

Abstract
Benign metastasizing leiomyoma is a rare condition usually affecting women of reproductive age with a history of uterine leiomyoma and characterized by soft tissue masses in various extrauterine sites. We report a case of a 46-year-old woman with previously resected uterine leiomyoma with subsequent pulmonary and tricuspid valve lesions. (Level of Difficulty: Intermediate.)
Key Words: benign metastasizing leiomyoma, hysterectomy, metastasis, tricuspid valve
Abbreviations and Acronyms: BML, benign metastasizing leiomyoma; CT, computed tomography
Graphical abstract

Benign metastasizing leiomyoma is a rare condition usually affecting women of reproductive age with a history of uterine leiomyoma…
Benign metastasizing leiomyoma (BML) is a rare entity predominantly affecting middle-aged women with a prior diagnosis of uterine fibroids and a history of myomectomy or hysterectomy (1). The most common site of metastasis for BML is the lung; however, BML also can metastasize to abdominal lymph nodes, liver, skeletal muscles, and thoracic structures (2). Although exceptionally rare, BML metastases to the heart also have been reported (3,4).
Learning Objectives
-
•
The tricuspid valve is an extremely rare site of metastasis; differential diagnosis of valvular lesions should be broad and inclusive.
-
•
To understand the combined role of clinical assessment and multimodality imaging in the evaluation of cardiac masses.
History of Presentation
A 46-year-old woman presented to the outpatient clinic with fever, chills, and a productive cough. She was at her usual state of health 3 weeks before the presentation. She had no other complaints. The physical examination demonstrated a new heart murmur but was negative for chest pain, exertional dyspnea, and extremity edema. She was prescribed moxifloxacin for likely community-acquired pneumonia, and chest radiograph and echocardiography were ordered.
Past Medical History
She had a history of supracervical hysterectomy at the age of 44 (premenopausal at that time) due to excessive vaginal bleeding from uterine fibroids. She had no other significant prior history. She denied smoking, alcohol intake, or substance abuse.
Differential Diagnosis
Given the murmur and symptoms, the differential diagnosis included structural valvular pathologies, such as stenosis/insufficiency and infective endocarditis.
Investigations
Initial chest radiograph (not shown) revealed ground-glass infiltrates, with possible bilateral lung nodules, consistent with suspected pneumonia. Mild cardiomegaly was also present. The transthoracic echocardiography showed a mobile basal right ventricular valve lesion with a severely dilated right atrium and left atrium (Figure 1A, Video 1), which was felt to be attached to tricuspid valve on subsequent transesophageal echocardiography (Figure 1B, Video 2), concerning for cardiac mass/vegetation. She also underwent a contrast-enhanced chest computed tomography (CT) scan (Figure 2A) that showed bilateral basilar lung nodules, which were suspicious for metastatic disease. To screen for the highly likely primary malignancy, an abdominopelvic CT scan with intravenous contrast (Figure 2B) was done and demonstrated a large soft tissue density mass filling the pelvis with adjacent cystic lesions in the central pelvis that may represent cystic neoplasm versus loculated ascites. There was a mass effect on bilateral ureters resulting in bilateral hydronephrosis; however, renal function was preserved at the time of presentation with serum creatinine levels of 0.75 mg/dl. For definitive characterization of right heart mass, cardiac magnetic resonance imaging (Figure 3) was done, which showed a nonenhancing elongated mobile pedunculated multilobulated lesion within the right ventricle that was possibly attached to the proximal interventricular septum or the septal leaflet of the tricuspid valve, likely favoring a thrombus or vegetation attached to tricuspid valve leaflet; a metastatic lesion was felt to be less likely. The lesion was seen encroaching onto the right ventricular outflow tract during systole.
Figure 1.

Right Heart Mass on Echocardiography
(A) Four-chamber transthoracic echo image demonstrating a pedunculated multilobulated mobile lesion in the basal right ventricle (yellow arrow). (B) Subsequent transesophageal echocardiography shows the lesion to be attached to the tricuspid valve leaflet (yellow arrow).
Online Video 1.
Transthoracic echocardiography showing mobile basal right ventricular lesion.
Online Video 2.
Transesophageal echocardiography demonstrating mobile lesion associated with tricuspid valve.
Figure 2.

