNL.41.12.1911 [DOI] [PubMed] [Google Scholar]
- 26.Phanthumchinda K, Jitapunkul S, Sitthi-Amorn C, Bunnag SC. Prevalence of dementia in an urban slum population in Thailand: validity of screening methods. Int J Geriatr Psychiatry. 1991;6(9):639-46. doi: 10.1002/gps.930060905 [DOI] [Google Scholar]
- 27.Bachman DL, Wolf PA, Linn R, et al. Prevalence of dementia and probable senile dementia of the Alzheimer type in the Framingham study. Neurology. 1992;42(1):115-119. doi: 10.1212/WNL.42.1.115 [DOI] [PubMed] [Google Scholar]
- 28.Corso EA, Campo G, Triglio A, Napoli A, Reggio A, Lanaia F. Prevalence of moderate and severe Alzheimer dementia and multi-infarct dementia in the population of southeastern Sicily. Ital J Neurol Sci. 1992;13(3):215-219. doi: 10.1007/BF02224392 [DOI] [PubMed] [Google Scholar]
- 29.Coria F, Gomez de Caso JA, Minguez L, Rodriguez-Artalejo F, Claveria LE. Prevalence of age-associated memory impairment and dementia in a rural community. J Neurol Neurosurg Psychiatry. 1993;56(9):973-976. doi: 10.1136/jnnp.56.9.973 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Newens AJ, Forster DP, Kay DW, Kirkup W, Bates D, Edwardson J. Clinically diagnosed presenile dementia of the Alzheimer type in the Northern Health Region: ascertainment, prevalence, incidence and survival. Psychol Med. 1993;23(3):631-644. doi: 10.1017/S0033291700025411 [DOI] [PubMed] [Google Scholar]
- 31.Liu HC, Chou P, Lin KN, et al. Assessing cognitive abilities and dementia in a predominantly illiterate population of older individuals in Kinmen. Psychol Med. 1994;24(3):763-770. doi: 10.1017/S0033291700027914 [DOI] [PubMed] [Google Scholar]
- 32.Liu HC, Lin KN, Teng EL, et al. Prevalence and subtypes of dementia in Taiwan: a community survey of 5297 individuals. J Am Geriatr Soc. 1995;43(2):144-149. doi: 10.1111/j.1532-5415.1995.tb06379.x [DOI] [PubMed] [Google Scholar]
- 33.Ott A, Breteler MM, van Harskamp F, et al. Prevalence of Alzheimer’s disease and vascular dementia: association with education: the Rotterdam study. BMJ. 1995;310(6985):970-973. doi: 10.1136/bmj.310.6985.970 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Shaji S, Promodu K, Abraham T, Roy KJ, Verghese A. An epidemiological study of dementia in a rural community in Kerala, India. Br J Psychiatry. 1996;168(6):745-749. doi: 10.1192/bjp.168.6.745 [DOI] [PubMed] [Google Scholar]
- 35.Perkins P, Annegers JF, Doody RS, Cooke N, Aday L, Vernon SW. Incidence and prevalence of dementia in a multiethnic cohort of municipal retirees. Neurology. 1997;49(1):44-50. doi: 10.1212/WNL.49.1.44 [DOI] [PubMed] [Google Scholar]
- 36.Chandra V, Ganguli M, Pandav R, Johnston J, Belle S, DeKosky ST. Prevalence of Alzheimer’s disease and other dementias in rural India: the Indo-US study. Neurology. 1998;51(4):1000-1008. doi: 10.1212/WNL.51.4.1000 [DOI] [PubMed] [Google Scholar]
- 37.Farrag A, Farwiz HM, Khedr EH, Mahfouz RM, Omran SM. Prevalence of Alzheimer’s disease and other dementing disorders: Assiut–Upper Egypt study. Dement Geriatr Cogn Disord. 1998;9(6):323-328. doi: 10.1159/000017084 [DOI] [PubMed] [Google Scholar]
- 38.Freyne A, Kidd N, Lawlor BA. Early onset dementia: a catchment area study of prevalence and clinical characteristics. Ir J Psychol Med. 1998;15(3):87-90. doi: 10.1017/S079096670000374830308757 [DOI] [Google Scholar]
