

Abstract
Objective: To compare and evaluate the regulatory effects of comprehensive psychological intervention on adverse emotions and immune status of cervical cancer patients during the perioperative period. Methods: A total of 109 cervical cancer patients admitted to our hospital were selected and divided into the conventional group (n=54) and the comprehensive group (n=55). The conventional group received conventional nursing intervention, while the comprehensive group received comprehensive psychological and conventional nursing intervention. The adverse emotions, social support degrees, level of hope, sleep quality, immune functions and nursing satisfaction were compared between the two groups. Results: On Day 10 after surgery, the comprehensive group had lower scores of hospital anxiety and depression scale-anxiety (HADS-A), and hospital anxiety and depression scale-depression (HADS-D), higher scores of social support rating scale (SSRS), intimate relationship, positive attitude, and attitude for actions, a higher excellent and good rate of social support degree (92.73% vs 75.93%), a lower Cortisol (Cor) level, and a higher level of interleukin-2 (IL-2) than the conventional group (P < 0.05). On Days 1, 3, 5, 7 and 10 after surgery, the scores of Pittsburgh sleep quality index (PSQI) in the comprehensive group were lower than those in the conventional group (P < 0.05). The overall degree of nursing satisfaction in comprehensive group (94.55%) was higher than that in the conventional group (79.63%) (P < 0.05). Conclusion: Comprehensive psychological intervention can remarkably improve the negative emotions, social support degree, level of hope, sleep quality, immune functions, and satisfaction of cervical cancer patients receiving conventional nursing intervention during the perioperative period.
Keywords: Comprehensive psychological intervention, perioperative period, cervical cancer, adverse emotions, immune status, regulation
Introduction
Cervical cancer ranks the third in the incidence of malignant rumors in women and has a negative impact on the physical and mental health of patients. Currently, cervical cancer has become a leading cause of cancer-related deaths in women [1]. Previously, cervical cancer was very common in middle-aged women. The changes in the lifestyle and advances in clinical diagnostic techniques have been witnessed over these years. Cervical cancer frequently occurs in young women, indicating that women with a wider age range are susceptible to developing cervical cancer [2].
Radical surgery is the preferred treatment for cervical cancer that is diagnosed at early stage. However, large and invasive surgery leads to the concerns of patients about the surgical effects and safety before surgery. In addition, patients are prone to post-traumatic stress disorder (PTSD) after surgery, which can easily lead to adverse emotions [3]. A qualitative study suggests that cervical cancer can affect the psychological states, physical symptoms and family functions of patients [4]. Clinical findings show that the incidence of postoperative anxiety in cervical cancer patients exceeds 20% [5]. A cross-sectional study revealed that the incidence of depression in cervical cancer patients is more than 20% within one week after surgery [6]. It has been reported that persistent negative emotions will affect the immune functions of cancer patients, and chronic stress caused by adverse emotions will affect the neuroendocrine system functions and cytokines, and eventually leads to a higher incidence of tumor recurrence [7]. Clinical nursing intervention is considered to be an effective method to control the adverse emotions of cancer patients. However, the conventional nursing intervention was mainly used for the treatment of gynecologic neoplasms previously, and some studies on psychological intervention were relatively simple and lacked comprehensiveness. In addition, different tools for evaluation of the adverse emotions of patients are adopted in different studies, and there are noticeable differences in the duration and specific measures of psychological nursing intervention. This will lead to varying conclusions on the influences of psychological nursing intervention on the emotions of cervical cancer patients.
Comprehensive psychological intervention refers to the corresponding psychological interventions performed on cervical cancer patients before and after surgery. Meanwhile, there are various contents and methods of psychological interventions, which ensure that patients can receive professional and effective psychological interventions during the perioperative period [8]. A study on the implementation of comprehensive psychological intervention in patients with benign cervical lesions showed that the psychological state of patients after receiving the intervention was significantly improved compared with the control group [9]. Another previous study has implemented comprehensive psychological interventions on patients with gynecological diseases, and found that not only the anxiety and depression of the patients were significantly reduced, but the self-efficacy after nursing was also significantly improved compared with the conventional group [10]. However, there have been few studies on the use of comprehensive psychological intervention in cervical cancer nursing, and the value of comprehensive psychological intervention in the nursing of cervical cancer patients has not been confirmed. Therefore, this research aimed to expand the application scope of comprehensive psychological intervention and explores more useful methods for cervical cancer nursing.
