

Abstract
Extant research has typically examined neighborhood characteristics in isolation using variable-centered approaches; however, there is reason to believe that perceptions of the neighborhood environment influence each other, requiring the use of person-centered approaches to study these relationships. The present study sought to determine profiles of youth that differ in their perceptions of their neighborhoods and objective neighborhood characteristics, and whether these profiles are associated with youth coping. Participants were low-income, African American youth (N = 733; 51.0% female, M age = 18.76 years, SD = 1.71) from a metropolitan city who were originally recruited for the Youth Opportunity program in Baltimore, Maryland. A latent profile analysis was conducted which included self-reported neighborhood social cohesion, collective efficacy, disorder, violence, and disadvantage derived from census data. Coping behaviors, specifically positive cognitive restructuring, problem-focused coping, distraction strategies, and avoidant behaviors were assessed via self-reported questionnaires. Four neighborhood profiles were identified: highest disorder (20.0%); highest violence/highest disadvantage (5.2%); high violence (26.6%); and highest cohesion/lowest disorder (48.2%). Individuals in the highest violence/highest disadvantage profile reported higher positive cognitive restructuring and problem-focused coping than the other profiles. These findings warrant an investigation into the individual assets and contextual resources that may contribute to more positive coping behaviors among youth in more violent and disadvantaged neighborhoods, which has the potential to improve resilient outcomes among youth in similar at-risk settings.
Keywords: Neighborhood risk and protective factors, Latent profiles, Urban youth, Coping
Introduction
Many urban neighborhoods experience high rates of poverty and violence, which often have pernicious effects on life-long mental and physical health (Boardman 2004; Boxer et al. 2008; Latkin and Curry 2003; Ross and Mirowsky 2001). While some urban neighborhoods may experience socioeconomic deprivation and crime, these neighborhoods may also possess assets and strengths that promote youth’s positive development, including approaches to coping with stressors. Many studies that have sought to understand neighborhood-level processes and their impact on coping have examined perceptions of neighborhood characteristics in isolation. However, perceptions of one neighborhood characteristic may influence perceptions of other neighborhood features, which in turn may affect youth’s coping. The paucity of work in this area suggests an important place for further investigation. The identification of neighborhood subgroups (or profiles) may provide a better understanding of the environments that youth are embedded in and clarify how these neighborhoods are associated with how youth cope with the stressors they experience. The purpose of the present study was to address these gaps by identifying profiles of youth that exhibited different perceptions of their neighborhood and varied on objective indicators of the neighborhood environment. A secondary aim was to examine whether profile membership was associated with youth’s coping behaviors.
The manner in which the neighborhood is conceptualized and studied (e.g., via self-reports, census data, observer ratings) varies dramatically across the literature. Indices of the neighborhood environment that have been extensively examined include neighborhood social cohesion, collective efficacy, violence, disorder, and disadvantage (Leventhal and Brooks-Gunn 2000; Sampson et al. 2002). Neighborhood social cohesion refers to positive interactions among neighbors, a feeling of kinship and trust among residents, and a sense of belonging, whereas neighborhood collective efficacy refers to shared social norms among neighbors and the extent to which neighbors will intervene on behalf of the public good (Kingston et al. 2009). Feelings of solidarity among neighbors and the level of neighborhood collective efficacy may be tremendously influenced by other neighborhood characteristics such as the level of violence, disorder, and disadvantage (Browning et al. 2015; Kliewer et al. 2004). Indeed, consistent with social disorganization theory, structural and compositional characteristics of the neighborhood such as poverty, abandoned buildings, or crime may hinder residents from forming social networks and from effectively surveilling youth (Markowitz et al. 2001). For example, in communities primarily comprised of single-parent families, there may be less time to form relationships with neighbors and fewer adults available to supervise young people, increasing the likelihood that youth may be exposed to harmful situations (Kingston et al. 2009). Moreover, in more violent communities, residents may not intervene when social norms are violated because they may not believe their actions will result in change.
Although structural disadvantage and disorder may have a substantial impact on the level of cohesion and collective efficacy in some neighborhoods, it is likely that substantial variability exists in these relationships. In line with pluralistic neighborhood theory, disadvantaged and disordered communities may also possess assets and strengths that support youth’s positive adjustment (Witherspoon and Ennett 2011). For example, it is possible that even within a disadvantaged and violent neighborhood, residents feel a sense of community and a responsibility to protect youth from potential adverse experiences, such as hanging out on dangerous streets (Witherspoon and Ennett 2011). In disadvantaged communities, families experiencing financial or other hardships may reach out to neighbors for support, thus facilitating positive prosocial relationships and trust among residents.
The literature reviewed above suggests that the relationship between neighborhood characteristics is complex and that a comprehensive understanding of the neighborhood environment requires an examination of multiple neighborhood processes concurrently. Extant research has typically examined neighborhood characteristics in isolation (e.g., cohesion or violence) using variable-centered approaches (e.g., structural equation modeling, correlations). While variable-centered techniques may increase understanding of neighborhood processes that operate among all individuals in a sample, person-centered methodologies allow for the identification of distinct subgroups of individuals that reside in different neighborhoods, but experience their neighborhoods similarly and vice versa. Determining subgroups of youth who report residing in disordered neighborhoods with lower levels of neighborhood cohesion/collective efficacy, for instance, may inform the tailoring of interventions aimed at promoting resident connectedness in certain neighborhoods, which may reduce crime and have the potential to promote youth’s positive adjustment (Browning et al. 2013; Sampson et al. 1997).
To date, only two studies have employed person-centered techniques to study neighborhood environments. Recently, Booth et al. (2018) identified neighborhood typologies by examining the racial and socioeconomic status composition of urban youth and observed 4 profiles: (1) a majority white, middle-class profile; (2) a majority Hispanic, low poverty profile; (3) a Black, low poverty profile; and (4) a Black, high poverty profile. In another study, Dupéré and Perkins (2007) identified subgroups of older adults who reported on their perceptions of neighborhood disorder, fear of crime, social ties, and social participation within multiple neighborhoods of Baltimore City. They observed 6 subgroups: (1) “generally advantaged”; (2) “very disadvantaged”; (3) “moderately disadvantaged”; (4) an “organized” subgroup (marked by high social participation); (5) an “anonymous” subgroup (marked by low social participation); and (6) a “middletown” profile (average fear of crime and average social participation). These results highlight variability in the demographic composition of neighborhoods, as well as differences in the subjective experiences that residents have within their communities.
Also, little work has considered how variability in the neighborhood environment influences how youth manage and cope with stressors. Coping has often been conceptualized as a conscious effort to regulate affective, behavioral, or physiological responses to stressors (Compas et al. 2001). Two higher order constructs of coping include approach or engagement coping and avoidance or disengagement coping. Engagement coping generally involves positive cognitive restructuring (i.e., thinking about stressors in a manner that emphasizes the positive, rather than negative, aspects of a stressor) and problem-focused coping (i.e., efforts made to mitigate the stressor). Conversely, disengagement coping typically involves the use of avoidant or distraction strategies, which are characterized by psychologically detaching or distancing oneself from stressful events. Given that coping has substantial effects on youth’s psychological well-being (Wadsworth and Berger 2011), an examination of contextual correlates associated with these behaviors is warranted.
