

Abstract
Introduction:
Depression is associated with increased negative affect (NA) and low positive affect (PA), as well as interpersonal difficulties. Although most studies examine symptoms and affect at only one time point, ecological momentary assessment (EMA) captures data on affect and activity in real time and across contexts. The present study used EMA to explore the links between in-person and virtual social interactions, depressive symptoms, and momentary affect.
Methods:
Emerging adults (N=86) completed a self-report measure of both general depression and dysphoria symptoms, followed by EMA surveys 8 times daily for one week, reporting momentary affect (PA and NA) and social context (in-person and virtual interactions with friends).
Results:
In-person, but not virtual, presence of friends was associated with increased PA overall. Depressive symptoms were linked to less time with in-person friends and elevated NA. There was also a significant interaction between in-person presence of friends and dysphoria in predicting NA, such that presence of in-person friends was associated with lower NA only for those low in dysphoria.
Discussion:
Findings suggest that time with in-person friends is associated with increased PA overall and decreased NA only for those lower in depressive symptoms, but these effects do not generalize to virtual interactions. Those with greater depressive symptoms may be less responsive to positive stimuli and experience less of an effect of friends’ presence on affect. Alternatively, maladaptive social behaviors characteristic of depression may influence the effect of social interactions on affect.
Keywords: depression, positive affect, negative affect, multilevel modeling, ecological momentary assessment, social support
Introduction
Depression often emerges across adolescence and young adulthood and is a leading cause of disability worldwide (Brhlikova et al., 2011; Kessler et al., 2005). As such, there is a critical need to understand underlying etiological factors involved in the development and maintenance of depression. Emotionality is one key factor, as depression is characterized by alterations in the experiences of both positive affect (PA) and negative affect (NA) (Watson & Tellegen, 1985). Interpersonal factors also impact PA and NA, and are known to be involved in the development of depression (Hammen, 1992; Joiner, 2000). Yet, most work focuses on affect and interpersonal processes assessed at a single time point, and there is a need to better understand the effects of social contexts and depressive symptoms on momentary affect assessed in real time.
High NA is broadly related to most forms of psychopathology, whereas low PA is thought to be more specifically linked to depression (Beck et al., 2003; Clark & Watson, 1991; Heller et al., 2019; Ripper et al., 2018; Shankman & Klein, 2003; Suslow et al., 2019; Watson, Clark and Carey, 1988). Most studies of PA and NA in depression focus on trait measures averaging affect across varying timespans, which can be susceptible to retrospective recall biases, particularly in depressed individuals (Ben-Zeev et al., 2009). Affect fluctuates throughout the day, and ecological momentary assessment (EMA) captures experiential data in real time in personally-relevant contexts over repeated samplings, minimizing retrospective bias and memory errors and advancing our understanding of dynamic patterns of emotionality (Kahneman & Krueger, 2006; Shiffman et al., 2008). A growing literature has used EMA to study momentary affect in clinical depression and community samples varying in depressive symptoms (Bylsma et al., 2011; Heller et al., 2019; Silk et al., 2011). EMA research supports prior evidence of elevated NA in depression, but effects of depression on PA are less consistent and may be more context-dependent (Bylsma et al., 2011; Forbes et al., 2012; Geyer et al., 2018; Heller et al., 2019; Kahneman et al., 2004; Kahneman & Krueger, 2006; Silk et al., 2011).
In addition to assessing individual patterns of emotionality, EMA methods are well suited for studying emotional reactivity to specific events and contexts. Compared to nondepressed individuals, depressed adults have been shown to experience more intense NA reactivity to both pleasant and stressful daily life events (Bylsma et al., 2011). There is evidence that interpersonal factors, including social support and interpersonal stress, are central to the emergence and maintenance of depression (Brose et al., 2017; Hames et al., 2013; Hammen, 1992, 2009; Joiner, 2000; Rudolph et al., 2008). Interpersonal dynamics also shape momentary affect, such that the presence of others has been associated both with increases in PA and decreases in NA in youths and adults (Geyer et al., 2018; Kahneman & Krueger, 2006; Silk et al., 2011; Schneiders et al., 2007; Weinstein & Mermelstein, 2007).
Effects of social context on affect likely depend on the specific roles of social partners. That is, presence of family compared with friends may have distinct effects on affect across development (Forbes et al., 2012; Fredrick et al., 2018; Pössel et al., 2018; Schneiders et al., 2007; Silk et al., 2011). Consistent with this possibility, PA has been shown to be higher when adolescents are with friends or outside of the home or school (Schneiders et al., 2007). Generally, youths reported reduced NA, including sadness and anger, when with peers compared to when alone or with family (Schneiders et al., 2007; Silk et al., 2011). Further, prior research indicates that the positive association between presence of friends and PA increases as adolescents age (Larson & Richards, 1991). The proportion of time spent with family decreases dramatically as youths grow older, which could lead to an enhanced effect of peers on momentary affect (Larson & Richards, 1991; Nelson et al., 2016). Relatedly, college students in social contexts reported significantly improved mood compared to when they were alone, which parallels findings in adolescents (Geyer et al., 2018). Adolescents and emerging adults now spend more time interacting with friends and peers through social media and texting, but existing research provides mixed evidence on the translation of this mood-buffering effect to virtual interactions (Bennett et al., 2019; Underwood & Ehrenreich, 2017).
Although the presence of friends, and social support more broadly, is generally associated with increased PA, friendships can also exert a maladaptive influence on affect under some circumstances (Forbes et al., 2012; Pössel et al., 2018; Saltzman & Holahan, 2002). Depression is characterized by difficulties in relationships and dysfunctional social behaviors, including negative feedback-seeking, excessive reassurance seeking, interpersonal conflict avoidance, and blame maintenance, which can occur simultaneously, precede, and compound to initiate and reinforce depression (Hammen 1992; Hames et al., 2013; Joiner, 2000). Individuals with depression have been shown to exhibit distinct patterns of emotional reactivity in social contexts compared to non-depressed people, including spending more time alone and less time with families and reporting higher NA across contexts (Silk et al., 2011). Those at high risk for psychopathology also tend to rate current social partners as less pleasant compared to lower risk adolescents (Schneiders et al., 2007). Together, depression is often characterized by high NA and low PA, as well as interpersonal stressors and dysfunctional social behaviors. EMA evidence indicates that momentary affect fluctuates depending on social context, and as such, there is a need to consider the unique and interactive effects of depression and social contexts on affect.
