

Abstract
Background:
Child maltreatment reports (CMR) are both common and strongly associated with various negative outcomes.
Objective:
To examine CMR risks by child age, early childhood context, current/cumulative economic status (welfare receipt), race, and other risk factors with a longitudinal dataset.
Participants and Setting:
The CAN sample included 2,111 children having a CMR ≤ age 3, suggestive of a harmful early childhood context. The AFDC sample included 1,923 children having AFDC but no CMR ≤ age 3, suggestive of early childhood protective factors despite poverty.
Methods:
We estimated the CMR likelihood at each age from 1–17 years based on various risk factors while following up children from 1995–2009.
Results:
During follow-up, CMR likelihoods were substantially higher for the CAN sample than for the AFDC sample. The age-CMR relationship was strongly negative for the CAN sample (OR=0.87, 95% CI=0.86–0.88). This relationship was weaker for the AFDC sample (OR=0.92, 0.89–0.95) and became non-significant for children who exited welfare. Current welfare receipt remained a strong predictor of CMR likelihoods for both CAN (OR=2.32, 1.98–2.71) and AFDC (OR=2.08, 1.61–2.68) samples. Prior welfare receipt moderately increased CMR likelihoods among those not currently on welfare. Controlling for other risk factors, White children had the highest likelihood of CMR. Other child and parent level vulnerabilities also increased CMR risk over time.
Conclusions:
This study highlights the importance of longitudinal analytic approaches and the utility of cross-sector administrative data in improving our ability to understand and predict CMRs over time.
Keywords: child maltreatment, child abuse, child protective services, multilevel growth curve model, administrative data analysis
Introduction
Child maltreatment is widespread and associated with a range of psychological, behavioral, medical, and social problems (Anda et al., 2006; Gilbert et al., 2009). Each year, over 4% of US children are reported to child protective services (CPS) for maltreatment concerns (U.S. DHHS, 2019). Rates of child maltreatment reports (CMRs) are highest among children under age four (U.S. DHHS, 2019), and age-related vulnerabilities have led many to focus on this group (Constantino et al., 2016). It is estimated, however, that one in three US children will have at least one CMR by age 18 (Kim, Wildeman, Jonson-Reid, & Drake, 2017), meaning risk continues throughout childhood. Yet, we know relatively little how CMR risk changes as children reach different developmental stages.
A large body of evidence supports that poverty is a strong risk factor for CMRs (Drake & Jonson-Reid, 2014; Pelton, 2015; Slack, Berger, & Noyes, 2017). Many prior studies have examined the relationships between poverty, other risk factors, and CMR risk (Beimers & Coulton, 2011; Courtney, Dworsky, Piliavin, & Zinn, 2005; Irwin, 2009; McDaniel & Slack, 2005; Needell, Cuccaro-Alamin, Brookhart, & Seon, 1999; Ovwigho, Leavitt, & Born, 2003; Putnam-Hornstein & Needell, 2011; Slack, Lee, & Berger, 2007). However, most prior studies disregard changes in risk factors over time using only baseline information to predict onset or recurrence. For example, while existing evidence well documents differences in CMR risk by economic status and/or racial group (Kim & Drake, 2018; Pelton, 2015; Putnam-Hornstein, Needell, King, & Johnson-Motoyama, 2013), we know little about whether these differences vary by child age. Further, studies are often too short in duration to assess risk across childhood and adolescence (≤ 5 years). Many studies have found a decreased risk of CMR by age (e.g., Kim et al., 2017; Sabol, Coulton, & Polousky, 2004), but it is not clear if this varies according to early childhood risk. For example, some research suggests that early maltreatment onset does not predict worse outcomes among children with multiple reports (Jaffee & Maikovich-Fong, 2011), suggesting later proximal conditions are more important. It is also possible that an early experience of poverty may confer risk (Luby et al., 2013) that increases the likelihood risk of later CMR.
Another limitation in the literature lies in how CMR is conceptualized. The federal government uses the word “victim” when a CMR receives a disposition of substantiated. However, relatively few cases (17% in 2017) meet this legal standard (U.S. DHHS, 2019). While prior studies have relied upon substantiated cases or receipt of child welfare services like foster care as the indicator of maltreatment (e.g., Beimers & Coulton, 2011; Ovwigho et al., 2003; Paxson & Waldfogel, 2003), a number of studies have found that substantiated and unsubstantiated children are at similar risk for a wide range of negative outcomes (Hussey et al., 2005; Kohl, Jonson-Reid, & Drake, 2009; Leiter, Myers, & Zingraff, 1994; Putnam-Hornstein, 2011). Other studies have relied on measures that may be a proxy for maltreatment rather than a direct measure of maltreatment (Berger, 2004). While criticism of CMR as a measure of maltreatment due to policy variations by region and possible biases in reporting exists, studies have found that official reports confer unique risk of later poor outcomes and show concurrent validity with related issues like child injury (Jonson-Reid, Drake, & Kohl, 2009; Putnam-Hornstein, 2011; Spivey, Schnitzer, Kruse, Slusher, & Jaffe, 2009). Finally, some studies have estimated risk of maltreatment based on retrospective self-report (e.g., Hussey, Chang, & Kotch, 2006), which makes it impossible to determine risk at a particular age.
To help close gaps in the existing knowledge base, this study explored child level change in risk of CMR over time from early childhood through adolescence. Drawing on a longitudinal multi-sector dataset it was possible to compare later CMR risk according to two different early childhood risk contexts (CMR versus poverty only at age ≤ 3) while documenting changes in family welfare use and select child and caregiver risk in each year.
Background: Research Questions and Conceptual Frameworks
The present study explored four research questions:
Does the relationship between child age and CMR risk differ by early childhood CMR context and economic status? If CMR risk is higher at younger ages due to the age-related vulnerabilities, then the risk should diminish over time. Prior studies have found a negative association between child age and CMR risk among low income populations (Beimers & Coulton, 2011; Cancian, Yang, & Slack, 2013; Irwin, 2009; Needell et al., 1999; Ovwigho et al., 2003; Slack et al., 2003). On the other hand, the life course perspective suggests that long term outcomes may be impacted by the enduring effects of early childhood contexts (White & Wu, 2014). Studies of CMR focused on recurrent reports and controlling for age of onset have been limited to a CPS population (Jaffee & Maikovich-Fong, 2011; Jonson-Reid, Emery, Drake, & Stahlschmidt, 2010). The context of poverty in early childhood may also increase later risk of CMR through its impact on child development (Luby et al., 2013) and stress on the family (Pelton, 2015). Over time, this could narrow differences in CMR risk between the two groups. The ecological perspective also suggests that age-related vulnerabilities may interact with factors like family economic status (Belsky, 1980). In other words, it is not known how early CMR compares to risk of later maltreatment conferred by early poverty while controlling for changes in risk factors and family economic status. The present study helps to fill this gap.
Is there an interaction between current economic state and the cumulative history of economic status related to risk of CMR? Studies that explore the impact of poverty at a given point in time have proposed theoretical links to specific forms of maltreatment. For example, neglect may occur when low socioeconomic status (at the family and/or community levels) limits resources for families to provide adequate care for their children (Berger, 2004; Maguire-Jack & Klein, 2015; Pelton, 1978, 1994) or leads to greater risk of harm from health and safety hazards (e.g., inadequate housing) (Pelton, 1978, 1994, 2015). Others suggest that poverty influences maltreatment risk via stress. Poverty may increase parental stress leading to neglect if parents withdraw from a caretaking role due to depression (Garbarino, 1977; Pelton, 2015). Poverty induced stress, however, may also lead to physical abuse because stress leads to reacting poorly to even trivial irritations by children (Pelton, 1978, 2015). The life course and developmental perspectives suggest that cumulative disadvantage affects social behaviors and norms (Geronimus, 1996; White & Wu, 2014). For example, families in chronic poverty may develop corporal punishment as a normative parenting behavior due to the continuing lack of resources to manage children’s behaviors with pecuniary incentives (Weinberg, 2001). This may increase the risk of child abuse (Stith et al., 2009). Studies have found that both current state and cumulative history of economic status are strongly associated with CMR risk (Doidge et al., 2017; Drake & Jonson-Reid, 2014; Kim & Drake, 2017; Pelton, 2015). However, it is unknown whether poverty history interacts with current economic status.
Does the relationship between race and CMR risk differ by child age and economic status? In the US, CMR risk is about two times higher among Black children than among White children (Drake et al., 2011). There have been two competing explanations posited in the child welfare literature. The racial bias perspective assumes that an unfair racial bias either at the reporting or early CPS screening level makes Black children more likely to have unnecessary CMRs (Hill, 2004, 2006; Morton, 1999; Sedlak et al., 2010). The differential risk perspective hypothesizes that Black children have a higher exposure to risk factors (e.g., poverty) related to maltreatment, which increases the likelihood of CMRs (Drake, Lee, & Jonson-Reid, 2009; Font, Berger, & Slack, 2012). Recent evidence shows that Black children have no higher CMR risk (and sometimes lower) than White children after controlling for risk factors, especially poverty (Drake et al., 2009; Kim & Drake, 2017; Maloney, Jiang, Putnam-Hornstein, Dalton, & Vaithianathan, 2017; Putnam-Hornstein et al., 2013). As yet, we know little about whether such relationships change according to a child’s age and current versus past economic history.
