

ABSTRACT
Background
Nudging and salient pricing are promising strategies to promote healthy food purchases, but it is possible their effects differ across food groups.
Objective
To investigate in which food groups nudging and/or pricing strategies most effectively changed product purchases and resulted in within–food groups substitutions or spillover effects.
Methods
In total, 318 participants successfully completed a web-based virtual supermarket experiment in the Netherlands. We conducted a secondary analysis of a mixed randomized experiment consisting of 5 conditions (within subject) and 3 arms (between subject) to investigate the single and combined effects of nudging (e.g., making healthy products salient), taxes (25% price increase), and/or subsidies (25% price decrease) across food groups (fruit and vegetables, grains, dairy, protein products, fats, beverages, snacks, and other foods). Generalized linear mixed models were used to estimate the incidence rate ratios and 95% CIs for changes in the number of products purchased.
Results
Compared with the control condition, the combination of subsidies on healthy products and taxes on unhealthy products in the nudging and price salience condition was overall the most effective, as the number of healthy purchases from fruit and vegetables increased by 9% [incidence rate ratio (IRR) = 1.09; 95% CI: 1.02, 1.18], grains by 16% (IRR = 1.16; 95% CI: 1.05, 1.28), and dairy by 58% (IRR = 1.58; 95% CI: 1.31, 1.89), whereas the protein and beverage purchases did not significantly change. Regarding unhealthy purchases, grains decreased by 39% (IRR = 0.72; 95% CI: 0.63, 0.82) and dairy by 30% (IRR = 0.77; 95% CI: 0.68, 0.87), whereas beverage and snack purchases did not significantly change. The groups of grains and dairy showed within–food group substitution patterns toward healthier products. Beneficial spillover effects to minimally targeted food groups were seen for unhealthy proteins (IRR = 0.81; 95% CI: 0.73, 0.91).
Conclusions
Nudging and salient pricing strategies have a differential effect on purchases of a variety of food groups. The largest effects were found for dairy and grains, which may therefore be the most promising food groups to target in order to achieve healthier purchases. The randomized trial on which the current secondary analyses were based is registered in the Dutch trial registry (NTR7293; www.trialregister.nl).
Keywords: grocery store intervention, choice architecture, price change, food policy, public health
Introduction
Unhealthy dietary patterns contribute to the development of obesity and noncommunicable diseases (1). It is increasingly recognized in theory (2, 3) and through evidence (4–7) that unhealthy dietary patterns are partly driven by an unhealthy food environment. Within the food environment, supermarkets form an important leverage point to influence dietary patterns as they serve as a major source of food for populations. Supermarket interventions are therefore a promising strategy to promote healthy food and beverage purchases (8).
Previous studies (8–12), including our own (13), have shown that nudging and pricing strategies—and especially their combination—can effectively influence food purchases. In a virtual supermarket experiment, we demonstrated that salient pricing strategies (i.e., taxing, subsidies, or both) and nudges combined significantly increased the total percentage of healthy purchases by ∼4%. However, these strategies may have differential effects across food groups that are masked when analyzing all healthy purchases combined. Studies on price elasticities, for example, show that consumers are more responsive to price changes in some food groups than in others (14, 15). In general, staple products (e.g., potatoes) are less responsive to price changes than more “luxury” foods (e.g., snacks) (16). Less is known about the responsiveness of different food groups to placement, promotion, and salience (elements of nudging) (10, 17). Most previous nudging studies focused on a single food group (8, 18), thereby limiting the possibility to compare nudge effectiveness across food groups. Some studies suggested that staple foods, in which purchases are largely driven by habitual behaviors, may be less responsive to nudging than nonstaple foods—more often based on impulse (19, 20).
Indirect effects of nudging and pricing strategies may be within–food group substitutions (e.g., shifting from refined to whole-grain bread) or between–food group spillover effects to other (nontargeted) food groups (e.g., increased purchases of dairy products when merely targeting cereals). It is well known that price increases in one group may lead to changed purchases in other food groups (i.e., cross-price elasticity) (15). However, less is known about within–food group substitutions relevant for public health. Insight into substitutions from unhealthier to healthier products within food groups requires detailed experimental data that are often unavailable. Moreover, current literature does not provide insight into spillover effects of nudges (21). Potential substitution or spillover effects may be favorable or unfavorable for the promotion of healthy diets and its public health impact.
Evidence on differential effects of strategies across food groups is required to provide better knowledge about what health effects may be expected from interventions and what approaches yield the largest impact. In the present study, we use data from the Supreme Nudge virtual supermarket experiment to explore as a secondary analysis in which food groups nudging and/or pricing strategies were most effective in changing healthy and unhealthy product purchases and whether the applied strategies resulted in within–food groups substitutions or spillover effects.
Methods
Study design and participants
This study is a secondary analysis of the Supreme Nudge virtual supermarket (SN VirtuMart) experiment (13). The SN VirtuMart is a 3-dimensional web-based virtual supermarket designed to investigate the single and combined effects of nudging and various pricing strategies on food purchases in the Netherlands. In this SN VirtuMart, we had set up a randomized mixed experimental study consisting of 3 study arms (between-subject design) and 5 study conditions (within-subject design) (Table 1). Participants were individually randomly allocated into 1 of the 3 study arms (25% tax, 25% subsidy, or 25% tax and subsidy) and, within these arms, were exposed to 5 study conditions (control, nudging, pricing, price salience, and price salience with nudging). The order in which the conditions were received within the study arms was individually randomized as well.
TABLE 1.
Design of the Supreme Nudge virtual reality supermarket study
| Arm | Condition 1: Control | Condition 2: Nudging1 | Condition 3: Price2 | Condition 4: Price salience3 | Condition 5: Nudging1 and price salience3 |
|---|---|---|---|---|---|
| Arm 1: 25% tax | Control | Nudging | Taxes | Salient taxes | Nudging and salient taxes |
| Arm 2: 25% subsidy | Control | Nudging | Subsidies | Salient subsidies | Nudging and salient subsidies |
| Arm 3: 25% tax and subsidy | Control | Nudging | Taxes and subsidies | Salient taxes and subsidies | Nudging and salient taxes and subsidies |
Nudging: bright orange–colored salience nudges promoting healthy products.
Price: a 25% price change in comparison to the baseline price, either for taxing of unhealthy products, subsidizing of healthy products, or a combination of both.
Price salience: a 25% price change in comparison to the baseline price, either for taxing of unhealthy products, subsidizing of healthy products, or a combination of both, which are actively communicated to the participant via “Discount” signage for subsidized products and a digital “news article” for the taxing.
Participants were recruited via a social media campaign using Facebook and Instagram. The social media campaign ran from mid-September to mid-December 2018. In October 2018, participants were also recruited via flyers distributed on the street, in real-world supermarkets, at local events, and by mail around the university campus and by postal service across various areas in the Netherlands.
