

Key Points
Question
How does timely methadone access for opioid use disorder compare between the US and Canada during COVID-19?
Findings
In this cross-sectional study of methadone clinics during COVID-19 in 13 US states and the District of Columbia and 3 Canadian provinces with the highest rates of opioid overdose deaths, more than 1 in 10 clinics were not accepting patients, one-third of which reported this was due to COVID-19. Canadian clinics offered appointments faster than US clinics.
Meaning
These findings suggest that methadone access may be worse than previously estimated and exacerbated by COVID-19 and that Canadian clinics may provide timelier access than US opioid treatment programs.
This cross-sectional study examines the proportion of clinics accepting new patients with opioid use disorder and time until first appointment in the US and Canada.
Abstract
Importance
Methadone access may be uniquely vulnerable to disruption during COVID-19, and even short delays in access are associated with decreased medication initiation and increased illicit opioid use and overdose death. Relative to Canada, US methadone provision is more restricted and limited to specialized opioid treatment programs.
Objective
To compare timely access to methadone initiation in the US and Canada during COVID-19.
Design, Setting, and Participants
This cross-sectional study was conducted from May to June 2020. Participating clinics provided methadone for opioid use disorder in 14 US states and territories and 3 Canadian provinces with the highest opioid overdose death rates. Statistical analysis was performed from July 2020 to January 2021.
Exposures
Nation and type of health insurance (US Medicaid and US self-pay vs Canadian provincial).
Main Outcomes and Measures
Proportion of clinics accepting new patients and days to first appointment.
Results
Among 268 of 298 US clinics contacted as a patient with Medicaid (90%), 271 of 301 US clinics contacted as a self-pay patient (90%), and 237 of 288 Canadian clinics contacted as a patient with provincial insurance (82%), new patients were accepted for methadone at 231 clinics (86%) during US Medicaid contacts, 230 clinics (85%) during US self-pay contacts, and at 210 clinics (89%) during Canadian contacts. Among clinics not accepting new patients, at least 44% of 27 clinics reported that the COVID-19 pandemic was the reason. The mean wait for first appointment was greater among US Medicaid contacts (3.5 days [95% CI, 2.9-4.2 days]) and US self-pay contacts (4.1 days [95% CI, 3.4-4.8 days]) than Canadian contacts (1.9 days [95% CI, 1.7-2.1 days]) (P < .001). Open-access model (walk-in hours for new patients without an appointment) utilization was reported by 57 Medicaid (30%), 57 self-pay (30%), and 115 Canadian (59%) contacts offering an appointment.
Conclusions and Relevance
In this cross-sectional study of 2 nations, more than 1 in 10 methadone clinics were not accepting new patients. Canadian clinics offered more timely methadone access than US opioid treatment programs. These results suggest that the methadone access shortage was exacerbated by COVID-19 and that changes to the US opioid treatment program model are needed to improve the timeliness of access. Increased open-access model adoption may increase timely access.
Introduction
Opioid overdose deaths are rising in the context of the COVID-19 pandemic.1,2,3 Timely access to medications for opioid use disorder (OUD) is critical to preventing overdose deaths,4 but COVID-19 may have disrupted the treatment delivery system. Methadone access may be uniquely vulnerable to disruption given the unique regulatory burden and increased risk of COVID-19 among individuals with OUD.5,6,7 Even small disruptions may adversely impact OUD outcomes, as access delays as short as 1 day are associated with decreased medication initiation and delays in methadone initiation are associated with increased illicit opioid use and overdose death.4,8,9
Several countries changed methadone provision policies in response to COVID-19. In the US, methadone for OUD can only be administered (observed medication dosing) or dispensed (take-home medication dosing) at Substance Abuse and Mental Health Service Administration (SAMHSA)–certified opioid treatment programs (OTPs). OTPs must meet multiple federal, state, and local requirements designed to minimize diversion and mandate the frequency of administration, toxicology screening, and behavioral treatment.10 Beginning in March 2020, SAMHSA allowed increased take-home medication and utilization of telemedicine for established patients.11,12,13 Canadian professional organizations also recommended increased take-home medication in March,14 but methadone provision was already less restricted prior to COVID-19 facilitating integration into other health care services.15 Specialty and primary care clinicians may prescribe methadone in-person or through telemedicine,16 and both administration and dispensing may occur within pharmacies.10,17 The flexibility of the Canadian regulatory environment allows for greater variation in the structure of methadone clinics (ie, a clinic providing a methadone order or prescription for OUD) relative to US OTPs.
Research on COVID-19 and methadone access has been limited to date. One study found the number of new patients initiating methadone was unchanged at an OTP in Seattle, Washington, after community transmission increased.18 Timely methadone access prior to COVID-19 was previously compared among pregnant and nonpregnant US Medicaid patients.19,20 To our knowledge, no prior studies have compared timely methadone access within US OTPs and Canadian clinics despite the underlying differences in delivery systems. Therefore, we assessed the timeliness of methadone access among methadone clinics within the US and Canada during COVID-19. We hypothesized more Canadian clinics would accept new patients and would offer a timelier first appointment relative to US OTPs.
Methods
Study Overview and Data Sources
We conducted a cross-sectional study of methadone clinics within selected US and Canadian jurisdictions between May 11 and June 17, 2020. For US jurisdictions, we obtained OTP data on May 4, 2020, from the SAMHSA behavioral health treatment services locator, which were derived from the 2019 National Survey of Substance Abuse Treatment Services.21 For Canadian provinces Alberta and Ontario, we obtained methadone clinic data on May 3, 2020, from the Alberta Health Services addiction and mental health service website and the ConnexOntario addiction, mental health, and problem gambling treatment services website.22,23 For the Canadian province of British Columbia, we obtained methadone clinic data from the January 2020 version of the British Columbia Centre directory on Substance Use Opioid Agonist Treatment Clinics.24 We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies. The Yale institutional review board determined that this study was exempt because it did not involve human participants.
