

Abstract
Background
In many studies, vitamin D has been found to be low in COVID-19 patients. In this study, we aimed to investigate the relationship between clinical course and inhospital mortality with parenteral administration of high-dose vitamin D3 within the first 24 h of admission to patients who were hospitalized in the intensive care unit (ICU) because of COVID-19 with vitamin D deficiency.
Methods
This study included 175 COVID-19 patients with vitamin D deficiency [25(OH) D <12 ng/mL] who were hospitalized in the ICU. Vitamin D3 group (n = 113) included patients who received a single dose of 300,000 IU vitamin D3 intramuscularly. Vitamin D3 was not administered to the control group (n = 62).
Results
Median C-reactive protein level was 10.8 mg/dL in the vitamin D3 group and 10.6 mg/dL in the control group (p = 0.465). Thirty-nine percent (n = 44) of the patients in the vitamin D3 group were intubated endotracheally, and 50% (n = 31) of the patients in the control group were intubated endotracheally (p = 0.157). Parenteral vitamin D3 administration was not associated with inhospital mortality by multivariate logistic regression analysis. According to Kaplan–Meier survival analysis, the median survival time was 16 d in the vitamin D3 group and 17 d in the control group (log-rank test, p = 0.459).
Conclusion
In this study, which was performed for the first time in the literature, it was observed that high-dose parenteral vitamin D3 administration in critical COVID-19 patients with vitamin D deficiency during admission to the ICU did not reduce the need for intubation, length of hospital stay, and inhospital mortality.
Subject terms: Metabolic bone disease, Risk factors, Infectious diseases, Malnutrition
Introduction
Cases of coronavirus disease 2019 (COVID-19) were first reported in late December 2019 in Wuhan, located in the Hubei province of central China. However, researchers define the period between mid-October and mid-November 2019 as the plausible interval when the first case of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in Hubei province [1]. In February 2020, the World Health Organization designated the disease COVID-19, which stands for COVID-19 [2].
The inflammatory response plays a critical role in COVID-19, and inflammatory cytokine storm increases the severity of COVID-19 [3, 4]. Cytokine storm results from dysregulation of the innate immune system with an outpouring of proinflammatory cytokines and chemokines, leading to abnormal activation of the adaptive immune pathway [5]. While the COVID-19-specific CD8(+) T cells and specific antibodies produced by B cells are essential in eliminating the virus, uncontrolled inflammation and cytokine release can cause destructive injury to the lungs and other organs [6].
Vitamin D has immunomodulatory functions and plays an anti-inflammatory role, particularly in viral infections [7–10]. In laboratory studies, vitamin D has been shown to stimulate the expression of both innate and adaptive immune function receptors in the respiratory tract [11–15]. It also increases the synthesis of cathelicidins and defensins, which are the main antimicrobial proteins in the body. It decreases viral replication rates and reduces the synthesis of proinflammatory cytokines, thereby reducing lung tissue damage caused by inflammation. Expression of inflammatory cytokines (e.g., IL-1α, IL-1β, and tumor necrosis factor-α) was inhibited by vitamin D and its insufficiency was associated with overexpression of Th1 cytokines [16].
At the early stages of COVID-19, a protective immune response is responsible for eliminating the virus and, therefore, strategies to improve immune responses are important [17]. As the disease progresses, lung inflammation and fibrosis occur due to the release of proinflammatory cytokines, namely interleukin (IL)-1B and IL-18, by activated macrophages and type 1 T helper (Th1) immune cells [18].
Recent studies have shown that low vitamin D levels in COVID-19 patients are associated with the severity of diseases and mortality [19–21]. Optimal serum levels of 25-hydroxyvitamin D have been suggested to have immunomodulatory and anti-inflammatory properties and could benefit COVID-19 patients [22, 23]. Whether vitamin D therapy is effective as an adjunctive immunomodulatory agent in the treatment of most diseases is controversial owing to heterogeneous findings from the clinical trials. No specific study has investigated the effect of high-dose parenteral vitamin D3 administration on the clinical course and mortality of patients with critically ill COVID-19 admitted to the intensive care unit (ICU) with vitamin D deficiency.
In this study, we aimed to investigate the effect of parenteral high-dose vitamin D3 (300,000 IU) administration on clinical course and inhospital mortality within the first 24 h of admission to critically ill patients hospitalized in the ICU with COVID-19 and vitamin D deficiency.
Materials and methods
This study included 175 critical patients with vitamin D deficiency who were admitted to the ICU of Şırnak State Hospital (a designated pandemic hospital in Turkey) with the diagnosis of COVID-19 between March 15, 2020 and November 30, 2020. SARS-CoV-2 positivity was based on the results of the real-time reverse transcriptase polymerase chain reaction test of nasopharyngeal and oropharyngeal swabs.
