

ABSTRACT
Traditional culture-based methods for identification and antimicrobial susceptibility testing (AST) of bacteria take 2 to 3 days on average. Syndromic molecular diagnostic panels have revolutionized clinical microbiology laboratories as they can simultaneously identify an organism and detect some of the most significant antimicrobial resistance (AMR) genes directly from positive blood culture broth or from various specimen types (e.g., whole blood, cerebrospinal fluid, and respiratory specimens). The presence or absence of an AMR marker associated with a particular organism can be used to predict the phenotypic AST results to more rapidly guide therapy. Numerous studies have shown that genotypic susceptibility predictions by syndromic panels can improve patient outcomes. However, an important limitation of AMR marker detection to predict phenotype is the potential discrepancies that may arise upon performing phenotypic AST of the recovered organism in culture. The focus of this minireview is to address how clinical laboratories should interpret rapid molecular results from commercial platforms in relation to phenotypic AST. Stepwise approaches and solutions are provided to resolve discordant results between genotypic and phenotypic susceptibility results.
KEYWORDS: antimicrobial resistance, antimicrobial susceptibility testing, molecular methods, predictions
INTRODUCTION
Diagnostic tools that offer rapid turnaround times (TATs) can have a significant clinical impact, particularly in patients with bloodstream infections (BSIs) (1, 2). Blood cultures with nonfastidious organisms often turn positive within 24 h postincubation, and the first opportunity to narrow or tailor the initial empirical therapy is based on the Gram stain result. Concurrently, blood culture broth is subcultured onto agar media and incubated for an additional 18 to 24 h (3). To deliver prompt identification of microorganisms grown in blood cultures, matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS) was introduced as a rapid method for the identification of bacterial organisms directly from positive blood culture broth or growth on solid media, leading to reductions in TATs (4). This combination of organism identification and institution-specific antibiograms can be used as a therapeutic decision point, but to appropriately target antimicrobial therapy, antimicrobial susceptibility testing (AST) through manual methods (e.g., disk diffusion, gradient diffusion, or broth microdilution methods) or automated systems (e.g., Vitek [bioMérieux, Durham, NC], Phoenix [Becton, Dickinson, Sparks, MD], and Microscan [Beckman Coulter, Sacramento, CA]) must be performed on pure, cultured isolates, which still require up to a total of 2 to 3 days for actionable results, a major barrier for clinicians (5). Further delays can take place if the culture is mixed, has insufficient growth, or contains a fastidious organism.
Syndromic molecular diagnostic panels have been a game-changer in the field as they can simultaneously identify the organism and detect some of the most significant antimicrobial resistance (AMR) genes directly from specimens. The presence or absence of an AMR marker associated with a particular organism can be used to predict the phenotypic AST results to more rapidly guide therapy. There are a number of tests cleared by the U.S. Food and Drug Administration (FDA) that can detect organisms and/or the respective AMR genes either from isolates after cultured growth (e.g., from positive blood culture broth or solid media) or directly from specimens (e.g., whole blood, cerebrospinal fluid, and respiratory samples) (6). A variety of molecular tests also exist for the detection of antimicrobial-resistant organisms or specific AMR markers for infection prevention and control purposes (i.e., surveillance cultures).
Several studies have shown that genotypic predictions of susceptibility results can improve patient outcomes. This is particularly true when the implementation of rapid molecular panels is combined with antimicrobial stewardship initiatives (1, 2). The turnaround time for identifying the pathogen and its associated AMR determinants after the implementation of a molecular panel has been shown to be at least 1.5 days faster than conventional testing for pathogen identification and routine AST (7). For example, detection of Staphylococcus aureus in the absence of the mecA gene can be predictive of methicillin (oxacillin)-susceptible S. aureus (MSSA), leading to opportunities for deescalation to a preferred agent such as oxacillin and discontinuation of vancomycin therapy a day earlier than with conventional methods. Alternatively, the detection of vancomycin-resistant enterococci (VRE) through the detection of vanA or vanB and Enterococcus species targets can prompt the escalation of antimicrobial therapy to agents such as daptomycin. The implementation of BSI molecular panels has been shown to reduce the inpatient length of stay, including intensive care unit (ICU) duration; hospital costs; and the duration of unnecessary antimicrobials (7–9).
An important limitation of rapid genotypic AMR detection using molecular panels is the potential discrepancies that may arise upon performing phenotypic AST of the recovered organism in culture. These discrepancies may have detrimental effects on patients as they may lead to inappropriate deescalation of antimicrobials or unnecessary escalation/exposure to broad-spectrum therapy. Thus, the focus of this minireview is to address how clinical laboratories should interpret rapid molecular results in relation to phenotypic AST. Stepwise approaches and solutions are provided to resolve discordant results between genotypic and phenotypic susceptibility results.
COMPARISON OF GENOTYPIC VERSUS PHENOTYPIC RESISTANCE DETECTION
Although dubbed “molecular,” genotypic tests utilize a variety of technologies such as reverse transcriptase PCR (RT-PCR), peptide nucleic acid fluorescence in situ hybridization (PNA-FISH), nested PCR, microarrays, and DNA hybridization. Genotypic detection is a constantly growing and changing field compared to traditional phenotypic methodologies (e.g., broth dilution and disk diffusion methods) that have become highly standardized over the decades. Aside from their rapidity, molecular methods allow the detection of both etiological agents and AMR genes even when the growth of the organism is difficult or not possible by growth-dependent, phenotypic tests. Genotypic testing does not depend on live cells for detection, which is ideal for patients who are already undergoing antimicrobial therapy since the growth of the live organism may be suppressed. Contrary to genotypic methods, which can be performed directly from specimens and isolates with a TAT of 1 to 5 h, conventional phenotypic tests are growth dependent and have a TAT of up to 48 h. Providers are typically more comfortable with and reliant on phenotypic methods after decades of interpreting results from such methods. Reports of phenotypic AST offer a profile of antimicrobial agents and their susceptibility results. Such reports may provide the MIC or disk zone diameter of each agent and their respective interpretations (e.g., S [susceptible] or R [resistant]) according to established Clinical and Laboratory Standards Institute (CLSI), FDA, or European Committee on Antimicrobial Susceptibility Testing (EUCAST) clinical breakpoints (10–12). On the other hand, genotypic detection methods are dependent on the molecular targets and are based on the assumption that the detected antimicrobial resistance genes convey elevated MICs that fall in the intermediate or, more often, the resistant interpretive category. Genotypic methods provide information regarding the mechanisms of antimicrobial resistance. While different laboratories have their own reporting structures, reporting simply “detected” or “not detected” for a specific molecular target will be less helpful as providers may not be well versed in the growing list of molecular mechanisms of AMR. We recommend that laboratories report results with an interpretative comment and relay the appropriate messages regarding AMR that are understandable by the patient-facing clinical team (e.g., detection of both S. aureus and mecA can be interpreted and reported as methicillin-resistant S. aureus). Communication between providers and the laboratory or antimicrobial stewardship team to generate appropriate comments would be ideal to ensure that accurate interpretation is achieved.
