

Abstract
Resilient, undercontrolled, and overcontrolled (RUO) personality types have been identified across the lifespan and are associated with psychiatric symptoms and functioning. However, it is unknown whether these types are identifiable in preschool-aged children using observational indices or whether they predict longitudinal outcomes. The current study used observationally coded five factor model (FFM) traits in a sample of preschoolers to identify whether personality traits cluster into types, whether types predict psychiatric symptoms and impairment across development, and whether types better predict outcomes than trait dimensions. Using a validated “thin slice” approach, preschool personality was observationally coded in a clinically enriched sample oversampled for depression (N=299). Latent class analysis tested how FFM dimensions organized into types, identifying resilient, undercontrolled and overcontrolled preschoolers. Types demonstrated baseline diagnostic differences and multilevel models indicated above baseline diagnoses, undercontrolled children exhibited elevated externalizing symptoms and worse functioning across development while overcontrolled and resilient children did not differ. Personality types and dimensions both provided similar predictive utility. RUO personality types are identifiable using FFM observational coding in clinically heterogeneous preschoolers and undercontrolled children demonstrated the most severe trajectories. Findings highlight that personality types are detectable at early ages and have unique predictive power for psychiatric outcomes across development compared with dimensions.
Keywords: preschool children, thin slice, personality types, Big Five, developmental psychopathology
Personality types have long been theorized to be associated with psychiatric disorders, dating from ancient Greece, with sanguine, phlegmatic, choleric and melancholic types conferring differential risk for physical and mental illness (Maher & Maher, 1994). Current thinking has continued to link personality and psychopathology, demonstrating in meta-analyses that indeed, dimensional personality is associated with a range of psychiatric disorders in adults (Kotov, Gamez, Schmidt, & Watson, 2010), with substantial evidence demonstrating similar relations in childhood (e.g., De Bolle, Beyers, De Clercq, & De Fruyt, 2012; De Fruyt, De Clercq, & De Bolle, 2017).
While adult personality assessment has come to focus on dimensional models of personality, a lengthy history and extent contingent within developmental psychology still argues for the value of personality assessment through types. Dimensional approaches have also extended to childhood personality assessment (Caspi, Roberts, & Shiner, 2005; Soto & Tacket, 2015), demonstrating the predictive utility of childhood personality for later outcomes (Caspi & Shiner, 2006; De Clercq, De Fruyt, & Widiger, 2009; Tackett, 2006). Despite the historical importance of types, there is less research focused on the association of psychopathology with types, especially in young children, compared to the dimensional approach. Thus, it is unclear whether early-emerging personality types in the preschool period exert longitudinal influence on developmental trajectories of psychiatric symptoms and outcomes. The current study tested how thin-sliced observed personality traits during the preschool period organize into personality types and whether these personality types prospectively predict trajectories of psychiatric symptoms and impairment across development. To address the longstanding argument between types and traits, we also compared the predictive validity of preschool types with dimensional traits.
Person-centered Approaches to Personality
A majority of literature assessing personality across the lifespan uses the dimensional Big 5, or Five Factor Model (FFM) to assesses extraversion, agreeableness, conscientiousness, neuroticism, and openness to experience (Caspi & Shiner, 2006; Costa & McCrae, 1992). The “Little 6” is a developmental adaptation of the Big 5 to young children that includes a sixth personality dimension of ‘activity’ (Soto & Tacket, 2015). Although this dimensional model is the most widely accepted conceptualization of childhood personality, an overlapping yet distinct approach with strong developmental roots is the person-centered, or “typological,” approach. Person-centered approaches focus on how constellations of personality dimensions cluster within a child and how these clusters differentiate between children (Grist & McCord, 2010).
Although person-centered approaches have received less attention than dimensional approaches, personality traits do not exist in isolation, so understanding how personality dimensions organize together within an individual provides a useful way to capture individual differences in personality (Beck & Jackson, 2019; Caspi et al., 2005; Zentner & Shiner, 2012). Additionally, given that individual personality dimensions tend to result in maladaptive outcomes at very extreme levels, there is potential merit in understanding combinations of dimensions that might allow conceptualizing children at high risk for targeted prevention efforts (Asendorpf, Denissen, & van Aken, 2008; Zentner & Shiner, 2012). However, there is controversy regarding the usefulness of types versus traits of personality. Although some research indicates types provide better predictive validity of psychopathology over traits, especially longitudinal outcomes (Asendorpf & Denissen, 2006; Hart, Atkins, Fegley, Robins, & Tracy, 2003), other literature indicates traits demonstrate stronger associations (Asendorpf, 2003; Costa Jr, Herbst, McCrae, Samuels, & Ozer, 2002).
One of the earliest and most well-known childhood based typologies is the resilient, undercontrolled, and overcontrolled types (RUO; Robins, John, Caspi, Moffitt, & Stouthamer-Loeber, 1996). The RUO types have been replicated across cultures and ages including children 4 – 6 years (Asendorpf & van Aken, 1999; Hart et al., 2003; Robins et al., 1996; Specht, Luhmann, & Geiser, 2014; Van den Akker, Deković, Asscher, Shiner, & Prinzie, 2013). Using dimensional FFM scales to obtain types in older children and adolescents, resilient individuals exhibit high extraversion, conscientiousness, agreeableness and openness and low neuroticism (Asendorpf, Borkenau, Ostendorf, & Van Aken, 2001; Robins et al., 1996). Undercontrolled individuals exhibit low agreeableness and conscientiousness and are impulsive, disobedient, and energetic (Asendorpf & van Aken, 1999; Donnellan & Robins, 2010). Overcontrolled individuals exhibit low extraversion and elevated neuroticism and are shy, inhibited, and tense, but also compliant, cooperative, and pro-social (Asendorpf et al., 2001; Donnellan & Robins, 2010).
Although research demonstrates RUO types can be identified in preschool-aged children (Asendorpf & van Aken, 1999; Caspi, 2000), including using parent-reported temperament measures (Komsi et al., 2006), some typological research demonstrates different numbers of types (Caspi & Silva, 1995; Wilson, Schalet, Hicks, & Zucker, 2013) or names of types (i.e., overcontrolled-resilient, resilient-undercontrolled, and brittle; Weir & Gjerde, 2002). For instance, in a large (n=1037) New Zealand sample five clusters were identified: undercontrolled, inhibited, confident, reserved, and well-adjusted (Caspi & Silva, 1995), while more recent work identified six parent-reported types across three samples (unregulated, regulated, high reactive, bold, average, and well-adjusted; Prokasky et al., 2017). Inconsistencies in number and characterizations of types is purportedly due to 1) measurement, as research has used behavioral, parent, and teacher reports of child personality to create types or 2) statistical techniques, using Q-factor or cluster analyses, rather than more sophisticated model-based approaches such as latent class analysis (LCA).
Regarding variation in measurement, parent or teacher report introduces informant bias, while observational measures of personality provides a different, objective third-party perspective. Regarding variation from statistical techniques, although cluster analysis and LCA provide somewhat overlapping results, LCA is model-based and determines the optimal number of groups, while optimal group number is determined by the researcher in cluster analysis (Donnellan & Robins, 2010). Additionally, the adult literature utilizes the FFM and the FFM has been employed to generate the RUO types in older adolescent and adult samples (Specht et al., 2014), however has not been used in preschoolers. Using the FFM as the basis of creating types in preschoolers aides in the continuity of personality assessment across the lifespan.
