

Abstract
Objective: The aim of the present study was to develop a nomogram to accurately predict the need for intervention in patients suffering from LUTS due to benign prostatic hyperplasia (BPH) and internally validate it. Material and methods: The data was collected from the community subjects from the state of Gujarat in western India. All the demographic data, physical examination, PSA, uroflowmetry and prostatic ultrasound was collected in 92 subjects and were followed up after 2 years. The data was analyzed and logistic regression model was used to build a predictive model. A nomogram was build using R software. Nomogram was internally validated using 50 subjects. Results: 92 subjects were analyzed for developing the nomogram. Out of these, 17 patients needed intervention. 8 patients were started on medical therapy and 9 patients were taken up for surgical intervention. Of all the statistically significant predictors, peak flow rate was the most significant and was followed by median lobe enlargement, PSA, prostate volume and IPSS. These variables were used to develop a prediction model for the intervention required using reduced logistic regression model. The predictive accuracy of the model was 95.65% with a sensitivity of 88.28%, a specificity of 97.33%, a positive predictive value (PPV) of 88.24%, and a negative predictive value (NPV) of 97.33%. The AUC of the model was 0.799. Internal validation was done on 50 subjects which had sensitivity, specificity and AUC of the model at 89.66%, 90.48% and 0.968 respectively. Conclusion: The study demonstrates the clinical application of nomogram which uses IPSS, PSA, peak flow rate, prostate volume and median lobe enlargement (intravesical prostatic volume). It has a sensitivity of 88.24%, specificity of 97.33%. It predicts the need for intervention in BPH patients with accuracy of 95.65% which was internally validated with an accuracy of 90%.
Keywords: BPH (Benign Prostatic Hyperplasia), nomogram, peak flow rate, intravesical prostatic protrusion, intervention, lower urinary tract symptoms (LUTS)
Introduction
The geriatric population in the world is increasing as the life expectancy is increasing globally. As benign prostatic hyperplasia is an age-related process, patients having lower urinary tract symptoms (LUTS) due to bladder outlet obstruction have also increased [1,2]. However, there are no clear guidelines as to when the medical management should be started and the decision to start medical management is very subjective. Although the medical management has benefitted many patients, the decision of surgical management is also subjective, depending on symptoms of patients. The EUA and AUA guidelines suggest that surgical treatment is necessary when patients have urinary retention, renal insufficiency, recurrent urinary tract infections, bladder stone, or gross hematuria due to an enlarged prostate [3-5]. However, there are many patients who have clinically bothersome symptoms which usually do not fit in the above indications. The decision to intervene surgically in a case of BPH is many times confounded by multiple clinical variables. A relative surgical indication may sometime be subjective depending on patient’s understanding and his preference for surgery [5]. Thus, an objective assessment of symptoms warrants the development of a clinical algorithm which can guide the need for therapeutic intervention in the form of medical management or surgical treatment.
Many tools are available to gauge the severity of symptoms and degree of prostatic enlargement like IPSS score, uroflowmetry, pressure flow studies and PSA levels. Each of these variables have their own pitfalls and advantages. IPSS is a symptom score but it is a subjective assessment and many times patients are unable to comprehend the questionnaire. Uroflowmetry is an objective assessment of flow but the single reading may be fallacious and may not be representative of daily flow pattern of the patient. A pressure flow study is an invasive method and may not be feasible in many patients. Serum PSA levels are usually used to rule out infectious or malignant conditions. But, none of these tools have been used collectively to reach a decision point to intervene in such patients [6,7].
The aim of the present study was to develop a nomogram to accurately predict the need for intervention, either medical or surgical, in patients suffering from LUTS due to benign prostatic hyperplasia (BPH) and internally validate it.