Despite their advantages, the ability of molecular panels to predict susceptibility is fully dependent on their list of targets and our understanding of mechanisms of resistance. For some antimicrobials, the lack of detection of an AMR marker does not necessarily indicate susceptibility because the mechanism of AMR may not be included as a target on molecular panels. In general, for Gram-positive organisms, a single mechanism of resistance accounts for most clinically significant resistance (e.g., mecA for methicillin-resistant S. aureus [MRSA] and vanA/B for VRE), and accuracies from 98 to 100% have been reported for predictions of susceptibility profiles (13–15). In contrast, predicting AMR among Gram-negative organisms is more complex as mechanisms are heterogeneous and results in lower accuracies, especially for predicting susceptibility due to the absence of an AMR gene(s). For example, the absence of blaCTX-M and blaKPC does not always equate to susceptibility to the cephalosporins and carbapenems, respectively, as off-panel mechanisms (e.g., porin loss, efflux pump, other extended-spectrum beta-lactamase [ESBL] or carbapenemase variants, and inducible or plasmid-mediated AmpC, etc.) may still result in phenotypic resistance (16, 17).
Furthermore, molecular assays are less accurate in detecting polymicrobial infections, whereas traditional growth methods would allow the visualization of different organisms or morphotypes in various concentrations (18). The detection of all the organisms in a polymicrobial infection by molecular panels can be concentration dependent, which may lead to the detection of the predominant pathogen(s) but missing of lower-burden or slower-growing pathogens within the same specimen. An important limitation is the inability to differentiate between a monomicrobial and a polymicrobial infection containing one or more Staphylococcus species (S. aureus, S. lugdunensis, and/or S. epidermidis) or Streptococcus species other than S. pneumoniae, S. pyogenes, S. agalactiae, and the S. anginosus group. As such, this complicates the prediction of methicillin resistance among Staphylococcus species if mecA is also detected as it is difficult to discern which organism the mecA gene belongs to. Similarly, it can be difficult to associate the AMR marker with a particular organism when multiple Gram-negative organisms are identified. Further examples and steps to resolve discrepancies caused by polymicrobial samples are described below.
WHAT CAN LABORATORIES DO TO RESOLVE DISCREPANCIES?
Genotype-to-phenotype correlations can be complex and depend on the methods, targets, and regions of targets detected for the different organisms-antimicrobial agents being evaluated (Table 1). Typically, three different scenarios could be encountered when phenotypic and genotypic resistance detection methods are compared. First, the genotype correlates with the phenotype, and no further testing is required. Second, an AMR gene is detected in an isolate that is phenotypically susceptible to the predicted agents affected by the AMR gene. Third, an AMR gene is not detected, but the isolate is found to be resistant to the predicted agents by phenotypic testing. While the clinical laboratory is not expected to exhaustively investigate further into all such discrepancies (scenarios 2 and 3), it is highly recommended as incorrect reports can result in patients being on inappropriate antimicrobial therapy and may lead to adverse events causing further harm to the patient. Moreover, health care providers may lose faith and trust in the clinical laboratory and in these more expensive diagnostic tests when discrepancies are overlooked by the laboratory. Overall, clinical laboratories should develop a consistent approach to resolve discordant results and consider a clear reporting structure to effectively communicate the results.
TABLE 1.
Examples of genetic alterations resulting in genotypic and phenotypic susceptibility discrepanciesa
| Organism | Genotype | Phenotype | Description | Discrepancy reason | Reference(s) |
|---|---|---|---|---|---|
| Staphylococcus aureus | mecA detected | Methicillin susceptible | Met-to-Ile change at amino acid residue 483 | Elimination of PBP2a transpeptidase activity | 38 |
| PBP2a detected, mecA not detected | Methicillin susceptible | Divergent SCCmec element | Remnant not functional | 39 | |
| SCCmec-orfX detected | Methicillin susceptible | SCCmec-orfX junction variants | Low specificity of proprietary target | 40 | |
| SCCmec detected | Methicillin susceptible | SCCmec remnant with ccr and partial mecA genes | Remnant not functional | 41 | |
| SCCmec detected | Methicillin susceptible | mecA deletions within SCCmec | Detectable by molecular methods, but remnant not functional | 43 | |
| SCCmec detected | Methicillin susceptible | Amplification of segments on right-extremity junction sequence of SCCmec | Retained segments do not contain the actual mecA gene | 42 | |
| mecA detected | Methicillin susceptible | Heterogeneously resistant large inoculum led to resistant phenotype; oxacillin induction increased MIC | Heterogeneously resistant large inoculum led to resistant phenotype | 38 | |
| mecA not detected | Methicillin resistant | Presence of mecA homologue (LGA251) | Not detectable by molecular target | 43 | |
| Enterococcus species | vanA detected | Vancomycin susceptible | Nucleotide deletions in Tn546 | Nonfunctional vanA | 44 |
| vanA detected | Vancomycin variableb | Silenced vanA (vanHAX) gene | Unexpressed vanA | 45 | |
| vanAB not detected | Vancomycin resistant | Presence of vanC | Not detectable by molecular target | 46 | |
| vanAB not detected | Vancomycin resistant | Presence of vanM | Not detectable by molecular target | 24 | |
| Enterobacterales | blaKPC detected | Carbapenem susceptible | Truncated blaKPC | Nonfunctional carbapenemase | 26 |
| blaCTX-M not detected | Cefotaxime or ceftriaxone resistant | blaTEM/SHV-derived ESBLs | Not detectable by molecular target | 16, 17 | |
| blaOXA-48 detected | Carbapenem variableb | blaOXA-48 and other mechanisms (e.g., other β-lactamases) | Alternative resistance mechanisms | 17 | |
| Carbapenemase not detected | Carbapenem resistant | Alternative carbapenem resistance mechanism (e.g., AmpC production combined with porin mutations and/or efflux) | Alternative carbapenem resistance mechanism | 47 | |
| Carbapenemase not detected | Carbapenem resistant | Test (e.g., Carba-R) cannot detect blaOXA-48-like and some other carbapenemases | Not detectable by molecular target | 48 | |
| Carbapenemase not detected | Imipenem resistance | Intrinsic low-level resistance (Morganella, Proteus spp., and Providencia spp.) | Intrinsic low-level resistance | 49 | |
| NA | Cefepime variableb | ESBL-carrying strains | Alternative resistance mechanisms | 50 | |
| NA | β-Lactam/inhibitor combination variableb | ESBL-carrying strains | Alternative resistance mechanisms | 51 | |
| NA | Cephalosporin variableb | Presence of multiple β-lactamases | Alternative resistance mechanisms | 17 | |
NA, not applicable.
Variable describes potentially resistant, intermediate resistant, and susceptible interpretations.
Aside from good laboratory practice, it is now a College of American Pathologists (CAP) requirement (MIC.21855, September 2019) to link antimicrobial resistance determinants and phenotypic susceptibility results to a specific organism in the final patient report. Additionally, laboratories should have a written procedure that describes the troubleshooting process of discrepancy analysis. Briefly, the requirement states that traditional microbiology culture methods should be utilized to confirm the isolation of pure organisms that were identified to have the anticipated AST profile. However, the extent of confirmatory testing is up to the discretion of the laboratory director.