The patients admitted to the ICU in our study did not have any previous history of hospitalization or admission to the hospital. The patients in our study consisted of those who presented to the Emergency Department for the first time due to severe hypoxic symptoms (such as dyspnea, hypoxia, and tachypnea) and then had a positive COVID-19 swab result. After obtaining a positive result for the COVID-19 swab at the Emergency Department, these patients were admitted to the ICU.
One hundred seventy-five patients included in the study were divided into two groups as vitamin D3 group (n = 113) and the control group (n = 62). In the first 24 h of admission of critically ill patients in the vitamin D3 group, 300,000 IU of vitamin D3 (Devit-3 ampoule, Deva company) was administered, confirming COVID-19 diagnosis. The patients who did not receive vitamin D3 were named the control group.
Blood samples were taken within the first hour of admission to the ICU. 25(OH) D, calcium, phosphorus, magnesium, albumin, urea, creatinine, aspartate aminotransferase, alanine aminotransferase, C-reactive protein (CRP), and D-dimer levels were measured in blood samples. 25 (OH) D levels were analyzed using the Cobas 6000 analyzer (Roche Diagnostics, Germany) and assessed by a chemiluminescent immunoassay.
Vitamin D deficiency was defined as a 25(OH)D level of <12 ng/mL (30 nmol/L).
The corrected calcium level was calculated using the following formula:
Corrected calcium (mg/dL) = measured total Ca (mg/dL) + 0.8 (4.0 − serum albumin [g/dL]), where 4.0 represents the average albumin level.
Information was obtained from the hospital management system and patients’ relatives, and the presence of comorbid diseases was recorded. Both groups were compared in terms of laboratory results, length of stay in the ICU, endotracheal intubation rate, and mortality.
The study protocol was approved by the local ethics committee (number: 2020/2318). Written informed consent was obtained from patients (when possible) or from their authorized representatives.
Exclusion criteria
Patients with previous use of vitamin D preparations, patients with hypercalcemia, kidney disease, liver disease, hypoparathyroidism, pregnancy status, and musculoskeletal disease were excluded from the study. Apart from this, all patients over 18 years old were included in the study.
Statistical analyses
The data were analyzed statistically using Statistical Package for Social Sciences for Windows v.22.0 program. Continuous variables were presented as median (interquartile range [IQR]) values, and categorical variables were presented as frequency rates and percentages. Chi-squared test was used to assess between-group differences with respect to categorical variables, while Mann–Whitney test was used to assess those with respect to nonparametric continuous variables. Univariate and multivariate logistic regression analyses were used to detect the predictors of mortality. Kaplan–Meier survival curves and log-rank tests were used to examine the overall survival. Statistical significance was defined as two‐sided P values ≤0.05.
Results
Vitamin D3 group, which received high-dose parenteral vitamin D3 treatment, consisted of 113 critically ill patients, while control group, which did not receive high-dose parenteral vitamin D3 therapy, consisted of 62 critically ill patients. A higher rate of males was observed in both groups in terms of gender (61% vs. 58%, p = 0.699). No difference was found in median age between vitamin D3 and the control group (74 years and 75 years, respectively, p = 0.431). The proportion of patients over the age of 65 was 60% (n = 68) in the vitamin D3 group and 70% (n = 43) in the control group (p = 0.228). When both groups were compared in terms of comorbid diseases, hypertension (45%), diabetes mellitus (41%), chronic lung disease (36%), cardiovascular disease (35%), cerebrovascular disease (14%), and cancer (6%) were the most common in total (Table 1). Among the comorbid diseases, only cardiovascular diseases were found to be significantly higher in the nonsurvivor group. However, there was no significant difference between the vitamin D3 and control group in terms of comorbid diseases.
Table 1.
Comorbid diseases of survivors and nonsurvivors.
| Comorbidity | Survivor (n = 102) |
Nonsurvivor (n = 73) |
Total (n = 175) |
P value |
|---|---|---|---|---|
| Hypertension | 40 (39%) | 39 (53%) | 79 (45%) | 0.063 |
| Diabetes mellitus | 38 (37%) | 34 (46%) | 72 (41%) | 0.217 |
| Cardiovascular disease | 28 (27%) | 34 (46%) | 62 (35%) | 0.009 |
| Chronic lung disease | 36 (35%) | 27 (37%) | 63 (36%) | 0.818 |
| Cerebrovascular disease | 14 (13%) | 10 (14%) | 24 (14%) | 0.996 |
| Cancer | 7 (6%) | 3 (4%) | 10 (6%) | 0.439 |
| Number of comorbid diseases | ||||
| 0 | 6 (6%) | 1 (1%) | 7 (4%) | 0.133 |
| 1 | 51 (50%) | 20 (27%) | 71 (40%) | 0.003 |
| 2 | 28 (27%) | 32 (43%) | 60 (34%) | 0.024 |
| 3 | 12 (11%) | 17 (23%) | 19 (10%) | 0.043 |
| ≥4 | 5 (5%) | 3 (4%) | 8 (4%) | 0.805 |
Categorical data shown as number (percentage). Chi-square test was used.
p < 0.05: significant (shown in bold).
