

Abstract
A 38-year-old asymptomatic man was referred by his general practitioner for a 3/6 systolic heart murmur, which was detected during a routine consultation. Echocardiography revealed a parachute mitral valve associated with a parachute-like membrane, causing significant subaortic obstruction that was eventually surgically resected with an excellent postoperative outcome. (Level of Difficulty: Beginner.)
Key Words: congenital heart disease, echocardiography, mitral valve, MR sequences
Abbreviations and Acronyms: AMVT, accessory mitral valve tissue; LVOT, left ventricular outflow tract; MRI, magnetic resonance imaging; PMV, parachute mitral valve
Graphical abstract

A 38-year-old asymptomatic man was referred by his general practitioner for a 3/6 systolic heart murmur, which was detected during a routine…
Case
History of presentation
A 38-year-old asymptomatic white male consulted for a routine checkup with his general practitioner who noticed a 3/6 protomesosystolic heart murmur at the left lower sternal border. The rest of the physical examination was normal. The patient was referred to the authors’ outpatient clinic for a transthoracic echocardiogram, which showed an abnormal mitral valve with likely 1 single posteromedial papillary muscle but without significant valve dysfunction. Attached to the anterior mitral leaflet was a supplementary mobile structure protruding into the left ventricular outflow tract (LVOT), causing an obstruction. The severity of LVOT obstruction was difficult to assess, but a peak velocity of almost 4 m/s (maximal gradient, 47 mm Hg) was measured using a Pedoff transducer in nonstandard right parasternal views (Figure 1, Video 1).
Learning Objectives
-
•
Transthoracic echocardiography is the examination of choice in the presence of a new or loud (≥3/6) systolic heart murmur.
-
•
Parachute mitral valve is a rare congenital anomaly, usually diagnosed in childhood, which is defined as the attachment of all mitral chordae tendinae to 1 papillary muscle, which typically leads to mitral stenosis and is often associated with left ventricular outflow obstructions.
-
•
A multidisciplinary team approach should be encouraged in associated congenital cardiac anomalies, in which no specific recommendations apply.
Figure 1.

Transthoracic Echocardiography
(A) Accessory mitral valve tissue (AMVT) protruding through the aortic valve, parasternal long-axis view. (B) AMVT attached to the anterior mitral leaflet (AML), parasternal short-axis view. (C) Single posteromedial papillary muscle (PM), parasternal short-axis view. (D) High velocities in the left ventricular outflow tract measured by continuous wave Doppler (Pedoff transducer), nonstandard right parasternal view. See Video 1.
Online Video 1.
Transthoracic Echocardiography
AVMT membrane protruding through the AV and attached to the AML, parasternal long-axis view.
Differential diagnosis
The supplementary echo structure inserted to the anterior mitral leaflet could correspond to a vegetation or to a primary or secondary cardiac tumor. However, in the absence of symptoms or signs and of any mitral valve dysfunction, the first differential diagnosis was a congenital abnormal mitral valve, likely a parachute mitral valve (PMV), associated with supernumerary tissue causing LVOT obstruction.
Investigations
Transesophageal echocardiography visualized a parachute-like structure attached to the anterior mitral leaflet and protruding through the aortic valve. In short-axis views, the obstruction was well characterized in the LVOT with blood only flowing around the parachute-like structure, which seemed impermeable (Figure 2, Videos 2 and 3). Cardiac resonance magnetic imaging did not reveal any other congenital defects but confirmed the PMV with all chordae attached to the posteromedial papillary muscle. A very small anterolateral papillary muscle was detected without any attachment to it. The parachute-like membrane was better characterized as a membranous accessory mitral valve tissue (AMVT) with insertions on both the anterior mitral leaflet and the posteromedial papillary muscle (Figure 3, Video 4). Maximal cycle ergometer exercise testing showed only a mild reduction of exercise capacity, corresponding to 8.5 metabolic equivalent of task (78% of predicted value) with a normal heart rate but a blunted blood pressure response with a peak value of 170/75 mm Hg. Finally, exercise echocardiography revealed a significant increase of LVOT obstruction with a peak measurable gradient of 60 mm Hg.
Figure 2.