The CLSI has published guidelines (appendix H, M100 standard Use of Molecular Assays for Resistance Detection) with suggestions on how to resolve discrepant results (10). Briefly, we discuss potential problems, examples, and solutions below. A more comprehensive description of the examples of discrepancies can be found in Table 1, with potential steps to resolution in Fig. 1 to 3.
FIG 1.

Workflow for resolving discrepant genotypic and phenotypic susceptibility results.
FIG 3.
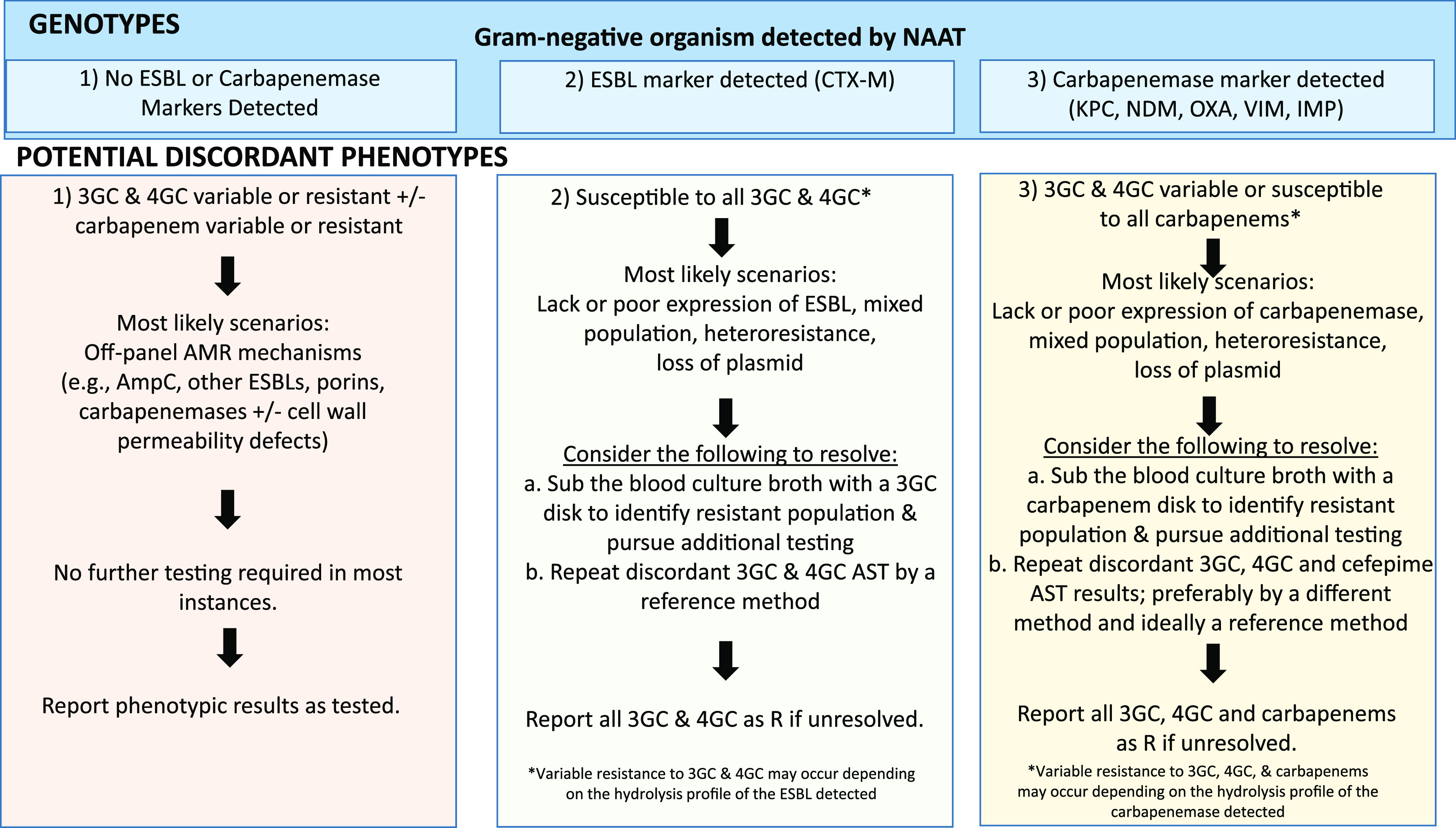
Potential steps and reporting structure for specific discrepant examples found in Gram-negative organisms (e.g., Enterobacterales). Abbreviations: R, resistant (described as having the potential to be both resistant and intermediate resistant); NAAT, nucleic acid amplification test; ESBL, extended-spectrum beta-lactamase; 3GC, third-generation cephalosporins; 4GC, fourth-generation cephalosporins; AMR, antimicrobial resistance; AST, antimicrobial susceptibility testing.
While we go over in detail three specific cases below, it is important for laboratorians to initially weigh the need for additional testing as repeat testing will cause delays in reporting, result in additional costs, and may not always resolve the discrepant results. Thus, if the discrepant results can be rationalized through an alternate explanation such as an off-panel mechanism of AMR resulting in phenotypic resistance, then further testing is often not required. The antimicrobial susceptibility profile may help explain a potential AMR mechanism (e.g., a porin alteration or an AmpC phenotype). If the results are unusual and cannot be explained otherwise, then additional troubleshooting is often required. Figure 1 describes the general workflow and basic steps in initiating the troubleshooting process. One of the first steps during troubleshooting is to check for pure isolation of the organism, and in the case of a mixed culture, individual isolates should be tested. Once the identification of the isolate is confirmed, original genotypic and phenotypic testing may be repeated. Furthermore, additional methods may be used to help with the discrepancy analysis such as performing a reference AST method if not applied initially or an additional test to target specific AMR mechanisms (e.g., confirmation of the ESBL gene using the phenotypic ESBL disk test on the recovered isolates, if appropriate). However, it is also noteworthy to mention that clerical or transcription errors should not be overlooked. Activity reports of the commercial systems should be reviewed, especially if the results are not interfaced. If discrepancies are due to consistent detection of a specific molecular target, the record of which modules had positive results should be reviewed. Lot numbers of blood bottles or reagents should be noted for trends, and environmental swipe testing may be considered to identify different sources of nucleic acid contamination. Technical issues should not be overlooked since inhibition of amplification can also interfere with detection; in such cases, contacting the company would be informative. If available, past reports from the patient can help ensure any consistency of organism and AMR markers identified.
