

Abstract
Objective:
Victimization is common in adolescence and is associated with negative outcomes, including school failure, and poor emotional, behavioral, and physical health. A deeper understanding of the risk of victimization can inform prevention and intervention efforts. This study tests the risky behavior model in adolescents, examining prospective associations between mean levels of and changes in delinquency and risk for victimization over four annual data collections.
Method:
Low-income adolescent (53.6% female; Mage = 12.13 years, SD = 1.62 years; 91.9% African American) and maternal caregiver dyads (N = 358) residing in urban neighborhoods in the mid-Atlantic region of the United States that had moderate-to-high levels of violence and/or poverty completed separate annual home interviews for 4 years. Maternal caregivers reported on adolescents’ delinquent behavior; adolescents reported on their victimization by community violence experiences.
Results:
Using a latent difference score model, results supported the risky behavior model for the first 2 years, but not the final data collection period. That is, levels of and changes in delinquent behavior were associated with more victimization by community violence at the subsequent time point for the first 2 study years. In contrast, there was no evidence for the opposite, specifically that victimization by community violence predicted delinquency.
Conclusion:
Knowing that both levels of delinquency and increases in delinquency place youth at heightened risk for victimization by community violence provides impetus to intervene. Screening for increases in delinquency among youth may be one way to target youth at high risk for victimization by community violence for fast-tracked intervention.
Keywords: risky behavior model, community violence exposure, delinquency, adolescents
Worldwide, about half of all youth report being victims of violence during the previous year (Hillis, Mercy, Amobi, & Kress, 2016). This makes childhood victimization more common than many other stressful life events, including parental death, divorce, or exposure to parental substance use disorder (Kessler et al., 2010). Youth who are victimized are more likely than nonvictimized youth to fare poorly in school (Holt, Finkelhor, & Kantor, 2007) show elevated levels of internalizing symptoms, such as depression, anxiety (Mrug & Windle, 2010), and posttraumatic stress disorder (Margolin & Vickerman, 2007), and report more physical health problems (Moffitt, 2013). Thus, understanding factors associated with risk for victimization—especially if they are modifiable—are important to developmental scientists, clinicians, and others working with youth.
One model that directly examines the etiology of victimization is the high-risk or risky behavior model (Bromet, Sonnega, & Kessler, 1998; Deykin & Buka, 1997; Giaconia et al., 2000; Haller & Chassin, 2014; Kilpatrick, Acierno, Resnick, Saunders, & Best, 1997). This model posits that individuals who engage in risky behaviors such as substance use and delinquency (e.g., destroying others’ things, lying) are more likely to be victimized. Specifically, these individuals may engage in risky behaviors such as sneaking out at night to spend time with friends and using substances, which may increase risk for violence. Much of the research on the risky behavior model has examined the link between substance use and victimization (Haller & Chassin, 2014), with few studies focusing on other externalizing or delinquent behaviors. The few articles testing whether delinquent behavior may precede victimization have yielded equivocal results, with some studies showing that externalizing behavior was associated with increased risk of victimization (Mrug & Windle, 2009; Schreck, Stewart, & Fisher, 2006), whereas another reported no association (Low & Espelage, 2014).
It is not clear why these studies showed discrepant findings. All three studies used two to three time points that were between 9 and 16 months apart and appeared to be well-powered (n: 603–1,500). The three studies varied in their race breakdown, but this does not account for the different findings, as the Mrug and Windle (2009) and Low and Espelage (2014) studies included a higher proportion of African Americans (78%, 52%, respectively), compared to the Schreck et al. (2006) study (15%). One possible explanation is that the two studies finding a significant effect of delinquent behavior on subsequent victimization either entirely or at least partially comprised urban participants, whereas the study failing to find this link recruited from a college town. The two studies finding effects of delinquency on victimization primarily asked about physical victimization (e.g., being beaten up) and included at least age and SES/family income as covariates. In contrast, the one study that did not find this association focused more on verbal victimization (e.g., made fun of) and did not include any demographic covariates. Thus, it may be that the risky behavior model is stronger among urban participants and/or when physical victimization is considered and when key covariates are included. All three of these studies examined levels of externalizing problems, rather than changes in externalizing behavior, and all relied on adolescent reports for both externalizing problems and victimization. The present study addresses important methodological gaps in this literature by examining both levels of and changes in parent-reported delinquency as predictors of subsequent adolescent-reported victimization in a sample of primarily African American urban youth.
All three of the previous studies also simultaneously examined whether a key alternative explanation might be explaining this link. Specifically, the self-medication model (Stewart, 1996) posits that individuals who experience violence may engage in risk-taking behaviors (e.g., substance use, delinquency) to cope with, or exert some control over, their mood and/or environment. In addition, general strain theory posits that those who are victimized experience anger, which increases the chances that they strive for “corrective action” in the form of delinquent activity (Ousey, Wilcox, & Fisher, 2011). The literature on victimization impacting externalizing behavior is vast (Coohey, Renner, & Sabri, 2013; Fowler, Tompsett, Braciszewski, Jacques-Tiura, & Baltes, 2009; Hay, & Evans, 2006; Mrug & Windle, 2010; Sullivan, Farrell, & Kliewer, 2006) and suggests that there is a prospective link. Thus, it is important that when testing the risky behavior model to simultaneously test for the alternate.
Relatively recently scholars interested in trying to understand the overlap between victimization and offending have attempted to understand the contexts in which this overlap occurs. For example, Berg, Stewart, Schreck, and Simons (2012) found that in contexts where there were strong neighborhood-level norms about violent conduct, there was substantial overlap between victimization and offending; however, this association was weak or nonexistent in contexts where neighborhood-level norms about violence were absent. Building on this theme of context, one way to gain clarity about relations between delinquency and victimization is to focus on one racial/ethnic group. African American youth are at higher risk than majority youth for both victimization and delinquency (Lanier, Maguire-Jack, Walsh, Drake, & Hubel, 2014; Leiber, Mack, & Feathersone, 2009) and have been studied less frequently, making them an appropriate focus of research attention. Further, recent analyses using a large multiracial sample from the National Longitudinal Study of Adolescent to Adult Health (Tillyer & Tillyer, 2016) found that minority adolescents were at heightened vulnerability to violent victimization when they engaged in some activities and minor forms of delinquency.
