

Abstract
Objective
To determine the effect of a physician assistant (PA) working in a secondary care hospital emergency department (ED) on the overall performance of the ED.
Design
A retrospective review of ED data from April 1, 2017, to September 30, 2017.
Setting
Belleville General Hospital, a secondary care hospital, ED in Ontario.
Participants
A physician assistant, 13 emergency physicians, and 7 family physicians.
Main outcome measures
Overall ED performance was evaluated using metrics from the Ontario Ministry of Health and Long-Term Care: rate of patients who left without being seen, provider initial assessment time at the 90th percentile, and the average provider initial assessment time for all patients over a 6-month period.
Results
In the PA group, there was a lower average daily left without being seen rate (3.4% vs 5.2%; P < .001), a lower provider initial assessment time at the 90th percentile (3.9 hours vs 4.5 hours; P < .001), a lower average provider initial assessment time (114.83 minutes vs 139.46 minutes; P < .001), and a lower average length of stay (313.85 minutes vs 348.91 minutes; P < .001).
Conclusion
This study suggests that a PA has a statistically significant positive effect on the overall performance of an ED. Future studies should examine the effect of a PA on quality of care and hospital funding.
Résumé
Objectif
Déterminer les effets de la présence d’un adjoint au médecin (AM) travaillant au service d’urgence (SU) d’un hôpital de soins secondaires sur le rendement global du SU.
Type d’étude
Une revue rétrospective des données du SU entre le 1er avril et le 30 septembre 2017.
Contexte
Le SU de l’Hôpital général de Belleville, un hôpital de soins secondaires en Ontario.
Participants
Un adjoint au médecin, 13 urgentologues et 7 médecins de famille.
Principaux paramètres à l’étude
Le rendement global de l’urgence a été évalué en fonction des indicateurs du ministère de la Santé et des Soins de longue durée de l’Ontario : taux de patients partis sans être vus, temps écoulé entre l’évaluation initiale par un professionnel au 90e percentile, et temps moyen écoulé avant l’évaluation initiale par un professionnel pour tous les patients sur une période de 6 mois.
Résultats
Dans le groupe doté d’un AM, il y avait un taux quotidien moyen plus faible de patients partis sans être vus (3,4 c. 5,2 %; p <,001), moins de temps écoulé jusqu’à l’évaluation initiale par un professionnel au 90e percentile (3,9 c. 4,5 heures; p <,001), un temps moyen moins long avant l’évaluation initiale par un professionnel (114,83 c. 139,46 minutes; p <,001), et une durée moyenne de séjour moins grande (313,85 c. 348,91 minutes; p <,001).
Conclusion
Cette étude fait valoir que la présence d’un AM a des effets positifs statistiquement significatifs sur le rendement global d’un SU. Des études futures devraient se pencher sur les effets de la présence d’un AM sur la qualité des soins et le financement des hôpitaux.
An aging population, coupled with changes in patient demand and choice of where they seek care, is placing increasing demand on emergency departments (EDs) worldwide.1 As a result, EDs have to become more efficient. Throughput—the rate at which patients are registered, assessed, treated, and ultimately admitted or discharged from the ED—continues to be a challenge in many Canadian EDs.2 To ensure seriously ill and injured patients are seen promptly, patients are triaged according to the Canadian Triage and Acuity Scale (CTAS), which was implemented in 1999.3 A more efficient process for accurately triaging, assessing, investigating, and treating patients should lead to reduced overall wait times in the ED and thus translate into higher throughput. Hospitals, therefore, are looking at ways to improve productivity through the use of allied health care professionals such as nurse practitioners and physician assistants (PAs).