CRP and D-dimer levels, which are the markers of inflammation, were not different between both groups. Critical patients in the vitamin D3 group had a median hospital stay of 9 days (IQR, 6–16 days) in the ICU, whereas critical patients in the control group also had a median hospital stay of 9 days (IQR, 5–17 days) (p = 0.649). While 39% (44) of the patients were endotracheal intubated in the vitamin D3 group, 50% (n = 31) of the patients were endotracheal intubated in the control group (p = 0.157). Inhospital mortality rate in the vitamin D3 group was 38% (n = 43) while it was 48% (n = 30) in the control group (p = 0.185). The total inhospital mortality rate of critical COVID-19 patients enrolled in the ICU was found to be 41% (n = 73). The demographic, laboratory, and clinical parameters of the groups are shown in Table 2.
Table 2.
Demographic and clinical results of the groups.
| Parameters | Vitamin D3 group (n = 113) |
Control group (n = 62) |
Total (n = 175) |
P value |
|---|---|---|---|---|
| Sex | ||||
| Male | 69 (61%) | 36 (58%) | 105 (60%) | 0.699 |
| Female | 44 (39%) | 26 (42%) | 70 (40%) | |
| Age, y, (IQR) | 74 (60–81) | 75 (62–83) | 74 (61–82) | 0.431 |
| Age (stratified) | ||||
| <50 | 4 (4%) | 4 (6%) | 8 (4%) | 0.378 |
| 50–65 | 41 (36%) | 15 (24%) | 56 (32%) | 0.101 |
| >65 | 68 (60%) | 43 (70%) | 111 (63%) | 0.228 |
| 25 (OH) D, ng/mL, (IQR) | 6.65 (5.06–9.1) | 7.14 (5.17–8.21) | 6.76 (5.07–8.54) | 0.512 |
| Corrected calcium, mg/dL, (IQR) | 8.1 (7.6–8.6) | 8.17 (7.77–8.72) | 8.1 (7.66–8.6) | 0.269 |
| Phosphor, mg/dL, (IQR) | 3.1 (2.3–4.1) | 3 (2.4–3.68) | 3.1 (2.4–4) | 0.398 |
| Magnesium, mg/dL, (IQR) | 1.8 (1.6–1.9) | 1.9 (1.7–2.1) | 1.8 (1.6–2) | 0.192 |
| Albumin, g/dL, (IQR) | 2.7 (2.31–3.19) | 2.73 (2.28–3.36) | 2.7 (2.31–3.2) | 0.819 |
| Urea, mg/dL, (IQR) | 55 (34–86) | 46 (31–80) | 50 (34–86) | 0.241 |
| Creatine, mg/dL, (IQR) | 1.1 (0.81–1.45) | 1.01 (0.74–1.42) | 1.06 (0.81–1.46) | 0.177 |
| AST, U/L, (IQR) | 29 (20–45) | 23 (16–45) | 28 (18–45) | 0.375 |
| ALT, U/L, (IQR) | 22 (15–40) | 24 (14–45) | 22 (15–43) | 0.509 |
| CRP, mg/dl, (IQR) | 10.8 (6.1–16.4) | 10.6 (5.5–16.25) | 10.85 (6.03–16.46) | 0.465 |
| D-dimer, ug/L, (IQR) | 1175 (750–2880) | 1290 (734–3587) | 1230 (750–2960) | 0.248 |
| Inhospital mortality (to November 30, 2020) | 43 (38%) | 30 (48%) | 73 (41%) | 0.185 |
| Lenght of stay, day, (IQR) | 9 (6–16) | 9 (5–17) | 9 (6–16) | 0.649 |
| Endotracheal intubated | 44 (39%) | 31 (50%) | 75 (43%) | 0.157 |
Categorical data shown as number (percentage). Non-normally distributed continuous variables displayed as median (IQR). Chi-square test was used to analyze the categorical variables. Mann–Whitney’s test was used for nonparametric continuous variables.