Materials and methods
General data
A total of 109 cervical cancer patients admitted to our hospital from July 2017 to December 2019 were selected as the study subjects, and were divided into the conventional group (n=54) and the comprehensive group (n=55). The conventional group received conventional nursing intervention, while the comprehensive group received comprehensive psychological intervention combined with conventional nursing intervention. Inclusion criteria: initially diagnosed as cervical cancer and treated with radical surgery, clinical stage I or IIa [11]; aged over 18 years; with clear understanding and excellent communication skills. All subjects signed the informed consent form. The study was reviewed and approved by the Ethics Committee of Northwest Woman’s and Children’s Hospital. Exclusion criteria: clinical stage IIa and above; patients previously treated with radiotherapy or chemotherapy; patients previously diagnosed as mental illness; patients treated with immunomodulators before enrollment; patients complicated by immune system diseases and endocrine disease.
Methods
The conventional group was treated with conventional nursing intervention during the perioperative period. The intervention, including preoperative guidance through making rounds, active cooperation during surgery, postoperative health education and discharge guidance, was performed from 1 day before surgery to 10 days after surgery.
The comprehensive group was treated with comprehensive psychological intervention combined with conventional nursing intervention during the perioperative period. The intervention was performed from 1 day before surgery to 10 days after surgery, and the psychological intervention lasted for about 1 hour every day. The intervention contents are as follows.
Comprehensive cognitive intervention: the cervical cancer-related knowledge was compiled into a self-management education manual, including conventional health education, images and models. The patients were informed of conducting independent reading and learning, and nursing staff offered small classes from time to time to explain important contents in the manual. Regarding patients with a family history of cervical cancer, women in their families should receive liquid-based cervical cytology screening once a year, and supervise their husbands to maintain excellent health habits. The explanation from nursing staff could help patients positively view their diseases, and actively cooperate with physicians for surgical treatment.
Behavioral intervention: the psychological state was evaluated once a day during the nursing intervention, the psychological issues of the patients were analyzed, and the patients were instructed to perform progressive muscle relaxation. In a quiet environment, the patients were kept lying flat in a comfortable bed, and were told to remove distractions, relax the body and place the hands naturally on the sides of the body. Light music or absolute music was played, the patients were instructed to contract the muscles for 10 seconds and then relax the muscles for 30 seconds, and this exercise was repeatedly performed. The relaxation exercise was conducted for 10 minutes every day.
Emotional intervention: patients with different adverse emotions were treated with different interventions. Nurses helped patients with depression share their inner feelings with nurses, families, friends, the sky and their favorite objects. Nurses shared surgical processes, skills and experience of physicians, and successfully treated cases with patients who were overly concerned about surgery. Nurses shared attention-diverting methods and methods for emotional self-regulation with all patients with adverse emotions.
Social support intervention: families and friends can provide social support for cervical cancer patients. Therefore, nurses should tell the relatives and friends to accompany the patients and provide their care and necessary support, and inform the relatives and friends that their attitude towards patients directly affects the emotional reactions of patients. Additionally, the relatives and friends were instructed to understand the extreme behaviors of the patients, and were informed of handling methods for the extreme behaviors. During the daily communication with patients, the topics should focus on the previous positive things or future expectations, so as to boost their confidence in treatment of the diseases. The support from the patients’ husbands is crucial. Nurses periodically organized patients and their husbands to receive education related to cervical cancer, so that their husbands could learn more about cervical cancer, understand the patients’ sufferings, offer more support and care to the patients, and show more understanding.
Observational indices
Adverse emotions: the evaluation was performed using the hospital anxiety and depression scale (HADS) [12] prepared by Zigmond AS and Snaith RP was evaluated once 3 days before surgery and 10 days after surgery, respectively. HADS includes hospital anxiety and depression scale-anxiety (HADS-A) and hospital anxiety and depression scale-depression (HADS-D). Each scale consists of 7 items scored using a scoring system of 0-3 points. The total score of each scale is 0-21 points, with scores ≥ 8 points indicating anxiety and depression.
Social support degree: the evaluation was performed using social support rating scale (SSRS) [13] once 3 days before surgery and 10 days after surgery, respectively. SSRS includes subjective support (3 items), objective support (4 items) and social support utilization (3 items), with the total score of 12-66 points. A higher score indicates a higher social support for patients. Scores of ≤ 33 points indicate poor social support, 33-45 points indicate good social support, and ≥ 45 points indicate excellent social support.
Level of hope: the evaluation was performed using Herth hope scale (HHS) [14] once 3 days before surgery and 10 days after surgery. HHS comprises 12 items, including 3 levels, namely, intimate relationship, positive attitude and attitude for actions. Each item was scored using a scoring system of 1-4 points, and each level was scored using a scoring system of 4-16 points. A higher total score indicates a higher level of hope.
