

Abstract
Public health researchers and social scientists highlight the promise of network-based strategies to inform and enhance interventions that curb risky adolescent health behaviors. However, we currently lack an understanding of how different variants of network-based interventions shape the distribution of targeted behaviors. The current project considers the effectiveness of five targeting strategies that are designed to have differential impacts on the health of program participants versus non-participants. Using simulations that are empirically-grounded in 28 observed school-based networks from the PROSPER study, we evaluate how these approaches shape long-term alcohol use for intervention participants and non-participants, separately, and consider whether contextual factors moderate their success. Findings suggest that enrolling well-connected adolescents results in the lowest drinking levels for non-participants, while strategies that target groups of friends excel at protecting participants from harmful influences. These trends become increasingly pronounced in contexts characterized by higher levels of peer influence.
Keywords: Health interventions, social networks, empirically-grounded simulations, adolescents, alcohol use
Introduction
Intervention science points to social networks as a powerful lever to encourage healthy behavior changes, enhance population-wide diffusion, and sustain the adoption of pro-social practices (Centola 2018; Hunter et al. 2019; Valente 2012). Given that young people’s social connections are known to shape their risky health behaviors (Haas et al. 2010; de la Haye et al. 2011; McMillan 2019), interventions that incorporate network principles into their design hold promise for combating adolescent substance use (Hunter et al. 2019; Shelton et al. 2019). Using network properties to inform the selection of intervention participants is an efficient means to reduce population-wide substance use when programs can only be delivered to a segment of a school or community (Campbell et al. 2008, Starkey et al. 2009). A vital step in implementing these interventions is deciding which adolescents make the best targets for promoting positive behavior change, yet we currently have a limited understanding of the tradeoffs facing different approaches. Heeding the call for more work on evaluating network interventions strategies (Valente 2012), the current study uses an empirically-grounded computational experiment to evaluate the impact of five different targeting strategies for enrolling adolescents in a drinking intervention. Then, to gain further insight into each approach’s strengths and weaknesses, we focus on the alcohol use of intervention participants and non-participants separately and consider how contextual factors moderate program success.
Network-based intervention targeting strategies can be classified into various classes, of which two relate to how participants are selected: individual and segmentation approaches (Hunter et al. 2019; Valente 2012). Both strategies aim to improve population health by exploiting relational processes such as social learning, peer reinforcement, and status-seeking. To achieve these goals, each approach relies on distinct principles of network structure to identify program participants. Individual interventions target well-connected network members, while segmentation approaches focus their delivery on groups of individuals.
Individual-Based Targeting
Individual-based targeting strategies highlight the fact that people occupy different positions in social networks – in short, some of us are “better connected” than others (Valente 2012). Those individuals who are well-connected and occupy highly central network positions tend to have a greater volume of direct and indirect social ties, allowing them to reach and influence more peers when compared to less connected actors. Network-based intervention programs can use these structural patterns to their advantage by enrolling those individuals who are the most connected in their communities (Paluck et al. 2016; Valente and Pumpuang 2007). For instance, some campaigns are designed to equip participants with the necessary skills for spreading the positive messages learned in the intervention to those who did not participate (e.g., Starkey et al. 2009). These programs select peer leaders who are in optimal positions for diffusing information and teach them the necessary skills for encouraging positive health practices (Kelly 2004). Thus, targeting influential individuals can result in spillover effects that enhance the broader community’s well-being (Rulison et al. 2015).
Targeting actors in strategic, central positions is not only effective for spreading an intervention’s impact but can have an inhibitory effect on the diffusion of risky health behaviors. Oftentimes, central actors bridge disparate parts of a network, thereby enhancing their ability to impede the spread of risky behaviors across otherwise disconnected social circles (Valente 2012). As a result, network-based interventions still hold promise for curtailing adolescents’ risky behaviors even if peer-education components are unsuccessful or not included in the curriculum. For instance, since well-connected peers have greater potential to legitimize underage drinking (Cohen and Prinstein 2006), their abstinence is apt to positively influence others by altering groups norms about alcohol use (Rulison et al. 2015). Although these inhibitory aspects of network interventions are sometimes overlooked, they are key to our current focus given that they play a simple, yet powerful, role in promoting population health.
Central positions carry a downside in that they can also heighten one’s exposure to practices (Friedkin 2001), such as harmful drinking. For instance, across many school environments, adolescents in more central positions are more likely to report drinking alcohol when compared to their less popular peers (Fujimoto and Valente 2015; Knecht et al. 2010; Kreager et al. 2011). Part of the reason behind this trend is that adolescents with more social connections have a greater chance of being tied to peers who drink and can negatively influence their own behaviors. Hence, by targeting youth in prominent network positions, practitioners should not only thwart the diffusion of pro-drinking practices, but also capture high-risk youth (Paluck et al. 2016; Starkey et al. 2009; Valente 2012).
Segmentation-Based Targeting
Interventions taking a segmentation approach (Valente 2012) are designed to recruit pairs or groups of friends to participate in an intervention together (e.g., Harper et al. 2014; Minnis et al. 2014; Shaya et al. 2014). These strategies hold promise for reducing drinking because adolescents’ networks typically consist of multiple cliques, or friendship groups, that cluster together peers with similar demographic characteristics, ideologies, and behaviors (Urberg et al. 1995). For instance, previous work finds that young people tend to drink alcohol at similar rates as their friends (Osgood et al. 2013), a pattern attributed to two general processes: friend selection and peer influence. On one hand, individuals tend to select friends who share their behaviors (McPherson, Smith-Lovin, and Cook 2001), which helps explain the similar drinking behaviors observed in adolescent friend groups (Knecht et al. 2010). On the other hand, adolescents tend to adopt their friends’ drinking behaviors through some form of peer influence (Light et al. 2013), resulting in friendship groups that become increasingly homogenous over time.
Segmentation-based targeting campaigns aim to protect participants from various sources of harmful influence by enrolling participants’ direct connections, who can then provide positive reinforcement and buffer the spread of negative influences from indirect social ties. Group-based targeting strategies can also encourage friends to reinforce the salubrious behaviors learned from the program after it ceases (Harper et al. 2014; Shaya et al. 2014). If the positive effects of a group-based intervention dissipate for one participant, for example, their friends who also participated in the program can continue to provide protection from sources of negative influence. Although such interventions are less common than approaches that enroll influential individuals (Valente 2012), targeting dyads and groups can help ensure that participants abstain from drinking in the long run.
Beyond providing this protection, targeting self-defined groups can also help locate influential individuals in the absence of prior knowledge of the social network (which can be costly to obtain). This is because they leverage the “friendship paradox” (Feld 1991, Kim et al. 2015), whereby a non-uniform distribution of friendship volume across individuals necessitates that the average number of friends for a target sample is less than the average number of friends that friends of the target sample have. Thus, intervention strategies that adopt this approach should have greater success at locating the most central adolescents in a population than programs that randomly select participants.
Evaluating Intervention Strategies
Although network-based interventions generally lead to better outcomes than non-network strategies (Beheshti et al. 2017; Campbell et al. 2008; Valente and Vega Yon 2020), all too often the focus of such evaluations is at the population level, leaving the question of who is impacted unanswered. What tends to go overlooked is that individual and segmentation-based interventions are explicitly designed to affect different subsets of a population. As a result, network members are apt to experience the health benefits of these interventions at varying magnitudes, and in certain instances, targeting approaches may favor some individuals at the expense of others.
On the one hand, programs that target central, well-connected actors aim to capture individuals who can impede the diffusion of risky behaviors to non-participants, or those who did not partake in the intervention (Starkey et al. 2009). For example, an intervention that aims to enroll the most influential adolescents in a population may operationalize individual-level centrality as friendship indegree, defined as the number of times someone was named as a friend by other network members (see Figure 1A). Targeting high-indegree individuals is apt to reduce the diffusion of risky health behaviors and result in better outcomes for non-participants since these targets are linked to many of their peers directly (e.g., all of the light gray nodes in Figure 1A). However, these connections also leave high indegree individuals at greater risk of exposure to negative influences that could counteract the intervention’s impact, especially if targets are not tied to other participants.
Figure 1.
