

Abstract
Accurate echocardiographic evaluation of the systemic right ventricle is challenging because of its specific morphology and contraction patterns. We present a detailed multimodality assessment of the systemic right ventricle, analyze the relative contribution of the longitudinal, radial, and anteroposterior components of systolic function, and identify reasons for a potential discrepancy among imaging modalities. (Level of Difficulty: Intermediate.)
Key Words: echocardiography, cardiac magnetic resonance, right ventricle, transposition of the great arteries, 3-dimensional imaging
Abbreviations and Acronyms: CMR, cardiovascular magnetic resonance; EF, ejection fraction; FAC, fractional area change; SRV, systemic right ventricle or ventricular; TAPSE, tricuspid annular plane systolic excursion; 2DE, 2-dimensional echocardiography; 3DE, 3-dimensional echocardiography
Central Illustration
Case Description
A 30-year-old asymptomatic woman with transposition of the great arteries and a previous Mustard repair presented for follow-up. Findings on 2-dimensional echocardiography (2DE) demonstrated a severely dilated systemic right ventricle (SRV), markedly abnormal septal motion with the interventricular septum bulging toward the left in systole, and severe systolic dysfunction (Figures 1A to 1C, Video 1).
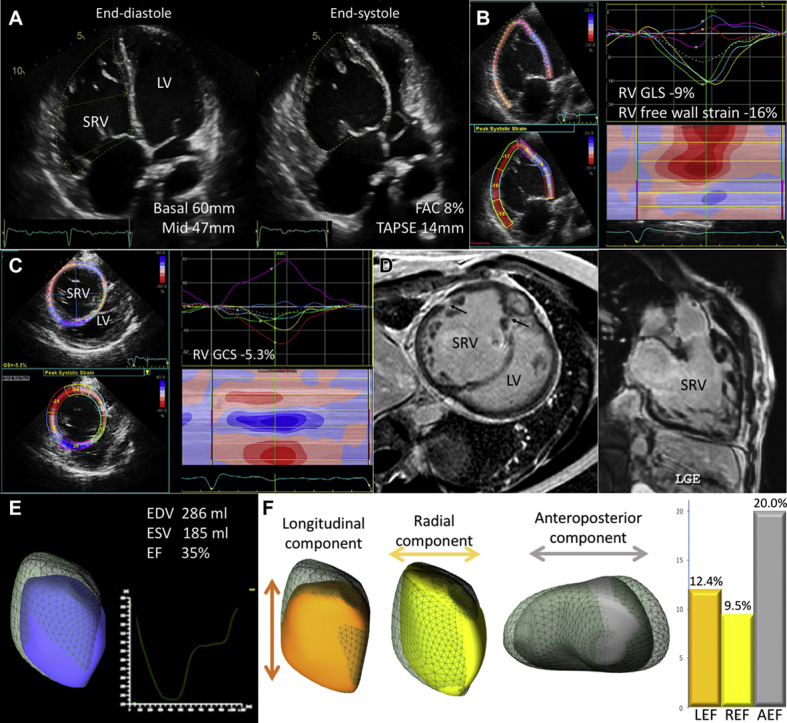
Figure 1.

Assessment of SRV Systolic Function
(A) 2-dimensional echocardiographic apical 4-chamber view. (B) 2-dimensional echocardiographic speckle tracking longitudinal strain showing severely reduced global strain partially contributed to by the stretched septal segments (dark blue and red curves). (C) 2-dimensional echocardiographic speckle tracking circumferential strain demonstrating a dominant contribution of the anterior and anterolateral segments (light blue, yellow, and red curves) and abnormal septal motion (purple curve). (D) Cardiac magnetic resonance demonstrating limited areas of fibrosis (arrows). (E) 3-dimensional echocardiographic volumetric analysis. (F) The ReVISION method analysis (Argus Cognitive, Lebanon, New Hampshire). AEF = anteroposterior ejection fraction; EDV = end-diastolic volume; EF = ejection fraction; ESV = end-systolic volume; FAC = fractional area change; GCS = global circumferential strain; GLS = global longitudinal strain; LEF = longitudinal ejection fraction; LGE = late gadolinium enhancement; LV = left ventricle; REF = radial ejection fraction; RV = right ventricular; SRV = systemic right ventricle; TAPSE = tricuspid annular plane systolic excursion.