Sleep quality: the evaluation was performed using Pittsburgh sleep quality index (PSQI) [15] once 3 days before surgery and on Days 1, 3, 5, 7 and 10 after surgery. PSQI comprises 7 items, including sleep quality, sleep time, duration of sleep, sleep efficiency, sleep disorder, hypnotics and daytime dysfunction, which are scored using a scoring system of 0-3 points based on the severity. The total score is 0-21 points. A higher score indicates a poorer quality of sleep.
Immune function: the levels of Cortisol (Cor) and interleukin-2 (IL-2) in the two groups were measured 3 days before surgery and 10 days after surgery. A total of 4 ml of venous blood was collected at the two time points and centrifuged at 3000 rpm/min for 5 minutes to obtain the serum. The serum was measured by an immune counter.
Nursing satisfaction: The evaluation was performed using the inpatient satisfaction questionnaire prepared by our hospital. The questionnaire comprises 15 questions, and each question is scored using a scoring system of 1-5 points. 1-5 points indicate very dissatisfied, dissatisfied, generally, generally satisfied and satisfied, respectively. The total score is 75 points. Scores of ≥ 60 points indicate satisfied, 30-60 points indicate generally satisfied, and ≤ 30 points indicate dissatisfied. The degree of satisfaction with nursing = satisfied rate + generally satisfied.
Statistical method
SPSS23.0 was used for statistical analysis. The enumeration data were expressed by [n (%)], and detected using X2 test. The measurement data were expressed by (x̅ ± s), and detected using t test. The multi-point comparison was performed using analysis of variance (ANVOA), and detected using F test. The graphics were made using Graphpad Prism 8. P < 0.05 indicated a statistically significant difference.
Results
General data
There was no statistically significant difference in gender, average age, average body mass index (BMI), staging, pathological type and surgical methods between the two groups (P > 0.05) (Table 1).
Table 1.
Comparison of general data between the two groups (x̅ ± s)/[n (%)]
| Data | Comprehensive group (n=55) | Conventional group (n=54) | t/X2 | P | |
|---|---|---|---|---|---|
| Age (year) | 53.29±12.49 | 54.37±13.08 | 0.441 | 0.660 | |
| BMI (kg/m2) | 22.19±1.43 | 23.04±1.51 | 0.604 | 0.547 | |
| Disease staging | Stage I | 25 (45.45) | 22 (40.74) | 0.247 | 0.619 |
| Stage IIa | 30 (54.55) | 32 (59.26) | |||
| Pathological type | Squamous carcinoma | 48 (87.27) | 45 (83.33) | 1.638 | 0.527 |
| Adenocarcinoma | 5 (9.09) | 8 (14.81) | |||
| Others | 2 (3.64) | 1 (1.85) | |||
| Surgical methods | Conization of cervix | 16 (29.09) | 17 (31.48) | 0.819 | 0.341 |
| Radical hysterectomy | 20 (36.36) | 19 (35.19) | |||
| Radical amputation of cervix | 19 (34.55) | 18 (33.33) | |||
Adverse emotions
On Day 3 before surgery, there was no statistically significant difference in the scores of HADS-A and HADS-D between the two groups (P < 0.05). The scores of HADS-A and HADS-D in the two groups on Day 10 after surgery were lower than those on Day 3 before surgery (P < 0.05). On Day 10 after surgery, the scores of HADS-A and HADS-D in the comprehensive group were lower than those in the conventional group (P < 0.05) (Figure 1).
Figure 1.
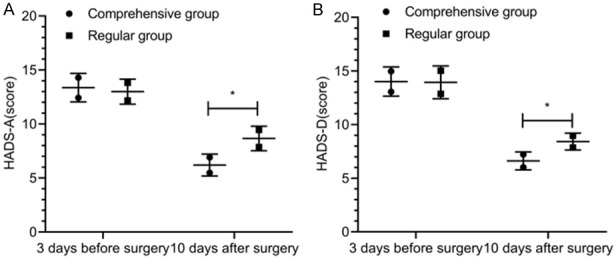
Adverse emotions. On Day 3 before surgery, there was no noticeable difference in the scores of HADS-A (A) and HADS-D (B) between the two groups (P > 0.05). On Day 10 after surgery, the scores of HADS-A (A) and HADS-D (B) in the comprehensive group were lower than those in the conventional group (P < 0.05). *indicates the comparison between the two groups (P < 0.05).