STAPHYLOCOCCUS AUREUS CASE STUDY: DETECTION OF AN AMR GENE FROM POSITIVE BLOOD CULTURE BROTH WITH RECOVERY OF AN ISOLATE THAT IS PHENOTYPICALLY SUSCEPTIBLE
A 5-year-old boy with a history of short gut syndrome, total parenteral nutrition, G-tube dependence, and recurrent bloodstream infections presented with symptoms of sepsis. Symptoms consisted of fevers, chills, tachycardia, and abnormal leukocyte counts, which prompted the physicians to draw blood cultures. Growth was detected by the automated blood culture instrument in 7 h after receipt by the laboratory, and Gram-positive cocci were observed on Gram stain. According to the laboratory protocol, a multiplex molecular assay was performed directly from the positive blood bottle, and Staphylococcus, Staphylococcus aureus, and mecA were detected. As such, MRSA was reported. The following day, growth on solid medium revealed two colony types that were identified by MALDI-TOF MS as S. aureus and S. haemolyticus. The next step was to isolate pure colonies of the mixed culture and then perform AST on the isolates to identify which organism harbored the mecA gene. Phenotypic AST revealed that the S. aureus isolate was oxacillin susceptible but that the S. haemolyticus isolate was oxacillin resistant. A penicillin binding protein 2a (PBP2a) (the protein encoded by mecA) lateral flow assay performed on the S. aureus isolate was negative, demonstrating that the S. aureus isolate was not methicillin resistant due to the lack of PBP2a production. Of note, in this scenario, there was no need to repeat the genotypic test as the phenotypic testing of the cultured growth was sufficient to resolve the discrepant results. The final report was amended 2.5 days after the initial report to reflect that the culture grew MSSA and methicillin-resistant S. haemolyticus. The primary care team was also notified of the amended report. The patient was initially placed on vancomycin and was not deescalated due to the complexity of his medical status. However, the patient was discharged 4 days later.
Unfortunately, a common scenario of false-positive resistance detection may arise from polymicrobial blood cultures that consist of both MSSA and mecA-positive coagulase-negative Staphylococcus (CoNS) species. One could incorrectly interpret the results as detection of an MRSA isolate and by associating the mecA gene with the S. aureus isolate as opposed to the CoNS isolate. Due to mixed cultures of S. aureus and CoNS, a false-positive report of MRSA such as the example described above can occur. To address this issue, commercial manufacturers have been updating their panels to include additional targets, such as the mec (SSCmec [staphylococcal cassette chromosome mec]-orfX) right-extremity junction (MREJ), to be able to link the mecA gene to the S. aureus genome (19). However, it should be noted that sensitivities and specificities ranging from 80% to 95% and 86% to 91%, respectively, for the identification of MRSA based on mecA/mecC and the MREJ have been reported (13, 20, 21). Importantly, a multicenter study revealed that the introduction of mecA/MREJ targets detected 38.1% (8/21) of culture-negative specimens, which allowed the opportunity to ensure proper antibiotic therapy and better infection control practices (20). Missed detections were due to differences in the primer sequences of the MREJ, polymicrobial cultures, or the presence of organisms at the levels of the limit of detection.
Among Staphylococcus species, most methicillin (oxacillin) resistance is mecA mediated and is rarely due to other mechanisms such as the mecA homologue mecC (10). Strains with mecC typically test resistant to cefoxitin but susceptible to oxacillin by MIC methods and will be negative for mecA and PBP2a as they do not detect mecC-mediated resistance. When the mecA gene is detected by the molecular panel but the recovered isolate tests susceptible to oxacillin, repeating a PBP2a assay (with or without induction around a cefoxitin disk) is recommended; a mecA colony nucleic acid amplification test (NAAT) can be performed if available. To ensure that phenotypic results are accurate, usage of the specific Staphylococcus species breakpoints (e.g., S. aureus versus different CoNS species) and methods to determine oxacillin susceptibility should be confirmed. Ultimately, isolates that test positive for mecA or PBP2a should be reported as methicillin (oxacillin) resistant. In cases where some isolates may have cefoxitin-induced expression of PBP2a, subculturing the organism from the blood bottle and placing a cefoxitin disk in the first quadrant as selective pressure would help isolate any of the isolates that have variable susceptibility when under drug exposure. Growth from the cefoxitin zone margin can be used for repeat testing. Additionally, performing cefoxitin AST has higher sensitivity for the detection of mecA in S. aureus (10, 22, 23). In the event that the discrepancy is unresolved, reporting the isolate as resistant is recommended (Fig. 2).
FIG 2.
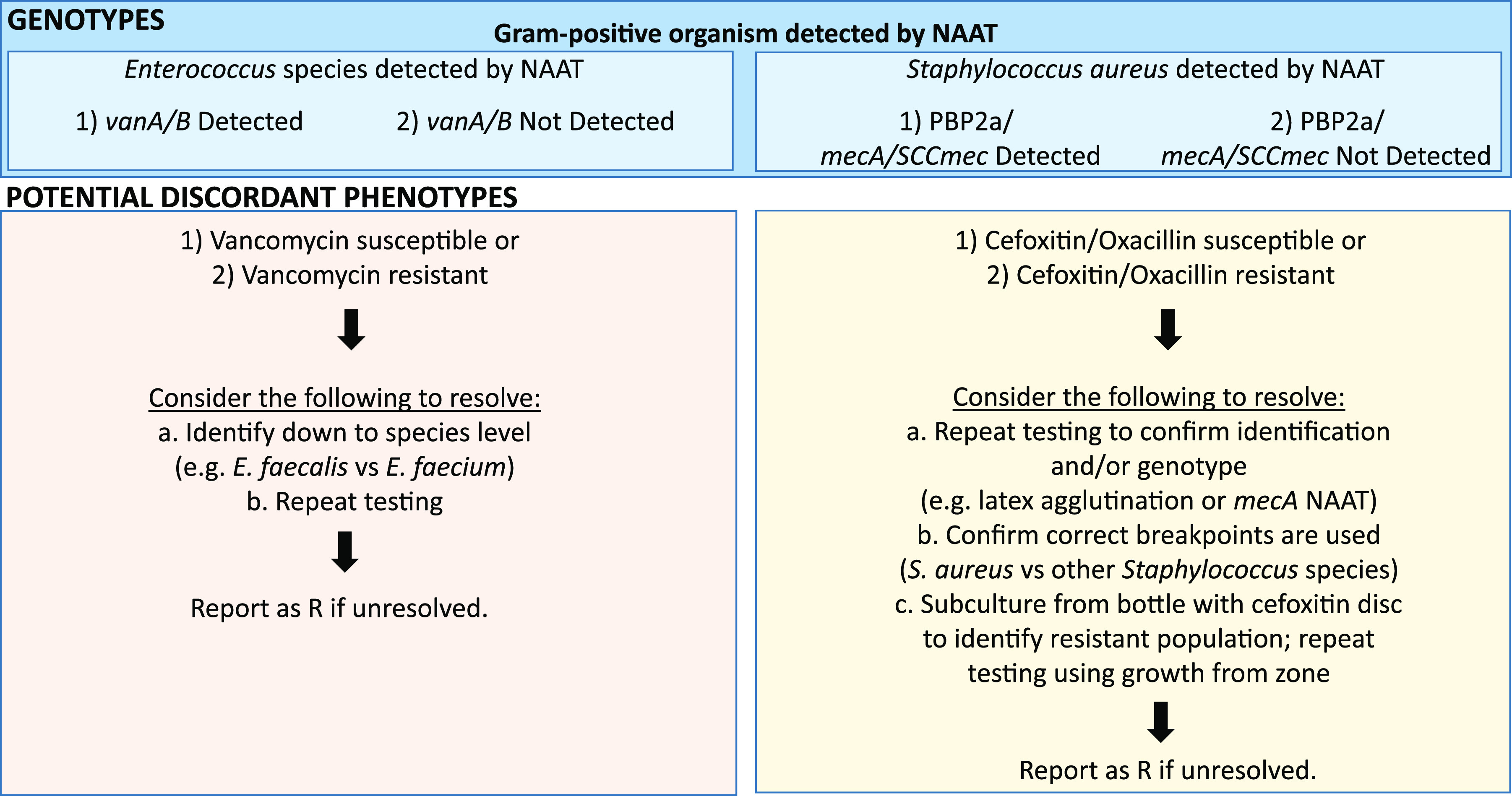
Potential steps and reporting structure for specific discrepant examples found in Gram-positive organisms (e.g., Enterococcus species and Staphylococcus aureus). Abbreviations: R, resistant (described as having the potential to be both resistant and intermediate resistant); NAAT, nucleic acid amplification test.
