

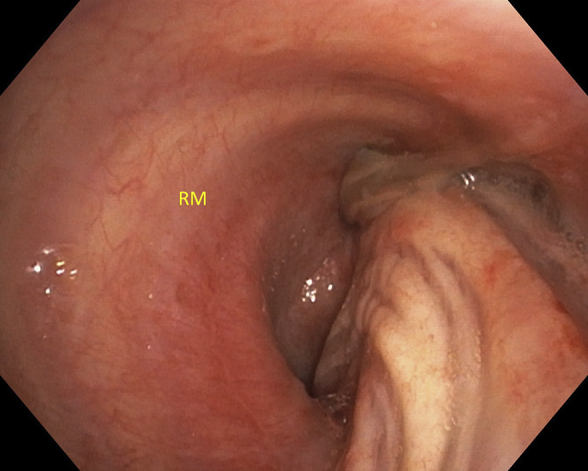
Distorted right mainstem (RM) bronchus without visualization of the right upper lobe bronchus.
Central Message.
We present the first reported case of spontaneous bilobar torsion in a patient who was managed via thoracoscopic pneumopexy and apical pleurectomy.
See Commentaries on pages 305 and 307.
Pulmonary torsion is a very rare but life-threatening condition. With a reported incidence of 0.089% to 0.4%,1,2 this phenomenon of parenchymal rotation around the bronchovascular axis is even more rare in the absence of recent surgery or trauma.3 Spontaneous lobar torsion can develop in the setting of an expansion of the pleural space (pneumothorax or pleural effusion) combined with pathologies that may distort the gross anatomic configuration of the lung (narrow lobar vascular pedicle, well-developed interlobar fissures, absence of an inferior pulmonary ligament, focal consolidation, or tumor).4, 5, 6 Diagnosis requires a high index of suspicion because clinical signs are nonspecific.7 Radiographic signs include lobar opacification, hilar displacement, interval positional change of opacified lung fields, bronchovascular distortion, and lobar air trapping.6, 7, 8, 9, 10 Bronchoscopy is diagnostic and may reveal an obstructed or distorted bronchial lumen, and vascular compromise progresses from ischemia to gangrene.11, 12, 13, 14 Urgent intervention is required and includes detorsion and fixation or resection of nonviable tissue.11,15, 16, 17 Whole lung and isolated lobar torsion has been previously described. To our knowledge, our case is the first reported case of spontaneous bilobar torsion.
A 73-year-old male smoker with a history of asthma and pulmonary embolism, and no history of thoracic surgery or trauma, presented with bilateral pneumonia. The patient had fevers up to 102.6°F, rigors, was hypotensive, and required fluid and vasopressor support. His oxygen saturation was 97% on room air and had coarse breath sounds on exam. Initial chest computed tomography (CT) demonstrated bilateral upper lobar consolidation and bilateral pleural effusions (Figure 1, A). The patient was appropriately treated for community-acquired pneumonia and never required intubation. His urine was positive for Streptococcus pneumoniae antigen, and blood cultures and subsequent respiratory cultures were negative.
Figure 1.

A, Initial admission computed tomography (CT) scan showing a coronal view of the right lung with right upper lobe (RUL) consolidation. The arrow is pointing to the RUL bronchus. B, CT 2 days after admission showing the right lower lobe (RLL) at the apex of the right chest and the consolidated RUL inferiorly and possibly right middle lobe (RML). Note the displacement of the RUL bronchus. C, Fiberoptic bronchoscopy demonstrating distal trachea, carina, left mainstem (LM) bronchus, and right mainstem (RM) bronchus. D, Distorted RM bronchus without visualization of the RUL bronchus.
Interval chest radiography 2 days later revealed migration of the initially observed right upper lobe opacification into the lower lung field. This prompted a repeat CT that demonstrated worsening right upper and middle lobar consolidation and distortion of the bronchial tree along with swirling of the pulmonary vasculature consistent with torsion (Figure 1, B, and Video 1). The patient was then transferred to our hospital and remained clinically stable. Apart from a mild leukocytosis, his laboratory profile was unremarkable. Bronchoscopy was performed and revealed a twisted appearance of the right mainstem bronchus and bronchus intermedius (Figure 1, C and D), precluding visualization of the distal airway. The bronchial orifice to the right upper lobe was not visible. Based on these findings, the patient was taken for thoracoscopic exploration. The operation was performed 28 hours after CT angiography was obtained.