Respondents were considered eligible for study participation when aged 18 years or older, were able to communicate in Dutch, had access to a computer with Internet, had a valid e-mail address, and were responsible for the household groceries. After study inclusion, participants were asked to imagine they did not have any groceries left at home. Next, they were asked to hypothetically purchase their weekly groceries in the SN VirtuMart during 5 consecutive weeks. They received a virtual budget based on their real-life grocery budgets as indicated by the participants in the baseline questionnaire. They could complete their weekly shop at the online checkout after spending between 50% and 125% of this weekly budget.
The original study protocol complies with the Declaration of Helsinki and was approved by the Medical Ethics Review Committee of VU University Medical Centre in Amsterdam (Office for Human Research Protections: IRB00002911). Informed consent was obtained from all the participants before they started the study.
Nudging and pricing strategies
The SN VirtuMart included 1175 different food items with market-conform prices and price promotions, reflecting a real-life Dutch supermarket setting and floor plan; only nonfood products and alcoholic beverages were excluded. All available products were categorized into 8 food groups and divided by healthy and unhealthy products within these groups (Table 2), based on the Dutch dietary guidelines (22). We made a selection of the available products to intervene on, with the aim to most accurately reflect a real-life scenario in which intervening on all foods at once would be unlikely. In total, 356 unhealthy products were taxed (37% of all unhealthy products), 195 of the healthy products were subsidized (89% of all healthy products), and 38 healthy products were nudged, out of which 36 were nudged and subsidized simultaneously (17% and 16% of all healthy products, respectively) (Table 2).
TABLE 2.
Food groups by healthy and unhealthy products and their intervention allocation within the virtual supermarket1
| Healthy products | Unhealthy or neutral products | |||
|---|---|---|---|---|
| Food group | Subsidized (–25%) and partly nudged | No intervention | Taxed (+25%) | No intervention |
| Fruit and vegetables (n = 95) | Fresh, frozen, and canned vegetables; fresh and frozen fruits; and apple sauce (n = 82; 86% of healthy fruit and vegetables) | Canned fruits and raw precut vegetables (n = 13; 14%) | NA | NA |
| Grains and potato (n = 166) | Whole-grain products (bread, pasta, rice, and crackers) (n = 14; 45% of healthy grains) | Whole-grain products (bread, crackers, breakfast grains) and fresh and unprocessed precut potatoes (n = 17; 55%) | Non-whole-grain products (bread, crackers, pasta, rice) (n = 36; 42% of unhealthy grains) | Non-whole-grain products (wraps, noodles, breakfast grains, and crackers), fried potatoes, and processed mashed potatoes (n = 49; 58%) |
| Dairy (n = 138) | Semiskimmed and skimmed dairy products and low-fat cheeses (n = 14; 88% of healthy dairy) | Skimmed coffee milk (n = 2;12%) | Sweetened semiskimmed and skimmed dairy products, full-fat dairy, custard, desserts, pudding, whipped cream, cooking cream, dairy drinks, chocolate milk, soy-dairy products (sweetened), and high-fat cheeses (n = 105; 86% of unhealthy dairy) | Pudding, ice cream, cream cheeses, and coffee milk (n = 17; 14%) |
| Other proteins (n = 154) | Fresh, frozen, and breaded fish; unsalted nuts; fresh and canned legumes (n = 51; 72% of healthy other proteins) | Unprocessed and low-fat meats, eggs, and canned fish (n = 20; 28%) | Salted nuts (n = 11; 13% of unhealthy other proteins) | Processed and high-fat meats and meat substitutes (salted) (n = 72; 87%) |
| Fats (n = 22) | NA | Olive oil, sunflower oil, vegetable oil, and margarine (n = 12; 100%) | NA | Frying oil, butter, and baking butter (n = 10; 100%) |
| Beverages (n = 139) | Tea bags, water, and flavored water (unsweetened) (n = 34; 61% of healthy beverages) | Filtered coffee products (n = 22; 39%) | Sodas and energy drinks (n = 32; 39% of unhealthy beverages) | Fruit juices, lemonade syrup, and unfiltered coffee products (n = 51; 61%) |
| Snacks (n = 249) | NA | NA | Fried salty snacks, chips, popcorn, candy, cakes, chocolate, licorice, and bubblegum (n = 149; 60% of unhealthy snacks) | Salty snacks, chips, popcorn, candy, cakes, cookies, rice crackers, bread sticks, dips, drinking broth, gingerbread, and water-based ice cream (n = 100; 40%) |
| Other foods (n = 262) | NA | NA | Pizza, sweetbread toppings (n = 23; 9% of unhealthy other foods) | Ready-to-eat meals, pancakes, canned soup, savory bread toppings, seasoning products, and baking products (n = 239; 91%) |
NA, not applicable.
The control condition represented a regular supermarket. In all conditions (including the control condition), the same realistic product promotions were placed at the end of aisles. The nudging condition included 3 types of bright orange–colored salience nudges. The first type of nudge consisted of shelf arrows pointing from a non-whole-grain product toward a whole-grain product. The second type consisted of a frame on the transparent fridge doors, highlighting the frozen vegetables section. The third type consisted of a frame as well, but this frame also included the text “Favorite” to additionally reflect a social norm. It was placed on the fridge doors around the skimmed dairy products and low-fat cheeses.
The pricing condition consisted of taxing of unhealthy foods and/or subsidizing of healthy foods. Both strategies encompassed a 25% price change in comparison to the baseline price. The price salience condition also included, next to the taxes and subsidies, a frame around the product indicating “Discount” for subsidized products, while presenting the regular price and the new subsidized price. For the taxed products, the price salience condition consisted of a digital “news article” that was presented before participants entered the SN VirtuMart to make respondents aware of price increases. The article stated a “sugar and fat tax of 25%” was now implemented in the Netherlands.
Study outcomes
The outcomes of this study were changes in the healthy and unhealthy product purchases within all food groups between the 4 intervention conditions compared with the control condition. Changes were calculated based on the number of items purchased. Using the number of items purchased enabled a consistent comparison of purchase changes between all food groups while also providing insights into within–food group substitution effects and within–food group spillover effects. Within–food group substitution effects were defined as an increase in healthy purchases with a simultaneous decrease in unhealthy purchases within the same food group. Within–food group spillover effects were defined as an increase or a decrease of purchases in food groups that were not targeted or minimally targeted by nudging or pricing strategies. Nontargeted was defined as the absence of an interventional strategy within the food group (e.g., group of fats) and minimally targeted when only a small proportion (<15%) of products were targeted (e.g., group of other foods). Detecting intervention effects derived from such a small proportion on the food group level was deemed implausible due to the initial sample size calculation of the SN VirtuMart experiment. The between-group spillover effects could be beneficial (increase in healthy purchases) or nonbeneficial (increase in unhealthy purchases) from a public health perspective.