Do changes in other risk factors over time predict CMR risk? Life course theory suggests that adversities experienced by children and families (e.g., mental health, injury) will strongly predict future CMRs (White & Wu, 2014). Others have suggested that early risk (e.g., early CMR) may not be predictive of later outcomes once changes in the context of risk over time are controlled (Jaffee & Maikovich-Fong, 2011; MacKenzie, Kotch, Lee, Augsberger, & Hutto, 2011). Maltreatment may also impact ongoing risk. Studies suggest higher risk of child behavior problems following maltreatment (e.g., Hussey et al., 2005) and higher risk of maltreatment among children with behavioral problems (Jaudes & Mackey-Bilaver, 2008). Although the present study is limited to child problems known to education, health or juvenile justice systems, it is the first to attempt to control for development of new risks over time.
Method
Data analyzed were drawn from a larger study based in St. Louis (City and County), Missouri (Jonson-Reid et al., 2009). The parent study linked multiple administrative data sets to trace children with a CMR or an AFDC case at time of sampling (1993–1994) to understand patterns of service use and outcomes. When there were multiple children in a family, the parent study randomly selected one child. This made the child level equivalent to the family level in the present study. The linkage and cleaning procedures are described in prior publications (Jonson-Reid et al., 2009, 2010). Human subject approval for the present study included individual agency agreements as well as Institutional Review Board approval by (omitted for blind review).
Sampling and Follow-up
The present study had two separate samples having very different early childhood contexts: children with a CMR in early childhood (the Child Abuse and Neglect [CAN] sample) and children with AFDC but no CMR in early childhood (the AFDC sample). Specifically, the CAN sample (N = 2,111) included the full population of children from Missouri CPS records who met the following criteria during the sampling period (i.e., 1993–1994): (1) having a first-time CMR for alleged neglect, physical abuse, or sexual abuse; (2) aged 3 or younger; and (3) residing in St. Louis. It is worth noting that the CAN sample included children with an AFDC case (78.6%), as well as children with no AFDC case (22.4%). The large proportion of children with an AFDC case in the CAN sample was consistent with the well-known relationship between poverty and CMRs (Pelton, 2015). The AFDC sample (N = 1,923) included children randomly selected from Missouri AFDC records who met the following criteria during the sampling period (i.e., 1993–1994): (1) having an active AFDC case; (2) having no current or prior CMR; (3) aged 3 or younger; and (4) residing in St. Louis. Before this selection, the parent study stratified AFDC records by child age and residential region (St. Louis City vs. County). Then, the parent study randomly selected the AFDC sample children that were similar in number to the CAN sample children for each stratum. The present study uses “AFDC” to describe a sample, as well as a participation in a welfare program. When “AFDC” indicates a sample, we always affix “sample” (i.e., the AFDC sample). Otherwise, “AFDC” indicates the AFDC program. AFDC was replaced by TANF during the study period, so the term “welfare” is used to refer to either after baseline.
Both groups were followed from January 1995 (after the close of the sampling period) through March 2009. Children born in 1991 were followed from age 4 to 17, children born in 1992 were followed from age 3 to 16, children born in 1993 were followed from age 2 to 15, and those born in 1994 were followed from age 1 to 14. Data were reformatted into age-year observations, leaving 32,348 (age-year) observations for the CAN sample and 25,596 observations for the AFDC sample. Follow-up was ended at the time of a child’s death (0.66% of the CAN and 0.41% of the AFDC group), out-of-home placement due to the desire to follow CMRs in the family of origin (21.25% and 3.70%), and childbirth which may be indicative of emancipation or no longer residing in the family of origin (0.009% and 0.004%). The final sample sizes were 25,258 observations of 2,111 children in 235 baseline tracts for the CAN sample and 24,552 observations of 1,923 children in 210 baseline tracts for the AFDC sample.
Variables and Data Sources
Table 1 lists the study variables and data sources. We established temporal order between predictors and CMRs based on dates of service contacts in the data. It should be noted that a contact date of a service (e.g., welfare) may or may not reflect the actual onset of a given problem (e.g., low economic status). It is also worth noting that most administrative records of this study are statewide. Families moving out of St. Louis but within Missouri, therefore, were not lost to the study. Records for special education and juvenile court were limited to the St Louis region. The geographic limitations are mitigated by the fact that more disadvantaged families tend to make shorter distance moves although they are frequent (Coulton, Theodos, & Turner, 2012). Further, census data indicate that when families move they are more likely to move from St Louis City to the County not to neighboring Illinois communities (Jaco, 2019).
Table 1.
Variable Description, Data Source, and Descriptive Statistics
| Variables | Description | Data source | % or M (SD) | |
|---|---|---|---|---|
| CAN sample | AFDC sample | |||
| Level-1 (age-year observation) | N1=25,258 | N1=24,552 | ||
| Outcome: CMR | 1=having a maltreatment report (CMR);0=no | CPS, 1995–2009 | 11.4% | 5.5% |
| Child age | Current child age (min=1;max=17;1 unit=1 year) | Birth, 1991–1994 | 8.87 (3.96) | 8.91 (3.95) |
| Current welfare | 1=on welfare (AFDC/TANF) at current age;0=no | Welfare, 1995–2009 | 35.6% | 30.7% |
| Prior welfare | % months on welfare by prior age | Welfare, 1991–2009 | 51 (37) | 50 (32) |
| TANF time limit | 1=reaching TANF lifetime limit; 0=no | Welfare, 1997–2009 | 3.9% | 2.9% |
| TANF no limit | 1=receiving TANF after 60-month limit; 0=no | Welfare, 1997–2009 | 5.6% | 3.7% |
| Prior CPS report | 0 prior report | CPS, 1991–2009 | - | 78.6% |
| 1 prior report | 49.2% | 13.5% | ||
| 2 prior reports | 22.3% | 4.5% | ||
| 3 prior reports (3+ for AFDC sample) | 11.7% | 3.4% | ||
| 4+ prior reports | 16.8% | - | ||
| FCS only | 1=prior Family Centered Services only;0=no | CPS, 1991–2009 | 26.6% | 7.6% |
| IIS w/ or w/o FCS | 1=prior Intensive In-home Services; 0=no | CPS, 1991–2009 | 9.1% | 2.8% |
| Child current injury | 1=ER injury record at current age; 0=no | ER, 1997–2009 | 4.8% | 4.5% |
| Child prior injury | 1=ER injury record before current age; 0=no | ER, 1997–2009 | 29.6% | 27.5% |
| Child current MH | 1=ER MH record at current age; 0=no | ER, 1997–2009 | 0.8% | 0.4% |
| Child prior MH | 1=ER MH record before current age; 0=no | ER, 1997–2009 | 3.4% | 1.8% |
| Child mental delay | 1=ER mental delay record; 0=no | ER, 1997–2009 | 0.5% | 0.2% |
| Child chronic health | 1=ER chronic/serious health record; 0=no | ER, 1997–2009 | 0.8% | 0.3% |
| Child current delinquency | 1=JC/arrest record at current age; 0=no | JC/Arrest, 1991–2009 | 1.9% | 1.3% |
| Child prior delinquency | 1=JC/arrest record before current age; 0=no | JC/Arrest, 1991–2009 | 3.9% | 2.7% |
| Child special education | 1=special education (SE) record; 0=no | SE, 1991–2006 | 16.4% | 10.6% |
| Parent current conviction | 1=conviction record at current age; 0=no | Conviction, 1975–2007 | 1.1% | 0.7% |
| Parent prior conviction | 1=conviction record before current age; 0=no | Conviction, 1975–2007 | 2.8% | 1.4% |
| Parent current arrest | 1=arrest record at current age; 0=no | Arrest, 1963–2008 | 0.7% | 0.4% |
| Parent prior arrest | 1=arrest record before current age; 0=no | Arrest, 1963–2008 | 8.6% | 4.5% |
| Level-2 (child/family) | N2=2,111 | N2=1,923 | ||
| Child race | Non-Hispanic/Latino White only | Birth, 1991–1994 | 32.3% | 16.8% |
| Non-Hispanic/Latino Black only | 66.4% | 81.5% | ||
| Other minority (Asian, Hispanic/Latino, etc.) | 1.3% | 1.7% | ||
| Child birth weight | Normal (≥2.5kg) | Birth, 1991–1994 | 89.5% | 91.3% |
| Low (<2.5kg, ≥1.5kg) | 9.0% | 7.4% | ||
| Very low (<1.5kg) | 1.5% | 1.3% | ||
| Birth year | 1991 | Birth, 1991–1994 | 33.2% | 31.2% |
| 1992 | 32.6% | 32.5% | ||
| 1993 | 25.7% | 27.6% | ||
| 1994 | 8.5% | 8.7% | ||
| Child sex | 1=female; 0=male | Birth, 1991–1994 | 47.9% | 47.0% |
| Medicaid at birth | 1=on Medicaid at subject child's birth; 0=no | Birth, 1991–1994 | 60.3% | 65.3% |
| Mom no high school | 1=no HS degree at subject child’s birth; 0=no | Birth, CPS, AFDC | 53.3% | 46.0% |
| Mom teen birth | 1=mom < age 20 at subject child's birth; 0=no | Birth, CPS, AFDC | 27.2% | 25.6% |
| Mom foster care | 1=mom in foster care during her youth; 0=no | CPS | 6.6% | 3.4% |
| Baseline no AFDC | 1=no AFDC at baseline (for CAN sample);0=no | AFDC, 1991–1994 | 22.4% | - |
| Level-3 (tract) | N3=235 | N3=210 | ||
| Baseline poverty rate | % persons whose income below poverty level | 1990 Census | 22.6 (16.0) | 25.4 (15.5) |
| Baseline mobility rate | % households that moved within last 5 years | 1990 Census | 45.2 (11.9) | 44.8 (12.4) |
| Baseline child/adult ratio | (# children aged 0 to 13)/(# adults aged 21+) | 1990 Census | 0.3 (0.1) | 0.3 (0.1) |
CPS = child protective services. ER = emergency room. MH = mental health. JC = juvenile court. Conviction = prison, parole, or probation. M = mean. SD = standard deviation. N1 = number of child-age observations. N2 = number of children. N3 = number of tracts.