The extent to which neighborhoods affect coping behaviors may depend on the nature and quality of the neighborhood (Boxer and Sloan-Power 2013; Dubow et al. 1997). The examination of neighborhood processes in relation to coping may be particularly relevant to consider during adolescence given that youth experience myriad potentially challenging social, cognitive, and biological changes, and often have greater exposure to extrafamilial influences during this developmental period (Drabick and Steinberg 2011). Positive neighborhood characteristics such as neighborhood cohesion and collective efficacy have been associated with engagement in positive coping strategies, whereas exposure to more impoverished, disorganized neighborhoods characterized by fewer institutional and social resources may hamper youth from developing adaptive coping skills (Kliewer et al. 2004). Youth that perceive their neighborhoods as higher in cohesion and collective efficacy may have more positive interactions with residents and stronger interpersonal ties to their community. These perceived environments may be protective for youth by providing them with social or instrumental support when they experience hardships. As a result, youth may be more likely to engage in more positive coping strategies and potentially view their neighborhoods as less threatening (Brenner et al. 2013; Kliewer et al. 2004). Conversely, youth who live in neighborhoods characterized by higher levels of poverty and violence and who perceive their neighborhoods as lower in cohesion/collective efficacy may have a more negative outlook and engage in avoidant (e.g., wishful thinking) or distraction coping (e.g., diverting one’s attention by engaging in a hobby) (Ayers et al. 1996; Compas et al. 2001). Available person-centered work has indicated that youth who reported moderate to low levels of disorder and crime and fewer social ties within their neighborhoods exhibited higher levels of well-being (Dupéré and Perkins 2007), a construct closely related to coping (Cicognani 2011). Taken together, these results suggest that perceptions and characteristics of the neighborhood may influence youth’s coping mechanisms, though there is a dearth of research in this area.
The Current Study
The present study sought to identify distinct subgroups (or profiles) of youth based on their perceptions of neighborhood social cohesion, collective efficacy, disorder, and violence and objective neighborhood characteristics, specifically disadvantage. The study aimed to identify whether profile membership was associated with youth’s engagement in the following coping behaviors: positive cognitive restructuring, problem-focused coping, avoidant, and distraction strategies. Given the dearth of person-centered research that has considered neighborhood processes concurrently, no specific hypotheses were generated regarding the profiles we expected to observe. However, it was anticipated that profiles characterized by (a) higher levels of disadvantage, disorder, violence, and lower levels of cohesion and collective efficacy would be associated with greater endorsement of avoidant and distraction coping and lower levels of positive cognitive restructuring and problem-focused coping; and (b) lower levels of disadvantage, disorder, and violence, and higher levels of cohesion and collective efficacy would be associated with higher levels of positive cognitive restructuring and problem-focused coping and lower levels of avoidant or distraction coping strategies. These expectations are grounded in variable-centered work that has linked fewer neighborhood social and economic resources and higher violence to more frequent use of distraction and avoidant coping strategies and less engagement in problem-focused coping and positive cognitive restructuring (Brenner et al. 2013; Kliewer et al. 2004).
Methods
Participants
Participants were predominantly African American youth originally recruited for the Youth Opportunity program in Baltimore, Maryland. Youth Opportunity programs are often located in poorer communities and aim to increase educational, occupational, and training services to adolescents and young adults (Sonenstein et al. 2011). The Youth Opportunity program was administered in two distinct neighborhoods—specifically the east and west sides of Baltimore—though participants could be from any neighborhood in the city, and indeed, came from 49 of Baltimore’s 55 community statistical areas. Inclusion criteria required youth to be between the ages of 16–23 and not be in foster care. Informed consent was obtained from adult participants and parental consent and assent were obtained from youth participants. The study was approved by the Johns Hopkins University School of Medicine Institutional Review Board. A more detailed description of the Youth Opportunity program and study design can be found elsewhere (Sonenstein et al. 2011; Tandon et al. 2014).
Data were collected at 3 time points: baseline (when the study began in 2008), 6 months after baseline, and 1–2 years following the administration of the baseline assessments. For the current study, only baseline data was used which included 782 youth (51.0% female; 93.7% African American; M age = 18.76 years, SD = 1.71). Given the very small percentage of the sample that was non-African American, only African Americans were included in the analyses (N = 733; 51.0% female; M age = 18.75 years, SD = 1.71, range = 16–23). About 27% of the sample were youth (<18 years of age) and approximately 73% of participants were young adults (18–23 years of age). About 60% of the sample participated in one of the Youth Opportunity programs. Approximately 10% of the sample reported being employed. Additional information regarding the analytic sample can be found in Table 1.
Table 1.
Characteristics of the analytic sample
| Characteristic | n (%) |
|---|---|
| Sex | |
| Male | 374 (51.0%) |
| Female | 359 (49.0%) |
| Years of schooling | |
| <9th grade | 98 (13.3%) |
| 9th grade | 188 (25.6%) |
| 10th grade | 174 (23.7%) |
| 11th grade | 143 (19.5%) |
| 12th grade | 98 (13.4%) |
| Beyond high school | 32 (4.4%) |
| General education degree | |
| Yes | 27 (4.5%) |
| No | 576 (95.5%) |
| Employed part- or full-time | |
| Yes | 85 (11.6%) |
| No | 648 (88.4%) |
| Intervention | |
| Yes | 418 (62.1%) |
| No | 255 (37.9%) |
| M (SD) | Range | n | |
|---|---|---|---|
| Age | 18.76 (1.71) | 16–23 | 733 |
| Cohesion | 6.76 (2.35) | 3–12 | 719 |
| Collective efficacy | 10.01 (3.31) | 4–16 | 726 |
| Disorder | 5.48 (4.67) | 0–14 | 556 |
| Violence | 1.37 (1.66) | 0–7 | 713 |
| Disadvantage | 1.90 (2.33) | −8.44–6.13 | 706 |
| Positive restructuring | 31.53 (8.53) | 12–48 | 731 |
| Problem-focused coping | 30.46 (8.57) | 12–48 | 732 |
| Distraction strategies | 20.06 (5.15) | 9–36 | 732 |
| Avoidant strategies | 29.22 (7.03) | 12–48 | 730 |
Participants with missing data (n = 191, 26.1%) differed from participants with complete data (n = 542, 73.9%) in terms of neighborhood social cohesion (t(717) = 2.61, p = 0.009), neighborhood collective efficacy (t(724) = 2.21, p = 0.027), and participant gender (χ2 (1) = 5.13, ϕ = 0.02, p = 0.015). Individuals with missing data were more likely to be male and reported lower levels of cohesion and collective efficacy. No other differences were found between individuals with complete data versus missing data.
