

Abstract
Background
The assessment of self-reported outcomes in neuromyelitis optica spectrum disorder (NMOSD) is limited by the lack of validated disease-specific measures. The SymptoMScreen (SyMS) is a patient-reported questionnaire for measuring symptom severity in different domains affected by multiple sclerosis (MS), but has not been thoroughly evaluated in NMOSD. The aim of this study was to assess the psychometric properties of the SyMS in a sample of patients with NMOSD.
Methods
A non-interventional, cross-sectional study in adult subjects with NMOSD (Wingerchuk 2015 criteria) was conducted at 13 neuroimmunology clinics applying the SyMS. A non-parametric item response theory procedure, Mokken analysis, was performed to assess the underlying dimensional structure and scalability of items and overall questionnaire. All analyses were performed with R (v4.0.3) using the mokken library.
Results
A total of 70 patients were studied (mean age: 47.5 ± 15 years, 80% female, mean Expanded Disability Status Scale score: 3.0 [interquartile range 1.5, 4.5]). Symptom severity was low (median SyMS score: 19.0 [interquartile range 10.0, 32.0]). The SyMS showed a robust internal reliability (Cronbach’s alpha: 0.90 [95% confidence interval 0.86, 0.93]) and behaved as a unidimensional scale with all items showing scalability coefficients > 0.30. The overall SyMS scalability was 0.45 conforming to a medium scale according to Mokken’s criteria. Fatigue and body pain were the domains with the highest scalability coefficients. The SyMS was associated with disability (rho: 0.586), and physical and psychological quality of life (rho: 0.856 and 0.696, respectively).
Conclusions
The SyMS shows appropriate psychometric characteristics and may constitute a valuable and easy-to-implement option to measure symptom severity in patients with NMOSD.
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is a rare neuroinflammatory condition targeting primarily the spinal cord and optic nerve and associated with severe disability [1,2]. Fatigue, pain, visual loss, and motor impairment are the most prevalent symptoms [3–5]. Depression and other psychiatric comorbid conditions are also common in NMOSD affecting well-being and quality of life [6,7]. However, little is known about the subjective experience of patients living with NMOSD [4,8,9]. In addition, the assessment of patients´ perspectives is limited by the lack of validated, self-reported, NMOSD-specific measures [9].
NMOSD and multiple sclerosis (MS) are different neuroinflammatory disorders, but share a heterogeneous spectrum of symptoms [1,7,10]. The SymptoMScreen (SyMS) is a validated, patient-reported questionnaire for measuring symptom severity in key domains affected by MS, and thus we hypothesized that it might be also relevant to gather the impact of NMOSD from the patients’ perspective [11,12].
The aim of this study was to assess the psychometric properties of the SyMS questionnaire in a sample of NMOSD patients.
Materials and methods
A non-interventional, cross-sectional study was conducted to assess the reliability, dimensional structure, and item characteristics of the SyMS in patients with NMOSD (PERSPECTIVES-NMO study). Eligibility criteria included age at least 18 years old and a diagnosis of NMOSD according to Wingerchuk 2015 criteria [13]. This study was conducted in accordance with the Good Clinical Practice Guidelines of the International Conference on Harmonisation and with the ethical principles of the Declaration of Helsinki and was approved by the investigational review board of Galicia (CEIm-G), Santiago de Compostela, Spain. Patients were consecutively recruited in the context of their follow-up visits at thirteen hospital-based neuroimmunology clinics between November 2019 and July 2020. All participants provided written informed consent.
SymptoMScreen questionnaire
The SyMS assesses symptom severity across twelve neurologic domains: mobility, hand function/dexterity, spasticity and stiffness, pain, sensory symptoms, bladder control, fatigue, vision, dizziness, cognition, depression, and anxiety [11,12,14]. Each item is assessed on a seven-point Likert scale: 0 (not at all affected) to 6 (total limitation). The total score ranges from 0 to 72, with higher scores indicating more severe symptom endorsement.