We extend the literature on alterations in affect and interpersonal relationships in depression by leveraging the benefits of multilevel modeling to analyze within-person associations between depressive symptoms, social contexts, and affect (2637 assessments nested within 86 emerging adult participants). Given that emerging adulthood is a high-risk period for the emergence of depression and is characterized by re-orientation in social relationships (see Kessler et al., 2005; Kessler et al., 2007; Nelson et al., 2016), we examined both the impacts of presence of friends and depressive symptoms on affect, using EMA to obtain a large amount of experiential data. We first tested the main effects of virtual and in-person interactions with friends on momentary PA and NA. We focused on presence of friends, rather than family, given prior evidence of developmental change in the effects of friends on PA/NA and because we expected limited variance in time spent with family among this sample of college students. After examining changes in affect across social contexts, we assessed the effects of depressive symptoms on affect, as well as the extent to which depressive symptoms moderated the association between presence of friends and PA and NA. We hypothesized that depressive symptoms would interact with presence of friends to predict PA/NA, such that effects of friends on increased PA and decreased NA would be strongest among those lower in depressive symptoms. Given that social anxiety and depression often co-occur (see Heller et al., 2018; Kessler et al., 2003; Shankman et al., 2003), and social anxiety impacts affect during social interactions, we included social anxiety symptoms as a covariate.
Method
Participants
As part of a larger study on social and emotional processing in emerging adults, 130 undergraduate students (ages 18–22 years) were recruited via flyers and the psychology research participant pool at Vanderbilt University. Participants were compensated with research credit or $30. In addition to the primary laboratory assessment, participants had the option to participate in EMA for additional compensation; they were paid $10 for participating in EMA and an additional $10 for completing 35 or more assessments. Written informed consent was obtained from all participants before beginning procedures. Following consent, participants completed questionnaires to assess internalizing symptoms and an electroencephalogram (EEG) battery (results of which are presented elsewhere, including Pegg & Kujawa, 2020). Following the lab assessment, the researcher provided instructions on EMA to be completed through participants’ own smartphones in the following week.
Of the 130 participants that completed the initial assessment, 89 participated in the optional EMA. Three participants did not provide a valid study ID in EMA questionnaires and were removed from analysis, resulting in a final sample of 86 participants. The mean age of the analyzed sample was 19.33 years (SD=1.17), 73.26% identified as female and 8.14% identified as Latinx. For race, 53.49% identified as White, 22.09% Asian, 15.12% Black/African American, 8.14% Multiracial, and 1.16% American Indian. Study procedures were approved by the Vanderbilt University Institutional Review Board.
Measures
At the initial assessment, participants completed the 64-item Inventory of Depression and Anxiety Symptoms (IDAS), a validated measure of depressive and anxiety symptoms comprised of two broad scales, general depression and dysphoria, along with specific symptom subscales, including social anxiety (Watson et al., 2007). The dysphoria scale measures emotional and cognitive symptoms of depression, whereas the general depression scale encompasses the dysphoria scale in addition to items from other IDAS subscales involving physiological symptoms of depression. The general depression scale and dysphoria scale both demonstrate convergent validity with other measures of depression (Watson et al., 2007). Primary analyses focused on the general depression scale as a broad measure of depressive symptoms; however, to explore whether the effects of depression on EMA measures were driven by emotional and cognitive components of depression, secondary analyses also tested the dysphoria subscale specifically. Internal consistencies for analyzed scales were Cronbach’s α=.86 for general depression, α=.87 for dysphoria, and α=.85 for social anxiety. Further, 16.28% of participants met the IDAS clinical cutoff for major depressive disorder and 33.72% met the cutoff for social anxiety disorder (Stasik-O’Brien et al., 2019).
Ecological Momentary Assessment
To assess emotions and social interactions in daily life, text messages were sent to participants’ phones through SurveySignal 8 times per day for 7 days (SurveySignal; Hofmann & Patel, 2015). Text messages were sent randomly between 8am and midnight and provided a link to a SurveyMonkey survey (SurveyMonkey Inc., 2019), which remained active for 30 minutes after being sent. Each survey prompted participants to report who they were with in person and/or interacting with by phone or online, as well as current PA and NA. The mean number of assessments completed was 31.2 (SD=13.8) out of 56; in total, we obtained 2637 assessments nested within 86 participants.
Social Context.
When asked about who they were with, participants selected one or more of the following: (a) Close friend, (b) A group of friends, (c) Romantic partner, (d) Family member, (e) Acquaintance, (f) Stranger, (g) Alone, and/or (h) Other (and were asked to specify). Next, participants were asked whether they were interacting with someone by phone, text, or social media, and if so, they were prompted to select from the same list of relationships. For the purposes of our analyses, we focused on the presence of friends (including close friend and/or a group of friends) as a variable of interest, which we hypothesized would be a common and emotionally-salient social context for this age group. We evaluated the effects of presence of friends both in-person and virtually as separate variables. Most participants endorsed some time with friends, with 93.02% reporting in-person presence of friends in at least one assessment and 83.72% reporting virtual interactions with friends in at least one assessment. In contrast, only 23.26% of participants endorsed any assessments with family in person, and thus, the presence of family variable was not included in analyses.
Positive and Negative Affect.
Affect was measured at each assessment using the Positive and Negative Affect Scales (PANAS; Watson, Clark, and Tellegen, 1988). Participants were asked to indicate the extent to which they felt each emotion at that moment. At each assessment, PA and NA were calculated by averaging responses to the 10 items which were rated on a 1–5 Likert-type scale (1=very slightly or not at all, 5=extremely). PA was calculated by averaging five items (active, proud, enthusiastic, excited, and interested), and NA was measured by another five items (distressed, upset, scared, irritable, and nervous). The PANAS scales display high internal consistency and strong convergent and discriminant validity with other measures of mood (Watson, Clark, and Tellegen, 1988). In the current sample, internal consistency was high for both PA (α=.84) and NA (α=.87).
Analytic Strategy
We used multilevel modeling (also known as hierarchical linear modeling) to examine the effects of social context and depressive symptoms on PA and NA. The data were hierarchically arranged in two levels, with assessments (level 1) nested within participants (level 2). Multilevel modeling is necessary when data are hierarchical because it accounts for dependencies introduced due to clustering, thus yielding more accurate estimates of effects and their standard errors (Raudenbush & Bryk, 2002). Level-1 variables (i.e., those measured at each assessment) included current PA and NA levels, as well as current social context (whether or not the participant reported being with a close friend and/or a group of friends at the time of the assessment, either virtually or in person). Level-2 variables (i.e., person-level variables) included symptoms of general depression, dysphoria, and social anxiety, and were collected at baseline.
We employed an iterative model build-up strategy, described below, to test the interactive effects of depressive symptoms and presence of friends on momentary affect. All analyses were conducted in R, version 4.0.2 (R Core Team, 2020) using the nlme package (Pinheiro et al., 2020). For each outcome variable of interest, PA and NA, we began with unconditional (or null) models and then imposed lag-1 continuous autoregressive correlation structure on the residuals. In subsequent steps, we introduced level-1 and level-2 predictors of interest and examined whether level-1 predictors should be allowed to have random slopes. Finally, where appropriate, we introduced cross-level interactions and later probed these interactions using graphical techniques. Predictors were centered following previous recommendations by methodologists (Enders & Tofighi, 2007; Raudenbush & Bryk, 2002). Level-2 predictors were grand-mean centered. Level-1 predictors were person-mean centered to isolate within-person effects.