Variables that were subject to change over time were added as (yes/no) indicators within each person year. For ease of presentation, only child demographics and the primary poverty and CMR measures are discussed here. Discussion of other child, family, and neighborhood level risk factors (drawn from birth records, child welfare services, emergency room data, special education records, juvenile justice records, criminal records, and Census data) is provided in Appendix A in the Supplement.
Dependent variable: Child Maltreatment Report (CMR).
Screened-out reports were not archived in the state system, but both substantiated and unsubstantiated reports were retained. We used a binary measure of any CMR as per the discussion in the introduction, coded 1 when having a CMR at a given age and 0 otherwise.
Current welfare and prior welfare.
We used welfare receipt status as a crude proxy of family economic status. Both AFDC and TANF income eligibility thresholds were about 50% of the federal poverty threshold for applicants and even lower for long-term recipients, indicative of a very low economic status (i.e., extreme poverty). We measured current welfare and prior welfare by the receipt status of Aid to Families with Dependent Children (AFDC) before 1997 or Temporary Assistance for Needy Families (TANF) from 1997 on. Current welfare was coded 1 when receiving welfare (AFDC or TANF) at the current age and 0 otherwise. Prior welfare was a continuous measure of the percentage of months receiving welfare from the subject child’s birth prior to the current age. As most of the sample children were receiving welfare at baseline, current welfare compared welfare recipients (= currently on welfare) and welfare leavers (= currently not on welfare) during the follow-up period. While some raise concerns about welfare leavers still enduring high levels of material hardship (Boushey & Gundersen, 2001; Miller, 2002), prior studies have found most exits from welfare associated with a sharp increase of income (Acs & Loprest, 2001; Miller, 2002; Moses, Mancuso, & Lieberman, 2000; Verma & Coulton, 2001). Improving economic conditions is the most common reason for leaving welfare (Coulton, Lickfelt, Lalich, & Cook, 2005; Loprest, 2002; Moses et al., 2000; Ovwigho et al., 2003). Previous studies of families eligible for welfare found that recipients were economically better off than non-recipients (Moffitt, 1992; Nicoll, 2015; Zedlewski, 2002).
Child age.
The time variable was child age in years. This variable was measured as a continuous variable, ranging from 1 to 17.
Child race and sex.
The subject child’s race was categorized as White (non-Hispanic/Latino White only), Black (non-Hispanic/Latino Black only), and “Other” (including Asian, Hispanic/Latino, and other minority groups) based on birth records. The St. Louis population mostly consisted of White (74%) and Black (23%) people. We could not further break down the “Other” race group as it was very small due to the demographics of the region at the time. The administrative records were limited to coding gender according to male or female.
Analysis
The “lme4” package (version 1.1–15) in R (version 3.4.4) was used for the analyses. Multilevel logistic growth curve models were used to estimate the change in likelihood of having any (first or any subsequent) CMR at each age from 1 to 17 years as a function of various predictors measured by administrative records. We used a multilevel design because age-year observations were nested in children and in turn, children were nested in their baseline residential tracts. The degree of dependency in the nested data can be measured by the intraclass correlation coefficient (ICC) (Snijders & Bosker, 2012). The level-2 ICC values were 0.33 for the CAN sample and 0.40 for the AFDC sample and the level-3 ICC values were almost zero for both samples. The ICC values indicated that 33% to 40% of the variance of the CMR likelihood was placed between level-2 units (children/families) while almost no variance was located between level-3 units (baseline tracts). Given the substantial degree of dependency, particularly between level-2 units, applying a traditional model would lead to severe type I errors. Multilevel modeling adjust standard errors according to the nested data structure (Luke, 2004). The model-building process involved making decisions about parsimony versus model fit, following the approach suggested by Snijders and Bosker (2012). We selected a final model by including only parameters with meaningful contributions to model fit (see Appendix B in the Supplement for details).
Results
Descriptive Results
Table 1 presents descriptive statistics. During the follow-up period, the CMR probability at a given age was higher for the CAN sample (11.4%) than the AFDC sample (5.5%). Most of the CAN sample children were also living in families receiving AFDC at baseline (only 22.4% not on AFDC). Both CAN and AFDC samples often received welfare (AFDC/TANF) at later ages, 35.6% and 30.7% across ages, respectively. Compared to the proportion of Black children in the St. Louis child population from Census data (35.1%), Black children were overrepresented by 1.9 times in the CAN sample (66.4%) and 2.3 times in the AFDC sample (81.5%). This was consistent with studies examining representation in poor or maltreated populations at the national level (Drake et al., 2011). Other risk factors controlled were generally more common in the CAN sample than the AFDC sample.
Final Multilevel Growth Curve Models
Table 2 reports the final models. The final models showed fairly high levels of accuracy in predicting future CMRs. The area under the ROC curve (AUC) indicates the overall level of predictive accuracy in balance between sensitivity and specificity. The final models predicted CMRs with 74.73% accuracy for the CAN sample (AUC = 74.73) and with 73.35% accuracy for the AFDC sample (AUC = 73.35). This suggests that using the estimated coefficients of the final models (γ in Table 2), one can predict a child’s CMR risk with an acceptable level of accuracy based on the child’s age and the child’s current state and prior history of risk factors. For example, Figure 1 presents the predicted risks by child age, current welfare, and prior welfare while fixing all other predictors to their grand mean.
Table 2.
Final Models of Child Maltreatment Report Likelihoods.