This questionnaire was developed in English and has been translated into 19 languages. A paper format is available free for download at https://www.symptomscreen.org/. The original Spanish version of the SyMS was administered in this study only replacing the term MS by NMOSD in the first statement: “Please circle one number that best describes how each NMOSD symptom has affected your everyday life activities“.
Statistical analysis
We analyzed the internal reliability of the SyMS with Cronbach’s alpha index. We assessed the underlying dimensional structure of the SyMS with a non-parametric item response theory procedure, Mokken analysis [15]. We also used Mokken analysis to assess the scalability of items and overall questionnaire. The scalability coefficients (Hi) for each item indicate the discrimination and weight each item has on the latent variable or dimension it is purported to measure. We required an internal reliability equal or greater than 0.70 but lower than 0.95 to define acceptable reliability. We required scalability coefficients (Hi) for each item and the overall scale (H), to be equal or greater than 0.30 to define an acceptable scale [15]. All analyses were done with R (v4.0.3) using the mokken library [16,17]. Associations between the SyMS and the Expanded Disability Status Scale (EDSS) and the 29-item Multiple Sclerosis Impact Scale (MSIS-29) were analyzed using Spearman’s rank correlation [18,19].
Results
A total of 70 patients were studied. The mean (± SD) age was 47.5 ± 15 years and 80% were female. The median EDSS score was 3.0 (interquartile range 1.5, 4.5). Seven patients (10%) required a walking aid and three (4.3%) used a wheelchair. Eighteen patients (27.7%) had uni- or bilateral visual acuity lower than 20/100. Overall symptom severity was low with a median SyMS score of 19.0 (interquartile range 10.0, 32.0). Sociodemographic and clinical characteristics of the sample are shown in Table 1.
Table 1. Demographic and clinical characteristics.
| n = 70 | |
|---|---|
| Age (years), mean ± SD | 47.5 ± 15 |
| Sex (female), n (%) | 56 (80) |
| Disease duration (years), mean ± SD | 9.9 ± 8.1 |
| Anti-aquaporin-4 antibodies, n (%) | 54 (77.1%) |
| Relapsing form, n (%) | 59 (84.2) |
| Single-attack form, n (%) | 11 (15.7) |
| Number of relapses since diagnosis, mean ± SD | 2.9 ± 2.3 |
| Number of relapses in the last year, mean ± SD | 0.5 ± 0.9 |
| EDSS score, median (IQR) | 3.0 (1.5, 4.5) |
| EDSS score ≥ 6, n (%) | 10 (14.3) |
| SymptoMScreen score, median (IQR) | 19.0 (10.0, 32.0) |
| Physical impact MSIS-29 score, mean ± SD | 41.9 ± 16.7 |
| Psychological impact MSIS-29 score, mean ± SD | 20.9 ± 8.3 |
EDSS = Expanded Disability Status Scale; MSIS-29 = 29-item Multiple Sclerosis Impact Scale; IQR = interquartile range; SD = standard deviation.
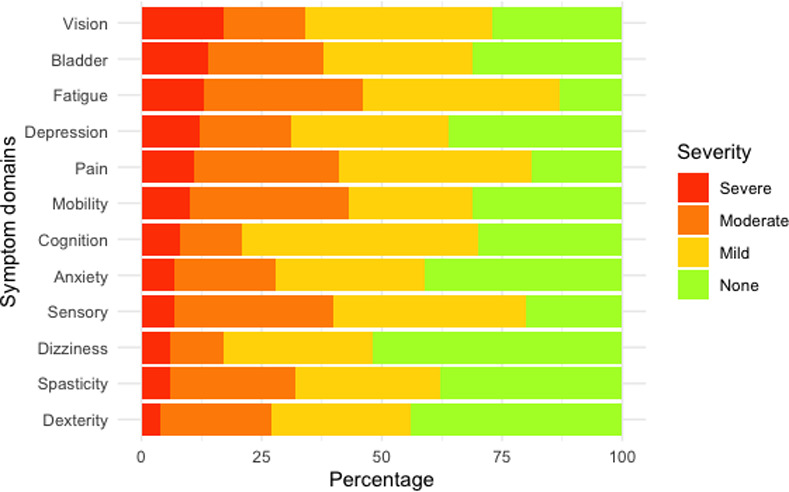
The SyMS showed a robust internal reliability (Cronbach’s alpha 0.90 [95% confidence interval 0.86, 0.93]) and behaved as a unidimensional scale with all items showing scalability coefficients Hi > 0.30. The overall SyMS scalability was 0.45 conforming to a medium scale according to Mokken’s criteria. Fatigue and body pain were the domains with the highest scalability coefficients, whereas vision and bladder control were the domains with the highest levels of perceived severity (Table 2 and Fig 1).