Study Sample
We included all clinics providing methadone for OUD within the US jurisdictions of Connecticut, District of Columbia, Kentucky, Maine, Massachusetts, Maryland, Michigan, Missouri, New Hampshire, Ohio, Rhode Island, Tennessee, Vermont, and West Virginia, and the Canadian provinces of Alberta, British Columbia, and Ontario, which represented the jurisdictions with the highest 2018 opioid overdose death rates within each nation (eMethods 1 in the Supplement).1,2 We selected 14 US and 3 Canadian jurisdictions to create the largest feasible sample of clinics of similar size within each nation. Two states, Tennessee and Missouri, had not expanded Medicaid at the time of the study.25 We excluded clinics serving special populations (ie, Veterans Health Administration), clinics with a wrong phone number, clinics without methadone treatment, and clinics requesting individual identification (ie, Medicaid plan number) preventing data collection (Figure).
Figure. Cohort Flow Diagram of Methadone Clinics Contacted in the US and Canada in 2020.
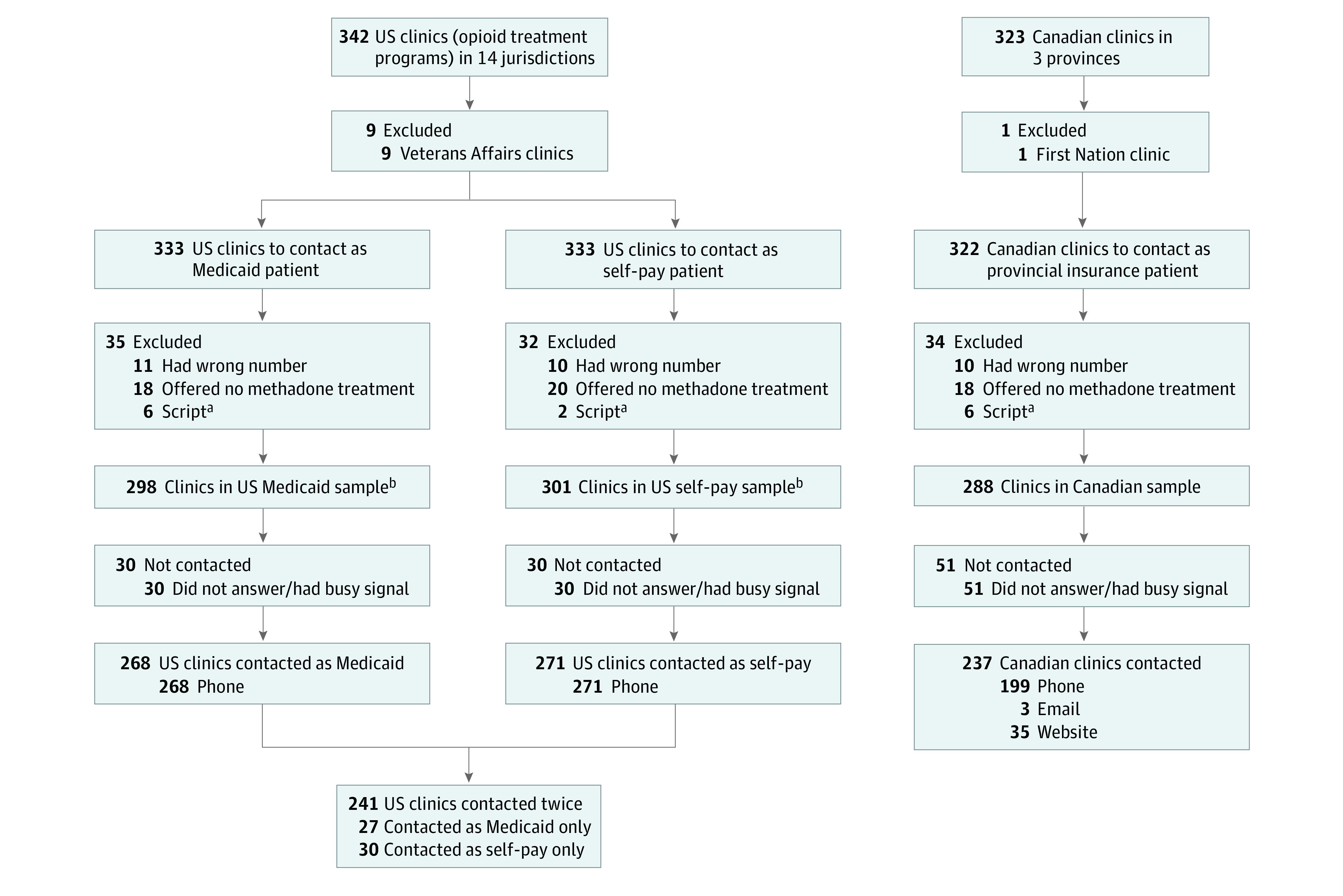
aExcluded because of clinic request for individual identification (ie, Medicaid plan number) preventing data collection.
bStandardized patient calls were made simulating a patient aged 30 years seeking to start methadone treatment. Within the US, clinics were contacted twice: once as a patient with Medicaid and once as a patient with no health insurance (self-pay). Within Canada, clinics were contacted once as a patient with provincial insurance.