| CAN sample (N1=25,258, N2=2,111, N3=235) |
AFDC sample (N1=24,552, N2=1,923, N3=210) |
||||||
|---|---|---|---|---|---|---|---|
| Fixed effect | γ | SE | OR (95% CI) | γ | SE | OR (95% CI) | |
| Level 1 predictors | |||||||
| Intercept | −3.1529 | .0878 | - | −3.8676 | .1307 | - | |
| Child agea | −0.1394 | .0087 | 0.87 (0.86, 0.88) | −0.0125 | .0147 | 0.99 (0.96, 1.02) | |
| Current welfare | 0.8402 | .0807 | 2.32 (1.98, 2.71) | 0.7311 | .1307 | 2.08 (1.61, 2.68) | |
| Prior welfarea (1 unit=10% point) | 0.0768 | .0130 | 1.08 (1.05, 1.11) | 0.1174 | .0192 | 1.12 (1.08, 1.17) | |
| Child agea × Current welfare | −0.0704 | .0183 | 0.93 (0.90, 0.97) | ||||
| Current welfare × Prior welfarea | −0.0782 | .0187 | 0.92 (0.89, 0.96) | −0.1457 | .0288 | 0.86 (0.82, 0.91) | |
| Prior CPS report: | |||||||
| 0 | - | - | - | Reference group | |||
| 1 | Reference group | 0.5165 | .1122 | 1.68 (1.35, 2.09) | |||
| 2 | 0.5308 | .0638 | 1.70 (1.50, 1.93) | 0.6097 | .1696 | 1.84 (1.32, 2.57) | |
| 3 (3+ for AFDC sample) | 0.9031 | .0769 | 2.47 (2.12, 2.87) | 0.9683 | .2154 | 2.63 (1.73, 4.02) | |
| 4+ | 1.1529 | .0852 | 3.17 (2.68, 3.74) | - | - | - | |
| FCS only | −0.2842 | .0610 | 0.75 (0.67, 0.85) | −0.2757 | .1262 | 0.76 (0.59, 0.97) | |
| IIS with and without FCS | 0.1611 | .0797 | 1.17 (1.00, 1.37) | 0.4337 | .1707 | 1.54 (1.10, 2.16) | |
| Child current injury | 0.4258 | .0895 | 1.53 (1.28, 1.82) | 0.5170 | .1242 | 1.68 (1.31, 2.14) | |
| Child prior injury | 0.0877 | .0620 | 1.09 (0.97, 1.23) | 0.1760 | .0875 | 1.19 (1.00, 1.42) | |
| Child current mental health | 1.3759 | .1760 | 3.96 (2.80, 5.59) | 1.1404 | .2852 | 3.13 (1.79, 5.47) | |
| Child prior mental health | 0.3241 | .1233 | 1.38 (1.09, 1.76) | 0.7202 | .1982 | 2.05 (1.39, 3.03) | |
| Child chronic health problem | 0.6179 | .2429 | 1.86 (1.15, 2.99) | - | - | - | |
| Child current delinquency | 0.8090 | .1500 | 2.25 (1.67, 3.01) | - | - | - | |
| Child prior delinquency | 0.1714 | .1322 | 1.19 (0.92, 1.54) | - | - | - | |
| Child special education | 0.1527 | .0699 | 1.16 (1.02, 1.34) | 0.2682 | .1122 | 1.31 (1.05, 1.63) | |
| Parent current conviction | 0.1591 | .2477 | 1.17 (0.72, 1.91) | - | - | - | |
| Parent prior conviction | −0.5307 | .1925 | 0.59 (0.40, 0.86) | - | - | - | |
| Parent current arrest | 0.5223 | .2071 | 1.69 (1.12, 2.53) | 0.8828 | .3256 | 2.42 (1.28, 4.58) | |
| Parent prior arrest | 0.0487 | .0903 | 1.05 (0.88, 1.25) | 0.5430 | .1469 | 1.72 (1.29, 2.30) | |
| Level 2 predictors | |||||||
| Child race (ref. White): Black | −0.1751 | .0622 | 0.84 (0.74, 0.95) | −0.4301 | .1035 | 0.65 (0.53, 0.80) | |
| Other | −0.8907 | .3470 | 0.41 (0.21, 0.81) | −0.8503 | .3688 | 0.43 (0.21, 0.88) | |
| Birth year (ref. 1991): 1992 | −0.1422 | .0638 | 0.87 (0.77, 0.98) | - | - | - | |
| 1993 | −0.2278 | .0698 | 0.80 (0.69, 0.91) | - | - | - | |
| 1994 | −0.1793 | .0982 | 0.84 (0.69, 1.01) | - | - | - | |
| Mom no high school | 0.2613 | .0563 | 1.30 (1.16, 1.45) | 0.4886 | .0837 | 1.63 (1.38, 1.92) | |
| Mom foster care | 0.2118 | .0946 | 1.24 (1.03, 1.49) | 0.4426 | .1843 | 1.56 (1.08, 2.23) | |
| Random effect | Variance | Variance | |||||
| Level-2: Intercept | 0.6740 | 1.2349 | |||||
| Level-2: Current welfare | 0.6165 | 1.3246 | |||||
| Level-3: Intercept | 0.0000 | 0.0000 | |||||
| Area under the ROC curve | 0.7473 | 0.7335 | |||||
Centered to grand mean. N1 = number of age-year observations. N2 = number of children. N3 = number of baseline residential tracts. ref. = reference group. γ = coefficient. SE = standard error. OR = odds ratio. CI = confidence interval. Significant odds ratios (p < .05) are in boldface. White = non-Hispanic/Latino White only. Black = non-Hispanic/Latino Black only. Other = other minority including Asian, Hispanic/Latino, and other minorities.
Figure 1. Estimated child maltreatment report likelihoods by child age, current welfare and prior welfare.
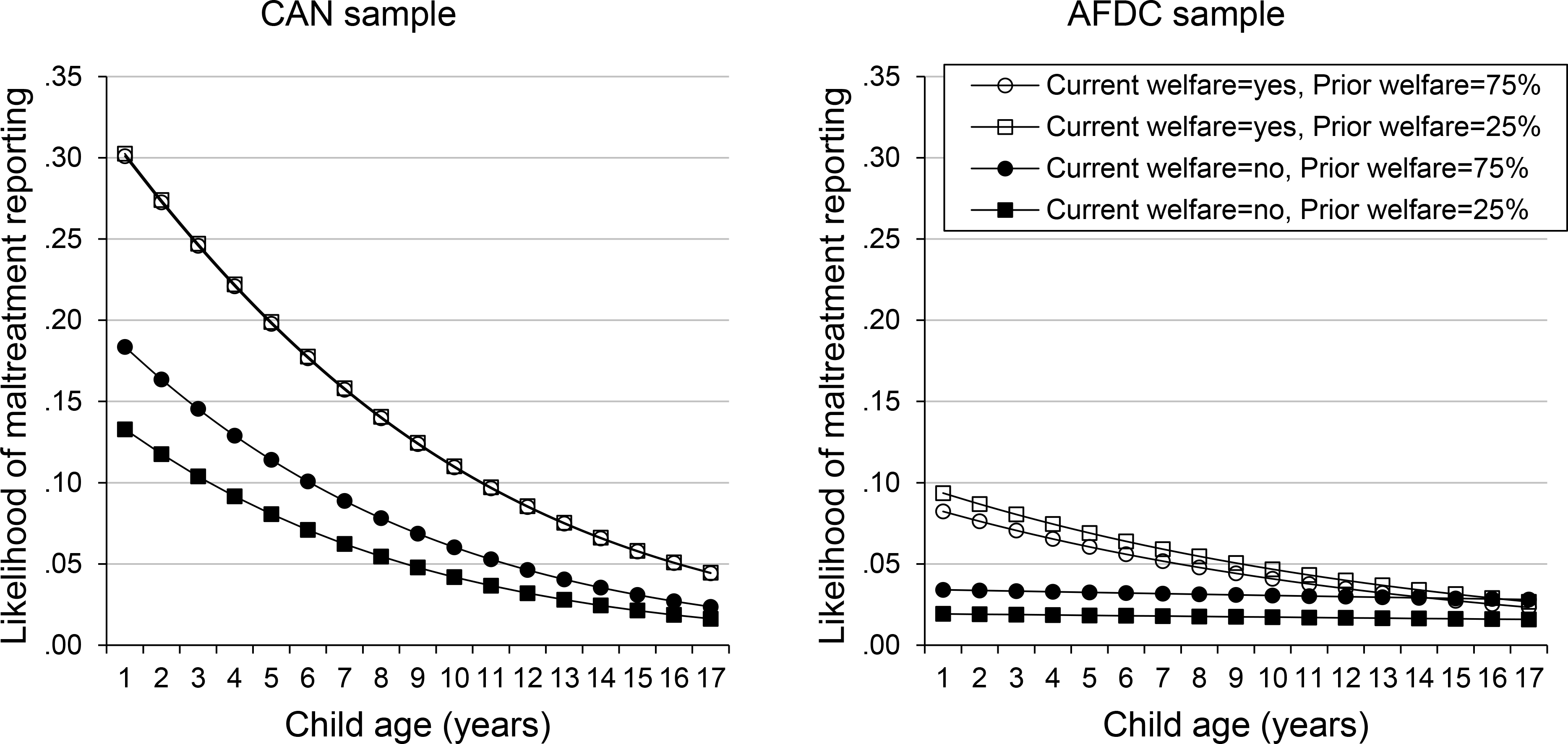
Note: Estimates are based on the final models in Table 2. All other variables are fixed to their grand mean. The “Current welfare=yes, Prior welfare=75%” and “Current welfare=yes, Prior welfare=25%” lines for the CAN sample are overlapped since the effect size of prior welfare is practically 0 when currently on welfare.
In the CAN sample, a one-year increase of child age decreased the CMR likelihood by 13% (odds ratio [OR] = 0.87, 95% confidence interval = 0.86–0.88). This relationship did not significantly vary by current welfare, prior welfare, or child race (see Appendix B in the Supplement). In the AFDC sample, child age alone was not significant (OR = 0.99, 0.96–1.02), whereas the child age × current welfare interaction was significant (OR = 0.93, 0.90–0.97). Due to the significant interaction, we computed odd ratios and confidence intervals of child age by current welfare (on welfare vs. not on welfare) from the model results (see Appendix C in the Supplement). The results showed that in the AFDC sample, there was no significant association between child age and the CMR likelihood while currently not on welfare (OR = 0.99, 0.96–1.02), whereas the CMR likelihood decreased by 8% per one-year increase of child age while currently on welfare (OR = 0.92, 0.89–0.95). These relationships did not differ by prior welfare history or child race (see Appendix B in the Supplement).