25 (OH) D 25-hydroxy vitamin D, IQR interquartile range, AST aspartate aminotransferase, ALT Ala-nine aminotransferase, CRP C-reactive protein.
When the patients included in the study were analyzed as survivors and nonsurvivors, it was found that 102 patients were alive and 73 patients were dead (Fig. 1). The median age of the survivors was 70 years (IQR, 60–80 year), whereas that of the nonsurvivors was 76 years (IQR, 62–82 year) (p = 0.199). High-dose parenteral vitamin D3 was administered in 69% (n = 70) of the survivors, whereas parenteral vitamin D3 was administered in 59% (n = 43) of the nonsurvivors (p = 0.185). The median CRP level of the nonsurvivor group was significantly higher than that of the survivor group (14.14 mg/dL vs. 7.57 mg/dL, respectively, p < 0.001). While 14% (n = 15) of the survivors were intubated endotracheally, 82% (n = 60) of the nonsurvivors were intubated endotracheally (p < 0.001). Corrected calcium and albumin levels were lower in the nonsurvivor group. The comparison of demographic, laboratory and clinical parameters of the survivor and nonsurvivor groups are shown in Table 3.
Fig. 1.
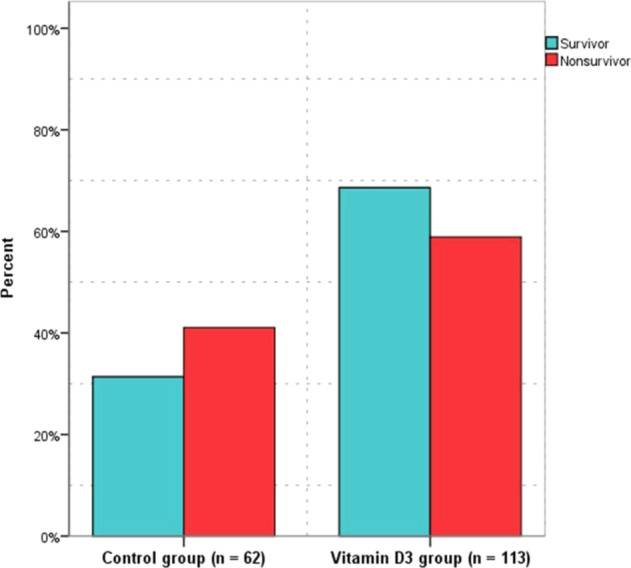
Percentage of survivors and nonsurvivors belonging to groups.
Table 3.
Comparison of demographic and clinical results of survivors and nonsurvivors.
| Parameters | Survivor (n = 102) |
Nonsurvivor (n = 73) |
P value |
|---|---|---|---|
| Sex | |||
| Male | 59 (58%) | 46 (63%) | 0.491 |
| Female | 43 (42%) | 27 (37%) | |
| Age, y, (IQR) | 70 (60–80) | 76 (62–82) | 0.199 |
| Age (stratified) | |||
| ≤50 | 6 (6%) | 2 (3%) | 0.326 |
| 50–65 | 37 (36%) | 19 (26%) | 0.152 |
| ≥65 | 59 (58%) | 52 (71%) | 0.070 |
| 25 (OH)D, ng/mL, (IQR) | 6.88 (5–8.21) | 6.72 (5.66–8.31) | 0.421 |
| Corrected calcium, mg/dL, (IQR) | 8.29 (7.86–8.9) | 7.8 (7.5–8.3) | <0.001 |
| Phosphor, mg/dL, (IQR) | 3.1 (2.5–4) | 3 (2.2–4.1) | 0.623 |
| Magnesium, mg/dL, (IQR) | 1.92 (1.67–2.05) | 1.83 (−1.64–2.06) | 0.522 |
| Albumin, g/dL, (SD) | 2.86 (0.6) | 2.61 (0.55) | 0.005 |
| Urea, mg/dL, (IQR) | 47 (34–74) | 62 (28–91) | 0.575 |
| Creatine, mg/dL, (IQR) | 1.03 (0.79–1.53) | 1.11 (0.89–1.38) | 0.129 |
| AST, U/L, (IQR) | 24 (18–45) | 29 (17–45) | 0.569 |
| ALT, U/L, (IQR) | 22 (16–45) | 22 (14–40) | 0.157 |
| CRP, mg/dl, (IQR) | 7.57 (3.85–13.75) | 14.14 (10.57–17.41) | <0.001 |
| D-dimer, ug/L, (IQR) | 1200 (751–2950) | 1260 (731–2960) | 0.928 |
| Received high doses parenteral vitamin D3 | 70 (69%) | 43 (59%) | 0.185 |
| Length of stay, day, (IQR) | 9 (5–19) | 8 (6–16) | 0.685 |
| Endotracheal intubated | 15 (14%) | 60 (82%) | <0.001 |
Categorical data shown as number (percentage). Non-normally distributed continuous variables displayed as median (IQR). Chi-square test was used to analyze the categorical variables. Mann–Whitney’s test was used for nonparametric continuous variables.