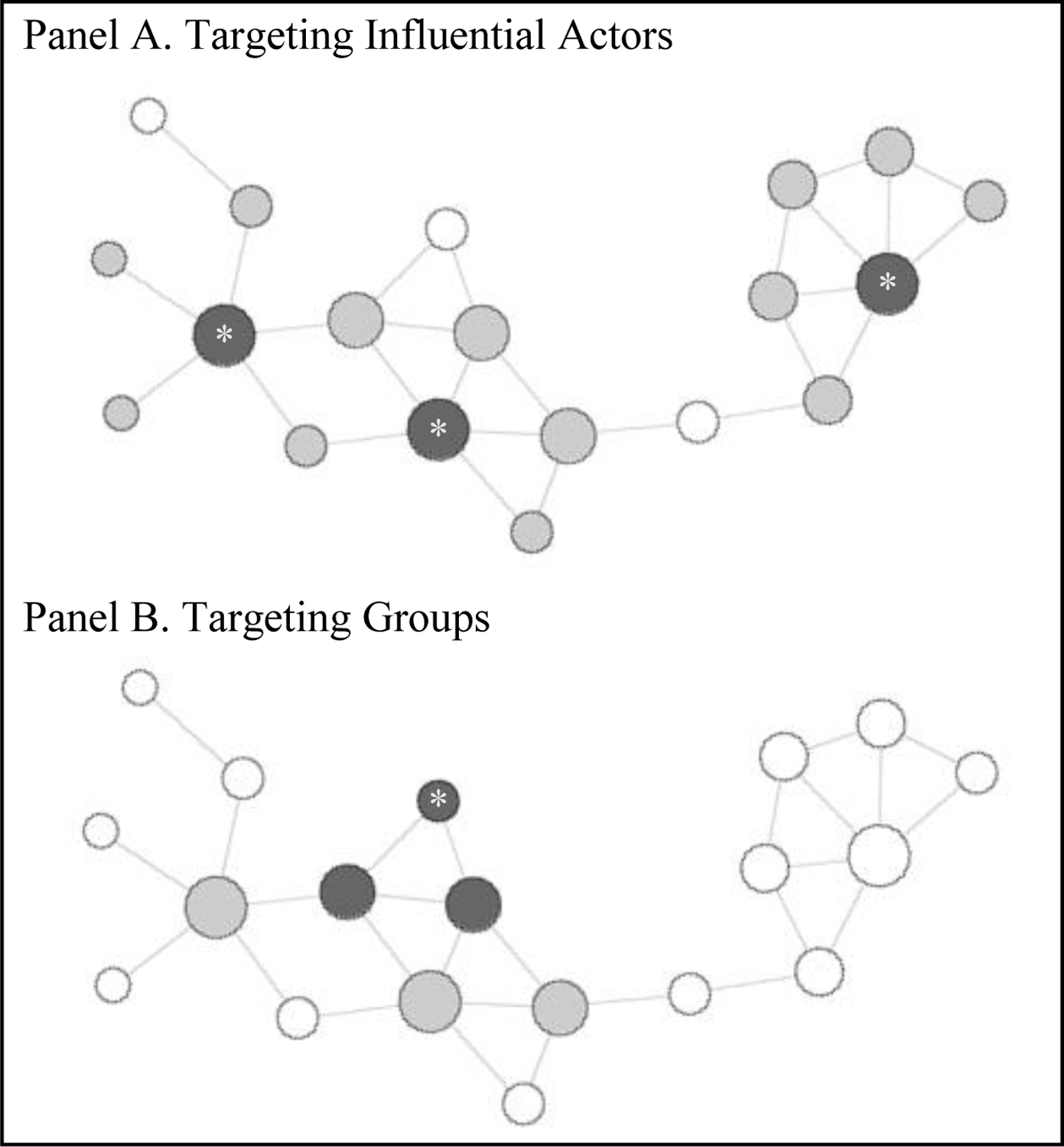
Illustration of strategies targeting individuals versus groups
Notes: Asterisks indicate that a node was invited to participate in the intervention by the practitioner. Dark gray nodes represent students who participated in the intervention (including friends invited by targets). Light gray nodes represent students with at least one direct connection to an intervention participant.
By contrast, enrolling groups of friends is expected to provide intervention participants with long-term protection from harmful influences (Harper et al. 2014). That is, group-based interventions focus on clusters of individuals where interaction is concentrated (see Figure 1B). Intervention programs that enroll friendship groups should encourage the development of long-lasting, healthy behaviors for participants since they are connected directly and can protect one another from sources of harmful influence. At the same time, such approaches may fail to reach non-participants, depending on the extent to which targeted groups are embedded in the larger network (e.g., the white nodes in Figure 1B are only reachable indirectly, and some at great distance).
Given that the tactics behind individual and segmentation-based interventions are distinct, their long-term effects for participants versus non-participants should differ in systematic ways. As such, there exists a tradeoff in how well an intervention can reach and sustain behavior change across these two subgroups. A handful of studies have examined effects of a particular intervention for participants and non-participants (Amirkhanian et al. 2015; Kelly et al. 1997; Latkin 1998). However, such comparisons are rarely made between individual and segmentation-based approaches. Among the limited prior work that compares network-based targeting approaches in a systematic manner, program success is typically assessed by considering population-level outcomes (Badham et al. 2016; Kim et al. 2015). Thus, we do not currently have a good understanding of how the various types of network-based interventions shape health outcomes for program participants versus non-participants.
It can be difficult to forecast how these strategies will impact participants and non-participants differently, as well as how they will shape population-wide prevalence. This is true in the abstract, but even more so in natural settings that vary greatly in distributions of alcohol use, network structure, and their association (Hunter et al. 2019; Latkin and Knowlton 2015), which can shape an intervention’s effectiveness (adams and Schaefer 2016). For instance, previous work finds that an identical network-based intervention can have vastly different outcomes when applied to seemingly analogous populations (Latkin and Knowlton 2015). Our present knowledge of how contextual level factors moderate the success of health interventions is quite limited, particularly in empirical settings (Shelton et al. 2018; Valente 2012).
Current Study
The current study uses a computational experiment to evaluate the potential impact of individual and segmentation-based intervention designs. While field experiments that administer network-based interventions offer one means to evaluate the effectiveness of different targeting campaigns (e.g., Kim et al. 2015; Starkey et al. 2009), their implementation is costly and time consuming, particularly when social network data are required (Wang et al. 2017). There is a long history of using simulations to evaluate intervention effects given the complexity involved with experiments in the natural world (adams and Schaefer 2016; Badham et al. 2016; Hallgren et al. 2017; Schaefer et al. 2013; Zhang et al. 2015). Beyond being more cost-effective, simulations readily account for contextual factors when estimating program impacts. This enables one to make rigorous comparisons of intervention designs across heterogeneous environments (Valente 2012).
We consider a total of five network-based intervention strategy variants. Our two individual-based approaches use social network information to draw participants from the most central positions in their school network, whereas our three segmentation designs identify a set of random targets and their friends. We go beyond prior research (e.g., Badham et al. 2018) by considering intervention effects for participants and non-participants separately and, as such, provide a roadmap for how to weigh the advantages and shortcomings of these approaches. While simulation techniques have been criticized for adopting assumptions with weak empirical backing, some of these concerns can be alleviated by informing a simulation’s conditions and parameter estimates with observed data (Ip et al. 2013). Here, we empirically-ground our simulations in observations of 28 school-based networks from the Promoting School-Community Partnerships to Enhance Resilience (PROSPER) study to better ensure that the contexts being evaluated accurately reflect those observed in the real world. We consider contextual variations in school-wide levels of peer influence and drinker popularity since these phenomena relate to patterns of actor centrality and network clustering. This approach provides additional insight to the network-level processes that moderate an intervention’s success.
Our empirically-grounded computational experiment is designed to answer the following questions:
RQ1: What is the relative effectiveness of network-based intervention strategies for reducing drinking across a school-based population of adolescents?
RQ2: How do intervention effects differ for targeted versus non-targeted youth?
RQ3: How do contextual factors moderate the effectiveness of network-based intervention strategies?
Methods
Data
Our simulations were informed by data on 4,819 high school students from the Promoting School-Community Partnerships to Enhance Resilience (PROSPER) study (Spoth et al. 2007). Students came from 28 school districts in the Midwestern US, with half randomly selected to participate in a substance abuse prevention program during students’ middle school years. To isolate the effects of our simulated interventions, we limited our sample to school districts in the control group that received no actual intervention (n = 14 districts).
Data were collected from two cohorts: students entering the 9th grade in 2005 and those entering in 2006. Self-administered surveys were distributed to students during the spring semesters of each academic year. We specifically focused on three waves collected during respondents’ 9th through 11th grade years because this represents a developmental period where drinking becomes increasingly common (Donovan 2004). Response rates were relatively high during these waves, ranging from 80–88%. We consider those students who were present for all three waves of interest to reduce biases that may arise from students moving in or out of each district.
In each wave of the survey, students were asked, “Who are your best and closest friends in your grade?” All respondents were permitted to nominate a maximum of seven within-community and within-grade friends. We use these nominations to construct 28 longitudinal friendship networks (14 schools × 2 cohorts). At each wave of the survey, respondents were also asked how often they had “beer, wine, wine coolers, or hard liquor” in the past month. Responses range from 1 = none to 5 = more than once per week. Following previous work (e.g., McMillan et al. 2018; Osgood et al. 2013), we recode students’ past month participation into three ordered categorical measures: 0 = none, 1 = once in the past month, and 2 = more than once in the past month.