Data Collection
Trained research team members contacted clinics at their publicly listed phone number. Consistent with prior studies,26 callers followed a standardized script simulating a patient aged 30 years seeking the next available appointment to initiate methadone (eMethods 2 and eMethods 3 in the Supplement). Each US clinic was contacted twice by different research team members: once as a patient with Medicaid and once as a patient with no health insurance (self-pay). In the US multiple payer system, up to two-thirds of patients pay for methadone services with Medicaid or self-pay owing to lack of health insurance.27,28 The Substance Use Disorder Prevention That Promotes Opioid Recovery and Treatment for Patients and Communities (SUPPORT) Act required state Medicaid programs to cover methadone treatment starting in October of 2020.29 Canadian clinics were contacted once as a patient with provincial insurance. Provincial insurance covers methadone-related medical visits for all citizens of a province. Clinics without successful contact (no answer or busy signal) after 3 attempts were classified as not contacted. One network of clinics in Ontario, Canada, did not answer requests by phone and its automated voice message directed callers to a website for open-access (weekly walk-in hours for new patients without appointment) information. Three clinics in this network were contacted by email to confirm the schedule. For all other clinics in this network, the next available appointment was determined according to the website.
Outcomes
Our primary outcomes were (1) accepting new patients for methadone treatment (yes/no) and (2) wait to first appointment (days). In person and telehealth visits were accepted for the first appointment. We collected secondary outcomes to further characterize methadone provision during COVID-19. Among all clinics, secondary outcomes included (1) status of methadone treatment among clinics not accepting new patients (not accepting new patients, wait list, required inpatient detoxification, only accepts transfer from another facility), (2) not accepting new patients due to COVID-19, (3) possible to start methadone at first visit (ie, completion of clinician’s order among US OTPs or prescription among Canadian clinics), (4) open-access model, (5) clinic COVID-19 adaptations (increased take-home medication, bottle drop-off service, groups or counseling cancellation, telehealth groups or counseling, telemedicine prescribing, other), and (6) available transportation assistance. To reduce question burden, US clinics were only asked about COVID-19 adaptations during Medicaid calls.
We also collected secondary outcomes specific to nation and health insurance. Secondary outcomes for US Medicaid included (1) accepting Medicaid and (2) Medicaid first visit copay. Secondary outcomes for US self-pay included (1) accepting self-pay and (2) first visit self-pay costs. Secondary outcomes for Canadian provincial insurance included first visit copay.
Informed by implementation of an OTP open-access model,30 we created a secondary composite outcome to examine the proportion of clinics completing 5 cascading events necessary for timely methadone access: (1) successfully contacted clinic, (2) accepted new patients, (3) offered an appointment, (4) offered methadone at the first visit, and (5) scheduled the first visit within 1 day.
Covariates
Clinics were classified as located in an urban or rural postal code according to the US Federal Office of Rural Health Policy and the Statistics Canada Population Centre rural area classification for postal codes.31,32 Because US and Canadian definitions for urban and rural were not equivalent, we did not make urban-rural comparisons.
Statistical Analysis
First, we identified the frequency of contacted and not contacted clinics in each jurisdiction and the frequency of rural clinics by nation and insurance. We completed descriptive analyses by nation and insurance for all primary and secondary outcomes. The proportion of clinics accepting new patients among US Medicaid and US self-pay contacts were compared with Canadian contacts using a χ2 test. We compared the mean wait to first appointment among US Medicaid and Canadian contacts and US self-pay and Canadian contacts using a 2-sample t test and among US Medicaid and US self-pay contacts using a paired t test. Next, we estimated the proportion (cumulative probability) of clinics completing 5 cascading events for timely methadone access using a Kaplan-Meier function to account for censored observations due to non-response among secondary outcomes. We compared the proportion of clinics completing the 5 cascading events by nation and insurance using a log-rank test.
As an exploratory analysis, we compared the wait to first appointment among contacts with vs without an open-access model and among contacts reporting vs not reporting COVID-19 adaptations (telemedicine prescribing, take-home medication, and bottle drop-off service) within each nation using a 2-sample t test. If a COVID-19 adaptation was associated with wait to first appointment, we repeated the analysis while accounting for clinic open-access status. As a sensitivity analysis, we repeated our analyses of our primary outcomes while excluding the network of clinics not accepting phone calls. Additionally, we repeated our analysis of the proportion of clinics accepting new patients, while including all clinics publicly listed as providing methadone for OUD (including clinics with a wrong phone number and without methadone treatment) to examine the patient experience of using the service directories. We used pairwise deletion for missing primary or secondary outcome data. All hypothesis tests were 2-sided with an α of .05. We completed our analysis using Stata 15 (StataCorp) from July 2020 to January 2021.
Results
Among 342 clinics within US jurisdictions, we excluded 9 Veterans Health Administration clinics and among 323 clinics within Canadian provinces, we excluded 1 First Nation clinic. We excluded 35 clinics from the US Medicaid sample, 32 clinics from the US self-pay sample, and 34 clinics from the Canadian sample because of a wrong phone number, lack of methadone treatment, or request for individual identification. We successfully contacted 268 clinics (90%) during US Medicaid calls, 271 clinics (90%) during US self-pay calls, and 237 clinics (82%) during Canadian calls (Table 1). Forty Medicaid contacts (15%), 43 self-pay contacts (16%), and 10 Canadian contacts (4%) were rural clinics.
Table 1. Geographic Characteristics of Contacted and Unable-to-Contact Methadone Clinics Within 14 US and 3 Canadian Jurisdictions in 2020.