Psychopathology and Preschool Personality Types
Although RUO personality types are consistently identified across ages and cultures (Asendorpf et al., 2001; Specht et al., 2014) and are replicable from childhood through adolescence (Klimstra, Hale Iii, Raaijmakers, Branje, & Meeus, 2010), no studies have looked at them in preschoolers using the FFM as the basis and few have looked at the association of these types with concurrent and longitudinal psychopathology within preschoolers. In older childhood samples, those in undercontrolled and overcontrolled groups demonstrate consistent relationships with psychopathology. Undercontrolled children exhibit elevated externalizing symptoms and moderately elevated internalizing symptoms as well as aggressiveness, delinquency and more conflict in relationships (Asendorpf et al., 2001; Donnellan & Robins, 2010; Robins et al., 1996; Van den Akker et al., 2013). Overcontrolled children exhibit elevated internalizing problems and often experience social difficulties, including loneliness and social withdrawal (Donnellan & Robins, 2010; Robins, John, & Caspi, 1998). Conversely, resilient children display few psychopathological symptoms, instead, being characterized by increased self-confidence, self-direction, and emotional stability (Donnellan & Robins, 2010). While this research indicates that personality types assessed later in childhood have important associations with psychopathology (Donnellan & Robins, 2010; Robins et al., 1998; Van den Akker et al., 2013), it is unknown whether RUO personality types during the preschool age are associated with concurrent psychopathology. Moreover, it is unknown whether observed FFM-based preschool personality types influence trajectories of psychiatric outcomes across development, an issue that is critical to inform earlier identification and intervention.
The Current Study
The current study addressed these unknowns by utilizing behaviorally coded FFM personality dimensions and employing latent class analysis in a large heterogeneous preschool sample enriched for clinical psychopathology that was followed longitudinally for 9 years. Because obtaining self-reports about their own personalities is not feasible due to cognitive limitations, and parent or teacher informants of preschool personality were not available, we observationally coded child personality using the ‘thin slice’ method. ‘Thin slice’ coding involves naïve observers making ‘snap judgments’ about an individual after watching short clips of the individual across contexts (Ambady, Bernieri, & Richeson, 2000). In both child and adult samples, thin slice methods indicate untrained individuals can quickly and accurately rate personality, demonstrating good within-rater and cross-context agreement (Ambady et al., 2000). Thin slice methods for assessing personality in children have been applied to existing data (Tackett et al., 2017) and predict later personality and psychopathology (Tacket, Lang, Markon, & Herzhoff, 2019). We have recently validated this method in preschoolers in the same sample, indicating both within and across task consistency comparable to or better than estimates found in adults (Whalen, Gilbert, Jackson, Barch, & Luby, 2020)
Utilizing this observed measure of preschool personality, the first objective was to investigate whether FFM dimensions organized into RUO personality types using LCA modeling techniques in a clinically heterogeneous sample of preschool-aged children. The second objective was to assess associations between preschool personality types and concurrent psychiatric diagnoses and prospective trajectories of symptoms of psychopathology and global functioning averaged across development. We hypothesized undercontrolled preschoolers would exhibit high externalizing symptoms and moderate depression and anxiety (internalizing) symptom trajectories across development, overcontrolled preschoolers would exhibit elevated depression and anxiety symptom trajectories, and resilient preschoolers would exhibit the lowest internalizing and externalizing trajectories. Moreover, we hypothesized that undercontrolled and overcontrolled preschoolers would demonstrate persistently worse global functioning trajectories compared with resilient preschoolers. The third objective was to test the usefulness of types predicting prospective symptoms and functioning compared with individual dimensions.
We have previously demonstrated associations between the individual FFM dimensions (but not types) with concurrent and prospective symptoms of psychopathology in the same sample (Gilbert et al., 2019). Specifically, higher extraversion and lower agreeableness and conscientiousness predicted depressive symptoms in adolescence, lower agreeableness and higher neuroticism predicted increased externalizing symptoms, and associations of conscientiousness with depressive symptoms and neuroticism with externalizing symptoms remained significant when controlling for baseline psychopathology (Gilbert et al., 2019). As such, we also wanted to compare whether dimensions or types provide better predictive validity. Hypotheses were not preregistered.
METHODS
Supplemental documents are posted to an open-science repository https://osf.io/ywnu9/. Two previously published papers have used the current observational personality data in the same sample, first, to validate the thin-slice approach in preschoolers (Whalen et al., 2020) and second, the thin slice FFM dimensional ratings (e.g., extraversion, neuroticism) were used to examine concurrent and prospective trajectories of the same symptoms of psychopathology presented here (Gilbert et al., 2019). However, this is the first paper that has examined whether or not personality types could be identified and whether these types predicted future psychiatric outcomes. Sixty plus other manuscripts have utilized the Preschool Depression Study (PDS) dataset, which commenced data collection in 2003 and data collection continues using parent, child, observational, neuroimaging, electroencephalogram recordings, and behavioral methods. The final author on this manuscript is the P.I. of this study and on all manuscripts from this large-scale project. Other than the two above-mentioned manuscripts, no other manuscripts have examined personality variables in this sample.
Participants
Participants included 299 children from the Preschool Depression Study (PDS)(Luby, Si, Belden, Tandon, & Spitznagel, 2009) who had usable observational data during the preschool waves. The PDS is an ongoing longitudinal study conducted at the Washington University School of Medicine (WUSM) in St. Louis. Children aged 3.0–5.11 years and their primary caregivers were recruited from daycares, preschools, and primary care sites in the St. Louis area using the Preschool Feelings Checklist from 2003–2005 to oversample for depression (Luby, Heffelfinger, Koenig-McNaught, Brown, & Spitznagel, 2004). Children were excluded for chronic illness, neurological disorders, Autism Spectrum Disorders, and speech, language, or cognitive delays. Of the 416 who met inclusion/exclusion criteria and were eligible for participation, 305 enrolled at baseline. The sample size was chosen to include all possible participants who completed baseline in 2003–2005 and had more than 10 observational assessments to employ the thin slice technique, leading to six children being excluded (n=299). To obtain the best approximation of preschool personality traits, observational data assessed across the first three preschool-aged assessments were combined. Age at baseline was calculated as mean age at the three assessments (M=5.36, SD=0.86, Min=3.13, Max=6.99). In total, children were followed for approximately 9 years, participating in up to 8 in-person visits, and the mean age at the final session was 13.57(0.97). Parental consent and child verbal assent were obtained before study participation. The Institutional Review Board at WUSM approved all procedures in accordance with ethical guidelines.
Measures
DSM-IV Psychiatric Diagnoses.
Trained staff conducted in-person diagnostic assessments with children and primary caregivers from study enrollment through the final follow-up assessment at approximately annual assessments. From baseline through age 7 the Preschool-Age Psychiatric Assessment (PAPA) (Egger et al., 2006) was used with primary caregivers, at age 8 the Childhood and Adolescent Psychiatric Assessment (CAPA) (Angold & Costello, 2000) was administered to caregivers, and at age 9 to the final assessment the CAPA was administered to child and caregiver. Interviews were audiotaped, reviewed for reliability, and calibrated for accuracy using methods previously described (Luby, Belden, Pautsch, Si, & Spitznagel, 2009). The presence of a preschool internalizing disorder included major depressive disorder (MDD), separation anxiety disorder (SAD), or generalized anxiety disorder (GAD) and preschool externalizing disorders included conduct disorder (CD), attention deficit hyperactivity disorder (ADHD) and oppositional defiant disorder (ODD).
Depression, Anxiety, and Externalizing Severity Scores.