Measures
Neighborhood social cohesion and collective efficacy
Neighborhood social cohesion and collective efficacy were assessed using 2 scales developed by Kerrigan et al. (2006). The neighborhood social cohesion scale includes 3 items (α = 0.75)1 rated on a 4-point Likert scale (1 = strongly agree to 4 = strongly disagree). A sample item is “people in my neighborhood are willing to help each other”. The neighborhood collective efficacy scale includes 4 items (α = 0.84) rated on a 4-point Likert scale (1 = very likely to 4 = very unlikely). Participants rated how likely it was that adults in their neighborhood would be willing to step in if children or teenagers were engaging in a number of behaviors, such as showing disrespect to an adult or hanging out in the street. Items were reverse coded and summed, with higher scores reflecting higher levels of social cohesion and collective efficacy. The neighborhood social cohesion and collective efficacy scales have shown adequate reliability and predictive validity (e.g., condom use) (Kerrigan et al. 2006).
Neighborhood disorder and violence
Neighborhood disorder was assessed using a 7-item measure (α = 0.91) developed by Perkins et al. (1992). Participants rated on a 3-point Likert scale (0 = not a problem to 2 = a big problem) whether a number of events were a problem in their neighborhoods, including vandalism, litter, trash in the streets, or people selling drugs. Neighborhood violence was assessed using items drawn from a subscale derived from the Life Events scale (D’Imperio et al. 2000). Participants were asked to report on a 2-point Likert scale (1 = yes, 2 = no) whether a violent event occurred within the neighborhood within the last 12 months. The neighborhood violence subscale includes 8 items (α = 0.74) (e.g., “seen or been around people shooting guns”). For both subscales, items were summed, with higher scores reflecting higher levels of neighborhood violence and disorder. The neighborhood disorder and violence scales have shown adequate reliability, strong correlations with independent observations of the neighborhood, and predictive validity (e.g., internalizing symptoms) (D’Imperio et al. 2000; Latkin and Curry 2003).
Objective neighborhood indicators
Neighborhood disadvantage was derived from 4 census block group level variables that signify material and social deprivation (Hippensteel et al. 2018; Pampalon et al. 2012). An unweighted sum index was computed from the z-scores of low educational attainment, unemployment, poverty, and lone parenthood. These scores were then appended to each participant based on their corresponding block group using the spatial join function in ArcGIS (Pampalon et al. 2012).
The research team included a census-level indicator, specifically community statistical area (CSA) information where each participant lived, to account for the fact that participants are nested within their neighborhoods which may influence their perceptions of the neighborhood environment. CSAs are a commonly-used neighborhood unit in Baltimore, and sociodemographic census data was joined to them in a geographic information system.
Coping behaviors
Coping behaviors were assessed using the Children’s Coping Strategies Checklist-Revision 1 (CCSC-R1) (Ayers et al. 1996). Positive cognitive restructuring (12 items, α = 0.91) includes 3 subscales: positivity (e.g., “you reminded yourself about all the things you have going for you”); control (e.g., “you told yourself you could handle this problem”); and optimism (e.g., “you told yourself it would be okay”). The problem-focused coping scale includes 3 subscales (12 items, α = 0.92), namely: cognitive decision making (e.g., “when you had problems in the past month, you thought about what you could do before doing something”); direct problem solving (e.g., “you did something to make things better”); and seeking understanding (e.g., “you thought about why it happened”). The distraction scale (9 items, α = 0.77) includes 2 subscales: distracting actions (e.g., “you watched television”) and physical release of emotions (e.g., “you did some exercise”). The avoidant scale (12 items, α = 0.83) includes 3 subscales: avoidant actions (“you tried to stay away from things that made you upset”); repression (“you tried to put it out of your mind”); and wishful thinking (“you imaged how you’d like things to be”). Items were rated on a 4-point Likert scale (1 = never to 4 = most of the time) and summed to create composite scores of positive cognitive restructuring, problem-focused coping, avoidant strategies, and distraction strategies. Higher scores reflect higher levels of positive cognitive restructuring, problem-focused coping, distracting actions, and avoidant strategies. These scales have been used in both child and adolescent samples and have shown adequate reliability in previous studies and predictive validity with psychological symptoms (e.g., conduct problems) (Ayers et al. 1996; Sandler et al. 1994). Correlations among the coping variables in the whole sample and the identified profiles (described in more detail below) can be found in the Supplementary Material.
Statistical Analyses
The primary analyses were conducted using Mplus Version 8.0 (Muthén and Muthén 1998–2017). Missing data was handled using Full Information Maximum Likelihood (FIML) estimation (Graham 2009). A latent profile analysis (LPA) was used to identify groups of youth that differ in their perceptions of their neighborhood (i.e., neighborhood social cohesion, collective efficacy, disorder, violence) and reside in neighborhoods of varying disadvantage. Given that youth are nested in neighborhoods and that their geographic location may influence their perceptions of neighborhood functioning, the research team used CSA data to account for participant nesting within their neighborhoods. This was done using the “CLUSTER” command in Mplus.
LPA begins with a one-profile model (“all neighborhoods are the same”), and the number of profiles is increased until there is no additional improvement in model fit (Nylund et al. 2007). Several model fit indices were examined, including the Akaike Information Criterion (AIC) (Akaike 1987), Bayesian Information Criterion (BIC) (Schwartz 1978), and sample-size adjusted BIC (ABIC) (Sclove 1987). The model that generates the smallest values on these fit indices is considered to have the best fit to the data. The Vuong-Lo-Mendell-Rubin Likelihood Ratio Test (VLMR LRT) was also used to evaluate model fit in addition to entropy, a measure of classification certainty which ranges from 0 to 1 (Masyn 2013). The size of the smallest profile was also considered as classes smaller than 5% may indicate model overfitting. The research team also examined whether profiles were distinct and conceptually meaningful.
To test whether the profiles differed on coping behaviors, the BCH method was used (Bolck et al. 2004). This method employs a weighted group analysis that reflects the measurement error of the latent profiles and avoids shifting of classes (Asparouhov and Muthén 2014; Lanza et al. 2014). The first step of the BCH method involves running an LPA that includes the indicators (i.e., neighborhood characteristics) without covariates (i.e., participant sex and age) or dependent variables (coping outcomes). The research team included participant gender and age as covariates in the model given variability in the age range in the sample and the fact that participant age and gender have been previously associated with coping behaviors (Amirkhan and Auyeung 2007; Hampel and Petermann 2006). Given that data were drawn from baseline assessments which occurred before the implementation of the Youth Opportunity program, we did not control for whether or not individuals participated in this program.
In the second step, the covariates and dependent variables are entered in the model, and the BCH weights are saved and used in the next step to ensure that membership in the neighborhood profiles is not influenced by the covariates or dependent variables (Asparouhov and Muthén 2014). The third step involves estimating whether the latent neighborhood profiles are associated with different levels of coping behaviors, while controlling for covariates (i.e., participant sex and age) that might unduly influence latent profile-distal outcome relations. The research team evaluated whether latent profile membership was associated with coping behaviors by evaluating significance of omnibus Wald chi-squared tests. Pairwise comparisons were examined if results from these omnibus tests were statistically significant at the p < 0.05 level.