All participants were included in the analysis regardless of the number of assessments completed. With maximum likelihood estimation, missing data is accommodated as part of the estimation process, so it is not necessary for all participants to have complete data (Peugh & Enders, 2004). To determine which assessments were completed outside of the 1-week timeframe, time at each assessment was centered for each person, such that time in hours was set to 0 at the first assessment. Assessments completed outside of the desired 7-day response window due to technical errors (e.g., the last assessment was completed more than 8 days later than the first assessment) were excluded from analysis.
Results
Descriptive Statistics
Table 1 reports the descriptive statistics and correlations between study variables. For level-1 variables, such as PA and NA, we computed person-means, which then informed the overall means and correlations among level-2 variables reported. Across assessments, there was a weak negative correlation between PA and NA. In-person presence of friends was moderately positively correlated with PA, but not significantly correlated with NA. Virtual interactions with friends was weakly positively correlated with PA, but not NA. In-person presence of friends was weakly positively correlated with virtual interactions. Across participants, general depression, dysphoria, and social anxiety were highly positively correlated with each other. Surprisingly, depressive symptoms and mean PA were not significantly correlated. There was a weak positive correlation between mean NA and dysphoria, but not general depression. Notably, frequency of in-person interactions with friends was weakly negatively correlated with depressive symptoms, while frequency of virtual interactions was not significantly correlated with depressive symptoms. Social anxiety symptoms were not significantly correlated with mean PA/NA, in-person presence of friends, or virtual interactions with friends. Number of assessments completed was not significantly associated with any study variables.
Table 1.
Descriptive Statistics and Bivariate Correlations between Study Variables (N=86)
| M (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. General depression | 42.7 (11.8) | – | |||||||
| 2. Dysphoria | 21.8 (6.9) | .95*** | – | ||||||
| 3. Social anxiety | 10.7 (4.9) | .50*** | .55*** | – | |||||
| 4. In-person presence of friends | 40% (5%) | −.30** | −.30** | .02 | – | ||||
| 5. Virtual interactions with friends | 20% (4%) | −.10 | −.09 | .00 | .06** | – | |||
| 6. PA | 2.0 (.5) | −.16 | −.13 | −.07 | .22*** | .04* | – | ||
| 7. NA | 1.5 (.6) | .21 | .23* | .15 | −.02 | −.02 | −.12*** | – | |
| 8. Number of assessments completed | 31.2 (13.8) | −.09 | −.08 | .09 | .06 | −.16 | .00 | .00 | – |
Note.
p<.05.
p<.01.
p<.001.
In-person and virtual interactions with friends are coded dichotomously (0=not present, 1=present), thus, the means and standard deviations are reported as percentages of assessments spent with friends in person and virtually. Degrees of freedom (Df) for correlations among level-1 variables = 2,635. Df for correlations involving level-2 variables = 84.
Unconditional Models
We began with two unconditional models (or null models) each with PA or NA as the dependent variable. Null models allow for the calculation of intraclass correlation (ICC), which quantifies the amount of variance at each level due to the nesting of assessments within participants. The ICCs for PA and NA were .42 and .51, respectively, indicating that 42% of the variance in PA and 51% of the variance in NA occurred at the between-subjects level (i.e., level 2), reiterating the need for multilevel modeling.
Effects of General Depression and Presence of Friends on PA and NA
Using the unconditional models for PA and NA as baselines (AIC=5357.51, BIC=5375.14 for PA; AIC=4261.06, BIC=4278.69 for NA), we proceeded with model build-up. To determine whether newly-added predictors resulted in improved model fit at each step, we examined the Akaike Information Criterion (AIC), the Bayesian Information Criterion (BIC), and conducted likelihood ratio tests when appropriate.
We first tested if imposing a lag-1 continuous auto-regressive correlation structure on the residuals improved model fit. As expected, reductions in AIC and BIC indicated that model fit had improved (AIC=5156.39, BIC=5179.90 for PA; AIC=3867.06, BIC=3890.57 for NA); auto-regressive correlation structures are frequently used in EMA data, as they account for time dependencies across assessments (Bolger & Laurenceau, 2013). We also tested whether adding a continuous time variable -- as a fixed or random effect -- would improve model fit. Although we were not anticipating a linear increase or decrease in PA or NA across assessments, including time as a predictor can be useful for accounting for unexpected linear trends (Grimm et al., 2016). For both PA and NA, the inclusion of time as a fixed or random effect did not result in improved model fit, and therefore was not included in later steps.
Next, we incorporated the level-1 predictor in-person presence of friends into each model. For PA, the fixed effect was significant (p<.001), and the addition of this predictor resulted in improved model fit (AIC=5039.47, BIC=5068.86). For NA, the fixed effect was not significant (p=.140), and the addition of the predictor did not improve model fit (AIC=3872.77, BIC=3902.15); however it was kept to test its interaction with depressive symptoms in later steps. Following this, we tested whether presence of friends should have a random slope. A random slope indicates that the relation between the predictor and the outcome is variable across persons. To determine whether a random slope was warranted, we again examined AIC and BIC compared to the previous model and conducted likelihood ratio tests to compare the random-slope model to the fixed-slope model. When restricted information maximum likelihood (REML) estimation is used, likelihood ratio tests are appropriate to examine when two models are nested in terms of a random effect (Snijders & Bosker, 2012). Upon inclusion of the random slope, likelihood ratio tests indicated significant improvement in model fit for both PA (χ2(2) = 11.25 p=.004; AIC=5032.22, BIC=5073.36) and NA (χ2(2) = 15.90, p<.001; AIC=3860.86, BIC=3901.99). Therefore, random slopes were retained in both models.
These steps were repeated with virtual interactions with friends. For both PA and NA, virtual interactions with friends yielded a non-significant fixed effect and did not improve model fit when included as either a fixed or random effect. Despite this, virtual interactions were retained as a fixed effect in subsequent models to compare its ultimate effect with that of in-person presence of friends, as well as to assess the effect of in-person presence of friends above and beyond any effect of virtual interactions.
Next, we included general depression as a level-2 predictor. Model fit indices suggested that its addition did not improve fit for PA (AIC=5046.33, BIC=5099.22) or NA (AIC=3874.83, BIC=3927.71). However, for PA, the effect of general depression was verging on significance (p=.068) and was significant in predicting NA (p=.038). We retained general depression as a predictor in both the PA and NA models to explore the possibility that it interacted with presence of friends to influence affect.
In the final step, we added a cross-level interaction term to determine whether general depression moderated the relationships between in-person presence of friends and affect. In both models, AIC and BIC indicated that the interaction term did not improve model fit. For PA, the interaction term was nonsignificant, whereas for NA, the interaction term trended towards significance (p=.06). Finally, we included social anxiety as a level-2 covariate to assess whether the observed effects held after controlling for social anxiety.
Refer to Table 2 for full information about the final models, which contained in-person presence of friends as a random effect, virtual interactions with friends as a fixed effect, general depression, and the general depression × in-person presence of friends interaction term. With PA as the outcome variable, there was a significant main effect of in-person presence of friends, b=.306, t(2548)=8.90, p<.001, but virtual interactions with friends was not significant, b=−.016, t(2548)=−.484, p=.629. The main effect of general depression trended toward significance, b=−.009, t(84)=1.766, p=.081. The interaction between general depression and presence of friends was not significant, b=.003, t(2548)=1.050, p=.294. All effects were nearly identical after controlling for social anxiety, and thus are not reported here.