In addition to ruling out alternative hypotheses and focusing on African American youth, it is important to include a number of other potentially important covariates. Specifically, previous work suggests there are age-related trends in delinquency such that individuals tend to show sharp increases by the beginning of adolescence (Zhang, Loeber, & Stouthamer-Loeber, 1997). Regarding victimization, per year physical victimizations tend to remain fairly stable or increase slightly across late childhood through later adolescence, while emotional bullying tends to decrease (Finkelhor, Turner, Ormrod, & Hamby, 2009). There also are sex differences, such that males show higher levels of delinquency compared to females (Moffitt, Caspi, Rutter, & Silva, 2001). Females tend to be at higher risk for sexual victimization (Wellman, 1993), whereas males tend to be more at risk for physical abuse (Thompson, Kingree, & Desai, 2004). Thus, associations between key study constructs and age, sex, and race will be explored.
The Current Study
The current study tested the risky behavior model by examining whether levels of and increases in delinquent behavior prospectively predicted victimization by community violence (VBCV) at the next time point, using data collected annually for 4 years. The present study addressed several gaps in the current literature. First, although most studies assess levels of externalizing behavior in tests of this model, the current study models both levels of delinquent behavior as well as changes in delinquent behavior. In addition, this study simultaneously models the alternative hypothesis, specifically that VBCV may precede delinquent behavior (i.e., self-medication model, or general strain theory). Third, it tests for effects of age, sex, and race. Finally, this study examines these questions in African American youth, an understudied group. Thus, the primary hypothesis for this study is that we will find support for the risky behavior model, specifically, that higher levels of and greater changes in delinquency will predict VBCV. In addition to testing this hypothesis, we will examine two other research questions: whether VBCV is prospectively associated with changes in delinquent behavior (alternative hypothesis) and whether the covariates of age, sex, and race are associated with VBCV and delinquency.
Method
Participants
Participants were 358 adolescents (53.6% female; M age = 12.13, SD = 1.62 years; 91.9% African American) and their maternal caregivers (86.3% were the child’s biological mother) enrolled in a 4-year longitudinal study of the effects of chronic environmental stressors on youth development. Much of the sample was poor; median household income from all sources at the start of the study was $401 to $500 per week. Educational attainment was diverse, but low overall. About one fourth of caregivers (23.0%) had less than a high school education. Close to a third of caregivers completed high school or earned a general education degree (general educational development; 31.2%), another 36.5% completed some college, or earned an associate’s or vocational degree, and 9.3% earned a bachelor’s degree or higher. Two thirds (40.6%) had never married. A third (31.9%) were married/cohabiting, 14.3% were separated, 11.2% were divorced, and 2% were widowed.
Procedure
The Institutional Review Board at Virginia Commonwealth University approved all study procedures. Participants were recruited from urban neighborhoods in the mid-Atlantic region of the United States that had moderate to high levels of violence and/or poverty according to police statistics and 2000 census data. Qualifying neighborhoods were canvassed via flyers posted door-to-door, and information about the study was presented at community events and through community agencies. Families were eligible if they spoke English, had a fifth or an eighth grader, and if the primary female caregiver could be present for the interview. In all, 63% of eligible participants agreed to be in the study, better than those of many community studies recruiting from disadvantaged neighborhoods (Luthar & Goldstein, 2004; Tingen et al., 2013). It was never the case that more than one child in the household was eligible to participate in the study, thus caregivers reported on the child participating in the study. Interviews were conducted annually for four data collection periods, primarily in participants’ homes, by trained research staff. Interviews began December 27, 2004, and ended June 17, 2009. Interviewers thoroughly reviewed the parent consent forms with the family before separating caregivers and adolescents and conducting a separate assent procedure with the adolescent. A Certificate of Confidentiality was obtained from the National Institutes of Health to protect families’ responses since adolescents were reporting on illegal behavior. Face-to-face interviews using visual aids were used to collect the data, and most questions were read aloud. Adolescents who passed a reading-screening test answered several sensitive questions in a booklet without interviewer assistance.
Interviewer training was thorough, taking place over 4 weeks. Interviewers completed training on research protocols and interview techniques, and completed practice sessions, paperwork, and related assignments. Research staff trained and gave feedback to the interviewers before they could start the interview process. Interviewers typically had bachelor’s degrees or master’s degrees, although a small percentage had not yet completed a degree. Interviewers ranged in age from 20 to 55, and included both men and women. Approximately half of the interviewing staff was African American. Tests for effects of interviewer race and sex revealed no systematic biases (all ps > .05). Interviews lasted approximately 2.5 hr and participants received $50 in gift cards/family each year. In addition, families received information about discounted health insurance for children and other resources at the time of the interview.
Measures
Victimization by community violence (VBCV)/.
At each of the four study timepoints youth reported on their past year VBCV using questions from the Survey of Children’s Exposure to Violence (Richters & Saltzman, 1990). Youth reported how often they had experienced seven types of victimization including being chased by gangs or older youth; asked to sell drugs; asked to use drugs; threatened with physical harm; slapped, hit, or punched; beaten up or mugged; or being in another situation where they felt scared and thought they would be hurt badly or die. Given the research on African American youth finding that some choose not to disclose their experiences with victimization to caregivers because they fear restriction of activities and freedom (Dinizulu, Grant, & McIntosh, 2014) we chose to use youth report of VCBV. These items began with the stem, “How many times in the past year have you yourself been …” Response options included 0 (never), 1 (1–8 times), 2 (once a month), 3 (once a week), and 4 (almost every day). Responses were summed to create a total victimization score. Correlations across the four timepoints ranged from .26 to .56, all ps < .001, with strongest correlations observed for contiguous years. Fowler, Tompsett, et al. (2009) reported that the Survey of Children’s Exposure to Violence is the most frequently used tool to assess youth’s exposure to community violence, and it appears to have good predictive validity. Cronbach αs in the present study ranged from .51 to .62 across the four study time points, which is quite low. However, it would not be expected that these items would necessarily hang together. It is atypical to report reliabilities for count variables of traumas/victimizations experienced because the experiences are not unidimensional (Dusing, Richards, Ochoa, & Onyeka, 2020).
Delinquency.
Caregivers reported on adolescent delinquency using the 13-item delinquency subscale from the Child Behavior Checklist (CBCL; Achenbach, 1991). Delinquent behaviors assessed in the scale include lack of guilt after misbehavior; lying or cheating; running away from home; setting fires; stealing at home and outside the home; truancy; vandalism; alcohol or drug use; use of obscene language; rumination about sex; preference for being with older youth; and hanging around with youth who get into trouble. Caregivers indicated how frequently their child engaged in specific behaviors over the past 3 months using a 3-point scale, ranging 0 (not true [as far as you know]), 1 (somewhat or sometimes true), and 2 (very true or often true). Scores are summed, and higher scores indicate more delinquent behavior. As one of the items (sets fires) was endorsed by no one at the third time point, this item was omitted from the composite scores as well as the invariance testing described in the following text. The CBCL is the most widely used parent-report measure of youth adjustment problems and has excellent reliability and validity (Achenbach, 1991). For example, the externalizing subscales of the CBCL have test–retest reliability coefficients ranging from .64 to .69, and discriminated between clinic-referred and nonreferred children (Achenbach, 1991). In addition, these subscales were highly correlated with observational rating of on-task behaviors (Achenbach, 1991). The Cronbach’s α coefficients for our sample were between .70 and .80 across the four study timepoints, which is similar to other alphas using the CBCL, at least for the Aggression subscale (Kennedy & Ceballo, 2016).