Social support degree
On Day 3 before surgery, there was no statistically significant difference in SSRS scores between the two groups (P > 0.05). The SSRS scores in the two groups on Day 10 after surgery were higher than those on Day 3 before surgery (P < 0.05). On Day 10 after surgery, SSRS scores in the comprehensive group were noticeably higher than those in the conventional group (P < 0.05) (Figure 2). On Day 10 after surgery, there were 23 cases with excellent social support, 28 cases with good social support and 4 cases with poor social support in the comprehensive group, with an excellent and good rate of 92.73%, while there were 19 cases with excellent social support, 22 cases with good social support and 13 cases with poor social support in the conventional group, with an excellent and good rate of 75.93%. On Day 10 after surgery, the excellent and good rate of social support in the comprehensive group was significantly higher than that in the conventional group (P < 0.05) (Table 2).
Figure 2.
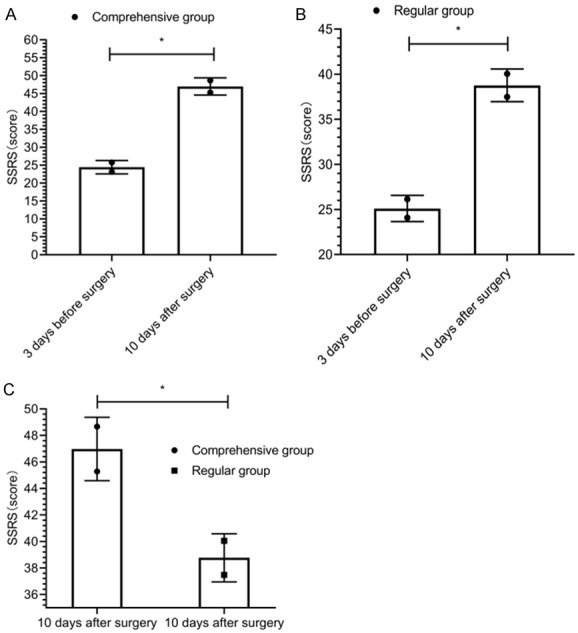
Social support degree. The scores of SSRS in the comprehensive group (A) and conventional group (B) on Day 3 before surgery were lower than those in the comprehensive group (A) and conventional group (B) on Day 10 after surgery (P > 0.05). On Day 10 after surgery, the scores of SSRS in the comprehensive group (C) were higher than those in the conventional group (P < 0.05). *indicates the comparison between the two groups (P < 0.05).
Table 2.
Comparison of excellent and good rates of social support between the two groups at 10 days after surgery [n (%)]
| Group | Excellent | Good | Poor | Excellent and good rate |
|---|---|---|---|---|
| Comprehensive group (n=55) | 23 (41.82) | 28 (50.91) | 4 (7.27) | 51 (92.73) |
| Conventional group (n=54) | 19 (35.19) | 22 (40.74) | 13 (24.07) | 41 (75.93) |
| X2 | 4.636 | |||
| P | 0.031 |
Level of hope
On Day 3 before surgery, there was no statistically significant difference in the scores of intimate relationship, positive attitude and attitude for actions in HHS between the two groups (P > 0.05). The scores of intimate relationship, positive attitude and attitude for actions in the two groups on Day 10 after surgery were higher than those on Day 3 before surgery (P < 0.05). On Day 10 after surgery, the scores of intimate relationship, positive attitude and attitude for actions in the comprehensive group were remarkably higher than those in the conventional group (P < 0.05) (Figure 3).
Figure 3.
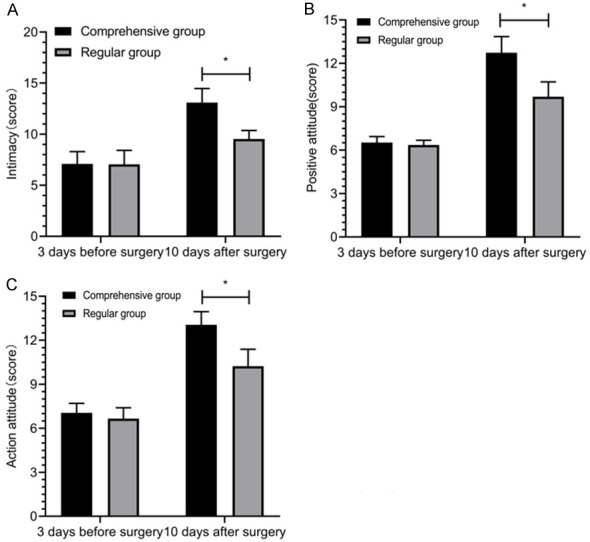
Level of hope. On Day 3 before surgery, there was no significant difference in the scores of intimate relationship (A), positive attitude (B) and attitude for actions (C) between the two groups (P > 0.05). On Day 10 after surgery, the scores of intimate relationship (A), positive attitude (B) and attitude for actions (C) in the comprehensive group were higher that those in the conventional group (P < 0.05). *indicates the comparison between the two groups (P < 0.05).