Table 2. Psychometric characteristics of the SymptoMScreen.
| Severity levels, n (%) | |||||
|---|---|---|---|---|---|
| Domain | Hi | None (score 0) | Mild (score 1+2) | Moderate (score 3+4) | Severe (score 5+6) |
| Mobility | 0.45 | 22 (31) | 18 (26) | 23 (33) | 7 (10) |
| Dexterity | 0.39 | 31 (44) | 20 (29) | 16 (23) | 3 (4) |
| Spasticity | 0.46 | 27 (39) | 21 (30) | 18 (26) | 4 (6) |
| Pain | 0.52 | 13 (19) | 28 (40) | 21 (30) | 8 (11) |
| Sensory symptoms | 0.49 | 14 (20) | 28 (40) | 23 (33) | 5 (7) |
| Bladder control | 0.39 | 21 (30) | 22 (31) | 17 (24) | 10 (14) |
| Fatigue | 0.53 | 9 (13) | 29 (41) | 23 (33) | 9 (13) |
| Vision | 0.36 | 19 (27) | 27 (39) | 12 (17) | 12 (17) |
| Dizziness | 0.43 | 36 (51) | 22 (31) | 8 (11) | 4 (6) |
| Cognition | 0.48 | 21 (30) | 34 (49) | 9 (13) | 6 (9) |
| Depression | 0.46 | 25 (36) | 23 (33) | 13 (19) | 9 (13) |
| Anxiety | 0.40 | 28 (40) | 22 (31) | 15 (21) | 5 (7) |
Hi = scalability coefficient.
Fig 1. Symptom severity.
Overall SyMS score showed a significant correlation with physical and psychological MSIS-29 scores (rho = 0.856 and 0.696, p<0.0001, respectively), and EDSS score (rho = 0.586, p<0.0001).
Discussion
NMOSD is a rare autoimmune, neuroinflammatory disease with a negative impact on patients´ independence and quality of life [4,8,20]. The unpredictability trajectory of the disease makes the experience of living with NMOSD even more difficult for patients and their caregivers [7,8,21].
The assessment of patient perspectives using standardized self-report instruments have been inconsistently conducted in patients with neuroinflammatory and demyelinating disorders [9,22]. Well-designed and validated patient-oriented outcome measures in NMSOD are needed to better capture the course of the disease and the response to treatments [3,4,9]. The US online community PatientsLikeMe developed the Neuromyelitis Optica Rating Scale (NMORS), a self-reported, eight-item instrument to assess symptoms and disability in patients with NMOSD [3]. The total score ranges from 0 to 100, with higher scores indicating more severe symptom severity. Moore et al. created a 46-item patient-reported questionnaire to assess the impact of NMOSD on life functioning and different symptom dimensions, including vision, mobility, bladder, bowel, mood, sexual dysfunction, pain, fatigue, and cognition [9]. However, neither of the two instruments is psychometrically validated.
The SyMS is a validated, brief and easy-to-implement questionnaire to quantify symptoms in MS [11,12]. The overall score correlates with clinical disability, physical and psychological health-related quality of life, and work productivity [14,23]. Green et al. assessed symptom severity using the SyMS in a sample of 43 patients with NMOSD and 85 with MS [24]. Although overall scores were similar in both populations, vision impairment, spasticity, pain, and bladder dysfunction were worse in patients with NMOSD compared to MS.