| Jurisdiction and insurance type | No. (%) | |
|---|---|---|
| Unable to contacta | Contacted | |
| US: Medicaid (n = 298)b | ||
| All US | 30 | 268 |
| Connecticut | 2 (7) | 28 (10) |
| District of Columbia | 0 | 3 (1) |
| Kentucky | 2 (7) | 24 (9) |
| Massachusetts | 2 (7) | 44 (16) |
| Maryland | 5 (17) | 63 (23) |
| Maine | 1 (3) | 6 (2) |
| Michigan | 4 (13) | 31 (12) |
| Missouri | 4 (13) | 9 (3) |
| New Hampshire | 1 (3) | 5 (2) |
| Ohio | 4 (13) | 21 (8) |
| Rhode Island | 2 (7) | 13 (5) |
| Tennessee | 1 (3) | 8 (3) |
| Vermont | 1 (3) | 5 (2) |
| West Virginia | 1 (3) | 8 (3) |
| Rural clinicc | 4 (13) | 40 (15) |
| US: self-pay (n = 301) | ||
| All US | 30 | 271 |
| Connecticut | 3 (10) | 27 (10) |
| District of Columbia | 0 | 3 (1) |
| Kentucky | 3 (10) | 23 (8) |
| Massachusetts | 5 (17) | 42 (15) |
| Maryland | 7 (23) | 60 (22) |
| Maine | 0 | 6 (2) |
| Michigan | 4 (13) | 33 (12) |
| Missouri | 3 (10) | 10 (4) |
| New Hampshire | 0 | 7 (3) |
| Ohio | 3 (10) | 22 (8) |
| Rhode Island | 0 | 14 (5) |
| Tennessee | 0 | 10 (4) |
| Vermont | 1 (3) | 6 (2) |
| West Virginia | 1 (3) | 8 (3) |
| Rural clinicc | 3 (10) | 43 (16) |
| Canada: provincial insurance (n = 288) | ||
| All Canadian | 51 | 237 |
| Alberta | 0 | 24 (10) |
| British Columbia | 22 (43) | 87 (37) |
| Ontario | 29 (57) | 126 (53) |
| Rural clinicc | 2 (4) | 10 (4) |
Clinics were designated unable to contact if no contact was made after 3 attempts (no answer or busy signal).
Standardized patient calls were made simulating a patient aged 30 years seeking to start methadone treatment. Within the US, clinics were contacted twice: once as a patient with Medicaid and once as a patient with no health insurance (self-pay). Within Canada, clinics were contacted once as a patient with provincial insurance.
Clinics were classified as located in an urban or rural postal code according to the US Federal Office of Rural Health Policy and the Statistics Canada Population Centre rural area classification for postal codes.
Clinics Accepting New Patients and Wait to First Appointment
New patients were accepted for methadone treatment at 231 clinics (86% [95% CI, 82%-90%]) during US Medicaid contacts, 230 clinics (85% [95% CI, 80%-89%]) during US self-pay contacts, and 210 clinics (89% [95% CI, 84%-92%]) during Canadian contacts (US Medicaid vs Canadian: P = .41; US self-pay vs Canadian: P = .22) (Table 2). Among clinics not accepting new patients, 20 of 37 US Medicaid contacts (54%), 20 of 42 US self-pay contacts (48%), and 12 of 27 Canadian clinics (44%) reported not accepting new patients because of COVID-19.
Table 2. Status of Methadone Treatment and Days to First Appointment Among Contacted Methadone Clinics Within 14 US and 3 Canadian Jurisdictions in 2020.
| Outcome | No. (%) | P value | ||
|---|---|---|---|---|
| US | Canada, Provincial insurance | |||
| Medicaida | Self-pay | |||
| Contacted clinics, No. | 268 | 271 | 237 | NA |
| Status of methadone | ||||
| Accepting new patients | 231 (86) | 230 (85) | 210 (89) | NA |
| Not accepting new patientsb | 20 (7) | 22 (8) | 25 (11) | NA |
| Wait list | 8 (3) | 9 (3) | 1 (0.5) | NA |
| Require inpatient detoxificationc | 2 (1) | 2 (1) | 0 (0) | NA |
| Only accepts transfersd | 7 (3) | 8 (3) | 1 (0.5) | NA |
| Contacted clinics reporting on appointment availability, No. | 257 | 268 | 237 | NA |
| Offered appointment | 190 (74) | 193 (72) | 196 (83) | NA |
| Days to first appointment | ||||
| Median (IQR) | 2 (1-4) | 3 (1-5) | 1 (1-3) | NA |
| Mean (95% CI) | 3.5 (2.9-4.2) | 4.1 (3.4-4.8) | 1.9 (1.7-2.1) | <.001e |
Abbreviation: IQR, interquartile range.
Standardized patient calls were made simulating a patient aged 30 years seeking to start methadone treatment. Within the US, clinics were contacted twice: once as a patient with Medicaid and once as a patient with no health insurance (self-pay). Within Canada, clinics were contacted once as a patient with provincial insurance.
Methadone treatment available but not currently accepting new patients for unspecified reasons.
Only accepts new patients after completion of inpatient detoxification.
Only accepts new patients transferred from another facility.
Two-sample t test with unequal variance for US Medicaid vs Canada and US self-pay vs Canada.
Among clinics reporting on appointment availability, 190 US Medicaid contacts (74%), 193 US self-pay contacts (72%), and 196 Canadian contacts (83%) offered to schedule an appointment. Reasons for not offering an appointment included (1) scheduler was not available or (2) administrative requirements. Among clinics offering an appointment, 157 of 178 US Medicaid contacts (88%), 150 of 179 US self-pay contacts (84%), and 137 of 146 Canadian clinics (94%) reported it was possible to start methadone at the first appointment.
The mean wait to first appointment was greater among US Medicaid contacts (3.5 days [95% CI, 2.9-4.2 days]) and US self-pay contacts (4.1 days [95% CI, 3.4-4.8 days]) than among Canadian contacts (1.9 days [95% CI, 1.7-2.1 days]) (P < .001) (US Medicaid vs US self-pay: P = .32). The proportion of clinics providing timely access (successfully contacted clinic, accepted new patients, offered an appointment, offered methadone at the first visit, and scheduled the first visit within 1 day) was lower among US Medicaid contacts (24% [95% CI, 19%-30%]) and US self-pay contacts (20% [95% CI, 16%-25%]) than among Canadian clinics (46% [95% CI, 39%-52%]; P < .001) (eTable 1 and eFigure in the Supplement).