The CMR likelihood was over two times higher while currently on welfare than not on welfare in both CAN sample (OR = 2.32, 1.98–2.71) and AFDC sample (OR = 2.08, 1.61–2.68). The relationship between prior welfare and CMR likelihood varied by current welfare status in both samples (see the Appendix B in the Supplement). This required additional computation to estimate odds ratios and confidence intervals of prior welfare by current welfare (see Appendix C in the Supplement). Among children in families not currently on welfare, a 10-percentage-point increase in prior welfare increased the CMR likelihood by 8% in the CAN sample (OR = 1.08, 1.05–1.11) and by 12 % in the AFDC sample (OR = 1.12, 1.08–1.17). While children were currently on welfare, this relationship disappeared for both the CAN (OR = 1.00, 0.97–1.03) and AFDC samples (OR = 0.97, 0.93–1.02).
Due to the complex interactions among child age, current welfare, and prior welfare, we plot prediction graphs in Figure 1. Overall, the CMR likelihood was much higher for the CAN sample than for the AFDC sample, especially at younger ages. The CAN sample children showed substantially higher CMR likelihoods at younger ages regardless of current welfare. The AFDC sample children also showed higher CMR likelihoods at younger ages, but only when currently on welfare. When currently not on welfare, the AFDC sample children showed no higher CMR risks at younger ages. The CMR likelihood was notably higher while currently on welfare. This gap persisted across ages in both samples, but was substantially diminished at older ages in the AFDC sample. Regarding prior welfare, a longer stay on welfare (i.e., 75% vs. 25% of the time) moderately increased CMR likelihoods only while currently not on welfare. In the CAN sample, the effect size of prior welfare was practically “0” when currently on welfare, and accordingly the corresponding prediction lines were almost completely overlapped. Among the AFDC sample children currently on welfare, those with a longer history of prior welfare had a slightly lower CMR likelihood. This difference, however, was not statistically significant.
Regarding race, Black children and other minority children had lower CMR likelihoods than White children in both samples while controlling for other variables. Compared to White children, the CMR likelihoods were lower by 16% to 35% for Black children (OR = 0.84, 0.74–0.95 in the CAN sample; OR = 0.65, 0.53–0.80 in the AFDC sample) and by 59% to 57% for other minority children (OR = 0.41, 0.21–0.81 in the CAN sample; OR = 0.43, 0.21–0.88 in the AFDC sample). These relationships did not significantly differ by child age, current welfare, and prior welfare (see Appendix B in the Supplement). Figure 2 shows that while controlling for other variables, Black children and other minority children have lower CMR likelihoods than White children at all ages from early childhood to adolescence regardless current welfare status.
Figure 2. Estimated child maltreatment report likelihoods by child age, current welfare and child race.

Note: Estimates are based on the final models in Table 2. All other variables are fixed to their grand mean. White = non-Hispanic/Latino White only. Black = non-Hispanic/Latino Black only. Other = other minority including Asian, Hispanic/Latino, and other minorities.
An interesting pattern of CMR risk emerged while comparing the current state and the prior history of child health and behavioral risk factors as well as parental arrest records. Generally, a currently noted risk factor had a larger effect size than the prior history of the same risk factor. For example, in the CAN sample, indication of a child’s current mental health problem in a given child/year increased the CMR likelihood by 3.96 times (OR = 3.96, 2.80–5.59). In comparison, child prior mental health problems increased the CMR likelihood by 1.38 times (OR = 1.38, 1.09–1.76).
Discussion
This is the first known published work examining the relationship of CMR risk over time with changes in economic and child and parental risk factors from early childhood to adolescence. This section reviews major findings followed by a discussion of limitations.
Regarding the first research question, our findings suggest that the relationship between child age and CMR risk differs by both early childhood context of CMR and economic status over time. Prior studies have found higher CMR risks among younger children (Kim et al., 2017; Sabol et al., 2004; Wildeman et al., 2014). However, our findings suggest that the presence and strength of this relationship varies by early risk and poverty. CMR risk was much higher at younger ages for children with a prior CMR in early childhood (i.e., the CAN sample). In contrast, among low-income children (AFDC sample) without a CMR in the first years of life, the relationship between age and CMR was weak or non-existent. Among AFDC sample children who exited welfare and were currently not on welfare, the CMR risk was not higher at younger ages. On the other hand, increased risk at younger ages did appear among children in the AFDC sample who were currently on welfare. It may be that age-related vulnerabilities such as physical and cognitive immaturity (Burman, 2016; Goodway, Ozmun, & Gallahue, 2019) and high care burden may interact with early risk and current economic status.
In regards to the second question, we found interaction between the current state and the cumulative history of economic status. Similar to some early work on AFDC and later child welfare involvement, a longer prior history of welfare receipt moderately increased CMR risk (e.g., Needell et al., 1999). However, in the present study, this only held for children currently not on welfare. When currently on welfare, prior welfare added no further risk. Although it may be premature to advance theoretical rationales for this interaction, our findings suggest that cumulative economic status does not further increase CMR risk when risk is already high due to current economic hardship. While the interaction is theoretically interesting, current economic status had a far more powerful relationship with CMR risk than the cumulative history of economic status in our model. Financial or material support for immediate economic hardship (Cancian et al., 2013; Rostad, Rogers, & Chaffin, 2017; Slack et al., 2017) may be the most practical intervention to reduce CMR risk among vulnerable children. Of course, further research is needed to understand how long such benefits may persist and what other resources or programs may be needed to more permanently reduce CMR risk.
The third research question focused on the relationship between race and CMR risk. We found that compared with White children, Black and other minority children had lower CMR risks while controlling for socioeconomic indicators and other risk factors over time. This relationship was consistent at all ages from early childhood to adolescence. Our findings are consistent with emerging evidence in studies done in different states that find Black children are equally or slightly less likely to be reported than similarly situated White children (Buek, Lakey, & Mandell, 2019; Drake et al., 2009; Kim & Drake, 2017; Maloney et al., 2017; Putnam-Hornstein et al., 2013). These findings suggest support for differential risk. For example, Black and certain other minority children face a much greater risk of growing up in poor families and/or poor neighborhoods (Drake & Rank, 2009). If we accept the premise that poverty increases the risk for maltreatment, then any group differentially at risk of poverty may be more at risk of CMR. Further, unlike later child welfare decisions like case closure or entry into care, a report of child maltreatment does not originate from child welfare. Roughly 40% of reports come from neighbors, family or self-report and those that do come from mandated reporters typically come from educators or law enforcement – not social workers (Drake, Jonson-Reid, & Kim, 2017; U.S. DHHS, 2019). Addressing differential risk exposure, especially poverty disparity, between Black and White children may be a promising strategy to address the pervasive racial difference in child welfare contact.
Finally, we explored whether findings in age-related risk varied by other child and parent characteristics over time. First, changes in CMR risk by age and economic status variables remained while controlling for child health, behavioral health and other risks as well as parent arrest over time. The final models showed 74.73% (the CAN sample) to 73.35% (the AFDC sample) accuracy in prediction, which were fairly high levels of accuracy. While there was support for the continued risk associated with an early maltreatment report (White & Wu, 2014), there was also support for the idea that early maltreatment may place a child at greater risk of a number of child level conditions and behaviors that may in turn increase the risk of ongoing maltreatment (MacKenzie et al., 2011). There was also evidence for an ever-increasing risk of ongoing maltreatment based on the number of prior CMRs which is consistent with ideas of increased risk of re-victimization once children experience one form of victimization (Finkelhor, Ormrod, & Turner, 2007). Importantly, near term risk conditions tended to be most predictive of CMR. While this does not indicate that current conditions are more important than cumulative risk in regard to child outcomes, it does suggest that addressing a families immediate material needs as well as existing child factors that are consistent with the child well-being metrics (Jonson-Reid & Drake, 2016) for child welfare are key to interrupting the next CMR episode.
Strengths and Limitations
This study has several strengths. First, we estimated future CMR risks of very young high-risk children frequently encountered by the state service systems (i.e., the CAN and AFDC samples). Our findings therefore may be useful for secondary prevention efforts by further stratifying risk levels among high-risk children. Second, we examined both current state and prior history of risk factors while considering their changes over time. This allowed for improving predictive accuracy, but also for identifying an interesting longitudinal pattern. We found that the recent status of risk factors was more strongly linked to current CMRs than prior history, suggesting that prompt supports for families’ present needs may reduce CMRs. Using linked administrative data allowed for measuring the dates associated with CMRs, welfare, and other relevant risk factors while reducing bias associated with measuring risk through retrospective recall. Finally, we used multilevel growth curve modeling, a powerful and flexible way to handle missing or censored observations and to examine longitudinal changes and cross-level influences simultaneously (Luke, 2008). This method allowed us to continue following up children even after the first event and examining the risk of subsequent CMRs at specific ages. Most prior studies estimate only the risk of the first event (e.g., the first-time CMR or the first recurrence of CMR). Instead, we provide models that are useful to predict a child’s risk at any age and at any stage of CMR (i.e., first, second, third, and any subsequent CMRs). Traditional approaches using baseline information may be more useful for early prevention efforts. However, our approach using both baseline information and over-time changes can be useful to identify families at imminent risk for ongoing maltreatment at different child ages.