Depression, anxiety, and externalizing severity scores were created at all school age assessments using the CAPA. The depression severity score was the sum of 9 core depression symptoms from DSM-IV MDD criteria. The anxiety severity score was the combined sum of core symptoms of SAD and GAD modules of the CAPA. The externalizing severity score was the combined sum of core symptoms of ADHD, ODD and CD modules of the CAPA. Internal consistencies for depression, anxiety and externalizing severity scores were α’s= 0.62, 0.69 and 0.92, respectively, for baseline (combined average scores across first three assessments) and α’s 0.63, 0.64 and 0.90, respectively averaged across longitudinal assessments.
Child Functional Assessment.
Child functioning was measured at each school-age assessment using the Child and Adolescent Functional Assessment Scale (CAFAS)(Hodges, 2000). The CAFAS measures psychosocial functioning and impairment in children across a variety of day-to-day functioning domains, such as home, preschool/school, and behavior toward others. The total score was used; higher scores indicate more impairment.
Observed Personality Dimensional Traits.
7,820 ratings of children during ages 3–6 years assessed thin slice personality measurements. Children were video recorded during structured Laboratory Temperament Assessment Battery (LABTAB) tasks, that include a variety of short experimenter-led structured interactions, such as playing together with a bubble-making toy (Popping Bubbles), having the child tell a story about their previous day activities while standing in front of two experimenters (Storytelling) and giving the child a transparent box with a desirable toy inside and giving incorrect ring of keys to open the box (Transparent Box; See Supplemental Table 1 for descriptions of all tasks utilized). Unacquainted observers were oriented to the thin slice procedure after given brief definitions of each of the FFM five dimensions (e.g., “extraverted: talkative, assertive, active, excitement-seeking and fun-loving”). After watching approximately 60 seconds of each experimenter-child observational task, observers rated each personality dimension (extraversion, agreeableness, conscientiousness, neuroticism and openness to experience) on a 1 (not at all) to 5 (extremely) scale. Although micro-analytic coding of temperament using the LABTAB tasks was initially commenced, it was not completed due to immense time investment necessary for multiple tasks across multiple ages. As such, given the large existing literature on observed temperament in early childhood, emerging consensus indicating temperament and personality are more alike than different (Grist & McCord, 2010) and to maintain consistency with lifespan approaches to personality, we utilized LABTAB to observationally code personality traits in very young children.
Observers included 27 undergraduate students and staff of the Early Emotional Development Program, all of whom were unacquainted with and blind to child diagnostic and demographic characteristics. 8–18 unique observers rated each child’s personality traits across 4–8 structured experimenter/child observation tasks, with an average of 25.7 (SD=5.13; Min=10, Max=33) ratings for each dimension. Ratings were then averaged across observers and across tasks for each personality dimension. Intraclass correlation coefficients (ICC) for single raters ranged from ICC=0.24–0.53, which is poor, however, thin slice ratings were averaged across 8–18 raters, and average raters (MICC=0.57; range 0.46–0.77) for a single task demonstrated moderate reliability (Koo & Li, 2016). Moreover, average rater reliability demonstrated equivalent or better magnitudes compared with adult and child studies using the thin slice methodology to assess personality (Borkenau, Mauer, Riemann, Spinath, & Angleitner, 2004; Tackett, Herzhoff, Kushner, & Rule, 2016) indicting meaningful individual differences were obtained. Moreover, cross-situational ICC’s (cross rater/cross task) were a mean of 0.82, notably higher than previous adult samples and consistent with previous older child samples (Borkenau et al., 2004; Tackett et al., 2016; Tackett et al., 2017) while thin slice observations demonstrated preliminary divergent and convergent validity with temperament (see for further details on validation in the current sample Whalen et al., 2020).
Statistical Analysis
We provide openly accessible data analysis scripts that allow to reproduce all reported results and include any information necessary to access these scripts at https://osf.io/ywnu9/. We do not provide the data needed to produce these results as participants provided data starting between 2003–2005 and we did not receive institutional approval to post anonymized data. Data will be provided from the corresponding author upon request. We report basic descriptive statistics (further descriptive statistics using this data can be accessed in two previous manuscripts using the thin slice procedure)(Gilbert et al., 2019; Whalen et al., 2020), exact p-values and confidence intervals, however, latent class analyses and multilevel models do not provide exact effect sizes, although we do provide model fit statistics instead.
We conducted latent class analysis (LCA) using Mplus version 8 to group subjects with similar preschool FFM personality dimensional ratings into distinct classes. LCA is a data-driven approach that aims to identify unobservable subgroups within a population. Models were fitted for 1 to 5 classes, and the optimal number of latent classes was determined by the Bayesian information criterion (BIC) and the Lo-Mendell-Rubin adjusted likelihood ratio test (LMR-ALRT). Models with lower BIC indicate better fit, and the LMR-ALRT assessed whether the current model was statistically superior to the model with one fewer class. Using the best fitting model-derived classes, we examined differences between latent classes in demographic indices, including sex, age, ethnicity, and a measure of socioeconomic status (income-to-needs ratio) in SPSS version 25. Significant differences in demographic variables were used as covariates in all longitudinal modeling analyses.
We then examined concurrent internalizing and externalizing (Y/N) psychiatric disorder status differences using chi-square tests, followed by individual diagnoses that comprised the internalizing/externalizing disorder status. Significant differences in concurrent psychiatric disorders were used as covariates in longitudinal models. To examine associations between types and prospective symptom trajectories, we used multilevel linear models of depression, anxiety and externalizing symptoms, and global functioning across all time points. Multilevel linear models were performed in SAS v9.4 and included random intercept and slope components with an unstructured covariance structure. Time was defined as age at each assessment wave (centered around median age 8). We controlled for sex, baseline mean age, and T1 income-to-needs ratio, baseline ADHD and CD in all analyses. To compare predictive utility of types versus dimensional traits, we completed regression analyses comparing adjusted R2 values (to account for number of predictors) using symptom severity/functioning scores averaged across all longitudinal assessments as outcomes. First, we compared two separate regression models, including all above-mentioned covariates. Second, to examine predictive utility of traits above types, we examined adjusted R2 change by comparing the model with covariates and types to a model with each of these predictors as well as traits. Third, to examine predictive utility of types above traits, we examined adjusted R2 change by comparing the model with covariates and traits to a model with each of these predictors as well as types.
RESULTS
Personality Types
Fit statistics for the LCA models with 1 to 5 latent classes are shown in Table 1. According to the LMR-ALRT, the 2-class model fit significantly better than the 1-class model (p=0.002), and the 3-class model was a significant improvement over the 2-class model (p=0.003). The 4-class model was not a statistical improvement over the 3-class model (p=0.44). The BIC continued to decrease as class number increased, although the degree of decrease in BIC was less pronounced for the 4- and 5-class models. Based on these statistics, the 3-class model was selected as the best fit.
Table 1.