Pelvic Mass and Pulmonary Metastases on CT Imaging
(A) Axial computed tomography (CT) chest in lung window settings demonstrates multiple rounded lower lobe predominant pulmonary nodules (yellow arrows), concerning for metastatic disease. (B) Abdominopelvic CT scan shows a large complex pelvic mass (yellow arrows) compressing on bilateral ureters with biopsy consistent with leiomyoma.
Figure 3.
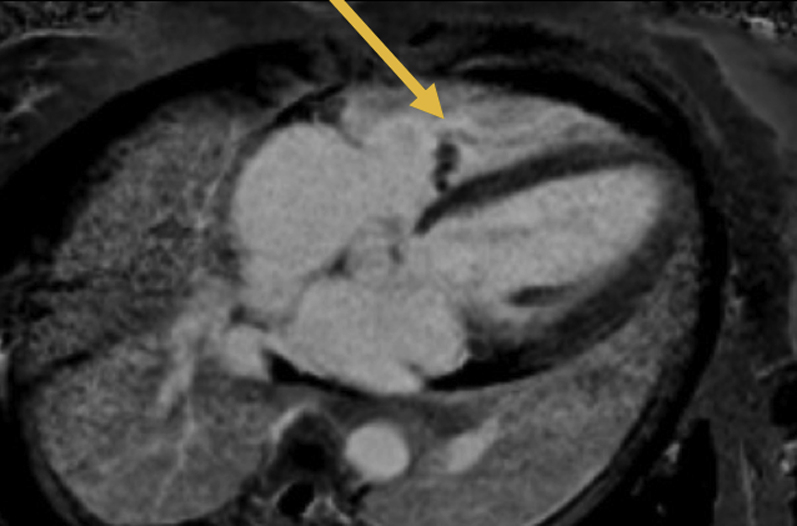
Right Heart Mass on Cardiac Magnetic Resonance Imaging
A 4-chamber delayed contrast-enhanced magnetic resonance image reveals the lobulated hypodense lesion with basal right ventricle (yellow arrow) without discernible contrast enhancement, a thrombus/vegetation was favored over a hypoperfused neoplasm.
Management
After the echocardiography results, she was admitted to the hospital. Blood cultures were drawn, and broad-spectrum antibiotics, vancomycin, and ceftriaxone were started and then discontinued following 48 h of negative blood cultures. Bilateral percutaneous nephrostomy tubes were placed with improvement in hydronephrosis. She also underwent a CT-guided biopsy of the pelvic mass, with pathology consistent with benign leiomyoma. Because of the vascular nature of the pelvic mass, she underwent coil embolization of feeding right internal iliac artery, before potential surgical resection.
She underwent cardiac surgery to resect the mass. Intraoperatively, a multilobulated mass, heavily incorporated between the chordae of the tricuspid valve, was identified that was not attached to the septum. The involved chordae were mainly related to the commissure of the anterior and septal leaflets and also on the septal leaflet next to the posterior leaflet, which were resected along with the mass and sent to tissue diagnosis (Figure 4A). Tricuspid valve repair was performed by leaflet plication and ring annuloplasty. Pathology of the cardiac mass revealed findings consistent with a benign or low-grade smooth muscle neoplasm (Figure 4B). Immunohistochemical stains showed that tumor cells stain positive for smooth muscle actin, desmin, estrogen receptor, and progesterone receptor, confirming BML.
Figure 4.

