

Abstract
Background/aims
We examined associations of ever crossing upwards ≥2 (vs <2) major weight-for-length (WFL) percentiles in the first 24 months with obesity at 5 years among white and black children.
Methods
We included 10 979 white and 1245 black children from the Linked CENTURY Study with percentile crossing data in all four 6-month periods in the first 24 months and obesity (age-specific and sex-specific body mass index ≥95th percentile) at 5 years. We used adjusted logistic regression models and stratified by race.
Results
64% of children crossed upwards ≥2 major WFL percentiles in the first 2 years. Among white children, 12% were obese vs 7% for <2 crossings, while among black children the frequencies were 23% vs 9%. Black children (adjusted OR 2.94, 2.04 to 4.23) who had ever crossed upwards ≥2 major WFL percentiles had a higher odds of obesity at age 5 than white children (adjusted OR 1.89, 1.64 to 2.18) (interaction p=0.02).
Conclusions
Our results suggest that rapid weight gain in infancy is more deleterious among black than white children for later obesity.
INTRODUCTION
Rapid weight gain during infancy and early childhood appears to raise the risk for later obesity. Woo Baidal et al recently found that 45/46 studies reported an association between higher infancy weight or weight gain during the first 1000 days of life and overweight (including obesity) in children aged <18 years.1 While the definition of weight gain varied across studies, relationships were consistent regardless of the type of measurement and growth chart used.
Until recently, clinicians in the USA routinely used the Centers for Disease Control and Prevention (CDC) growth charts to monitor young children’s growth during well-child visits by collecting repeated measurements of weight and length or height. The CDC growth charts include major percentile lines indicating the 5th, 10th, 25th, 50th, 75th, 90th and 95th percentiles for age and sex.2 Taveras et al found that upward crossing of ≥2 (vs <2) major weight-for-length (WFL) percentiles in the first 24 months of life was associated with obesity at ages 5 and 10 years.3 Among the four 6-month intervals in those first 24 months, upward crossing of ≥2 major WFL percentiles during the first 6 months was associated with the highest prevalence of later obesity.
While black (11.3%) and Hispanic (16.7%) children aged 2–5 years are more likely to be obese than white (3.5%) children,4 little is known of how the association between rapid weight gain and later obesity may differ by race/ethnicity, a variable often poorly measured in clinical databases. We used the Linked Collecting Electronic Nutrition Trajectory Data Using e-Records of Youth (CENTURY) Study, created by linkage of clinical and public health data sources, to examine associations of ever crossing upwards ≥2 (vs <2) major WFL percentiles in the first 24 months of life with obesity at age 5 years among white and black children.
METHODS
The Linked CENTURY Study is a longitudinal clinical database of well-child visits for 200 343 singleton children through age 18 years linked to each child’s Massachusetts birth certificate (74.2% of participants in the original CENTURY Study were linked).5 While the original CENTURY Study contained children’s clinical growth data, race/ethnicity was missing for 36% of participants, and linkage with birth certificates provided most of those missing data. From each birth certificate we extracted data on maternal race, self-reported in the categories white, black, Asian/Pacific Islander, American Indian and other, which was available for 98.7% of the participants.5 For this analysis, we restricted the study population to white and black participants. We also obtained birth weight, marital status and maternal education from the birth certificate.
Medical assistants measured length or height and weight according to the written protocol of the department of paediatrics at Harvard Vanguard Medical Associates (currently Atrius Health). More details on the measurements are available else-where.5 We used height and weight measurements to calculate age-specific and sex-specific WFL percentiles for children <24.0 months and body mass index (BMI) percentiles for children aged 2–18 years based on the CDC growth charts from 2000.2 The main exposure was ever crossing upwards ≥2 major WFL percentiles (ie, rise in BMI) during any of the four 6-month intervals (±30 days) in the first 24 months of life (1–6, 6–12, 12–18, 18–24). We used the CDC’s predefined major percentile lines (5th, 10th, 25th, 50th, 75th, 90th and 95th percentiles).
In a validation study among 160 children aged 0 through 23 months conducted at one of the participating health centres, the usual clinical paper-and-pencil method systematically overestimated children’s length compared with a reference method using a recumbent length measuring board.6 This bias did not depend meaningfully on the age or sex of the child. Thus, we used a regression correction factor to adjust for this systematic overestimation: ((0.953×length measured by paper-and-pencil method)+1.8 cm).6 The main outcome was obesity at age 5 years defined as a BMI ≥95th percentile for age and sex.2
We included 12 224 children, including 10 979 white and 1245 black children, who had data on percentile crossing in all four 6-month periods in the first 24 months of life and BMI data at age 5 years (mean (SD) was 5.25 years (0.33); range=5.00–5.99 years). We used logistic regression models to examine the association of ever crossing upwards ≥2 (vs <2) major WFL percentiles during any of the four intervals in the first 24 months of life with obesity at age 5 years. We adjusted all models for sex, age, birth weight, marital status, maternal education and 5-year time period at outcome, and stratified by race. We conducted all analyses using SAS V.9.3.