Population characteristics
Data on participant characteristics were obtained via the online baseline questionnaire. Part of the baseline questionnaire asked participants about their sex (male/female), age (years), highest educational attainment (8 categorical levels), weight (kg), and height (cm). The BMI was calculated as weight divided by height squared (kg/m2). Educational level was categorized into 2 groups; low educational level included those who completed primary education, intermediate vocational education, and higher secondary education, and high educational level included those who completed higher vocational education or university. Further details on population characteristics have been described elsewhere (13).
Statistical analyses
Descriptive statistics included participant characteristics presented by study arm, consisting of age and BMI (mean ± SD), sex and educational level [n (%)], and the number of items purchased per food group in the control condition [median (Q1–Q3)]. Graphical inspection of the number of items purchased within all food groups indicated a Poisson distribution of the outcome data. Regular Poisson models assume an equal variance to the mean. In almost all of our food group outcomes, the variance was larger than the mean, indicating overdispersion. A few food group outcomes showed mild indications for overdispersion (e.g., for healthy grains and potatoes in the taxing arm, a mean of 4.2 items were purchased with a variance of 4.7 items), whereas most others showed large indications for overdispersion (e.g., for healthy dairy in the subsidy arm, a mean of 5.5 items were purchased with a variance of 17.2 items).
As the assumption of equal variance to the mean was violated, we selected the most suitable regression model for discrete count data using a model selection function via the R statistical software package glmmTMB (23, 24). The Akaike information criterion was used to select whether a generalized linear mixed model (GLMM), zero-inflated GLMM, and hurdle model, with a Poisson, Conway–Maxwell Poisson, or negative binomial distribution, best fitted the outcome data (i.e., purchases within all individual food groups). The Akaike information criterion is a measure to rank the quality of each model, relative to all other fitted models. Based on this ranking, the GLMMs with a Conway–Maxwell Poisson distribution appeared the most adequate fit for our food group outcome data. Therefore, we fitted separate models for each of the food group outcomes using GLMMs with a Conway–Maxwell Poisson distribution with a random intercept at the participant level, to estimate the incidence rate ratios (IRRs) and 95% CIs for products purchased within all food groups during the 4 experimental conditions in comparison to the control condition. IRRs in which the 95% CIs did not include 1 were considered statistically significant.
The Conway–Maxwell Poisson distribution is a flexible generalization of the Poisson distribution that is suitable for modeling of overdispersed as well as underdispersed count data. Modeled with the glmmTMB package, the Conway–Maxwell Poisson distribution is interpretable as a log-linear model (24, 25). The IRR reflects the percent change of the experimental condition compared with the control condition. For instance, a percentage increase for a positive IRR such as 1.09 reflects a 9% increase (26), and a percentage decrease for a negative IRR such as 0.89 reflects a (1/0.89 = 1.12) 12% decrease (27).
Data were a priori stratified by study arm as previous analyses of these data revealed a decrease in unhealthy purchases in the taxing arm, whereas there was no increase in the healthy purchases (13). The only exception was the evaluation of the nudging condition, for which we analyzed the total study sample (i.e., the 3 pricing arms combined) because all participants were exposed to the same nudging intervention irrespective to which pricing arm they were randomly allocated.
Results
In total, 455 participants enrolled in the study, of whom 346 completed all 5 shops. Useable data were available for 318 of those participants, as in the other cases, participants received an incorrect grocery budget or used an incorrect login code (Supplementary Figure 1). The study population consisted of ∼40% males, with a mean age of 35 y and a mean BMI of 25, and around half of the study population completed a high-level education (Table 3). These study characteristics were comparable across the pricings arms. Depending on the pricing arm, the median number of fruit and vegetables purchased in the control condition was 10 to 12 items, and this food group was the most frequently purchased food group. Other frequently purchased food groups were unhealthy other products (median purchase 7–10 items), snacks (4–6 items), and unhealthy dairy products (4.5–5 items), in contrast to healthy and unhealthy fats, which were the least frequently purchased food group (0–1 item) (Table 3).
TABLE 3.
Study population characteristics and the number of items purchased per food group in the control condition, by study arms (n = 318)1
| Characteristic | 25% tax (n = 108) | 25% subsidy (n = 119) | 25% tax and 25% subsidy (n = 91) |
|---|---|---|---|
| Study population characteristics | |||
| Sex, n males (%) | 46 (43) | 47 (40) | 31 (34) |
| Age, y, mean ± SD | 36.8 ± 15.4 | 35.5 ± 15.8 | 34.1 ± 13.4 |
| BMI, kg/m2, mean ± SD2 | 24.7 ± 5.0 | 25.5 ± 5.0 | 25.4 ± 4.6 |
| High educational level,3n (%) | 53 (49) | 52 (44) | 41 (45) |
| Number of items purchased in the control condition, median (Q1–Q3) | |||
| Healthy fruit and vegetables | 10.0 (7.0–14.0) | 11.0 (8.0–15.0) | 12.0 (7.0–18.5) |
| Healthy grains and potatoes | 4.0 (3.0–5.0) | 3.0 (2.0–5.0) | 4.0 (3.0–5.0) |
| Healthy dairy products | 2.0 (0.0–3.0) | 1.0 (0.0–3.0) | 1.0 (1.0–3.0) |
| Healthy protein products | 3.0 (2.0–4.3) | 3.0 (2.0–4.0) | 3.0 (2.0–5.0) |
| Healthy beverages | 1.5 (1.0–3.0) | 1.0 (0.0–2.0) | 2.0 (1.0–3.0) |
| Healthy fats | 0.0 (0.0–1.0) | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) |
| Unhealthy grains and potatoes | 4.0 (2.0–6.0) | 4.0 (2.0–6.0) | 4.0 (3.0–7.0) |
| Unhealthy dairy products | 4.5 (2.8–8.0) | 5.0 (3.0–9.0) | 5.0 (3.0–8.0) |
| Unhealthy beverages | 2.5 (1.0–4.3) | 3.0 (1.0–6.0) | 4.0 (2.0–5.5) |
| Unhealthy snacks | 4.0 (2.0–7.3) | 4.0 (2.0–8.0) | 6.0 (3.0–9.0) |
| Unhealthy other products | 8.0 (5.0–11.0) | 7.0 (4.0–12.0) | 10.0 (6.0–12.5) |
| Unhealthy protein products | 4.0 (3.0–6.0) | 4.0 (2.5–7.0) | 5.0 (3.0–7.5) |
| Unhealthy fats | 0.0 (0.0–1.0) | 0.0 (0.0–1.0) | 0.0 (0.0–1.0) |
Q, quartile.