Results
LPA indicated that the lowest BIC, AIC, and ABIC was associated with the five-profile model. However, in this model, a class emerged that was very similar to another class in terms of violence and disadvantage. Given good entropy and the fact that each class was distinct in the 4-class model, this model was selected for further analyses (see Table 2 for model fit indices).
Table 2.
Fit indices for latent profile analysis models with 1–5 profiles
| Number of profiles | Number of free parameters | Log likelihood | AIC | BIC | ABIC | VLMR LRT (p) | Entropy | Smallest class size n (%) |
|---|---|---|---|---|---|---|---|---|
| 1 | 10 | −5300.45 | 10620.89 | 10666.49 | 10634.73 | - | - | 706 |
| 2 | 18 | −5120.69 | 10277.39 | 10359.46 | 10302.30 | 0.151 | 0.87 | 168 (27.8%) |
| 3 | 24 | −5053.64 | 10155.27 | 10264.70 | 10188.50 | 0.261 | 0.90 | 37 (5.2%) |
| 4 | 28 | −5060.71 | 10177.42 | 10305.09 | 10216.18 | 0.390 | 0.79 | 37 (5.2%) |
| 5 | 34 | −5016.57 | 10101.14 | 10256.17 | 10148.21 | 0.460 | 0.81 | 37 (5.2%) |
VLMR LRT and entropy are not calculated for the 1-profile model. Model highlighted in bold represents the best-fitting model
AIC Akaike Information Criterion, BIC Bayesian Information Criterion, ABIC Sample-size Adjusted BIC, VLMR LRT Vuong Lo-Mendell Rubin Likelihood Ratio Test
Based on the means of the neighborhood characteristics (Fig. 1), Profile 1 (n = 141; 20.0%) was named “highest disorder.” Participants in this class reported low cohesion (~0.50 SD below the sample M), average collective efficacy (around sample M), the highest disorder (~1.00 SD above the sample M), low violence (~0.50 SD below the sample M), and resided in areas characterized by very high disadvantage (~2.50 SD below the sample M). The second profile (n = 37; 5.2%) was named “highest violence, highest disadvantage” and was characterized by low cohesion (~0.50 SD below the sample M), average collective efficacy (around the sample M), high disorder (~0.50 SD above sample M), and the highest levels of violence and disadvantage in the sample (~2.50 SD above the sample M). Profile 3 (n = 188, 26.6%) was named “high violence” as this subgroup was characterized by average cohesion and collective efficacy (around the sample M), slightly above average disorder (~0.25 SD above the sample M), and high violence and disadvantage (~1.00 SD above sample M). The fourth profile (n = 348, 47.5%) was named “highest cohesion/lowest disorder” and was marked by the highest cohesion in the sample (~0.25 SD above the sample M), average collective efficacy (around the sample mean), high disadvantage (~1.50 SD above sample M), low violence (~0.50 SD below the sample M), and the lowest disorder (~0.50 SD below the mean).
Fig. 1.
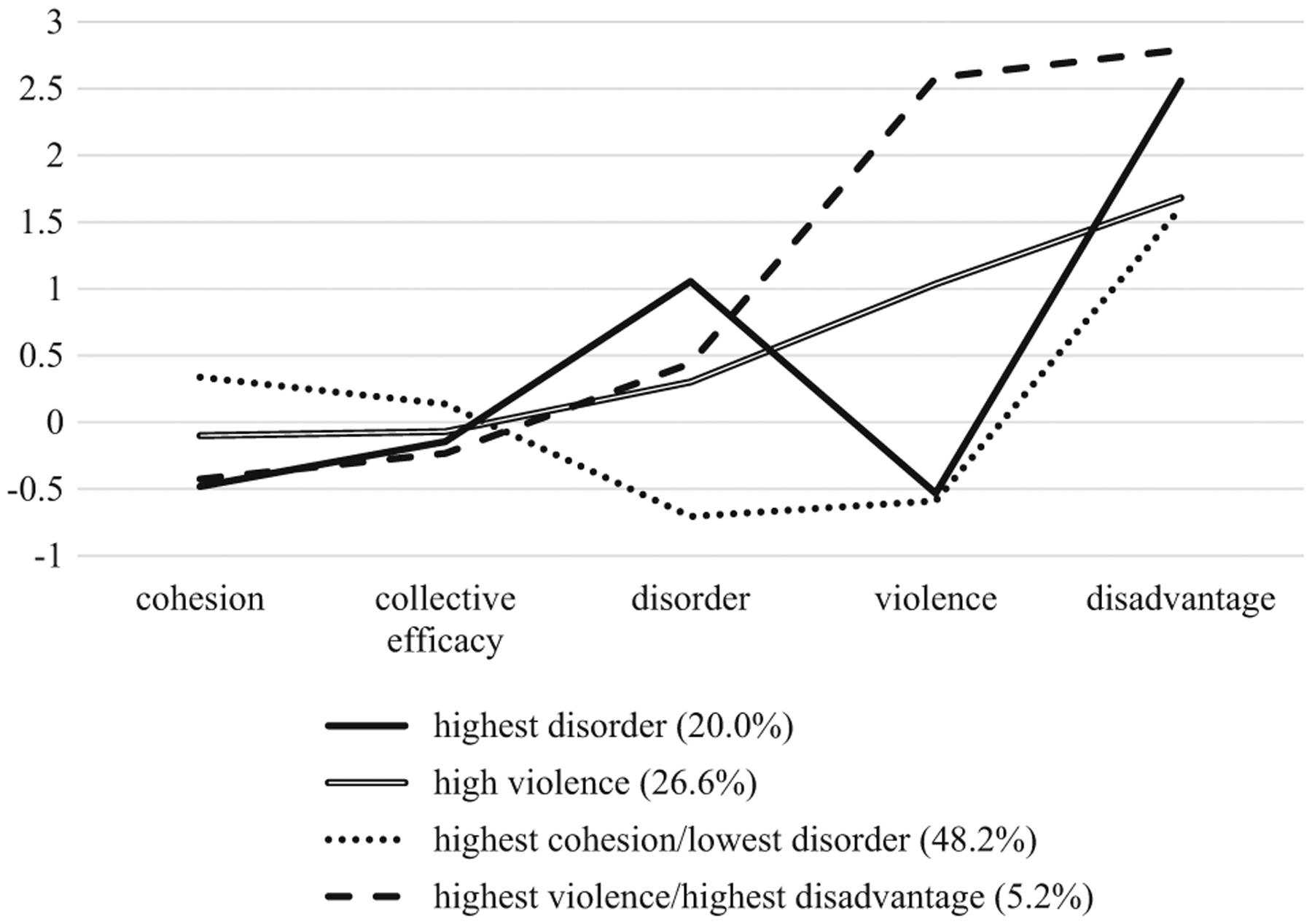
Standardized neighborhood characteristics in the 4-class model
As shown in Table 3, between profile differences were found with regard to positive cognitive restructuring (χ2 = 15.26, p = 0.002) and problem-focused coping (χ2 = 8.06, p = 0.045). The highest violence/highest disadvantage profile reported higher levels of positive cognitive restructuring compared to the highest disorder profile (z = 3.75, p < 0.005), high violence profile (z = 2.20, p = 0.028), and highest cohesion/lowest disorder profile (z = 3.00, p = 0.003) (see Table 4 for profile means and standard deviations of the coping variables). The high violence profile also reported higher levels of positive cognitive restructuring compared to the highest disorder profile (z = 2.31, p = 0.021). No differences were found between the (a) highest disorder and the highest cohesion/lowest disorder profile (z = 1.39, p = 0.166) or between the (b) high violence and the highest cohesion/lowest disorder profile (z = 1.04, p = 0.300).