Targeting Strategies
We considered six targeting strategies: the first five selected participants based upon properties of the 9th grade network (i.e., Time 1), while the sixth enrolled students randomly. Our first two approaches represent individual-based strategies that enrolled the most connected actors in a network using operationalizations of centrality that are commonly applied in the network-based intervention literature. One targeted adolescents with the highest indegree centrality (following Kim et al. 2015; Zhang et al. 2015), or those respondents who received the most friendship nominations. In addition to being well-known and visible in their networks, high indegree youth are situated in optimal positions for influencing, and being influenced by, the drinking behaviors of their peers. The second strategy enrolled individuals who bridge disconnected parts of the broader network, as measured by betweenness (following Badham et al. 2016; Valente and Vega Yon 2020). Betweenness centrality is calculated by finding all geodesics in a network (i.e., the shortest paths that connect each pair of actors) and then calculating the proportion of geodesics on which each individual is situated (Freeman 1979). High betweenness adolescents tend to link disconnected parts of a network, enabling them to serve as gatekeepers who can impede the spread of alcohol use. In the case of ties among each centrality measure, we randomly selected from those students tied at the cutoff level.
Our next three strategies leverage segmentation approaches by identifying a random sample of adolescents to participate, and having either (1) one friend, (2) up to three friends, or (3) all of their friends join them in the intervention (following Centola 2018; Kim et al. 2015). If a randomly selected student nominated more than the requisite number of friends, we determined the friends they brought by randomly selecting from their friend list. Students who did not make any friendship nominations were allowed to participate under these strategies, but could not bring additional friends. Lastly, to serve as a control condition, we implemented a sixth strategy that randomly selected all program participants.
We specified the number of participants in each intervention according to three different dosage levels: 10%, 20%, and 30% of the total number of students in the network. Due to financial and time constraints, most interventions that target subsamples enroll 10 to 20% of eligible individuals from the population of interest (Valente and Pumpuang 2007). Here, we also considered targeting scenarios with dosage levels of 30% as this offered more leverage to test whether intervention effects differ in important ways according to the participation rate. At each dosage level, we required that the average number of participants be equal across conditions, thereby holding the participation rate constant. This resulted in 18 program conditions, organized as a 6×3 factorial design.
Interventions
Our interventions were introduced at wave 1 (9th grade) and consisted of two components. First, we reduced the initial drinking level of all participants to zero, which represents a successful immediate effect of the program. Intervention campaigns do not solely aim to reduce problem behaviors in the near term, however, they also aspire to maintain these reductions by inoculating program participants, so they continue to lead healthy, pro-social lives (Griffin and Botvin 2010). As a result, our interventions included a second component that allowed us to account for long-term effects by inoculating participants so that their future drinking would be shaped solely by individual factors, rather than influence from friends. This inoculation can be conceptualized as a set of skills that inform healthy decision-making and information about the consequences of mimicking friends’ alcohol use. Furthermore, the inoculation allows students who did not drink alcohol and schools with low drinking prevalence to still benefit from the intervention.
Analytic Plan
We used the simulation capacities within the Stochastic Actor Oriented Model (SAOM) framework to simulate a variety of intervention campaigns that target adolescent drinking (following adams and Schaefer 2016; Schaefer et al. 2013). Our methodological approach consisted of three steps, which we discuss next in further detail:
Fit a separate model of network and behavior coevolution to each observed school network to obtain school-specific parameter estimates.
Use fitted models as the basis for simulations that manipulate the strategy used to target students for an “intervention program” and record drinking prevalence after each run.
Statistically compare average drinking across the manipulated experimental conditions and test effects of context.
Step 1: Fit SAOMs to Observed Data.
Our first step was to model the observed data with SAOMs (Snijders 2001; Steglich et al. 2010). SAOMs incorporate a simulation-based algorithm during the model fitting process (which we also used for the computational experiment). During estimation, the SAOM simulates sequences of distinct network and behavior changes from the perspective of each actor in an effort to obtain parameter estimates that reproduce distributions of network and behavior features from the observed data. Changes are dictated by separate functions to model friendship and individual behavior simultaneously. For more details on the statistical properties that underlie SAOMs, we refer the reader to Snijders (2001).
Our SAOMs included several effects of interest, as well as many controls. Most notably, the behavior function of our SAOM included the average drinking similarity effect to estimate whether influence from friends shaped individual drinking behavior. This effect considers whether an individual’s alcohol use tends to resemble that of their friends over time. Positive values of the coefficient suggest that friends influence one another to either maintain, increase, or decrease their alcohol consumption to achieve a level similar to their friends’ average. Additionally, the network function of our SAOMs included a drinking alter effect to measure whether alcohol use is associated with being chosen as a friend (i.e., popularity). A positive coefficient would suggest that respondents who drink at higher levels are more likely to receive friendship nominations. We also included a variety of other behavior and network effects that are discussed in the Supplemental Materials (Section A).
Given our current focus, we do not interpret the estimated SAOM coefficients here. For a substantive interpretation of the coefficients included in our models, we point the reader to previous research that applies SAOMs to analyze adolescent drinking in the PROSPER data (e.g., McMillan et al. 2018; Osgood et al. 2013).
Step 2: Simulations.
Using the same algorithm that initially fit each SAOM, we simulated the coevolution of friendship and drinking behavior according to each intervention condition. For a given condition, we first applied the intervention to a subsample of students in each network. We set each selected participant’s initial 9th grade drinking level to zero, representing a successful short-term effect of the program. We accounted for long-term effects by introducing a new methodological technique that models the inoculation effects of program participation in an SAOM framework. Previous work that uses simulations to investigate the effectiveness of such campaigns tends to assume that the adoption of new behaviors is permanent (Badham et al. 2016; Valente and Vega Yon 2020) or ignore the potential long-term effects of participation outside the behavior itself (Zhang et al. 2015). In other words, problem behavior is manipulated as an initial condition, but all other conditions (e.g., susceptibility to peer influence) remain constant.
Here, we created a binary variable that indicates whether a student is inoculated by the drinking prevention campaign (1 = inoculated). Since the behavior-shaping effects of prevention campaigns are not necessarily permanent, we allowed the effect of inoculation to dissipate over time. Throughout the simulation, participants were randomly selected to lose the protective benefits of the inoculation. We parametrized our models so that the effect of inoculation faded for all participants by the end of the simulation, which reflects evidence from randomized controlled trials on the long-term impacts of health interventions on adolescents (Campbell et al. 2008). It is also important to note that while our inoculation prevents adolescent from being influenced by their friends’ drinking behaviors, inoculated adolescents can still increase their alcohol use. Namely, individual-level factors in the model that predict drinking will still operate and increase one’s likelihood of drinking (e.g., gender, sensation-seeking). Background factors that lead to drinking can therefore exert an effect on post-intervention alcohol use even while an individual is still inoculated. We did not assume that the interventions include a peer education component, wherein inoculated participants learn the necessary skills and confidence to dissuade their peers from drinking (Kelly 2004; Starkey et al. 2009). Thus, inoculated students had the same potential to influence their peers’ drinking behaviors as non-inoculated adolescents. We include technical details about the inoculation parameter in the Supplemental Materials (Section B).
Following this procedure, we simulated network-drinking coevolution for each network. The simulation gave actors multiple opportunities to change either their friendships or drinking behavior. Apart from the inoculation process described above, actor decisions were governed by the parameter estimates from the SAOM initially fit to their respective network. We conducted 1,000 simulation runs under each condition for all 28 networks, resulting in 504,000 simulation runs (6 targeting strategies × 3 dosage levels × 28 networks × 1,000 runs = 504,000 simulation runs). We also simulated 1,000 runs for each network under a scenario where we did not manipulate the drinking behaviors of any students to represent the baseline prevalence level in the absence of an intervention. At the end of each run, we recorded the distribution of individual drinking behavior. For each condition and school, we calculated the average level of drinking across the 1,000 simulation runs for all students, then separately for participants and non-participants. Since we maintained the same model specifications and rate effects from our estimated SAOMs, these prevalence estimates represent the average drinking levels two years after the intervention’s implementation.
Step 3: Comparing across Targeting Strategies.
Our comparison of drinking outcomes consisted of three parts, corresponding to each research question. First, we used paired t tests to compare the final drinking levels for our different targeting strategies. Then, we conducted additional t tests for the participant and non-participant subsamples to determine how each intervention affects the two sub-populations. Finally, to account for the clustered nature of our data and answer our third research question regarding contextual effects, we constructed three-level multi-level models (MLMs). Here, the first level represents the intervention targeting strategy, the second represents the dosage level, and the third represents the school-based network. The MLM for the final drinking levels (Yijk) is defined as:
This equation includes a network-level intercept (γ000) and several predictors at the level of the intervention strategy (Xijk), dosage amount (Djk), and school-based network (Nk).