Fit statistics of latent class analysis of FFM observed personality dimensions with 1 to 5 latent classes
| Number Latent Classes | BIC | LMR-ALRT p-value | Entropy | Class N’s |
|---|---|---|---|---|
| 1 | 1490.9 | -- | 1.000 | 299 |
| 2 | 1268.9 | 0.0015 | 0.799 | 89, 210 |
| 3 | 1148.1 | 0.0030 | 0.764 | 82, 100, 117 |
| 4 | 1098.6 | 0.4380 | 0.779 | 57, 61, 84, 97 |
| 5 | 1058.4 | 0.0246 | 0.812 | 35, 46, 59, 68, 91 |
Mean scores and correlations between the five personality traits by latent class are shown in Supplementary Table 1 and Figure 1. Class 1 (n=82; Probability of Class 1 assignment Mean(SD)(range)= .92(.14)(.42–1.0)) displayed higher levels of extraversion and openness, lower levels of conscientiousness and agreeableness, and relatively high levels of neuroticism, appearing to be an undercontrolled group. Class 2 (n=100; Probability of Class 2 assignment Mean(SD)(range)= .88(.15)(.50–1.0)) displayed higher agreeableness and conscientiousness, lower extraversion and openness, and relatively high neuroticism, indicating an overcontrolled type characterized by being inhibited and shy. Class 3 (n=117; Probability of Class 3 assignment Mean(SD)(range)= .88(.14)(.41–1.0)) displayed relatively high levels on all traits except neuroticism, indicating a resilient type, or a well-adjusted or socially desirable group. A multivariate generalized linear model was conducted to explore differences in personality traits between classes in SPSS version 25. The overall GLM indicated significant differences in personality traits between classes (Wilks’ λ=0.17, F(10,584)=84.29, p<0.001). Follow up ANOVAs revealed group difference across all personality dimensions (p’s<.001) with Bonferroni corrections demonstrating all groups significantly differing from each other except neuroticism, for which the undercontrolled and overcontrolled groups did not differ.
Figure 1.
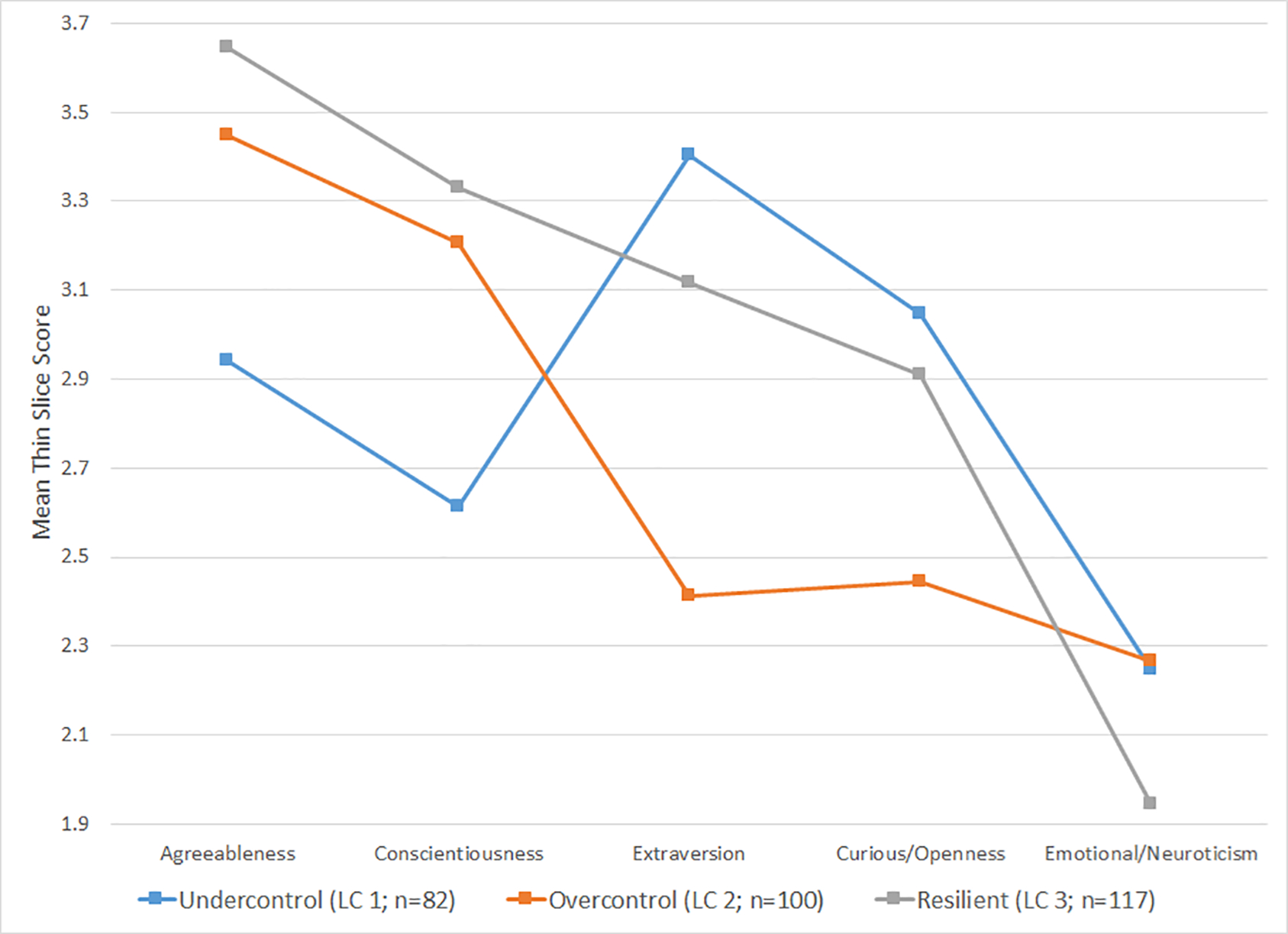
Mean scores on the FFM thin slice variables in the 3-class model
Demographic Differences
Latent classes significantly differed on age, F(2,298)=10.08, p<.001; undercontrolled children (M=5.00, SD=.88) were younger than overcontrolled (M=5.50, SD=.74) and resilient children (M=5.48, SD=.88) and sex, χ2(2)=9.29, p=.01, with higher percentages of females comprising the resilient (59%) compared with overcontrolled (43%) and undercontrolled (39%) groups. Types also differed on income-to-needs, F(2,271)=8.61, p=.002: undercontrolled children come from lower income families (M=1.72, SD=1.29) compared with resilient children. Lastly, types differed by race, χ(4)=12.28, p=.02, undercontrolled had the fewest Caucasians (40%), followed by the overcontrolled (55% Caucasian) and then resilient group (62% Caucasian). A follow-up ANOVA revealed income-to-needs significantly differed by race, F(2,271)=89.55, p<.001; Bonferroni corrections indicated Caucasians (M=2.69, SD=.81) endorsed higher income-to-needs compared with bi-racial and other minorities (M=2.13, SD=1.22) compared with Black (M=1.05, SD=.91) children. Although differences in race were evident across types, due to multicollinearity of income-to-needs and race, only income-to-needs was used as a covariate. All longitudinal analyses controlled for age, sex, and income-to-needs.
Baseline Diagnostic Differences
Personality types did not differ based on the presence of an internalizing, χ2(2)=2.08, p=.35 or externalizing disorder, χ2(2)=4.65, p=.06 (see Supplemental Figure 1, although pairwise comparisons in logistic regressions indicated significant differences in externalizing disorders, see Supplemental Table 6). Further parsing of baseline diagnostic differences demonstrated types only differed on ADHD, χ2(2)=14.51, p=.001 and CD, χ2(2)=6.72, p=.04, as the undercontrolled group demonstrated significantly higher rates of both disorders compared with the other groups (Supplemental Figure 1). No other baseline diagnostic differences were found. All longitudinal analyses controlled for baseline ADHD and CD.
Longitudinal Symptom Profiles and Functioning: RUO Personality Types
Results of the longitudinal multilevel models of psychiatric outcomes by RUO types are shown in Table 2 (growth models without predictors in Supplemental Table 3). The undercontrolled type demonstrated significantly higher externalizing symptoms and worse functioning scores (higher scores signify worse functioning) compared to resilient children (Supplemental Figure 2). There were no significant differences between the resilient or undercontrolled types compared with the overcontrolled type. Next, a personality type by time interaction was added to all models, to test if childhood type predicted changes in symptoms during childhood and adolescence. Each of these terms was not significant; symptom and functioning trajectories did not differ by personality type.