Eight missing values.
3Participant who completed higher vocational education or university.
The effects of nudging and pricing strategies on changes in purchases from various food groups compared with the control condition are graphically shown in Figures 1 –4, separately for each experimental condition. A numeric overview of the results is also provided in Supplementary Table 1.
FIGURE 1.
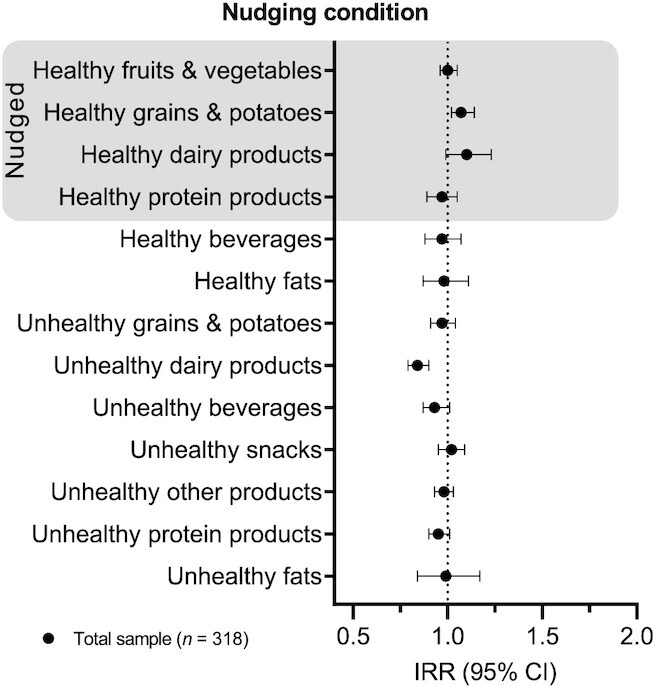
The effect of nudging on purchases from various healthy and unhealthy food groups. Analysis was based on a generalized linear mixed model with a Conway–Maxwell Poisson distribution with a random intercept at the participant level, to estimate the incidence rate ratios (IRRs) and 95% CIs for changes in products purchased within all food groups in the nudging condition in comparison to the control condition (total sample n = 318).
FIGURE 4.
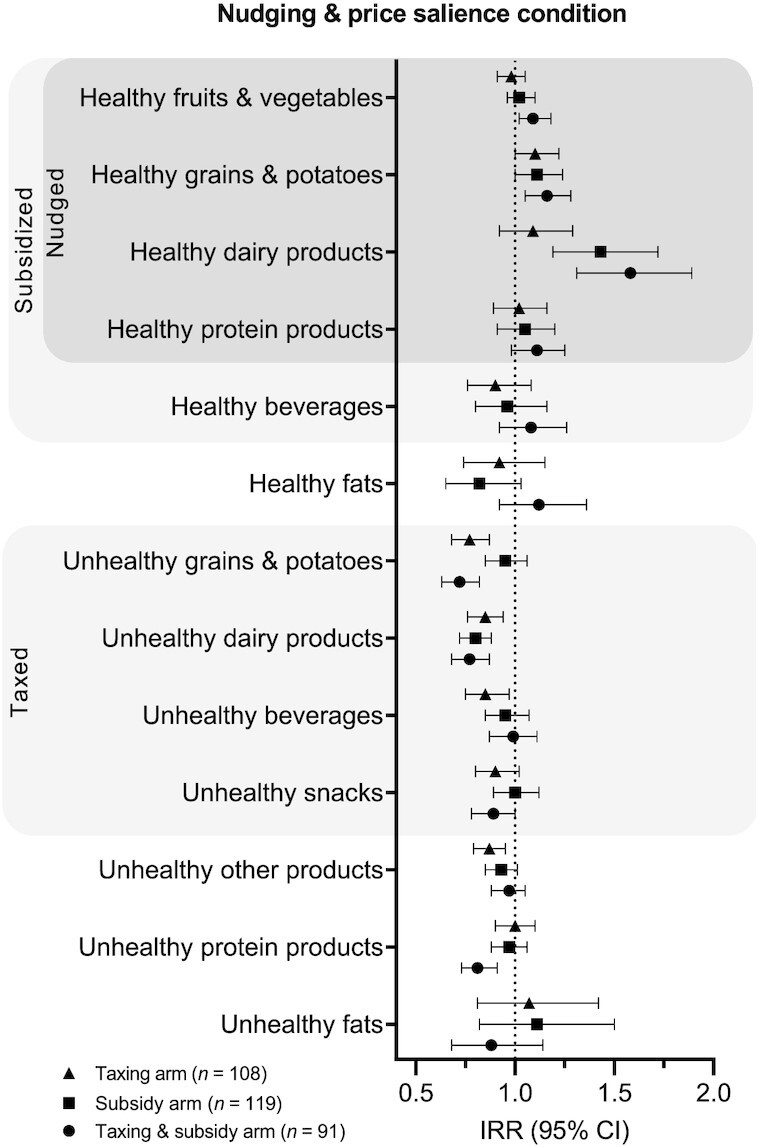
The effect of nudging and salient pricing strategies on purchases from various healthy and unhealthy food groups. Analysis was based on a generalized linear mixed model with a Conway–Maxwell Poisson distribution with a random intercept at the participant level, to estimate the incidence rate ratios (IRRs) and 95% CIs for changes in products purchased within all food groups in the price salience and nudging condition in comparison to the control condition (tax arm, n = 108; subsidy arm, n = 119; tax and subsidy arm, n = 91).
Differential effects across targeted food groups
Differential effects of the nudging and pricing strategies were observed across all study conditions. The nudging condition showed an increase in the healthy grains purchases of 7% (IRR = 1.07; 95% CI: 1.01, 1.14) and a nonsignificant increase of 10% in healthy dairy (IRR = 1.10; 95% CI: 0.99, 1.23), whereas no significant differences were found for vegetables and other protein products, which were also targeted (Figure 1). The price condition showed that subsidies did not significantly increase the targeted healthy purchases (Figure 2). Taxes decreased the unhealthy dairy product purchases by 14% (IRR = 0.88; 95% CI: 0.79, 0.98) but did not significantly change purchases of other targeted unhealthy products (i.e., grains, beverages, and snacks). In the price salience condition, subsidies increased all targeted healthy purchases (i.e., fruit and vegetables, grains, dairy products, and other protein products) except for beverage purchases (Figure 3). Taxes did not significantly decrease the targeted unhealthy purchases (i.e., grains, dairy, beverages, and snacks). Subsidies in the nudging and price salience condition resulted in an increase in healthy dairy purchases by 43% (IRR = 1.43; 95% CI: 1.19, 1.72) but did not significantly change the purchases of the also targeted fruit and vegetables, grains, protein products, and beverages (Figure 4). Taxes decreased the number of unhealthy grains by 30% (IRR = 0.77; 95% CI: 0.68, 0.87), unhealthy dairy products by 18% (IRR = 0.85; 95% CI: 0.76, 0.94), and unhealthy beverages by 18% (IRR = 0.85; 95% CI: 0.75, 0.97), whereas snack purchases did not significantly change (Figure 4).