Table 2.
Results of Hierarchical Linear Models with General Depression and Time with Friends Predicting Momentary Affect
| Predictor | Positive Affect | Negative Affect | ||||
|---|---|---|---|---|---|---|
| b (SE) | t | p | b (SE) | t | p | |
| Intercept | 2.04 (0.06) | 33.93 | <.001 | 1.53 (0.06) | 26.87 | <.001 |
| In-person presence of friends | .31 (0.03) | 8.90 | <.001 | −.04 (0.03) | −1.47 | .141 |
| Virtual interactions with friends | −.02 (0.03) | −.48 | .629 | .01 (0.03) | .34 | .737 |
| General depression | −.01 (0.01) | −1.77 | .081 | .01 (0.00) | 2.36 | .021 |
| Interaction term (in-person presence of friends X general depression) | .00 (0.00) | 1.05 | .294 | .00 (0.00) | 1.88 | .061 |
Note. N=86. Only fixed effects are included.
With NA as the outcome variable, in-person presence of friends was not significant, b=−.039, t(2548)=−1.48, p=.140, nor was virtual interactions with friends, b=.009, t(2548)=.34, p=.737. General depression had a significant main effect, b=.011, t(84)=2.36, p=.021, but after controlling for social anxiety, this effect was slightly dampened; b=.0108, t(84)=1.92, p=.058. The interaction between in-person presence of friends and general depression was trending towards significance for NA, b=.004, t(2548)=1.88, p=.061. Notably, after controlling for social anxiety, the interaction effect for NA remained largely unchanged, b=.004, t(2549)=1.89, p=.059. Because this interaction effect was not statistically significant, we chose not to probe it further.
Effects of Dysphoria and Presence of Friends on PA and NA
Next, we conducted the same model build-up steps described previously, now including dysphoria as a predictor rather than general depression. Once again, for both PA and NA, after introducing autocorrelated residuals, in-person presence of friends as a random effect, and virtual interactions with friends as a fixed effect, we added dysphoria symptoms as a level-2 predictor. For PA, the main effect of dysphoria was nonsignificant and did not improve model fit. For NA, however, dysphoria yielded a significant effect (p=.024). Dysphoria was retained in both models to assess cross-level interaction effects. In the final step, the dysphoria × in-person presence of friends term was introduced. In both models, AIC and BIC indicated that the interaction term did not improve model fit. However, for NA, the interaction term was statistically significant (p=.011) and thus was retained. Social anxiety was also included as a covariate.
Refer to Table 3 for full information about the final models, which contained in-person presence of friends as a random effect, virtual interactions with friends as a fixed effect, dysphoria, and the dysphoria × in-person presence of friends interaction term. With PA as the outcome variable, there was a significant main effect of in-person presence of friends, b=.306, t(2548)=8.95, p<.001, whereas virtual interactions were not significant, b=−.017, t(2548)=−.500, p=.618. Dysphoria did not have a significant main effect, b=−.013, t(84)=1.408, p=.163. The interaction between dysphoria and presence of friends was also not significant, b=.007, t(2548)=1.261, p=.207. All effects were nearly identical after controlling for social anxiety, and thus are not reported here.
Table 3.
Results of Hierarchical Linear Models with Dysphoria and Time with Friends Predicting Momentary Affect
| Predictor | Positive Affect | Negative Affect | ||||
|---|---|---|---|---|---|---|
| b (SE) | t | p | b (SE) | t | p | |
| Intercept | 2.04 (0.06) | 33.63 | <.001 | 1.53 (0.06) | 27.03 | <.001 |
| In-person presence of friends | 0.31 (0.03) | 8.95 | <.001 | −0.04 (0.03) | −1.45 | .146 |
| Virtual interactions with friends | −0.02 (0.03) | −.50 | .618 | 0.01 (0.03) | .30 | .763 |
| Dysphoria | −0.01 (0.01) | −1.41 | .163 | 0.02 (0.01) | 2.60 | .011 |
| Interaction term (in-person presence of friends X dysphoria) | 0.01 (0.01) | 1.26 | .207 | 0.01 (0.00) | 2.52 | .012 |
Note. N=86. Only fixed effects are included.
With NA as the outcome variable, there was not a significant main effect of in-person presence of friends, b=−.038, t(2548)=−1.45, p=.146, or virtual interactions with friends, b=.008, t(2548)=.30, p=.763. Dysphoria had a significant main effect, b=.022, t(84)=2.60, p=.011. The interaction between in-person presence of friends and dysphoria was significant, b=.010, t(2548)=2.52, p=.012. After controlling for social anxiety, this interaction effect remained significant, b=.010, t(2548)=2.52, p=.012, indicating that the effect of in-person presence of friends on NA differed by participants’ dysphoria severity and was not better accounted for by social anxiety.
As shown in Figures 1 and 2, dysphoria moderated the relationship between in-person presence of friends and NA. To further probe the interaction, we calculated simple intercepts, simple slopes, and regions of significance (Preacher et al., 2006). As shown in Figure 1, at 1 SD below the mean for dysphoria, presence of friends was associated with lower NA, b=−.11, SE=.04, t(2548)=−2.88, p=.005. The effect of friends on NA was not significant for those with mean levels of dysphoria, b=−.04, SE=.03, t(2548)=−1.45, p =.15, or for those 1 SD above the mean, b=.03, SE=.04, t(2548)=.79, p =.434. Further, as shown in Figure 2, the upper and lower bounds for the Johnson-Neyman region of significance for dysphoria were 20.32 and 44.43. Specifically, raw dysphoria scores below 20.32 and above 44.43 were associated with a statistically significant slope relating presence of friends to NA. Of note, a dysphoria score of 44.43 is out of range for our sample, so we focus on the 20.32 cutoff. For individuals with dysphoria scores < 20.32, the slope relating in-person presence of friends to NA is significant and negative. For all other individuals, in-person presence of friends and NA were not significantly related.
Figure 1.