Our study found that the SyMS is a patient-reported instrument with a high internal reliability and a unidimensional construct also in patients with NMOSD. These results enable its implementation in clinical practice to capture the impact of the disease in multiple relevant and clinically meaningful symptom domains. To our knowledge, this is the first study to assess psychometric issues of the SyMS questionnaire in NMOSD, and its results help to support its use and add to the scarce presence of patient-reported measures in NMOSD.
Less tangible symptoms, usually not detected on the standard neurological examination like fatigue, pain or cognitive problems may be often more important to patients’ sense of well-being and quality of life than physical disability in MS [25]. More than forty percent of 522 NMOSD patients participating in a recent survey reported moderate or severe disability due to fatigue and pain [3]. Cognitive impairment in NMOSD may already affect patients with a low level of physical disability [26]. A meta-analysis including 25 studies and 761 patients found a prevalence of cognitive impairment of 34% (95% CI:31–37%) [27]. Longer disease duration, fatigue, pain, and sleep disturbances were associated with cognitive impairment [26]. These “less overt impairments” stress the need for including patient-centered measures in clinical practice.
Our study population included a sample of clinically stable NMOSD patients with a medium degree of physical disability and mostly with positive anti-aquaporin-4 antibodies. The fact that most of the recruitment period coincided with the onset of the COVID-19 pandemic could influence the selection of patients with this profile, since the most disabled patients avoided conducting face-to-face consultations. The results may thus not be generalizable to subjects with less stable disease status or higher disability and other serologic subtypes. The small sample size due to a low prevalence of NMOSD did not allow us to perform a parametric confirmatory factor analysis and compare the fit of different solutions to data [28]. Further studies with a larger sample size are needed to confirm the unidimensional structure of the SyMS. Despite this limitation, the sample of 70 subjects was managed at 13 different clinics on a national level, representing NMOSD patients across the country.
Conclusion
Although the SyMS is not a disease-specific measurement, it shows appropriate psychometric characteristics and may constitute a brief and reliable option to assess symptom severity in patients with NMOSD.
Acknowledgments
The authors would like to thank all patients, their families and the investigators who participated in the PERSPECTIVES-NMO study.
Data Availability
Qualified researchers may request access to individual patient level data through the clinical study data request platform (https://vivli.org/). Further details on Roche's criteria for eligible studies are available here (https://vivli.org/members/ourmembers/). For further details on Roche's Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_trials/our_commitment_to_data_sharing.htm).
Funding Statement
This study was funded by the Medical Department of Roche Farma Spain (ML41397). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1.Marignier R, Cobo Calvo A, Vukusic S. Neuromyelitis optica and neuromyelitis optica spectrum disorders. Curr Opin Neurol. 2017; 30(3):208–15. doi: 10.1097/WCO.0000000000000455 . [DOI] [PubMed] [Google Scholar]