- 39.Urakami K, Adachi Y, Wakutani Y, et al. Epidemiologic and genetic studies of dementia of the Alzheimer type in Japan. Dement Geriatr Cogn Disord. 1998;9(5):294-298. doi: 10.1159/000017074 [DOI] [PubMed] [Google Scholar]
- 40.Andreasen N, Blennow K, Sjödin C, Winblad B, Svärdsudd K. Prevalence and incidence of clinically diagnosed memory impairments in a geographically defined general population in Sweden: the Piteå Dementia Project. Neuroepidemiology. 1999;18(3):144-155. doi: 10.1159/000026206 [DOI] [PubMed] [Google Scholar]
- 41.Campion D, Dumanchin C, Hannequin D, et al. Early-onset autosomal dominant Alzheimer disease: prevalence, genetic heterogeneity, and mutation spectrum. Am J Hum Genet. 1999;65(3):664-670. doi: 10.1086/302553 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hatada K, Okazaki Y, Yoshitake K, Takada K, Nakane Y. Further evidence of westernization of dementia prevalence in Nagasaki, Japan, and family recognition. Int Psychogeriatr. 1999;11(2):123-138. doi: 10.1017/S1041610299005682 [DOI] [PubMed] [Google Scholar]
- 43.Wang W, Wu S, Cheng X, et al. Prevalence of Alzheimer’s disease and other dementing disorders in an urban community of Beijing, China. Neuroepidemiology. 2000;19(4):194-200. doi: 10.1159/000026255 [DOI] [PubMed] [Google Scholar]
- 44.Bowirrat A, Treves TA, Friedland RP, Korczyn AD. Prevalence of Alzheimer’s type dementia in an elderly Arab population. Eur J Neurol. 2001;8(2):119-123. doi: 10.1046/j.1468-1331.2001.00183.x [DOI] [PubMed] [Google Scholar]
- 45.Jitapunkul S, Kunanusont C, Phoolcharoen W, Suriyawongpaisal P. Prevalence estimation of dementia among Thai elderly: a national survey. J Med Assoc Thai. 2001;84(4):461-467. [PubMed] [Google Scholar]
- 46.Vas CJ, Pinto C, Panikker D, et al. Prevalence of dementia in an urban Indian population. Int Psychogeriatr. 2001;13(4):439-450. doi: 10.1017/S1041610201007852 [DOI] [PubMed] [Google Scholar]
- 47.Ratnavalli E, Brayne C, Dawson K, Hodges JR. The prevalence of frontotemporal dementia. Neurology. 2002;58(11):1615-1621. doi: 10.1212/WNL.58.11.1615 [DOI] [PubMed] [Google Scholar]
- 48.Ibach B, Koch H, Koller M, Wolfersdorf M; Workgroup for Geriatric Psychiatry of the Psychiatric State Hospitals of Germany; Workgroup for Clinical Research of the Psychiatric State Hospitals of Germany . Hospital admission circumstances and prevalence of frontotemporal lobar degeneration: a multicenter psychiatric state hospital study in Germany. Dement Geriatr Cogn Disord. 2003;16(4):253-264. doi: 10.1159/000072810 [DOI] [PubMed] [Google Scholar]
- 49.Rosso SM, Donker Kaat L, Baks T, et al. Frontotemporal dementia in the Netherlands: patient characteristics and prevalence estimates from a population-based study. Brain. 2003;126(pt 9):2016-2022. doi: 10.1093/brain/awg204 [DOI] [PubMed] [Google Scholar]
- 50.De Ronchi D, Berardi D, Menchetti M, et al. Occurrence of cognitive impairment and dementia after the age of 60: a population-based study from Northern Italy. Dement Geriatr Cogn Disord. 2005;19(2-3):97-105. doi: 10.1159/000082660 [DOI] [PubMed] [Google Scholar]