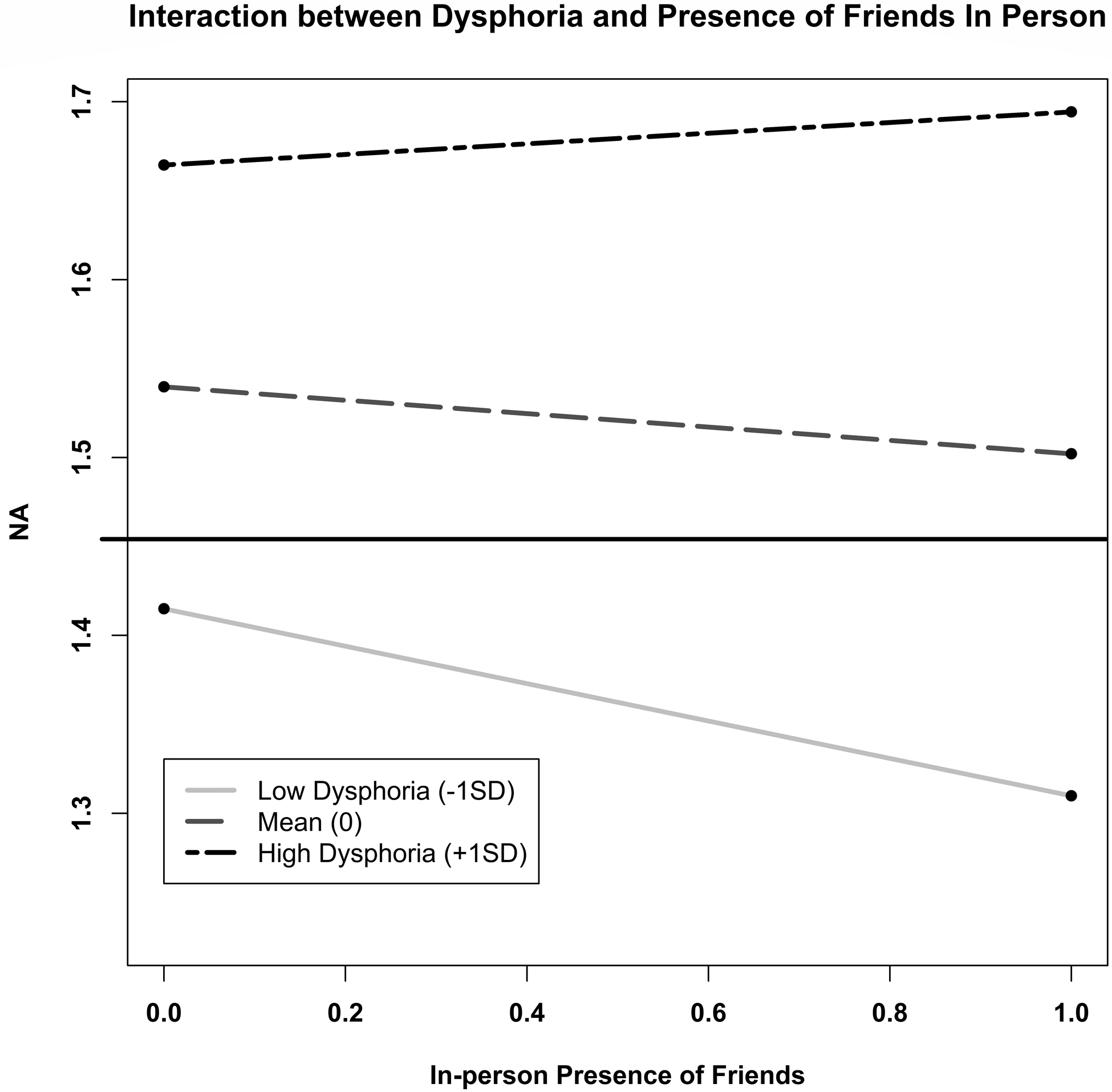
Dysphoria Symptoms Moderate the Relationship between In-Person Presence of Friends and Momentary Negative Affect (NA). Simple Slopes Depicting the Association between Presence of Friends and NA for Participants with High, Mean, and Low Dysphoria.
Figure 2.
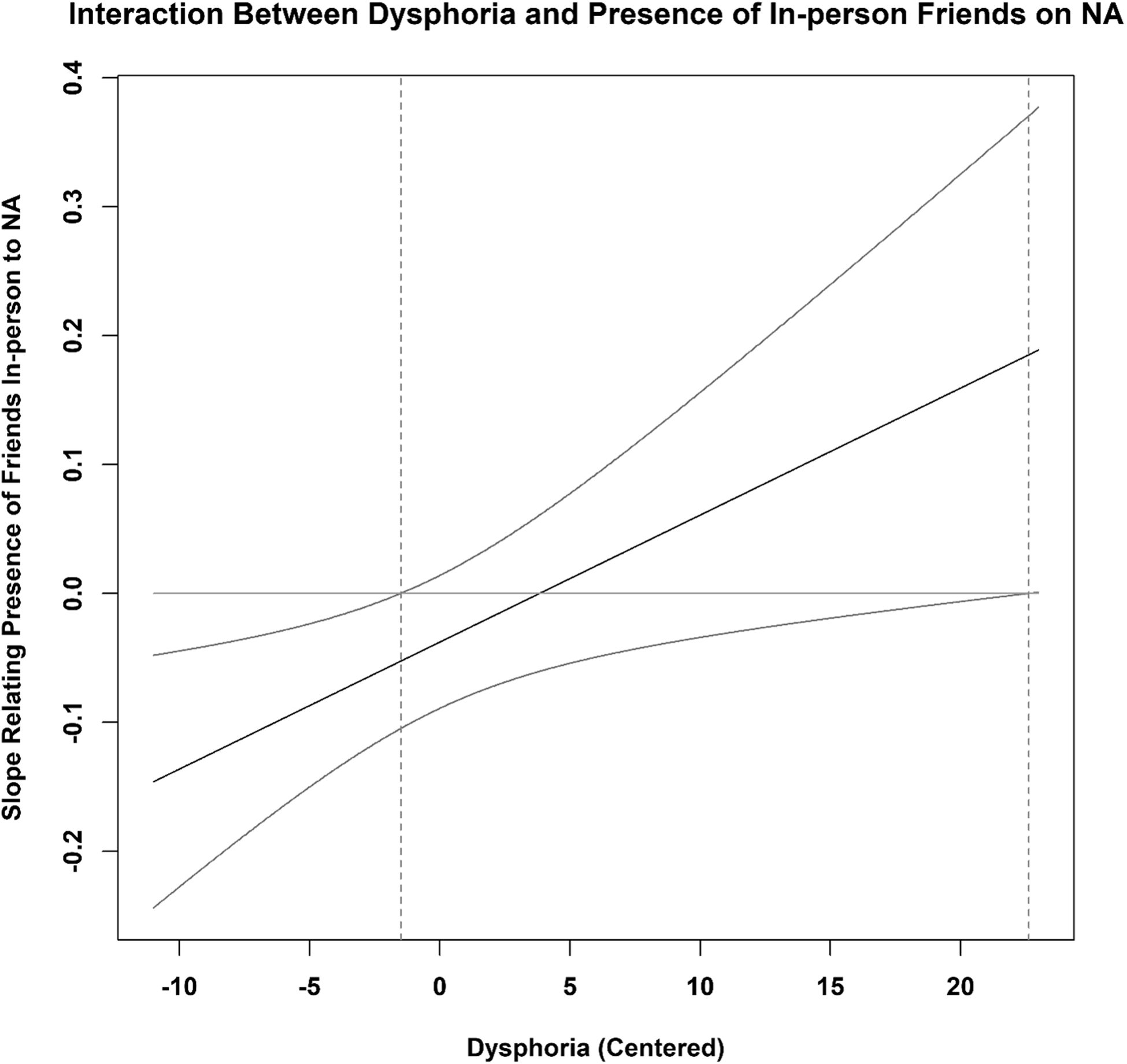
Dysphoria Symptoms Moderate the Relationship between In-Person Presence of Friends and Momentary Negative Affect (NA). Association (and Confidence Bands) between Dysphoria Symptoms and the Slope of the Relation between Time with Friends and NA.