Table 3.
Summary of wald tests and pairwise comparisons for coping behaviors
| Variable | Omnibus χ2 test | Pairwise comparisons | |
|---|---|---|---|
| χ2 | p-value | ||
| Positive cognitive restructuring | 15.26 | 0.002 | 4> 1, 2, 3; 2> 1 |
| Problem focused coping | 8.06 | 0.045 | 4 > 1, 2, 3 |
| Distracting actions | 4.27 | 0.234 | - |
| Avoidant actions | 7.44 | 0.059 | - |
Profile 1 = highest disorder; Profile 2 = high violence; Profile 3 = highest cohesion/lowest disorder; Profile 4 = highest violence/highest disadvantage
Table 4.
Means and standard deviations of coping variables based on profile membership
| Profile | Positive cognitive restructuring | Problem-focused coping | Avoidant strategies | Distraction strategies |
|---|---|---|---|---|
| Highest disorder | 31.48 (12.21) | 30.04 (11.11) | 29.49 (6.85) | 20.16 (6.10) |
| High violence | 32.66 (8.24) | 31.71 (9.80) | 30.98 (5.83) | 22.28 (4.76) |
| Highest cohesion/lowest disorder | 30.84 (11.38) | 29.79 (11.65) | 27.90 (8.24) | 19.22 (5.68) |
| Highest violence/highest disadvantage | 34.06 (7.44) | 34.03 (9.07) | 32.48 (7.18) | 22.28 (7.88) |
Regarding problem-focused coping, the highest violence/highest disadvantage profile reported higher levels of problem-focused coping than the (a) high disorder profile (z = 2.76, p = 0.006), (b) high violence profile (z = 1.97, p = 0.048), and the (c) highest cohesion/lowest disorder profile (z = 2.17, p = 0.030). There were no differences between the high disorder and the high violence profile (z = 1.21, p = 0.226), and the high disorder profile and the highest cohesion/lowest disorder profile (z = 0.84, p = 0.402). There were also no differences between the high violence profile and highest cohesion/lowest disorder profile (z = 0.43, p = 0.665). No between-profile differences were found with regard to avoidant coping (χ2 = 7.44, p = 0.059) or distraction coping (χ2 = 4.27, p = 0.234).
Discussion
Long-standing neighborhood and social ecological theories of development acknowledge the role of the neighborhood as a critical contextual factor that can affect how youth cope with daily life events and stressors. While a number of studies have focused on single neighborhood characteristics in relation to youth’s coping behaviors (e.g., Brenner et al. 2013; Kliewer et al. 2004), a dearth of work has considered whether the clustering of neighborhood characteristics is associated with youth’s coping strategies. Identifying profiles of neighborhood functioning may increase awareness of the ecological environments that youth occupy and elucidate how these contexts are associated with how youth approach and navigate stressful experiences. Accordingly, the present study sought to (a) identify profiles of inner-city young people that exhibited different perceptions of their neighborhoods and experienced different levels of neighborhood disadvantage and (b) explore whether these profiles were linked with different coping behaviors.
Four neighborhood profiles were identified. There was a highly disordered subgroup that reported low levels of cohesion, collective efficacy and violence; resided in highly disadvantaged areas, and reported the highest levels of disorder in the sample. A very high violence and very high disadvantaged subgroup was also observed which was characterized by low cohesion and collective efficacy, high disorder, and reported the highest levels of violence and disadvantage. The third profile was coined high violence as this subgroup was characterized by average cohesion, collective efficacy, and disorder; high disadvantage, and high violence. The fourth profile was named highest cohesion/lowest disorder and was marked by average collective efficacy, high disadvantage, low violence, and participants reported the highest cohesion and lowest disorder in the sample. Although these subgroups for the most part mimic those identified by Dupéré and Perkins (2007), additional subgroups were observed in the current sample, including profiles characterized by high to very high levels of neighborhood violence and disadvantage, and high disorder. Despite the fact that the sample investigated by Dupéré and Perkins (2007) included participants that lived in Baltimore neighborhoods like the current study sample, the differences in subgroups observed may be due to differences in the (a) indicators used in the analyses (e.g., self-reported violence; objective disadvantage), (b) demographic makeup of the samples, and (c) time period during which the neighborhood was assessed. Participants in the current study were African American adolescents and young adults, while Dupéré and Perkins (2007) included a more racially heterogenous sample of older adults who reported on their neighborhoods nearly 2 decades before the current study was implemented. These findings demonstrate the importance of studying neighborhoods over time given changes in neighborhood environments that often occur, and of considering perspectives from individuals across developmental periods and racial and socio-economic backgrounds.
In terms of the most salient findings, the profiles observed differed in coping behaviors such that youth in the highest violence and disadvantaged subgroup reported higher levels of positive cognitive restructuring and problem-focused coping compared to the other profiles. The high violence subgroup also reported higher levels of positive cognitive restructuring than the highest cohesion/lowest disorder subgroup, inconsistent with expectations. In line with the John Henryism phenomenon, youth experiencing significant psychosocial stressors and violence may engage in active coping mechanisms as a means to survive and thrive in an unpredictable setting (Bennett et al. 2004). It is possible that youth who witness frequent community violence and that live in very disadvantaged neighborhoods characterized by unemployment and poverty may become desensitized to their surroundings and be less affected by these experiences. Consistent with adaptation models of development and stress inoculation theories, regular exposure to violence and disadvantage may provide the opportunity for youth to develop emotion and regulatory coping skills that facilitate adaptation to these stressors and other life events (Epstein 1983; Ng-Mak et al. 2004). This idea is supported by some work indicating that higher levels of community violence is associated with lower levels of emotional distress among urban youth (Ng-Mak et al. 2004). Youth who reported the highest levels of violence and that resided in very disadvantaged areas may have also learned that thinking about the positive things in their lives and attempting to actively solve their problems allows them to persist in the face of adversities.