To support the creating of a single sum score composite from the delinquency items for each of the 4 assessments, confirmatory factor analyses were conducted for two purposes. First, the 13 delinquency items at each assessment period were fit to a single common factor model to test for their configural unidimensionality. Second, longitudinal item metric and scalar measurement invariance was tested jointly to determine if the latent variable delinquency construct was being equivalently defined at each of the waves.
Demographics.
Youth reported their biological sex, age, and race. Sex was coded 1 = male, 2 = Female. For race, youth were asked, “What race do you consider yourself to be? You can choose more than one.” Response options included Asian American, African American, Hispanic or Latino/a, White, Caucasian, or European, American Indian, or other. Pilot testing indicated that youth did not distinguish between race and ethnicity. These distinctions were not probed in this study. For analytic purposes, race was dichotomized into African American (0) versus other (1) given the sample distribution.
Attrition and Missingness in Sample
Attrition varied across the study time points, with 89.1% of the sample (N = 319) retained at Time 2, 84.0% of that sample (N = 268) retained at Time 3, and 92.2% of the Time 3 sample (N = 247) retained at Time 4. At Time 4, 69.0% of the original Time 1 sample participated. At each time point, youth who remained in the study versus youth who attrited were compared on demographics (age, sex), delinquency, and VBCV using χ2 and t tests as appropriate to determine if there were systematic differences on the study variables between these two groups of youth. Comparisons between youth who attrited by Time 2 and youth who remained in the study on Time 1 variables revealed no differences in attrition by sex, χ2(1) = 0.50, p = .50; age, t(356) = 1.18, p = .24; delinquency, t(355) = −0.46, p = .65; or VBCV, t(354) = −.074, p = .94. Comparisons between youth who attrited by Time 3 similarly revealed no differences in attrition by sex, χ2(1) = 0.82, p = .39; age, t(356) = 1.81, p = .07; delinquency, t(355) = 1.46, p = .15; or victimization, t(354) = 1.05, p = .29. This pattern continued at Time 4 for delinquency, t(355) = 1.71, p = .09 and VBCV, t(354) = 1.13, p = .26. However, at Time 4 a greater percentage of males (36.7%) than females (26.0%) had left the study, χ2(1) = 4.77, p = .03, and adolescents who attrited were older (Mage = 12.45, SD = 1.71 years) than adolescents who remained in the study (Mage = 11.98, SD = 1.57 years), t(356) = 2.53, p = .012. An execution of Little’s missing completely at random (MCAR) test yielded χ2(76) = 75.034, with a NS p value, suggesting that data on the delinquency and VBCV at all time points are MCAR.
Data Analytic Plan
To test study questions, a latent difference score model (Kievit et al., 2018; Klopack & Wickrama, 2020; McArdle, 2001; McArdle, & Hamagami, 2001) was conducted. This approach builds on an autoregressive cross panel model, which examines effects of constructs on one another across time, controlling for the time-stable effects. Within these models, the residual from the autoregression of a variable assessed at t + 1 on the same variable at t becomes a difference score when the autoregression coefficient is fixed to 1 (i.e., perfect prediction). Within these models, disturbances associated with each endogenous variable are set equal to 0 to aid in model identification (Newsom, 2015). This model was estimated within a structural equation modeling framework in Mplus Version 8 (Muthen & Muthen, 1998–2017). As data are MCAR, we used full information maximum likelihood, using the maximum likelihood robust estimator, robust to nonnormality of variables (Muthen, 2013). The parameters of interest were baseline (Year 1) past 3-month delinquent behavior, Year 2 delinquent behavior, Year 3 delinquent behavior, Year 4 delinquent behavior, and change between each time point. For each occasion except the first, a latent variable representing the difference was specified with a loading set to 1, and the auto-regressive parameters between each observed variable were set to 1. Correlations among baseline delinquent behavior and change scores were estimated. Other parameters of interest were Year 1 to Year 4 past year VBCV.
The primary study hypothesis was that levels of and changes in delinquent behavior would prospectively predict VBCV at the next time point. The alternative hypothesis and second question was whether VBCV would predict levels of change in delinquent behavior, and the third question was whether demographic covariates would be significantly associated with either VBCV or delinquency. Positive effects on change scores suggest that higher values of a predictor or covariate are associated with more change. As the preliminary linear growth model of delinquent behavior in this dataset suggests that the linear growth component is positive, predictors/covariates associated with “greater change” in symptoms signify factors related to increased linear growth.
Zero-order correlations between child sex, age, and race with delinquency and VBCV were examined to test whether this model ought to be stacked on these constructs in the form of multiple group models. If, in the context of a multiple group model, the χ2 difference test suggested a significant decrease in fit by forcing paths to be equal across groups, a model stacked on sex or grade would be pursued. If the test suggested no significant decrease in fit, one overall model would be used as the final model. If one overall model was selected, sex, grade, and race would be initially entered as covariates, but omitted if nonsignificant (p < .05).
Results
Preliminary Analyses
At baseline, nearly two thirds (65.9%) of the youth in this study reported at least one VBCV event in the previous year, and a third of the sample (33.5%) reported two or more VBCV experiences the year prior. These statistics were fairly consistent across subsequent years, dropping slightly for overall VBCV by Time 4. Figure 1 displays the occurrence of specific VBCV experiences in the past year by study time point. As seen in Figure 1, the most commonly reported VBCV experience by far was being slapped, punched, or hit. Other frequent VBCV experiences included being threatened with serious physical harm; feeling so scared in a situation that the threat of physical injury or death felt imminent; and being asked to use or to sell drugs—the only two types of VBCV that more, versus fewer, youth experienced consistently over time.
Figure 1.