Recently, the Ontario Ministry of Health and Long-Term Care has incorporated parameters into its process to evaluate the performance of individual EDs, such as the left without being seen (LWBS) metric, which is defined as the rate of patients who have registered at the ED and have been triaged, but who leave before being seen by a PA, physician, or nurse practitioner. The Ontario Ministry of Health and Long-Term Care has a target of no more than 3% LWBS for all those presenting to an ED.4
The ministry is also monitoring the provider initial assessment (PIA) time, which is the elapsed time from the point a patient first registers at the ED and includes the time to triage the patient, the time spent in the waiting room, and the time spent waiting when brought into the emergency area until the designated provider (in Ontario that would be a PA, physician, or nurse practitioner) makes contact. The ministry recommends that the 90th percentile should not be greater than 3 hours.4
In Ontario, PAs are academically prepared either through the military, or through a program—such as the one at McMaster University in Hamilton, Ont, or at the University of Toronto in Ontario—where they complete a 2-year curriculum to acquire necessary skills and theoretical knowledge. Physician assistants in Ontario are not independent medical practitioners and currently lack regulatory status,1,5 so they must operate under the supervision of a licensed physician for which they serve as a “physician extender” through medical directives. In some EDs, PAs’ skills are used to assess and develop treatment plans for less acutely ill and injured patients, and perform time-consuming activities such as suturing, incising, draining, and caring for wounds. This permits the attending physicians to see more patients and increase their throughput, and enables them to spend the necessary time with the more acutely ill and injured patients. The PA acts in many ways like a skilled resident.
The LWBS percentage has been used both nationally and internationally as a measure of barriers to health care access.5 Emergency departments in Ontario, therefore, have been implementing innovative solutions to achieve these metrics within their funding envelopes. Furthermore, patients who LWBS might pose a substantial risk to their own health and might be a legal risk to the hospital.5,6 It is now accepted that there is a direct correlation between door-to-room times, length of stay, wait times, overall morbidity and mortality,6 and rates of LWBS.2 Internationally, LWBS rates vary from 0% to 20%.7-9 One strategy has been to employ alternate health care providers, such as nurse practitioners or PAs, to see patients in a more expedient manner and assist with patient flow within the ED. There are few papers in the literature that have specifically examined PA productivity; most are from hospitals outside of Canada where there might or might not be formal PA training as currently exists in Canada, or there might be different conditions of employment. Brook et al found that their PAs consistently saw between 1.16 and 2.4 patients per hour depending on the acuity of the patients.10 It would appear that most patients seen by PAs in this study had an emergency severity index score of 4 or 5 and were seen solely by the PA without direct oversight by an attending physician.10 These scores would be similar to CTAS levels 4 and 5 in Canada.
In Ontario, while a PA can initiate investigations and treatment, all patients must ultimately be seen and reviewed by an attending physician before discharge. In the United States, some researchers have looked at productivity of both physicians and PAs based upon relative value units, which incorporate payment, risk, and insurance into an equation based upon the revenue generated.10-12 This calculation is less sensitive in Canada given its universal health care system.
While PAs have been used elsewhere for some time,11 they have only recently been introduced as part of the health care team in Ontario.13 Optimal use of these allied health care professionals is still being determined in the provincial health care setting.14
The objective of this study was to determine the effect of a PA working in a mid-sized urban ED during peak volume times on the overall efficiency of the ED, using metrics currently employed by the Ontario Ministry of Health and Long-Term Care.
METHODS
Setting
Belleville General Hospital is a mid-sized urban community hospital in Ontario with a catchment population of 125 000. The hospital has coverage 24 hours per day, 7 days per week for internal medicine, general surgery, orthopedic surgery, pediatrics, radiology, family medicine, and psychiatry. There is also partial urology and ears, nose, and throat coverage. Those requiring specialty care other than in these areas are transferred to a nearby tertiary care centre.
There are approximately 38 000 patient visits to the ED annually. The patient population is mixed, with 20% pediatric (aged 16 and younger), 40% aged 17 to 65 years, and 40% older than 65 years. Of these, 1.3% are assessed as CTAS level 1, 22.2% are level 2, 47.5% are level 3, 27.3% are level 4, and 1.7% are level 5. On average, 22% of patients presenting to the ED are referred to on-call consultants, and of those, 50% are ultimately admitted to an inpatient ward.
The ED is staffed by 13 full-time emergency physicians certified in emergency medicine by either the College of Family Physicians of Canada or the Royal College of Physicians and Surgeons of Canada, along with 7 family physicians who work in the “green zone” (patients at CTAS levels 3, 4, and 5), which runs 7 days per week from 2 pm to 11 pm. During the study period, the ED was funded under the provincial alternate funding payment model for 45 hours of physician coverage daily.