Material and method
Patients and evaluation
After approval from Institutional Ethics Committee (Approval number: EC/722/2021), the data for our study was collected from community subjects in Western India in the year 2001 to 2003. The study cohort was population of districts of Anand and Kheda in the state of Gujarat, India. The population of male persons in these districts of age more than 40 years was 455616 spread over 672 villages. According to sampling of 2-2.5% for villages and 5% sampling number for people per village, there was a study cohort of 2040 subjects. Prescreening co-ordination was done with handbills, TV advertisement, newspaper and local contacts. Initially, 2600 subjects were evaluated at baseline and 2004 subjects completed the formalities. Out of 2004 subjects, 1899 were available for analysis. Out of these, 217 patients were suspected for Ca prostate and were excluded. In the rest of the patients, sonography data could be collected in 300 subjects (Figure 1). All the demographic data of the subjects were collated, these included age, weight, height and body mass index. All the subjects underwent physical examination in the form of abdominal examination and digital rectal examination. The subjects were given IPSS questionnaires and asked to fill about their symptoms and quality of life. Transrectal ultrasound was performed with a 7.5 MHz probe and prostate volume (PV) and intravesical prostatic protrusion were evaluated. The prostatic volume was calculated using the ellipsoid formula (p/6 width × height × depth of prostate/prostate). A single operator performed all the ultrasound measurements. Serum PSA levels (Immunoradiometric assay technique) (Diagnostic system Lab, Texas, US, Standard reference range was 0.0 to 4.0 ng/ml) were measured and uroflowmetry was done in all patients. PSA determination was done prior to any prostatic manipulations including DRE and TRUS. Subjects who had neurological disorders, renal insufficiency, bladder stones, prostate cancer, urethral stricture and previous pelvic surgery were excluded from the study. We also excluded subjects already receiving medical therapy for BPH.
Figure 1.

Selecting the study cohort.
The subjects were contacted and asked to attend a follow up visit at two years after the baseline visit. The parameters noted were weight, physical examination including digital rectal examination, IPSS, PSA, uroflowmetry, transrectal ultrasound. A total of 92 subjects could be followed up successfully. Based on the indications, subjects were offered treatment in the form of medical therapy or surgical therapy in the form of (Transurethral resection of Prostate) TURP.
Internal validation was done by 1000 bootstrapping re-samples and on 50 subjects who were different from the original data set but belonged to the same community population. The discriminatory performance of the nomogram was determined with the calculated area under receiver-operating characteristic curve for these subjects.
Statistical analysis
We used SPSS Version 24 (SPSS Inc., Chicago, IL, USA) to analyze the data. Patients were categorized into those requiring intervention and no intervention. The demographic and clinical data characteristics were compared between sub cohorts using the Pearson’s Chi-square test, Fischer’s exact test for categorical variables and Student’s t-test for continuous variables. All statistical tests were two sided with statistical significance set at p-value of less than 0.05 considered as significant. Variables were subjected to the univariate and multivariate analysis. Then, logistic regression analysis was done to determine the parameters for the development of the nomogram for a binary response variable as falling in to intervention group or non-intervention group. We determined the logistic regression model using identified predictors (measured before two years) as age (in years), symptomatic score (IPSS), peak flow rate, quality of life (QoL), total prostate volume, median lobe (intravesical prostatic protrusion) and PSA (ng/ml). The beta-coefficients of the logistic regression model were used to create a nomogram. The ROC and area under the curve (AUC) were calculated for the individual variables in the nomogram. The clinical nomogram was formed to fit the regression model in ‘R’ for windows version 2.15.0 by the rms package (http://www.r-project.org). When the prediction model showed that the calculated probability of requiring intervention was 50% or more, it was considered that intervention was necessary. Using this reduced logistic regression model, and using R software (http://www.r-project.org) [19], a nomogram was created as shown in the Figure 2. The final model was internally validated from 1000 bootstrap resamples to minimize the overfit bias. Validation was also independently done for 50 test subjects with regards to accuracy, sensitivity and specificity and ROC curve for the discriminatory performance.
Figure 2.

Nomogram.
Results
Patient characteristics
Data of 92 subjects was available for the final analysis. Out of these subjects, 17 patients needed intervention. 8 patients were started on medical therapy and 9 patients were taken up for surgical intervention. Descriptive characteristics of all the subjects (n=92) are shown in Table 2. The mean age of the patients was 62±9.2 years. The mean IPSS score was 13±8.5. The mean peak flow rate was 18±8 ml/seconds. The mean PSA was 1±1.38 ng/ml. The mean prostate volume and mean intravesical prostatic protrusion was 22±8.97 cc and 3±2.17 mm respectively. In the intervention group, the mean IPSS score was 18.7±8.7. The mean peak flow rate and PSA in intervention group was 12±5.01 ml/sec and 3.05±2.13 ng/ml respectively. The prostate volume and median lobe (IVPP) in intervention group was 26.34±9.76 cc and 4.7±1.72 mm respectively.