Table 2.
Multilevel Models of Depression, Externalizing and Anxiety Symptoms and Global Functioning by Personality Types (N=274)
| Estimate | SE | 95% CI of Est. | t | p | |
|---|---|---|---|---|---|
| DV: Depression Core Severity Score | |||||
| Intercept | 2.00 | 0.16 | (1.69, 2.32) | 12.43 | <0.0001 |
| Female gender | −0.03 | 0.15 | (−0.32, 0.26) | −0.21 | 0.84 |
| Baseline Mean age | 0.24 | 0.09 | (0.06, 0.42) | 2.66 | 0.01 |
| Baseline income-to-needs ratio | −0.08 | 0.06 | (−0.21, 0.04) | −1.29 | 0.20 |
| ADHD | 1.13 | 0.18 | (0.78, 1.48) | 6.39 | <0.0001 |
| Conduct disorder | 0.78 | 0.19 | (0.41, 1.14) | 4.20 | <0.0001 |
| Undercontrol vs. Resilient | 0.19 | 0.20 | (−0.20, 0.57) | 0.94 | 0.35 |
| Overcontrol vs. Resilient | −0.03 | 0.17 | (−0.36, 0.30) | −0.19 | 0.85 |
| Time | 0.06 | 0.02 | (0.02, 0.09) | 3.53 | 0.0005 |
| Time squared | −0.01 | 0.01 | (−0.02, 0.00) | −1.66 | 0.10 |
| DV: Externalizing Dimensional Score | |||||
| Intercept | 2.75 | 0.47 | (1.82, 3.67) | 5.85 | <0.0001 |
| Female gender | −0.22 | 0.43 | (−1.07, 0.62) | −0.52 | 0.60 |
| Baseline Mean age | 0.54 | 0.26 | (0.02, 1.06) | 2.03 | 0.043 |
| Baseline income-to-needs ratio | −0.21 | 0.19 | (−0.58, 0.16) | −1.10 | 0.27 |
| ADHD | 7.88 | 0.51 | (6.87, 8.89) | 15.31 | <0.0001 |
| Conduct disorder | 5.08 | 0.54 | (4.02, 6.15) | 9.44 | <0.0001 |
| Undercontrol vs. Resilient | 1.14 | 0.57 | (0.01, 2.27) | 1.99 | 0.05 |
| Overcontrol vs. Resilient | −0.25 | 0.49 | (−1.21, 0.71) | −0.51 | 0.61 |
| Time | −0.32 | 0.04 | (−0.40, −0.24) | −7.45 | <0.0001 |
| Time squared | −0.03 | 0.01 | (−0.05, −0.00) | −2.04 | 0.04 |
| DV: Anxiety Dimensional Score | |||||
| Intercept | 0.92 | 0.19 | (0.56, 1.29) | 4.95 | <0.0001 |
| Female gender | 0.28 | 0.17 | (−0.05, 0.61) | 1.69 | 0.09 |
| Baseline Mean age | 0.29 | 0.10 | (0.08, 0.49) | 2.76 | 0.01 |
| Baseline income-to-needs ratio | −0.07 | 0.07 | (−0.21, 0.07) | −0.96 | 0.34 |
| ADHD | 0.43 | 0.20 | (0.04, 0.82) | 2.20 | 0.03 |
| Conduct disorder | 0.43 | 0.21 | (0.02, 0.84) | 2.06 | 0.04 |
| Undercontrol vs. Resilient | 0.37 | 0.23 | (−0.07, 0.82) | 1.65 | 0.10 |
| Overcontrol vs. Resilient | −0.04 | 0.19 | (−0.41, 0.33) | −0.22 | 0.82 |
| Time | −0.22 | 0.02 | (−0.26, −0.18) | −10.71 | <0.0001 |
| Time squared | 0.01 | 0.01 | (−0.01, 0.02) | 1.04 | 0.30 |
| DV: Global Functioning Score | |||||
| Intercept | 9.94 | 2.24 | (5.53, 14.35) | 4.44 | <0.0001 |
| Female gender | −1.21 | 2.07 | (−5.30, 2.87) | −0.58 | 0.56 |
| Baseline Mean age | 4.97 | 1.27 | (2.48, 7.46) | 3.93 | 0.0001 |
| Baseline income-to-needs ratio | 0.15 | 0.90 | (−1.61, 1.92) | 0.17 | 0.87 |
| ADHD | 19.26 | 2.46 | (14.42, 24.11) | 7.83 | <0.0001 |
| Conduct disorder | 20.85 | 2.69 | (15.73, 25.96) | 8.03 | <0.0001 |
| Undercontrol vs. Resilient | 8.90 | 2.78 | (3.42, 14.37) | 3.20 | 0.02 |
| Overcontrol vs. Resilient | 1.00 | 2.33 | (−3.59, 5.60) | 0.43 | 0.67 |
| Time | −2.10 | 0.19 | (−2.47, −1.71) | −10.91 | <0.0001 |
| Time squared | 0.23 | 0.06 | (0.11, 0.34) | 3.95 | <0.0001 |
Note: Comparisons of Overcontrol vs. Undercontrol were non-significant in all models. Higher scores of global functioning indicate more impairment.
In addition, time was significantly associated with each dependent variable: depression severity scores linearly increased and anxiety scores linearly decreased as subjects aged while externalizing and functioning scores demonstrated non-linear quadratic trajectories. Older baseline age was significantly associated with elevated scores in all models. No outcomes significantly differed by sex or income-to-needs.
Types versus Traits
To address utility of types compared to continuous traits, adjusted R2 between types and traits in separate models were examined in a series of regression models. Types accounted for more variance in depressive and externalizing symptoms and functioning while traits accounted for more variance in anxiety symptoms (Table 3). Next, to examine the predictive validity of traits over types, we examined the additional variance explained by traits over a model with covariates and types. R2 change was only significant for anxiety symptoms, with agreeableness predicting symptoms (β=.32, t=2.87, p=.004; full regression results in Supplemental Table 4). Traits did not provide any additional predictive utility for depression, externalizing symptoms and functioning once accounting for types. As a supplemental analysis, we also examined the predictive validity of types over traits, examining the additional variance explained by types over a model with covariates and traits, demonstrating that R2 was only significant for anxiety symptoms again, with the undercontrolled group predicting elevated symptoms (β=.26, t=2.70, p=.007; Supplemental Table 5).
Table 3.
Adjusted R2 of types and dimensional traits predicting symptoms and functioning averaged across longitudinal assessments
| Model 1 | Model 2 | Model 3 | |
|---|---|---|---|
| Type | Traits | Traits (over types) | |
| Anxiety | .122 | .132 | .150* |
| Depression | .327 | .326 | .324 |
| Externalizing | .612** | .611* | .612 |
| Functioning | .399* | .397 | .398 |
Note: Model 1 is the predictive utility of types, Model 2 is the predictive utility of traits. Model 3 examined the predictive utility of traits over and above types. All models include covariates of mean baseline age, sex, baseline income to needs, baseline ADHD and baseline CD. Significance values are F change for each model.
p<.05
p<.01
DISCUSSION
The current study demonstrated that observed thin-slice FFM personality traits organize into the resilient, undercontrolled and overcontrolled (RUO) personality types as early as the preschool period of development (ages 3–6). Second, types demonstrate far-reaching impact on psychopathology into adolescence. RUO personality types observed in a clinically enriched preschool-aged sample of children demonstrated that the undercontrolled personality type was associated with concurrent externalizing disorders and, over and above the influence of baseline disorders, personality type continued to predict higher externalizing symptoms and worse global functioning across child development. Lastly, types and dimensions provided similar predictive utility. Findings suggest preschool personality types are early emerging, can be identified using observational indices, and demonstrate associations with psychiatric developmental outcomes across childhood.