Sleep quality
On Day 3 before surgery, there was no statistically significant difference in PSQI scores between the two groups (P > 0.05). On Days 1, 3, 5, 7 and 10 after surgery, PSQI scores were decreased in the two groups, and PSQI scores in the comprehensive group were lower than those in the conventional group (P < 0.05). On Days 5, 7 and 10 after surgery, PSQI scores in the conventional group were lower than those in the convention group on Day 3 before surgery (P < 0.05). There was no statistically significant difference in PSQI scores in the conventional group between on Days 1 and 3 after surgery and on Day 3 before surgery (P > 0.05) (Figure 4).
Figure 4.
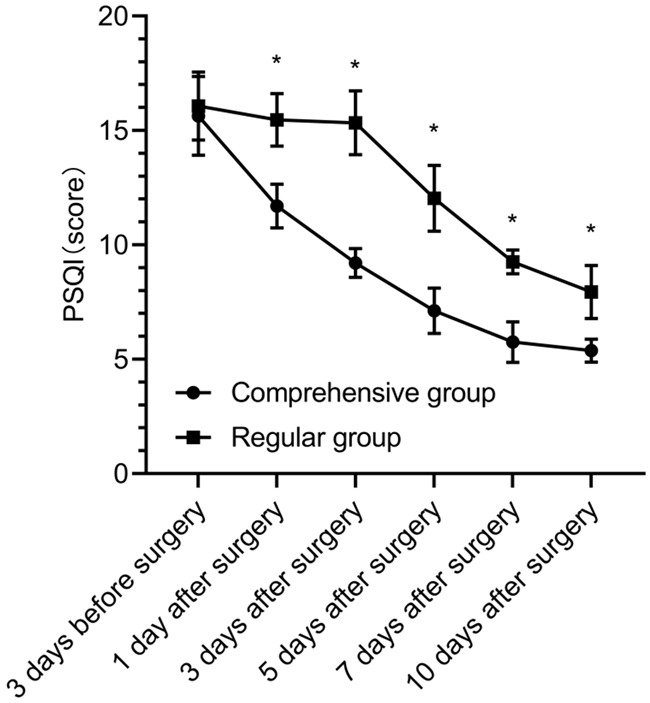
Sleep quality. On Day 3 before surgery, there was no marked difference in the scores of PSQI between the two groups (P > 0.05). On Days 1, 3, 5, 7 and 10 after surgery, the scores of PSQI in the comprehensive group were lower than those in the conventional group (P < 0.05). *indicates the comparison between the two groups (P < 0.05).
Immune function
On Day 3 before surgery, there was no statistically significant difference in the levels of Cor and IL-2 between the two groups (P > 0.05). On Day 10 after surgery, the levels of Cor were decreased in the two groups, while the levels of IL-2 were increased. There were statistically significant differences in the levels of Cor and IL-2 in the two groups between on Day 10 after surgery and on Day 3 before surgery (P < 0.05). On Day 10 after surgery, the comprehensive group had a lower level of Cor and a higher level of IL-2 than the conventional group (P < 0.05) (Figure 5).
Figure 5.
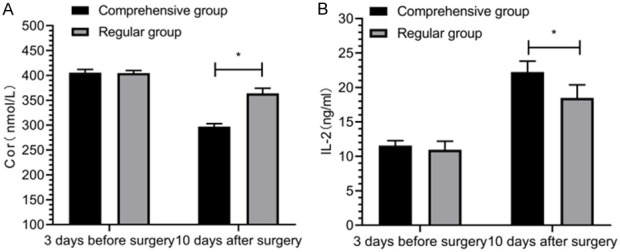
Cor and IL-2. On Day 3 before surgery, there was no significant difference in the levels of Cor (A) and IL-2 (B) between the two groups (P > 0.05). On Day 10 after surgery, the comprehensive group had a lower level of Cor (A) and a higher level of IL-2 (B) compared with the conventional group (P < 0.05). *indicates the comparison between the two groups (P < 0.05).