ENTEROCOCCUS SPECIES CASE STUDY: ABSENCE OF AN AMR GENE REPORTED WITH RECOVERY OF AN ISOLATE THAT IS PHENOTYPICALLY RESISTANT
A 64-year-old female was admitted to the orthopedic unit with a fractured femur, poorly controlled diabetes, and hypertension (24). Upon screening of her rectal swab, a vancomycin-resistant Enterococcus faecium strain was isolated, but neither vanA nor vanB was detected by molecular tests. Possible explanations driving this discrepant result include a mixed population, heteroresistance, misidentification of an intrinsically resistant Enterococcus species harboring vanC, or vancomycin resistance mediated by another van gene. Clinically, this is a scenario where discrepancy analysis is not necessarily required. However, in this case, the first step was to confirm the isolate identification. Biochemical tests, motility assays, and repeat tests with the Vitek 2 Gram-positive card, MALDI-TOF MS, and even species-specific PCR were performed to confirm that the isolate was E. faecium. Susceptibility testing using the Etest confirmed resistance to vancomycin (>256 mg/liter [resistant]) as well as ampicillin (>32 mg/liter [resistant]) and susceptibility to teicoplanin (1 mg/liter [susceptible]) and quinupristin-dalfopristin (0.75 mg/liter [susceptible]), suggesting that this could be an E. faecium isolate with vanB. As part of this hospital’s infection control policy, all VRE isolates were screened for vanA and vanB, for which this isolate tested negative. Hence, further sequencing, multilocus sequence typing (MLST), and Southern blot hybridization confirmed the vanM operon in the isolate belonging to MLST type 78 and clonal complex 17, which has been associated with epidemic nosocomial outbreaks and infections (25).
Vancomycin resistance in Enterococcus can be mediated by different van gene clusters, and at least eight clusters have been described in detail. Typically, only two targets (vanA or vanB) are included on molecular panels, and thus, these two genes are commonly involved in discrepancy scenarios. While the example described above provided elaborate means of troubleshooting, it is not expected from typical clinical microbiology laboratories to pursue such thorough workup. In general, upon confirmation of a pure culture, identification of the isolate down to the species level (e.g., E. faecalis, E. faecium, or E. gallinarum, etc.) would be beneficial as E. gallinarum and E. casseliflavus are intrinsically resistant to vancomycin. AST should be repeated, and if the discrepancy is not resolved, the isolate should be reported as vancomycin resistant. In cases where genotypic and phenotypic results match and resistance is due to vanA or vanB, one should consider reporting the molecular result and linking to the particular organism (e.g., vancomycin-resistant E. faecium) (Fig. 2).
ENTEROBACTERALES CASE STUDY: DETECTION OF AN AMR GENE WITH RECOVERY OF AN ISOLATE THAT IS PHENOTYPICALLY SUSCEPTIBLE
A 27-year-old man with a past medical history of brain injury, paraplegia, and seizure disorder was admitted to the emergency department after replacement of his gastrostomy-jejunostomy tube (26). He presented with severe dehydration, tachycardia, fever, and emesis. The blood bottle flagged positive, and a molecular panel identified Escherichia coli and also the detection of blaKPC. Phenotypic AST resulted in susceptibility to meropenem (≤0.125 μg/ml), imipenem (≤0.25 μg/ml), ertapenem (≤0.125 μg/ml), ceftriaxone (≤0.5 μg/ml), ceftazidime (≤0.5 μg/ml), and piperacillin-tazobactam (8/4 μg/ml [susceptible]). To resolve the discrepancy, the isolate was first retested by the molecular assay and by phenotypic AST, which yielded the same results as the first set of tests. Next, to confirm carbapenemase expression, a modified carbapenem inactivation method (mCIM) was performed, which was negative, prompting a follow-up study to understand why there was no carbapenemase expression despite the detection of the gene. Sequencing of the isolates revealed a C-to-T mismatch changing glutamate to a stop codon in blaKPC, resulting in a truncated carbapenemase.
In the scenario described above, reasons for this discrepancy can include a mixed culture, a heteroresistant subpopulation, a loss of plasmid-mediated resistance with a lack of selective pressure, a lack of expression of the antimicrobial resistance gene, intact porins in the presence of low-level KPC expression resulting in low carbapenem MICs, or a false-positive resistance marker result (Fig. 3). When a carbapenemase gene is detected in an isolate that is susceptible to all carbapenems, such as in the scenario described above, susceptibility testing should be repeated using a reference method and phenotypic tests for carbapenemase activity such as CarbaNP and mCIM, which can be used to confirm the expression of a broad range of carbapenemases (27). When carbapenemase genes are not detected but resistance to carbapenems is observed, it is likely that other resistance mechanisms (AmpC, porin mutations, and efflux pumps) are causing the resistance phenotype (17). Rare carbapenemases not included on molecular panels, such as GES, IMI, and SME types, may also be possible, depending on the organism. To increase the potential of detecting a carbapenemase producer, the positive blood culture broth or suspected isolate can be grown on an agar plate with a carbapenem disk on the first quadrant. A Cepheid Carba-R test can then be run on a sweep of the isolate growing near the carbapenem disk, which acts as a selective pressure. It may also be worth considering commercial platforms consisting of immunochromatographic tests such as Resist-4 O.K.N.V. (Coris) or NG-Test Carba 5, with a time to result of 15 min, or antimicrobial susceptibility testing-based systems like CPO Detect (Becton, Dickinson) (28–30).
Given the numerous mechanisms of antimicrobial resistance found in Gram-negative organisms, multiple false-positive and false-negative reports have been reported (Table 1). Discrepancies in the detection of ESBL target genes (e.g., blaCTX-M) may be found in isolates susceptible or with variable resistance to 3rd- and 4th-generation cephalosporins such as ceftriaxone, cefotaxime, ceftazidime, and cefepime. Of note, variable resistance to 3rd- and 4th-generation cephalosporins can be expected based on the ESBL enzymes as they may confer different cephalosporin hydrolysis profiles (e.g., CTX-M enzymes hydrolyze ceftriaxone better than ceftazidime, whereas the opposite is true for some SHV/TEM ESBL variants). However, the CLSI recommends that cefepime susceptibility should be confirmed using a reference method (10). In summary, if a discrepancy is not resolved or if resistance profiles are switched upon repeat confirmatory testing, it is recommended to err on the side of caution and report the isolate as resistant. If the discrepant genotype and phenotype results are reported, one should consider appending a comment to the results indicating that an infectious disease consult is recommended (Fig. 3).