At the intervention level, we included a set of categorical variables to indicate the targeting strategy, where random selection served as our reference group. Since behavioral prevalence is systematically associated with the strength of various behavior and network change processes (Schaefer et al. 2013), we included additional predictors at the school network level that were based on estimates from the SAOMs. First was the average similarity measure of peer influence to test whether contexts in which adolescents more often rely on others for behavioral guidance are more responsive to program effects. To test if network-based interventions are affected by drinker popularity within each school context, we also included the estimated coefficients for the drinking alter effect. Our MLMs contained several additional controls at the level of the intervention strategy, dosage amount, and school-based network, which are discussed in the Supplemental Materials (Section C).
To explore how context-level variations shape intervention effectiveness, we estimated additional MLMs with cross-level interactions between our network-level peer influence measure and intervention-level measures that indicated the targeting strategy. A significant interaction would suggest that certain interventions perform particularly better, or worse, depending on the strength of peer influence in the network. Another set of MLMs included cross-level interactions between the measures for network-level drinker popularity and targeting strategy.
Results
Comparison of Targeting Strategies for All Students
In our baseline condition where students’ drinking behaviors were not manipulated, the final average drinking level of the full sample was 0.740 after simulating the equivalent of two years of change (see Table 1). This average closely resembles the observed final average drinking level across our empirical networks. All five interventions and the random targeting strategy produced significantly lower drinking levels when compared to this baseline condition (p < 0.001). Additionally, with increased dosage, average drinking decreased across all intervention scenarios.
Table 1.
Average drinking levels by condition for full sample (participants and non-participants)
| 10% Dosage | 20% Dosage | 30% Dosage | |
|---|---|---|---|
| Random | 0.678 (0.156) |
0.621 (0.144) |
0.571 (0.142) |
| Indegree | 0.658* (0.155) |
0.597* (0.150) |
0.547* (0.148) |
| Betweenness | 0.673 (0.152) |
0.612 (0.148) |
0.561* (0.145) |
| Bring 1 Friend | 0.676 (0.156) |
0.619 (0.145) |
0.569 (0.143) |
| Bring 3 Friends | 0.677 (0.157) |
0.619 (0.145) |
0.568 (0.143) |
| Bring All Friends | 0.678 (0.157) |
0.620 (0.146) |
0.570 (0.143) |
| Baseline (no intervention) | 0.740 (0.179) |
||
| Empirical Data | 0.740 (0.164) |
Notes: Standard deviations presented in parentheses.
Significantly different from random targeting strategy according to a paired t test (p < 0.05).
When considering the total population’s final average drinking, it is apparent that some targeting strategies performed better than others (Research Question 1). Targeting students with the highest indegree significantly outperformed the random targeting approach across all dosage levels (p < 0.001). For example, when 30% of each school’s student body was enrolled in an intervention program, the average drinking of the full sample was 0.024 points lower in the two years following an intervention with the indegree versus the random targeting strategy. The betweenness targeting strategy also resulted in significantly lower drinking levels than the random targeting approach when 30% of each school’s student body was enrolled in the intervention. However, at lower dosage levels, there were no significant differences. Across all dosage levels, the three “bring friends” strategies resulted in final population-wide drinking levels that were not significantly different from the random targeting approach.
Comparison of Targeting Strategies by Participation Status
When intervention participants and non-participants were considered separately (Research Question 2), we found the average drinking level of participants was almost always significantly lower for network-based program strategies when compared to the random targeting approach (see Table 2). Across all dosage levels, betweenness-based approaches reduced targeted students’ average drinking levels by 0.043 additional points than random targeting strategies. Targeted students also reported drinking levels that were significantly lower than the random approach after participating in the indegree-based or “bring all friends” campaigns (p < 0.05).
Table 2.
Average drinking rates across conditions by participation status
| 10% Dosage | 20% Dosage | 30% Dosage | |
|---|---|---|---|
| Participants | |||
| Random | 0.386 (0.137) |
0.372 (0.143) |
0.360 (0.148) |
| Indegree | 0.358* (0.146) |
0.344* (0.154) |
0.337* (0.155) |
| Betweenness | 0.343* (0.143) |
0.337* (0.145) |
0.326* (0.153) |
| Bring 1 Friend | 0.381* (0.144) |
0.369 (0.147) |
0.357 (0.152) |
| Bring 3 Friends | 0.373* (0.145) |
0.362* (0.152) |
0.347 (0.160) |
| Bring All Friends | 0.367* (0.145) |
0.356* (0.151) |
0.348* (0.155) |
| Non-participants | |||
| Random | 0.710 (0.163) |
0.683 (0.155) |
0.660 (0.152) |
| Indegree | 0.692* (0.164) |
0.664* (0.162) |
0.640* (0.158) |
| Betweenness | 0.711 (0.163) |
0.688 (0.165) |
0.669 (0.162) |
| Bring 1 Friend | 0.709 (0.164) |
0.681 (0.156) |
0.658 (0.154) |
| Bring 3 Friends | 0.712 (0.164) |
0.684 (0.156) |
0.643 (0.173) |
| Bring All Friends | 0.713* (0.165) |
0.688* (0.157) |
0.665 (0.154) |
Notes: Standard deviations presented in parentheses.
Significantly different from random targeting strategy according to a paired t test (p < 0.05).
Next, we used paired t tests to compare average drinking levels among non-participants (see Table 2). In general, the difference in final drinking levels for random versus network-based interventions was less pronounced than for targeted students, however, important variations still exist. Across all dosage levels, the indegree-based strategy resulted in the lowest average drinking levels for non-participants, falling 0.018 points below that for the random interventions (p < 0.05). There were no significant differences between the random and betweenness-based, “bring one friend,” or “bring three friends” targeting strategies. In fact, at some dosage levels the “bring all friends” intervention resulted in significantly higher levels of non-participant drinking than would be expected to occur by randomly targeting participants (p < 0.05).
Next, we considered whether these differences hold after accounting for a variety of controls and the clustered nature of our data by applying a set of multi-level models (MLMs). Looking at participants, these models affirmed that several of the network-based targeting strategies outperformed the random strategy at reducing students’ drinking levels (Table 3, Model 1). The indegree (b = −0.018, p < 0.001), betweenness (b = −0.037, p < 0.001), “bring three friends” (b = −0.013, p < 0.01), and “bring all friends” strategies (b = −0.016, p < 0.01) all resulted in final participant drinking levels that were significantly lower than the random targeting approach. We found no significant differences between the “bring one friend” and random targeting approaches.
Table 3.
Multi-level regression model for participants’ and non-participants’ average drinking levels
| Participants | Non-Participants | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
| Est. | SE | Est. | SE | Est. | SE | Est. | SE | |||||
| Program Design | ||||||||||||
| Indegree | −0.018 | (0.005) | *** | −0.012 | (0.007) | −0.023 | (0.005) | *** | 0.013 | (0.006) | * | |
| Indegree × Influence | −0.005 | (0.005) | −0.034 | (0.004) | *** | |||||||
| Betweenness | −0.037 | (0.005) | *** | −0.020 | (0.007) | ** | −0.009 | (0.005) | 0.005 | (0.006) | ||
| Betweenness × Influence | −0.015 | (0.005) | ** | −0.012 | (0.004) | ** | ||||||
| Bring 1 Friend | −0.004 | (0.005) | 0.002 | (0.007) | −0.010 | (0.005) | * | 0.000 | (0.006) | |||
| Bring 1 × Influence | −0.006 | (0.005) | −0.009 | (0.004) | * | |||||||
| Bring 3 Friends | −0.013 | (0.005) | ** | 0.001 | (0.007) | −0.012 | (0.005) | ** | −0.001 | (0.006) | ||
| Bring 3 × Influence | −0.012 | (0.005) | * | −0.010 | (0.004) | * | ||||||
| Bring All Friends | −0.016 | (0.005) | ** | −0.002 | (0.007) | −0.004 | (0.005) | 0.003 | (0.006) | |||
| Bring All × Influence | −0.013 | (0.005) | ** | −0.006 | (0.004) | |||||||
| Initial Drinking of Targets | 0.017 | (0.016) | 0.021 | (0.016) | −0.110 | (0.016) | *** | −0.094 | (0.015) | *** | ||
| 20% Dosage | −0.006 | (0.004) | −0.006 | (0.004) | −0.026 | (0.008) | ** | −0.026 | (0.008) | ** | ||
| 30% Dosage | −0.022 | (0.004) | *** | −0.022 | (0.004) | *** | −0.047 | (0.008) | *** | −0.047 | (0.008) | *** |
| School Composition | ||||||||||||
| Cohort | −0.016 | (0.030) | −0.016 | (0.030) | 0.013 | (0.036) | 0.013 | (0.036) | ||||
| Number of Students | 0.001 | (0.000) | 0.001 | (0.000) | 0.000 | (0.000) | 0.001 | (0.000) | ||||
| Average Initial Drinking | 0.406 | (0.110) | ** | 0.402 | (0.110) | ** | 0.942 | (0.132) | *** | 0.925 | (0.132) | *** |
| Proportion of Girls | 0.006 | (0.392) | 0.007 | (0.392) | 0.999 | (0.472) | * | 1.004 | (0.472) | * | ||
| Proportion Non-White | −0.214 | (0.316) | −0.215 | (0.316) | −0.425 | (0.380) | −0.428 | (0.380) | ||||
| Modeled Processes | ||||||||||||
| Peer Influence (average similarity) | −0.102 | (0.016) | *** | −0.093 | (0.016) | *** | −0.025 | (0.019) | −0.014 | (0.019) | ||
| Drinker Popularity (drinking alter) | 0.143 | (0.038) | ** | 0.143 | (0.038) | ** | 0.118 | (0.046) | * | 0.118 | (0.046) | * |
| Density | −0.084 | (0.051) | −0.084 | (0.051) | −0.012 | (0.062) | −0.010 | (0.062) | ||||
| Clustering (transitive triplets) | −0.194 | (0.121) | −0.194 | (0.120) | 0.044 | (0.145) | 0.045 | (0.145) | ||||
| Same Drinking (drinking similarity) | −0.047 | (0.076) | −0.046 | (0.076) | 0.115 | (0.092) | 0.116 | (0.092) | ||||
| Intercept | 0.121 | (0.319) | 0.112 | (0.319) | −0.421 | (0.384) | −0.431 | (0.384) | ||||
| Variance Components | ||||||||||||
| Intercept | 0.000 | 0.000 | 0.001 | *** | 0.001 | *** | ||||||
| Level 1 | 0.001 | 0.001 | 0.001 | 0.001 | ||||||||
| Level 2 | 0.005 | *** | 0.005 | *** | 0.007 | *** | 0.007 | *** | ||||
Notes:
p < 0.05
p < 0.01
p < 0.001.