Nursing satisfaction degree
In the comprehensive group, there were 22 patients who were satisfied with nursing intervention, 30 patients who were generally satisfied with nursing intervention, and 3 patients who were dissatisfied with nursing intervention, with the total nursing satisfaction of 94.55%. In the conventional group, there were 18 patients who were satisfied with nursing intervention, 25 patients who were generally satisfied with nursing intervention, and 11 patients who were dissatisfied with nursing intervention, with the total nursing satisfaction of 79.63%. The nursing satisfaction degree in the comprehensive group was remarkably higher than that in the conventional group (P < 0.05) (Table 3).
Table 3.
Comparison of nursing satisfaction degrees between the two groups [n (%)]
| Group | Satisfied | Generally satisfied | Dissatisfied | Total satisfaction degree |
|---|---|---|---|---|
| Comprehensive group (n=55) | 22 (44.00) | 30 (54.55) | 3 (5.45) | 52 (94.55) |
| Conventional group (n=54) | 18 (33.33) | 25 (46.30) | 11 (20.37) | 43 (79.63) |
| X2 | 4.165 | |||
| P | 0.041 |
Discussion
Since cervical cancer surgery may cause trauma to the reproductive organs, patients, especially young female patients, are concerned about the female characteristics and postoperative images. As a result, they bear a heavy psychological burden from the influences of diseases and treatment [16]. Additionally, the restricted self-care abilities of patients during the hospital stay may easily result in adverse emotions [17]. A study have indicated that the incidences of anxiety and depression in cervical cancer patients are about 30% and 32%, respectively [18]. On Day 3 before surgery, the average scores of HADS-A and HADS-D in the two groups were over 8 points, suggesting that anxiety and depression occurred. The scores of HADS-A and HADS-D in the comprehensive group were lower than those in the conventional group on Day 10 after surgery (P < 0.05), indicating that the anxiety and depression of patients could be alleviated to a greater extent through implementation of comprehensive psychological intervention. This may be due to the reason that comprehensive psychological intervention enables patients to learn more knowledge about diseases and treatment, correct their previous misconceptions about diseases, establish a correct cognition, and positively view diseases and treatment, so as to alleviate or even eliminate the adverse emotions.
Clinical findings show that the social support obtained by patients with malignant tumors is closely related to their psychological states and attitudes toward diseases and treatment, and patients with a higher social support are more willing to cooperate with treatment, and can obtain higher therapeutic effects [19]. In this study, there was no significant difference in SSRS scores between the two groups on Day 3 before surgery. However, the SSRS scores in the comprehensive group were markedly higher than those in the conventional group on Day 10 after surgery, supporting that the comprehensive psychological intervention could improve the social support degree of patients compared with conventional nursing intervention. During the implementation of comprehensive nursing intervention, the support from relatives and friends of patients should be obtained, and the role of patients’ husbands should be highlighted, so that they could feel care and support from their relatives, friends and husbands during the perioperative period. Social support refers to the external resources that are accessible to individuals. Good social support can help individuals maintain positive emotions, making patients have the courage to respond to challenges and prevent dysgnosia and adverse emotions [20]. On Day 10 after surgery, the excellent and good rate of social support in the comprehensive group (92.73%) was higher than that in the conventional group (75.93%) (P < 0.05). Actually, active psychological intervention can effectively improve the adverse emotions of cervical cancer patients, and the social support degree in the comprehensive group is improved more remarkably compared with that in the conventional group [21], which are consistent with the findings of this study.
On Day 10 after surgery, the scores of intimate relationship, positive attitude and attitude for actions in the evaluation of the level of hope in the comprehensive group were higher than those in the conventional group (P < 0.05). This demonstrated that the comprehensive psychological intervention could improve the level of hope of patients, and the elevated level of hope enabled patients to positively view diseases and actively cooperate with treatment. In addition, a higher level of hope suggested a lower incidence of patients’ adverse emotions and less influences on sleep quality. On Days 1, 3, 5, 7 and 10 after surgery, PSQI scores in the comprehensive group were lower than those in the conventional group (P < 0.05), suggesting that comprehensive psychological intervention was conducive to improving the sleep quality of patients. It has been shown that the incidence of sleep disorders is closely related to emotional disorders, individuals’ inner anguish, and psychiatric disorders. Through implementation of comprehensive psychological intervention, the individual nervous system can be regulated, and the body and mind of patients feel relaxed, so as to adjust the adverse emotions, thereby achieve better sleep quality [22]. Cortisol (Cor) level is an indicator for the immune level and can exert immune-suppressing effects [23]. IL-2, a lymphokine, can play an anti-infection and anti-tumor role. The level of IL-2 is also an indicator for the immune status [24]. On Day 10 after surgery, the Cor level was decreased and the IL-2 level was increased in the two groups, and the changes in the levels of Cor and IL-2 in the comprehensive group were significant different with those in the conventional group (P < 0.05), indicating that comprehensive psychological intervention could remarkably improve the immune status of patients. In the comprehensive psychological intervention, multiple measures regarding cognition, emotions, behaviors and social support have been implemented. After nursing intervention, patients’ views on diseases were changed, their mental stress was alleviated, and they could actively communicate with their husbands, positively view treatment and postoperative physical changes, and maintain a higher confidence in their postoperative lives. The total nursing satisfaction degree in the comprehensive group (94.55%) was higher than that in the conventional group (79.63%) (P < 0.05). Indeed, it has been shown that psychological intervention can improve the nursing satisfaction of cervical cancer patients (95% vs 75%) (P < 0.05) [9], which is consistent with the result of this study. This is due to the reason that comprehensive psychological intervention is superior to traditional nursing intervention, and the use of comprehensive psychological intervention can eliminate the doubts and concerns of patients, leading to a higher degree of satisfaction.