Despite concerning 2DE findings, other test results were reassuring:
-
•
During bicycle stress echocardiography, the patient exercised for 8:35 min on the World Health Organization protocol with an adequate hemodynamic response, reaching 90% of maximum heart rate. She remained asymptomatic, with no electrocardiographic changes and SRV systolic function visually improving at peak.
-
•
Cardiac magnetic resonance (CMR) showed an SRV end-diastolic volume of 275 ml and an ejection fraction (EF) of 40%. Late gadolinium enhancement suggested only mild fibrosis in a small area of free wall and septal insertion point (Figure 1D).
-
•
Right-sided heart catheterization demonstrated normal pulmonary artery pressures (26, 8, and 16 mm Hg) and normal end-diastolic pressure (5 mm Hg).
-
•
B-type natriuretic peptide level was 72 ng/l.
-
•
3-dimensional echocardiography (3DE) demonstrated an SRV end-diastolic volume of 286 ml and an EF of 35% (Figure 1E).
To analyze the reasons for significant underestimation of SRV systolic function by 2DE (e.g., fractional area change [FAC] 8%) versus other tests (CMR EF 40%, 3DE EF 35%, good exercise test results, and B-type natriuretic peptide level), we performed the advanced 3DE analysis using the ReVISION software (Argus Cognitive, Lebanon, New Hampshire) and aiming to quantify the contribution of the longitudinal, radial, and anteroposterior components of the SRV wall motion separately. A 3DE mesh model of the SRV was decomposed along 3 directions providing longitudinal, radial, and anteroposterior EF (Figure 1F). The relative contribution of the anteroposterior component was dominant (20.0%) compared with longitudinal (12.4%) and radial (9.5%) components. These results suggest that shortening in the anteroposterior direction caused by the circumferentially oriented myofibers provided partial compensation for impaired longitudinal (post–cardiac surgery) and radial components (secondary to abnormal septal motion resulting from the pressure difference between the ventricles).
During 2-year follow-up, the patient remained asymptomatic and had a successful pregnancy.
Given that SRV dysfunction is a key factor associated with morbidity and mortality, the accurate evaluation of SRV performance is crucial (1). Accuracy of conventional echocardiographic parameters is suboptimal: neither tricuspid annular plane systolic excursion (TAPSE) nor S′ correlated with CMR-derived SRV EF, whereas FAC showed only moderate correlation (2). Conversely, 3DE provides more granular understanding of the role of different components of the SRV systolic function (3). Importantly, FAC, TAPSE, and longitudinal strain do not take into account anteroposterior contraction, thus leading to underestimation of SRV systolic function by these parameters. SRV systolic function is more accurately assessed by 3DE and CMR. Our results highlight the importance of 3DE imaging in the thorough assessment of SRV systolic function.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Footnotes
The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the Author Center.
Appendix
For a supplemental video, please see the online version of this article.
Appendix
2-Dimensional Echocardiographic Apical 4-Chamber View in a Patient With Transposition of the Great Arteries Post-Atrial Switch Operation The systemic right ventricle is significantly dilated with abnormal motion of the interventricular septum bulging toward the left ventricle in systole.
References
- 1.Kalogeropoulos A.P., Deka A., Border W. Right ventricular function with standard and speckle-tracking echocardiography and clinical events in adults with D-transposition of the great arteries post atrial switch. J Am Soc Echocardiogr. 2012;25:304–312. doi: 10.1016/j.echo.2011.12.003. [DOI] [PubMed] [Google Scholar]
- 2.Schneider M., Beichl M., Nietsche C. Systematic evaluation of systemic right ventricular function. J Clin Med. 2019;9:107. doi: 10.3390/jcm9010107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lakatos B.K., Nabeshima Y., Tokodi M. Importance of nonlongitudinal motion components in right ventricular function: three-dimensional echocardiographic study in healthy volunteers. J Am Soc Echocardiogr. 2020;33:995–1005.e1. doi: 10.1016/j.echo.2020.04.002. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
2-Dimensional Echocardiographic Apical 4-Chamber View in a Patient With Transposition of the Great Arteries Post-Atrial Switch Operation The systemic right ventricle is significantly dilated with abnormal motion of the interventricular septum bulging toward the left ventricle in systole.