Open-Access Model and COVID-19 Adaptations
Open-access model utilization was reported by 57 Medicaid contacts (30%), 57 self-pay contacts (30%), and 115 Canadian contacts (59%) offering an appointment. The open-access model was associated with a shorter wait to first appointment relative to clinics without an open-access model in both nations (Table 3). To adapt services to COVID-19, more than 50% of US Medicaid and Canadian contacts reported providing telemedicine prescribing (Table 4). Adaptations such as increased take-home medication allowance, bottle drop-off services, and telehealth for groups and counseling were reported more frequently among US vs Canadian contacts. Among US clinics without an open-access model, adoption (vs no adoption) of increased take-home medication was associated with a shorter wait to first appointment (Table 3). More than half (57%; 100 contacts) of US Medicaid contacts, 86% (143 contacts) of US self-pay contacts, and 84% (104 contacts) of Canadian contacts provided no transportation assistance (eTable 2 in the Supplement).
Table 3. Days to First Appointment for Methadone by Clinic Open Access Model or COVID-19 Adaptation Among US and Canadian Methadone Clinics in 2020.
| Variable | Days to first appointment | ||||
|---|---|---|---|---|---|
| No. | Yes, mean (95% CI) | No. | Yes, mean (95% CI) | P value | |
| Open access modela | |||||
| US Medicaidb | 57 | 1.9 (1.5-2.4) | 133 | 4.2 (3.3-5.1) | <.001 |
| US self-pay | 57 | 2.5 (1.9-3.0) | 136 | 4.8 (3.8-5.7) | <.001 |
| Canadian | 115 | 1.6 (1.3-1.8) | 80 | 2.3 (1.9-2.8) | .003 |
| Telemedicine prescribingc | |||||
| US Medicaid | 73 | 3.4 (2.5-4.4) | 77 | 3.3 (2.5-4.2) | .89 |
| Canadian | 59 | 2.1 (1.6-2.6) | 54 | 1.7 (1.3-2.1) | .23 |
| Increased take-home medicationsd | |||||
| US Medicaid | 52 | 2.6 (1.9-3.3) | 100 | 3.8 (2.9-4.7) | .04 |
| Increased take-home medications by clinic open access status | |||||
| US Medicaid with open access | 14 | 2.0 (1.0-3.0) | 31 | 1.7 (1.2-2.3) | .62 |
| US Medicaid without open access | 38 | 2.8 (1.9-3.7) | 69 | 4.7 (3.5-5.9) | .01 |
| Bottle drop-off serviced | |||||
| US Medicaid | 17 | 3.7 (1.4-6.0) | 133 | 3.3 (2.7-4.0) | .72 |
Weekly walk-in hours for new patients without appointment.
Standardized patient calls were made simulating a patient aged 30 years seeking to start methadone treatment. Within the US, clinics were contacted twice: once as a patient with Medicaid and once as a patient with no health insurance (self-pay). Within Canada, clinics were contacted once as a patient with provincial insurance.
To reduce question burden, US clinics were not asked about COVID-19 adaptations during self-pay calls.
Adaptations (take-home medication and bottle drop-off service among Canadian clinics were too infrequent for comparison).
Table 4. Adaptations to COVID-19 Among Methadone Clinics in the US and Canada in 2020.
| Adaptation | No. (%) | |
|---|---|---|
| US Medicaid (n = 189)a | Canadian provincial insurance (n = 123) | |
| Increased take-home medicationb | 59 (31) | 3 (2) |
| Bottle drop-off servicec | 18 (10) | 1 (1) |
| Groups/counseling cancellation | 31 (16) | 2 (2) |
| Telehealth groups/counseling | 88 (47) | 6 (5) |
| Telemedicine prescribing | 96 (51) | 68 (55) |
| Other adaptation | 126 (67) | 75 (61) |
Standardized patient calls were made simulating a patient aged 30 years seeking to start methadone treatment. Within the US, clinics were contacted twice: once as a patient with Medicaid and once as a patient with no health insurance (self-pay). Within Canada, clinics were contacted once as a patient with provincial insurance. To reduce question burden, US clinics were not asked about COVID-19 adaptations during self-pay calls.
Increased allowance of take-home medication.
Service to deliver methadone to the patient in the community.
First Visit Costs
Among US Medicaid contacts, 198 of 225 (88%) accepted Medicaid and 157 of 167 (94%) required no copayment. The median (IQR) first visit Medicaid copay was US $25 (US $12-$70). The median (IQR) first visit cost among clinics not accepting Medicaid was US $75 (US $16-$140). During US self-pay contacts, 217 of 228 (95%) allowed first visit self-pay at a median (IQR) of US $87 (US $18-$144). Among Canadian contacts, 13 of 168 (8%) reported a median (IQR) first visit copay of CAD $3.75 (CAD $2-$68) (US $2.72 on May 30, 2020).
Sensitivity Analysis
After exclusion of the 38 clinics not scheduling by phone, our primary outcomes were consistent. New patients were accepted at 173 of 199 Canadian contacts (87% [95% CI, 81%-91%]) with a mean of 2.0 days to first appointment (95% CI, 1.7-2.2 days). Upon inclusion of all clinics publicly listed as providing methadone, 231 of 285 clinics during US Medicaid contacts (81% [95% CI, 76%-85%]), 230 of 290 clinics during US self-pay contacts (79% [95% CI, 74%-83%]), and 210 of 255 clinics during Canadian contacts (82% [95% CI, 77%-87%]) accepted new patients.
Discussion
In this cross-sectional study of methadone clinics during COVID-19 in 13 US states and the District of Columbia and 3 Canadian provinces with the highest rates of opioid overdose deaths, more than 1 in 10 clinics were not accepting new patients. More than one-third of clinics not accepting new patients reported that this was due to COVID-19. Canadian methadone clinics offered appointments faster than US OTPs. Fewer than half of Canadian clinics and fewer than one-quarter of US clinics (Medicaid or self-pay) offered appointments with the possibility of starting methadone within 1 day of contact. Together, our results suggest that a greater portion of Canadian methadone clinics provide timely access to methadone relative to US OTPs, but impediments to timely access are present at most clinics in both nations.