Induction of general anesthesia and intubation was uneventful. Bronchoscopy was performed to confirm appropriate placement of the left-sided double lumen endotracheal tube and appeared similar to the initial bronchoscopic findings. After the patient was positioned in the lateral decubitus position, he became acutely hypoxic and hypotensive. Ventilatory recruitment maneuvers were administered along with inotropic support and resulted in prompt stabilization of the patient. Bronchoscopy was repeated to reassess the position of the double lumen endotracheal tube and the right-sided bronchial anatomy unexpectedly appeared normal.
We proceeded with thoracoscopy and this revealed viable but atelectatic right upper and middle lobes with a narrow common bronchovascular pedicle and an incomplete horizontal fissure (Figure 2, A). The oblique fissure was complete. The inferior pulmonary ligament was present and well developed. All three lobes were reapproximated and pneumopexied with suture (Figure 2, B), and an apical pleurectomy was performed. All lobes were fully re-expanded after ventilation was resumed to the right lung. The postoperative course was unremarkable, and the patient was discharged on postoperative day 4 (See Figure 3, A-D, for chronology of chest radiographs from admission to postoperative clinic visit and Video 1 for a stacked scrolling image of the patient's CT scan).
Figure 2.

A, Thoracoscopic view demonstrating atelectatic right upper lobe (RUL) and right middle love (RML) with a narrow common bronchovascular pedicle. B, Suture pneumopexy of RUL and right lower lobe (RLL).
Figure 3.

Chronology of chest radiographs from admission to discharge. A, Admission chest radiograph from the outside hospital demonstrating right upper lobe (RUL) consolidation. B, Interval chest radiograph showing migration of the RUL consolidation to right lower lung field. C, Immediate postoperative chest radiograph after thoracoscopic exploration. D, Postoperative chest radiograph 3 weeks after discharge from the hospital.
Discussion
Although few, most reports in the literature regarding spontaneous pulmonary torsion have either required lobectomy or pneumonectomy.11,15, 16, 17 In this case, the mechanism for torsion was believed to be related to a densely consolidated right upper lobe (Figure 1, A) that rotated around a common narrow pedicle (Figure 2, A) shared with the middle lobe. This, in addition to having a nearly complete oblique fissure and expansion of the potential pleural space by an effusion, caused a nearly 180° rotation of the upper and middle lobes from a normal anatomical position to the lower half of the hemithorax, displacing the right lower lobe superiorly.
Resection was not required by our patient. The detorsion of the lobes before exploration may have been related to intubation, lateral decubitus positioning, and recruitment maneuvers. Moreover, the bilobar torsion (middle and upper lobes) was incomplete, preventing irreversible ischemia and resulting only in atelectasis. The hypotension that occurred after positioning the patient may have been related to anesthetic agents and hypovolemia or the release of systemic inflammatory mediators after the bronchovascular pedicle detorsed and venous drainage was re-established.11,18, 19, 20 Our case highlights the importance of early recognition and prompt management of pulmonary torsion. When the lung parenchyma is viable, we recommend surgical fixation of the lobes with sutures or staplers and partial pleurectomy to prevent recurrence.
Acknowledgments
The authors thank Clinical Associate Professor of Radiology Mauricio S. Galizia, MD, for his assistance in the interpretation of the chest imaging scans.
Footnotes
Disclosures: The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
This Case Report was a winner of the Case Report Competition of the AATS 100th Annual Meeting.
Supplementary Data
Video with audio of coronal views of computed tomography angiography demonstrating course of right pulmonary artery and displaced right upper and lower lobes. Video available at: https://www.jtcvs.org/article/S2666-2507(21)00100-0/fulltext.