FIGURE 2.
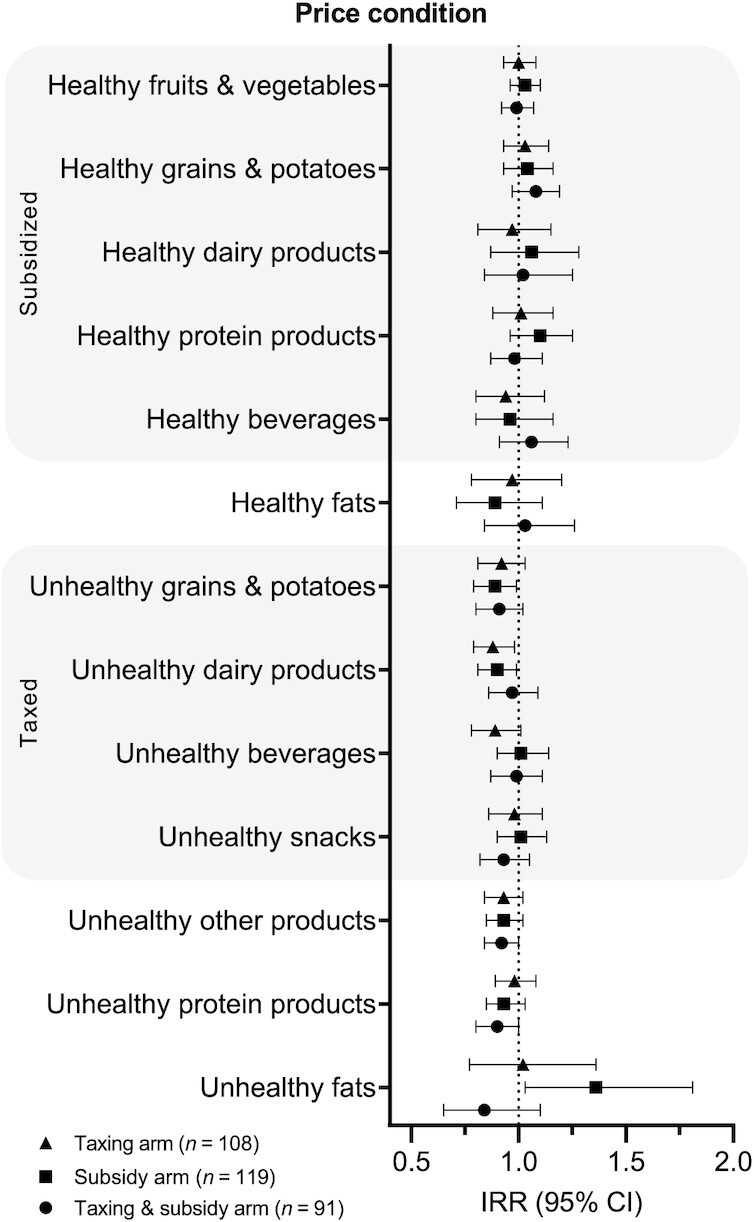
The effect of pricing strategies on purchases from various healthy and unhealthy food groups. Analysis was based on a generalized linear mixed model with a Conway–Maxwell Poisson distribution with a random intercept at the participant level, to estimate the incidence rate ratios (IRRs) and 95% CIs for changes in products purchased within all food groups in the pricing condition in comparison to the control condition (tax arm, n = 108; subsidy arm, n = 119; tax and subsidy arm, n = 91).
FIGURE 3.
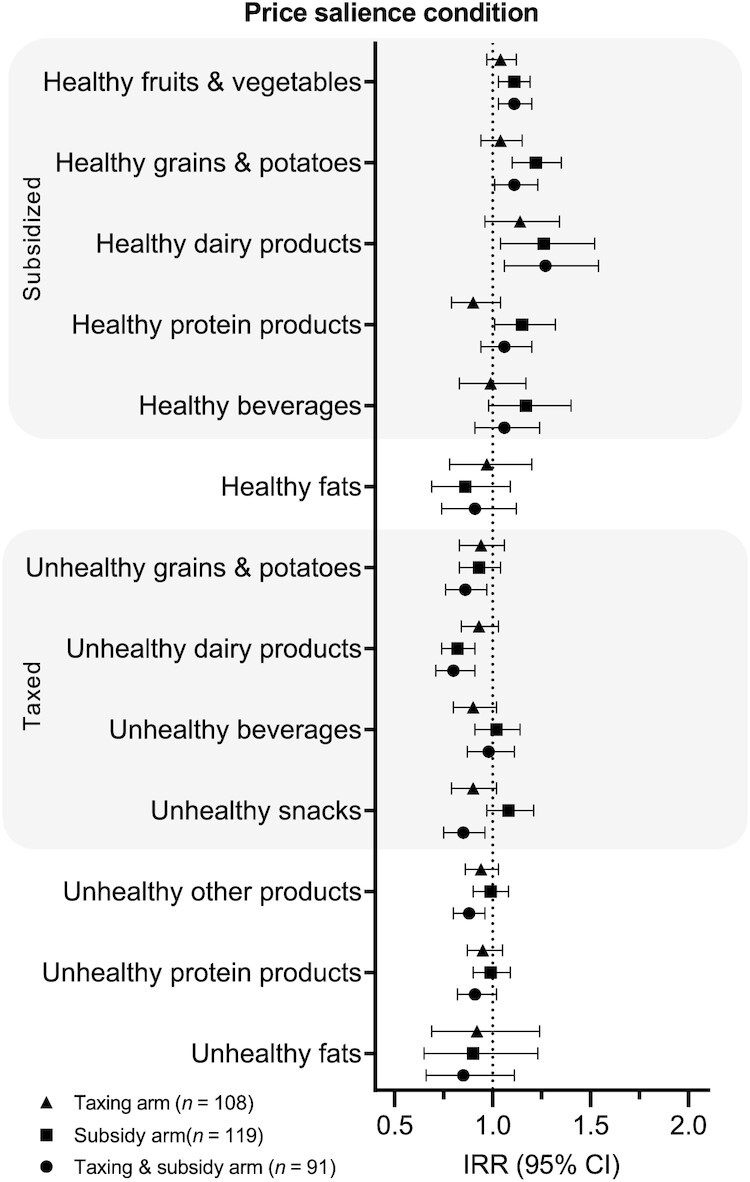
The effect of salient pricing strategies on purchases from various healthy and unhealthy food groups. Analysis was based on a generalized linear mixed model with a Conway–Maxwell Poisson distribution with a random intercept at the participant level, to estimate the incidence rate ratios (IRRs) and 95% CIs for changes in products purchased within all food groups in the price salience condition in comparison to the control condition (tax arm, n = 108; subsidy arm, n = 119; tax and subsidy arm, n = 91).