Study design
To address wait times and LWBS rates that exceeded acceptable provincial targets, a PA was added to ED staff during the study period. The PA was trained by the 2-year McMaster University program and worked primarily in the green zone. The PA was tasked with seeing and treating patients at CTAS levels 4 and 5, who encompass 29.0% of all ED visits. The PA’s shift ran from 11 am to 11 pm, which corresponded to the highest volume time of the day. Once triaged, appropriate patients were assigned to the green zone, where their charts would be placed in a rack and they would be assessed in sequence by the PA or family physician. The process was the same for both PA and control days. All patients seen by the PA were also seen and reviewed by an attending physician (or family physician, depending on time of day) before discharge or referral. It was hypothesized that in so doing, the physicians would have more time to see higher-acuity patients (CTAS levels 1, 2, and 3 patients) in addition to reviewing those seen by the PA.
The study period ran from April 1, 2017, until September 30, 2017. The study group consisted of all patients seen from 12:01 am through to 11:59 pm on any day that the PA worked. The control group consisted of those patients seen on any day the PA did not work. The number of days worked by the PA was 87 versus 96 in the control group. The PA’s work schedule was determined 30 to 60 days before work, such that the PA worked a shift cycle of 4 consecutive days with 5 days off. Adjustments made for holidays and days off were such that the resultant schedule did not represent any predetermined pattern that could be anticipated. There was an equal distribution of weekdays, weekends, and holidays during the study period between the PA and control groups. Nurses, physicians, and other support staff within the ED were unaware of the nature of the study, the personal schedule of the PA, or the timing of the study so as to control for bias such as the Hawthorne effect.
Data collection and analysis
The data in this study were derived from the National Ambulatory Care Reporting System15 metadata (managed by the Canadian Institute for Health Information), which the hospital submits to the Ontario Ministry of Health and Long-Term Care quarterly as a requirement for the alternate funding program.
To determine the PA’s effect on the efficiency of the ED, an evaluation of the ED was performed using metrics from the Ontario Ministry of Health and Long-Term Care, which included LWBS rate, PIA time at the 90th percentile, and the average PIA time for all patients during a 6-month period. The PIA times have been used as a measure of both quality of care and ED efficiency. In addition, we examined the average length of stay for all triage levels of patients, which is the time from the moment a patient sits at the triage nurse’s station and a chart is initiated, to the moment the attending emergency physician indicates that either the patient be discharged or that a consultation with another physician or specialist is required.
All analyses were conducted with SAS, version 9.4. The independent samples 2-tailed t test was used to test for differences in means, and results were considered statistically significant at P < .01.
RESULTS
The PA saw 9701 patients in total during the 87 days (mean [SD] 111.5 [11.1] patients per day). There were 10 776 patients in total for the 96 days when the PA was not working (mean [SD] 112.3 [12.4]). The acuity profile of the 2 groups by CTAS level was not significantly different when analyzed by t test (Table 1).
Table 1.
Description of PA and control groups: None of the differences between groups were statistically significant (number of days worked not compared).
| COMPARATOR | PA GROUP | CONTROL GROUP |
|---|---|---|
| No. of days worked | 87 | 96 |
| Mean (SD) no. of patients seen per day | 111.5 (11.1) | 112.3 (12.4) |
| Patients by CTAS level, % | ||
| • 1 | 1.0 | 1.3 |
| • 2 | 22.1 | 23.2 |
| • 3 | 48.7 | 47.7 |
| • 4 | 26.3 | 26.1 |
| • 5 | 1.9 | 1.7 |
| Days of the week present, n (%) | ||
| • Monday | 15 (17.2) | 11 (11.5) |
| • Tuesday to Friday | 46 (52.9) | 58 (60.4) |
| • Saturday and Sunday | 26 (29.9) | 27 (28.1) |
CTAS—Canadian Triage and Acuity Scale, PA—physician assistant.