Another potential explanation for these findings is that youth may have highly supportive relationships with peers, mentors, or adults in more violent and disadvantaged neighborhoods, which may influence how youth think about and approach challenges. In line with positive developmental frameworks, youth may possess internal assets (i.e., talents, skills) and external resources (e.g., family members) that influence the expression of optimal functioning (Gaylord-Harden et al. 2018). Research has shown that youth that have at least one supportive relationship (e.g., with parents or adults) are more likely to feel connected, more confident in the decisions they make, and less likely to engage in high-risk behaviors (Gambone et al. 2002). Thus, it is possible that supportive positive relationships buffer the deleterious impacts of disadvantage and violence on youth and enable youth to develop coping behaviors characterized by positive cognitive reframing and problem solving. Future research is needed to understand individual and environmental factors that influenced why youth in the most violent and disadvantaged communities evidenced higher levels of positive cognitive restructuring and problem solving relative to their peers. Such information can be used to leverage and inform interventions aimed at bolstering the coping behaviors among youth who respond maladaptively to stressors.
The finding that youth across the profiles resided in highly disadvantaged areas and reported low to average levels of neighborhood social cohesion and collective efficacy highlights that high levels of poverty, lower levels of resident attachment to one another, and minimal informal monitoring of youth are pervasive problems across Baltimore. Given that social cohesion and informal surveillance of youth may reduce crime and health-compromising behaviors among young people, neighborhood-level interventions should attempt to build positive relationships among residents and establish a consensus regarding appropriate norms for youth behavior. Such an approach may help reduce crime, strengthen community ties, and promote youth’s well-being. Moreover, neighborhood programs should focus on providing educational and occupational services, in addition to social and economic support to residents across Baltimore neighborhoods, to help reduce the level of disadvantage in these settings. Other planning-related interventions that have been known to increase these social goals could include community beautification and greening programs (Sadler et al. 2017), redevelopment in the form of mixed-income housing (MacGregor 2010), or improved urban design and permeable urban form (Anderson and Baldwin 2017). Many of these tenets reflect the central philosophy of New Urbanism, and could be adopted by communities to achieve goals such as those listed above (Talen 2002).
Some limitations of the study require acknowledgement. Data were drawn from Baltimore City, a metropolitan region with one of the highest crime rates in this country. Thus, it is unclear whether the neighborhood profiles identified would be observed in, for instance, rural communities or other urban areas. In addition, the study sample included only African American adolescents. Future work should investigate whether the neighborhood profile-coping associations observed in the current study are generalizable to individuals of other racial and ethnic backgrounds. In addition, data were drawn from a single time point; thus, causal relationships between neighborhood profile membership and coping behaviors cannot be concluded. Last, future work should consider incorporating different neighborhood indicators (e.g., number of parks/green spaces) and analyzing the neighborhood variables under investigation using different methods (e.g., hierarchical linear modeling, multi-level modeling) to examine whether findings from the current study are replicated.
Conclusion
Neighborhoods are complex ecological systems that can have a tremendous impact in shaping access to opportunities and the extent to which youth thrive or flounder in the face of adversity. While most researchers have approached studying the neighborhood by examining neighborhood processes in isolation, there is reason to believe that perceptions of neighborhood characteristics influence each other and are shaped by objective neighborhood characteristics. To better capture the intricate nature of the neighborhood environment on youth’s coping, neighborhood-level processes were modeled concurrently (through latent profile analysis) and examined in relation to youth’s reported coping strategies. The most salient finding was that youth in the most disadvantaged and violent communities reported higher levels of positive cognitive restructuring and problem solving. Late adolescents and emerging adults often experience a number of changes and transitions and developing the ability to respond appropriately to these experiences is critical for successful adaptation. Thus, identifying individual-specific and external assets that contribute to engagement in adaptive coping strategies among seemingly the most vulnerable youth is warranted. Such work may guide ecological-transactional models of development and have the potential to inform research and practice aimed at fostering resilience among at-risk adolescents and young adults.
Supplementary Material
Acknowledgements
We thank all study participants, in addition to D.T., the principal investigator of the current project.
Funding
Funding for the implementation of the Healthy Minds at Work intervention came from the Robert Wood Johnson Foundation, the Jacob and Hilda Blaustein Foundation, The Abell Foundation, the Leonard and Helen R. Stulman Foundation, The Annie E. Casey Foundation, Aaron Straus and Lillie Straus Foundation, and the France-Merrick Foundation. The research portion of Healthy Minds at Work was developed as the core research project of the Johns Hopkins Center for Adolescent Health, a prevention research center funded by the Centers for Disease Control and Prevention (grant no. 1-U48-DP-000040).
Biography
Jill A. Rabinowitz is an assistant scientist at Johns Hopkins Bloomberg School of Public Health in the Department of Mental Health. Her work involves examining the interplay between micro- and macro- early childhood environments and genetic variants that are associated with children’s development and long-term health, with a particular interest in examining these relationships among diverse populations. Ultimately, her work aims to elucidate the joint contributions of early childhood exposures and genetics to inform translational efforts and interventions aimed at improving children’s mental and physical health.
Terrinieka Powell is an associate professor at Johns Hopkins Bloomberg School of Public Health in the Department of Population, Family and Reproductive Health. She has expertise in adolescent health, qualitative methods, community-engaged approaches to research, as well as intervention development and implementation science. She is trained as a Community Psychologist committed to improving adolescent health outcomes through partnerships with churches, schools, families, health departments and community-based organizations. Her current and past grant research and funding demonstrate her persistent attempts to seek and secure support for her research and enhances her ability to improve the lives of vulnerable young people.
Richard Sadler is an assistant professor in the Division of Public Health at Michigan State University in Flint. A geographer by training, his work explores the connections between the built environment and health behaviors/outcomes. The central goal of his work is to uncover the ‘invisible patterns’ in our urban landscapes to guide better evidence-based practices in land use, urban, and social policy.
Beth Reboussin is a biostatistician in the School of Medicine at Wake Forest University whose research focuses on the development and application of latent class methods to understand the processes underlying youth and young adult substance use.
Kerry Green is an associate professor in the School of Public Health at the University of Maryland. Her work is focused on improving the health and well-being of disadvantaged populations. Much of her research involves identifying risk and protective factors over the life course for urban African Americans. Dr. Green’s work is concentrated in two main areas: (1) long-term consequences of substance use and (2) the interrelationship of substance use, violence, and mental health over the life course.
Adam Milam has expertise in spatial and hierarchical methods. His research interests include the impact of neighborhood environment on children and adolescent exposure to alcohol, tobacco, and other drugs. Dr. Milam’s research also focuses on policy interventions to reduce child and adolescent exposure and use of alcohol, tobacco, and marijuana.
Mieka Smart is an assistant professor in the College of Human Medicine at Michigan State University. Her research interests include the prevention of mental illness and using systematic observations to monitor and evaluate public health policy interventions. She uses spatial and time series data analysis methods to understand the predictors and correlate of drug and alcohol problems.
Debra Furr-Holden is an Associate Dean for Public Health Integration and Director of the Flint Center for Health Equity Solutions. Her work is focused on behavioral health equity and policy-level interventions to promote health equity. My action-oriented research is embedded with the principles and practices of Community-Based Participatory Research (CBPR).
Amanda Latimore is an associate scientist at Johns Hopkins Bloomberg School of Public Health in the Department of Epidemiology. Her work focuses on community-informed applications of social epidemiology in and out of the classroom. Her role as the Bloomberg American Health Initiative Public Sector Initiatives Lead is to support and facilitate the bridge between academia and public service agencies and provide technical assistance for local and state agency-led health initiatives.