Although rates of methadone initiation were unchanged at an OTP serving 2630 patients in Seattle, Washington, during COVID-19,18 methadone clinics in both nations reported not accepting new patients due to COVID-19 despite adaptation efforts. Our results are consistent with other reports of disruptions to treatment services by individuals with substance use disorder during COVID-19.33 Our results suggest that previous studies overestimate methadone availability when all clinics are assumed to accept new patients.34,35,36,37 Importantly, people using public treatment directories to initiate methadone during the study period had approximately a 1 in 5 chance of engaging with a clinic not accepting new patients and innovations are needed to improve the quality of methadone service information.
Relative to Canadian clinics, we found the US approach of limiting methadone provision to specialized OTPs was not associated with more timely access to care. The mean difference in wait to first appointment between US OTPs and the less-regulated Canadian clinics was approximately 2 days, and previous research suggests this difference is clinically meaningful as patients with same-day access have 7.5 times the odds of arriving for their medication initiation visit relative to 2 or more days wait.8,9 Our results suggest explanations for the observed difference in wait times. Uptake of an open-access model was greater in Canada and was associated with more timely methadone access in both nations. Open-access model adoption does not require removal of regulatory restrictions and US and Canadian agencies should consider implementation interventions and reimbursement changes to expand adoption.38 Delays in access due to insufficient clinic capacity may be more likely within the US relative to Canada,36 which has allowed methadone provision within a greater variety of clinical settings and has reduced regulatory restrictions in response to the overdose epidemic.15 The greater complexity of the US multiple payer system may also delay access relative to Canada, and the cost of a first appointment may create an additional barrier within the US. Three months prior to the SUPPORT Act Medicaid requirement, we observed greater Medicaid acceptance among US OTPs relative to observed 2019 rates.20
Methadone clinics in both nations adapted their services to COVID-19. Telemedicine prescribing was reported by more than half of clinics within both nations. Although telemedicine was not associated with timely access, it may still reduce COVID-19 transmission. That increased take-home medication allowance, bottle drop-off services, and telehealth for groups and counseling were reported more frequently among US vs Canadian clinics suggests US OTPs required greater adaptation because of the mandated colocation of services. Within Canada, adaptions such as bottle drop-off services may have occurred at pharmacies. Among US clinics without an open-access model, increased take-home medication allowance was associated with timelier methadone access. Relaxation of take-home medication requirements may benefit patients initiating methadone at some OTPs, and future research should examine if this policy could reduce overdose, despite the potential risk of diversion, by increasing access.
That most clinics in both nations did not offer transportation assistance adds to concern over the high travel burden of methadone provision,34,37,39 a problem likely exacerbated by COVID-19 public transportation disruptions.40 Our US results suggest transportation assistance is less available to patients without health insurance. Greater adoption of mobile methadone units (methadone provisioning vehicles) could mitigate this barrier, and the US Drug Enforcement Agency recently proposed ending a moratorium on new mobile units.41
Limitations
This study has several limitations. Although we contacted more than 80% of clinics for our primary outcomes, differences between respondents and nonrespondents may bias our results for secondary outcomes with lower response rates. The self-report of COVID-19 disruptions and adaptations may result in recall bias. However, US OTPs offered an appointment to 89% of Medicaid patients during a 2019 audit study compared with the 74% observed in our study.20 Although relatively few US patients receiving methadone utilize private insurance, we did not examine this population. Past research suggests US private insurance is also associated with access barriers.42 Although this study found evidence of more timely access to methadone within Canadian provinces, it underestimates true access within Canada because primary care prescribing may occur, although this is not the norm.43,44,45 These results examine access at the clinic level and do not assess the impact of nearby alternate clinics. However, consideration of coordination among nearby clinics is likely to further improve timely access in Canada compared with the US given the known geographic limitations of methadone availability within the US.34 We report the cost of the first appointment, and the cost of the medication may be an additional cost. These results may not extend to jurisdictions with lower rates of overdose deaths. Our results represent COVID-19 disruptions during late May and early June of 2020, a time when COVID-19 cases were being reported within all study jurisdictions but initial social distancing measures were being scaled back.46,47,48 How disruptions evolve should be a focus of further research.
Conclusions
More than 10% of methadone clinics within jurisdictions with the highest rates of opioid overdose deaths in the US and Canada were not accepting new patients. Canadian methadone clinics were able to offer more timely methadone access relative to US OTPs. These results suggest that COVID-19 exacerbated the shortage in methadone access and changes to the US OTP model are needed to improve the timeliness of access. Timely access may be improved with increased open-access model adoption.