Table 2.
Descriptive statistics of patients (n=92)
| Variable | Mean | Std. Deviation |
|---|---|---|
| Age before 2 years (years) | 59.5761 | 9.27863 |
| Age after 2 years (years) | 61.5543 | 9.27168 |
| IPSS before 2 years | 13.2609 | 8.81665 |
| IPSS after 2 years | 12.8696 | 8.59238 |
| Qmax before 2 years (ml/sec) | 19.5000 | 7.68830 |
| Qmax after 2 years (ml/sec) | 18.0000 | 8.62147 |
| PSA before 2 years (ng/ml) | 1.4511 | 1.38163 |
| Quality of life before 2 years | 3.2609 | 2.09589 |
| Quality of life after 2 years | 2.6413 | 1.77021 |
| Prostate Volume before 2 years (cc) | 19.7888 | 9.16497 |
| Prostate Volume after 2 years (cc) | 22.0116 | 8.97513 |
| Median Lobe before 2 years (mm) | 3.9239 | 1.40042 |
| Median Lobe after 2 years (mm) | 2.7391 | 2.17311 |
| Weight (kg) | 63.3859 | 14.60752 |
| Height (cm) | 160.3587 | 18.72507 |
| BMI (kg/m2) | 24.1630 | 5.62804 |
Logistic regression models for prediction of intervention
The parameters included in the logistic regression model were age, S. PSA, peak flow rate (Qmax), prostate volume before 2 years, median lobe enlargement (intravesical prostatic protrusion), IPSS score, height, weight, BMI and quality of life. Among these, IPSS, peak flow rate, prostatic volume, median lobe and PSA were statistically significant predictors of benign prostatic hyperplasia in multivariate analysis. Weight, BMI and quality of life were not statistically significant parameters (Table 4).
Table 4.
Univariate and multivariate analysis of variables
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
|
|
|
|||
| B | Sig. | B | Sig. | |
| Age | -0.104 | 0.079 | -1.00 | 0.081 |
| Symptomatic Score (7*5=35) Before 2 years | 0.088 | 0.007 | 0.087 | 0.192 |
| Qmax before 2 years | -0.280 | 0.000 | -0.366 | 0.008 |
| PSA | 0.861 | 0.000 | 0.749 | 0.078 |
| Prostate Volume before 2 years | 0.084 | 0.004 | 0.087 | 0.109 |
| Median Lobe Before | 0.458 | 0.015 | 0.587 | 0.118 |
| Quality of life before 2 years | 0.267 | 0.051 | 0.239 | 0.414 |
| Weight | -0.056 | 0.029 | -0.528 | 0.355 |
| Height | 0.022 | 0.527 | 0.516 | 0.277 |
| BMI | -0.188 | 0.013 | 1.266 | 0.391 |
Table 3 shows multiple logistic regression models based on all patient predictors. Of all the statistically significant predictors, peak flow rate was the most significant and it was followed by median lobe enlargement, PSA, prostate volume and IPSS. These variables were used to develop a prediction model for the intervention required using reduced logistic regression model. The predictive accuracy of the model was 95.65% with a sensitivity of 88.28%, a specificity of 97.33%, a positive predictive value (PPV) of 88.24%, and a negative predictive value (NPV) of 97.33% (Table 5). The AUC of the model was 0.799 (Figure 3, Supplementary Table 1).
Table 3.