Omitted categories are random targeting for program design and 10% for dosage level.
Our MLMs predicting the average drinking of non-participants also suggested that certain network-based targeting approaches tend to outperform the random condition (see Table 3, Model 3). After accounting for controls and the clustered nature of our data, we found that the indegree (b = −0.023, p < 0.001), “bring one friend” (b = −0.010, p < 0.05), and “bring three friends” strategies (b = −0.012, p < 0.01) resulted in final average drinking levels for non-participants that were significantly lower than the random targeting approach. The betweenness-based and “bring all friends” targeting approaches did not result in significantly different average drinking levels for non-participants when compared to the random approach.
Contextual Differences
To offer insight to how context matters for intervention effectiveness, Figure 2 presents the distribution of drinking rates relative to the random scenario across school networks. The figure makes it clear that the network interventions produced lower drinking rates in most schools, particularly among participants. It is also apparent that some of the network-based strategies have a wider variance of effect than others.
Figure 2.
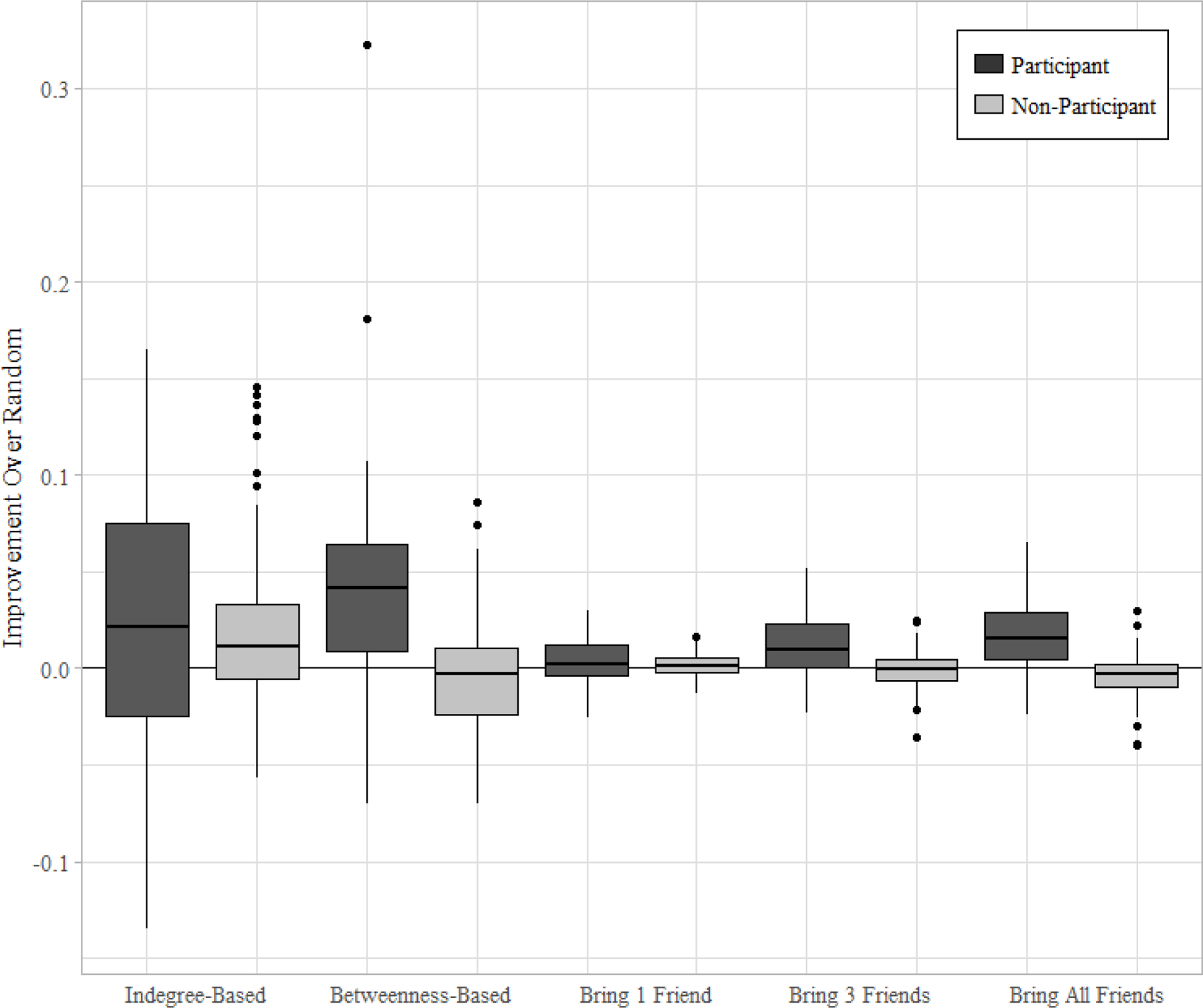
Differences between average drinking for participants and non-participants following random versus network-based interventions
We explored this variation by examining whether peer influence and drinker popularity moderate intervention effects (Research Question 3). For participants (Table 3, Model 2), there were significant and negative interactions between the drinking influence variable and the indicators for betweenness (b = −0.015, p < 0.01), “bring three friends” (b = −0.012, p < 0.05), and “bring all friends” strategies (b = −0.013, p < 0.01). These findings suggest that in networks with high levels of drinking influence, the aforementioned approaches result in final drinking levels for targeted students that are especially lower than random approaches (see Figure 3). We did not find any evidence that drinker popularity moderated the relationship between targeting approach and drinking levels of intervention participants (see Supplemental Materials, Section D).
Figure 3.