25(OH) D 25-hydroxy vitamin D, IQR interquartile range, AST aspartate aminotransferase, ALT alanine aminotransferase, CRP C-reactive protein.
p < 0.05: significant (shown in bold).
In multivariate logistic regression analysis of clinical parameters, corrected calcium level, CRP level, and endotracheal intubation rate were found to be associated with inhospital mortality (Table 4). However, 25(OH) D level and administration of high-dose parenteral vitamin D3 were not found to be associated with inhospital mortality.
Table 4.
Univariate and multivariate logistic regression analysis of the relationship between mortality and clinical parameters.
| Parameters | Crude OR (95% Cl) | P value | Adjusted OR (95% Cl) | P value |
|---|---|---|---|---|
| Gender (male) | 1.24 (0.67–2.3) | 0.491 | 2.1 (0.79–5.6) | 0.135 |
| Age, y | 1.01 (0.99–1.04) | 0.131 | 1.02 (0.99–1.06) | 0.091 |
| 25(OH)D, ng/mL | 1.06 (0.93–1.21) | 0.359 | 1.3 (1.02–1.64) | 0.058 |
| Corrected calcium, mg/dL | 0.53 (0.35–0.79) | 0.002 | 0.29 (0.14–0.62) | 0.002 |
| Albumin, g/dL | 1.07 (0.89–1.29) | 0.427 | 2.3 (0.91–5.76) | 0.075 |
| CRP, mg/dl | 1.1 (1.05–1.15) | <0.001 | 1.12 (1.04–1.2) | 0.002 |
| Endotracheal intubated | 26 (11.8–60.3) | <0.001 | 57 (17.8–182.3) | <0.001 |
| Received high doses parenteral vitamin D3 | 0.65 (0.35–1.22) | 0.186 | 0.61 (0.23–1.6) | 0.320 |
25(OH)D 25-hydroxy vitamin D, CRP C-reactive protein, OR odds ratio, CI Confidence interval.
p < 0.05: significant (shown in bold).
According to the Kaplan–Meier survival analysis, the median survival time was 16 d (95% CI, 13.57–18.42) in the vitamin D3 group and 17 d (95% CI, 10.2–23.79) in the control group (Fig. 2; log-rank test, p = 0.459).
Fig. 2.
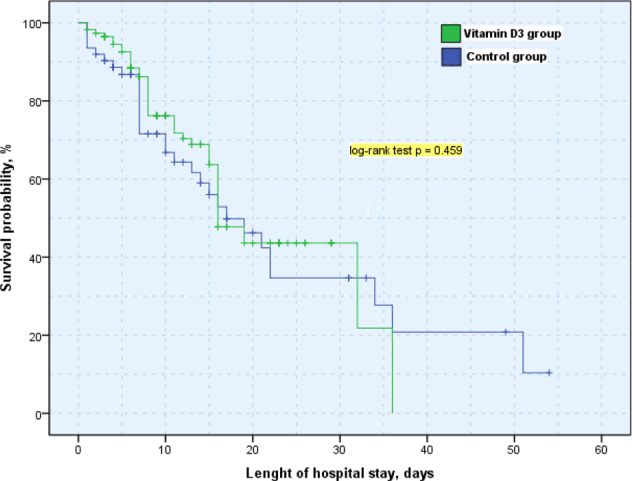
Survival of the groups according to Kaplan–Meier analysis.
Discussion
The majority of critical patients in the ICU included in our study were male with the median age of 74 years. This finding was similar to the studies in the literature [24–27]. Among the comorbid diseases, only cardiovascular diseases were found to be significantly higher in the nonsurvivor group. There was no statistically significant difference between the two groups in terms of other comorbid diseases. Similar results were obtained in studies conducted in the literature [28–30].
In many studies conducted by researchers, 25(OH) D levels was found to be low in COVID-19 patients and was associated with the severity of the disease [19–21]. In a study conducted by Meltzer et al. 489 patients who had PCR tests and 25(OH) D levels measured in the last 1 year were examined; the rate of patients who were positive for COVID-19 was found to be 12.2% in the group with sufficient vitamin D levels and 21.6% in the group with vitamin D deficiency [31]. In another study involving 191,779 patients with COVID-19 tests at the US National Clinical Laboratory, people with 25(OH) D <20 ng/mL had a 54% higher risk of COVID-19 compared to people with 30–34 ng/mL of vitamin D level [32]. Similar to the literature, the 25(OH) D levels of COVID-19 critical patients in the ICU was found to be low in our study.