Discussion
We evaluated the effects of depressive symptoms and social context on momentary affect across 2637 assessments nested within 86 emerging adult participants. Several key findings emerged. First, the presence of friends was associated with overall increases in PA, but this effect did not generalize to virtual interactions (i.e., talking by phone, text, or social media). Second, emerging adults high in depressive symptoms were less likely to report being with friends. Finally, symptoms of dysphoria, which include the emotional and cognitive aspects of depression, moderated the effects of friends’ presence on NA, such that friends were associated with lower NA only for individuals low on dysphoria. Overall, emerging adults with depressive symptoms reported reduced PA and greater NA and were less sensitive to the effects of social context on NA. Not only do emerging adults high in dysphoria spend less time with friends, but the time they do spend with friends does not appear to reduce NA in the same way observed for those low in dysphoria. Interestingly, this finding only applied to time spent with friends in person and did not extend to virtual interactions. Notably, the effect of friends’ presence on NA was not significant for emerging adults reporting mean levels of dysphoria, indicating that even mild depressive symptoms are associated with a lack of NA-dampening when with friends.
Our results support previous findings that youths with depression spend more time alone and report greater NA across social contexts than those without depression (Silk et al., 2011). Furthermore, our finding that dysphoria symptoms were associated with higher NA and lower PA aligns with previous research on NA and PA in depression (Beck et al., 2003; Geyer et al., 2018; Heller et al., 2019; Suslow et al., 2019). The interaction between dysphoria and time with friends is broadly consistent with prior evidence that, across social contexts, those with or at high risk for depression report higher NA and rate social partners as less pleasing compared to those without depression (Schneiders et al., 2007; Silk et al., 2011). This may be due in part to evidence linking depression to interpersonal difficulties including stress generation, interpersonal conflict avoidance and excessive reassurance-seeking (Hammen, 1992; Joiner, 2000). Our results contrast somewhat with a prior EMA study that did not find that anxiety or depression moderated the relationship between social context (alone vs. not alone) and affect, which may be due to the larger number of assessments in the current study and our evaluation of the effects of specific social relationships (Geyer et al., 2018).
Individuals high in dysphoria experience more negative mood states, which could play a role in the observed difference in mood-buffering across emerging adults. Drawing on interpersonal theories of depression (see Hames et al., 2013; Joiner, 2000), negative emotional states specifically associated with dysphoria may lead to less beneficial or maladaptive interactions with friends, which in turn worsen symptoms and modulate the mood-buffering effect of friends. Perceived lack of social efficacy may account for the increase in NA and lack of NA-buffering from presence of friends among emerging adults with moderate-to-high dysphoria symptoms. While spending time with friends is linked to improved mood (see Geyer et al., 2018; Silk et al., 2011), participants high in dysphoria may not reap the same benefits as those low in dysphoria because they misperceive or worry about their social competence when interacting with others (Geyer et al., 2018; Hammen 1992; Hammen, 2009).
Interestingly, the main effect of in-person presence of friends on NA was not significant in our final models. Although this is contrary to evidence that suggests friends are associated with a decrease in NA (see Silk et al., 2011; Weinstein & Mermelstein, 2007), lack of NA-buffering overall may be partially due to the variation in depressive symptoms across the sample. Further, prior studies that did find a buffering effect involved younger adolescents, who are less likely to spend time with friends compared to our sample of college students who spend most of their time with friends, potentially reducing the overall magnitude of effects on NA. On the other hand, the presence of friends in person, but not virtually, was associated with increased PA; this effect was consistent across all levels of dysphoria. Consistent with this finding, past work has indicated that the presence of others improves mood among adolescents, regardless of depression status (Geyer et al., 2018; Kahneman & Krueger, 2006; Weinstein & Mermelstein, 2007). It appears that emerging adults with depressive symptoms can experience increased positive emotion in the presence of friends, and this is broadly consistent with prior evidence that youths with depression report a greater PA to NA ratio when spending time with friends (Silk et al., 2011).
Both general depression and dysphoria were moderately positively correlated with NA, however this correlation was somewhat stronger for dysphoria and reached statistical significance. Probing this further indicated that dysphoria moderated the effect of presence of friends on NA whereas the interaction with general depression did not reach significance. This could be because the general depression scale includes items assessing physical symptoms such as insomnia, appetite changes, and suicidality (Watson et al., 2007). Our results indicate that the emotional and cognitive aspects of depression specifically, captured by the dysphoria scale, may be more linked to momentary affect and sensitivity to social context than depressive symptoms more broadly.
Importantly, we did not find evidence that virtual interactions with friends decreased NA or increased PA. The potentially beneficial effects of friends on affect do not appear to extend to online or phone interactions. That is, friends’ presence in person offers a unique buffering effect on NA among individuals with low dysphoric symptoms, as well as an enhancing effect on PA regardless of dysphoria severity, whereas interacting with friends online had no significant effects. From a clinical perspective, promoting in-person interactions with friends and directly addressing reduction of NA in interpersonal relationships may be particularly important for treating depressive symptoms in emerging adults. At the same time, these results must be interpreted cautiously in that we asked participants to report on their own use of social media and other platforms, which was likely insufficient to capture the complexity of use throughout the day. Integrating EMA with passive data collection is needed to better understand the effects of social interactions on momentary affect. For example, integration of smartphones that automatically monitor and record physical activity, device data, app use, and geospatial information could be beneficial.
Limitations of the current study include that it was conducted over a relatively short time span (1 week) without a long-term follow-up and involved a college student sample. Further, all measures were self-report, which can be subject to bias. The process of repeatedly administering assessments can impact participants’ feelings and behaviors, producing retest artifacts; notably, however, one study found that repeated administration of the PANAS was not linked to testing effects (Sharpe & Gilbert, 1997). Repeated assessments, particularly through mobile interventions, may also generate therapeutic effects, such as self-empowerment, and improve depressive symptoms (Depp et al., 2015; Simons et al., 2015), which warrants further consideration in future work. EMA captures a large amount of data in personally salient settings through multiple assessments, which increases ecological validity and allows for easy acquisition and comparison of momentary affect by social context (Shiffman et al., 2008). EMA also involves collection of information in real time, bypassing retrospective bias and memory errors (Ben-Zeev et al., 2009; Shiffman et al., 2008).
Conclusion
This study investigated links between depression, social context, and momentary affect and is among the first studies to compare the effects of in-person presence of friends vs. virtual interactions with friends on momentary affect using multilevel modeling. Emerging adults high in dysphoria spent less time with friends in person and reported higher overall NA. Further, a buffering effect of friends on NA emerged, but only among those low in symptoms of dysphoria. On the other hand, virtual interactions with friends were not significantly related to NA or PA. Future research should extend these methods to a clinical sample, comparing the effects of social contexts on affect, and evaluate other potential moderating factors, such as implicit beliefs.