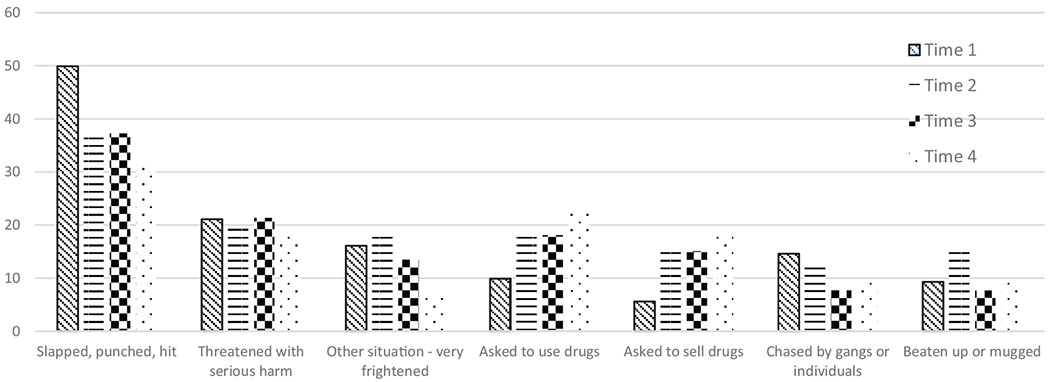
Percentage of the sample who experienced specific types of victimization in the past year at each time point.
Table 1 presents descriptive statistics and bivariate correlations for delinquency and VBCV across all study timepoints based on nonimputed data. With the exception of one correlation, all associations between delinquency and VBCV within and across time points were significant. With respect to demographic associations with delinquency and VBCV, patterns of association were more strongly associated with age and sex than race. Age was significantly and positively associated with delinquency at Time 1, r = .16, p = .002 and with VBCV at Times 2, r = .18, p = .002 and 4, r = .15, p = .02. For sex, caregivers reported that males had higher levels of delinquency than females at Time 1, t(355) = 2.82, p = .005 and Time 2, t(310) = 2.04, p = .042; and adolescent males reported more VBCV than females at all time points, Time 1 t(356) = 4.56, p < .001; Time 2 t(316) = 4.31, p < .001; Time 3 t(269) = 5.00, p < .001; and Time 4 t(245) = 3.37, p = .001. Comparisons across race (African Americans vs. non-African Americans) yielded no significant differences.
Table 1.
Descriptive Information on and Associations Between Caregiver-Reported Delinquency and Adolescent-Reported Victimization Across the Four Study Time Points
| Variable | T1 Del | T2 Del | T3 Del | T4 Del | T1 Vic | T2 Vic | T3 Vic | T4 Vic | M | SD | Range |
|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 Del | — | .63*** | .55*** | .51*** | .24*** | .38*** | .22*** | .19** | 3.08 | 2.79 | 0–13 |
| T2 Del | — | .65*** | .65*** | .25*** | .37*** | .25*** | .11 | 3.07 | 3.15 | 0–21 | |
| T3 Del | — | .74*** | .17** | .29*** | .29*** | .19** | 2.93 | 2.89 | 0–15 | ||
| T4 Del | — | .16* | .24*** | .20** | .20** | 3.15 | 3.49 | 0–18 | |||
| T1 Vic | — | .49*** | .48*** | .26*** | 1.49 | 1.76 | 0–9 | ||||
| T2 Vic | — | .53*** | .34*** | 1.59 | 2.04 | 0–11 | |||||
| T3 Vic | — | .41*** | 1.43 | 1.86 | 0–12 | ||||||
| T4 Vic | — | 1.32 | 1.78 | 0–9 |
Note. Del = Delinquency; Vic = Victimization.
p < .05.
p < .01.
p < .001.
The results of the two psychometric validity analyses for evaluating the delinquency construct are as follows. The configural invariance test of a single unidimensional common factor for the 12 items across the 4 timepoints resulted in satisfactory omnibus model fits (confirmatory fit index [CFI] = 0.972, Tucker–Lewis Index [TLI] = 0.968, and root mean square error of approximation [RMSEA] = 0.017, confidence interval [CI] [0.009, 0.023]). Forcing joint metric (factor loadings) and scalar (item thresholds) invariance and using the configural model as a baseline comparison produced no evidence of noninvariance of the delinquency factor across the timepoints (, p = .053; CFI = 0.971, ΔCFI = 0.001; TLI = 0.968, ΔTLI = 0.000; RMSEA = 0.017, CI = [0.009, 0.023]; ΔRMSEA = 0.000). These modeling results provide support for creating single composite sum scores from the 12 delinquency items at each of the assessment time-points.
Test of Our Primary Hypothesis
Given that age and sex were associated with delinquency and VBCV across multiple time points, we initially tested whether the model we intended to test should be stacked on child sex or child grade at baseline. Specifically, we estimated multigroup models in which all parameters were set equal to one another for males and females, χ2 = 126.86 (52), and then allowed to be freely estimated, χ2 = 102.99 (32), and then set equal for fifth graders at baseline and 8th graders at baseline, χ2 = 129.74 (52), and then allowed to be freely estimated, χ2 = 103.63 (32). Both χ2 difference tests indicate that there was not a significant decrease in fit when paths were constrained to be equal across sex, χ2 difference = 23.86 (20), NS, or grade, χ2 difference = 26.11 (20), NS. Therefore, one overall model, not stacked on sex or grade at baseline, was estimated as part of the final model.
The final latent difference score model indicated good fit, χ2(19) = 43.86, RMSEA: .07; CFI: .96; SRMR: .04. In testing our hypothesis, at the first two lags, both levels and changes in delinquent behavior were associated with VBCV at the next time point. Specifically, those adolescents whose caregivers reported more delinquent behavior at Year 1 (β = .29, p < .001) and who reported increases in delinquent behavior between Year 1 and Year 2 (β = .12, p < .05) were likely to report more VBCV in Year 2. In addition, those adolescents whose caregivers reported more delinquent behavior at Year 2 (β = .16, p < .05) and who reported greater increases in delinquent behavior between Year 2 and Year 3 (β = .18, p < .05) were likely to report more VBCV in Year 3. Neither Year 3 delinquent behavior nor changes in delinquent behavior between Years 3 and 4 were associated with VBCV in Year 4.
Testing the Two Additional Research Questions
In testing the second research question, there was no support for the alternative to our hypothesis—the self-medication model. That is, at no time point did number of VBCV predict change in delinquency at the subsequent time point. Regarding covariates, our third research question, the story was mixed. Race was not associated with VBCV or delinquent behavior at any time point so it was dropped from the analyses. Sex and age were associated with Year 1 past 3 months delinquent behavior, such that males (β = −.13, p < .01) and older children (β = .14, p < .01) had parents who reported more delinquency. Additionally, males reported more VBCV at Year 1 (β = −.24, p < .001), and males (β = −.11, p < .05) and older children (β = .13, p < .01) reported more at Year 2. Finally, males reported more VBCV at Year 3 (β = −20, p < .001). See Table 2 and Figure 2 for depiction of findings. Finally, consistent with the univariate analyses, stability paths for VBCV were all significant. Specifically, those with more past year VBCV at Year 1 reported more past year VBCV at Year 2 (β = .39, p < .001), which was related to more past VBCV at Year 3 (β = .47, p < .001), which predicted past year VBCV at Year 4 (β = .40, p < .001), the final year of data collection.