Left without being seen metric
Figure 1 outlines the average LWBS rate for the 2 groups during the entire 6-month study period. The average daily percent LWBS in the PA group was 3.4%, versus 5.2% in the control group (P < .001). Furthermore, the number of days in which the ED met or did not exceed the provincial target of 3% LWBS was 36 days out of 87 days in the PA group (41.4%) compared to 22 days out of 96 days in the control group (22.9%).
Figure 1.
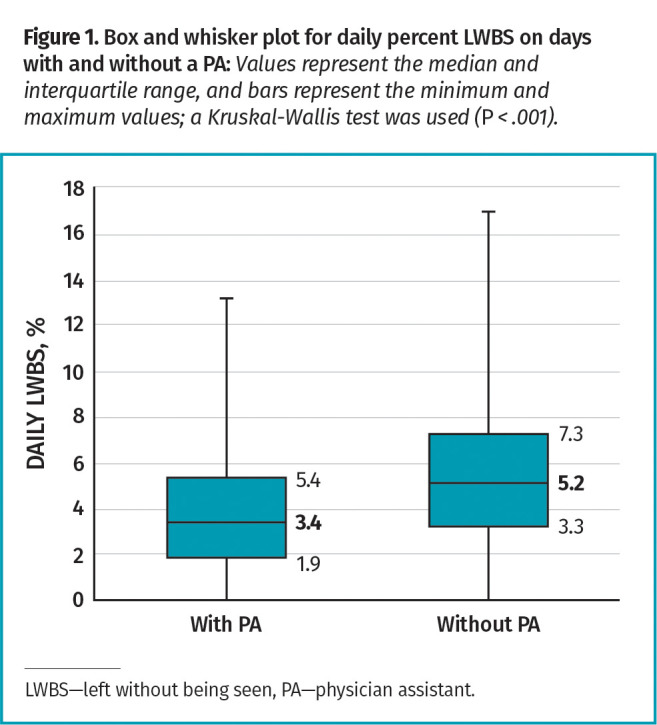
Box and whisker plot for daily percent LWBS on days with and without a PA: Values represent the median and interquartile range, and bars represent the minimum and maximum values; a Kruskal-Wallis test was used (P < .001).
Provider initial assessment time
Figure 2 addresses the PIA time at the 90th percentile (ie, 10% of all patients waited this long or more). During the study period, the 90th percentile PIA time for the PA group was 3.9 hours, whereas for the control group (no PA working) it was 4.5 hours (P < .001). In our ED, we also used an average PIA time in order to provide a clearer picture of overall PIA time performance. The average PIA time for the 2 groups is shown in Figure 3. For those days in which a PA worked from 11 am to 11 pm, the average PIA time was 114.83 minutes over 24 hours, whereas for the control group it was 139.46 minutes (P < .001). This is consistent with a similar, but less dramatic, decrease in 90th percentile PIA time (Figure 3).
Figure 2.
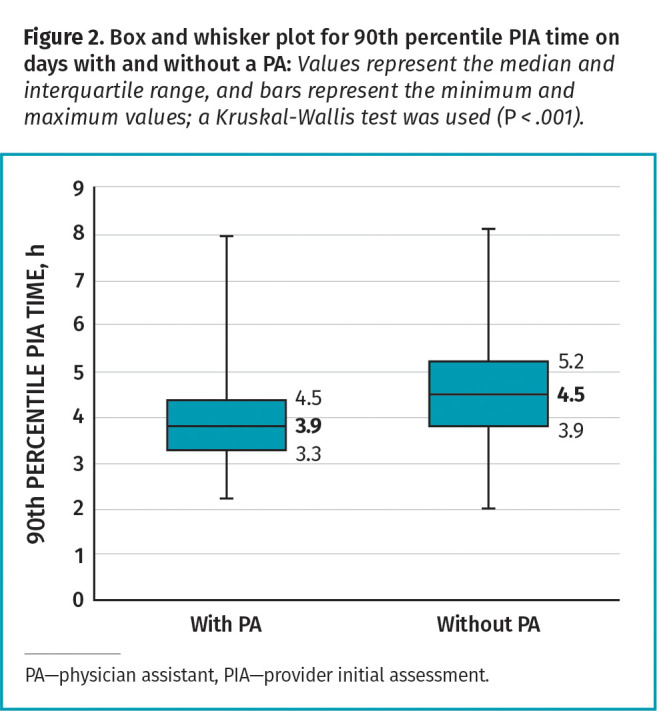
Box and whisker plot for 90th percentile PIA time on days with and without a PA: Values represent the median and interquartile range, and bars represent the minimum and maximum values; a Kruskal-Wallis test was used (P < .001).