CONSTANT COMMUNICATION BETWEEN MANUFACTURERS AND CLINICAL LABORATORIES
If the laboratory has been noticing an increase in discrepant results whether for pathogen identification or AMR gene detection, it is imperative that manufacturers are notified to ensure that an appropriate investigation is conducted (31). This will be of great benefit for other customers who are also using the platforms or supplies.
Due to the increased risk of false-positive or false-negative results, several recalls have been issued by the FDA after investigations were initiated (32). In the case of the Cepheid Xpert MRSA/SA test for detecting MRSA from blood cultures, false-positive detections were discovered to be associated with contaminants from blood culture media containing traces of nucleic acid. Similar issues were observed with Proteus nucleic acid contaminants in blood culture media with the FilmArray BCID panel (33).
While molecular assays are rapid, they are unable to detect new resistance genes or novel variants with changes in primer-probe annealing sites. Traditional microbiological methods still have their merits. Despite the longer time to result, performing manual AST or traditional phenotypic tests can account for the new genotypes, mutations, and technical issues with the molecular test and provide a more comprehensive antibiotic susceptibility profile, especially for a patient who may have contraindications for a particular drug. An added benefit is that manual AST would allow clinical laboratorians to determine if a culture is mixed due to the examination of purity plates. Recognizing the benefits of phenotypic susceptibility testing, Accelerate PhenoTest BC (Accelerate Diagnostics, Tucson, AZ) is currently the only FDA-cleared panel that can perform rapid phenotypic susceptibility testing on positive blood cultures providing MICs and categorical interpretations in approximately 7 h (34). Overall, it is extremely important that commercial companies continue to improve their molecular panels by incorporating circulating resistance genes or understanding the problems that clinical laboratories are having in order to maximize the utility of their test.
IT’S A TEAM EFFORT
Clinical microbiologists are experts on topics such as AMR mechanisms, performance characteristics of diagnostic platforms, and interpretation of susceptibility reports. Laboratories should be vigilant in ensuring that they provide the most accurate results possible while also utilizing clear communicative reports for the clinicians to understand. It is important to emphasize that the implementation of new diagnostic assays should be a team effort. Studies have shown that clear and concise communication through collaboration with antimicrobial stewardship and/or infectious diseases physicians led to successful and timelier deescalation and optimization of antimicrobials and decreases in overall health care costs and mortality rates (1, 2, 15). As more technologies, especially complex syndromic panels, are being implemented, a collaborative effort must be in place with the clinical microbiologists, clinicians, and antimicrobial stewardship teams to fully maximize the power of rapid diagnostic tests (35). The increased use of informatics and electronic medical records has also been shown to be beneficial. Antimicrobial stewardship teams can better track the antimicrobial decisions of the providers, leading to increased communication between providers and the pharmacy teams, allowing prompt optimization of antimicrobial usage (36, 37). Continuous provider education, dissemination of appropriate information, and proactive consultation with the laboratory director may be ways to ensure understanding between the laboratory and the clinicians. Working closely together to minimize miscommunication coupled with new technology will allow us to provide the best patient care possible.
ACKNOWLEDGMENTS
P.J.S. reports grants and personal fees from Accelerate Diagnostics, OpGen Inc., and BD Diagnostics; grants from bioMérieux Inc., Affinity Biosensors, and Hardy Diagnostics; and personal fees from Roche Diagnostics and Shionogi Inc. outside the submitted work. P.J.S. receives travel reimbursement from ASM, CAP, and the CLSI. J.D.B. reports grants and personal fees from BioFire Diagnostics, personal fees from Accelerate Diagnostics, and grants from Luminex Corporation outside the submitted work.
Contributor Information
Patricia J. Simner, Email: psimner1@jhmi.edu.
Alexander J. McAdam, Boston Children’s Hospital
REFERENCES
- 1.Banerjee R, Teng CB, Cunningham SA, Ihde SM, Steckelberg JM, Moriarty JP, Shah ND, Mandrekar JN, Patel R. 2015. Randomized trial of rapid multiplex polymerase chain reaction-based blood culture identification and susceptibility testing. Clin Infect Dis 61:1071–1080. 10.1093/cid/civ447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Avdic E, Wang R, Li DX, Tamma PD, Shulder SE, Carroll KC, Cosgrove SE. 2017. Sustained impact of a rapid microarray-based assay with antimicrobial stewardship interventions on optimizing therapy in patients with Gram-positive bacteraemia. J Antimicrob Chemother 72:3191–3198. 10.1093/jac/dkx267. [DOI] [PubMed] [Google Scholar]
- 3.Kuper KM, Boles DM, Mohr JF, Wanger A. 2009. Antimicrobial susceptibility testing: a primer for clinicians. Pharmacotherapy 29:1326–1343. 10.1592/phco.29.11.1326. [DOI] [PubMed] [Google Scholar]
- 4.Schulthess B, Brodner K, Bloemberg GV, Zbinden R, Böttger EC, Hombach M. 2013. Identification of Gram-positive cocci by use of matrix-assisted laser desorption ionization–time of flight mass spectrometry: comparison of different preparation methods and implementation of a practical algorithm for routine diagnostics. J Clin Microbiol 51:1834–1840. 10.1128/JCM.02654-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jorgensen JH, Ferraro MJ. 2009. Antimicrobial susceptibility testing: a review of general principles and contemporary practices. Clin Infect Dis 49:1749–1755. 10.1086/647952. [DOI] [PubMed] [Google Scholar]
- 6.Bard JD, Lee F. 2018. Why can’t we just use PCR? The role of genotypic versus phenotypic testing for antimicrobial resistance testing. Clin Microbiol Newsl 40:87–95. 10.1016/j.clinmicnews.2018.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Felsenstein S, Bender JM, Sposto R, Gentry M, Takemoto C, Dien Bard J. 2016. Impact of a rapid blood culture assay for Gram-positive identification and detection of resistance markers in a pediatric hospital. Arch Pathol Lab Med 140:267–275. 10.5858/arpa.2015-0119-OA. [DOI] [PubMed] [Google Scholar]
- 8.Walker T, Dumadag S, Lee CJ, Lee SH, Bender JM, Cupo Abbott J, She RC. 2016. Clinical impact of laboratory implementation of Verigene BC-GN microarray-based assay for detection of Gram-negative bacteria in positive blood cultures. J Clin Microbiol 54:1789–1796. 10.1128/JCM.00376-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pardo J, Klinker KP, Borgert SJ, Butler BM, Giglio PG, Rand KH. 2016. Clinical and economic impact of antimicrobial stewardship interventions with the FilmArray blood culture identification panel. Diagn Microbiol Infect Dis 84:159–164. 10.1016/j.diagmicrobio.2015.10.023. [DOI] [PubMed] [Google Scholar]
- 10.Clinical and Laboratory Standards Institute. 2020. Performance standards for antimicrobial susceptibility testing; thirtieth informational supplement. M100-S30. Clinical and Laboratory Standards Institute, Wayne, PA. [Google Scholar]
- 11.US Food and Drug Administration. 2020. FDA-recognized antimicrobial susceptibility test interpretive criteria. US Food and Drug Administration, Silver Spring, MD. https://www.fda.gov/drugs/development-resources/fda-recognized-antimicrobial-susceptibility-test-interpretive-criteria. Accessed 15 November 2020. [Google Scholar]
- 12.European Committee on Antimicrobial Susceptibility Testing. 2020. Clinical breakpoints—bacteria (v 10.0). https://www.eucast.org/clinical_breakpoints/. Accessed 15 November 2020.