RESULTS
Table 1 shows that 6974 (64%) white children and 797 (64%) black children crossed upwards ≥2 major WFL percentiles in the first 2 years. Among white children, 837 (12%) of them were obese compared with 277 (7%) for those who crossed <2 major WFL percentiles. Among black children, 186 (23%) were obese who crossed ≥2 major WFL percentiles compared with 42 (9%) who crossed <2. Black children (adjusted OR 2.94, 95% CI 2.04 to 4.23) who had ever crossed upwards ≥2 major WFL percentiles (vs <2) had a higher odds of obesity at age 5 than white children (adjusted OR 1.89, 1.64 to 2.18). A significant interaction (p=0.02) indicated that the association varied by children’s race/ethnicity, such that black children had a stronger association between crossed upwards ≥2 major WFL percentiles (vs <2) and obesity at age 5 than white children.
Table 1.
Characteristics and adjusted odds of obesity at age 5 years among white and black children who had ever crossed upwards ≥2 vs <2 major weight-for-length percentiles in the first 24 months of life (N=12 224)
| Characteristic | White (N=10 979) | Black (N=1245) | ||||
|---|---|---|---|---|---|---|
| N (column %) | N (row %) with obesity | OR (95% CI) | N (column %) | N (row %) with obesity | OR (95% CI) | |
| Number of major weight-for-length percentile crossings in the first 24 months | ||||||
| <2 major weight-for-length percentiles | 4 005 (36.5) | 277 (6.9) | 1.0 | 448 (36.0) | 42 (9.4) | 1.0 |
| ≥2 major weight-for-length percentiles | 6 974 (63.5) | 837 (12.0) | 1.89 (1.64 to 2.18) | 797 (64.0) | 186 (23.3) | 2.94 (2.04 to 4.23) |
| Sex | ||||||
| Male | 5 662 (51.6) | 603 (10.7) | 1.0 | 611 (49.1) | 107 (17.5) | 1.0 |
| Female | 5 317 (48.4) | 511 (9.6) | 0.99 (0.88 to 1.13) | 634 (50.9) | 121 (19.1) | 1.31 (0.96 to 1.77) |
| 5-Year time period at 5-year visit | ||||||
| 1985 to <1990 | 499 (4.5) | 24 (4.8) | 0.43 (0.28 to 0.66) | 32 (2.6) | 8 (25.0) | 1.21 (0.50 to 2.94) |
| 1990 to <1995 | 1940 (17.7) | 129 (6.7) | 0.56 (0.45 to 0.70) | 138 (11.1) | 18 (13.0) | 0.43 (0.23 to 0.78) |
| 1995 to <2000 | 2769 (25.2) | 259 (9.4) | 0.83 (0.69 to 0.99) | 346 (27.8) | 55 (15.9) | 0.65 (0.44 to 0.97) |
| 2000 to <2005 | 3184 (29.0) | 397 (12.5) | 1.08 (0.92 to 1.27) | 365 (29.3) | 62 (17.0) | 0.68 (0.47 to 1.00) |
| 2005 to 2008 | 2587 (23.6) | 305 (11.8) | 1.0 | 364 (29.2) | 85 (23.4) | 1.0 |
| Marital status | ||||||
| Married | 10 409 (94.8) | 1031 (9.9) | 0.76 (0.59 to 0.97) | 769 (61.8) | 149 (19.4) | 1.14 (0.83 to 1.58) |
| Not married | 568 (5.2) | 83 (14.6) | 1.0 | 476 (38.2) | 79 (16.6) | 1.0 |
| Maternal education | ||||||
| ≤12 years | 2050 (18.7) | 262 (12.8) | 1.0 | 387 (31.3) | 67 (17.3) | 1.0 |
| 13–15 years | 6098 (55.6) | 628 (10.3) | 0.82 (0.70 to 0.96) | 703 (56.8) | 134 (19.1) | 1.06 (0.75 to 1.48) |
| 16+ years | 2814 (25.7) | 222 (7.9) | 0.67 (0.55 to 0.81) | 147 (11.9) | 23 (15.7) | 0.76 (0.44 to 1.31) |
| Mean (SD) | Mean (SD) | |||||
| Birth weight, kg | 3.53 (0.50) | 1114 (10.2) | 1.71 (1.50 to 1.95) | 3.32 (0.52) | 228 (18.3) | 2.04 (1.51 to 2.76) |
| Age at outcome, months | 63.0 (4.0) | 1114 (10.2) | 1.00 (0.99 to 1.02) | 63.4 (3.7) | 228 (18.3) | 0.99 (0.95 to 1.03) |
Figure 1 illustrates the prevalence of obesity at age 5 associated with crossing upwards ≥2 major WFL percentiles during each of the four 6-month periods in the first 24 months, according to the category of starting WFL percentile at the start of each interval. For white children, crossing upwards ≥2 major WFL percentiles in the first 6 months was associated with the highest prevalence of obesity at age 5 years, except for those who started at the 75 to <90th percentile. For black children, crossing upwards ≥2 major WFL percentiles in the first 6 months was associated with the highest prevalence of obesity at age 5 years only for those who started at the <25th percentile.