Figure 3.
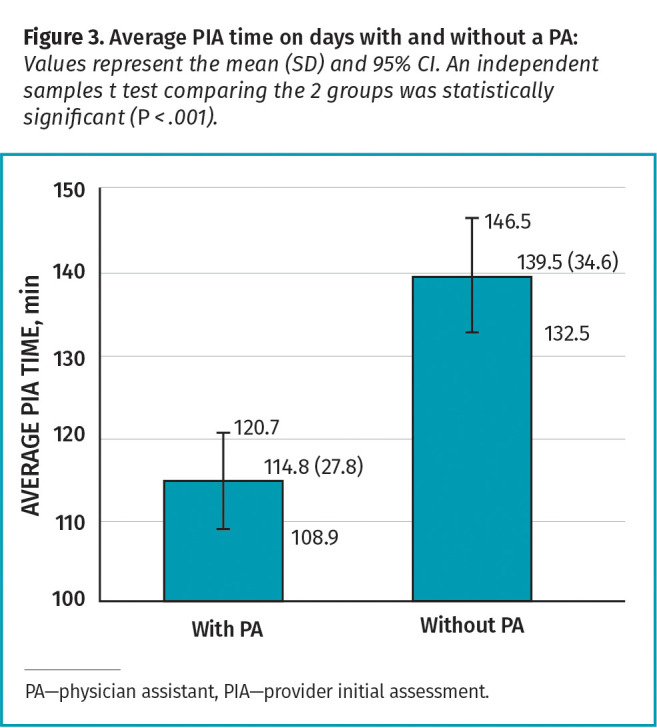
Average PIA time on days with and without a PA: Values represent the mean (SD) and 95% CI. An independent samples t test comparing the 2 groups was statistically significant (P < .001).
Average length of stay
The average length of stay for the PA and control groups can be seen in Figure 4. The average length of stay for the PA group was 313.85 minutes, whereas in the control group it was 348.91, with an average difference per patient of 35.06 minutes in favour of the PA group (P < .001).
Figure 4.
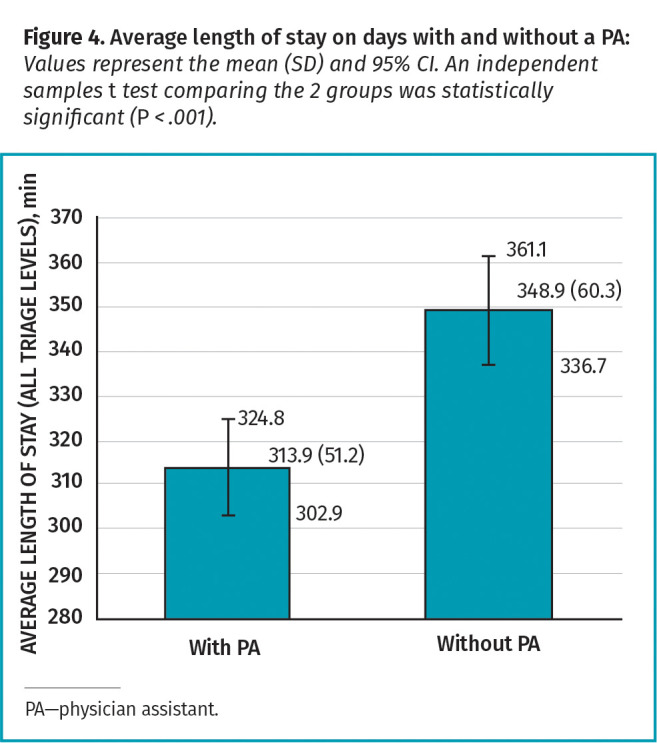
Average length of stay on days with and without a PA: Values represent the mean (SD) and 95% CI. An independent samples t test comparing the 2 groups was statistically significant (P < .001).