In a recent study by Murai et al. 240 hospitalized patients with COVID-19 who were moderate to severely ill were given a single oral dose of 200,000 IU vitamin D3. Between the vitamin D3 group (n = 120) and the placebo group (n = 120), there was no difference in length of stay and inhospital mortality rate [33]. In another study by Han et al. mechanically ventilated adult ICU patients showed that administering high doses of oral vitamin D3 (total vitamin D3 dose = 250,000 IU or 500,000 IU) did not differ between ICU length of stay and hospital mortality [34]. In the VITdAL-ICU study by Amrein et al. 492 critically ill patients (vitamin D3 group, n = 249; placebo group, n = 243) followed in the ICU. Monthly maintenance doses of 90,000 IU were given during the month. At the end of the study, the length of hospital stay and hospital mortality was not different between the groups [35].
In our study, no difference was observed in the length of hospital stay, endotracheal intubation, and mortality rates in critical patients in the ICU after high-dose parenteral D3 administration in the early period. In another study with 341,484 UK Biobank participants, no relationship was found between vitamin D level and the severity of COVID-19 and mortality [36].
Adequate vitamin D intake can be obtained through adequate sun exposure and a diet rich in vitamin D. The critical COVID-19 patients in our study were patients with malnutrition and advanced age comorbidities without adequate exposure to sunlight. Since nutrients have various roles in maintaining the function of the immune system, optimal nutrition is important in establishing an appropriate immune response [37]. Since nutritional problems and insufficient sunlight exposure can weaken the immune system, susceptibility to all infections, especially respiratory tract infection, can be observed. Therefore, as a sign of malnutrition, it can be said that patients with malnutrition may have a more severe infection as vitamin D levels reflect the nutritional level of the person rather than the direct effect of low vitamin D on the severe course of COVID-19 infection and high mortality rate.
Another reason why vitamin D administration did not show a difference in terms of mortality in our study may be because the administered vitamin D could not find enough time to show sufficient activity in the body due to the rapid progression of COVID-19, resulting in mortality in a short time.
A study by Castillo et al. showed that administering high doses of calcifediol to 76 patients hospitalized in the non-ICU diagnosed of COVID-19 reduces the need for ICU admission [38]. Our study included the therapeutic administration of vitamin D3 immediately after COVID-19 diagnosis based on the nasopharyngeal swab result. In addition, the patients who were enrolled in the study consisted of critical patients who developed severe acute respiratory distress syndrome (ARDS). We found that vitamin D3 was ineffective at this critical stage since severe ARDS developed in the patients. We believe that prophylactic vitamin D3 administration before the entry of SARS-CoV-2 or therapeutic vitamin D3 administration to clinically mild COVID-19 patients without developing severe ARDS may show immunomodulatory effects in such patients.
There are some limitations in our study. First, critical patients who were administered high doses of vitamin D3 during admission to the ICU resulted in death in a short time because of the rapid progression of COVID-19, which did not leave enough time for us to look at the control vitamin D level. Secondly, the study was conducted in a single center. Larger, multicenter studies are required to obtain more conclusive evidence.
Conclusion
Early administration of therapeutic high-dose parenteral vitamin D3 in critical COVID-19 patients in the ICU did not reduce the need for intubation, length of hospital stay, and inhospital mortality. The immunomodulatory effects of vitamin D3 may be observed with prophylactic administration before the diagnosis of COVID-19 infection or therapeutic administration in patients with mild symptoms of COVID-19 immediately after viral detection.
Supplementary information
{kind=link}
COMPETING INTERESTS
The authors declare no competing interests.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
The online version contains supplementary material available at 10.1038/s41430-021-00984-5.
References
- 1.Pekar J, Worobey M, Moshiri N, Scheffler K, Wertheim JO. Timing the SARS-CoV-2 index case in Hubei province. Science. 2021;eabf8003. 10.1126/science.abf8003. [DOI] [PMC free article] [PubMed]
- 2.World Health Organization. Director-General’s remarks at the media briefing on 2019-nCoV on 11 February 2020. http://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020. Accessed 12 Feb 2020.