Table 2.
Unstandardized Regression Coefficients, Standard Errors, Standardized Regression Coefficients, and 95% Confidence Intervals (for Unstandardized Effects) for Final Study Model
| Variable | B | SE | β | 95% confidence interval |
|---|---|---|---|---|
| Time 1 Delinquency | ||||
| Age | .23** | .09 | .14** | [0.07, .40] |
| Sex | −.75** | .28 | −.13** | [−1.30, −.20] |
| Delinquency-Deviation 1 | ||||
| Time 1 Victimization | .06 | .10 | .04 | [−0.13, .25] |
| Delinquency-Deviation 2 | ||||
| Time 2 Victimization | −.03 | .09 | −.02 | [−0.21, −.16] |
| Delinquency-Deviation 3 | ||||
| Time 3 Victimization | −.07 | .10 | −.06 | [−0.26, .11] |
| Time 1 Victimization | ||||
| Sex | −.83*** | .19 | −.24*** | [−1.19, −.46] |
| Time 2 Victimization | ||||
| Age | .17** | .06 | .13** | [0.06, .28] |
| Sex | −.45* | .20 | −.11* | [−0.83, −.06] |
| Time 1 Delinquency | .21*** | .04 | .29*** | [0.13, .29] |
| Delinquency Deviation 1 | .10* | .05 | .12* | [0.01, .18] |
| Time 1 Victimization | .46*** | .07 | .39*** | [0.31-.60] |
| Time 3 Victimization | ||||
| Sex | −.75*** | .19 | −.20* | [−1.12, −.38] |
| Time 2 Delinquency | .10* | .04 | .16* | [0.02, .17] |
| Delinquency Deviation 2 | .13* | .06 | .18* | [0.03, .24] |
| Time 2 Victimization | .44*** | .07 | .47*** | [0.30-.58] |
| Time 4 Victimization | ||||
| Time 3 Delinquency | .07 | .05 | .12 | [−0.02, .16] |
| Delinquency Deviation 3 | .05 | .05 | .06 | [−0.32, .11] |
| Time 3 Victimization | .37*** | .07 | .40*** | [0.24, .50] |
Note. Note that as part of the latent change score model, stability paths for delinquency, and effects of change scores on delinquency at the next time point were set to 1; although modeled, these effects are not displayed.
p < .05.
p < .01.
p < .001.
Figure 2.
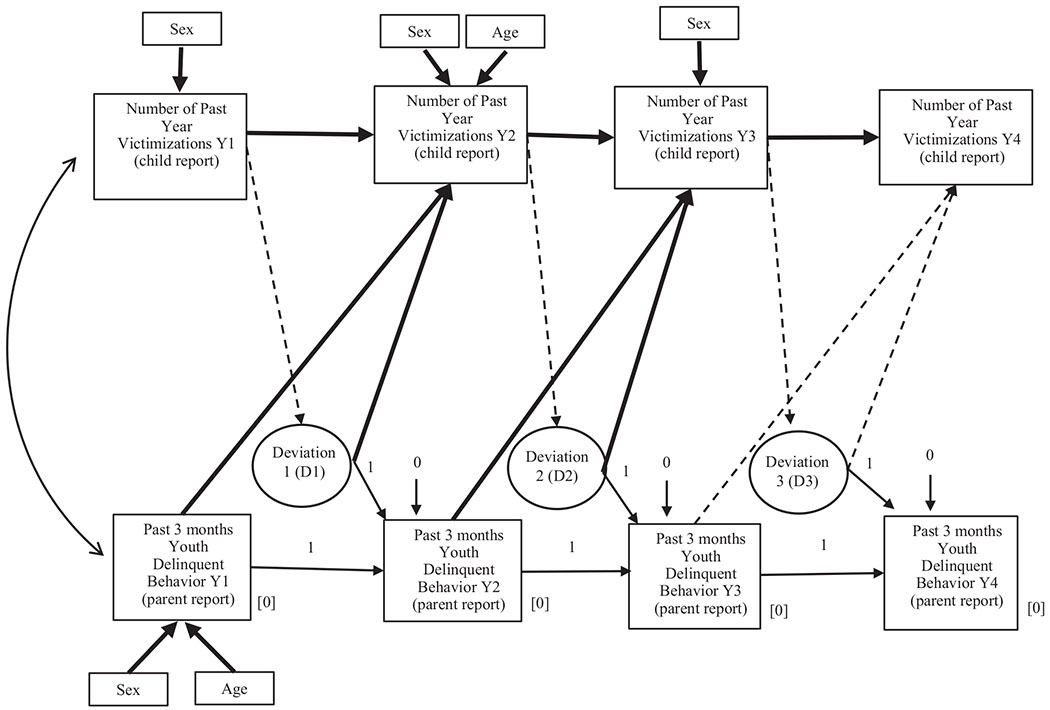
Final study results.
Post Hoc Power Analyses
In addition to estimating the various model parameters described above, we used Mplus to conduct Monte Carlo (MC) stimulations (Muthen & Muthen, 2002) to empirically determine what power we had to detect the different hypothesized model effects. We had sufficient power (>.8) to detect some of the path effect sizes in the risky behavior model, but none of the path effects in the self-medication model. Specifically, with our sample size of n = 358, we had sufficient power to detect effects of change in, and levels of, delinquency on victimization for the first two time lags. The MC simulation results indicated insufficient power to detect effects of victimization on changes in delinquency. Furthermore, we extended the power analyses by examining sample sizes of n = 750, 1,000, 2,000, 5,000, and 10,000, to determine what sample sizes would be needed to obtain sufficient power to statistically detect these effects. The MC simulations indicated that we did not have sufficient power to detect these effects at the first two lags until a sample size of n = 10,000, and even with such a large sample size, would not detect effects at the third lag. Thus, although we cannot rule out the possibility that we did not find significant effects for the self-medication model because we were underpowered, these MC simulation results suggest extreme and unreasonably large sample sizes would be needed to be able to detect such effects.
Discussion
This study tested one primary hypothesis: (a) whether higher levels of and greater changes in delinquency predicted subsequent VBCV, consistent with the risky behavior model. Simultaneously, the study tested two additional research questions: (b) whether VBCV was prospectively associated with changes in delinquent behavior, consistent with the self-medication model, and whether (c) age, sex, and race were associated with VBCV and delinquency. Results of each will be discussed in turn.