- 13.Buchan BW, Ginocchio CC, Manii R, Cavagnolo R, Pancholi P, Swyers L, Thomson RB, Jr, Anderson C, Kaul K, Ledeboer NA. 2013. Multiplex identification of Gram-positive bacteria and resistance determinants directly from positive blood culture broths: evaluation of an automated microarray-based nucleic acid test. PLoS Med 10:e1001478. 10.1371/journal.pmed.1001478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Siu GK, Chen JH, Ng TK, Lee RA, Fung KS, To SW, Wong BK, Cheung S, Wong IW, Tam MM, Lee SS, Yam WC. 2015. Performance evaluation of the Verigene Gram-positive and Gram-negative blood culture test for direct identification of bacteria and their resistance determinants from positive blood cultures in Hong Kong. PLoS One 10:e0139728. 10.1371/journal.pone.0139728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mestas J, Polanco CM, Felsenstein S, Dien Bard J. 2014. Performance of the Verigene Gram-positive blood culture assay for direct detection of Gram-positive organisms and resistance markers in a pediatric hospital. J Clin Microbiol 52:283–287. 10.1128/JCM.02322-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tamma PD, Sharara SL, Pana ZD, Amoah J, Fisher SL, Tekle T, Doi Y, Simner PJ. 2019. Molecular epidemiology of ceftriaxone non-susceptible Enterobacterales isolates in an academic medical center in the United States. Open Forum Infect Dis 6:ofz353. 10.1093/ofid/ofz353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Paterson DL, Bonomo RA. 2005. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev 18:657–686. 10.1128/CMR.18.4.657-686.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Claeys KC, Heil EL, Pogue JM, Lephart PR, Johnson JK. 2018. The Verigene dilemma: Gram-negative polymicrobial bloodstream infections and clinical decision making. Diagn Microbiol Infect Dis 91:144–146. 10.1016/j.diagmicrobio.2018.01.012. [DOI] [PubMed] [Google Scholar]
- 19.Tenover FC, Tickler IA, Le VM, Dewell S, Mendes RE, Goering RV. 2019. Updating molecular diagnostics for detecting methicillin-susceptible and methicillin-resistant Staphylococcus aureus isolates in blood culture bottles. J Clin Microbiol 57:e01195-19. 10.1128/JCM.01195-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Buchan BW, Windham S, Balada-Llasat JM, Leber A, Harrington A, Relich R, Murphy C, Dien Bard J, Naccache S, Ronen S, Hopp A, Mahmutoglu D, Faron ML, Ledeboer NA, Carroll A, Stone H, Akerele O, Everhart K, Bonwit A, Kwong C, Buckner R, Warren D, Fowler R, Chandrasekaran S, Huse H, Campeau S, Humphries R, Graue C, Huang A. 2020. Practical comparison of the BioFire FilmArray Pneumonia panel to routine diagnostic methods and potential impact on antimicrobial stewardship in adult hospitalized patients with lower respiratory tract infections. J Clin Microbiol 58:e00135-20. 10.1128/JCM.00135-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Murphy CN, Fowler R, Balada-Llasat JM, Carroll A, Stone H, Akerele O, Buchan B, Windham S, Hopp A, Ronen S, Relich RF, Buckner R, Warren DA, Humphries R, Campeau S, Huse H, Chandrasekaran S, Leber A, Everhart K, Harrington A, Kwong C, Bonwit A, Dien Bard J, Naccache S, Zimmerman C, Jones B, Rindlisbacher C, Buccambuso M, Clark A, Rogatcheva M, Graue C, Bourzac KM. 2020. Multicenter evaluation of the BioFire FilmArray Pneumonia/Pneumonia Plus panel for detection and quantification of agents of lower respiratory tract infection. J Clin Microbiol 58:e00128-20. 10.1128/JCM.00128-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Broekema NM, Van TT, Monson TA, Marshall SA, Warshauer DM. 2009. Comparison of cefoxitin and oxacillin disk diffusion methods for detection of mecA-mediated resistance in Staphylococcus aureus in a large-scale study. J Clin Microbiol 47:217–219. 10.1128/JCM.01506-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Swenson JM, Tenover FC, Cefoxitin Disk Study Group . 2005. Results of disk diffusion testing with cefoxitin correlate with presence of mecA in Staphylococcus spp. J Clin Microbiol 43:3818–3823. 10.1128/JCM.43.8.3818-3823.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Teo JW, Krishnan P, Jureen R, Lin RT. 2011. Detection of an unusual van genotype in a vancomycin-resistant Enterococcus faecium hospital isolate. J Clin Microbiol 49:4297–4298. 10.1128/JCM.05524-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Top J, Willems R, van der Velden S, Asbroek M, Bonten M. 2008. Emergence of clonal complex 17 Enterococcus faecium in The Netherlands. J Clin Microbiol 46:214–219. 10.1128/JCM.01351-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Salimnia H, Veltman J, Chandrasekar PH, Pogue JM, Mynatt R, Salimnia T, Marshall SH, Hujer AM, Bonomo RA. 2020. Carbapenem-susceptible Klebsiella pneumoniae and Escherichia coli isolates carrying a truncated KPC carbapenemase: a challenge for rapid molecular diagnostics. J Clin Microbiol 58:e01627-19. 10.1128/JCM.01627-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Tamma PD, Simner PJ. 2018. Phenotypic detection of carbapenemase-producing organisms from clinical isolates. J Clin Microbiol 56:e01140-18. 10.1128/JCM.01140-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Jenkins S, Ledeboer NA, Westblade LF, Burnham C-AD, Faron ML, Bergman Y, Yee R, Mesich B, Gerstbrein D, Wallace MA, Robertson A, Fauntleroy KA, Klavins AS, Malherbe R, Hsiung A, Simner PJ. 2020. Evaluation of NG-Test Carba 5 for rapid phenotypic detection and differentiation of five common carbapenemase families: results of a multicenter clinical evaluation. J Clin Microbiol 58:e00344-20. 10.1128/JCM.00344-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kolenda C, Benoit R, Carricajo A, Bonnet R, Dauwalder O, Laurent F. 2018. Evaluation of the new multiplex immunochromatographic O.K.N.V. K-SeT assay for rapid detection of OXA-48-like, KPC, NDM, and VIM carbapenemases. J Clin Microbiol 56:e01247-18. 10.1128/JCM.01247-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Simon M, Gatermann S, Pfeifer Y, Reischl U, Gessner A, Jantsch J. 2019. Evaluation of the automated BD Phoenix CPO Detect panel in combination with the β-CARBA assay for detection and classification of carbapenemase-producing Enterobacterales. J Microbiol Methods 156:29–33. 10.1016/j.mimet.2018.11.024. [DOI] [PubMed] [Google Scholar]
- 31.Humphries RM, Hindler JA. 2016. Emerging resistance, new antimicrobial agents…but no tests! The challenge of antimicrobial susceptibility testing in the current US regulatory landscape. Clin Infect Dis 63:83–88. 10.1093/cid/ciw201. [DOI] [PubMed] [Google Scholar]
- 32.US Food and Drug Administration. 2010. Class 1 device recall Cepheid Xpert MRSA/SA blood culture. US Food and Drug Administration, Silver Spring, MD. [Google Scholar]
- 33.Butler-Wu S, Davis R. 2020. Genotypic false detections from blood culture bottles: are we only seeing the tip of the iceberg? American Society for Microbiology, Washington, DC. https://asm.org/ASM/media/Policy-and-Advocacy/BlCx-contaminating-DNA-FINAL.pdf?ext=.pdf. Accessed 22 March 2021.