Transesophageal Echocardiography
(A) AVMT membrane protruding through the AV and attached to the AML, mid-esophageal long-axis view. (B) AVMT membrane protruding between opened AL, mid-esophageal short-axis view. (C) Anterograde aortic flow around the AVMT membrane on color Doppler, mid-esophageal long-axis view. (D) Anterograde aortic flow around AVMT membrane on color Doppler, mid-esophageal short-axis view. See Videos 2 and 3. AL = aortal valve leaflets; AV = aortic valve; other abbreviations as in Figure 1.
Online Video 2.
Transesophageal Echocardiography
AVMT membrane protruding through the AV, mid-esophageal long-axis view.
Online Video 3.
Transesophageal Echocardiography
Anterograde aortic flow around AVMT membrane on color Doppler with non-significant AV regurgitation, mid-esophageal biplane view.
Figure 3.

Cardiac MRI
AMVT attached to both the AML and the posteromedial PM on a long-axis view, cine cardiac MRI images. See Video 4. LA = left atrium; LV = left ventricle; MRI = magnetic resonance imaging; other abbreviations as in Figure 1.
Online Video 4.
Cardiac MRI
AMVT attached to both AML and posteromedial PM on long-axis view, cine cardiac MRI images.
Management
This case was discussed in a multidisciplinary meeting with congenital heart disease specialists and congenital cardiac surgeons. Those in favor of an intervention pointed out the presence of significant LVOT obstruction that could eventually become symptomatic or even cause sudden death and the possible thromboembolic risk related to the presence of a significant amount of AMVT. Those not in favor of an intervention noted the absence of symptoms and the risk of destabilizing the geometry of the mitral valve by excising AMVT, which could require mitral valve repair or even replacement. The patient was informed of the risk-benefit balance and finally opted for surgery. Open heart surgery with subtotal resection of the parachute-like membrane through aortotomy was performed (Figure 4). Great care was taken to avoid injury of primary chordae and subsequent destabilization of the mitral valve. A small part of the AMVT was left in place because it was too close to the anterior mitral leaflet to allow resection without risking significant valve insufficiency.
Figure 4.
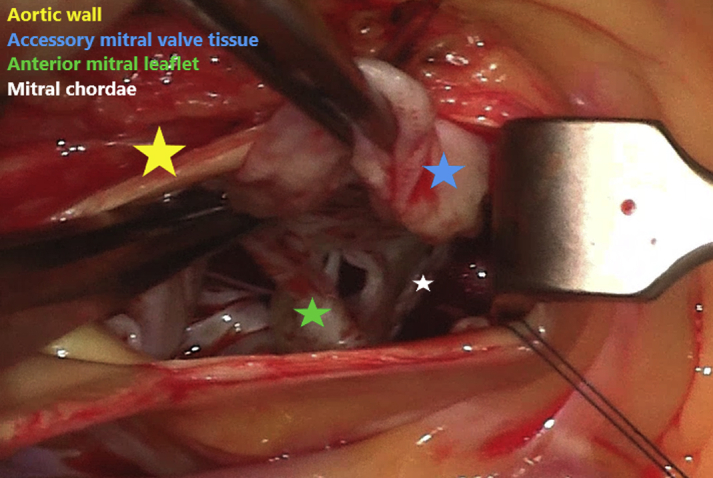
Surgical View of the Accessory Mitral Valve Tissue
Discussion
PMV is a rare congenital anomaly defined as the attachment of all mitral chordae tendinae to one papillary muscle. Its origin seems to be an abnormal division of the predecessor of the papillary muscle between the 5th and 19th weeks of gestation, forcing them to condense into a single muscle. The chordae tendinae in PMV are often underdeveloped and hence short and thick, leading to decreased mobility of the valve leaflets causing mitral stenosis. Mitral regurgitation is also often present due to a prolapsing mechanism. True PMV is distinguished from parachute-like mitral valve, defined as 2 asymmetrical papillary muscles with most of the chordae attached to 1 of them, the small anterolateral papillary muscle is located higher in the left ventricular wall (1). Most cases of PMV are associated with other congenital heart disorders. Shone et al. (2) described a classical association of 4 obstructive malformations known as Shone’s complex and consisting of PMV with a supravalvular ring of the left atrium, subaortic stenosis, and coarctation of the aorta. Most patients are symptomatic during childhood, and asymptomatic PMV in adults is a rare condition. Hakim et al. (3) reported 10 cases of isolated PMV discovered in adults, only 1 of whom was asymptomatic at the time of diagnosis.
