

Abstract
Clinic closures across the United States in response to the coronavirus disease 2019 (COVID-19) pandemic meant that many audiology services were reduced to phone calls, video visits, and modified services (e.g., curbside, mail-ins, drop offs). Audiologists and other providers needed a way to manage hearing- and ear-related complaints via telehealth. A simple pure tone air conduction threshold test performed at home was used to determine which patients needed to come into the clinic for an in-person appointment. This case will review a 56-year-old male who was being treated for an idiopathic sudden sensorineural hearing loss prior to clinic closure. He had on file a comprehensive audiogram at first onset of symptoms and was treated with oral steroids. Virtual hearing testing was then utilized for a variety of other patients from teenagers to adults to triage hearing- and ear-related complaints while clinics were closed for in-person visits.
Keywords: COVID-19, audiogram, hearing loss, telehealth, virtual audiogram, uHear, hearing test, sudden hearing loss
The World Health Organization (WHO) estimates that 466 million people or 5% of the world's population live with hearing loss. This number is expected to rise to 900 million over the next 30 years. 1 2 One way of responding to this growing number is by making basic hearing health assessments more accessible to the greater population. Applications (apps) for smart phones have been developed to reach more communities to assess their hearing health from home. 3 Specifically, these apps were developed to reach communities which are underserved. 3 These apps are available on a wide variety of phones including both Android and iPhone iOS platforms. There are free and low-cost versions. The free apps became very helpful for the treatment and management of hearing loss while keeping patients in their homes during the COVID 19 pandemic.
During the COVID-19 pandemic, stay at home orders were issued for highly populated counties in Pennsylvania on March 23, 2020, and for the entire state by April 1, 2020. For this case review, the clinic is in Allegheny County which includes the city of Pittsburgh. Allegheny County remained heavily restricted until June 5, 2020. During this time, otolaryngology and audiology services were reduced to modified services, phone calls, and video visits with little time to react and plan. The use of two apps was implemented to provide some objective test results for patients with hearing- and ear-related complaints. This allowed the clinic to prescreen patients before coming into the office when the audiologist was in. There was 1 day per week for in-person appointments for comprehensive audiograms with an audiologist. These appointments were reserved for those who were considered emergencies to reduce the risk of COVID-19 transmission.
Two apps were chosen to perform a pure tone air conduction threshold search with ear-specific data. These apps were chosen based on their ease of use, that there was no direct marketing to purchase a device based on results, and that an audiogram was produced for the result. uHear was chosen for iPhone/iPad iOS users. uHear has been reviewed and validated by most publications based on the pure tone average (PTA) of the app results and comprehensive audiograms performed in a clinic. 4 This app performs an automated modified Hughson Westlake procedure; there is only a “heard it” button for the user to press when the tone is audible. An ascending procedure is used until there is a “heard it” response. 5 This is a method commonly used when completing a comprehensive audiogram. 6 The approximate time to complete this test is 5 minutes and it produces an audiogram once completed ( Figs. 1 and 2 ).
Figure 1.

The patient's first comprehensive audiogram 5 days after idiopathic sudden sensorineural hearing loss onset.
Figure 2.

The patient's speech understanding scores and presentation levels 5 days after idiopathic sudden sensorineural hearing loss onset.
The other app chosen for Android users is called “Hearing Test.” The validation for this app comes from comparing adult audiometric thresholds performed on appropriate equipment with those obtained on the Android-based app. Results showed that all thresholds obtained from 250 to 8,000 Hz were within 2.6 dB of those obtained by a licensed professional on approved equipment. It also showed that retest reliability was high. 7 Hearing Test offers a pure tone air conduction assessment from 250 to 8,000 Hz. Calibration is required prior to starting the test. The user would select if their headphones came with their phone or tablet, “bundled headphones” or “unbundled headphones,” which are purchased separately from the phone or tablet. Unbundled headphones must be calibrated with the app. Calibration is a single tone being presented and slowly increased in volume. The user would select when they can hear the tone. The app creators recommend that a normal hearing person calibrate the device. 8 If the user has known hearing loss, they should request the assistance of another person in the home to calibrate for them. The user is presented with a blank audiogram and would adjust the red Os for the right ear and blue Xs for the left ear. At each presentation level, they can click one of the three responses: “I cannot hear,” “I can hear,” or “Barely audible” to determine their threshold. The user will do this for each octave from 250 to 8,000 Hz as well as 6,000 Hz. The app can identify when masking is needed with an asymmetry of 40 dB (dB) and applies it automatically. The user can see their results as they adjust and test themselves. Once the test is completed, the user is presented with an audiogram ( Fig. 3 ).
Figure 3.