Results from the combined taxing and subsidy arm in the nudging and price salience condition generally showed larger effects than the individual effects of the subsidies and taxes (Figure 4). More specifically, the combination of subsidies and taxes increased the number of fruit and vegetables purchases by 9% (IRR = 1.09; 95% CI: 1.02, 1.18), healthy grains by 16% (IRR = 1.16; 95% CI: 1.05, 1.28), and healthy dairy products by 58% (IRR = 1.58; 95% CI: 1.31, 1.89), whereas healthy protein and beverage purchases did not significantly change. Furthermore, unhealthy grain purchases decreased by 39% (IRR = 0.72; 95% CI: 0.63, 0.82) and unhealthy dairy by 30% (IRR = 0.77; 95% CI: 0.68, 0.87), whereas unhealthy beverages and snack purchases did not significantly change.
Substitution effects within food groups
The nudging condition showed within–food group substitutions among dairy products. Purchases of the nontargeted unhealthy dairy products decreased by 19% (IRR = 0.84; 95% CI: 0.79, 0.90), while simultaneously, the targeted healthy dairy product purchases increased nonsignificantly by 10% (IRR = 1.10; 95% CI: 0.99, 1.23) (Figure 1). Whereas the price condition showed nonsignificant trends toward increased purchases of healthy dairy products and grains with simultaneous decreased purchases of unhealthy dairy products and grains (Figure 2), the price salience and nudging and price salience conditions showed significant within–food group substitution patterns for dairy products and grains (Figures 3 and 4). The within–food group substitution patterns were not seen among beverages.
Spillover effects to nontargeted or minimally targeted food groups
Neither the nudging condition nor the price condition showed between–food group spillover effects to nontargeted or minimally targeted food groups (Figures 1 and 2). The price salience condition, however, showed beneficial between-group spillover effects within the combined subsidies and taxes arm among the minimally targeted unhealthy other products, as purchases decreased by 14% (IRR = 0.88; 95% CI: 0.81, 0.96) (Figure 3). In the nudging and price salience condition, taxes decreased the purchases of the minimally targeted unhealthy other products by 15% (IRR = 0.87; 95% CI: 0.79, 0.95), whereas the combination of subsidies with taxes decreased the minimally targeted unhealthy protein products by 24% (IRR = 0.81; 95% CI: 0.73, 0.91) (Figure 4).
Sensitivity analyses
The results of the sensitivity analyses in which we explored the combined effects of the pricing arms in the total study sample showed the same pattern as the main results; that is, the nudging combined with pricing strategies were the most effective, and the largest effects were seen in the targeted groups of grains and dairy products (Supplementary Table 2). Healthy grains purchased increased by 12% (IRR = 1.12; 95% CI: 1.06, 1.19) and healthy dairy by 36% (IRR = 1.36; 95% CI: 1.23, 1.51), while simultaneously, the unhealthy grains decreased by 22% (IRR = 0.82; 95% CI: 0.77, 0.88) and unhealthy dairy by 25% (IRR = 0.80; 95% CI: 0.75, 0.86).
Discussion
Building on earlier results from the SN VirtuMart experiment, providing evidence for an overall beneficial effect of combined nudging and salient pricing strategies on healthy purchases (13), the current secondary analysis of this experiment shows that these strategies have differential effects across food groups. Nudging combined with pricing strategies were found to be more effective among grains and dairy compared with other food groups (i.e., fruit and vegetables, other protein products, beverages, and snacks). Furthermore, the combined nudging and pricing strategies resulted in within–food group substitutions for the groups of grains and dairy. Last, the applied strategies also caused beneficial within–food group spillover effects to the minimally targeted groups of unhealthy protein and unhealthy other products.
This study was, to the best of our knowledge, the first to comprehensively investigate the single and combined effects of nudging and pricing strategies across various food groups. We used a strong experimental within-subject combined with a between-subject design in which participants acted as their own control and used objectively measured outcome data. Our results, however, should be considered in light of their limitations. First, the comparison of intervention effects within food groups is complicated by the fact that certain food groups were more heavily targeted by nudging and/or pricing strategies than others. Thus, the intervention allocation could partly explain the stronger effects seen in some food groups. This could explain the observed effects in the dairy group. In contrast, grains showed the second largest increase in healthier purchases, whereas it was less targeted by nudging and pricing strategies compared with beverages, other proteins, and fruit and vegetables. It therefore seems unlikely that such effects completely explain our results. Second, due to the original design of the SN VirtuMart, possibilities for food group categorization were limited to mostly large and sometimes heterogeneous food groups to secure adequate power; among protein products and beverages, this may have attenuated potential effects. Third, our analytic approach did not account for multiple testing, and doing so would have led to less statistically significant findings. However, given our aim to provide insights into which food groups were accountable for the overall healthier purchases, we think it is justified to mainly focus on effect sizes and patterns in findings across study arms and conditions, rather than statistical significance. Fourth, truly capturing real-life purchasing behavior in a virtual supermarket setting may be challenging. Nevertheless, previous studies have shown that purchases made in a virtual setting are comparable to real life (28, 29), and 78% of our participants indicated they felt their virtual purchases reflected their real-life purchases. Fifth, our study sample may not fully reflect the average Dutch population, as participants were on average younger, higher educated, and more often female. Our inclusion criterion “primary household shopper” likely resulted in more females, whereas the younger population is likely due to the recruitment strategies used (e.g., Facebook).
Besides the intervention allocation across food groups and the heterogeneity within some of the groups, inherent food group differences may also explain the observed differential effects across food groups. Inherent group differences refer to the nature of the food groups themselves that make them more or less prone to intervention effectiveness. Although some studies have suggested that staple foods may be less prone to nudging and pricing strategies (16, 19, 20), our results suggest otherwise. It may be hypothesized that products within the groups of dairy products and within the group of grains are relatively comparable in product types and taste. Product substitutions with a comparable alternative may be easier. For instance, beverage purchases may be less subjected to impulse behaviors and more strongly depend on habitual behaviors (30), and soda may be less interchangeable with tea or water than high-fat yogurt with low-fat yogurt.