Acknowledgments
This work was supported in part by the Vanderbilt CTSA grant UL1TR002243 from NCATS/NIH. SP was supported by NIH/NIMH T32-MH018921 during completion of this work. Portions of these findings were presented online as a poster at the 32nd Association for Psychological Science Annual Convention. We have no declarations of interest to disclose.
References
- Beck JG, Novy DM, Diefenbach GJ, Stanley MA, Averill PM, & Swann AC (2003). Differentiating anxiety and depression in older adults with generalized anxiety disorder. Psychological Assessment, 15(2), 184–192. 10.1037/1040-3590.15.2.184 [DOI] [PubMed] [Google Scholar]
- Ben-Zeev D, Young MA, & Madsen JW (2009). Retrospective recall of affect in clinically depressed individuals and controls. Cognition and Emotion, 23(5), 1021–1040. 10.1080/02699930802607937 [DOI] [Google Scholar]
- Bennett BL, Whisenhunt BL, Hudson DL, Wagner AF, Latner JD, Stefano EC, & Beauchamp MT (2020). Examining the impact of social media on mood and body dissatisfaction using ecological momentary assessment. Journal of American College Health, 68(5), 502–508. 10.1080/07448481.2019.1583236 [DOI] [PubMed] [Google Scholar]
- Bolger N, & Laurenceau JP (2013). Intensive longitudinal methods: An introduction to diary and experience sampling research. Guilford Publications. [Google Scholar]
- Brhlikova P, Pollock AM, & Manners R (2011). Global burden of disease estimates of depression - How reliable is the epidemiological evidence? Journal of the Royal Society of Medicine, 104(1), 25–34. 10.1258/jrsm.2010.100080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brose A, Wichers M, & Kuppens P (2017). Daily stressful experiences precede but do not succeed depressive symptoms: Results from a longitudinal experience sampling study. Journal of Social and Clinical Psychology, 36(3), 196–220. 10.1521/jscp.2017.36.3.196 [DOI] [Google Scholar]
- Bylsma LM, Taylor-Clift A, & Rottenberg J (2011). Emotional reactivity to daily events in major and minor depression. Journal of Abnormal Psychology, 120(1), 155–167. 10.1037/a0021662 [DOI] [PubMed] [Google Scholar]
- Depp CA, Ceglowski J, Wang VC, Yaghouti F, Mausbach BT, Thompson WK, & Granholm EL (2015). Augmenting psychoeducation with a mobile intervention for bipolar disorder: A randomized controlled trial. Journal of Affective Disorders, 174, 23–30. 10.1016/j.jad.2014.10.053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders CK, & Tofighi D (2007). Centering predictor variables in cross-sectional multi-level models: A new look at an old issue. Psychological Methods, 12(2), 121–138. 10.1037/1082-989X.12.2.121 [DOI] [PubMed] [Google Scholar]
- Forbes EE, Stepp SD, Dahl RE, Ryan ND, Whalen D, Axelson DA, Birmaher B, & Silk JS (2012). Real-world affect and social context as predictors of treatment response in child and adolescent depression and anxiety: An ecological momentary assessment study. Journal of Child and Adolescent Psychopharmacology, 22(1), 37–47. 10.1089/cap.2011.0085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fredrick SS, Demaray MK, Malecki CK, & Dorio NB (2018). Can social support buffer the association between depression and suicidal ideation in adolescent boys and girls? Psychology in the Schools, 55(5), 490–505. 10.1002/pits.22125 [DOI] [Google Scholar]
- Geyer EC, Fua KC, Daniel KE, Chow PI, Bonelli W, Huang Y, Barnes LE, & Teachman BA (2018). I did OK, but did I like it? Using ecological momentary assessment to examine perceptions of social interactions associated with severity of social anxiety and depression. Behavior Therapy, 49(6), 866–880. 10.1016/j.beth.2018.07.009 [DOI] [PubMed] [Google Scholar]
- Grimm KJ, Ram N, & Estabrook R (2016). Growth modeling: Structural equation and multi-level modeling approaches. Guilford Publications. [Google Scholar]
- Hames JL, Hagan CR, & Joiner TE (2013). Interpersonal processes in depression. Annual Review of Clinical Psychology, 9(1), 355–377. 10.1146/annurev-clinpsy-050212-185553 [DOI] [PubMed] [Google Scholar]
- Hammen C (1992). Cognitive, life stress, and interpersonal approaches to a developmental psychopathology model of depression. Development and Psychopathology, 4(1), 189–206. 10.1017/S0954579400005630 [DOI] [Google Scholar]
- Hammen C (2009). Adolescent depression: Stressful interpersonal contexts and risk for recurrence. Current Directions in Psychological Science, 18(4), 200–204. 10.1111/j.1467-8721.2009.01636.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heller AS, Fox AS, & Davidson RJ (2019). Parsing affective dynamics to identify risk for mood and anxiety disorders. Emotion, 19(2), 283–291. 10.1037/emo0000440 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofmann W, & Patel PV (2015). SurveySignal: A convenient solution for experience sampling research using participants’ own smartphones. Social Science Computer Review, 33(2), 235–253. 10.1177/0894439314525117 [DOI] [Google Scholar]
- Joiner TE (2000). Depression’s vicious scree: Self-propagating and erosive processes in depression chronicity. Clinical Psychology: Science and Practice, 7(2), 203–218. 10.1093/clipsy.7.2.203 [DOI] [Google Scholar]
- Kahneman D, & Krueger AB (2006). Developments in the measurement of subjective well-being. Journal of Economic Perspectives, 20(1), 3–24. 10.1257/089533006776526030 [DOI] [Google Scholar]
- Kahneman D, Krueger AB, Schkade DA, Schwarz N, & Stone AA (2004). A survey method for characterizing daily life experience: The day reconstruction method. Science, 306(5702), 1776–1780. 10.1126/science.1103572 [DOI] [PubMed] [Google Scholar]
- Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, & Üstün TB (2007). Age of onset of mental disorders: A review of recent literature. Current Opinion in Psychiatry, 20(4), 359–364. 10.1097/YCO.0b013e32816ebc8c [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, Rush AJ, Walters EE, Wang A, Rovner B, & Casten R (2003). The epidemiology of major depressive disorder. Evidence-Based Eye Care, 4(4), 186–187. 10.1097/00132578-200310000-00002 [DOI] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, & Walters EE (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry, 62(6), 593–602. 10.1001/archpsyc.62.6.593 [DOI] [PubMed] [Google Scholar]
- Larson RW, & Richards MH (1991). Daily companionship in late childhood and early adolescence: Changing developmental contexts. Child Development, 62(2), 284–300. 10.2307/1131003 [DOI] [PubMed] [Google Scholar]
- Nelson EE, Jarcho JM, & Guyer AE (2016). Social re-orientation and brain development: An expanded and updated view. Developmental Cognitive Neuroscience, 17, 118–127. 10.1016/j.dcn.2015.12.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pegg S, Arfer K, & Kujawa A (2020). The effects of a brief motivation manipulation on reward responsiveness: A multi-method study with implications for depression. International Journal of Psychophysiology, 150, 100–107. 10.1016/j.ijpsycho.2020.02.004 [DOI] [PubMed] [Google Scholar]
- Peugh JL, & Enders CK (2004). Missing data in educational research: A review of reporting practices and suggestions for improvement. Review of Educational Research, 74(4), 525–556. 10.3102/00346543074004525 [DOI] [Google Scholar]
- Pinheiro J, Bates D, DebRoy S, Sarkar D, & R Core Team. (2020). nlme: Linear and Nonlinear Mixed Effects Models. (R package version 3.1–149) [Computer software]. https://CRAN.R-project.org/package=nlme.