- 2.Papp V, Magyari M, Aktas O, Berger T, Broadley SA, Cabre P, et al. Worldwide incidence and prevalence of NMO: A systematic review. Neurology. 2021; 96(2):59–77. doi: 10.1212/WNL.0000000000011153 Epub 2020 Dec 11. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Eaneff S, Wang V, Hanger M, Levy M, Mealy MA, Brandt AU, et al. Patient perspectives on neuromyelitis optica spectrum disorders: data from the PatientsLikeMe online community. Mult Scler Relat Disord. 2017; 17:116–22. doi: 10.1016/j.msard.2017.07.014 Epub 2017 Jul 11. . [DOI] [PubMed] [Google Scholar]
- 4.Beekman J, Keisler A, Pedraza O, Blaschke TF, Smith TJ, Yeaman MR. Neuromyelitis optica spectrum disorder: Patient experience and quality of life. Neurol Neuroimmunol Neuroinflamm. 2019; 6(4):e580. doi: 10.1212/NXI.0000000000000580 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Asseyer S, Cooper G, Paul F. Pain in NMOSD and MOGAD: A systematic literature review of pathophysiology, symptoms, and current treatment strategies. Front Neurol. 2020; 11:778. doi: 10.3389/fneur.2020.00778 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shi Z, Chen H, Lian Z, Liu J, Feng H, Zhou H. Factors that impact health-related quality of life in neuromyelitis optica spectrum disorder: anxiety, disability, fatigue and depression. J Neuroimmunol. 2016; 293:54–8. doi: 10.1016/j.jneuroim.2016.02.011 Epub 2016 Feb 16. . [DOI] [PubMed] [Google Scholar]
- 7.Barzegar M, Badihian S, Mirmosayyeb O, Ashtari F, Jamadi M, Emami S, et al. Comparative study of quality of life, anxiety, depression, and fatigue among patients with neuromyelitis optica spectrum disorder and multiple sclerosis: the first report from Iran. Mult Scler Relat Disord. 2018; 22:161–5. doi: 10.1016/j.msard.2018.04.009 Epub 2018 Apr 14. . [DOI] [PubMed] [Google Scholar]
- 8.Mutch K, Methley A, Moore P, Jacob A. Life on hold: the experience of living with neuromyelitis optica. Disabil Rehabil. 2014; 36(13):1100–07. doi: 10.3109/09638288.2013.833301 Epub 2013 Sep 12. . [DOI] [PubMed] [Google Scholar]
- 9.Moore P, Jackson C, Mutch K, Methley A, Pollard C, Hamid S, et al. Patient-reported outcome measure for neuromyelitis optica: pretesting of preliminary instrument and protocol for further development in accordance with international guidelines. BMJ Open. 2016; 6(9):e011142. doi: 10.1136/bmjopen-2016-011142 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Masuda H, Mori M, Uzawa A, Uchida T, Ohtani R, Kuwabara S. Difference in fatigue and pain between neuromyelitis optica spectrum disorder and multiple sclerosis. PLoS One. 2020; 15(4):e0224419. doi: 10.1371/journal.pone.0224419 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Green R, Kalina J, Ford R, Pandey K, Kister I. SymptoMScreen: a tool for rapid assessment of symptom severity in MS across multiple domains. Appl Neuropsychol Adult. 2017; 24(2):183–9. doi: 10.1080/23279095.2015.1125905 Epub 2016 Apr 14. . [DOI] [PubMed] [Google Scholar]
- 12.Meca-Lallana J, Maurino J, Hernández-Pérez MA, Sempere AP, Brieva L, García-Arcelay E, et al. Psychometric properties of the SymptoMScreen questionnaire in a mild disability population of patients with relapsing-remitting multiple sclerosis: quantifying the patient’s perspective. Neurol Ther. 2020; 9(1):173–9. doi: 10.1007/s40120-020-00176-6 Epub 2020 Jan 18. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wingerchuk DM, Banwell B, Bennet JL, Cabre P, Carroll W, Chitnis T, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. 2015; 85(2):177–89. doi: 10.1212/WNL.0000000000001729 Epub 2015 Jun 19. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fitzgerald KC, Salter A, Tyry T, Fox RJ, Cutter G, Mowry EM, et al. Validation of the SymptoMScreen with performance-based or clinician-assessed outcomes. Mult Scler Relat Disord. 2019; 29:86–93. doi: 10.1016/j.msard.2019.01.031 Epub 2019 Jan 24. . [DOI] [PubMed] [Google Scholar]
- 15.Mokken RJ. Nonparametric models for dichotomous responses. In: van der Linden WJ, Hambleton RK, eds. Handbook of Modern Item Response Theory. New York, NY: Springer-Verlag; 2010:351–67. [Google Scholar]