Comparative statistics of subjects with respect to intervention
| Variable | Intervention | N | Mean | Std. Deviation | p-value* | 95% CI for the Diff | |
|---|---|---|---|---|---|---|---|
|
| |||||||
| Lower | Upper | ||||||
| Age (Before 2 years) | No | 75 | 58.3067 | 8.75488 | 0.005* | -11.63652 | -2.10309 |
| Yes | 17 | 65.1765 | 9.70976 | ||||
| Age (After 2 years) | No | 75 | 60.2933 | 8.76691 | 0.006 | -11.59000 | -2.05863 |
| Yes | 17 | 67.1176 | 9.64937 | ||||
| IPSS (Before 2 years) | No | 75 | 12.0267 | 8.41005 | 0.009* | -11.19890 | -2.15953 |
| Yes | 17 | 18.7059 | 8.73760 | ||||
| IPSS (After 2 years) | No | 75 | 11.6667 | 8.12293 | 0.004 | -10.91449 | -2.10512 |
| Yes | 17 | 18.1765 | 8.83343 | ||||
| Qmax (Before 2 years) | No | 75 | 21.2000 | 7.16976 | 0.000* | 5.55180 | 12.84820 |
| Yes | 17 | 12.0000 | 5.01248 | ||||
| Qmax (After 2 years) | No | 75 | 20.7733 | 6.88432 | 0.000 | 12.08247 | 18.49622 |
| Yes | 17 | 5.7647 | 2.90537 | ||||
| PSA (before 2 years) | No | 75 | 1.1467 | .87816 | 0.008* | -2.30370 | -.99120 |
| Yes | 17 | 2.7941 | 2.22246 | ||||
| QoL (Before 2 years) | No | 75 | 3.0533 | 2.13651 | 0.045 | -2.22296 | -.02332 |
| Yes | 17 | 4.1765 | 1.66716 | ||||
| QoL (After 2 years) | No | 75 | 2.4800 | 1.74263 | 0.066 | -1.80511 | .05923 |
| Yes | 17 | 3.3529 | 1.76569 | ||||
| Prostate Volume (Before 2 years) | No | 75 | 18.3244 | 8.42130 | 0.001* | -12.55462 | -3.29541 |
| Yes | 17 | 26.2494 | 9.76387 | ||||
| Prostate Volume (After 2 years) | No | 75 | 20.9467 | 7.94946 | 0.016 | -10.42587 | -1.10080 |
| Yes | 17 | 26.7100 | 11.70908 | ||||
| Median Lobe (Before 2 years) | No | 75 | 3.7467 | 1.26377 | 0.010* | -1.68336 | -.23507 |
| Yes | 17 | 4.7059 | 1.72354 | ||||
| Median Lobe (After 2 years) | No | 75 | 2.0133 | 1.36058 | 0.000 | -4.75445 | -3.10124 |
| Yes | 17 | 5.9412 | 2.22122 | ||||
| Weight | No | 75 | 64.6600 | 15.09680 | 0.079 | -5.71557 | 2.97471 |
| Yes | 17 | 57.7647 | 10.87732 | ||||
| Height | No | 75 | 159.7067 | 20.44027 | 0.468 | .94286 | 14.59530 |
| Yes | 17 | 163.2353 | 7.14606 | ||||
| BMI | No | 75 | 24.7307 | 5.81787 | 0.041 | .79058 | 6.02151 |
| Yes | 17 | 21.6588 | 3.92843 | ||||
Table 5.
Sensitivity, specificity and accuracy of nomogram
| Sensitivity | Specificity | Pred+ | Pred- | Accuracy | Error | OR |
|---|---|---|---|---|---|---|
| 88.24 | 97.33 | 88.24 | 97.33 | 95.65 | 4.35 | 273.75 |
| True Positive Rate | True Negative Rate | Positive predictive value | Negative predictive value | Diagnostic Effectiveness | Misclassification Rate | Diagnostic Odds Ratio |
Figure 3.
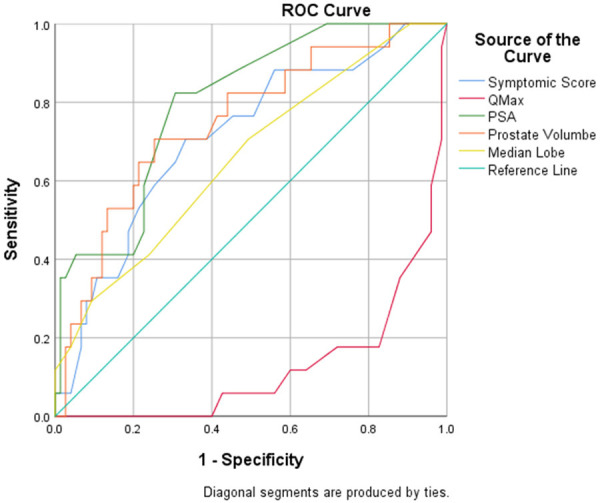
ROC curves.