eMethods 1. Identification of Clinics
eMethods 2. Data Collection Team and Procedures
eMethods 3. Methadone Audit Study Patient Scripts
eTable 1. Methadone Treatment Access Cascade Among Methadone Clinics Within the US and Canada in 2020
eTable 2. Transportation Assistance Among Methadone Clinics During Coronavirus 2019 (COVID-19) in the US and Canada in 2020
eFigure. Methadone Treatment Access Cascade Among Methadone Clinics Within the US and Canada in 2020
References
- 1.Special Advisory Committee on the Epidemic of Opioid Overdoses . Opioid-related harms in Canada. Accessed August 27, 2020. https://health-infobase.canada.ca/substance-related-harms/opioids/
- 2.Wilson N, Kariisa M, Seth P, Smith H IV, Davis NL. Drug and opioid-involved overdose deaths—United States, 2017-2018. MMWR Morb Mortal Wkly Rep. 2020;69(11):290-297. doi: 10.15585/mmwr.mm6911a4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ochalek TA, Cumpston KL, Wills BK, Gal TS, Moeller FG. Nonfatal opioid overdoses at an urban emergency department during the COVID-19 pandemic. JAMA. 2020;324(16):1673-1674. doi: 10.1001/jama.2020.17477 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Larochelle MR, Bernson D, Land T, et al. Medication for opioid use disorder after nonfatal opioid overdose and association with mortality: a cohort study. Ann Intern Med. 2018;169(3):137-145. doi: 10.7326/M17-3107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Joudrey PJ, Edelman EJ, Wang EA. Methadone for opioid use disorder-decades of effectiveness but still miles away in the us. JAMA Psychiatry. 2020;77(11):1105-1106. doi: 10.1001/jamapsychiatry.2020.1511 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang QQ, Kaelber DC, Xu R, Volkow ND. COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol Psychiatry. Published online September 14, 2020:1-10. doi: 10.1038/s41380-020-00880-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Becker WC, Fiellin DA. When epidemics collide: coronavirus disease 2019 (COVID-19) and the opioid crisis. Ann Intern Med. 2020;173(1):59-60. doi: 10.7326/M20-1210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Roy PJ, Choi S, Bernstein E, Walley AY. Appointment wait-times and arrival for patients at a low-barrier access addiction clinic. J Subst Abuse Treat. 2020;114:108011. doi: 10.1016/j.jsat.2020.108011 [DOI] [PubMed] [Google Scholar]
- 9.Schwartz RP, Highfield DA, Jaffe JH, et al. A randomized controlled trial of interim methadone maintenance. Arch Gen Psychiatry. 2006;63(1):102-109. doi: 10.1001/archpsyc.63.1.102 [DOI] [PubMed] [Google Scholar]
- 10.Calcaterra SL, Bach P, Chadi A, et al. Methadone matters: what the United States can learn from the global effort to treat opioid addiction. J Gen Intern Med. 2019;34(6):1039-1042. doi: 10.1007/s11606-018-4801-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Priest KC. The COVID-19 pandemic: practice and policy considerations for patients with opioid use disorder. HealthAffairs . Published 2020. Accessed October 27, 2020. https://www.healthaffairs.org/do/10.1377/hblog20200331.557887/full/
- 12.SAMHSA . Opioid Treatment Program (OTP) guidance. Published 2020. Accessed June 18, 2021. https://www.samhsa.gov/sites/default/files/otp-guidance-20200316.pdf
- 13.Davis CS, Samuels EA. Opioid policy changes during the COVID-19 pandemic—and beyond. J Addict Med. 2020;14(4):e4-e5. doi: 10.1097/ADM.0000000000000679 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lam V, Sankey C, Wyman J, Zhang M. COVID-19 opioid agonist treatment guidance. Published online 2020. Accessed June 18, 2021. https://www.camh.ca/-/media/files/covid-19-modifications-to-opioid-agonist-treatment-delivery-pdf.pdf?la=en&hash=261C3637119447097629A014996C3C422AD5DB05
- 15.Priest KC, Gorfinkel L, Klimas J, Jones AA, Fairbairn N, McCarty D. Comparing Canadian and United States opioid agonist therapy policies. Int J Drug Policy. 2019;74:257-265. doi: 10.1016/j.drugpo.2019.01.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bruneau J, Rehm J, Wild TC, et al. Telemedicine support for addiction services: national rapid guidance document. Published 2020. Accessed June 18, 2021. https://crism.ca/wp-content/uploads/2020/05/CRISM-National-Rapid-Guidance-Telemedicine-V1.pdf
- 17.Leshner AI, Mancher M. Medications for Opioid Use Disorder Save Lives. National Academies of Sciences, Enginneering, and Medicine; 2019. [PubMed] [Google Scholar]
- 18.Peavy KM, Darnton J, Grekin P, et al. Rapid implementation of service delivery changes to mitigate COVID-19 and maintain access to methadone among persons with and at high-risk for HIV in an opioid treatment program. AIDS Behav. 2020;24(9):2469-2472. doi: 10.1007/s10461-020-02887-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Patrick SW, Buntin MB, Martin PR, et al. Barriers to accessing treatment for pregnant women with opioid use disorder in Appalachian states. Subst Abus. 2019;40(3):356-362. doi: 10.1080/08897077.2018.1488336 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Patrick SW, Richards MR, Dupont WD, et al. Association of pregnancy and insurance status with treatment access for opioid use disorder. JAMA Netw Open. 2020;3(8):e2013456-e2013456. doi: 10.1001/jamanetworkopen.2020.13456 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.SAMHSA . Behavioral health treatment services locator. Accessed August 27, 2020. https://findtreatment.samhsa.gov/
- 22.Alberta Health Services . Addiction and mental health. Accessed August 27, 2020. https://www.albertahealthservices.ca/amh/amh.aspx
- 23.ConnexOntario . Addiction, mental health, and problem gambling treatment services. Accessed August 27, 2020. https://www.connexontario.ca/
- 24.British Columbia Centre on Substance Use . OAT clinics accepting new patients. Accessed August 27, 2020. https://www.bccsu.ca/oat-clinics-accepting-new-patients/
- 25.Kaiser Family Foundation . Status of state Medicaid expansion decisions: interactive map. Published November 2, 2020. Accessed December 2, 2020. https://www.kff.org/medicaid/issue-brief/status-of-state-medicaid-expansion-decisions-interactive-map/