- 51.Zhang ZX, Zahner GEP, Román GC, et al. Dementia subtypes in China: prevalence in Beijing, Xian, Shanghai, and Chengdu. Arch Neurol. 2005;62(3):447-453. doi: 10.1001/archneur.62.3.447 [DOI] [PubMed] [Google Scholar]
- 52.Das SK, Biswas A, Roy T, et al. A random sample survey for prevalence of major neurological disorders in Kolkata. Indian J Med Res. 2006;124(2):163-172. [PubMed] [Google Scholar]
- 53.Zhou DF, Wu CS, Qi H, et al. Prevalence of dementia in rural China: impact of age, gender and education. Acta Neurol Scand. 2006;114(4):273-280. doi: 10.1111/j.1600-0404.2006.00641.x [DOI] [PubMed] [Google Scholar]
- 54.Martens PJ, Fransoo R, Burland E, Burchill C, Prior HJ, Ekuma O; Need to Know Team . Prevalence of mental illness and its impact on the use of home care and nursing homes: a population-based study of older adults in Manitoba. Can J Psychiatry. 2007;52(9):581-590. doi: 10.1177/070674370705200906 [DOI] [PubMed] [Google Scholar]
- 55.Molero AE, Pino-Ramírez G, Maestre GE. High prevalence of dementia in a Caribbean population. Neuroepidemiology. 2007;29(1-2):107-112. doi: 10.1159/000109824 [DOI] [PubMed] [Google Scholar]
- 56.Banerjee TK, Mukherjee CS, Dutt A, Shekhar A, Hazra A. Cognitive dysfunction in an urban Indian population: some observations. Neuroepidemiology. 2008;31(2):109-114. doi: 10.1159/000146252 [DOI] [PubMed] [Google Scholar]
- 57.Bottino CMC, Azevedo D Jr, Tatsch M, et al. Estimate of dementia prevalence in a community sample from São Paulo, Brazil. Dement Geriatr Cogn Disord. 2008;26(4):291-299. doi: 10.1159/000161053 [DOI] [PubMed] [Google Scholar]
- 58.Raina S, Razdan S, Pandita KK, Raina S. Prevalence of dementia among Kashmiri migrants. Ann Indian Acad Neurol. 2008;11(2):106-108. doi: 10.4103/0972-2327.41878 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Sahadevan S, Saw SM, Gao W, et al. Ethnic differences in Singapore’s dementia prevalence: the Stroke, Parkinson’s Disease, Epilepsy, and Dementia in Singapore study. J Am Geriatr Soc. 2008;56(11):2061-2068. doi: 10.1111/j.1532-5415.2008.01992.x [DOI] [PubMed] [Google Scholar]
- 60.Smith K, Flicker L, Lautenschlager NT, et al. High prevalence of dementia and cognitive impairment in indigenous Australians. Neurology. 2008;71(19):1470-1473. doi: 10.1212/01.wnl.0000320508.11013.4f [DOI] [PubMed] [Google Scholar]
- 61.Wangtongkum S, Sucharitkul P, Silprasert N, Inthrachak R. Prevalence of dementia among population age over 45 years in Chiang Mai, Thailand. J Med Assoc Thai. 2008;91(11):1685-1690. [PubMed] [Google Scholar]
- 62.Arslantaş D, Ozbabalik D, Metintaş S, et al. Prevalence of dementia and associated risk factors in Middle Anatolia, Turkey. J Clin Neurosci. 2009;16(11):1455-1459. doi: 10.1016/j.jocn.2009.03.033 [DOI] [PubMed] [Google Scholar]
- 63.Spada RS, Stella G, Calabrese S, et al. Prevalence of dementia in mountainous village of Sicily. J Neurol Sci. 2009;283(1-2):62-65. doi: 10.1016/j.jns.2009.02.311 [DOI] [PubMed] [Google Scholar]
- 64.Ziegler U, Doblhammer G. Prevalence and incidence of dementia in Germany—a study based on data from the public sick funds in 2002. Article in German. Gesundheitswesen. 2009;71(5):281-290. doi: 10.1055/s-0028-1119384 [DOI] [PubMed] [Google Scholar]