After the development of nomogram, a total of 50 subjects were enrolled in an internal validation group analysis. The descriptive data of the internal validation group is given in Table 6. The bootstrap-corrected performance of the nomogram was similar to the original nomogram. In the internal validation group of 50 subjects, the prediction model was found to have an AUC of 0.958 (95% CI, 0.906-1) with accuracy of 90.0%. The sensitivity, specificity, positive predictive value, and negative predictive value were 89.66%, 90.48%, 92.86%, and 86.36% respectively (Figure 4 and Supplementary Table 2). When the data of the patients was charted on the nomogram created by ‘R’ software, the patients who underwent surgical treatment had probability more than 0.7 in all the nine cases. While in patients of medical management, the probability was more than 0.5 in the eight cases. So, we can assume that when the patient data is entered in the nomogram, if the probability of intervention is more than 0.7, then the patient will require surgical treatment, and if it is between 0.5 to 0.7, then the patient will require medical management. If it is less than 0.5, then the patient can be observed.
Table 6.
Patients of internal validation (n=50)
| Variable | Mean Value | Std Deviation |
|---|---|---|
| Age (years) | 63.57 | 9.5 |
| IPSS | 17.0 | 7.09 |
| Peak flow rate (ml/sec) | 13.09 | 5.3 |
| PSA (ng/ml) | 2.0 | 1.6 |
| Prostatic Volume (cc) | 36.0 | 19.02 |
| Intravesical Prostatic Protrusion (IVPP) (mm) | 3.0 | 2.89 |
Figure 4.
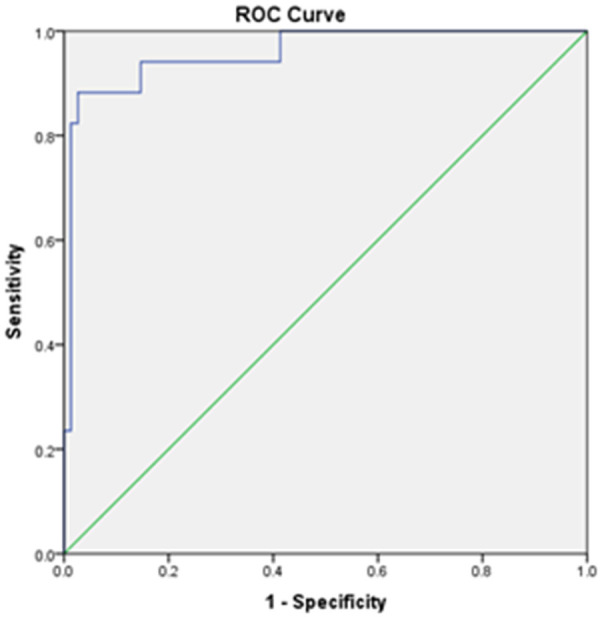
ROC curve for the internal validation group.
Discussion
Patients having BPH can present with varied symptoms, most common being bothersome lower urinary tract symptoms. These patients have a varied differential diagnosis and LUTS can be multifactorial. When the LUTS is ascribed to bladder outlet obstruction due to BPH, it is based on multiple factors. The symptoms of LUTS are very subjective and to show that the LUTS is bothersome, the subjective symptoms have been converted into objective terms by IPSS score and Quality of Life score (QoL). But, many other factors like peak flow rate, prostatic volume, median lobe enlargement in the form of intravesical prostatic protrusion, PSA and post void residual urine are also very important to predict whether a patient can be observed or he will need intervention in the form of medical therapy or surgical therapy. Ideally, pressure flow studies are considered one of the best diagnostic modality to confirm bladder outlet obstruction and need for intervention. But it is invasive procedure and often, it is not feasible in all the patients. Also, it can be fallacious in some patients due to previous medications or episode of acute retention. Our aim was to develop an algorithm/nomogram which would give us the same sensitivity and specificity as that of pressure flow studies in predicting the need for intervention in patients with BPH.
Several authors have tried to develop clinical decision guidance nomograms for the prediction of significant bladder outlet obstruction due to BPH [6,8-12]. A nomogram uses algorithms or mathematical formula to precisely predict the probability of an outcome [13]. The characteristic of nomogram is that the continuous variables remain continuous, so the predictive power is maximized and it allows for the combined use of all important data parameters. To develop a nomogram for bladder outlet obstruction due to BPH, the risk factors affecting the development of BPH have to be known. These risk factors have been suggested through many analyses of population-based and clinical trials [14-17]. These risk factors are higher age, severe obstructive symptoms, lower peak flow rate, high prostate volume, intravesical prostatic protrusion and higher serum PSA levels [18,20]. Each of these is a risk factor for BPH progression, but for the individual patients, the increasing number and severity of these risk factors increases the absolute risk of BPH progression. We aimed to identify the patients at highest risk for intervention, while improving decision-making at the individual patient level.