- 34.Pancholi P, Carroll KC, Buchan BW, Chan RC, Dhiman N, Ford B, Granato PA, Harrington AT, Hernandez DR, Humphries RM, Jindra MR, Ledeboer NA, Miller SA, Mochon AB, Morgan MA, Patel R, Schreckenberger PC, Stamper PD, Simner PJ, Tucci NE, Zimmerman C, Wolk DM. 2018. Multicenter evaluation of the Accelerate PhenoTest BC kit for rapid identification and phenotypic antimicrobial susceptibility testing using morphokinetic cellular analysis. J Clin Microbiol 56:e01329-17. 10.1128/JCM.01329-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Morency-Potvin P, Schwartz DN, Weinstein RA. 2017. Antimicrobial stewardship: how the microbiology laboratory can right the ship. Clin Microbiol Rev 30:381–407. 10.1128/CMR.00066-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Katzman M, Kim J, Lesher MD, Hale CM, McSherry GD, Loser MF, Ward MA, Glasser FD. 2019. Customizing an electronic medical record to automate the workflow and tracking of an antimicrobial stewardship program. Open Forum Infect Dis 6:ofz352. 10.1093/ofid/ofz352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Forrest GN, Van Schooneveld TC, Kullar R, Schulz LT, Duong P, Postelnick M. 2014. Use of electronic health records and clinical decision support systems for antimicrobial stewardship. Clin Infect Dis 59(Suppl 3):S122–S133. 10.1093/cid/ciu565. [DOI] [PubMed] [Google Scholar]
- 38.Bressler AM, Williams T, Culler EE, Zhu W, Lonsway D, Patel JB, Nolte FS. 2005. Correlation of penicillin binding protein 2a detection with oxacillin resistance in Staphylococcus aureus and discovery of a novel penicillin binding protein 2a mutation. J Clin Microbiol 43:4541–4544. 10.1128/JCM.43.9.4541-4544.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Shore AC, Deasy EC, Slickers P, Brennan G, O’Connell B, Monecke S, Ehricht R, Coleman DC. 2011. Detection of staphylococcal cassette chromosome mec type XI carrying highly divergent mecA, mecI, mecR1, blaZ, and ccr genes in human clinical isolates of clonal complex 130 methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother 55:3765–3773. 10.1128/AAC.00187-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rossney AS, Herra CM, Brennan GI, Morgan PM, O’Connell B. 2008. Evaluation of the Xpert methicillin-resistant Staphylococcus aureus (MRSA) assay using the GeneXpert real-time PCR platform for rapid detection of MRSA from screening specimens. J Clin Microbiol 46:3285–3290. 10.1128/JCM.02487-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Shore AC, Rossney AS, O’Connell B, Herra CM, Sullivan DJ, Humphreys H, Coleman DC. 2008. Detection of staphylococcal cassette chromosome mec-associated DNA segments in multiresistant methicillin-susceptible Staphylococcus aureus (MSSA) and identification of Staphylococcus epidermidis ccrAB4 in both methicillin-resistant S. aureus and MSSA. Antimicrob Agents Chemother 52:4407–4419. 10.1128/AAC.00447-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Stamper PD, Louie L, Wong H, Simor AE, Farley JE, Carroll KC. 2011. Genotypic and phenotypic characterization of methicillin-susceptible Staphylococcus aureus isolates misidentified as methicillin-resistant Staphylococcus aureus by the BD GeneOhm MRSA assay. J Clin Microbiol 49:1240–1244. 10.1128/JCM.02220-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.García-Álvarez L, Holden MTG, Lindsay H, Webb CR, Brown DFJ, Curran MD, Walpole E, Brooks K, Pickard DJ, Teale C, Parkhill J, Bentley SD, Edwards GF, Girvan EK, Kearns AM, Pichon B, Hill RLR, Larsen AR, Skov RL, Peacock SJ, Maskell DJ, Holmes MA. 2011. Meticillin-resistant Staphylococcus aureus with a novel mecA homologue in human and bovine populations in the UK and Denmark: a descriptive study. Lancet Infect Dis 11:595–603. 10.1016/S1473-3099(11)70126-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Gagnon S, Lévesque S, Lefebvre B, Bourgault AM, Labbé AC, Roger M. 2011. vanA-containing Enterococcus faecium susceptible to vancomycin and teicoplanin because of major nucleotide deletions in Tn1546. J Antimicrob Chemother 66:2758–2762. 10.1093/jac/dkr379. [DOI] [PubMed] [Google Scholar]
- 45.Sivertsen A, Pedersen T, Larssen KW, Bergh K, Rønning TG, Radtke A, Hegstad K. 2016. A silenced vanA gene cluster on a transferable plasmid caused an outbreak of vancomycin-variable enterococci. Antimicrob Agents Chemother 60:4119–4127. 10.1128/AAC.00286-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Courvalin P. 2006. Vancomycin resistance in Gram-positive cocci. Clin Infect Dis 42(Suppl 1):S25–S34. 10.1086/491711. [DOI] [PubMed] [Google Scholar]
- 47.Larkin PMK, Realegeno S, Ward KW, Garner OB, Yang S. 2020. An unusual carbapenem resistant Escherichia coli carrying plasmid-mediated AmpC and mutated ompC in a patient with recurrent urinary tract infections. IDCases 20:e00781. 10.1016/j.idcr.2020.e00781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dortet L, Fusaro M, Naas T. 2016. Improvement of the Xpert Carba-R kit for the detection of carbapenemase-producing Enterobacteriaceae. Antimicrob Agents Chemother 60:3832–3837. 10.1128/AAC.00517-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Girlich D, Bonnin RA, Dortet L, Naas T. 2020. Genetics of acquired antibiotic resistance genes in Proteus spp. Front Microbiol 11:256. 10.3389/fmicb.2020.00256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Wang R, Cosgrove SE, Tschudin-Sutter S, Han JH, Turnbull AE, Hsu AJ, Avdic E, Carroll KC, Tamma PD. 2016. Cefepime therapy for cefepime-susceptible extended-spectrum β-lactamase-producing Enterobacteriaceae bacteremia. Open Forum Infect Dis 3:ofw132. 10.1093/ofid/ofw132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Rawat D, Nair D. 2010. Extended-spectrum β-lactamases in Gram negative bacteria. J Glob Infect Dis 2:263–274. 10.4103/0974-777X.68531. [DOI] [PMC free article] [PubMed] [Google Scholar]