DISCUSSION
Our objective was to identify and quantify any difference in the efficiency of the overall function of an ED over a full 24-hour period during which a PA worked 12 hours. In all of our evaluations, the presence of a PA was the independent variable. During our study period, there was similar distribution between the days when the PA worked and the days when there was no PA. This makes this study unique, as it minimizes the confounding variables with respect to time and operation of the ED. Any changes or innovations within the ED, hospital, or community, however minor, that were made during the study period, would presumably have affected both groups equally.
We specifically looked at the entire 24-hour period for each group as we believe the effect of a PA extends not only to the patients and the period of time that the PA worked, but also to the entire ED, as it permits the attending physicians to potentially see and assess others more expediently before, during, and after the PA’s shift. Metrics pertaining to the specific time frame that a PA is working in the ED do not provide a complete picture as to how the entire ED is affected (positively or negatively) by their presence during an entire 24-hour period.
The performance measures discussed in this article reflect those used internally in our ED (average length of stay and average PIA time) and those that have been specifically targeted by the Ontario Ministry of Health and Long-Term Care as priorities in their “Pay for Results” evaluations,16 such as LWBS and PIA time at the 90th percentile.
Left without being seen
Our first question pertained to the rate of LWBS, as this has a considerable effect on the efficiency and quality of care in all EDs. The number of LWBS has been used as a surrogate marker for the efficiency of an ED. This metric reflects the number (or percentage) of patients who register at the ED, but then leave without medical assessment. Many LWBS are triaged as being moderately or substantially ill or injured, with a CTAS level of 3 and in some cases with a level of 2. This group of patients is considered by some to be at increased risk of serious adverse events if left untreated. Most EDs have an accurate picture of this rate, which ranges from less than 1% to greater than 10% of all patients presenting to the ED.6 Minimizing the size of this group is presumed to contribute to a lower overall morbidity and mortality.
During the course of the study, the LWBS rate was consistently lower for the PA days compared to the control days. It is worth noting that this was in spite of increased year over year monthly volumes of up to 10% during the study period. The average LWBS percentage in the control group did not change appreciably, suggesting that newer processes implemented in the ED were effective in addressing a larger volume of patients without a corresponding increase in LWBS.17 Moreover, there was a decrease in daily LWBS rate to 3.4% for the PA group versus the daily LWBS rate of 5.2% for the control group. Furthermore, the number of days in which the ED met or did not exceed the Ontario Ministry of Health and Long-Term Care’s provincial metric of 3% (ie, ≤ 3%) was higher in the PA group (41.4%) compared to the control group (22.9%).
Provider initial assessment
The second metric we used to evaluate ED performance was PIA time at the 90th percentile. A time of no more than 3 hours has been set as a provincial target for the 90th percentile. Neither group met the target during the study period. Interestingly, the PA group had a consistently lower PIA time compared with the control group and this difference was statistically significant (P < .001). This suggests that patients were seen more efficiently and spent less time waiting on PA days than non-PA days.
The average PIA time was 114.83 minutes in the PA group versus 139.46 minutes in the control group (P < .001). While decreasing the PIA time has a direct effect on the LWBS, it might or might not have had any effect on length of stay, as that might be more reflective of the overall efficiency of the ED (which includes metrics such as laboratory and radiology turnaround times).
Average length of stay
The average length of stay is a combination of PIA time and time from assessment to either discharge or referral to another specialist. As shown in Figure 4, the average length of stay is consistently lower on days when a PA is working than on control days. The monthly difference in average length of stay between the 2 groups ranged from an average of 21.4 minutes per patient to an average of 52.3 minutes per patient. For the entire study period, the average length of stay for all triage levels in the PA group was 313.85 minutes, compared to 348.91 minutes in the control group. This was an average difference of 35.06 minutes (P < .001). It would appear that the shortened PIA time that we experienced with the PA group did indeed contribute to a shortened length of stay for the patient.