- 65.Mathuranath PS, Cherian PJ, Mathew R, et al. Dementia in Kerala, South India: prevalence and influence of age, education and gender. Int J Geriatr Psychiatry. 2010;25(3):290-297. doi: 10.1002/gps.2338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Ng TP, Leong T, Chiam PC, Kua EH. Ethnic variations in dementia: the contributions of cardiovascular, psychosocial and neuropsychological factors. Dement Geriatr Cogn Disord. 2010;29(2):131-138. doi: 10.1159/000275668 [DOI] [PubMed] [Google Scholar]
- 67.Nunes B, Silva RD, Cruz VT, Roriz JM, Pais J, Silva MC. Prevalence and pattern of cognitive impairment in rural and urban populations from Northern Portugal. BMC Neurol. 2010;10:42. doi: 10.1186/1471-2377-10-42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Phung TK, Waltoft BL, Kessing LV, Mortensen PB, Waldemar G. Time trend in diagnosing dementia in secondary care. Dement Geriatr Cogn Disord. 2010;29(2):146-153. doi: 10.1159/000269933 [DOI] [PubMed] [Google Scholar]
- 69.Raina SK, Razdan S, Pandita KK. Prevalence of dementia in ethnic Dogra population of Jammu district, North India: a comparison survey. Neurol Asia. 2010;15(1):65-69. [Google Scholar]
- 70.Winblad I, Viramo P, Remes A, Manninen M, Jokelainen J.. Prevalence of dementia—a rising challenge among ageing populations. Eur Geriatr Med. 2010;1(6):330-333. doi: 10.1016/j.eurger.2010.10.002 [DOI] [Google Scholar]
- 71.Adelman S, Blanchard M, Rait G, Leavey G, Livingston G. Prevalence of dementia in African-Caribbean compared with UK-born White older people: two-stage cross-sectional study. Br J Psychiatry. 2011;199(2):119-125. doi: 10.1192/bjp.bp.110.086405 [DOI] [PubMed] [Google Scholar]
- 72.Borroni B, Alberici A, Grassi M, et al. Prevalence and demographic features of early-onset neurodegenerative dementia in Brescia County, Italy. Alzheimer Dis Assoc Disord. 2011;25(4):341-344. doi: 10.1097/WAD.0b013e3182147f80 [DOI] [PubMed] [Google Scholar]
- 73.Huriletemuer H, Wen S, Zhang C, et al. An epidemiological study of Alzheimer’s disease in elderly Mongolian and Han populations living in rural areas of Inner Mongolia. Aging Clin Exp Res. 2011;23(5-6):470-475. doi: 10.1007/BF03325243 [DOI] [PubMed] [Google Scholar]
- 74.Nielsen TR, Vogel A, Phung TK, Gade A, Waldemar G. Over- and under-diagnosis of dementia in ethnic minorities: a nationwide register-based study. Int J Geriatr Psychiatry. 2011;26(11):1128-1135. [DOI] [PubMed] [Google Scholar]
- 75.Bernardi L, Frangipane F, Smirne N, et al. Epidemiology and genetics of frontotemporal dementia: a door-to-door survey in southern Italy. Neurobiol Aging. 2012;33(12):2948.e1-2948.e10. doi: 10.1016/j.neurobiolaging.2012.06.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.El Tallawy HN, Farghly WMA, Shehata GA, et al. Prevalence of dementia in Al Kharga District, New Valley Governorate, Egypt. Neuroepidemiology. 2012;38(3):130-137. doi: 10.1159/000335655 [DOI] [PubMed] [Google Scholar]
- 77.Gilberti N, Turla M, Alberici A, et al. Prevalence of frontotemporal lobar degeneration in an isolated population: the Vallecamonica study. Neurol Sci. 2012;33(4):899-904. doi: 10.1007/s10072-011-0865-0 [DOI] [PubMed] [Google Scholar]