Figure 1.
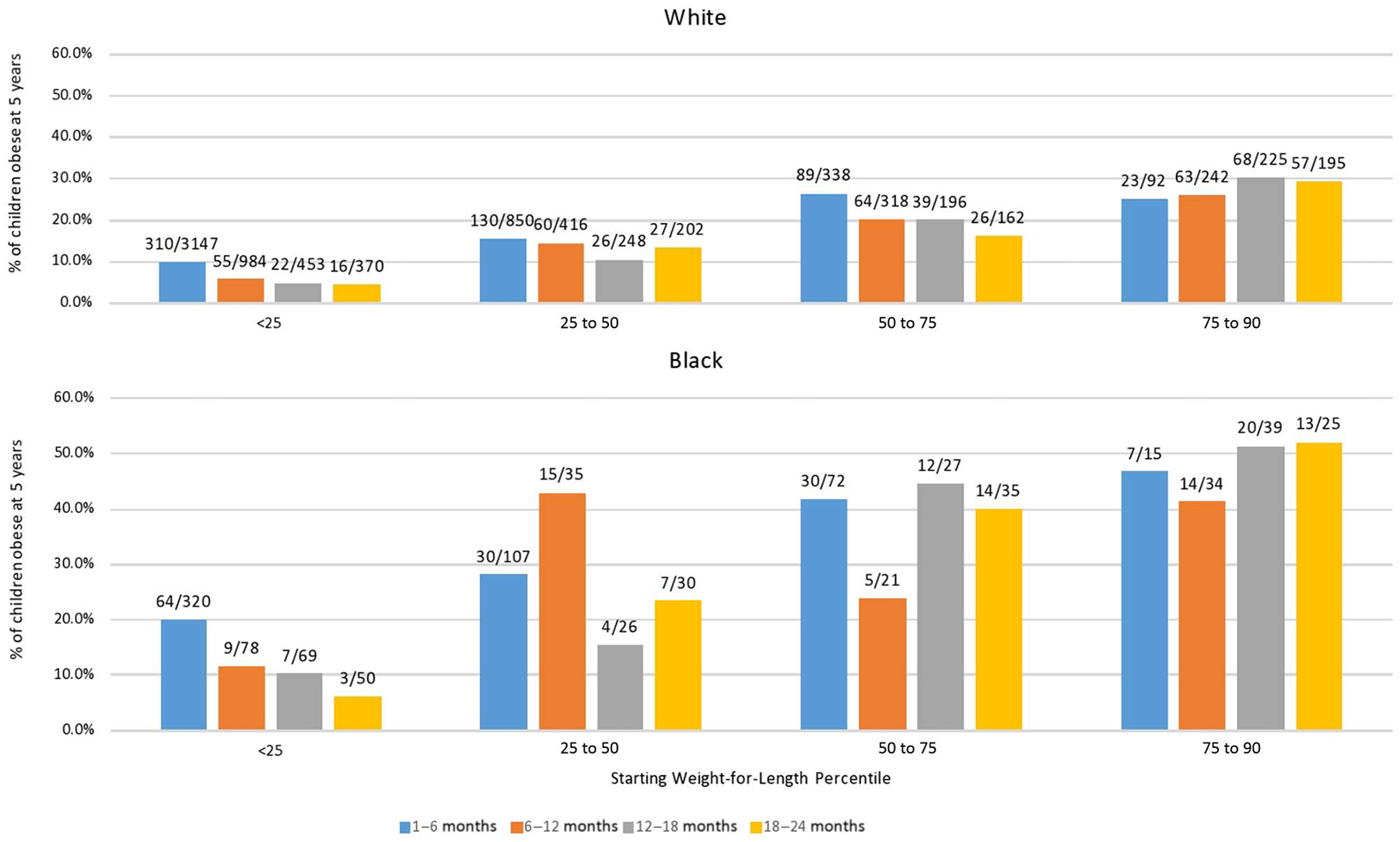
Prevalence of obesity (defined as body mass index ≥95th percentile) at age 5 years among white and black children associated with crossing upwards 2 or more major weight-for-length percentile lines (Centers for Disease Control and Prevention 2000 growth charts) during each of four 6-month age intervals in the first 24 months of life, according to the category of starting weight-for-length percentile at the start of each interval. The denominators are the number of participants who crossed ≥2 major percentiles during the 6-month age interval. The numerators are the number of participants who were obese at 5 years among those who crossed ≥2 major percentiles. Children whose starting weight-for-length percentile was ≥90th were excluded because they could not cross upwards 2 major percentile lines.