There are, however, limitations to the present approach. Despite the established temporal ordering, we are unable to establish causal relationships as there may be unmeasured factors that could influence the parameter estimates. This is not an uncommon problem in research focused on risk conditions that are not ethically amenable to randomization (e.g., poverty or usual care services in response to referral). Further, observing families in context is often vital to understanding complex longitudinal and socio-ecological processes related to engaging with multiple child, family and adult serving systems.
Another limitation concerns the use of welfare receipt as a proxy of economic status and child maltreatment reports as an outcome rather than actual child maltreatment events. Welfare receipt does not capture the full range of economic status and material need that may impact a family’s functioning (e.g., Berger, 2004). On the other hand, prior studies have consistently found that welfare receipt (Irwin, 2009; McDaniel & Slack, 2005; Slack et al., 2003) and other economic indicators (Courtney et al., 2005; Dworsky, Courtney, & Zinn, 2007; Maguire-Jack & Klein, 2015) were strongly associated with child maltreatment while controlling for marital status and other variables. Additionally, welfare receipt and the possible implications for families present in both welfare and CPS systems are arguably very relevant for policy (Berrick, Frame, Langs, & Varchol, 2006; Slack et al., 2007).
The second concern relates to whether or not a CMR reflects actual maltreatment concerns. Much of this was addressed in the introduction and background provided with the research question and is not repeated here. As stated, CMR have been found to be sufficient markers of a number of later outcomes (Hussey et al., 2005; Putnam-Hornstein, 2011), concurrent outcomes like child injury that may be indicative of maltreatment (Spivey et al., 2009), and child outcomes across domains controlling for poverty (Jonson-Reid et al., 2009). Further, data measuring maltreatment across multiple years have been found to predict similar incidence rates as lifetime self-report studies (Kim et al., 2017). Thus, the present of repeated measures of CMR over time decreases the likelihood of detection. It is, however, not possible to know whether a report reflects actual onset of abuse and neglect or simply when the concerns were sufficient to be noticed by others.
Other limitations are related to our use of secondary data. First, access to records for children with neither welfare receipt nor CMR in early childhood were not possible in the parent study. Therefore, findings cannot be generalized to child populations without early risk related to poverty or maltreatment. Second, this study provides no estimate for risk at birth due to the parent study’s sampling design. National data have identified exceptionally high CMR risks prior to the first year of life (Kim et al., 2017; U.S. DHHS, 2019; Wildeman et al., 2014). Future research is needed that can track groups prior to birth and continue throughout adolescence. Administrative data is by design limited to variables of interest for a given system. We were unable to assess need as compared to service receipt or system encounter. Nor are there sufficient indicators of protective factors in most administrative datasets. While the presence of a CMR in early childhood may be a good proxy for risk, the absence of a CMR is not the same as the presence of protective factors. Because the data came from a single state, outstate mobility could not be tracked or estimated. However, as stated in the methods, we believe the nature of the population and the unique context of the study location mitigate this concern. Our ability to examine parent level factors was largely limited to mothers due to the demographics of the families involved in welfare and CPS systems and we were unable to control for parental risk factors such as substance abuse. We also chose to limit community poverty controls to baseline due to the limitations in how addresses are captured over time. Only those with repeated CMR or welfare receipt would have updated addresses. Finally, another limitation has to do with the simple binary measure of most risk factors. While large administrative data can assure strong generalizability, such data commonly miss nuanced contextual information. For instance, the binary measure of child mental health does not provide a measure of functioning or severity.
Implications
Our study provides correlational evidence useful in evaluation of several theoretical perspectives of CMR risk. We found higher CMR risks at younger ages, especially among children who experienced a CMR in early childhood. This is consistent with the life course perspective (White & Wu, 2014) and supports the need for early intervention with young families to try to offset ongoing risk. While recent investments have been made in approaches like home visitation, most models have not shown strong effects in regard to preventing CMR (Jonson-Reid, Drake, Dunnigan, Kohl, & Auslander, 2020). Second, ecological transactional perspectives (Belsky, 1980; MacKenzie et al., 2011) suggest that other factors may interact with early childhood context to affect the relationship between child age and ongoing CMR risk. Our data suggest that interrupting ongoing CMR risk requires the ability to attend to current material needs as well as address child needs that may have arisen as a result of earlier experiences with poverty or CMR. The long established strong association of poverty with maltreatment reports (Pelton, 1994, 2015) has now been supplemented by an emerging body of research demonstrating that even small supplements to income can reduce maltreatment rates (Cancian et al., 2013; McLaughlin, 2017; Rostad et al., 2017). In regard to primary prevention, we need to identify ways of promoting protective early childhood context among the welfare population without CMR histories (Berrick et al., 2006; Putnam-Hornstein & Needell, 2011).
Concern continues regarding the overrepresentation of certain ethnic/racial groups in our child welfare system. Our work and others suggests that attempts to address disparities related to race in CPS contact must attend to the differential needs present among families. This includes attention to the resources in a community that need to be in place in order for a family to successfully parent (Maguire-Jack & Klein, 2015). This does not mean that we ignore potential biases in CPS or in other systems that inappropriately lead to under or overserving a population. Careful monitoring of flows in and through systems by race should continue as we improve the availability and quality of services to support families.
Finally, while primary prevention and early intervention are clearly preferable, the continued import of current child level risk, continued CMRs and welfare receipt, suggest that effective intervention at later stages is possible but must attend to a broader set of needs. Several years ago, child well-being outcomes were added to federal child welfare standards, but most states have struggled to meet those metrics. Although evidence-based parenting programs designed to address child behavior problems are believed to hold promise in preventing maltreatment by reducing the challenges to parenting related to the child’s behaviors (Barth, 2009), much less is known about how attending to child well-being (including intermediate effects of early maltreatment) over time may reduce ongoing CMR risk. It is also possible that addressing these more proximal concerns may have benefits in reducing risk for other forms of victimization outside the home (Finkelhor et al., 2007). Improved cross-sector data systems that allow for understanding engagement across systems to address child behavioral, educational and health needs are needed to understand what services families may or may not be accessing and the quality of care given within those systems to support these efforts (Jonson-Reid & Drake, 2016).
Supplementary Material
Acknowledgments
Human Participant Protection: The current study’s data were obtained from a larger longitudinal study which linked data from various Missouri administrative systems and Census data. The parent study is permitted to use these data with human subjects’ approval by all service system agencies and the Washington University Hilltop Institutional Review Board. All personal identifiers (e.g., names) were already removed prior to accessing the data for the present study.
Funding: The current study received no funding, but used data already available from a parent linked administrative data study. The parent study was funded by the National Institute of Mental Health, R01 MH 061733-04 A1 with a later extension funded by the Centers for Disease Control CE001190. Points of view and opinions expressed in the current study are the author’s and do not necessarily express the views or opinions of the parent study or the funding agencies.