- 78.Lopes MA, Ferrioli E, Nakano EY, Litvoc J, Bottino CM. High prevalence of dementia in a community-based survey of older people from Brazil: association with intellectual activity rather than education. J Alzheimers Dis. 2012;32(2):307-316. doi: 10.3233/JAD-2012-120847 [DOI] [PubMed] [Google Scholar]
- 79.Wada-Isoe K, Ito S, Adachi T, et al. Epidemiological survey of frontotemporal lobar degeneration in Tottori prefecture, Japan. Dement Geriatr Cogn Dis Extra. 2012;2(1):381-386. doi: 10.1159/000342972 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Mayeda ER, Haan MN, Kanaya AM, Yaffe K, Neuhaus J. Type 2 diabetes and 10-year risk of dementia and cognitive impairment among older Mexican Americans. Diabetes Care. 2013;36(9):2600-2606. doi: 10.2337/dc12-2158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Nordström P, Nordström A, Eriksson M, Wahlund LO, Gustafson Y. Risk factors in late adolescence for young-onset dementia in men: a nationwide cohort study. JAMA Intern Med. 2013;173(17):1612-1618. doi: 10.1001/jamainternmed.2013.9079 [DOI] [PubMed] [Google Scholar]
- 82.Raina SK, Raina S, Chander V, Grover A, Singh S, Bhardwaj A. Identifying risk for dementia across populations: a study on the prevalence of dementia in tribal elderly population of Himalayan region in Northern India. Ann Indian Acad Neurol. 2013;16(4):640-644. doi: 10.4103/0972-2327.120494 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Bartoloni L, Blatt G, Insua I, et al. A population-based study of cognitive impairment in socially vulnerable adults in Argentina: the Matanza Riachuelo study preliminary results. Dement Neuropsychol. 2014;8(4):339-344. doi: 10.1590/S1980-57642014DN84000006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Bawih Inu P, Othman Z, Drahman I.. Dementia among Elderly Melanau: a community survey of an indigenous people in East Malaysia. Int Med J. 2014;21(5):468-471. [Google Scholar]
- 85.Ding D, Zhao Q, Guo Q, et al. The Shanghai Aging Study: study design, baseline characteristics, and prevalence of dementia. Neuroepidemiology. 2014;43(2):114-122. doi: 10.1159/000366163 [DOI] [PubMed] [Google Scholar]
- 86.El Tallawy HN, Farghly WM, Badry R, et al. Prevalence of dementia in Al-Quseir city, Red Sea Governorate, Egypt. Clin Interv Aging. 2014;9:9-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Li SQ, Guthridge SL, Eswara Aratchige P, et al. Dementia prevalence and incidence among the indigenous and non-indigenous populations of the Northern Territory. Med J Aust. 2014;200(8):465-469. doi: 10.5694/mja13.11052 [DOI] [PubMed] [Google Scholar]
- 88.Momtaz YA, Hamid TA, Ibrahim R. Gastritis may boost odds of dementia. Am J Alzheimers Dis Other Demen. 2014;29(5):452-456. doi: 10.1177/1533317513518654 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Neita SM, Abel WD, Eldemire-Shearer D, James K, Gibson RC. The prevalence and associated demographic factors of dementia from a cross-sectional community survey in Kingston, Jamaica. Int J Geriatr Psychiatry. 2014;29(1):103-105. doi: 10.1002/gps.3982 [DOI] [PubMed] [Google Scholar]
- 90.Nyberg J, Åberg MA, Schiöler L, et al. Cardiovascular and cognitive fitness at age 18 and risk of early-onset dementia. Brain. 2014;137(pt 5):1514-1523. doi: 10.1093/brain/awu041 [DOI] [PubMed] [Google Scholar]