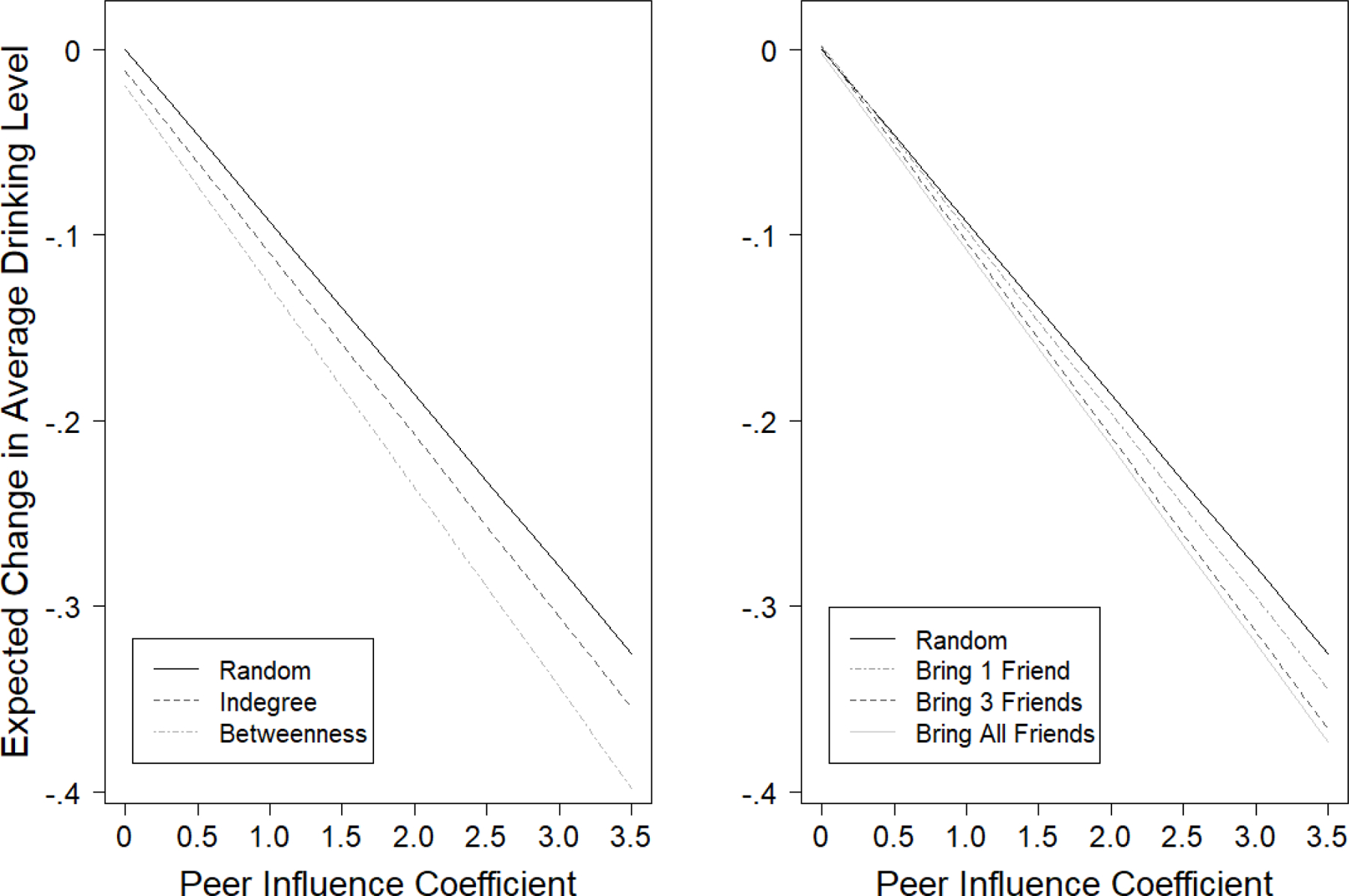
Expected change in average drinking level for participants by intervention type and network-level peer influence
Turning to non-participants (Table 3, Model 4), we uncovered significant and negative interactions between the network-level drinking influence variable and the intervention-level indicators for the indegree (b = −0.034, p < 0.001), betweenness (b = −0.012, p < 0.01), “bring one friend” (b = −0.009, p < 0.05), and “bring three friends” strategies (b = −0.010, p < 0.05) (Table 3, Model 4). These findings suggest that when compared to random targeting, strategies that selected participants according to these four network-based approaches were expected to reduce non-participant drinking rates to an even greater extent in networks defined by high levels of peer influence (see Figure 4). We did not find evidence that drinker popularity moderated the relationship between targeting approach and final drinking levels of non-participants (see Supplemental Materials, Section D).
Figure 4.
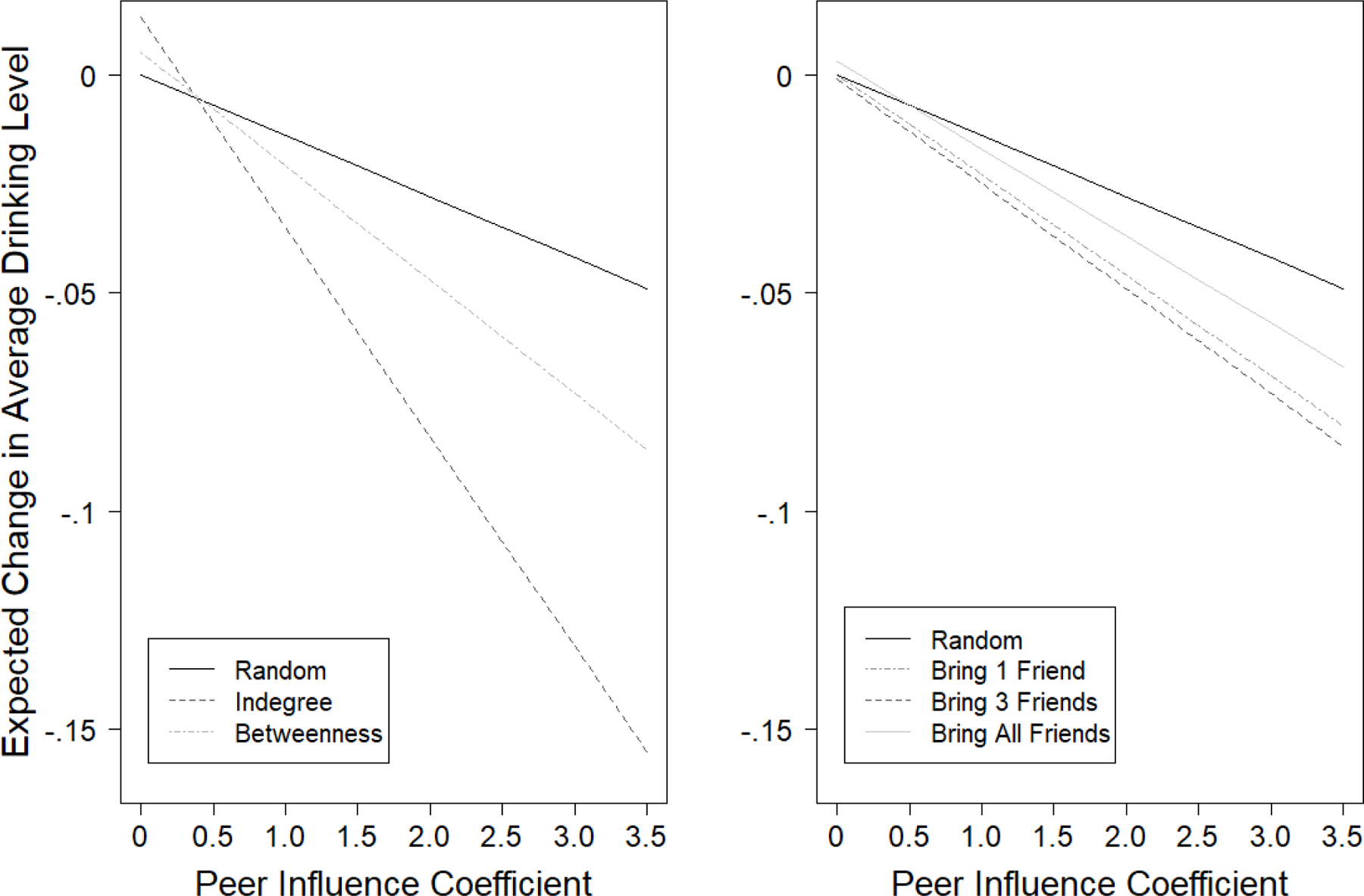
Expected change in average drinking level for non-participants by intervention type and network-level influence
Discussion
School-based interventions hold great potential to combat the health risks associated with adolescent drinking. Since program resources are often limited, however, efficiency is important when designing these interventions. Here, we evaluated network-based recruitment strategies as one means to increase an intervention’s effectiveness. These strategies represent various individual- and segmentation-based approaches that all leverage the fact that adolescent drinking is shaped by the behaviors and attitudes of one’s social connections. We devised a computational experiment to compare how the five network-based enrollment strategies differently impacted the drinking behaviors of participants and non-participants within the same school ecologies. All strategies led to lower population-wide drinking rates when compared to the baseline condition. However, when we consider targeted and non-targeted adolescents separately, we found evidence that under certain scenarios, some network-based targeting strategies perform significantly better than others.
Individual-Based Targeting Strategies.
Complementing previous work (Badham et al. 2016; Valente and Vega Yon 2020), we found that both the indegree- and betweenness-based targeting strategies hold promise for disrupting the natural diffusion of risky health behaviors. Indegree-based targeting strategies led to the lowest average drinking levels for students who did not participate in the intervention. This likely results from the fact that high indegree individuals have more connections through which they can influence others’ drinking behaviors, including those of non-participants. Betweenness-based interventions did not perform as well, on average. Only in networks where peer influence was stronger did these strategies outperform random approaches. We expect this to be the case because high betweenness actors are situated in unique positions for connecting the network, but do not necessarily have large numbers of ties. Without a higher volume of connections, high betweenness actors are limited in their ability to thwart the diffusion of risky behaviors, especially when processes of peer influence are weak and one’s direct impact on others is less likely to spread further.
When compared to alternative strategies, we found that targeting influential actors also led to the lowest drinking levels among participants. Whereas highly central individuals are often of interest to intervention campaigns because of their increased visibility to peers in the network, individuals in such positions also face heightened risks of exposure (Friedkin 2001). Central actors are tied to larger numbers of peers, who may belong to disconnected groups, and this is apt to increase their exposure to a range of drinking behaviors, including those at the risky end. Our finding that actors in central positions experienced positive benefits from being targeted suggests that the inoculation provided by the program afforded long-term protections to these individuals who would otherwise be at risk of experiencing negative peer influence.