Darius Tandon is an associate professor in Feinberg School of Medicine at Northwestern University. His research interests focus on the prevention of mental disorders and promotion of positive well-being among vulnerable populations. He has conducted intervention studies with adolescents and young adults as well as perinatal populations.
Footnotes
Data Sharing and Declaration This manuscript’s data will not be deposited. However, data from the current study can be obtained from the Principal Investigator, D.T.
Conflict of Interest The authors declare that they have no conflict of interest.
Ethical Approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional review board at the Johns Hopkins School of Public Health (IRB #NA 00021362) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent Informed consent was obtained from all individual participants included in the study.
Supplementary information The online version of this article (https://doi.org/10.1007/s10964-019-01176-y) contains supplementary material, which is available to authorized users.
All alphas reported were calculated based on the current study sample.
References
- Akaike H (1987). Factor analysis and AIC. Psychometrika, 52, 317–332. [Google Scholar]
- Amirkhan J, & Auyeung B (2007). Coping with stress across the lifespan: absolute vs. relative changes in strategy. Journal of Applied Developmental Psychology, 28, 298–317. 10.1016/j.appdev.2007.04.002. [DOI] [Google Scholar]
- Anderson J, & Baldwin C (2017). Building well-being: Neighbourhood flourishing and approaches for participatory urban design intervention. In Phillips R & Wong C (Eds), Handbook of community well-being research (pp. 313–337). Dordrecht: Springer. [Google Scholar]
- Asparouhov T, & Muthén B (2014). Auxiliary variables in mixture modeling: using the BCH method in mplus to estimate a distal outcome model and an arbitrary secondary model. Mplus Web-notes: No. 21, 1–22. [Google Scholar]
- Ayers TS, Sandier IN, West SG, & Roosa MW (1996). A dispositional and situational assessment of children’s coping: testing alternative models of coping. Journal of Personality, 64(4), 923–958. [DOI] [PubMed] [Google Scholar]
- Bennett GG, Merritt MM, Sollers JJ III, Edwards CL, Whitfield KE, Brandon DT, & Tucker RD (2004). Stress, coping, and health outcomes among African-Americans: a review of the John Henryism hypothesis. Psychology and Health, 19(3), 617–632. 10.1080/0887044042000193505. [DOI] [Google Scholar]
- Boardman JD (2004). Stress and physical health: the role of neighborhoods as mediating and moderating mechanisms. Social Science & Medicine, 58, 2473–2483. 10.1016/j.socscimed.2003.09.029. [DOI] [PubMed] [Google Scholar]
- Bolck A, Croon M, & Hagenaars J (2004). Estimating latent structure models with categorical variables: one-step versus three-step estimators. Political Analysis, 12, 3–27. 10.1093/pan/mph001. [DOI] [Google Scholar]
- Booth JM, Teixeira S, Zuberi A, & Wallace JM (2018). Barrios, ghettos, and residential racial composition: examining the racial makeup of neighborhood profiles and their relationship to self-rated health. Social Science Research, 69, 19–33. 10.1016/j.ssresearch.2017.10.002. [DOI] [PubMed] [Google Scholar]
- Boxer P, Sheffield AS, Terranova AM, Kithakye M, Savoy SC, & Mcfaul AF (2008). Coping with exposure to violence: relations to emotional symptoms and aggression in three urban samples. Journal of Child and Family Studies, 17, 881–893. 10.1007/s10826-008-9196-z. [DOI] [Google Scholar]
- Boxer P, & Sloan-Power E (2013). Coping with violence: a comprehensive framework and implications for understanding resilience. Trauma, Violence, & Abuse, 14, 209–221. 10.1177/1524838013487806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brenner AB, Zimmerman MA, Bauermeister JA, & Caldwell CH (2013). Neighborhood context and perceptions of stress over time: an ecological model of neighborhood stressors and intrapersonal and interpersonal resources. American Journal of Community Psychology, 51, 544–556. 10.1007/s10464-013-9571-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Browning CR, Soller B, Gardner M, & Brooks-Gunn J (2013). “Feeling disorder” as a comparative and contingent process: gender, neighborhood conditions, and adolescent mental health. Child and Adolescent Health and Well-Being, 54, 296–314. 10.1177/0022146513498510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Browning CR, Soller B, & Jackson AL (2015). Neighborhoods and adolescent health-risk behavior: an ecological network approach. Social Science & Medicine, 125, 163–172. 10.1016/j.socscimed.2014.06.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicognani E (2011). Coping strategies with minor stressors in adolescence: relationships with social support, self-efficacy, and psychological well-being. Journal of Applied Social Psychology, 41, 559–578. 10.1111/j.1559-1816.2011.00726.x. [DOI] [Google Scholar]
- Compas BE, Connor-Smith JK, Saltzman H, Thomsen AH, & Wadsworth ME (2001). Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychological Bulletin, 127, 87–127. 10.1037//0033-2909.127.1.87. [DOI] [PubMed] [Google Scholar]
- D’Imperio RL, Dubow EF, & Ippolito MF (2000). Resilient and stress-affected adolescents in an urban setting. Journal of Clinical Child Psychology, 29, 129–142. [DOI] [PubMed] [Google Scholar]
- Drabick DAG, & Steinberg L (2011). Developmental psycho-pathology. In: Brown BB, Prinstein MJ, (Eds) Encyclopedia of adolescence. (Vol. 3). (pp. 136–142). San Diego, CA, USA: Academic Press. [Google Scholar]
- Dubow EF, Edwards S, & Ippolito MF (1997). Life stressors, neighborhood disadvantage, and resources: a focus on inner-city children’s adjustment. Journal of Clinical Child Psychology, 26, 130–144. [DOI] [PubMed] [Google Scholar]
- Dupéré V, & Perkins DD (2007). Community types and mental health: a multilevel study of local environmental stress and coping. American Journal of Community Psychology, 39, 107–119. 10.1007/s10464-007-9099-y. [DOI] [PubMed] [Google Scholar]
- Epstein S (1983). Natural healing process of the mind: graded stress innoculation as an inherent coping mechanism. In M. D & Y. M (Eds), Stress reduction and prevention (pp. 39–66). New York, NY, US: Plenum Press. [Google Scholar]
- Gambone MA, Klem AM, & Connell JP (2002). Finding out what matters for youth: testing key links in a community action framework for youth development. Philadelphia: Youth Development Strategies, Inc., and Institute for Research and Reform in Education. [Google Scholar]
- Gaylord-Harden NK, Barbarin O, Tolan PH, & Murry VMB (2018). Understanding development of African American boys and young men: moving from risks to positive youth development. American Psychologist, 73, 753–767. 10.1037/amp0000300. [DOI] [PubMed] [Google Scholar]