To determine the effect of our findings on the overall function of the ED, we multiplied the average difference in length of stay per patient in the PA group (35.06 minutes) by the average daily number of patients seen in the PA group (111.5), resulting in 3909 minutes (65.15 hours) of “extra stretcher availability” during a 24-hour period. This is the equivalent to increasing the capacity of the ED by 2.7 stretchers. While some patients who are in ambulatory care can be examined or treated in chairs (ie, those at CTAS level 5), most patients require a stretcher at some point during their visit for examination or treatment. Increasing the stretcher capacity of an ED by either increasing the floor space and equipment or by more effectively using existing resources accomplishes the same result: more capacity to see patients within a given period of time. This might be useful in EDs where the limiting factor is physical resources rather that physician availability.
Limitations
This study did not specifically address the quality of care provided. There is nothing to suggest that the actual patient care differed between the PA group and the control group, as an attending physician was involved in the care and treatment of all patients. We also did not include a cost-benefit analysis from a funding perspective, as this study focused on the operational efficiency metrics used in our ED and those of the Ontario Ministry of Health and Long-Term Care. Future studies should look at funding implications and benefits of increased volumes and throughput with a PA. Finally, it would be advantageous to examine quality of care and patient satisfaction in Ontario following the implementation of a PA in the ED.
Conclusion
The inclusion of a PA in a mid-sized community secondary care hospital ED provided a statistically significant improvement in PIA times at the 90th percentile, average PIA times, LWBS rate reduction, and average length of stay compared with a concurrent control group with no PA.
Editor’s key points
▸ Ontario hospitals are seeking ways to improve emergency department (ED) efficiency through the use of allied health care professionals, such as nurse practitioners or physician assistants (PAs). Although PAs are not independent medical practitioners and require oversight by licensed physicians, they can perform time-consuming tasks and develop plans for patients who are less severely ill or injured, allowing physicians to spend more time with acutely injured patients.
▸ The Ontario Ministry of Health and Long-Term Care can evaluate the performance and efficiency of EDs using the left without being seen metric, which is the daily rate of patients who register at the ED but leave before being seen; the provider initial assessment time, which is the time from patient registration to being seen by a physician, PA, or nurse practitioner; and the average length of stay, which is the time from triage to either discharge or referral.
▸ This study found an improvement in ED efficiency following the implementation of a PA. Moreover, having a PA allowed the ED to increase its stretcher availability by 2.7 times, thereby giving the ED the capacity to see more patients within a given period of time.
Points de repère du rédacteur
▸ Les hôpitaux de l’Ontario cherchent des façons d’améliorer l’efficacité des services d’urgence (SU) en recourant à d’autres professionnels de la santé, comme des infirmières praticiennes ou des adjoints au médecin (AM). Même si les adjoints au médecin ne sont pas des praticiens médicaux indépendants et qu’ils doivent être supervisés par des médecins autorisés, ils peuvent exécuter des tâches qui prennent du temps et élaborer des plans pour les patients moins gravement malades ou blessés, ce qui permet aux médecins de passer plus de temps auprès des patients gravement blessés.
▸ Le ministère de la Santé et des Soins de longue durée de l’Ontario peut évaluer le rendement et l’efficacité des SU d’après l’indicateur du nombre de patients partis sans être vus, mesuré selon le taux quotidien de patients qui se sont inscrits au SU, mais sont partis avant d’avoir été vus par un médecin; selon le temps écoulé jusqu’à l’évaluation initiale par un professionnel, notamment le temps entre l’inscription du patient et le moment d’être vu par un médecin, un AM ou une infirmière praticienne; et selon la durée moyenne du séjour, soit le temps entre le triage et le congé ou l’aiguillage.
▸ Cette étude a fait valoir une amélioration dans l’efficacité du SU à la suite de la mise en place d’un AM. De plus, le fait d’être doté d’un AM a permis au SU d’augmenter de 2,7 fois la disponibilité de civières, ce qui a donc permis au SU de voir plus de patients dans une période de temps donnée.