Building from prior research identifying RUO personality types in young children using parent report and similar patterns using FFM dimensions in older children, adolescents and adults, (Caspi, 2000; Donnellan & Robins, 2010; Komsi et al., 2006; Specht et al., 2014), the current study provides the first observed identification of the RUO types using the FFM dimensions in a clinically heterogeneous preschool sample. Observational ratings have proven difficult to identify and replicate the RUO types in past literature (Donnellan & Robins, 2010), however, current findings indicate observed FFM personality dimensions in preschoolers organize together to create types well defined in older children and adults. Utilizing the FFM as the basis of the types provides consistency with adolescent and adult RUO literature, and by focusing on personality rather than temperament, findings fit within a lifespan approach to understanding the influence of personality across development (Jackson & Hill, 2019). Moreover, we replicated the RUO types using latent class analysis, a more sophisticated model-based analytical technique than Q-factor (Asendorpf & van Aken, 1999) and cluster analysis (Komsi et al., 2006). Third, we replicated the RUO types across a clinically heterogeneous sample of preschoolers. Previous research has detected these types in convenience or community samples, yet given the strong link between child personality and psychopathology (De Fruyt et al., 2017), it is important to verify that types are consistent across samples.
The preschool undercontrolled personality type was associated with two concurrent externalizing disorders, ADHD and CD. High extraversion and openness and low agreeableness and conscientiousness differentiated the undercontrolled group from the resilient and overcontrolled groups and many of these tendencies overlap with symptoms of ADHD and CD. A spectrum theory of personality purports that personality and pathology exist on a spectrum from normal to extreme (Widiger & Smith, 2008) with recent work indicating overlap of latent structure of the two constructs (Mike, King, Oltmanns, & Jackson, 2018). Concurrent findings support this theory. Additionally, above and beyond baseline diagnoses, an undercontrolled preschool personality type independently predicted continued externalizing and functioning trajectories compared with resilient and overcontrolled children across development. Findings are consistent with past research indicating undercontrolled children and adolescents demonstrate high externalizing problems, although did not indicate moderate internalizing problems (Donnellan & Robins, 2010; Van den Akker et al., 2013).
Although overcontrolled children often exhibit elevated internalizing symptoms (Asendorpf & van Aken, 1999; Robins et al., 1996) overcontrolled children showed no psychiatric differences compared with resilient children. Although unexpected, the current sample was clinically heterogeneous, highly comorbid, and oversampled for preschool depression, possibly indicating that in the context of severe early psychopathology, overcontrolled children are not as easily distinguishable from resilient children. Conversely, these findings might also suggest the overcontrolled and resilient preschoolers display a constellation of personality traits that act as a protective mechanism for later psychiatric symptoms in childhood in the presence of early diagnoses. Of note, overcontrolled children exhibited significantly higher neuroticism than the resilient children. As such, we speculate the overcontrolled personality type might confer developmental adaptions for young children while maladaptive outcomes might become evident only later in adolescence and adulthood, or, in other life areas, such as socially.
Indeed, identifying RUO personality types in a clinical sample of preschoolers provides an additional aspect of personality that was associated with risk or resilience. Although there has been recent interest in utilizing identified types, including biotypes (Clementz et al., 2015) and personality types (Gerlach, Farb, Revelle, & Nunes Amaral, 2018) to predict outcomes, the prevailing adult personality literature promotes a dimensional model using the FFM or related traits (Reed et al., 2019; Widiger & Trull, 2007). However, the personality type model is not orthogonal to this perspective, especially in developmental samples. First, as found in the current sample, FFM dimensions are less pronounced in early childhood (Mõttus, Soto, & Slobodskaya, 2017), suggesting it may be warranted to examine constellations of personality traits in developmental samples. Second, the types do not necessarily promote categorical classification. Rather, types can be conceptualized dimensionally, such that children vary on how overcontrolled or undercontrolled they are, as evidenced by the latent class analysis, which provides the probability of each individual being in a latent class. Indeed, children will vary on their prototypical “undercontrolled-ness,” for instance; more extreme manifestations of these types might demonstrate stronger associations with psychopathology. Stated otherwise, being in the undercontrolled or overcontrolled groups is not inherently maladaptive, but rather, similar to spectrum models of personality (Widiger & Smith, 2008), is a dimensional constellation of personality tendencies that may confer risk or protection for various pathologies. Third, when trait dimensions with the most predictive power are combined, predictive power is even greater, highlighting the unique validity of examining trait dimensions in combination, especially from a developmental perspective.
Comparing predictive validity of types versus dimensions, findings suggest types and dimensions both provided useful information. Incremental analyses demonstrated that types better predicted externalizing symptoms and functioning while dimensions better predicted anxiety. However, incremental validity (R2) was almost identical, demonstrating that types and traits provide very similar ability to predict psychopathology across the lifespan. This parallels results from our previous study examining dimensions and longitudinal psychopathology which found that above baseline pathology, neuroticism predicted externalizing symptoms while conscientiousness predicted depressive symptoms (Gilbert et al., 2019). Together, findings demonstrate slightly different associations using dimensions and types and that personality strongly predicts externalizing symptoms, although, does not clarify whether dimensions or types are stronger predictors.
Limitations of the current study should be noted. First, the sample was enriched for preschool depression and many preschoolers had clinical disorders at baseline. The severity of the sample may indicate a lack of generalizability to community samples and the resilient type may not be entirely resilient given the restricted range of healthy children. Additionally, neuroticism ratings were lower and less variable than expected, possibly because we oversampled for internalizing disorders or because neuroticism is more difficult to observationally assess in young children (Borkenau et al., 2004). Related, given many of the children had baseline diagnoses, causal relationships between preschool personality and initial onset of psychopathology cannot be determined, and as mentioned, may be due to a spectrum model where personality and psychopathology share a bi-directional relationship. Second, our assessment was an observed measure of personality, and behaviors indexed might have tapped into both traits and symptoms, although this is an issue whenever observational methods identifying personality are employed. Related, although the observed measure of personality was conducted across three separate time points, the thin slice technique might have also indexed age, as the undercontrolled group was younger than the other two. Given the importance of integrating development in personality assessment, this is an area for future investigation. Third, correlations between the dimensional traits were high, possibly due to method overlap, questioning the distinctiveness of each trait used to create the personality types while findings from the latent class analysis could be due to high intercorrelations of dimensional personality. Fourth, we observationally coded the “Big 5” personality dimensions, rather than the “Little 6,” which includes activity as a sixth childhood personality dimension (Soto & Tacket, 2015). Although this was done to maintain consistency across lifespan approaches to personality, we may have missed meaningful information by not including this sixth dimension. Lastly, we did not include a parent-reported measure of the FFM in preschool-aged children and so are unable to compare whether latent classes could be derived from parent report compared with observed FFM. However, this also speaks to our ability to capitalize on existing video recorded observations to assess preschool personality when it was not otherwise assessed. Researchers without parent or teacher-reported personality assessments could similarly utilize this method to assess personality types and dimensions in secondary data analyses of otherwise rich datasets.