DISCUSSION
We found that rapid weight gain in infancy conferred a higher odds of obesity at age 5 among black than white children. Our findings expand on those of Taveras et al, who reported that crossed upwards ≥2 major WFL percentiles increased obesity at ages 5 and 10 years, but these authors could not explore racial/ethnic differences due to missing information.3 We also found increasing trends of obesity across 5-year time periods, consistent with the existing literature.
We created the Linked CENTURY Study by linking each child’s clinical record and birth certificate.5 Information from the birth certificate can help enhance clinical databases by filling in missing child race/ethnicity information and capturing information not routinely collected, such as maternal education.5 Despite near-complete race/ethnicity data in our analyses, we were able to include only white and black children because sample sizes for other racial/ethnic groups were too small. While the birth certificate captures the mother’s race/ethnicity and not the child’s, in our dataset there was a 91% agreement between mothers’ and children’s race/ethnicity.
Our study highlights the advantages of linking clinical and population-based databases to identify racial differences in risk factors for obesity. Since clinicians routinely use growth charts to monitor children’s growth during well-child visits, our findings provide further support3 that counting the number of major percentiles a child crosses may have clinical utility for identifying those at higher risk for later obesity.4 Further research to ascertain the underlying causes of rapid weight gain during infancy,1 and the extent to which those causes also differ by race/ethnicity (ie, infant feeding or sleep patterns), is critical for the development of evidence-based policies and programmes to address the obesity epidemic in the USA.
What is already known on this topic?
Taveras et al3 found that upward crossing of ≥2 (vs <2) major weight-for-length percentiles in the first 24 months was associated with later obesity.
There is little known of how the association between rapid weight gain and later obesity may differ by race/ethnicity.
What this study adds?
Rapid weight gain in infancy conferred a higher odds of obesity at age 5 among black than white children.
Funding
This work was partially funded by grants from the NIH (R00 HD068506) to Dr Hawkins and the National Center for Chronic Disease Prevention and Health Promotion (contract no. 200-2008-M-26882) to Dr Taveras. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Footnotes
Competing interests None declared.
Ethics approval The Institutional Review Boards at Boston College and Harvard Pilgrim Health Care reviewed this study and considered it exempt.
Data sharing statement No data from the Linked Collecting Electronic Nutrition Trajectory Data Using e-Records of Youth Study are publicly available.
REFERENCES
- 1.Woo Baidal JA, Locks LM, Cheng ER, et al. Risk factors for childhood obesity in the first 1,000 days: a systematic review. Am J Prev Med 2016;50:761–79. [DOI] [PubMed] [Google Scholar]
- 2.Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000 CDC growth charts for the United States: methods and development. Vital Health Stat 11 2002;246:1–190. [PubMed] [Google Scholar]
- 3.Taveras EM, Rifas-Shiman SL, Sherry B, et al. Crossing growth percentiles in infancy and risk of obesity in childhood. Arch Pediatr Adolesc Med 2011;165:993–8. [DOI] [PubMed] [Google Scholar]
- 4.Ogden CL, Carroll MD, Kit BK, et al. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014;311:806–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hawkins SS, Gillman MW, Rifas-Shiman SL, et al. The Linked CENTURY Study: linking three decades of clinical and public health data to examine disparities in childhood obesity. BMC Pediatr 2016;16:32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rifas-Shiman SL, Rich-Edwards JW, Scanlon KS, et al. Misdiagnosis of overweight and underweight children younger than 2 years of age due to length measurement bias. Med Gen Med 2005;7:56. [PMC free article] [PubMed] [Google Scholar]