Footnotes
Financial Disclosure/Conflict of Interest: None
References
- Acs G, & Loprest P (2001). Final synthesis report of findings from ASPE’s “leavers” grants. Washington, DC. [Google Scholar]
- Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield C, Perry BD, … Giles WH (2006). The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience, 256(3), 174–186. 10.1007/s00406-005-0624-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barth RP (2009). Preventing child abuse and neglect with parent training: Evidence and opportunities. The Future of Children, 19(2), 95–118. 10.1353/foc.0.0031 [DOI] [PubMed] [Google Scholar]
- Beimers DL, & Coulton CJ (2011). Do employment and type of exit influence child maltreatment among families leaving Temporary Assistance for Needy Families? Children and Youth Services Review, 33(7), 1112–1119. 10.1016/j.childyouth.2011.02.002 [DOI] [Google Scholar]
- Belsky J (1980). Child maltreatment: An ecological integration. American Psychologist, 35(4), 320–335. 10.1037/0003-066X.35.4.320 [DOI] [PubMed] [Google Scholar]
- Berger LM (2004). Income, family structure, and child maltreatment risk. Children and Youth Services Review, 26(8), 725–748. 10.1016/j.childyouth.2004.02.017 [DOI] [Google Scholar]
- Berrick JD, Frame L, Langs J, & Varchol L (2006). Working together for children and families: Where TANF and child welfare meet. Journal of Policy Practice, 5(2–3), 27–42. 10.1300/J508v05n02_03 [DOI] [Google Scholar]
- Boushey H, & Gundersen B (2001). When work just isn’t enough: Measuring hardships faced by families after moving from welfare to work. Briefing paper. Washington, DC. [Google Scholar]
- Buek KW, Lakey DL, & Mandell DJ (2019). Paternity establishment at birth and early maltreatment: Risk and protective effects by maternal race and ethnicity. Child Abuse & Neglect, 95(March), 104069. 10.1016/j.chiabu.2019.104069 [DOI] [PubMed] [Google Scholar]
- Burman E (2016). Deconstructing Developmental Psychology. Routledge. 10.4324/9781315727127 [DOI] [Google Scholar]
- Cancian M, Yang M, & Slack KS (2013). The effect of additional child support income on the risk of child maltreatment. Social Service Review, 87(3), 417–437. 10.1086/671929 [DOI] [Google Scholar]
- Constantino JN, Ben-David V, Navsaria N, Spiegel TE, Glowinski AL, Rogers CE, & Jonson-Reid M (2016). Two-generation psychiatric intervention in the prevention of early childhood maltreatment recidivism. American Journal of Psychiatry, 173(6), 566–573. 10.1176/appi.ajp.2015.15070944 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coulton CJ, Lickfelt S, Lalich N, & Cook T (2005). How are they managing? A retrospective of Cuyahoga County families leaving welfare (final report). Cleveland, OH: Center for Urban Poverty and Social Change, Mandel School of Applied Social Science, Case Western Reserve University. [Google Scholar]
- Coulton CJ, Theodos B, & Turner MA (2012). Residential mobility and neighborhood change: Real neighborhoods under the microscope. Cityscape: A Journal of Policy Development and Research, 14(3), 55–90. [Google Scholar]
- Courtney ME, Dworsky A, Piliavin I, & Zinn A (2005). Involvement of TANF applicant families with child welfare services. Social Service Review, 79(1), 119–157. 10.1086/426720 [DOI] [Google Scholar]
- Doidge JC, Higgins DJ, Delfabbro P, Edwards B, Vassallo S, Toumbourou JW, & Segal L (2017). Economic predictors of child maltreatment in an Australian population-based birth cohort. Children and Youth Services Review, 72, 14–25. 10.1016/j.childyouth.2016.10.012 [DOI] [Google Scholar]
- Drake B, Jolley JM, Lanier P, Fluke J, Barth RP, & Jonson-Reid M (2011). Racial bias in child protection? A comparison of competing explanations using national data. Pediatrics, 127(3), peds.2010–1710. 10.1542/peds.2010-1710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Drake B, & Jonson-Reid M (2014). Poverty and child maltreatment. In Korbin JE & Krugman RD (Eds.), Handbook of child maltreatment (pp. 131–148). Springer; Netherlands. [Google Scholar]
- Drake B, Jonson-Reid M, & Kim H (2017). Surveillance bias in child maltreatment: A tempest in a teapot. International Journal of Environmental Research and Public Health, 14(12), 971. 10.3390/ijerph14090971 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Drake B, Lee SM, & Jonson-Reid M (2009). Race and child maltreatment reporting: Are Blacks overrepresented? Children and Youth Services Review, 31(3), 309–316. 10.1016/j.childyouth.2008.08.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Drake B, & Rank MR (2009). The racial divide among American children in poverty: Reassessing the importance of neighborhood. Children and Youth Services Review, 31(12), 1264–1271. 10.1016/j.childyouth.2009.05.012 [DOI] [Google Scholar]
- Dworsky A, Courtney ME, & Zinn A (2007). Child, parent, and family predictors of child welfare services involvement among TANF applicant families. Children and Youth Services Review, 29(6), 802–820. 10.1016/j.childyouth.2006.12.007 [DOI] [Google Scholar]
- Finkelhor D, Ormrod RK, & Turner HA (2007). Re-victimization patterns in a national longitudinal sample of children and youth. Child Abuse & Neglect, 31(5), 479–502. 10.1016/j.chiabu.2006.03.012 [DOI] [PubMed] [Google Scholar]
- Font SA, Berger LM, & Slack KS (2012). Examining racial disproportionality in child protective services case decisions. Children and Youth Services Review, 34(11), 2188–2200. 10.1016/j.childyouth.2012.07.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garbarino J (1977). The human ecology of child maltreatment: A conceptual model for research. Journal of Marriage and Family, 39(4), 721–735. Retrieved from http://www.jstor.org/stable/350477 [Google Scholar]
- Geronimus AT (1996). Black/white differences in the relationship of maternal age to birthweight: a population-based test of the weathering hypothesis. Social Science & Medicine, 42(4), 589–597. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8643983 [DOI] [PubMed] [Google Scholar]
- Gilbert R, Widom CS, Browne K, Fergusson D, Webb E, & Janson S (2009). Burden and consequences of child maltreatment in high-income countries. The Lancet, 373(9657), 68–81. 10.1016/S0140-6736(08)61706-7 [DOI] [PubMed] [Google Scholar]
- Goodway JD, Ozmun JC, & Gallahue DL (2019). Understanding motor development: Infants, children, adolescents, adults. Jones & Bartlett Learning. [Google Scholar]
- Hill RB (2004). Institutional racism in child welfare. Race & Society, 7(1), 17–33. [Google Scholar]
- Hill RB (2006). Synthesis of research on disproportionality in child welfare: An update. Washington, DC: The Casey-CSSP Alliance for Racial Equity in the Child Welfare System. [Google Scholar]
- Hussey JM, Chang JJ, & Kotch JB (2006). Child maltreatment in the United States: Prevalence, risk factors, and adolescent health consequences. Pediatrics, 118(3), 933–942. 10.1542/peds.2005-2452 [DOI] [PubMed] [Google Scholar]
- Hussey JM, Marshall JM, English DJ, Knight ED, Lau AS, Dubowitz H, & Kotch JB (2005). Defining maltreatment according to substantiation: Distinction without a difference? Child Abuse and Neglect, 29(5 SPEC. ISS.), 479–492. 10.1016/j.chiabu.2003.12.005 [DOI] [PubMed] [Google Scholar]
- Irwin M (2009). The impact of race and neighborhood on child maltreatment: A multi-level discrete time hazard analysis. Unpublished doctoral dissertation, Case Western Reserve University, Cleveland, OH. [Google Scholar]
- Jaco C (2019, March 5). St. Louis is no longer a majority black city. What’s next? MetroSTL. Retrieved from https://metrostl.com/2019/03/05/st-louis-is-no-longer-a-majority-black-city-whats-next/ [Google Scholar]
- Jaffee SR, & Maikovich-Fong AK (2011). Effects of chronic maltreatment and maltreatment timing on children’s behavior and cognitive abilities. Journal of Child Psychology and Psychiatry, 52(2), 184–194. 10.1111/j.1469-7610.2010.02304.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaudes PK, & Mackey-Bilaver L (2008). Do chronic conditions increase young children’s risk of being maltreated? Child Abuse & Neglect, 32(7), 671–681. 10.1016/j.chiabu.2007.08.007 [DOI] [PubMed] [Google Scholar]
- Jonson-Reid M, & Drake B (2016). Child well-being: Where is it in our data systems? Journal of Public Child Welfare, 10(4), 457–465. 10.1080/15548732.2016.1155524 [DOI] [Google Scholar]
- Jonson-Reid M, Drake B, Dunnigan A, Kohl PL, & Auslander WF (2020). Preventing child maltreatment. In Rank MR (Ed.), Toward a Livable Life: A 21st Century Agenda for Social Work. New York, NY: Oxford University Press. [Google Scholar]
- Jonson-Reid M, Drake B, & Kohl PL (2009). Is the overrepresentation of the poor in child welfare caseloads due to bias or need? Children and Youth Services Review, 31(3), 422–427. 10.1016/j.childyouth.2008.09.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jonson-Reid M, Emery CR, Drake B, & Stahlschmidt MJ (2010). Understanding chronically reported families. Child Maltreatment, 15(4), 271–281. 10.1177/1077559510380738 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim H, & Drake B (2017). Duration in poverty-related programs and number of child maltreatment reports. Child Maltreatment, 22(1), 14–23. 10.1177/1077559516679512 [DOI] [PubMed] [Google Scholar]