Despite these limitations, the current study benefited from a large sample of intensive observational data that were followed prospectively for approximately a decade. Findings illustrate that observed personality clusters into the well-established RUO types in children as young as preschool. Moreover, these personality types were associated with concurrent diagnostic status and prospectively predicted symptoms and functioning. Although, identifying the individual FFM dimensions may be the most parsimonious assessment of personality in young children, being able to conceptualize the patterns of these individual dimensions into personality types may provide an equally important additional metric that denotes psychiatric risk or protection. Moreover, given these types exist on a dimensional spectrum themselves, extremely high overcontrolled or undercontrolled presentations early in development might provide a nuanced and important early identification marker that could lend itself to specific forms of intervention.
Supplementary Material
Acknowledgements
All phases of this study were supported by NIH Grant: R01MH064769-06A1. Dr. Gilbert’s work was supported by NIH Grants: K23MH115074-01 (PI: Gilbert) and T32MH100019 (PI’s: Barch and Luby). Dr. Whalen’s work was supported by NIH grants: L30MH108015 (PI: Whalen), K23MH118426-01 (PI: Whalen) and T32MH100019 (PI’s: Barch and Luby). The sponsors did not play any role in study design, collection, analysis, interpretation of data, writing report or decision to submit the article for publication. The authors wish to thank the children and caregivers of the Preschool Depression Study for their time and dedication to this project and the staff and students of the Preschool Depression Study for their tireless efforts in the coding of preschool personality traits.
The Institutional Review Board at WUSM approved all procedures in accordance with ethical guidelines.
Footnotes
Conflict of Interest
Drs. Gilbert, Whalen, Jackson, Barch and Luby and Ms. Tillman report no conflict of interests.
REFERENCES
- Ambady N, Bernieri FJ, & Richeson JA (2000). Toward a histology of social behavior: judgemental accuracy from thin slices of the beavioral stream. In Zanna M (Ed.), Advances in Experimental Social Psychology. San Diego, CA: Academic. [Google Scholar]
- Angold A, & Costello EJ (2000). The Child and Adolescent Psychiatric Assessment (CAPA). Journal of American Academy of Child and Adolescent Psychiatry, 39(1), 39–48. [DOI] [PubMed] [Google Scholar]
- Asendorpf JB (2003). Head-to-head comparison of the predictive validity of personality types and dimensions. European Journal of Personality, 17, 327–346. [Google Scholar]
- Asendorpf JB, Borkenau P, Ostendorf F, & Van Aken MAG (2001). Carving personality description at its joints: Confirmation of three replicable personality prototypes for both children and adults. European Journal of Personality, 15(3), 169–198. [Google Scholar]
- Asendorpf JB, & Denissen JJ (2006). Predictive validity of personality types versus personality dimensions from early childhood to adulthood: Implications for the distinction between core and surface traits. Merrill-Palmer Quarterly-- Journal of Developmental Psychology, 52, 486–513. [Google Scholar]
- Asendorpf JB, Denissen JJ, & van Aken MA (2008). Inhibited and aggressive preschool children at 23 years of age: Personality and social transitions into adulthood. Dev Psychol, 44(4), 997–1011. [DOI] [PubMed] [Google Scholar]
- Asendorpf JB, & van Aken MA (1999). Resilient, overcontrolled, and undercontrolled personality prototypes in childhood: Replicability, predictive power, and the trait-type issue. Journal of Personality and Social Psychology, 77, 815–832. [DOI] [PubMed] [Google Scholar]
- Beck ED, & Jackson JJ (2019). Consistency and change in idiographic personality: A longitudinal ESM network study. Journal of Personality and Social Psychology. [DOI] [PubMed] [Google Scholar]
- Borkenau P, Mauer N, Riemann R, Spinath FM, & Angleitner A (2004). Thin slices of behavior as cues of personality and intelligence. Journal of Personality and Social Psychology, 86, 599–614. doi: 10.1037/0022-3514.86.4.599 [DOI] [PubMed] [Google Scholar]
- Caspi A (2000). The child is father of the man: Personality continuities from childhood to adulthood. Journal of Personality and Social Psychology, 78(1), 158–172. [DOI] [PubMed] [Google Scholar]
- Caspi A, Roberts BW, & Shiner RL (2005). Personality development: Stability and change. Annual Review of Psychology, 56, 453–484. [DOI] [PubMed] [Google Scholar]
- Caspi A, & Shiner RL (2006). Personality development. In Damon W, Lerner R, & Eisenberg N (Eds.), Handbook of child psychology (6th ed., Vol. 3 Social emotional and personality development, pp. 300–364). New York: Wiley. [Google Scholar]
- Caspi A, & Silva PA (1995). Temperamental qualities at age three predict personality traits in young adulthood: Longitudinal evidence from a birth cohort. Child Development, 66, 486–498. doi: 10.2307/1131592 [DOI] [PubMed] [Google Scholar]
- Clementz BA, Sweeney JA, Hamm JP, Ivleva EI, Ethridge LE, Pearlson GD, … Tamminga CA (2015). Identification of Distinct Psychosis Biotypes Using Brain-Based Biomarkers. American Journal of Psychiatry, 173(4), 373–384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costa P Jr, Herbst JH, McCrae RR, Samuels J, & Ozer DJ (2002). The replicability and utility of three personality types. European Journal of Personality(16), S73–S87. [Google Scholar]
- Costa PT, & McCrae RR (1992). Professional Manaul: Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI). Odessa, FL: Psychological Assessment Resources. [Google Scholar]
- De Bolle M, Beyers W, De Clercq B, & De Fruyt F (2012). General personality and psychopathology in referred and nonreferred children and adolescents: An investigation of continuity, pathoplasty and complication models. Journal of Abnormal Psychology, 121(4), 958. doi: 10.1037/a0027742.supp [DOI] [PubMed] [Google Scholar]
- De Clercq B, De Fruyt F, & Widiger TA (2009). Integrating a developmental perspective in dimensional models of personality disorders. Clinical Psychology Review, 29(2), 154–162. doi: 10.1016/j.cpr.2008.12.002 [DOI] [PubMed] [Google Scholar]
- De Fruyt F, De Clercq B, & De Bolle M (2017). The five-factor model of personality and consequntial outcomes in childhood and adolescence. In Widiger TA (Ed.), The Oxford Handbook of the Five Factor Model (pp. 507–520). New York: Oxford University Press. [Google Scholar]
- Donnellan BM, & Robins RW (2010). Resilient, overcontrolled and undercontrolled personality types: Issues and controversies. Social and Personality Psychology Compass, 3, 1–14. [Google Scholar]
- Egger HL, Erkanli A, Keeler G, Potts E, Walter BK, & Angold A (2006). Test-retest reliability of the Preschool Age Psychiatric Assessment (PAPA). Journal of American Academy of Child and Adolescent Psychiatry, 45(5), 538–549. [DOI] [PubMed] [Google Scholar]
- Gerlach M, Farb B, Revelle W, & Nunes Amaral LA (2018). A robust data-driven approach identifies four personality types across four large data sets. Nature Human Behaviour, 2(10), 735–742. doi: 10.1038/s41562-018-0419-z [DOI] [PubMed] [Google Scholar]
- Gilbert KE, Whalen DJ, Tillman R, Barch DM, Luby J, & Jackson JJ (2019). Observed personality in preschool: Associations with current and longitudinal symptoms. Journal of Abnormal Child Psychology. doi: 10.1007/s10802-019-00567-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grist CL, & McCord DM (2010). Individual differences in preschool children: Temperament or personality? Infant and Child Development, 19, 264–274. doi: 10.1002/icd.663 [DOI] [Google Scholar]