In general, we found support for the risky behavior model. Specifically, at two of the three (i.e., the first two) time lags, youth with higher levels of delinquency and youth with greater reported changes in delinquency experienced more VBCV. These findings replicate prior work in this area reporting that higher levels of delinquency were associated with more VBCV, at least among adolescents living in urban areas (Mrug & Windle, 2009; Schreck et al., 2006). In addition, these findings extend this area of work by showing that it is not only higher levels, but also increases in delinquency, that are associated with higher risk for VBCV. These findings suggest that even if adolescents are not engaging in high levels of delinquency, they may be at risk for subsequent VBCV if they show an increase in these externalizing behaviors. The results we report here also extend prior work by suggesting that such findings hold when different reporters are used to assess VBCV and delinquency, thus providing confidence that mono-reporter bias is not driving the observed associations.
Interestingly, we found no support for the self-medication model or general strain theory. That is, at none of our three time lags was VBCV prospectively linked to changes in delinquency. Although there is a literature citing prospective associations of VBCV with delinquency (Coohey et al., 2013; Fowler, Toro, Tompsett, & Baltes, 2009; Hay, & Evans, 2006; Mrug & Windle, 2010; Sullivan et al., 2006), all of these studies examined levels of (vs. changes in) VBCV and delinquency, used adolescent reports of both VBCV and delinquency, and did not simultaneously model the prospective associations from delinquency to VBCV. Thus, although those who experience more VBCV may be at risk for engaging in higher levels of delinquency, it does not seem to be the case that those who experience more VBCV then show greater changes in delinquency. It may also be that the significant association between VBCV and subsequent delinquency in the larger literature is being driven by some shared reporter bias, and that when multiple reporters are utilized, this association disappears.
Finally, multiple subgroups of individuals may exist—some of whom are more likely to respond to VBCV in a manner consistent with the self-medication model, whereas others are more likely to respond to delinquency consistent with the risky behavior model. A third group may be vulnerable to both pathways. Additional research in this area, including mixture models that allow for extraction of potentially latent groups (e.g., latent class or latent profile analysis), is needed to better understand under what circumstances links in the self-medication model may or may or not hold.
In terms of demographic covariates, race was unrelated to all study variables, so it was dropped from the analyses. We expected racial differences in the frequency of VBCV and delinquency given the racial and ethnic differences in these constructs reported in prior literature (Lanier et al., 2014; Leiber et al., 2009). These nonsignificant findings may have been driven by lack of power, as most (91.9%) of the sample was African American.
Interestingly, although fit estimates did not support use of multiple group models stacked on grade or sex, being male and an older adolescent were sporadically associated with VBCV and delinquency. Specifically, males reported more VBCV than females. As our victimization measure focused on physical victimizations (e.g., being slapped, chased, beaten up), this sex difference is consistent with a larger literature finding that boys tend to experience more physical aggression than girls (Thompson et al., 2004). At the second and fourth time points, older adolescents reported more VBCV than younger adolescents. Although the literature in this area is quite small, this finding is generally consistent with prior work finding that the likelihood of physical victimizations seems to tend to increase slightly between late childhood and later adolescence (Finkelhor et al., 2009).
In terms of age and sex differences in delinquency, males and older children had parents who reported more delinquency early in the study, but not at later time points. That older adolescents displayed more delinquency early in the study compared to younger adolescents is somewhat consistent with work finding that individuals tend to show increases in delinquency in the transition to adolescence (Zhang et al., 1997). However, it is not clear why this difference did not hold at later time points. One possibility is that with age and increased cognitive maturity, adolescents were not less delinquent, but became more adept at hiding their behavior from their parents, or “strategically disclosing” information to them (Jäggi, Drazdowski, & Kliewer, 2016).
Similarly, although the finding that males show higher levels of delinquency fits with prior work (Moffitt et al., 2001), it is not entirely clear why this finding also did not extend past the early time points. One possible explanation is that there are fewer observed sex differences in delinquency among African American youth relative to youth of other races and ethnicities (Jang, 1993). Using six waves of panel data collected from urban, African American adolescents participating in the Rochester Youth Development study, Jang found that while African American boys were more delinquent than African American girls, the sexes were comparable on the type of offenses in which they engaged. Boys engaged in more serious offenses more often, and these types of offenses accounted for a greater proportion of boys’ total delinquent activity, which largely accounted for the male-female differences in delinquency. None-the-less, Jang found fewer sex differences in this urban African American sample relative to other studies, which he partly attributed to more equal treatment of the sexes in African American compared to White families.
Limitations
This study has a number of strengths, including use of multiple reporters, a longitudinal design, and the ability to rule out an alternative explanation in finding support for the risky behavior model. However, it is important to acknowledge its limitations. First, we relied on survey measures, rather than using multimodal assessments (e.g., diagnostic interviews). Thus, there may be bias common to parent and adolescent report of these constructs that affected our findings. Second, as we included maternal-adolescent dyads, we cannot say whether findings would have held if we used paternal reports as well. Third, we chose to assess and utilize youth reports of victimization because of prior work finding that African American youth who were victimized chose not to disclose this information because of fear that their freedoms would be restricted (Dinizulu et al., 2014). We chose to assess and utilize maternal reports of delinquency to reduce the threat of mono-reporter bias. However, it is possible that youth underreported their victimization experiences and/or that mothers over- or underreported their child’s delinquent behavior. Thus, our findings may be limited to models in which youth report of victimization and maternal reports of delinquency are used. Finally, because our study was comprised of primarily African American, urban adolescents, we could not test for differences based on living in rural versus urban settings. Thus, findings may not generalize to those who are not urban and African American.
Research Implications
These findings have important research-related implications. This study uses a latent difference model to test reciprocal relations between delinquency and VBCV. In so doing, this study found that in an urban sample of primarily African American adolescents, delinquency and changes in delinquency are stronger drivers of VBCV than VBCV is of changes in delinquency. This may be due to the nature of the types of victimizations endorsed. Specifically, adolescents who are destructive, lie, and break rules are more likely to place themselves in social situations in which physical victimizations are more likely to occur. The fact that we did not find support for the reverse suggests that after taking these associations into account, there is no unique impact of physical victimization on changes in delinquency.
Clinical Implications
These findings have important clinical implications. Specifically, it is useful for clinicians working with adolescents to understand that youth who display more, as well as increases in, delinquent behavior, are at risk to be physically victimized. In terms of implications for clinical work, it may be useful for clinicians to assess current levels of delinquency, and whether delinquent behaviors have recently increased, as those with increasing delinquency are more likely to be victimized. Thus, current levels of and changes in delinquency may be useful screening tools to identify those at risk for experiencing more VBCV. Once clinicians have identified youth at risk for VBCV, it may be useful for them to talk with them about the impact that rule-breaking behaviors may have on risk for violence exposure. Ideally, clinicians would be able to help adolescents engage in positive activity scheduling, involvement with extracurricular pursuits and with prosocial peers that may give them skills for the future, in an effort to reduce risk for subsequent physical victimizations.