The uHear testing screen.
This clinic was treating a patient for a sudden sensorineural idiopathic hearing loss (ISSNHL) in the right ear. ISSNHL is characterized by a change of at least 30 dB across three consecutive frequencies within 72 hours. 9 An ISSNHL should be diagnosed with a comprehensive audiologic evaluation. 10 This is done to confirm that it is a sensorineural hearing loss, and not a conductive hearing loss. A conductive hearing loss would be caused by any pathology in the outer or middle ear space. ISSNHL can be controversial in terms of treatment. It is estimated that 45 to 65% of cases will spontaneously recover. 11 Regardless, ISSNHL is commonly treated with a dose of oral steroids for 2 weeks as reported by 98% of otolaryngologists and 8% will try intratympanic steroids. 10 12 Intratympanic steroids are injected directly into the tympanic membrane. In this clinic, ENT providers commonly prescribe 2 weeks of high-dose oral steroids and attempt intratympanic membrane injections if no improvement is noted.
Case Presentation
This clinic was following up a 56-year-old male with ISSNHL in the right ear. His comprehensive audiogram revealed normal hearing through 2,000 Hz sloping to a moderately severe to severe sensorineural hearing loss in the left ear and normal hearing at 250 Hz sloping to moderately severe through 2,000 Hz rising to moderate sensorineural hearing loss. There was also an asymmetry in speech understanding at 60% understanding in the right ear and 96% in the left ear. The left ear is considered an approximate baseline as he reports symmetrical hearing prior to this incident. The ENT provider treated him with a high dose of oral steroids. If oral steroids did not improve hearing, he would be seen back in the office for intratympanic steroid injections ( Figs. 4 and 5 ).
Figure 4.

The Hearing Test app testing screen.
Figure 5.