- 91.Palmer K, Kabir ZN, Ahmed T, et al. Prevalence of dementia and factors associated with dementia in rural Bangladesh: data from a cross-sectional, population-based study. Int Psychogeriatr. 2014;26(11):1905-1915. doi: 10.1017/S1041610214001392 [DOI] [PubMed] [Google Scholar]
- 92.Raina SK, Raina S, Chander V, Grover A, Singh S, Bhardwaj A. Is dementia differentially distributed? a study on the prevalence of dementia in migrant, urban, rural, and tribal elderly population of Himalayan region in northern India. N Am J Med Sci. 2014;6(4):172-177. doi: 10.4103/1947-2714.131243 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Withall A, Draper B, Seeher K, Brodaty H. The prevalence and causes of younger onset dementia in Eastern Sydney, Australia. Int Psychogeriatr. 2014;26(12):1955-1965. doi: 10.1017/S1041610214001835 [DOI] [PubMed] [Google Scholar]
- 94.Heath CA, Mercer SW, Guthrie B. Vascular comorbidities in younger people with dementia: a cross-sectional population-based study of 616 245 middle-aged people in Scotland. J Neurol Neurosurg Psychiatry. 2015;86(9):959-964. doi: 10.1136/jnnp-2014-309033 [DOI] [PubMed] [Google Scholar]
- 95.Ji Y, Shi Z, Zhang Y, et al. Prevalence of dementia and main subtypes in rural northern China. Dement Geriatr Cogn Disord. 2015;39(5-6):294-302. doi: 10.1159/000375366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Luukkainen L, Bloigu R, Moilanen V, Remes AM. Epidemiology of frontotemporal lobar degeneration in northern Finland. Dement Geriatr Cogn Dis Extra. 2015;5(3):435-441. doi: 10.1159/000440858 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Radford K, Mack HA, Draper B, et al. Prevalence of dementia in urban and regional Aboriginal Australians. Alzheimers Dement. 2015;11(3):271-279. doi: 10.1016/j.jalz.2014.03.007 [DOI] [PubMed] [Google Scholar]
- 98.Subramaniam M, Chong SA, Vaingankar JA, et al. Prevalence of dementia in people aged 60 years and above: results from the WiSE Study. J Alzheimers Dis. 2015;45(4):1127-1138. doi: 10.3233/JAD-142769 [DOI] [PubMed] [Google Scholar]
- 99.César KG, Brucki SM, Takada LT, et al. Prevalence of cognitive impairment without dementia and dementia in Tremembé, Brazil. Alzheimer Dis Assoc Disord. 2016;30(3):264-271. doi: 10.1097/WAD.0000000000000122 [DOI] [PubMed] [Google Scholar]
- 100.Egeberg A, Hansen PR, Gislason GH, Thyssen JP. Patients with rosacea have increased risk of dementia. Ann Neurol. 2016;79(6):921-928. doi: 10.1002/ana.24645 [DOI] [PubMed] [Google Scholar]
- 101.Huang F, Shang Y, Luo Y, et al. Lower prevalence of Alzheimer’s disease among Tibetans: association with religious and genetic factors. J Alzheimers Dis. 2016;50(3):659-667. doi: 10.3233/JAD-150697 [DOI] [PubMed] [Google Scholar]
- 102.Kosteniuk JG, Morgan DG, O’Connell ME, et al. Simultaneous temporal trends in dementia incidence and prevalence, 2005-2013: a population-based retrospective cohort study in Saskatchewan, Canada. Int Psychogeriatr. 2016;28(10):1643-1658. doi: 10.1017/S1041610216000818 [DOI] [PubMed] [Google Scholar]
- 103.Parlevliet JL, Uysal-Bozkir Ö, Goudsmit M, et al. Prevalence of mild cognitive impairment and dementia in older non-western immigrants in the Netherlands: a cross-sectional study. Int J Geriatr Psychiatry. 2016;31(9):1040-1049. doi: 10.1002/gps.4417 [DOI] [PubMed] [Google Scholar]