Segmentation Targeting Strategies.
Taking advantage of the fact that adolescents tend to drink alcohol at similar levels as their friends (Knecht et al. 2010; Osgood et al. 2013), our three “bring friends” strategies invited self-defined pairs or groups of friends to participate in the intervention. Similar to the findings of randomized trials (e.g., Shaya et al. 2014), the “bring friends” strategies tended to result in better health outcomes for participants, with the “bring all friends” approach leading to the lowest participant drinking averages when compared to random targeting. Processes of social protection can help explain why we observe these effects. For instance, if the inoculation from the intervention wears off for one participant, they are more likely to have a direct tie to someone who participated in the intervention, continues to abstain from drinking, and can protect them from sources of direct and indirect negative influence. As larger friend groups are targeted, individuals have more connections to provide this protection, particularly in networks where the strength of peer influence is high.
Nonetheless, a tradeoff emerged across our three “bring friends” strategies. Namely, those strategies that were more effective at lowering the drinking levels for participants were the least effective at reducing non-participants’ drinking levels. We suspect that this pattern emerged because, while targeting clusters of friends helps protect participants from negative influences, it also enhances social closure. As larger groups of friends are targeted, participation becomes increasingly localized in the network, with more regions of the social landscape unaffected by the intervention. This concentrates participation among individuals who share social ties, thereby limiting the number of links from participants to non-participants and leaving inoculated participants with fewer opportunities to influence the drinking behaviors of non-participants.
In addition to these empirical findings, the current study makes several methodological contributions. First, our results highlight the value in evaluating intervention impacts for participants and non-participants separately. Previous intervention research occasionally uses this distinction as a tool to assess a program’s diffusion potential (e.g., Amirkhanian et al. 2015). However, we argue that it is crucial to consider the outcomes of both participants and non-participants in order to compare the impact of different targeting strategies in a systematic manner. For instance, we find that some of our “bring friends” strategies result in significantly lower drinking rates for intervention participants when compared to random targeting strategies. This improvement, however, is at the expense of non-participants who drink at significantly higher rates after the program commences. Practitioners should be aware of these tradeoffs as this will help them design network-based intervention will best suit their program goals.
Additionally, we developed a methodological approach within the SAOM framework that not only manipulates actors’ initial behaviors, but also models how the effects of the intervention dissipate over time. In our case, participants were inoculated to resist peer influence, and the effect of this protection diminished as the simulation progressed. This methodological development represents an improvement upon existing techniques as it allows one to estimate simulations that better reflect the long-term effects of interventions that are observed in randomized controlled trials (e.g., Campbell et al. 2008). Our method could be applied to other SAOM-based computational experiments to allow the strength of effects to vary across time, as well as across individual participants. For instance, this framework could be applied to simulate the effectiveness of peer-led interventions that teach participants communication skills to enhance their positive influence on peers’ risky health behaviors (e.g., Kelly 2004; Starkey et al. 2009).
Finally, our computational experiment benefited by drawing upon 28 different social network contexts. These varied contexts gave our experiment a more reasonable specification of the range of strengths for different simulated processes, allowing for a more robust test. Our large sample of networks also enabled us to consider how context-level factors shape the effectiveness of our various targeting strategies. We found that network-based intervention campaigns tended to produce the lowest levels of drinking for both participants and non-participants in contexts where peer influence played a stronger role in shaping individual drinking behavior. Context-level variations in drinker popularity, on the other hand, did not shape the effectiveness of the network-based intervention campaigns studied here. These results shed some light on why previous work finds that the same network-interventions can have varying degrees of success across otherwise similar populations (Latkin and Knowlton 2015). Subtle differences in network processes, such as the tendency to mimic friends’ alcohol use, can be the difference between an intervention’s success and failure.
Our study demonstrates both the strengths and drawbacks of applying network-based interventions to combat adolescent drinking. However, there are limitations to the current project that should be acknowledged. First, we constrained positive and negative peer influence to operate at equivalent magnitudes. Prior work has shown that influence processes may only operate in one direction (Haas and Schaefer 2014), which is something that would moderate the effectiveness of the intervention strategies studied here. Since our interventions are designed to help students combat the negative ramifications of peer influence, we expect our network-based targeting approaches would perform particularly well in networks where influence processes tend to encourage drinking. Second, our simulations assumed the intervention programs operate with complete participation, efficiency, and fidelity. These assumptions allowed for a cleaner, more parsimonious test, but would need to be calibrated with empirical data in any attempt to generalize anticipated intervention effects in a natural setting. It is possible to build off our methodological approach to model additional intricacies that shape adolescent drinking intervention campaigns, such as when a program’s impact varies across individual adolescents. One could simulate interventions where the strength of inoculation differs according to individual-level psychological and demographic characteristics (e.g., self-control or gender), one’s previous experience with drinking, and exposure to alcohol from actors outside of the school environment (e.g., parents), for example. Though not always available in practice, empirical estimates of these social processes could account for such variations and increase the ecological validity of the simulation methods adopted here. Finally, the contexts we studied were primarily in rural and semi-rural school districts, meaning that large, urban schools were not well represented. Future work should consider whether the dynamics studied here similarly shape school-based interventions in a more diverse set of environments.
Our project sheds light on an important tradeoff confronting network-based interventions. Programs may seek to enroll central individuals with the greatest potential to improve the health behaviors of non-participants or target clusters of friends in an effort to provide long-term protection to participants. Our novel computational experiment found that these strategies have different implications for long-term population health. Researchers and practitioners should consider the varying effects of network-based interventions for participants and non-participants, as well as context-level features, when designing intervention campaigns that target risky adolescent health behaviors. The current project demonstrates that empirically-grounded simulations hold promise for considering the tradeoffs that confront network-based intervention design.
Supplementary Material
Highlights:
Compare individual and segmentation approaches to network-based interventions
Approaches have different impacts for participant and non-participant alcohol use
Non-participants saw more benefits from individual-based targeting approaches
Tradeoffs emerged for participants and non-participants in segmentation targeting
More positive impacts in contexts defined by higher levels of peer influence
Acknowledgments
This research was supported in part by the W.T. Grant Foundation (8316) and National Institute on Drug Abuse (RO1-DA08225; T32-DA-017629; F31-DA-024497), and uses data from PROSPER, a project directed by R. L. Spoth and funded by grant RO1-DA013709 from the National Institute on Drug Abuse. This work was also supported by Pennsylvania State University and the National Science Foundation under an IGERT award # DGE-1144860, Big Data Social Science.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- adams jimi, and Schaefer David R. 2016. “How Initial Prevalence Moderates Network-Based Smoking Change: Estimating Contextual Effects with Stochastic Actor-Based Models.” Journal of Health and Social Behavior 57(1):22–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amirkhanian Yuri, Kelly Jeffrey, Takacs Judit, Timothy McAuliffe Anna Kuznetsova, Toth Tamas, Mocsonaki Laszlo, DiFranceisco Wayne, and Meylakhs Anastasia, 2015. “Effects of a Social Network HIV/STD Prevention Intervention for Men Who Have Sex with Men in Russia and Hungary: A Randomized Controlled Trial.” AIDS 29(5):583–593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Badham Jennifer, Kee Frank, and Hinter Ruth. 2016. “Simulating Network Intervention Strategies: Implications for Adoption of Behaviour.” Network Science 6:265–280. [Google Scholar]