- Hart D, Atkins R, Fegley S, Robins RW, & Tracy JL (2003). Personality and development in childhood: A person-centered approach. Monographs of the Society for Research in Child Development, 68, i–122. [PubMed] [Google Scholar]
- Hodges K (2000). CAFAS Self-Training Manual. Ann Arbor MI: Kay Hodges. [Google Scholar]
- Jackson JJ, & Hill PL (2019). Lifespan development of conscientiousness. In McAdams DP, Shiner RL, & Tackett JL (Eds.), Handbook of Personality Across the Lifespan. New York: Guilford Press. [Google Scholar]
- Klimstra TA, Hale Iii WW, Raaijmakers QAW, Branje SJT, & Meeus WHJ (2010). A developmental typology of adolescent personality. European Journal of Personality, 24(4), 309–323. doi: 10.1002/per.744 [DOI] [Google Scholar]
- Komsi N, Räikkönen K, Pesonen A-K, Heinonen K, Keskivaara P, Järvenpää A-L, & Strandberg TE (2006). Continuity of temperament from infancy to middle childhood. Infant Behavior and Development, 29(4), 494–508. [DOI] [PubMed] [Google Scholar]
- Koo TK, & Li MY (2016). A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. Journal of chiropractic medicine, 15(2), 155–163. doi: 10.1016/j.jcm.2016.02.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kotov R, Gamez W, Schmidt F, & Watson D (2010). Linking “Big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin, 136(5), 768–821. doi: 10.1037/a0020327 [DOI] [PubMed] [Google Scholar]
- Luby JL, Belden AC, Pautsch J, Si X, & Spitznagel E (2009). The clinical significance of preschool depression: Impairment in functioning and clinical markers of the disorder. Journal of Affective Disorders, 112, 111–119. doi: 10.1016/j.jad.2008.03.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luby JL, Heffelfinger A, Koenig-McNaught AL, Brown K, & Spitznagel E (2004). The Preschool Feelings Checklist: A brief and sensitive screening measure for depression in young children. Journal of American Academy of Child and Adolescent Psychiatry, 43(6), 708–717. doi: 10.1097/01.chi.0000121066.29744.08 [DOI] [PubMed] [Google Scholar]
- Luby JL, Si Z, Belden AC, Tandon M, & Spitznagel E (2009). Preschool depression: Homotypic continuity and course over 24 months. Archives of General Psychiatry, 66(8), 897–905. doi: 10.1001/archgenpsychiatry.2009.97 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maher BA, & Maher WB (1994). Personality and psychopathology: A historical perspective. Journal of Abnormal Psychology, 103(1), 72–77. doi: 10.1037/0021-843X.103.1.72 [DOI] [PubMed] [Google Scholar]
- Mike A, King H, Oltmanns T, & Jackson JJ (2018). Obsessive, compulsive and conscientious? The relationship between OCPD and personality traits. Journal of Personality, 86, 952–972. [DOI] [PubMed] [Google Scholar]
- Mõttus R, Soto CJ, & Slobodskaya HR (2017). Are All Kids Alike? The Magnitude of Individual Differences in Personality Characteristics Tends to Increase from Early Childhood to Early Adolescence. European Journal of Personality, 31(4), 313–328. doi: 10.1002/per.2107 [DOI] [Google Scholar]
- Prokasky A, Rudasill K, Molfese VJ, Putnam S, Gartstein M, & Rothbart M (2017). Identifying child temperament types using cluster analysis in three samples. Journal of Research in Personality, 67, 190–201. doi: 10.1016/j.jrp.2016.10.008 [DOI] [Google Scholar]
- Reed GM, First MB, Kogan CS, Hyman SE, Gureje O, Gaebel W, … Saxena S (2019). Innovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disorders. World Psychiatry, 18(18), 3–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robins RW, John OP, & Caspi A (1998). The typological approach to studying personality. In Cairns RB, Bergman LR, & Kagan J (Eds.), Methods and models for studying the individual (pp. 135–160). Thousand Oaks, CA: Sage Publications. [Google Scholar]
- Robins RW, John OP, Caspi A, Moffitt TE, & Stouthamer-Loeber M (1996). Resilient, overcontrolled, and undercontrolled boys: Three replicable personality types. Journal of Personality and Social Psychology, 70(1), 157–171. doi: 10.1037/0022-3514.70.1.157 [DOI] [PubMed] [Google Scholar]
- Soto CJ, & Tacket JL (2015). Personality Traits in Childhood and Adolescence. Current Directions in Psychological Science, 24(5), 358–362. doi: 10.1177/0963721415589345 [DOI] [Google Scholar]
- Specht J, Luhmann M, & Geiser C (2014). On the consistency of personality types across adulthood: latent profile analyses in two large-scale panel studies. J Pers Soc Psychol, 107(3), 540–556. doi: 10.1037/a0036863 [DOI] [PubMed] [Google Scholar]
- Tacket JL, Lang JWB, Markon KE, & Herzhoff K (2019). A correlated traits, correlated methods model for thin-slice child personality assessment. Psychological Assessment, 31(4), 545–556. doi: 10.1037/pas0000635 [DOI] [PubMed] [Google Scholar]
- Tackett JL (2006). Evaluating models of the personality-psychopathology relationship in children and adolescents. Clin Psychol Rev, 26(5), 584–599. doi: 10.1016/j.cpr.2006.04.003 [DOI] [PubMed] [Google Scholar]
- Tackett JL, Herzhoff K, Kushner SC, & Rule N (2016). Thin slices of childhood personality: Perceptual, situational and behavioral contributions. Journal of Personality and Social Psychology, 110, 150–166. doi: 10.1037/pspp0000044 [DOI] [PubMed] [Google Scholar]
- Tackett JL, Smack AJ, Herzhoff K, Rearson KW, Daoud S, & Granic I (2017). Measuring child personality when child personality was not measured: Application of a thin-slice approach. Personality and Mental Health, 11(4), 4–17. doi: 10.1002/pmh.1351 [DOI] [PubMed] [Google Scholar]
- Van den Akker AL, Deković M, Asscher JJ, Shiner RL, & Prinzie P (2013). Personality types in childhood: Relations to latent trajectory classes of problem behavior and overreactive parenting across the transition into adolescence. Journal of Personality and Social Psychology, 104(4), 750–764. doi: 10.1037/a0031184 [DOI] [PubMed] [Google Scholar]
- Weir RC, & Gjerde PR (2002). Preschool personality prototypes: Internal coherence, cross-study replicability, and developmental outcomes in adolescence. Personality and Social Psychology Bulletin, 28, 1229–1241. [Google Scholar]
- Whalen DJ, Gilbert KE, Jackson JJ, Barch DM, & Luby JL (2020). Using a Thin Slice Coding Approach to Assess Preschool Personality Dimensions. Journal of Personality Assessment, 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Widiger TA, & Smith GT (2008). Personality and psychopathology. In John OP, Robins RW, & Pervin LA (Eds.), Handbook of Personality: Theory and Research (3rd ed., pp. 743–769). New York: Guilford. [Google Scholar]
- Widiger TA, & Trull TJ (2007). Plate tectonics in the classifcation of personality disorder: Shifting to a dimensional model. American Psychologist, 62(2), 71–83. [DOI] [PubMed] [Google Scholar]
- Wilson S, Schalet BD, Hicks BM, & Zucker RA (2013). Identifying early childhood personality dimensions using the California child Q-sort and prospective associations with behavioral and psychosocial development. Journal of Research on Personality, 47. doi: 10.1016/j.jrp.2013.02.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zentner M, & Shiner RL (2012). Fifty years of progress in temperament research: A synthesis of major themes, findings and challenges and a look forward. In Zentner M & Shiner RL (Eds.), Handbook of Temperament (pp. 673–700). NY: Guilford Press. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.