Evidence is scarce about the management of asymptomatic subaortic obstructions in published studies (4). Most often it is caused by a membrane attached to the aortic valve, causing valvular dysfunction. In the present case, subaortic obstruction was caused by this large AMVT prolapsing into the LVOT. AMVT is a rare condition, with an incidence of 1/26,000 persons according to Prifti et al. (5), and none of the reported cases were similar to the present case (6,7).
Follow-up
Perioperative outcome showed successful relief of the obstruction by the AMVT and mild mitral regurgitation. Postoperative course was uneventful with the exception of a readmission 2 weeks after discharge for pericarditis, successfully treated by using nonsteroidal anti-inflammatory drugs. The patient participated in a cardiac rehabilitation program and showed significant improvement of exercise capacity (Table 1). He remained totally asymptomatic without exercise intolerance and transthoracic echocardiography at 6 months did not show any progression of mitral regurgitation.
Table 1.
Evolution of Exercise Capacity Before and 6 Months After Surgery∗
| Before Surgery | 6 Months After Surgery | |
|---|---|---|
| Power output (W) | 161 | 238 |
| Metabolic equivalent of task | 8.5 | 10 |
| Percentage of predicted value∗ | 78 | 114 |
The percentage of predicted value presented in the table are derived from equations of: Hansen JE, Sue DY, Wasserman K. Predicted values for clinical exercise testing. Am Rev Respir Dis 1984;129:S49–55.
Conclusions
This paper describes the case of an incidentally diagnosed PMV that was unusually associated with a large parachute-like membranous AMVT causing significant LVOT obstruction and that was successfully resected by open heart surgery.
Footnotes
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Informed consent was obtained for this case.
Appendix
For supplemental videos, please see the online version of this paper.
References
- 1.Oosthoek P.W., Wenink A.C., Wisse L.J., Gittenberger-de Groot A.C. Development of the papillary muscles of the mitral valve: morphogenetic background of parachute-like asymmetric mitral valves and other mitral valve anomalies. J Thorac Cardiovasc Surg. 1998;116:36–46. doi: 10.1016/S0022-5223(98)70240-5. [DOI] [PubMed] [Google Scholar]
- 2.Shone J.D., Sellers R.D., Anderson R.C., Adams P., Jr., Lillehei C.W., Edwards J.E. The developmental complex of “parachute mitral valve,” supravalvular ring of left atrium, subaortic stenosis, and coarctation of aorta. Am J Cardiol. 1963;11:714–725. doi: 10.1016/0002-9149(63)90098-5. [DOI] [PubMed] [Google Scholar]
- 3.Hakim F.A., Kendall C.B., Alharthi M., Mancina J.C., Tajik J.A., Mookadam F. Parachute mitral valve in adults-a systematic overview. Echocardiography. 2010;27:581–586. doi: 10.1111/j.1540-8175.2009.01143.x. [DOI] [PubMed] [Google Scholar]
- 4.Stout K.K., Daniels C.J., Aboulhosn J.A. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73:e81–e192. doi: 10.1016/j.jacc.2018.08.1029. [DOI] [PubMed] [Google Scholar]
- 5.Prifti E., Bonacchi M., Bartolozzi F., Frati G., Leacche M., Vanini V. Postoperative outcome in patients with accessory mitral valve tissue. Med Sci Monit. 2003;9:RA126–RA133. [PubMed] [Google Scholar]
- 6.Li Y., Hu Y., Wang J., Liu L. A rare case of accessory mitral valve tissue causing left ventricular outflow tract obstruction associated with parachute mitral valve, ventricular septal defect, bicuspid aortic valve, unruptured aneurysm of aortic sinus: a case report. Eur Heart J Case Rep. 2018;2:yty082. doi: 10.1093/ehjcr/yty082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nikolic A., Joksimovic Z., Jovovic L. Exuberant accessory mitral valve tissue with possible true parachute mitral valve: a case report. J Med Case Rep. 2012;6:292. doi: 10.1186/1752-1947-6-292. [DOI] [PMC free article] [PubMed] [Google Scholar]