- Beheshti Rahmatollah, Jalalpour Mehdi, and Glass Thomas A. 2017. “Comparing Methods of Targeting Obesity Interventions in Populations: An Agent-Based Simulation.” SSM – Population Health 3:211–218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell R, Starkey F, Holliday J, Audrey S, Bloor M, Parry-Langdon N, Hughes R, & Moore L (2008). An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): A cluster randomised trial. The Lancet, 371, 1595–1602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centola Damon. 2018. How Behavior Spreads. Princeton, NJ: Princeton University Press. [Google Scholar]
- Cohen Geoffrey L., and Prinstein Mitchell J. 2006. “Peer Contagion of Aggression and Health Risk Behavior Among Adolescent Males: An Experimental Investigation of Effects on Public Conduct and Private Attitudes.” Child Development 77(4):967–983. [DOI] [PubMed] [Google Scholar]
- de la Haye Kayla, Robins Garry, Mohr Philip, and Wilson Carlene. 2011. “How Physical Activity Shapes, and is Shaped by, Adolescent Friendships.” Social Science & Medicine 73(5):719–728. [DOI] [PubMed] [Google Scholar]
- Donovan John E. 2004. “Adolescent Alcohol Initiation: A Review of Psychosocial Risk Factors.” Journal of Adolescent Health 35(6):529.e7–529.e18. [DOI] [PubMed] [Google Scholar]
- Feld Scott. 1991. “Why Your Friends have More Friends than You Do.” American Journal of Sociology 96:1464–77. [Google Scholar]
- Freeman Linton C. 1979. “Centrality in Social Networks: Conceptual Clarification.” Social Networks 27(1):55–71. [Google Scholar]
- Friedkin Noah. 2001. “Norm Formation in Social Influence Networks.” Social Networks 23(3):167–189. [Google Scholar]
- Fujimoto Kayo, and Valente Thomas W. 2015. “Multiplex Congruity: Friendship Networks and Perceived Popularity as Correlates of Adolescent Alcohol Use.” Social Science & Medicine 125:173–181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffin Kenneth W., and Botvin Gilbert J. 2010. “Evidence-Based Interventions for Preventing Substance Use Disorders in Adolescents.” Child & Adolescent Psychiatric Clinics 19(3):505–526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haas Steven A. and Schaefer David R. 2014. “With a Little Help from My Friends? Asymmetrical Social Influence on Adolescent Smoking Initiation and Cessation.” Journal of Health and Social Behavior 55(2):126–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haas Steven A., Schaefer David R., and Kornienko Olga. 2010. “Health and the Structure of Adolescent Social Networks.” Journal of Health and Social Behavior 51(4):424–439. [DOI] [PubMed] [Google Scholar]
- Hallgren Kevin A., McCrady Barbara S., Caudell Thomas P., Witkiewitz Katie, and Tonigan J. Scott. 2017. “Simulating Drinking in Social Networks to Inform Alcohol Prevention and Treatment Efforts.” Psychology of Addictive Behaviors 31(7):763–774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hunter Ruth F., de la Haye Kayla, Murray Jennifer M., Badham Jennifer, Valente Thomas W., Clarke Mike, and Kee Frank. 2019. “Social Network Interventions for Health Behaviours and Outcomes: A Systematic Review and Meta-Analysis.” PLoS Med 16(9): e1003890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harper Gary W., Dolcini M. Margaret, Benhorin Shira, Watson Susan E., and Boyer Cherrie B. 2014. “The Benefits of a Friendship-Based HIV/STI Prevention Intervention for African American Youth.” Youth & Society 46(5):591–622. [Google Scholar]
- Ip Edward H., Rahmandad Hazhir, Shoham David A., Hammond Ross, Huang Terry T.K., Wang Youfa, and Mabry Patricia L. 2013. “Reconciling Statistical and Systems Science Approaches to Public Health.” Health Education & Behavior 40(1):123S–131S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelly Jeffrey A. 2004. “Popular Opinion Leaders and HIV Prevention Peer Education: Resolving Discrepant Findings, and Implications for the Development of Effective Community Programmes.” AIDS CARE 16(2):139–150. [DOI] [PubMed] [Google Scholar]
- Kim David A., Hwong Alison R., Stafford Derek, Hughes D. Alex, O’Mally A. James, Fowler James H., and Christakis Nicholas A. 2015. “Social Network Targeting to Maximise Population Behaviour Change: A Cluster Randomised Controlled Trial.” The Lancet 386:145–153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knecht Andrea B., Burk William J., Weesie Jeroen, and Steglich Christian. 2010. “Friendship and Alcohol Use in Early Adolescence: A Multilevel Social Network Approach.” Journal of Research on Adolescence 21(2):475–487. [Google Scholar]
- Kreager Derek A., Rulison Kelly, and Moody James. 2011. “Delinquency and the Structure of Adolescent Peer Groups.” Criminology 49(1):95–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Latkin Carl. 1998. “Outreach in Natural Settings: The Use of Peer Leaders for HIV Prevention Among Injecting Drug Users’ Networks.” Public Health Reports 113:151–159. [PMC free article] [PubMed] [Google Scholar]
- Latkin Carl, and Knowlton Amy. 2015. “Social Network Assessments and Interventions for Health Behavior Change: A Critical Review.” Behavioral Medicine 41(3):90–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Light John M., Greenan Charlotte C., Rusby Julie C., Nies Kimberly M., Snijders Tom A.B. 2013. “Onset to First Alcohol Use in Early Adolescence: A Network Diffusion Model.” Journal of Research on Adolescence 23(3):487–499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minnis Alexandra M., Evan van Dommelen-Gonzalez Ellen Luecke, Dow William, Bautista-Arredondo Sergio, and Padian Nancy S. 2014. “Yo Puedo – A Conditional Cash Transfer and Life Skills Intervention to Promote Adolescent Sexual Health: Results of a Randomized Feasibility Study in San Francisco.” Journal of Adolescent Health 55:85–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMillan Cassie. 2019. “Tied Together: Adolescent Friendship Networks, Immigrant Status, and Health Outcomes.” Demography 56(3):1075–1103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMillan Cassie, Felmlee Diane, and Osgood D. Wayne. 2018. “Peer Influence, Friend Selection, and Gender: How Network Processes Shape Adolescent Smoking, Drinking, and Delinquency.” Social Networks 55:86–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McPherson Miler, Smith-Lovin Lynn, and Cook James M. 2001. “Birds of a Feather: Homophily in Social Networks.” Annual Review of Sociology 27:415–444. [Google Scholar]
- Osgood D. Wayne, Ragan Daniel T., Wallace Lacey, Gest Scott D., Feinberg Mark E., and Moody James. 2013. “Peers and the Emergence of Alcohol Use: Influence and Selection Processes in Adolescent Friendship Networks.” Journal of Research on Adolescence 23(3):500–512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paluck Elizabeth L., Shepherd Hana, and Aronow Peter M. 2016. “Changing Climates of Conflict: A Social Network Experiment in 56 Schools.” Proceedings of the National Academy of Sciences 113(3):566–571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rulison Kelly L., Feinberg Mark, Gest Scott D., and Osgood D. Wayne. 2015. “Diffusion of Intervention Effects: The Impact of a Family-Based Substance Use Prevention Program on Friends of Participants.” Journal of Adolescent Health 57:433–440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaefer David R., adams jimi, and Haas Steven A. 2013. “Social Networks and Smoking: Exploring the Effects of Peer Influence and Smoker Popularity through Simulations.” Health Education & Behavior 40(1S):24S–32S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaya Fadia T., Chirikov Viktor V., Howard DeLeonardo, Foster Clyde, Costas Julian, Snitker Soren, Frimpter Jeffrey, and Kucharski Kathrin. 2014. “Effects of Social Networks Intervention in Type 2 Diabetes: A Partial Randomised Study.” Journal of Epidemiology and Community Health 68:326–332. [DOI] [PubMed] [Google Scholar]
- Snijders Tom A.B. 2001. “The Statistical Evaluation of Social Network Dynamics.” Sociological Methodology 31:361–395. [Google Scholar]
- Shelton Rachel, Lee Matthew, Brotzman Laura, Crookes Danielle, Jandorf Lina, Erwin Deborah, and Gage-Bouchard Elizabeth. 2019. “Use of Social Network Analysis in the Development, Dissemination, Implementation, and Sustainability of Health Behavior Interventions for Adults: A Systematic Review.” Social Science & Medicine 220:81–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth Richard, Redmond Cleve, Shin Chungyeol, Greenberg Mark, Clair Scott, and Feinberg Mark. 2007. “Substance-Use Outcomes at 18 Months Past Baseline: The PROPSER Community-University Partnership Trial” American Journal of Preventive Medicine 32(5):395–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Starkey Fenella, Audrey Suzanne, Holliday Jo, Moore Laurence, and Campbell Rona. 2009. “Identifying Influential Young People to Undertake Effective Peer-Led Health Promotion: The Example of A Stop Smoking In Schools Trial (ASSIST).” Health Education Research 24(6):977–988. [DOI] [PubMed] [Google Scholar]
- Steglich Christian, Snijders Tom A.B., and Pearson Michael. 2010. “Dynamic Networks and Behavior: Separating Selection from Influence.” Sociological Methodology 40:329–393. [Google Scholar]
- Valente Thomas W. 2012. “Network Interventions.” Science 337(6090):49–53. [DOI] [PubMed] [Google Scholar]
- Valente Thomas W., and Pumpuang Patchareeya. 2007. “Identifying Opinion Leaders to Promote Behavioral Change.” Health Education & Behavior 34(6):881–896. [DOI] [PubMed] [Google Scholar]
- Valente Thomas W., and Vega Yon George G. 2020. “Diffusion/Contagion Processes on Social Networks.” Health Education & Behavior 47:235–248. [DOI] [PubMed] [Google Scholar]
- Wang Cheng, Hipp John R., Butts Carter T., Jose Rupa, and Lakon Cynthia M. 2017. “Peer Influence, Peer Selection, and Adolescent Alcohol Use: A Simulation Study Using a Dynamic Network Model of Friendship Ties and Alcohol Use.” Prevention Science 18:382–393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang Jun, Tong Liping, Lamberson Peter J., Durazo-Arvizu Ramón A., Luke Amy H., and Shoham David A. 2015. “Leveraging Social Influence to Address Overweight and Obesity using Agent-Based Models: The Role of Adolescent Social Networks.” Social Science & Medicine 125:203–213. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.