Gross Specimen and Pathological Appearance of Right Heart Mass
(A) Gross specimen of the tricuspid valve mass: a smooth, tan-white, firm, and lobulated mass measuring 4.8 × 2.5 × 1.3 cm with an attached portion of chordae tendinae. (B) Pathological examination (hematoxylin and eosin staining with ×20 magnification) revealed spindle-shaped cells mostly arranged in a parallel fashion and containing pink (eosinophilic) cytoplasm with oval or diamond-shaped nuclei and no atypia or mitoses, consistent with low-grade smooth muscle neoplasm/benign metastasizing leiomyoma.
She experienced right heart failure postoperatively, manifesting as weight gain and lower extremity edema and was treated with loop diuretics successfully. She was also started on leuprolide, gonadotropin-releasing hormone analog, for the treatment of her BML.
Discussion
To our knowledge, this is the third case of BML affecting the tricuspid valve (5), and the ninth case of heart involvement reported in the literature (3,4,6). Thukkani et al. (7) previously described coexisting tricuspid valve and retroperitoneal metastatic involvement by BML. The lesions were discovered 10 years after hysterectomy in a 36-year-old woman with a known history of intravenous leiomyomatosis and multiple BML metastases to the lung. Involvement by BML metastases was also noted by Nayar et al. (5), who described the case of a woman of age 35, status postsurgery for leiomyomatosis with a vascular extension, who was found with multiple metastatic nodules in the lungs and numerous cardiac masses in the right atrium, right ventricle, tricuspid valve, and right pulmonary artery.
Because cardiac involvement in BML is usually asymptomatic or may only present with a heart murmur, metastases in the heart can be discovered incidentally (8). Meddeb et al. (8) reported incidentally detected BML involving the right ventricle and lungs on CT scan following a car accident in a 36-year-old woman who had undergone hysterectomy for leiomyoma 12 years prior. The heart mass was surgically removed, and its uterine origin was highlighted by immunohistochemical reactions for estrogen receptor, progesterone receptor, smooth muscle α-actin, and desmin. Cai et al. (6) also reported coexisting BML metastases in a 37-year-old woman with prior hysterectomy history, involving the heart (specifically in the right ventricle), both lungs, right arm, abdominal wall, muscles, liver, and pelvis (6). The histological and immunohistochemical study of the right arm nodule revealed aspects compatible with a benign tumor of uterine lineage.
Follow-Up
She is currently on pharmacotherapy for the right heart failure. Although there was slight shrinkage of the mass at follow-up, the gynecology-oncology tumor board decided against surgical resection of the pelvic mass because of adjacent vascular encasement and her comorbid conditions, mainly the right heart failure.
Conclusions
BML is a rare disorder that affects women of fertile age with metastases generally reported long after the initial treatment of uterine fibroids. Heart/tricuspid valve metastatic involvement is extremely rare, and treatment of choice consisted of surgical removal of the encountered mass, with a favorable evolution and no recurrence if total resection is performed.
Footnotes
All authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Informed consent was obtained for this case.
Appendix
For supplemental videos, please see the online version of this paper.
References
- 1.Steiner P.E. Metastasizing fibroleiomyoma of the uterus: Report of a case and review of the literature. Am J Pathol. 1939;15:89–110.7. [PMC free article] [PubMed] [Google Scholar]
- 2.Chen S., Liu R.M., Li T. Pulmonary benign metastasizing leiomyoma: a case report and literature review. J Thorac Dis. 2014;6:E92–E98. doi: 10.3978/j.issn.2072-1439.2014.04.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Consamus E.N., Reardon M.J., Ayala A.G., Schwartz M.R., Ro J.Y. Metastasizing leiomyoma to heart. Methodist DeBakey Cardiovasc J. 2014;10:251–254. doi: 10.14797/mdcj-10-4-251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Galvin S.D., Wademan B., Chu J., Bunton R.W. Benign metastasizing leiomyoma: a rare metastatic lesion in the right ventricle. Ann Thorac Surg. 2010;89:279–281. doi: 10.1016/j.athoracsur.2009.06.050. [DOI] [PubMed] [Google Scholar]
- 5.Nayar A.C., McAleer E.P., Tunick P.A., Applebaum R.M., Colvin S.B., Kronzon I. Benign metastasizing leiomyomatosis diagnosed by echocardiography. Echocardiography. 2002;19:571–572. doi: 10.1046/j.1540-8175.2002.00571.x. [DOI] [PubMed] [Google Scholar]
- 6.Cai A., Li L., Tan H., Mo Y., Zhou Y. Benign metastasizing leiomyoma. Case report and review of the literature. Herz. 2014;39:867–870. doi: 10.1007/s00059-013-3904-1. [DOI] [PubMed] [Google Scholar]
- 7.Thukkani N., Ravichandran P.S., Das A., Slater M.S. Leiomyomatosis metastatic to the tricuspid valve complicated by pelvic hemorrhage. Ann Thorac Surg. 2005;79:707–709. doi: 10.1016/j.athoracsur.2003.08.038. [DOI] [PubMed] [Google Scholar]
- 8.Meddeb M., Chow R.D., Whipps R., Haque R. The heart as a site of metastasis of benign metastasizing leiomyoma: case report and review of the literature. Case Rep Cardiol. 2018;2018 doi: 10.1155/2018/7231326. [DOI] [PMC free article] [PubMed] [Google Scholar]