- 104.Sharifi F, Fakhrzadeh H, Varmaghani M, et al. Prevalence of dementia and associated factors among older adults in Iran: National Elderly Health Survey (NEHS). Arch Iran Med. 2016;19(12):838-844. [DOI] [PubMed] [Google Scholar]
- 105.Wong SL, Gilmour H, Ramage-Morin PL. Alzheimer’s disease and other dementias in Canada. Health Rep. 2016;27(5):11-16. [PubMed] [Google Scholar]
- 106.Yue W, Wang XD, Shi Z, et al. The prevalence of dementia with Lewy bodies in a rural area of China. Parkinsonism Relat Disord. 2016;29:72-77. doi: 10.1016/j.parkreldis.2016.05.022 [DOI] [PubMed] [Google Scholar]
- 107.Ahmadi-Abhari S, Guzman-Castillo M, Bandosz P, et al. Temporal trend in dementia incidence since 2002 and projections for prevalence in England and Wales to 2040: modelling study. BMJ. 2017;358:j2856. doi: 10.1136/bmj.j2856 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Banerjee TK, Dutta S, Das S, et al. Epidemiology of dementia and its burden in the city of Kolkata, India. Int J Geriatr Psychiatry. 2017;32(6):605-614. doi: 10.1002/gps.4499 [DOI] [PubMed] [Google Scholar]
- 109.Basta M, Simos P, Bertsias A, et al. Association between insomnia symptoms and cognitive impairment in the Cretan Aging Cohort. Eur Geriatr Med. 2018;9(5):697-706. doi: 10.1007/s41999-018-0086-7 [DOI] [PubMed] [Google Scholar]
- 110.Dominguez J, Fe de Guzman M, Reandelar M, Thi Phung TK. Prevalence of dementia and associated risk factors: a population-based study in the Philippines. J Alzheimers Dis. 2018;63(3):1065-1073. doi: 10.3233/JAD-180095 [DOI] [PubMed] [Google Scholar]
- 111.Kodesh A. Prevalence and comorbidities of dementia in Israel: a nationally representative cohort study. Int Psychogeriatr. 2018;1-5. [DOI] [PubMed] [Google Scholar]
- 112.Kurl S, Laukkanen JA, Lonnroos E, Remes AM, Soininen H. Cardiorespiratory fitness and risk of dementia: a prospective population-based cohort study. Age Ageing. 2018;47(4):611-614. doi: 10.1093/ageing/afy060 [DOI] [PubMed] [Google Scholar]
- 113.Kvello-Alme M, Bråthen G, White LR, Sando SB. The prevalence and subtypes of young onset dementia in central Norway: a population-based study. J Alzheimers Dis. 2019;69(2):479-487. doi: 10.3233/JAD-181223 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Petersen MS, Restorff M, Stórá T, Waldemar G, Joensen S. Trend in the incidence and prevalence of dementia in the Faroe Islands. J Alzheimers Dis. 2019;71(3):969-978. doi: 10.3233/JAD-190341 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Ruano L, Araújo N, Branco M, et al. Prevalence and causes of cognitive impairment and dementia in a population-based cohort from northern Portugal. Am J Alzheimers Dis Other Demen. 2019;34(1):49-56. doi: 10.1177/1533317518813550 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Masika GM, Yu DSF, Li PWC. Accuracy of the Montreal Cognitive Assessment in detecting mild cognitive impairment and dementia in the rural African population. Arch Clin Neuropsychol. 2021;36(3):371-380. doi: 10.1093/arclin/acz086 [DOI] [PubMed] [Google Scholar]