- 16.Van der Ark LA. Mokken scale analysis in R. J Stat Soft. 2007; 20(11):1–19. doi: 10.18637/jss.v020.i11 [DOI] [Google Scholar]
- 17.Van der Ark LA. New developments in Mokken scale analysis in R. J Stat Soft. 2012; 48(5):1–27. doi: 10.18637/jss.v048.i05 [DOI] [Google Scholar]
- 18.Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983; 33(11):1444–52. doi: 10.1212/wnl.33.11.1444 . [DOI] [PubMed] [Google Scholar]
- 19.Hobart J, Lamping D, Fitzpatrick R, Riazi A, Thompson A. The Multiple Sclerosis Impact Scale (MSIS-29): a new patient-based outcome measure. Brain. 2001; 124(Pt 5):962–73. doi: 10.1093/brain/124.5.962 . [DOI] [PubMed] [Google Scholar]
- 20.Siritho S, Thavorncharoensap M, Chanatittarat C, Pasogpakdee P, Apiwattanakul M, Prayoonwiwat N, et al. Health utilities of patients with multiple sclerosis and neuromyelitis optica spectrum disorders in Thailand. Mult Scler Relat Disord. 2018; 24:151–6. doi: 10.1016/j.msard.2018.07.004 Epub 2018 Jul 4. . [DOI] [PubMed] [Google Scholar]
- 21.Mutch K, Methley A, Hamid S, Moore P, Jacob A. If they are OK, we are OK: the experience of partners living with neuromyelitis optica. Disabil Rehabil. 2017; 39(13):1279–86. doi: 10.1080/09638288.2016.1193233 Epub 2016 Jul 3. . [DOI] [PubMed] [Google Scholar]
- 22.Brichetto G, Zaratin P. Measuring outcomes that matter most to people with multiple sclerosis: the role of patient-reported outcomes. Curr Opin Neurol. 2020; 33(3):295–9. doi: 10.1097/WCO.0000000000000821 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kister I, Hartung HP, Vermersch P, Buffels R, Kuhelj R, Clinch W, et al. Construct validity and internal consistency of patient-reported SymptoMScreen in phase IIIb trials of ocrelizumab in relapsing multiple sclerosis (ENSEMBLE and CASTING). Int J MS Care. 2019; 21 (Suppl 1):75–6. [Google Scholar]
- 24.Green R, Nathanson J, Kister I. Multi-dimensional assessment of symptom severity in matched NMO and MS patients. ECTRIMS Online Library. Green R. 09/15/2016; 146171; P330. https://onlinelibrary.ectrims-congress.eu/ectrims/2016/32nd/146171/rivka.green.multi-dimensional.assessment.of.symptom.severity.in.matched.nmo.html.
- 25.Green R, Cutter G, Friendly M, Kister I. Which symptoms contribute the most to patients’ perception of health in multiple sclerosis? Mult Scler J Exp Transl Clin. 2017; 3(3):2055217317728301. doi: 10.1177/2055217317728301 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Czarnecka D, Oset M, Karlińska I, Stasiołek M. Cognitive impairment in NMOSD-More questions than answers. Brain Behav. 2020; 10(11):e01842. doi: 10.1002/brb3.1842 Epub 2020 Oct 6. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Moghadasi AN, Mirmosayyeb O, Mohammadi A, Sahraian MA, Ghajarzadeh M. The prevalence of cognitive impairment in patients with neuromyelitis optica spectrum disorders (NMOSD): A systematic review and meta-analysis. Mult Scler Relat Disord. 2021; 49:102757. doi: 10.1016/j.msard.2021.102757 Epub 2021 Jan 15. . [DOI] [PubMed] [Google Scholar]
- 28.Chamot E, Kister I, Cutter GR. Bifactor structure of clinical disability in relapsing multiple sclerosis. Mult Scler Relat Disord. 2014; 3(2):176–85. doi: 10.1016/j.msard.2013.06.005 Epub 2013 Jul 12. . [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Qualified researchers may request access to individual patient level data through the clinical study data request platform (https://vivli.org/). Further details on Roche's criteria for eligible studies are available here (https://vivli.org/members/ourmembers/). For further details on Roche's Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_trials/our_commitment_to_data_sharing.htm).