Other studies also observed differential effects of nudging and pricings strategies across food groups. The prospective effect of price changes across food groups on dietary intake was estimated in a meta-analysis (2). In line with our findings, subsidies were able to significantly increase fruit and vegetable consumption, whereas they did not significantly increase healthier beverage consumption. A study by Foster et al. (31) found that a combination of supermarket nudges (placement, signage, and product availability) increased healthy dairy sales, whereas another comparable study (signage, prime placement, and taste testing) reported that dairy sales remained unaffected (32). Comparable to our study, the same study reported increased healthy grain sales following nudges (32). Effects of nudging and pricing on purchases from different food groups warrant further investigation.
To achieve within–food group substitutions, other studies also concluded that dairy is promising to target with nudging (31, 33) and pricing strategies (14). However, a study estimating between–food group cross-price elasticities found that a price increase on dairy decreased the demand for dairy but simultaneously also unfavorably decreased the demand for fruit and vegetables (15). Our results do not confirm these nonbeneficial spillover effects. Our findings among beverages are in contrast to previous studies showing taxation reduces unhealthy beverage purchases and also promotes healthy beverage purchases (34, 35). Alternatively, similar to our findings, previous nudging studies on beverage sales show there were no substitution effects among beverages (31, 33). Regarding grains, a prediction study concluded that the cross-price elasticities within the groups of cereals and bread are very low (36). However, the food group categorization in this study did not differentiate between healthfulness of products. Although our results indicate otherwise, other nudging studies promoting healthy grains did not show evidence for within–food group substitutions (31, 33), possibly due to the nudge type used and the specific grains products targeted.
This combination of findings indicates that especially the groups of dairy and grains are promising to target with nudging and pricing strategies to achieve healthier purchases. For grains, the combination of nudging and pricing strategies seems important to enhance within–food group substitutions, whereas for dairy, solely implementing nudges also seems promising. Furthermore, real-life effect sizes of the combination of nudging and pricing strategies across food groups need to be established (29). Studies should focus on the promotion of a high number of the healthy foods while simultaneously discouraging unhealthy foods within the same group to promote within–food group substitutions. Multiple food groups across the supermarket should be targeted to enhance a shift toward a healthier dietary pattern on a population level and ultimately have an impact on public health (37).
In conclusion, the current secondary analysis of the SN VirtuMart experiment showed that nudging and pricing strategies do not have an equal effect on purchases for each food group. Dairy products and grains seem to be the most promising food groups to target in order to achieve healthier purchases. These food groups showed the largest shift in purchasing behaviors to healthier products following the implementation of nudges, salient subsidies, or salient taxes and the combination of all strategies. Future studies should focus on investigating (real-life) purchasing effects of the combination of nudging and pricing strategies equally balanced across multiple food groups in the supermarket.
Supplementary Material
ACKNOWLEDGEMENTS
The authors’ contributions were as follows––JMS: designed the current study, conducted the analysis, and drafted the manuscript; JCH: was responsible for the data collection and initial data preparation process; JDM, JWJB, and JL: supervised and along with JCH provided substantial contributions to study conception and contributed to writing the manuscript; and all authors: critically read and approved the final manuscript. The authors report no conflicts of interest.
Notes
This study was conducted as part of the doctoral thesis of JMS. Her work, as well as that of JCH and JDM, is supported through the Supreme Nudge program funded by the Dutch Heart Foundation and the Netherlands Organization for Health Research and Development (CVON2016-04). JDM is further funded by an NWO VENI grant on “Making the Healthy Choice Easier—Role of the Local Food Environment” (grant 451-17-032). The funders have no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript, nor have they authority on the decision to submit the manuscript for publication.
Supplemental Tables 1 and 2 and Supplemental Figure 1 are available from the “Supplementary data” link in the online posting of the article and from the same link in the online table of contents at https://academic.oup.com/ajcn/.
Abbreviations used: GLMM, generalized linear mixed model; IRR, incidence rate ratio; SN VirtuMart, Supreme Nudge virtual supermarket.
Contributor Information
Josine M Stuber, Department of Epidemiology and Data Science, Amsterdam Public Health Research Institute, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands; Upstream Team, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands.
Jody C Hoenink, Department of Epidemiology and Data Science, Amsterdam Public Health Research Institute, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands; Upstream Team, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands.
Joline W J Beulens, Department of Epidemiology and Data Science, Amsterdam Public Health Research Institute, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands; Upstream Team, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands; Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, Netherlands.
Joreintje D Mackenbach, Department of Epidemiology and Data Science, Amsterdam Public Health Research Institute, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands; Upstream Team, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands.
Jeroen Lakerveld, Department of Epidemiology and Data Science, Amsterdam Public Health Research Institute, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands; Upstream Team, Amsterdam UMC, VU University Amsterdam, Amsterdam, Netherlands.
Data Availability
Deidentified individual participant data described in the manuscript, code book, and analytic code will be made available upon request pending application and approval.
References
- 1. GBD 2017 Risk Factor Collaborators.. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet North Am Ed. 2018;392(10159):1923–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Afshin A, Penalvo J, Del Gobbo L, Kashaf M, Micha R, Morrish K, Pearson-Stuttard J, Rehm C, Shangguan S, Smith JDet al. CVD prevention through policy: a review of mass media, food/menu labeling, taxation/subsidies, built environment, school procurement, worksite wellness, and marketing standards to improve diet. Curr Cardiol Rep. 2015;17(11):98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Adams J, Mytton O, White M, Monsivais P. Why are some population interventions for diet and obesity more equitable and effective than others? The role of individual agency. PLoS Med. 2016;13(4):e1001990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, Moodie ML, Gortmaker SL. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378(9793):804–14. [DOI] [PubMed] [Google Scholar]