- 117.United Nations, Department of Economic and Social Affairs, Population Dynamics. (2019). World Population Prospects 2019. 2019. Accessed September 2, 2020. https://population.un.org/wpp/DataQuery/
- 118.Prince MJ, Bryce R, Ferri CP. World Alzheimer Report 2011: The Benefits of Early Diagnosis and Intervention. Alzheimer’s Disease International; 2011. [Google Scholar]
- 119.Johnson JK, Diehl J, Mendez MF, et al. Frontotemporal lobar degeneration: demographic characteristics of 353 patients. Arch Neurol. 2005;62(6):925-930. doi: 10.1001/archneur.62.6.925 [DOI] [PubMed] [Google Scholar]
- 120.Neary D, Snowden J, Mann D. Frontotemporal dementia. Lancet Neurol. 2005;4(11):771-780. doi: 10.1016/S1474-4422(05)70223-4 [DOI] [PubMed] [Google Scholar]
- 121.Attems J, Jellinger KA. The overlap between vascular disease and Alzheimer’s disease—lessons from pathology. BMC Med. 2014;12(1):206. doi: 10.1186/s12916-014-0206-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Fiest KM, Jetté N, Roberts JI, et al. The prevalence and incidence of dementia: a systematic review and meta-analysis. Can J Neurol Sci. 2016;43(suppl 1)(suppl 1):S3-S50. doi: 10.1017/cjn.2016.18 [DOI] [PubMed] [Google Scholar]
- 123.Rücker G, Schwarzer G, Carpenter JR, Schumacher M. Undue reliance on I2 in assessing heterogeneity may mislead. BMC Med Res Methodol. 2008;8(1):79. doi: 10.1186/1471-2288-8-79 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Wilkinson T, Ly A, Schnier C, et al. ; UK Biobank Neurodegenerative Outcomes Group and Dementias Platform UK . Identifying dementia cases with routinely collected health data: a systematic review. Alzheimers Dement. 2018;14(8):1038-1051. doi: 10.1016/j.jalz.2018.02.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Romero JP, Benito-León J, Mitchell AJ, Trincado R, Bermejo-Pareja F. Under reporting of dementia deaths on death certificates using data from a population-based study (NEDICES). J Alzheimers Dis. 2014;39(4):741-748. doi: 10.3233/JAD-131622 [DOI] [PubMed] [Google Scholar]
- 126.Thygesen LC, Ersbøll AK. When the entire population is the sample: strengths and limitations in register-based epidemiology. Eur J Epidemiol. 2014;29(8):551-558. doi: 10.1007/s10654-013-9873-0 [DOI] [PubMed] [Google Scholar]
- 127.World Bank . Why use GNI per capita to classify economies into income groupings? 2020. Accessed May 25, 2020. https://datahelpdesk.worldbank.org/knowledgebase/articles/378831-why-use-gni-per-capita-to-classify-economies-into
- 128.Schwarzer G, Chemaitelly H, Abu-Raddad LJ, Rücker G. Seriously misleading results using inverse of Freeman-Tukey double arcsine transformation in meta-analysis of single proportions. Res Synth Methods. 2019;10(3):476-483. doi: 10.1002/jrsm.1348 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods 1. Search Strategy for PubMed
eMethods 2. Data Extraction Sheet
eMethods 3. Quality Assessment Tool
eTable 1. World Bank Classification
eTable 2. Detailed Information on Studies Included in the Review
eTable 3. Results Data Analyses of Subgroups
eTable 4. Prevalence of Dementia With Lewy Bodies/Parkinson Disease Dementia in the 4 Eligible Studies
eFigure 1. Flowchart of Included and Excluded Studies
eFigure 2. Forest Plot 5-Year Age Bands for All-Type YOD
eResults. Subgroup Analyses Within Subtypes of Dementia