- 3.Yang PH, Ding YB, Xu Z, Pu R, Li P, Yan J, et al. Increased circulating level of interleukin-6 and CD8+ T cell exhaustion are associated with progression of COVID-19. Infect Dis Poverty. 2020;9:161.. doi: 10.1186/s40249-020-00780-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zumla A, Hui DS, Azhar EI, Memish ZA, Maeurer M. Reducing mortality from 2019-nCoV: host-directed therapies should be an option. Lancet. 2020;395:e35–6. doi: 10.1016/S0140-6736(20)30305-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bilezikian JP, Bikle D, Hewison M, Castro ML, Formenti AM, Gupta A, et al. MECHANISMS IN ENDOCRINOLOGY: vitamin D and COVID-19. Eur J Endocrinol. 2020;183:R133–47. doi: 10.1530/EJE-20-0665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Abraham J, Dowling K, Florentine S. Can optimum solar radiation exposure or supplemented vitamin D intake reduce the severity of COVID-19 symptoms? Int J Environ Res Public Health. 2021;18:740.. doi: 10.3390/ijerph18020740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Charoenngam N, Holick MF. Immunologic effects of vitamin D on human health and disease. Nutrients. 2020;12:2097. doi: 10.3390/nu12072097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Grant WB, Lahore H, McDonnell SL, Baggerly CA, French CB, Aliano JL, et al. Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths. Nutrients. 2020;12:988.. doi: 10.3390/nu12040988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Prietl B, Treiber G, Pieber TR, Amrein K. Vitamin D and immune function. Nutrients. 2013;5:2502–21. doi: 10.3390/nu5072502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tamer G, Mesçi B. Role of vitamin D in the immune system. Turkjem. 2013;17:5–7. doi: 10.4274/Tjem.1938. [DOI] [Google Scholar]
- 11.Greiller CL, Suri R, Jolliffe DA, Kebadze T, Hirsman AG, Griffiths CJ, et al. Vitamin D attenuates rhinovirus-induced expression of intercellular adhesion molecule-1 (ICAM-1) and platelet-activating factor receptor (PAFR) in respiratory epithelial cells. J Steroid Biochem Mol Biol. 2019;187:152–9. doi: 10.1016/j.jsbmb.2018.11.013. [DOI] [PubMed] [Google Scholar]
- 12.Brockman-Schneider RA, Pickles RJ, Gern JE. Effects of vitamin D on airway epithelial cell morphology and rhinovirus replication. PLoS ONE. 2014;9:e86755. doi: 10.1371/journal.pone.0086755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chen Y, Zhang J, Ge X, Du J, Deb DK, Li YC. Vitamin D receptor inhibits nuclear factor κ B activation by interacting with IκB kinase β protein. J Biol Chem. 2013;288:19450–8. doi: 10.1074/jbc.M113.467670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Martineau AR, Jolliffe DA, Hooper RL, Greenberg L, Aloia JF, Bergman P, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 2017;356:i6583. doi: 10.1136/bmj.i6583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gombart AF, Borregaard N, Koeffler HP. Human cathelicidin antimicrobial peptide (CAMP) gene is a direct target of the vitamin D receptor and is strongly up-regulated in myeloid cells by 1,25-dihydroxyvitamin D3. FASEB J. 2005;19:1067–77. doi: 10.1096/fj.04-3284com. [DOI] [PubMed] [Google Scholar]
- 16.Hughes DA, Norton R. Vitamin D and respiratory health. Clin Exp Immunol. 2009;158:20–5. doi: 10.1111/j.1365-2249.2009.04001.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ebadi M, Montano-Loza AJ. Perspective: improving vitamin D status in the management of COVID-19. Eur J Clin Nutr. 2020;74:856–9. doi: 10.1038/s41430-020-0661-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Conti P, Ronconi G, Caraffa A, Gallenga CE, Ross R, Frydas I, et al. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by Coronavirus-19 (COVI-19 or SARS-CoV-2): anti-inflammatory strategies. J Biol Regul Homeost Agents. 2020;34. 10.23812/CONTI-E. [DOI] [PubMed]
- 19.Munshi R, Hussein MH, Toraih EA, Elshazli RM, Jardak C, Sultana N, et al. Vitamin D insufficiency as a potential culprit in critical COVID-19 patients. J Med Virol. 2021;93:733–40. doi: 10.1002/jmv.26360. [DOI] [PubMed] [Google Scholar]