In summary, comprehensive psychological intervention can remarkably improve adverse emotions, social support, level of hope, sleep quality, immune function, satisfaction of cervical cancer patients during the perioperative period, thus confirming the implementation value of comprehensive psychological nursing intervention in the treatment of cervical cancer patients during the perioperative period. However, only two groups were established in this study, the patients with early cervical cancer were enrolled, the differences in effects of comprehensive psychological intervention on cervical cancer patients at different ages and with different severity were not further explored, in the future studies.
Acknowledgements
A survey of stigma and the humanistic care intervention development for female hepatitis patients after surgery Funded by Science and Technology Agency of Shaanxi Province, Grant No. 2019KRM172; The current status of breast feeding in Xi’an and the effects of intervention during pregnancy and after delivery Funded by Science and Technology Agency of Shaanxi Province, Grant No. 2018SF-224; A survey of the prevalence, risk factors, and intervention effects of depression among pregnant woman Funded by Science and Technology Agency of Shaanxi Province, Grant No. 2011K14-07-06.
Disclosure of conflict of interest
None.
References
- 1.Fang J, Zhang H, Jin S. Epigenetics and cervical cancer: from pathogenesis to therapy. Tumour Biol. 2014;35:5083–5093. doi: 10.1007/s13277-014-1737-z. [DOI] [PubMed] [Google Scholar]
- 2.Olusola P, Banerjee HN, Philley JV, Dasgupta S. Human papilloma virus-associated cervical cancer and health disparities. Cells. 2019;8:622. doi: 10.3390/cells8060622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bogani G, Leone Roberti Maggiore U, Rossetti D, Ditto A, Martinelli F, Chiappa V, Ferla S, Indini A, Sabatucci I, Lorusso D, Raspagliesi F. Advances in laparoscopic surgery for cervical cancer. Crit Rev Oncol Hematol. 2019;143:76–80. doi: 10.1016/j.critrevonc.2019.07.021. [DOI] [PubMed] [Google Scholar]
- 4.McCree R, Giattas MR, Sahasrabuddhe VV, Jolly PE, Martin MY, Usdan SL, Kohler C, Lisovicz N. Expanding cervical cancer screening and treatment in tanzania: stakeholders’ perceptions of structural influences on scale-up. Oncologist. 2015;20:621–626. doi: 10.1634/theoncologist.2013-0305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lestyani Nasution C, Afiyanti Y, Milanti A. The relationship of the preexisting anxiety problem with the demographic profile of cervical cancer patients. Enferm Clin. 2018;28(Suppl 1):199–202. [Google Scholar]
- 6.Shyu IL, Hu LY, Chen YJ, Wang PH, Huang BS. Risk factors for developing depression in women with cervical cancer: a nationwide population-based study in Taiwan. Int J Womens Health. 2019;11:135–141. doi: 10.2147/IJWH.S193003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gu D, Ao X, Yang Y, Chen Z, Xu X. Soluble immune checkpoints in cancer: production, function and biological significance. J Immunother Cancer. 2018;6:132. doi: 10.1186/s40425-018-0449-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chad-Friedman E, Coleman S, Traeger LN, Pirl WF, Goldman R, Atlas SJ, Park ER. Psychological distress associated with cancer screening: a systematic review. Cancer. 2017;123:3882–3894. doi: 10.1002/cncr.30904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Isaka Y, Inada H, Hiranuma Y, Ichikawa M. Psychological impact of positive cervical cancer screening results among Japanese women. Int J Clin Oncol. 2017;22:102–106. doi: 10.1007/s10147-016-1023-8. [DOI] [PubMed] [Google Scholar]