{kind=link}
References
- 1.Cable D.G., Deschamps C., Allen M.S., Miller D.L., Nichols F.C., Trastek V.F. Lobar torsion after pulmonary resection: presentation and outcome. J Thorac Cardiovasc Surg. 2001;122:1091–1093. doi: 10.1067/mtc.2001.117839. [DOI] [PubMed] [Google Scholar]
- 2.Hennink S., Wouters M.W.J.M., Klomp H.M., Baas P. Necrotizing pneumonitis caused by postoperative pulmonary torsion. Interact Cardiovasc Thorac Surg. 2008;7:144–145. doi: 10.1510/icvts.2007.158378. [DOI] [PubMed] [Google Scholar]
- 3.Ohde Y., Nakagawa K., Okumura T., Kondo H. Spontaneous pulmonary torsion secondary to pseudo-Meigs' syndrome. Interact Cardiovasc Thorac Surg. 2005;4:59–60. doi: 10.1510/icvts.2004.096594. [DOI] [PubMed] [Google Scholar]
- 4.Raynaud C., Lenoir S., Caliandro R., Raffenne L., Validire P., Gossot D. Spontaneous middle lobe torsion secondary to pleural effusion. Chest. 2009;136:281–283. doi: 10.1378/chest.08-2373. [DOI] [PubMed] [Google Scholar]
- 5.Moser E.S., Proto A.V. Lung torsion: case report and literature review. Radiology. 1987;162:639–643. doi: 10.1148/radiology.162.3.3544030. [DOI] [PubMed] [Google Scholar]
- 6.Felson B. Lung torsion: radiographic findings in nine cases. Radiology. 1987;162:631–638. doi: 10.1148/radiology.162.3.3809475. [DOI] [PubMed] [Google Scholar]
- 7.Lal A., Akhtar J., Jindal V., Ullah A. Rare cause of respiratory failure: a twist in the tale. Ann Am Thorac Soc. 2018;15:880–883. doi: 10.1513/AnnalsATS.201802-122CC. [DOI] [PubMed] [Google Scholar]
- 8.Childs L., Ellis S., Francies O. Pulmonary lobar torsion: a rare complication following pulmonary resection, but one not to miss. BJR Case Rep. 2016;3:20160010. doi: 10.1259/bjrcr.20160010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nguyen J.C., Maloney J., Kanne J.P. Bilateral whole-lung torsion after bilateral lung transplantation. J Thorac Imaging. 2011;26:W17. doi: 10.1097/RTI.0b013e3181e35ab5. [DOI] [PubMed] [Google Scholar]
- 10.Ternes T., Trump M., de Christenson M.R., Howell G., Stewart J. Spontaneous middle-lobe torsion. Radiol Case Rep. 2015;8:812. doi: 10.2484/rcr.v8i1.812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dai J., Xie D., Wang H., He W., Zhou Y., Hernández-Arenas L.A. Predictors of survival in lung torsion: a systematic review and pooled analysis. J Thorac Cardiovasc Surg. 2016;152:737–745.e3. doi: 10.1016/j.jtcvs.2016.03.077. [DOI] [PubMed] [Google Scholar]
- 12.Cohn S.M. Taylor & Francis; Milton Park, United Kingdom: 2007. Complications in Surgery and Trauma. [Google Scholar]
- 13.Wong P.S., Goldstraw P. Pulmonary torsion: a questionnaire survey and a survey of the literature. Ann Thorac Surg. 1992;54:286–288. doi: 10.1016/0003-4975(92)91386-n. [DOI] [PubMed] [Google Scholar]
- 14.Ekstein S.F., McCambridge A., Edell E.S., Koo C.W., Blackmon S.H. Case of spontaneous whole-lung torsion with literature review. J Thorac Dis. 2018;10:E690–E693. doi: 10.21037/jtd.2018.08.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Venuta F., Anile M., de Giacomo T., Coloni G.F. Prevention of middle lobe torsion after right upper lobectomy with a polymeric sealant. J Thorac Cardiovasc Surg. 2012;143:240–241. doi: 10.1016/j.jtcvs.2011.06.033. [DOI] [PubMed] [Google Scholar]
- 16.Uramoto H., Takenoyama M., Hanagiri T. Simple prophylactic fixation for lung torsion. Ann Thorac Surg. 2010;90:2028–2030. doi: 10.1016/j.athoracsur.2010.07.040. [DOI] [PubMed] [Google Scholar]
- 17.Le Pimpec-Barthes F., Arame A., Pricopi C., Riquet M. Prevention of middle lobe torsion or bronchial plication using anti-adhesive membrane: a simple, safe and uncomplicated technique! Eur J Cardiothorac Surg. 2011;39:1059–1069. doi: 10.1016/j.ejcts.2010.09.033. [DOI] [PubMed] [Google Scholar]
- 18.Larsson S., Lepore V., Dernevik L., Nilsson F., Selin K. Torsion of a lung lobe: diagnosis and treatment. Thorac Cardiovasc Surg. 1988;36:281–283. doi: 10.1055/s-2007-1020097. [DOI] [PubMed] [Google Scholar]
- 19.Apostolakis E., Koletsis E.N., Panagopoulos N., Prokakis C., Dougenis D. Fatal stroke after completion pneumonectomy for torsion of left upper lobe following left lower lobectomy. J Cardiothorac Surg. 2006;1:25. doi: 10.1186/1749-8090-1-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hendriks J., Van Schil P., De Backer W., Hauben E., Vanmaele R., Van Marck E. Massive cerebral infarction after completion pneumonectomy for pulmonary torsion. Thorax. 1994;49:1274–1275. doi: 10.1136/thx.49.12.1274. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video with audio of coronal views of computed tomography angiography demonstrating course of right pulmonary artery and displaced right upper and lower lobes. Video available at: https://www.jtcvs.org/article/S2666-2507(21)00100-0/fulltext.