- 20.Merzon E, Tworowski D, Gorohovski A, Vinker S, Cohen AG, Green I, et al. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: an Israeli population-based study. FEBS J. 2020;287:3693–702. doi: 10.1111/febs.15495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Maghbooli Z, Sahraian MA, Ebrahimi M, Pazoki M, Kafan S, Tabriz HM, et al. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLoS ONE. 2020;15:e0239799.. doi: 10.1371/journal.pone.0239799. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 22.Mitchell F. Vitamin-D and COVID-19: do deficient risk a poorer outcome? Lancet Diabetes Endocrinol. 2020;8:570.. doi: 10.1016/S2213-8587(20)30183-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Martineau AR, Forouhi NG. Vitamin D for COVID-19: a case to answer? Lancet Diabetes Endocrinol. 2020;8:735–6. doi: 10.1016/S2213-8587(20)30268-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Thomson RJ, Hunter J, Dutton J, Schneider J, Khosravi M, Casement A, et al. Clinical characteristics and outcomes of critically ill patients with COVID-19 admitted to an intensive care unit in London: a prospective observational cohort study. PloS ONE. 2020;15:e0243710. doi: 10.1371/journal.pone.0243710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Güven M, Gültekin H. Could serum total cortisol level at admission predict mortality due to coronavirus disease 2019 in the intensive care unit? A prospective study. Sao Paulo Med J. 2021;S1516-31802021005016206. 10.1590/1516-3180.2020.0722.R1.2302021. [DOI] [PMC free article] [PubMed]
- 26.Solmaz I, Özçaylak S, Alakuş ÖF, Kılıç J, Kalın BS, Güven M, et al. Risk factors affecting ICU admission in COVID-19 patients; Could air temperature be an effective factor? Int J Clin Pract. 2020;e13803. 10.1111/ijcp.13803. [DOI] [PubMed]
- 27.Asan A, Üstündağ Y, Koca N, Şimşek A, Sayan HE, Parildar H, et al. Do initial hematologic indices predict the severity of COVID-19 patients? Turk J Med Sci. 2020;10.3906/sag-2007-97. 10.3906/sag-2007-97. [DOI] [PMC free article] [PubMed]
- 28.Guan WJ, Liang WH, Zhao Y, Liang HR, Chen ZS, Li YM, et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. Eur Respir J. 2020;55:2000547.. doi: 10.1183/13993003.00547-2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Atkins JL, Masoli JAH, Delgado J, Pilling LC, Kuo CL, Kuchel GA, et al. Preexisting comorbidities predicting COVID-19 and mortality in the UK Biobank Community Cohort. J Gerontol A Biol Sci Med Sci. 2020;75:2224–30. doi: 10.1093/gerona/glaa183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gonçalves TJM, Gonçalves SEAB, Guarnieri A, Risegato RC, Guimarães MP, Freitas DCD, et al. Prevalence of obesity and hypovitaminosis D in elderly with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Clin Nutr ESPEN. 2020;40:110–4. doi: 10.1016/j.clnesp.2020.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Meltzer DO, Best TJ, Zhang H, Vokes T, Arora V, Solway J. Association of vitamin D status and other clinical characteristics with COVID-19 test results. JAMA Netw Open. 2020;3:e2019722.. doi: 10.1001/jamanetworkopen.2020.19722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kaufman HW, Niles JK, Kroll MH, Bi C, Holick MF. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS ONE. 2020;15:e0239252.. doi: 10.1371/journal.pone.0239252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Murai IH, Fernandes AL, Sales LP, Pinto AJ, Goessler KF, Duran CSC, et al. Effect of a single high dose of vitamin D3 on hospital length of stay in patients with moderate to severe COVID-19: a randomized clinical trial. JAMA. 2021;325:1053–60. doi: 10.1001/jama.2020.26848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Han JE, Jones JL, Tangpricha V, Brown MA, Brown LAS, Hao L, et al. High dose vitamin D administration in ventilated intensive care unit patients: a pilot double blind randomized controlled trial. J Clin Transl Endocrinol. 2016;4:59–65. doi: 10.1016/j.jcte.2016.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Amrein K, Schnedl C, Holl A, Riedl R, Christopher KB, Pachler C, et al. Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vitamin D deficiency: the VITdAL-ICU randomized clinical trial. JAMA. 2014;312:1520–30. doi: 10.1001/jama.2014.13204. [DOI] [PubMed] [Google Scholar]
- 36.Hastie CE, Pell JP, Sattar N. Vitamin D and COVID-19 infection and mortality in UK Biobank. Eur J Nutr. 2020;1–4. 10.1007/s00394-020-02372-4. [DOI] [PMC free article] [PubMed]
- 37.Calder PC. Nutrition, immunity and COVID-19. BMJ Nutr Prev Health. 2020;3:74–92. doi: 10.1136/bmjnph-2020-000085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Entrenas Castillo M, Entrenas Costa LM, Vaquero Barrios JM, Alcalá Díaz JF, Miranda JL, Bouillon R, et al. “Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: a pilot randomized clinical study”. J Steroid Biochem Mol Biol. 2020;203:105751.. doi: 10.1016/j.jsbmb.2020.105751. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.