- 5. Vogel C, Abbott G, Ntani G, Barker M, Cooper C, Moon G, Ball K, Baird J. Examination of how food environment and psychological factors interact in their relationship with dietary behaviours: test of a cross-sectional model. Int J Behav Nutr Phy. 2019;16:1–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Anderson ES, Winett RA, Wojcik JR. Self-regulation, self-efficacy, outcome expectations, and social support: social cognitive theory and nutrition behavior. Ann Behav Med. 2007;34(3):304–12. [DOI] [PubMed] [Google Scholar]
- 7. Marteau TM, Hollands GJ, Fletcher PC. Changing human behavior to prevent disease: the importance of targeting automatic processes. Science. 2012;337(6101):1492–5. [DOI] [PubMed] [Google Scholar]
- 8. Hartmann-Boyce J, Bianchi F, Piernas C, Riches SP, Frie K, Nourse R, Jebb SA. Grocery store interventions to change food purchasing behaviors: a systematic review of randomized controlled trials. Am J Clin Nutr. 2018;107(6):1004–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Adam A, Jensen JD. What is the effectiveness of obesity related interventions at retail grocery stores and supermarkets? A systematic review. BMC Public Health. 2016;16:1247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Harbers MC, Beulens JWJ, Rutters F, de Boer F, Gillebaart M, Sluijs I, van der Schouw YT. The effects of nudges on purchases, food choice, and energy intake or content of purchases in real-life food purchasing environments: a systematic review and evidence synthesis. Nutr J. 2020;19(1):103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Afshin A, Penalvo JL, Del Gobbo L, Silva J, Michaelson M, O'Flaherty M, Capewell S, Spiegelman D, Danaei G, Mozaffarian D. The prospective impact of food pricing on improving dietary consumption: a systematic review and meta-analysis. PLoS One. 2017;12(3):e0172277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Shaw SC, Ntani G, Baird J, Vogel CA. A systematic review of the influences of food store product placement on dietary-related outcomes. Nutr Rev. 2020;78:1030–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Hoenink JC, Mackenbach JD, Waterlander W, Lakerveld J, van der Laan N, Beulens JWJ. The effects of nudging and pricing on healthy food purchasing behavior in a virtual supermarket setting: a randomized experiment. Int J Behav Nutr Phys Act. 2020;17(1):98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Andreyeva T, Long MW, Brownell KD. The impact of food prices on consumption: a systematic review of research on the price elasticity of demand for food. Am J Public Health. 2010;100(2):216–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Cornelsen L, Green R, Turner R, Dangour AD, Shankar B, Mazzocchi M, Smith RD. What happens to patterns of food consumption when food prices change? Evidence from a systematic review and meta-analysis of food price elasticities globally. Health Econ. 2015;24(12):1548–59. [DOI] [PubMed] [Google Scholar]
- 16. USDA.. Economic research services: commodity and food elasticities. Washington, DC: US Department of Agriculture; 2019; [Internet]. Available from: https://www.ers.usda.gov/data-products/commodity-and-food-elasticities/. [Google Scholar]
- 17. Marchiori DR, Adriaanse MA, De Ridder DTD. Unresolved questions in nudging research: putting the psychology back in nudging. Soc Personal Psychol. 2017;11(1):e12297. [Google Scholar]
- 18. Vecchio R, Cavallo C. Increasing healthy food choices through nudges: a systematic review. Food Qual Prefer. 2019;78:103714. [Google Scholar]
- 19. de Wijk RA, Maaskant AJ, Polet IA, Holthuysen NTE, van Kleef E, Vingerhoeds MH. An in-store experiment on the effect of accessibility on sales of wholegrain and white bread in supermarkets. PLoS One. 2016;11(3):e0151915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Inman JJ, Winer RS, Ferraro R. The interplay among category characteristics, customer characteristics, and customer activities on in-store decision making. J Marketing. 2009;73(5):19–29. [Google Scholar]
- 21. Karpyn A, McCallops K, Wolgast H, Glanz K. Improving consumption and purchases of healthier foods in retail environments: a systematic review. Int J Environ Res Public Health. 2020;17(20):7524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Kromhout D, Spaaij CJ, de Goede J, Weggemans RM. The 2015 Dutch food-based dietary guidelines. Eur J Clin Nutr. 2016;70(8):869–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Brooks ME, Kristensen K, van Benthem KJ, Magnusson A, Berg CW, Nielsen A, Skaug HJ, Machler M, Bolker BM. glmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. The R Journal. 2017;9(2):378–400. [Google Scholar]
- 24. Magnusson A, Skaug HJ, Nielsen A, Berg CW, Kristensen K, Maechler M, Bentham K, Bolker BM, Sadat N, Lüdecke Det al. Package ‘glmmTMB’: generalized linear mixed models using template model builder. Version 1.0.2.1. Vienna (Austria): The Comprehensive R Archive Network; 2020. [Google Scholar]
- 25. Huang A. Mean-parametrized Conway-Maxwell-Poisson regression models for dispersed counts. Stat Model. 2017;17(6):359–80. [Google Scholar]
- 26. Twisk JWR. Poisson multilevel analysis. In: Applied multilevel analysis: a practical guide for medical researchers. Cambridge (UK): Cambridge University Press; 2006. p. 54. [Google Scholar]
- 27. Twisk JWR. Categorical and ‘count’ outcome variables. In: Applied longitudinal data analysis for epidemiology: a practical guide. Cambridge (UK): Cambridge University Press; 2003. p. 160–2. [Google Scholar]
- 28. Waterlander WE, Jiang YN, Steenhuis IHM, Mhurchu CN. Using a 3D virtual supermarket to measure food purchase behavior: a validation study. J Med Internet Res. 2015;17(4):e107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. van Herpen E, van den Broek E, van Trijp HCM, Yu T. Can a virtual supermarket bring realism into the lab? Comparing shopping behavior using virtual and pictorial store representations to behavior in a physical store. Appetite. 2016;107:196–207. [DOI] [PubMed] [Google Scholar]
- 30. Hultén P, Vanyushyn V. Impulse purchases of groceries in France and Sweden. J Consumer Marketing. 2011;28(5):376–84. [Google Scholar]
- 31. Foster GD, Karpyn A, Wojtanowski AC, Davis E, Weiss S, Brensinger C, Tierney A, Guo WS, Brown J, Spross Cet al. Placement and promotion strategies to increase sales of healthier products in supermarkets in low-income, ethnically diverse neighborhoods: a randomized controlled trial. Am J Clin Nutr. 2014;99(6):1359–68. [DOI] [PubMed] [Google Scholar]
- 32. Gamburzew A, Darcel N, Gazan R, Dubois C, Maillot M, Tome D, Raffin S, Darmon N. In-store marketing of inexpensive foods with good nutritional quality in disadvantaged neighborhoods: increased awareness, understanding, and purchasing. Int J Behav Nutr Phy. 2016;13:104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Hobin E, Bollinger B, Sacco J, Liebman E, Vanderlee L, Zuo F, Rosella L, L'Abbe M, Manson H, Hammond D. Consumers' response to an on-shelf nutrition labelling system in supermarkets: evidence to inform policy and practice. Milbank Q. 2017;95(3):494–534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Colchero MA, Molina M, Guerrero-Lopez CM. After Mexico implemented a tax, purchases of sugar-sweetened beverages decreased and water increased: difference by place of residence, household composition, and income level. J Nutr. 2017;147(8):1552–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Thow AM, Downs S, Jan S. A systematic review of the effectiveness of food taxes and subsidies to improve diets: understanding the recent evidence. Nutr Rev. 2014;72(9):551–65. [DOI] [PubMed] [Google Scholar]
- 36. Harding M, Lovenheim M. The effect of prices on nutrition: comparing the impact of product- and nutrient-specific taxes. J Health Econ. 2017;53:53–71. [DOI] [PubMed] [Google Scholar]
- 37. Rose G. Sick individuals and sick populations. Int J Epidemiol. 1985;14(1):32–8. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Deidentified individual participant data described in the manuscript, code book, and analytic code will be made available upon request pending application and approval.