- Kim H, & Drake B (2018). Child maltreatment risk as a function of poverty and race/ethnicity in the USA. International Journal of Epidemiology, 47(3), 780–787. 10.1093/ije/dyx280 [DOI] [PubMed] [Google Scholar]
- Kim H, Wildeman C, Jonson-Reid M, & Drake B (2017). Lifetime prevalence of investigating child maltreatment among US children. American Journal of Public Health, 107(2), 274–280. 10.2105/AJPH.2016.303545 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kohl PL, Jonson-Reid M, & Drake B (2009). Time to leave substantiation behind: Findings from a national probability study. Child Maltreatment, 14(1), 17–26. 10.1177/1077559508326030 [DOI] [PubMed] [Google Scholar]
- Leiter J, Myers KA, & Zingraff MT (1994). Substantiated and unsubstantiated cases of child maltreatment: Do their consequences differ? Social Work Research, 18(2), 67–82. 10.1093/swr/18.2.67 [DOI] [Google Scholar]
- Loprest P (2002). Who returns to welfare? Washington, DC: Urban Institute. [Google Scholar]
- Luby J, Belden A, Botteron K, Marrus N, Harms MP, Babb C, … Barch D (2013). The effects of poverty on childhood brain development: The mediating effect of caregiving and stressful life events. JAMA Pediatrics, 167(12), 1135. 10.1001/jamapediatrics.2013.3139 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luke DA (2004). Multilevel modeling. Thousand Oaks, CA: Sage Publications. [Google Scholar]
- Luke DA (2008). Multilevel growth curve analysis for quantitative outcomes. In Menard S (Ed.), Handbook of longitudinal research: Design, measurement, and analysis (pp. 545–564). Elsevier. [Google Scholar]
- MacKenzie MJ, Kotch JB, Lee L-C, Augsberger A, & Hutto N (2011). A cumulative ecological–transactional risk model of child maltreatment and behavioral outcomes: Reconceptualizing early maltreatment report as risk factor. Children and Youth Services Review, 33(11), 2392–2398. Retrieved from http://www.sciencedirect.com/science/article/pii/S019074091100332X [Google Scholar]
- Maguire-Jack K, & Klein S (2015). Parenting and proximity to social services: Lessons from Los Angeles County in the community context of child neglect. Child Abuse & Neglect, 45, 35–45. 10.1016/j.chiabu.2015.04.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maloney T, Jiang N, Putnam-Hornstein E, Dalton E, & Vaithianathan R (2017). Black–White differences in child maltreatment reports and foster care placements: A statistical decomposition using linked administrative data. Maternal and Child Health Journal, 21(3), 414–420. 10.1007/s10995-016-2242-3 [DOI] [PubMed] [Google Scholar]
- McDaniel M, & Slack KS (2005). Major life events and the risk of a child maltreatment investigation. Children and Youth Services Review, 27(2), 171–195. 10.1016/j.childyouth.2004.08.015 [DOI] [Google Scholar]
- McLaughlin M (2017). Less money, more problems: How changes in disposable income affect child maltreatment. Child Abuse & Neglect, 67, 315–321. 10.1016/j.chiabu.2017.03.006 [DOI] [PubMed] [Google Scholar]
- Miller C (2002). Leavers, stayers, and cyclers: An analysis of the welfare caseload. Washington, DC. [Google Scholar]
- Moffitt R (1992). Incentive effects of the U.S. welfare system: A review. Journal of Economic Literature, 30(1), 1–61. Retrieved from http://www.jstor.org/stable/2727878 [Google Scholar]
- Morton TD (1999). The increasing colorization of America’s child welfare system: The overrepresentation of African-American children. Policy & Practice of Public Human Services, 57(4), 23–30. [Google Scholar]
- Moses A, Mancuso DC, & Lieberman CJ (2000). Examining circumstances of individuals and families who leave TANF: Assessing the validity of administrative data. Belmont, CA: The SPHERE Institute. [Google Scholar]
- Needell B, Cuccaro-Alamin S, Brookhart A, & Seon L (1999). Transitions from AFDC to child welfare in california. Children and Youth Services Review, 21(9–10), 815–841. 10.1016/S0190-7409(99)00055-9 [DOI] [Google Scholar]
- Nicoll KL (2015). Why do eligible households not participate in public antipoverty programs?: A review. Journal of Poverty, 19(4), 445–465. 10.1080/10875549.2015.1015069 [DOI] [Google Scholar]
- Ovwigho PC, Leavitt KL, & Born CE (2003). Risk factors for child abuse and neglect among former TANF families: Do later leavers experience greater risk? Children and Youth Services Review, 25(1–2), 139–163. 10.1016/S0190-7409(02)00269-4 [DOI] [Google Scholar]
- Paxson C, & Waldfogel J (2003). Welfare reforms, family resources, and child maltreatment. Journal of Policy Analysis and Management, 22(1), 85–113. 10.1002/pam.10097 [DOI] [Google Scholar]
- Pelton LH (1978). Child abuse and neglect: The myth of classlessness. American Journal of Orthopsychiatry, 48(4), 608–617. 10.1111/j.1939-0025.1978.tb02565.x [DOI] [PubMed] [Google Scholar]
- Pelton LH (1994). The role of material factors in child abuse and neglect. In Melton GB & Barry FD (Eds.), Protecting children from abuse and neglect: Foundations for a new national strategy. Guilford Press. [Google Scholar]
- Pelton LH (2015). The continuing role of material factors in child maltreatment and placement. Child Abuse & Neglect, 41, 30–39. 10.1016/j.chiabu.2014.08.001 [DOI] [PubMed] [Google Scholar]
- Putnam-Hornstein E (2011). Report of maltreatment as a risk factor for injury death: A prospective birth cohort study. Child Maltreatment, 16(3), 163–174. 10.1177/1077559511411179 [DOI] [PubMed] [Google Scholar]
- Putnam-Hornstein E, & Needell B (2011). Predictors of child protective service contact between birth and age five: An examination of California’s 2002 birth cohort. Children and Youth Services Review, 33(11), 2400–2407. 10.1016/j.childyouth.2011.07.010 [DOI] [Google Scholar]
- Putnam-Hornstein E, Needell B, King B, & Johnson-Motoyama M (2013). Racial and ethnic disparities: A population-based examination of risk factors for involvement with child protective services. Child Abuse & Neglect, 37(1), 33–46. 10.1016/j.chiabu.2012.08.005 [DOI] [PubMed] [Google Scholar]
- Rostad WL, Rogers TM, & Chaffin MJ (2017). The influence of concrete support on child welfare program engagement, progress, and recurrence. Children and Youth Services Review, 72, 26–33. 10.1016/j.childyouth.2016.10.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sabol W, Coulton C, & Polousky E (2004). Measuring child maltreatment risk in communities: A life table approach. Child Abuse & Neglect, 28(9), 967–983. 10.1016/j.chiabu.2004.03.014 [DOI] [PubMed] [Google Scholar]
- Sedlak AJ, Mettenburg J, Basena M, Petta I, McPherson K, Green A, & Li S (2010). Fourth national incidence study of child abuse and neglect (NIS-4): Report to congress. Washington, DC: US Department of Health and Human Services. [Google Scholar]
- Slack KS, Berger LM, & Noyes JL (2017). Introduction to the special issue on the economic causes and consequences of child maltreatment. Children and Youth Services Review, 72, 1–4. 10.1016/j.childyouth.2016.11.013 [DOI] [Google Scholar]
- Slack KS, Holl JL, Lee BJ, McDaniel M, Altenbernd L, & Stevens AB (2003). Child protective intervention in the context of welfare reform: The effects of work and welfare on maltreatment reports. Journal of Policy Analysis and Management, 22(4), 517–536. 10.1002/pam.10152 [DOI] [Google Scholar]
- Slack KS, Lee BJ, & Berger LM (2007). Do welfare sanctions increase child protection system involvement? A cautious answer. Social Service Review, 81(2), 207–228. 10.1086/516831 [DOI] [Google Scholar]
- Snijders TAB, & Bosker RJ (2012). Multilevel analysis: An introduction to basic and advanced multilevel modeling (2nd ed.). Sage Publications. [Google Scholar]
- Spivey MI, Schnitzer PG, Kruse RL, Slusher P, & Jaffe DM (2009). Association of injury visits in children and child maltreatment reports. The Journal of Emergency Medicine, 36(2), 207–214. 10.1016/j.jemermed.2007.07.025 [DOI] [PubMed] [Google Scholar]
- Stith SM, Liu T, Davies LC, Boykin EL, Alder MC, Harris JM, … Dees JEMEG (2009). Risk factors in child maltreatment: A meta-analytic review of the literature. Aggression and Violent Behavior, 14(1), 13–29. 10.1016/j.avb.2006.03.006 [DOI] [Google Scholar]
- U.S. Department of Health and Human Services. (2019). Child maltreatment 2017. Retrieved February 5, 2019, from https://www.acf.hhs.gov/cb/research-data-technology/statistics-research/child-maltreatment
- Verma N, & Coulton C (2001). Monitoring outcomes for Cuyahoga County’s welfare leavers: How are they faring? New York, NY. [Google Scholar]
- Weinberg B. a. (2001). An incentive model of the effect of parental income on children. Journal of Political Economy, 109(2), 266–280. 10.1086/319556 [DOI] [Google Scholar]
- White KR, & Wu Q (2014). Application of the life course perspective in child welfare research. Children and Youth Services Review, 46, 146–154. 10.1016/j.childyouth.2014.08.018 [DOI] [Google Scholar]
- Wildeman C, Emanuel N, Leventhal JM, Putnam-Hornstein E, Waldfogel J, & Lee H (2014). The prevalence of confirmed maltreatment among US children, 2004 to 2011. JAMA Pediatrics, 168(8), 706. 10.1001/jamapediatrics.2014.410 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zedlewski SR (2002). Left behind or staying away? Eligible parents who remain off TANF. Washington, DC. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.