Footnotes
Contributors
All authors contributed to the concept and design of this study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
References
- 1.Braun CT, Gnägi CR, Klukowska-Rötzler J, Ahmad SS, Ricklin ME, Exadaktylos AK.. Trends and weekly cycles in a large Swiss emergency centre: a 10 year period at the University Hospital of Bern. Int J Environ Res Public Health 2017;14(10):1239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pielsticker S, Whelan L, Arthur AO, Thomas S.. Identifying patient door-to-room goals to minimize left-without-being-seen rates. West J Emerg Med 2015;16(5):611-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Murray M, Bullard M, Grafstein E; CTAS National Working Group; CEDIS National Working Group . Revisions to the Canadian Emergency Department Triage and Acuity Scale implementation guidelines. CJEM 2004;6(6):421-7. [PubMed] [Google Scholar]
- 4.Ministry of Health and Long-Term Care . Hospital emergency departments. Toronto, ON: Office of the Auditor General of Ontario; 2010. Available from: https://www.auditor.on.ca/en/content/annualreports/arreports/en10/305en10.pdf. Accessed 2021 Feb 1. [Google Scholar]
- 5.Hsia RY, Asch SM, Weiss RE, Zingmond D, Liang LJ, Han W, et al. . Hospital determinants of emergency department left without being seen rates. Ann Emerg Med 2011;58(1):24-32.e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Guttmann A, Schull MJ, Vermeulen MJ, Stukel TA.. Association between waiting times and short term mortality and hospital admission after departure from emergency department: population based cohort study from Ontario, Canada. BMJ 2011;342:d2983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Carron PN, Yersin B, Trueb L, Gonin P, Hugli O.. Missed opportunities: evolution of patients leaving without being seen or against medical advice during a six-year period in a Swiss tertiary hospital emergency department. Biomed Res Int 2014;2014:690368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Baibergenova A, Leeb K, Jokovic A, Gushue S.. Missed opportunity: patients who leave emergency departments without being seen. Healthc Policy 2006;1(4):35-42. [PMC free article] [PubMed] [Google Scholar]
- 9.Parekh KP, Russ S, Amsalem DA, Rambaran N, Wright SW.. Who leaves the emergency department without being seen? A public hospital experience in Georgetown, Guyana. BMC Emerg Med 2013;13:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Brook C, Chomut A, Jeanmonod RK.. Physician assistants contribution to emergency department productivity. West J Emerg Med 2012;13(2):181-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Doan Q, Sabhaney V, Kissoon N, Sheps S, Singer J.. A systematic review: the role and impact of the physician assistant in the emergency department. Emerg Med Australas 2011;23(1):7-15. [DOI] [PubMed] [Google Scholar]
- 12.Hooker RS, Klocko DJ, Larkin GL.. Physician assistants in emergency medicine: the impact of their role. Acad Emerg Med 2011;18(1):72-7. Epub 2010 Dec 16. [DOI] [PubMed] [Google Scholar]
- 13.Ashton CW, Aiken A, Duffie D.. Physician assistants—a solution to wait times in Canada? Healthc Manage Forum 2007;20(2):38-42. [DOI] [PubMed] [Google Scholar]
- 14.Dies NF, Taylor MT.. Ontario physician assistants. Decision time. Can Fam Physician 2019;65:243-5 (Eng), 249-51 (Fr). [PMC free article] [PubMed] [Google Scholar]
- 15.Canadian Institute for Health Information . National Ambulatory Care Reporting System metadata (NACRS). Toronto, ON: Canadian Institute for Health Information; 2021. Available from: https://www.cihi.ca/en/national-ambulatory-care-reporting-system-metadata-nacrs. Accessed 2021 Jan 18. [Google Scholar]
- 16.Newsroom Ontario . Pay for results program. Toronto, ON: Government of Ontario; 2010. Available from: https://news.ontario.ca/en/backgrounder/13340/pay-for-results-program. Accessed 2021 Feb 1. [Google Scholar]
- 17.De la Roche MRP, Froats M, Bell A, McDonald L, Bolton C, Devins R, et al. . Estimation of unregistered patients who left without being seen. At an urban mid-sized Canadian community emergency department. Can Fam Physician 2021;67:114-20. [DOI] [PMC free article] [PubMed] [Google Scholar]