- Pössel P, Burton SM, Cauley B, Sawyer MG, Spence SH, & Sheffield J (2018). Associations between social support from family, friends, and teachers and depressive symptoms in adolescents. Journal of Youth and Adolescence, 47(2), 398–412. 10.1007/s10964-017-0712-6 [DOI] [PubMed] [Google Scholar]
- Preacher K, Curran P, & Bauer D (2006). Computational tools for probing interactions in multiple linear regression, multi-level modeling, and latent curve analysis. Journal of Educational and Behavioral Statistics, 31(4), 437–448. 10.3102/10769986031004437 [DOI] [Google Scholar]
- Raudenbush SW, & Bryk AS (2002). Hierarchical linear models: Applications and data analysis methods (Vol. 1). Sage Publications. [Google Scholar]
- Ripper CA, Boyes ME, Clarke PJF, & Hasking PA (2018). Emotional reactivity, intensity, and perseveration: Independent dimensions of trait affect and associations with depression, anxiety, and stress symptoms. Personality and Individual Differences, 121, 93–99. 10.1016/j.paid.2017.09.032 [DOI] [Google Scholar]
- R Core Team. (2020). R: A language and environment for statistical computing (Version 4.0.2) [Computer software]. R Foundation for Statistical Computing. https://www.R-project.org/ [Google Scholar]
- Rudolph KD, Flynn M, & Abaied JL (2008). A developmental perspective on interpersonal theories of youth depression. In Abela JRZ & Hankin BL (Eds.), Handbook of depression in children and adolescents (p. 79–102). Guilford Press. [Google Scholar]
- Saltzman KM, & Holahan CJ (2002). Social support, self efficacy, and depressive symptoms: An integrative model. Journal of Social and Clinical Psychology, 21(3), 309–322. 10.1521/jscp.21.3.309.22531 [DOI] [Google Scholar]
- Schneiders J, Nicolson NA, Berkhof J, Feron FJ, DeVries MW, & Van Os J (2007). Mood in daily contexts: Relationship with risk in early adolescence. Journal of Research on Adolescence, 17(4), 697–722. 10.1111/j.1532-7795.2007.00543.x [DOI] [Google Scholar]
- Shankman SA, & Klein DN (2003). The relation between depression and anxiety: An evaluation of the tripartite, approach-withdrawal and valence-arousal models. Clinical Psychology Review, 23(4), 605–637. 10.1016/S0272-7358(03)00038-2 [DOI] [PubMed] [Google Scholar]
- Sharpe PJ, & Gilbert DG (1998). Effects of repeated administration of the beck inventory and other measures of negative mood states. Personality and Individual Differences, 24(4), 457–463. https://psycnet.apa.org/doi/10.1016/S0191-8869(97)00193-1 [Google Scholar]
- Shiffman S, Stone AA, & Hufford MR (2008). Ecological momentary assessment. Annual Review of Clinical Psychology, 4, 1–32. 10.1146/annurev.clinpsy.3.022806.091415 [DOI] [PubMed] [Google Scholar]
- Silk JS, Forbes EE, Whalen DJ, Jakubcak JL, Thompson WK, Ryan ND, Axelson DA, Birmaher B, & Dahl RE (2011). Daily emotional dynamics in depressed youth: A cell phone ecological momentary assessment study. Journal of Experimental Child Psychology, 110(2), 241–257. 10.1016/j.jecp.2010.10.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons CJP, Hartmann JA, Kramer I, Ho P, Van Bemmel AL, Delespaul P, Van, Os J, & Wichers M (2015). Effects of momentary self-monitoring on empowerment in a randomized controlled trial in patients with depression. 30, 900–906. 10.1016/j.eurpsy.2015.09.004 [DOI] [PubMed] [Google Scholar]
- Snijders TA, & Bosker RJ (2011). Multi-level analysis: An introduction to basic and advanced multi-level modeling. (2nd ed.). Sage Publications. [Google Scholar]
- Stasik-O’Brien SM, Brock RL, Chmielewski M, Naragon-Gainey K, Koffel E, McDade-Montez E, O’Hara MW, & Watson D (2019). Clinical utility of the Inventory of Depression and Anxiety Symptoms (IDAS). Assessment, 26(5), 944–960. 10.1177/1073191118790036 [DOI] [PubMed] [Google Scholar]
- SurveyMonkey Inc. (2019). SurveyMonkey: The World’s Most Popular Free Online Survey Tool. Surveymonkey.Com. http://www.surveymonkey.com
- Suslow T, Bodenschatz CM, Kersting A, Quirin M, & Günther V (2019). Implicit affectivity in clinically depressed patients during acute illness and recovery. BMC Psychiatry, 19(1), 1–9. 10.1186/s12888-019-2365-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Underwood MK, & Ehrenreich SE (2017). The power and the pain of adolescents’ digital communication: Cyber victimization and the perils of lurking. The American Psychologist, 72(2), 144–158. 10.1016/j.physbeh.2017.03.040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson D, Clark LA, & Carey G (1988). Positive and negative affectivity and their relation to anxiety and depressive disorders. Journal of Abnormal Psychology, 97(3), 346–353. 10.1037/0021-843X.97.3.346 [DOI] [PubMed] [Google Scholar]
- Watson D, Clark LA, & Tellegen A (1988). Development and validation of brief measures of positive and negative affect: The PANAS scale. Journal of Personality and Social Psychology, 54(6), 1063–1070. 10.1037/0022-3514.54.6.1063 [DOI] [PubMed] [Google Scholar]
- Watson D, O’Hara MW, Simms LJ, Kotov R, Chmielewski M, McDade-Montez EA, Gamez W, & Stuart S (2007). Development and validation of the Inventory of Depression and Anxiety Symptoms (IDAS). Psychological Assessment, 19(3), 253–268. 10.1037/1040-3590.19.3.253 [DOI] [PubMed] [Google Scholar]
- Watson D, & Tellegen A (1985). Toward a consensual structure of mood. Psychological Bulletin, 98(2), 219–235. 10.1037/0033-2909.98.2.219 [DOI] [PubMed] [Google Scholar]
- Weinstein SM, & Mermelstein R (2007). Relations between daily activities and adolescent mood: The role of autonomy. Journal of Clinical Child and Adolescent Psychology, 36(2), 182–194. 10.1080/15374410701274967 [DOI] [PMC free article] [PubMed] [Google Scholar]