Choo and colleagues [5] developed four formulas, with the formula which could be used even when one or two parameters were not available. They found that age, total prostate volume, peak flow rate, post void residual urine, IPSS voiding subscore, IPSS storage subscore, IPSS quality of life and BOO index were independent predictive parameters associated with requiring prostatic surgery.
According to Denunzio [6], only peak flow rate and transitional zone volume were significantly associated with increased risk of bladder outlet obstruction due to BPH in the multivariate analysis. They developed nomogram with peak flow rate and transitional zone volume with accuracy of 83% for the detection of BOO in patients with LUTS due to BPH. Another nomogram was created with IPSS, peak flow rate and residual urine which with predictive accuracy of 81%.
Slavin depicted on multivariate analysis, that baseline serum PSA, prostate volume, Qmax, and a previous requirement for selective alpha1-blocker treatment were all predictors of BPH progression. The AUA-SI score was not a significant predictor of progression. They created a nomogram to predict the probability of acute urinary retention and/or surgical intervention within 2 years, the nomogram consisted of AUA-SI score, history of prior alpha blockers, prostate volume, PSA, peak flow rate and history of dutasteride therapy [18].
YJ Lee and colleagues created a nomogram including patient age, IPSS, peak flow rate, prostate volume, post void residue and transitional zone index with an accuracy of 80.9%. Using logistic regression model [2]. The clinical significance of peak flow rate for the prediction of bladder outlet obstruction in our study is similar with the observations from previous studies performed in men with LUTS due to BPH [2,5,6,18]. The comparison of criteria included in different nomograms is compared in the Table 1.
Table 1.
Comparison on different variables used for nomograms for BPH
| Nomogram | De Nunzio [6] | K.M Slawin [18] | M.S. Choo [5] | Y.J. Lee [2] | Present study |
|---|---|---|---|---|---|
| Aim of Study | Diagnose Benign Prostatic Obstruction | To predict AUR/Surgical Intervention with/without Dutasteride | Predict BOO/Surgery in LUTS | Predict BOO in men with non-neurogenic LUTS refractory to medication | Predicting intervention in General population |
| Parameters | |||||
| Age | ✓ | ✓ | |||
| IPSS/AUA-SI | AUA-SI | IPSS | IPSS | IPSS | |
| BPH Impact Index | ✓ | ✓ | |||
| Qmax | ✓ | ✓ | ✓ | ✓ | ✓ |
| PSA | ✓ | ✓ | |||
| Prostate Volume | ✓ | ✓ | ✓ | ✓ | |
| Transitional Zone Volume | ✓ | ||||
| Transitional Zone Index | ✓ | ||||
| Median Lobe Projection | ✓ | ||||
| Residual Urine | ✓ |
The principal strength of our study lies in the fact that it was conducted using community-based database of the western region of India to develop scoring system for prediction of medical or surgical intervention. We developed a nomogram using the IPSS score, prostate volume, median lobe of prostate (intravesical prostatic protrusion) and peak flow rate values based on our study findings and information available from current literature. The nomogram showed high accuracy (95.65%) for the detection of clinically significant bladder outlet obstruction due to benign enlargement of prostate which required medical therapy or surgical intervention. The combination of five parameters can be used to make a decision regarding initiating therapy to the patient.
Another imperative fact in our study is that our nomogram has also included measurement of median lobe of prostate in the form of intravesical prostatic protrusion. The intravesical prostatic protrusion is an independent variable which can predict progression for surgical intervention, but it has not been included in any nomogram as of now. According to K.T. Foo, intravesical prostatic protrusion is a better indicator for bladder outlet obstruction than prostate volume [20]. We have for the first time included median lobe protrusion in our nomogram (IVPP- intravesical prostatic protrusion). Its inclusion makes our nomogram more sensitive. Our nomogram showed high accuracy (95.65%) for the need of intervention for LUTS due to BPH. Thus, the combination of these variables could be used to identify patients at high risk of intervention who can thus be spared from the discomfort of a pressure flow study. Conversely, patients at low risk of intervention according to our nomogram can undergo invasive pressure flow study or directly intervention.