A uHear audiogram report with a summary of the results.
The patient had begun treatment for ISSNHL 1 week prior to the stay-at-home order and subsequent clinic closures. Once he completed the initial treatment, he was to be seen for an updated comprehensive audiogram in order for the ENT provider to recommend further treatment. By this time, clinics had been closed. A virtual audiogram was performed to determine eligibility to come into the office for treatment.
The virtual audiogram protocol was developed for patients to assess their hearing and provide an audiologist with objective data. The main use of these tests was to assess if asymmetry was present or if the patient had a significant change in hearing compared with an audiogram that was already on record. The purpose of the virtual audiograms was neither to diagnose a type/degree of hearing loss nor to determine hearing aid candidacy. The goal was to use this mechanism to triage patients.
Method
The required materials for this assessment are a smart phone or tablet (can be Android or Apple iPhone) and pair of wired headphones. Bluetooth headphones were discouraged, as they do not provide a steady signal and provide less accurate test results. The user/patient is also encouraged to perform this assessment in a room with low ambient noise.
The patient had a telehealth follow-up appointment, at which he completed a pure tone air conduction threshold test at home. In cases like this, the ENT provider typically placed a consult to an audiologist. An audiologist would contact the patient by phone call to instruct them on which app they were to download, explain how to complete the test, basic pure tone instructions, and how to send the results electronically by taking a screen shot. Some patients required in-depth instructions related to downloading the app and taking a screen of the results. The make and model of phone was required to determine which app they would be utilizing. Both apps produced an audiogram for which a screenshot was taken and emailed to the audiologist so that it could be uploaded in the medical record for the ENT provider to review. After the results were received, the audiologist would contact the patient again to review the results and answer all relevant questions. There are obvious limitations to this type of activity. The users were not using professionally calibrated equipment and they were not in a soundproof test booth. 13 This type of testing did not provide speech or bone conduction thresholds; therefore, the type of hearing loss could not be identified. However, this provided an option for care and treatment for all hearing and ear patients. All limitations were taken into consideration.
There is still limited evidence that validates pure tone air conduction threshold applications. 1 The Hearing Test app for androids appears in far less research than uHear. However, a screening tool that produced an audiogram was highly valuable for the circumstances at this time.
Results
The patient completed his virtual audiogram via the Hearing Test app. He reported that his hearing had improved to baseline in the right ear. His wife calibrated the app for him. Pure tone air conduction thresholds from 500 to 2,000 Hz showed significant improvement. Despite significant improvement, a slight asymmetry remained in the low and high frequencies. It was recommended to the patient that he return for a comprehensive audiogram once the clinic returned to normal function. The ENT provider recommended that the patient stay home and follow up via telehealth during this time. The patient did follow up with audiology via telehealth to briefly discuss hearing aid benefits. They understood that to proceed with hearing aids, a complete audiometric evaluation was still required under Pennsylvania state law. 14 If the patient's thresholds had not improved significantly, he would have been offered an in-office visit. At this time, he would have had a complete audiometric evaluation and intratympanic membrane injections if calibrated test results did not show an improvement ( Fig. 6 ).
Figure 6.
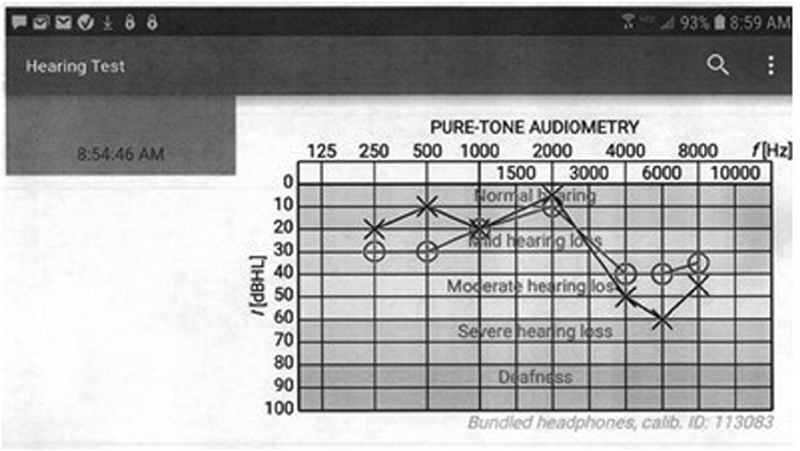
The patient's Hearing Test audiogram after 2 weeks of oral steroids.
Conclusion
Telehealth services have been available for audiologists in a variety of ways well before the COVID-19 pandemic began. There are resources to program hearing aids remotely and visual demonstrations of tasks like changing wax guards for patients at home. The availability of some apps like Hearing Test and uHear allowed audiologists to pivot care to a virtual model during stay-at-home orders across the country. A virtual audiogram protocol was developed to improve accessibility of audiologist services and create a triage system that helped determine which patients needed to be seen in person versus which patients could reasonably complete follow-up appointments via telemedicine. The patient described in this case report experienced a subjective improvement in hearing thresholds. After completing the virtual audiogram which was consistent with his report, he was cleared to stay home, complete a telemedicine follow-up appointment, and reduce the risk of transmission of COVID-19 in the office.
Footnotes
Conflict of Interest No conflicts to report.
References
- 1.World Health Organization. 2017Deafness and Hearing LossAccessed February 27, 2017 at:http://www.who.int/mediacentre/factsheets/fs300/en/
- 2.Schmucker C, Kapp P, Motschall E, Loehler J, Meerpohl J J. Prevalence of hearing loss and use of hearing aids among children and adolescents in Germany: a systematic review. BMC Public Health. 2019;19(01):1277. doi: 10.1186/s12889-019-7602-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Swanepoel W, Clark J L, Koekemoer D. Telehealth in audiology: the need and potential to reach underserved communities. Int J Audiol. 2010;49(03):195–202. doi: 10.3109/14992020903470783. [DOI] [PubMed] [Google Scholar]
- 4.Bright T, Pallawela D. Validated smartphone-based Apps for ear and hearing assessments: a review. JMIR Rehabil Assist Technol. 2016;3(02):e13. doi: 10.2196/rehab.6074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jerger J. The evolution of the audiometric pure-tone technique. Hearing Review. 2018;25(09):12–18. [Google Scholar]
- 6.Carhart R, Jerger J F. Preferred method for clinical determination of pure-tone thresholds. J Speech Hear Disord. 1959;24(04):330–345. [Google Scholar]
- 7.Masalski M, Grysiński T, Kręcicki T. Hearing tests based on biologically calibrated mobile devices: comparison with pure-tone audiometry. JMIR Mhealth Uhealth. 2018;6(01):e10. doi: 10.2196/mhealth.7800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Masalski M, Grysiński T, Kręcicki T. Biological calibration for web-based hearing tests: evaluation of the methods. J Med Internet Res. 2014;16(01):e11. doi: 10.2196/jmir.2798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Xie W, Dai Q, Liu J, Liu Y, Hellström S, Duan M. Analysis of clinical and laboratory findings of idiopathic sudden sensorineural hearing loss. Sci Rep. 2020;10(01):6057. doi: 10.1038/s41598-020-63046-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kuhn M, Heman-Ackah S E, Shaikh J A, Roehm P C. Sudden sensorineural hearing loss: a review of diagnosis, treatment, and prognosis. Trends Amplif. 2011;15(03):91–105. doi: 10.1177/1084713811408349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mattox D E, Simmons F B.Natural history of sudden sensorineural hearing loss Ann Otol Rhinol Laryngol 197786(4, Pt 1):463–480. [DOI] [PubMed] [Google Scholar]
- 12.Shemirani N L, Schmidt M, Friedland D R. Sudden sensorineural hearing loss: an evaluation of treatment and management approaches by referring physicians. Otolaryngol Head Neck Surg. 2009;140(01):86–91. doi: 10.1016/j.otohns.2008.09.022. [DOI] [PubMed] [Google Scholar]
- 13.Frank T. ANSI update: maximum permissible ambient noise levels for audiometric test rooms. Am J Audiol. 2000;9(01):3–8. doi: 10.1044/1059-0889(2000/003). [DOI] [PubMed] [Google Scholar]
- 14.Hearing Aid Sales Registration LawP.L. 1182, No. 262.1976