Acknowledgments
The authors have no known conflicts of interest to disclose. Data reported in this article was supported by funding from the National Institute on Drug Abuse Grants K01 DA015442 01A1 and R21 DA 020086-02 awarded to Wendy Kliewer. Writing of this article was supported by the National Institute on Alcohol Abuse and Alcoholism Grant 1 KO1 AA028058-01 and the Virginia Commonwealth University Presidential Research Quest (PeRQ) Fund awarded to Kaitlin Bountress.
Contributor Information
Kaitlin Bountress, Department of Psychiatry, School of Medicine and Virginia Institute for Psychiatric and Behavioral Genetics, Virginia Commonwealth University.
Steven H. Aggen, Department of Psychiatry, School of Medicine and Virginia Institute for Psychiatric and Behavioral Genetics, Virginia Commonwealth University.
Wendy Kliewer, Department of Psychology, Virginia Commonwealth University.
References
- Achenbach TM (1991). Manual for the Child Behavior Checklist/4–18 and 1991 Profile. Burlington: University of Vermont, Department of Psychiatry. [Google Scholar]
- Berg MT, Stewart EA, Schreck CJ, & Simons RL (2012). The victim–offender overlap in context: Examining the role of neighborhood street culture. Criminology, 50, 359–390. 10.1111/j.1745-9125.2011.00265.x [DOI] [Google Scholar]
- Bromet E, Sonnega A, & Kessler RC (1998). Risk factors for DSM–III–R posttraumatic stress disorder: Findings from the National Comorbidity Survey. American Journal of Epidemiology, 147, 353–361. 10.1093/oxfordjournals.aje.a009457 [DOI] [PubMed] [Google Scholar]
- Coohey C, Renner LM, & Sabri B (2013). Victimization, parenting, and externalizing behavior among Latino and White adolescents. Journal of Family Violence, 28, 359–368. 10.1007/s10896-013-9503-3 [DOI] [Google Scholar]
- Deykin EY, & Buka SL (1997). Prevalence and risk factors for posttraumatic stress disorder among chemically dependent adolescents. The American Journal of Psychiatry, 154, 752–757. 10.1176/ajp.154.6.752 [DOI] [PubMed] [Google Scholar]
- Dinizulu SM, Grant KE, & McIntosh JM (2014). The influence of nondisclosure on the mental health of urban African-American adolescents exposed to community violence. Journal of Prevention and Intervention in the Community, 42, 208–220. 10.1080/10852352.2014.916583 [DOI] [PubMed] [Google Scholar]
- Dusing CR, Richards M, Ochoa N, & Onyeka C (2020). Children’s exposure to violence across contexts in relation to posttraumatic stress symptoms. Psychology of Violence, 10, 182–191. 10.1037/vio0000247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finkelhor D, Turner H, Ormrod R, & Hamby SL (2009). Violence, abuse, and crime exposure in a national sample of children and youth. Pediatrics, 124, 1411–1423. 10.1542/peds.2009-0467 [DOI] [PubMed] [Google Scholar]
- Fowler PJ, Tompsett CJ, Braciszewski JM, Jacques-Tiura AJ, & Baltes BB (2009). Community violence: A meta-analysis on the effect of exposure and mental health outcomes of children and adolescents. Development and Psychopathology, 21, 227–259. 10.1017/S0954579409000145 [DOI] [PubMed] [Google Scholar]
- Fowler PJ, Toro PA, Tompsett CJ, & Baltes BB (2009). Community and family violence: Indirect effects of parental monitoring on externalizing problems. Journal of Prevention and Intervention in the Community, 37, 302–315. 10.1080/10852350903196308 [DOI] [PubMed] [Google Scholar]
- Giaconia RM, Reinherz HZ, Hauf AC, Paradis AD, Wasserman MS, & Langhammer DM (2000). Comorbidity of substance use and post-traumatic stress disorders in a community sample of adolescents. American Journal of Orthopsychiatry, 70, 253–262. 10.1037/h0087634 [DOI] [PubMed] [Google Scholar]
- Haller M, & Chassin L (2014). Risk pathways among traumatic stress, posttraumatic stress disorder symptoms, and alcohol and drug problems: A test of four hypotheses. Psychology of Addictive Behaviors, 28, 841–851. 10.1037/a0035878 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hay CE, & Evans MM (2006). Violent victimization and involvement in delinquency: Examining predictions from general strain theory. Journal of Criminal Justice, 34, 261–274. 10.1016/j.jcrimjus.2006.03.005 [DOI] [Google Scholar]
- Hillis S, Mercy J, Amobi A, & Kress H (2016). Global prevalence of past-year violence against children: A systematic review and minimum estimates. Pediatrics, 137, e20154079. 10.1542/peds.2015-4079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holt MK, Finkelhor D, & Kantor GK (2007). Multiple victimization experiences of urban elementary school students: Associations with psychosocial functioning and academic performance. Child Abuse and Neglect, 31, 503–515. 10.1016/j.chiabu.2006.12.006 [DOI] [PubMed] [Google Scholar]
- Jäggi L, Drazdowski TK, & Kliewer W (2016). What parents don’t know: Disclosure and secrecy in a sample of urban adolescents. Journal of Adolescence, 53, 64–74. 10.1016/j.adolescence.2016.08.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jang SJ (1993). Sex differences in delinquency among African-American adolescents: A longitudinal study (Unpublished doctoral thesis). State University of New York at Albany, Albany, NY. [Google Scholar]
- Kennedy TM, & Ceballo R (2016). Emotionally numb: Desensitization to community violence exposure among urban youth. Developmental Psychology, 52, 778–789. 10.1037/dev0000112 [DOI] [PubMed] [Google Scholar]
- Kessler RC, McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, … Williams DR (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. The British Journal of Psychiatry, 197, 378–385. 10.1192/bjp.bp.110.080499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kievit RA, Brandmaier AM, Ziegler G, van Harmelen AL, de Mooij SMM, Moutoussis M, … Dolan RJ (2018). Developmental cognitive neuroscience using latent change score models: A tutorial and applications. Developmental Cognitive Neuroscience, 33, 99–117. 10.1016/j.dcn.2017.11.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kilpatrick DG, Acierno R, Resnick HS, Saunders BE, & Best CL (1997). A 2-year longitudinal analysis of the relationships between violent assault and substance use in women. Journal of Consulting and Clinical Psychology, 65, 834–847. 10.1037/0022-006X.65.5.834 [DOI] [PubMed] [Google Scholar]