- Graham JW (2009). Missing data analysis: making it work in the real world. Annual Review of Psychology, 60(1), 549–576. 10.1146/annurev.psych.58.110405.085530. [DOI] [PubMed] [Google Scholar]
- Hampel P, & Petermann F (2006). Perceived stress, coping, and adjustment in adolescents. Journal of Adolescent Health, 38, 409–415. 10.1016/j.jadohealth.2005.02.014. [DOI] [PubMed] [Google Scholar]
- Hippensteel CL, Sadler RC, Milam AJ, Nelson V, & Furr-Holden CD (2018). Using zoning as a public health tool to reduce oversaturation of alcohol outlets: an examination of the effects of the new “300 foot rule” on packaged goods stores in a mid-Atlantic city. Prevention Science, 20, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kerrigan D, Witt S, Glass B, Chung S, & Ellen J (2006). Perceived neighborhood social cohesion and condom use among adolescents vulnerable to HIV/STI. AIDS and Behavior, 10, 723–729. 10.1007/s10461-006-9075-9. [DOI] [PubMed] [Google Scholar]
- Kingston B, Huizinga D, & Elliott DS (2009). A test of social disorganization theory in high-risk neighborhoods. Youth and Society, 41, 53–79. 10.1126/science.62.1605.0xii-s. [DOI] [Google Scholar]
- Kliewer W, Cunningham JN, Diehl R, Parrish KA, Walker JA, Atiyeh C, & Mejia R (2004). Violence exposure and adjustment in inner-city youth: child and caregiver emotion regulation skill, caregiver-child relationship quality, and neighborhood cohesion as protective factors. Journal of Clinical Child and Adolescent Psychology, 33, 477–487. [DOI] [PubMed] [Google Scholar]
- Lanza ST, Tan X, & Bray BC (2014). A latent class analysis with distal outcomes: a flexible model-based approach. Structural Equation Modeling: A Multidisciplinary Approach, 20, 1–26. 10.1080/10705511.2013.742377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Latkin CA, & Curry AD (2003). Stressful neighborhoods and depression: a prospective study of the impact of neighborhood disorder. Journal of Health and Social Behavior, 44, 34–44. [PubMed] [Google Scholar]
- Leventhal T, & Brooks-Gunn J (2000). The neighbourhoods they live in: the effects of neighbourhood resilience on child and adolescent outcomes. Psychological Bulletin, 126, 309–337. 10.1037//0033-2909.126.2.309. [DOI] [PubMed] [Google Scholar]
- MacGregor C (2010). Urban regeneration as a public health intervention. Journal of Social Intervention: Theory and Practice, 19, 38. 10.18352/jsi.225. [DOI] [Google Scholar]
- Markowitz FE, Bellair PE, Liska AE, & Liu J (2001). Extending social disorganization theory: modeling the relationships between cohesion, disorder, and fear. Criminology, 39, 293–319. 10.1111/j.1745-9125.2001.tb00924.x. [DOI] [Google Scholar]
- Masyn K (2013). Latent class analysis and finite mixture model. In Little TD (Ed.), The Oxford handbook of quantitative methods, Vol. 2: Statistical Analysis. New York, NY, US: Oxford University Press. [Google Scholar]
- Muthén LK, & Muthén BO (1998–2017). Mplus user’s guide. Eighth Edn Los Angeles, CA, US: Muthén & Muthén. [Google Scholar]
- Ng-Mak DS, Salzinger S, Feldman RS, & Stueve CA (2004). Pathologic adaptation to community violence among inner-city youth. American Journal of Orthopsychiatry, 74, 196–208. 10.1037/0002-9432.74.2.196. [DOI] [PubMed] [Google Scholar]
- Nylund KL, Asparouhov T, & Muthén BO (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Structural Equation Modeling, 14(4), 535–569. 10.1080/10705510701575396. [DOI] [Google Scholar]
- Pampalon R, Hamel D, Gamache P, Philibert MD, Simpson A, October S, & Simpson A (2012). An area-based material and social deprivation Iidex for public health in Québec and Canada. Canadian Journal of Public Health, 103, S17–S22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perkins DD, Meeks JW, & Taylor RB (1992). The physical environment of street blocks and resident perceptions of crime and disorder: Implications for theory and adjustment. Journal of Environmental Psychology, 12, 21–34. [Google Scholar]
- Ross CE, & Mirowsky J (2001). Neighborhood disadvantage, disorder, and health. Journal of Health and Social Behavior, 42, 258–276. [PubMed] [Google Scholar]
- Sadler RC, Pizarro J, Turchan B, Gasteyer SP, & McGarrell EF (2017). Exploring the spatial-temporal relationships between a community greening program and neighborhood rates of crime. Applied Geography, 83, 13–26. 10.1016/j.apgeog.2017.03.017. [DOI] [Google Scholar]
- Sampson RJ, Morenoff JD, & Gannon-Rowley T (2002). Assessing “neighborhood effects”: social processes and new directions in research. Annual Review of Psychology, 28, 443–478. 10.1146/annurev.soc.28.110601.141114. [DOI] [Google Scholar]
- Sampson RJ, Raudenbush SW, Earls F, Sampson RJ, Raudenbush SW, & Earls F (1997). Neighborhoods and violent crime: a multilevel study of collective efficacy. Science, 277, 918–924. [DOI] [PubMed] [Google Scholar]
- Sandler IN, Tein J, & West SG (1994). Coping, stress, and the psychological symptoms of children of divorce: a cross-sectional and longitudinal study. Child Development, 65(6), 1744. 10.2307/1131291. [DOI] [PubMed] [Google Scholar]
- Schwartz G (1978). Estimating the dimension of a model. Annals of Statistics, 6, 461–464. [Google Scholar]
- Sclove SL (1987). Application of model-selection criteria to some problems in multivariate analysis. Psychometrika, 52, 333–343. [Google Scholar]
- Sonenstein FL, Marshall BD, & Tandon D (2011). Employment and training programs: a context for reaching out of school youth with mental health and other health programs. Adolescent Medicine: State of the Art Reviews (AM: STARS), 22(3), 441–457. [PMC free article] [PubMed] [Google Scholar]
- Talen E (2002). The social goals of new urbanism. Housing Policy Debate, 13(1), 165–188. 10.1080/10511482.2002.9521438. [DOI] [Google Scholar]
- Tandon SD, Latimore AD, Clay E, Mitchell L, Tucker M, & Sonenstein FL (2014). Depression outcomes associated with an intervention implemented in employment training programs for low-income adolescents and young adults. JAMA Psychiatry, 72, 31–39. 10.1001/jamapsychiatry.2014.2022. [DOI] [PubMed] [Google Scholar]
- Wadsworth ME, & Berger LE (2011). Adolescents coping with poverty-related family stress: prospective predictors of coping and psychological symptoms. Journal of Youth and Adolescence, 35, 57–70. 10.1007/s10964-005-9022-5. [DOI] [Google Scholar]
- Witherspoon D, & Ennett S (2011). An examination of social disorganization and pluralistic neighborhood theories with rural mothers and their adolescents. Journal of Youth and Adolescence, 40, 1243–1253. 10.1007/s10964-009-9499-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.