The limitation of our study is that a few parameters like post void residual urine and transitional zone volume were not evaluated. The maximum prostate volume in our study was 80 cc and maximum PSA value was 9.4 ng/ml. So, our nomogram can be applied to prostate volumes below 80 cc only.
Conclusion
The study demonstrates the clinical application of a nomogram which uses IPSS, PSA, peak flow rate, prostate volume and median lobe enlargement (intravesical prostatic volume) and it has a sensitivity of 88.24%, specificity of 97.33% and positive predictive value of 88.24% It predicts the need for intervention in BPH patients with accuracy of 95.65% which was internally validated with an accuracy of 90%.
Disclosure of conflict of interest
None.
Abbreviations
- LUTS
Lower Urinary Tract Symptoms
- EUA
European Urological Association
- AUA
American Urological Association
- BPH
Benign Prostatic Hyperplasia
- IPSS
International Prostatic Symptoms Score
- PSA
Prostatic Specific Antigen
- DRE
Digital Rectal Examination
- TRUS
Trans Rectal Ultrasonography
- TURP
Transurethral Resection of Prostate
- AUA-SI
American Urological Association Symptom Index
Supporting Information
References
- 1.Choo MS, Han JH, Shin TY, Ko K, Lee WK, Cho ST, Lee SK, Lee SH. Alcohol, smoking, physical activity, protein, and lower urinary tract symptoms: prospective longitudinal cohort. Int Neurourol J. 2015;19:197–206. doi: 10.5213/inj.2015.19.3.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lee YJ, Lee JK, Kim JJ, Lee HM, Oh JJ, Lee S, Lee SW, Kim JH, Jeong SJ. Development and validation of a clinical nomogram predicting bladder outlet obstruction via routine clinical parameters in men with refractory nonneurogenic lower urinary tract symptoms. Asian J Androl. 2019;21:486–492. doi: 10.4103/aja.aja_127_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.EAU guidelines on management of non-neurogenic male lower urinary tract symptoms (LUTS), including Benign prostatic obstruction (BPO). Edn. presented at the EAU Annual congress Barcelona. Arnhem: EAU Guidelines Office; 2019. Mar, [Google Scholar]
- 4.Foster HE, Dahm P, Kohler TS, Lerner LB, Parsons JK, Wilt TJ, McVary KT. Surgical management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA Guideline Amendment 2019. J Urol. 2019;202:592–8. doi: 10.1097/JU.0000000000000319. [DOI] [PubMed] [Google Scholar]
- 5.Choo MS, Yoo C, Cho SY, Jeong SJ, Jeong CW, Ku JH, Oh SJ. Development of decision support formulas for the prediction of bladder outlet obstruction and prostatic surgery in patients with lower urinary tract symptom/benign prostatic hyperplasia: part I, development of the formula and its internal validation. Int Neurourol J. 2017;21:S55–65. doi: 10.5213/inj.1734852.426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.De Nunzio C, Autorino R, Bachmann A, Briganti A, Carter S, Chun F, Novara G, Sosnowski R, Thiruchelvam N, Tubaro A, Ahyai S EAU Young Academic Urologists BPH Group Arnhem, The Netherlands. The diagnosis of benign prostatic obstruction: development of a clinical nomogram. Neurourol Urodyn. 2016;35:235–240. doi: 10.1002/nau.22705. [DOI] [PubMed] [Google Scholar]
- 7.Abrams P, Chapple C, Khoury S, Roehrborn C, de la Rosette J International Consultation on New Developments in Prostate Cancer and Prostate Diseases. Evaluation and treatment of lower urinary tract symptoms in older men. J Urol. 2013;189:S93–S101. doi: 10.1016/j.juro.2012.11.021. [DOI] [PubMed] [Google Scholar]