- 26.Beetham T, Saloner B, Wakeman SE, Gaye M, Barnett ML. Access to office-based buprenorphine treatment in areas with high rates of opioid-related mortality: an audit study. Ann Intern Med. 2019;171(1):1-9. doi: 10.7326/M18-3457 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Orgera K, Tolbert J. Key facts about uninsured adults with opioid use disorder. Kaiser Family Foundation . Published July 15, 2019. Accessed October 27, 2020. https://www.kff.org/uninsured/issue-brief/key-facts-about-uninsured-adults-with-opioid-use-disorder/
- 28.Fingerhood MI, King VL, Brooner RK, Rastegar DA. A comparison of characteristics and outcomes of opioid-dependent patients initiating office-based buprenorphine or methadone maintenance treatment. Subst Abus. 2014;35(2):122-126. doi: 10.1080/08897077.2013.819828 [DOI] [PubMed] [Google Scholar]
- 29.Musumeci MB, Tobert J. Federal legislation to address the opioid crisis: Medicaid provisions in the SUPPORT Act. Kaiser Family Foundation . Published October 5, 2018. Accessed January 24, 2021. https://www.kff.org/medicaid/issue-brief/federal-legislation-to-address-the-opioid-crisis-medicaid-provisions-in-the-support-act/
- 30.Madden LM, Farnum SO, Eggert KF, et al. An investigation of an open-access model for scaling up methadone maintenance treatment. Addiction. 2018;113(8):1450-1458. doi: 10.1111/add.14198 [DOI] [PubMed] [Google Scholar]
- 31.HRSA . Federal Office of Rural Health Policy (FORHP) Data Files. Official website of the U.S. Health Resources & Services Administration. Published April 28, 2017. Accessed August 27, 2020. https://www.hrsa.gov/rural-health/about-us/definition/datafiles.html
- 32.Statistics Canada . Postal Code Conversion File. Published December 13, 2017. Accessed August 27, 2020. https://www150.statcan.gc.ca/n1/en/catalogue/92-154-X
- 33.Huhn AS, Strain EC, Jardot J, et al. Treatment Disruption and Childcare Responsibility as Risk Factors for Drug and Alcohol Use in Persons in Treatment for Substance Use Disorders During the COVID-19 Crisis. J Addict Med. 2021. doi: 10.1097/ADM.0000000000000813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Joudrey PJ, Edelman EJ, Wang EA. Drive times to opioid treatment programs in urban and rural counties in 5 US states. JAMA. 2019;322(13):1310-1312. doi: 10.1001/jama.2019.12562 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Abraham AJ, Andrews CM, Yingling ME, Shannon J. Geographic disparities in availability of opioid use disorder treatment for Medicaid enrollees. Health Serv Res. 2018;53(1):389-404. doi: 10.1111/1475-6773.12686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Mojtabai R, Mauro C, Wall MM, Barry CL, Olfson M. Medication treatment for opioid use disorders in substance use treatment facilities. Health Aff (Millwood). 2019;38(1):14-23. doi: 10.1377/hlthaff.2018.05162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Eibl JK, Gomes T, Martins D, et al. Evaluating the effectiveness of first-time methadone maintenance therapy across northern, rural, and urban regions of Ontario, Canada. J Addict Med. 2015;9(6):440-446. doi: 10.1097/ADM.0000000000000156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Joseph G, Torres-Lockhart K, Stein MR, Mund P, Nahvi S. Reimagining patient-centered care in opioid treatment programs: lessons from the Bronx during COVID-19. J Subst Abuse Treat. Published online December 3, 2020:108219. doi: 10.1016/j.jsat.2020.108219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Iloglu S, Joudrey PJ, Wang EA, Thornhill TA IV, Gonsalves G. Expanding access to methadone treatment in Ohio through federally qualified health centers and a chain pharmacy: a geospatial modeling analysis. Drug Alcohol Depend. 2021;220:108534. doi: 10.1016/j.drugalcdep.2021.108534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Tirachini A, Cats O.. COVID-19 and Public Transportation: Current Assessment, Prospects, and Research Needs. J Public Trans. 2020;22(1). doi: 10.5038/2375-0901.22.1.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Knopf A. DEA proposal for mobile methadone finally released. Alcoholism & Drug Abuse Weekly. 2020;32(10):3-4. doi: 10.1002/adaw.32650 [DOI] [Google Scholar]
- 42.Polsky D, Arsenault S, Azocar F. Private coverage of methadone in outpatient treatment programs. Psychiatr Serv. 2020;71(3):303-306. doi: 10.1176/appi.ps.201900373 [DOI] [PubMed] [Google Scholar]
- 43.Eibl JK, Morin K, Leinonen E, Marsh DC. The state of opioid agonist therapy in Canada 20 years after federal oversight. Can J Psychiatry. 2017;62(7):444-450. doi: 10.1177/0706743717711167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Livingston JD, Adams E, Jordan M, MacMillan Z, Hering R. Primary care physicians’ views about prescribing methadone to treat opioid use disorder. Subst Use Misuse. 2018;53(2):344-353. doi: 10.1080/10826084.2017.1325376 [DOI] [PubMed] [Google Scholar]
- 45.Kurdyak P, Jacob B, Zaheer J, Fischer B. Patterns of methadone maintenance treatment provision in Ontario: policy success or pendulum excess? Can Fam Physician. 2018;64(2):e95-e103. [PMC free article] [PubMed] [Google Scholar]
- 46.Public Health Agency of Canada . Coronavirus disease (COVID-19): outbreak update. Published August 4, 2020. Accessed August 27, 2020. https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection.html
- 47.Johns Hopkins Coronavirus Resource Center . Impact of opening and closing decisions by state. Accessed October 2, 2020. https://coronavirus.jhu.edu/data/state-timeline
- 48.USAFacts . US coronavirus cases and deaths. Published August 27, 2020. Accessed August 27, 2020. https://usafacts.org/visualizations/coronavirus-covid-19-spread-map
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods 1. Identification of Clinics
eMethods 2. Data Collection Team and Procedures
eMethods 3. Methadone Audit Study Patient Scripts
eTable 1. Methadone Treatment Access Cascade Among Methadone Clinics Within the US and Canada in 2020
eTable 2. Transportation Assistance Among Methadone Clinics During Coronavirus 2019 (COVID-19) in the US and Canada in 2020
eFigure. Methadone Treatment Access Cascade Among Methadone Clinics Within the US and Canada in 2020