- 10.Murtagh FE, Burns A, Moranne O, Morton RL, Naicker S. Supportive care: comprehensive conservative care in end-stage kidney disease. Clin J Am Soc Nephrol. 2016;11:1909–1914. doi: 10.2215/CJN.04840516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tsikouras P, Zervoudis S, Manav B, Tomara E, Iatrakis G, Romanidis C, Bothou A, Galazios G. Cervical cancer: screening, diagnosis and staging. J BUON. 2016;21:320–325. [PubMed] [Google Scholar]
- 12.Julian LJ. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A) Arthritis Care Res (Hoboken) 2011;63(Suppl 11):S467–472. doi: 10.1002/acr.20561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tong X, Chen J, Park SP, Wang X, Wang C, Su M, Zhou D. Social support for people with epilepsy in China. Epilepsy Behav. 2016;64:224–232. doi: 10.1016/j.yebeh.2016.08.010. [DOI] [PubMed] [Google Scholar]
- 14.Ripamonti CI, Buonaccorso L, Maruelli A, Bandieri E, Boldini S, Pessi MA, Chiesi F, Miccinesi G. Hope Herth Index (HHI): a validation study in Italian patients with solid and hematological malignancies on active cancer treatment. Tumori. 2012;98:385–392. doi: 10.1177/030089161209800317. [DOI] [PubMed] [Google Scholar]
- 15.Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2016;25:52–73. doi: 10.1016/j.smrv.2015.01.009. [DOI] [PubMed] [Google Scholar]
- 16.Marquina G, Manzano A, Casado A. Targeted agents in cervical cancer: beyond bevacizumab. Curr Oncol Rep. 2018;20:40. doi: 10.1007/s11912-018-0680-3. [DOI] [PubMed] [Google Scholar]
- 17.Chen NN, Moran MB, Frank LB, Ball-Rokeach SJ, Murphy ST. Understanding cervical cancer screening among latinas through the lens of structure, culture, psychology and communication. J Health Commun. 2018;23:661–669. doi: 10.1080/10810730.2018.1500661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kaur M, Agnihotri M, Das K, Rai B, Ghai S. Effectiveness of an interventional package on the level of anxiety, depression, and fatigue among patients with cervical cancer. Asia Pac J Oncol Nurs. 2018;5:195–200. doi: 10.4103/apjon.apjon_56_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Korotkin BD, Hoerger M, Voorhees S, Allen CO, Robinson WR, Duberstein PR. Social support in cancer: how do patients want us to help? J Psychosoc Oncol. 2019;37:699–712. doi: 10.1080/07347332.2019.1580331. [DOI] [PubMed] [Google Scholar]
- 20.Uchino BN, Trettevik R, Kent de Grey RG, Cronan S, Hogan J, Baucom BRW. Social support, social integration, and inflammatory cytokines: a meta-analysis. Health Psychol. 2018;37:462–471. doi: 10.1037/hea0000594. [DOI] [PubMed] [Google Scholar]
- 21.Blumenthal JA, Zhu Y, Koch GG, Smith PJ, Watkins LL, Hinderliter AL, Hoffman BM, Rogers JG, Chang PP, O’Connor C, Johnson KS, Sherwood A. The modifying effects of social support on psychological outcomes in patients with heart failure. Health Psychol. 2019;38:502–508. doi: 10.1037/hea0000716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Friedrich A, Schlarb AA. Let’s talk about sleep: a systematic review of psychological interventions to improve sleep in college students. J Sleep Res. 2018;27:4–22. doi: 10.1111/jsr.12568. [DOI] [PubMed] [Google Scholar]
- 23.Soetrisno , Sulistyowati S, Ardhianto A, Hadi S. The effect of logotherapy on the expressions of cortisol, HSP70, Beck Depression Inventory (BDI), and pain scales in advanced cervical cancer patients. Health Care Women Int. 2017;38:91–99. doi: 10.1080/07399332.2016.1237952. [DOI] [PubMed] [Google Scholar]
- 24.Lagunas-Cruz MDC, Valle-Mendiola A, Trejo-Huerta J, Rocha-Zavaleta L, Mora-García ML, Gutiérrez-Hoya A, Weiss-Steider B, Soto-Cruz I. IL-2 induces transient arrest in the G1 phase to protect cervical cancer cells from entering apoptosis. J Oncol. 2019;2019:7475295. doi: 10.1155/2019/7475295. [DOI] [PMC free article] [PubMed] [Google Scholar]