- 8.Griffiths CJ, Harding C, Blake C, McIntosh S, Drinnan MJ, Robson WA, Abrams P, Ramsden PD, Pickard RS. A nomogram to classify men with lower urinary tract symptoms using urine flow and noninvasive measurement of bladder pressure. J Urol. 2005;174:1323–1326. doi: 10.1097/01.ju.0000173637.07357.9e. discussion 1326; author reply 1326. [DOI] [PubMed] [Google Scholar]
- 9.Oelke M, Hofner K, Jonas U, de la Rosette JJ, Ubbink DT, Wijkstra H. Diagnostic accuracy of noninvasive tests to evaluate bladder outlet obstruction in men: detrusor wall thickness, uroflowmetry, postvoid residual urine, and prostate volume. Eur Urol. 2007;52:827–834. doi: 10.1016/j.eururo.2006.12.023. [DOI] [PubMed] [Google Scholar]
- 10.Franco G, De Nunzio C, Leonardo C, Tubaro A, Ciccariello M, De Dominicis C, Miano L, Laurenti C. Ultrasound assessment of intravesical prostatic protrusion and detrusor wall thickness--new standards for noninvasive bladder outlet obstruction diagnosis? J Urol. 2010;183:2270–2274. doi: 10.1016/j.juro.2010.02.019. [DOI] [PubMed] [Google Scholar]
- 11.Yurt M, Suer E, Gulpinar O, Telli O, Arikan N. Diagnosis of bladder outlet obstruction in men with lower urinary tract symptoms: comparison of near infrared spectroscopy algorithm and pressure flow study in a prospective study. Urology. 2012;80:182–186. doi: 10.1016/j.urology.2012.03.022. [DOI] [PubMed] [Google Scholar]
- 12.Steele GS, Sullivan MP, Sleep DJ, Yalla SV. Combination of symptom score, flow rate and prostate volume for predicting bladder outflow obstruction in men with lower urinary tract symptoms. J Urol. 2000;164:344–348. [PubMed] [Google Scholar]
- 13.Eastham JA, Kattan MW, Scardino PT. Nomograms as predictive models. Semin Urol Oncol. 2002;20:108–115. doi: 10.1053/suro.2002.32936. [DOI] [PubMed] [Google Scholar]
- 14.Jacobsen SJ, Jacobson DJ, Girman CJ, Roberts RO, Rhodes T, Guess HA, Lieber MM. Natural history of prostatism: risk factors for acute urinary retention. J Urol. 1997;158:481–487. doi: 10.1016/s0022-5347(01)64508-7. [DOI] [PubMed] [Google Scholar]
- 15.Jacobsen SJ, Girman CJ, Guess HA, Rhodes T, Oesterling JEL. Natural history of prostatism: longitudinal changes in voiding symptoms in community dwelling men. J Urol. 1996;155:595–600. doi: 10.1016/s0022-5347(01)66461-9. [DOI] [PubMed] [Google Scholar]
- 16.Roehrborn CG, Boyle P, Bergner D, Gray T, Gittelman M, Shown T, Melman A, Bracken RB, deVere White R, Taylor A. Serum prostate-specific antigen and prostate volume predict long-term changes in symptoms and flow rate: results of a four-year, randomized trial comparing finasteride versus placebo. Urology. 1999;54:662–669. doi: 10.1016/s0090-4295(99)00232-0. [DOI] [PubMed] [Google Scholar]
- 17.Roehrborn CG, McConnell JD, Lieber M, Kaplan S, Geller J, Malek GH, Castellanos R, Coffield S, Saltzman B, Resnick M. Serum prostate-specific antigen concentration is a powerful predictor of acute urinary retention and need for surgery in men with clinical benign prostatic hyperplasia. Urology. 1999;53:473–480. doi: 10.1016/s0090-4295(98)00654-2. [DOI] [PubMed] [Google Scholar]
- 18.Slawin KM, Kattan MW. The use of nomograms for selecting BPH candidates for dutasteride therapy. Rev Urol. 2004;6:S40. [PMC free article] [PubMed] [Google Scholar]
- 19.Zhang Z, Kattan MW. Drawing Nomograms with R: applications to categorical outcome and survival data. Ann Transl Med. 2017;5:211. doi: 10.21037/atm.2017.04.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wang D, Huang H, Law YM, Foo KT. Relationships between prostatic volume and intravesical prostatic protrusion on transabdominal ultrasound and benign prostatic obstruction in patients with lower urinary tract symptoms. Ann Acad Med Singapore. 2015;44:60–65. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.