- Klopack ET, & Wickrama K (2020). Modeling latent change score analysis and extensions in Mplus: A practical guide for researchers. Structural Equation Modeling, 27, 97–110. 10.1080/10705511.2018.1562929 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanier P, Maguire-Jack K, Walsh T, Drake B, & Hubel G (2014). Race and ethnic differences in early childhood maltreatment in the United States. Journal of Developmental and Behavioral Pediatrics, 35, 419–426. 10.1097/DBP.0000000000000083 [DOI] [PubMed] [Google Scholar]
- Leiber M, Mack KY, & Feathersone RA (2009). Family structure, family processes, economic factors, and delinquency: Similarities and differences by race and ethnicity. Youth Violence and Juvenile Justice, 7, 79–99. 10.1177/1541204008327144 [DOI] [Google Scholar]
- Low S, & Espelage D (2014). Conduits from community violence exposure to peer aggression and victimization: Contributions of parental monitoring, impulsivity, and deviancy. Journal of Counseling Psychology, 61, 221–231. 10.1037/a0035207 [DOI] [PubMed] [Google Scholar]
- Luthar SS, & Goldstein A (2004). Children’s exposure to community violence: Implications for understanding risk and resilience. Journal of Clinical Child and Adolescent Psychology, 33, 499–505. 10.1207/s15374424jccp3303_7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Margolin G, & Vickerman KA (2007). Post-traumatic stress in children and adolescents exposed to family violence: I. Overview and issues. Professional Psychology: Research and Practice, 38, 613–619. 10.1037/0735-7028.38.6.613 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McArdle JJ (2001). A latent difference score approach to longitudinal dynamic structural analyses. In Cudeck R, Toit SD, & Sörbom D (Eds.), Structural equation modeling: Present and future (pp. 342–380). Lincolnwood, IL: Scientific Software International. [Google Scholar]
- McArdle JJ, & Hamagami F (2001). Latent difference score structural models for linear dynamic analyses with incomplete longitudinal data. In Sayer LMCAG (Ed.), Decade of behavior. New methods for the analysis of change (pp. 139–175). 10.1037/10409-005 [DOI] [Google Scholar]
- Moffitt TE (2013). Childhood exposure to violence and lifelong health: Clinical intervention science and stress-biology research join forces. Development and Psychopathology, 25, 1619–1634. 10.1017/S0954579413000801 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moffitt TE, Caspi A, Rutter M, & Silva PA (2001). Sex differences in antisocial behaviour: Conduct disorder, delinquency, and violence in the Dunedin Longitudinal Study. New York, NY: Cambridge University Press. 10.1017/CBO9780511490057 [DOI] [Google Scholar]
- Mrug S, & Windle M (2009). Bidirectional influences of violence exposure and adjustment in early adolescence: Externalizing behaviors and school connectedness. Journal of Abnormal Child Psychology, 37, 611–623. 10.1007/s10802-009-9304-6 [DOI] [PubMed] [Google Scholar]
- Mrug S, & Windle M (2010). Prospective effects of violence exposure across multiple contexts on early adolescents’ internalizing and externalizing problems. Journal of Child Psychology and Psychiatry, 51, 953–961. 10.1111/j.1469-7610.2010.02222.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthen BO (2013). Non-normal distribution. Retrieved from http://www.statmodel.com/discussion/messages/11/1535.html
- Muthen LK, & Muthen BO (1998–2017). Mplus version 8 user’s guide. Los Angeles, CA: Author. [Google Scholar]
- Muthen LK, & Muthen BA (2002). How to use a Monte Carlo study to decide on sample size and determine power. Structural Equation Modeling, 9, 599–620. 10.1207/S15328007SEM0904_8 [DOI] [Google Scholar]
- Newsom JT (2015). Longitudinal structural equation modeling: A comprehensive introduction. New York, NY: Routledge. [Google Scholar]
- Ousey GC, Wilcox P, & Fisher B (2011). Something old, something new: Revisiting competing hypotheses of the victimization-offending relationship among adolescents. Journal of Quantitative Criminology, 27, 53–84. 10.1007/s10940-010-9099-1 [DOI] [Google Scholar]
- Richters JE, & Saltzman W (1990). Survey of exposure to community violence: Self-report version. Rockville, MD: Author. [Google Scholar]
- Schreck CJ, Stewart EA, & Fisher BS (2006). Self-control, victimization, and their influence on risky lifestyles: A longitudinal analysis using panel data. Journal of Quantitative Criminology, 22, 319–340. 10.1007/s10940-006-9014-y [DOI] [Google Scholar]
- Stewart SH (1996). Alcohol abuse in individuals exposed to trauma: A critical review. Psychological Bulletin, 120, 83–112. 10.1037/0033-2909.120.1.83 [DOI] [PubMed] [Google Scholar]
- Sullivan TN, Farrell AD, & Kliewer W (2006). Peer victimization in early adolescence: Association between physical and relational victimization and drug use, aggression, and delinquent behaviors among urban middle school students. Development and Psychopathology, 18, 119–137. 10.1017/S095457940606007X [DOI] [PubMed] [Google Scholar]
- Thompson MP, Kingree JB, & Desai S (2004). Gender differences in long-term health consequences of physical abuse of children: Data from a nationally representative survey. American Journal of Public Health, 94, 599–604. 10.2105/AJPH.94.4599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tillyer MS, & Tillyer R (2016). Race, ethnicity, and adolescent violent victimization. Journal of Youth and Adolescence, 45, 1497–1511. 10.1007/s10964-016-0416-3 [DOI] [PubMed] [Google Scholar]
- Tingen MS, Andrews JO, Heath J, Turnmire AE, Waller JL, & Treiber FA (2013). Comparison of enrollment rates of African-American families into a school-based tobacco prevention trial using two recruitment strategies in urban and rural settings. American Journal of Health Promotion, 27, e91–e100. 10.4278/ajhp.110204-QUAN-53 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wellman MM (1993). Child sexual abuse and gender differences: Attitudes and prevalence. Child Abuse and Neglect, 17, 539–547. 10.1016/0145-2134(93)90028-4 [DOI] [PubMed] [Google Scholar]
- Zhang Q, Loeber R, & Stouthamer-Loeber M (1997). Developmental trends of delinquent attitudes and behaviors: Replications and synthesis across domains, time, and samples. Journal of Quantitative Criminology, 13, 181–215. 10.1007/BF02221307 [DOI] [Google Scholar]