

Innovators and early adopters push the field forward.
Central Message.
Minimally invasive pulmonary valve replacement through a 6-cm left anterior minithoracotomy is a new surgical innovation that may benefit select patients undergoing primary and redo operations.
See Article page 127.
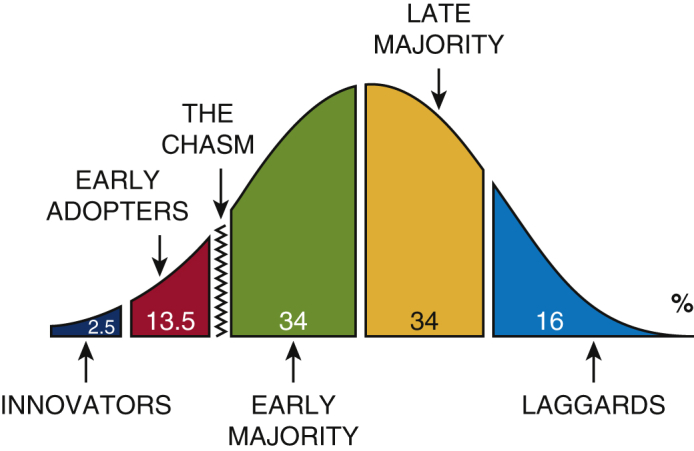
The diffusion of innovation theory is a framework in business that describes how ideas spread.1 New ideas are created and endorsed by innovators, subsequently picked up by early adopters, and may or may not reach a critical point where the early majority, late majority, and laggards join (Figure 1). Factors influencing this process include the relative value of the product, the channels through which the idea is discussed, time, and the social systems within which consumers exist. In surgery, innovation is often limited by our risk-averse nature.
Figure 1.
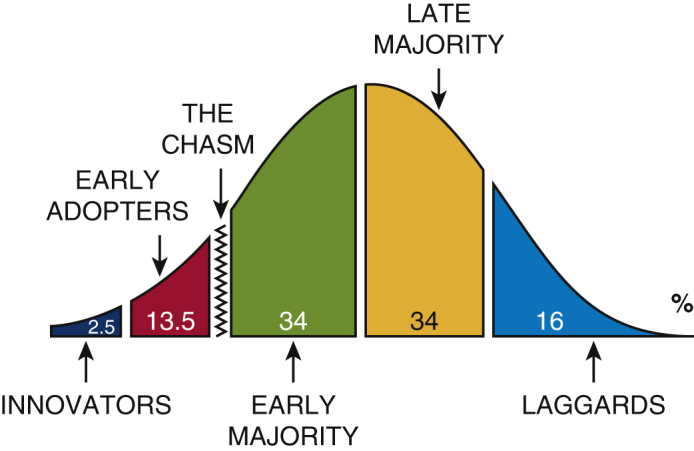
Innovators and early adopters push the field forward.
In this issue of JTCVS Techniques, Said2 demonstrates the technique for minimally invasive pulmonary valve replacement (miPVR) through a 6-cm left anterior minithoracotomy. In his series of 6 patients, no patients were converted to a larger incision. One patient experienced a femoral artery pseudoaneurysm, due to a now modified percutaneous cannulation strategy, and no other complications were recorded. The average postoperative length of stay was 2 days. The team should be congratulated on a successful series and impressive postoperative length of stay. While the approach has been reported before, their experience and operative video is a strong addition to the literature and will undoubtedly help other surgeons with their first miPVR.
Since late 2018, our group has performed 19 operations, including 14 redo PVRs following primary tetralogy of Fallot repair, through a 5-cm left anterior mini-incision.3,4 In our series, the median age for patients undergoing left anterior mini-incision was 16 years old (13-23 years) with a median body mass index of 20 (19-29). Two patients with body mass indexes of >30 and multiple previous median sternotomies were converted to sternotomy due to dense adhesions and inadequate exposure. Otherwise, patients were discharged on postoperative day 4 without sternal precautions. While this report does an excellent job documenting the procedure, surgeons may benefit from 2 key modifications. To decrease the incidence of distal-limb ischemia or arterial injury during cardiopulmonary bypass, we establish femoral access through a 6-mm end-to-side Dacron graft in all cases. Postoperatively, the vessel is repaired with a bovine pericardial patch. In addition, we use interrupted horizontal mattress sutures with pledgets to sew in the posterior aspect of the valve, securing the suture inferiorly in the right ventricular outflow tract with COR-KNOT fasteners (LSI Solutions, Victor, NY). This helps decrease torque on the valve and outflow tract, which is hard to avoid when running the suture circumferentially.
For the miPVR approach to be adopted by others, the benefits of avoiding sternal precautions will have to outweigh the fear of failure or risk of major complications. Perhaps the biggest limitation of this technique is the inability to easily arrest the heart if needed. Although many surgeons routinely perform beating-heart PVR when the atrial septum is intact, other surgeons prefer to arrest the heart or fibrillate in all cases due to the theoretic risk of unrecognized intracardiac shunts, which could lead to air entrainment and neurologic injury. Although this risk is quite low, as with any early surgical innovation with an emerging risk profile, an honest and informed discussion with the patient and family about one's experience with the operation, and presumed risks and benefits, is required before proceeding.
Footnotes
Disclosures: The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
References
- 1.Rogers E. 5th ed. Simon and Schuster; New York: 2003. Diffusion of Innovations. [Google Scholar]
- 2.Said S.M. Minimally invasive pulmonary valve replacement via left anterior minithoracotomy. J Thorac Cardiovasc Surg Tech. 2021;6:127–129. doi: 10.1016/j.xjtc.2020.11.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nellis J.R., Vekstein A.M., Meza J.M., Andersen N.D., Haney J.C., Turek J.W. Left anterior mini-incision for pulmonary valve replacement following tetralogy of Fallot repair. Innovations. 2020;15:106–110. doi: 10.1177/1556984520911025. [DOI] [PubMed] [Google Scholar]
- 4.Vekstein A.M., Nellis J.R., Meza J.M., Andersen N.D., Haney J.C., Turek J.W. Left anterior mini-incision for pulmonary valve replacement in a 12-year-old. Innovations. 2020;15:111–113. doi: 10.1177/1556984520911026. [DOI] [PubMed] [Google Scholar]