

Abstract
Objectives To examine pediatricians' perspectives on administrative tasks including electronic health record (EHR) documentation burden and their effect on work–life balance and life and career satisfaction.
Methods We analyzed 2018 survey data from the American Academy of Pediatrics (AAP) Pediatrician Life and Career Experience Study (PLACES), a longitudinal cohort study of early and midcareer pediatricians. Cohorts graduated from residency between 2002 and 2004 or 2009 and 2011. Participants were randomly selected from an AAP database (included all pediatricians who completed U.S. pediatric residency programs). Four in 10 pediatricians (1,796 out of 4,677) were enrolled in PLACES in 2012 and considered participants in 2018. Data were weighted to adjust for differences between study participants and the overall population of pediatricians. Chi-square and multivariable logistic regression examined the association of EHR burden on work–life balance (three measures) and satisfaction with work, career, and life (three measures). Responses to an open-ended question on experiences with administrative tasks were reviewed.
Results A total of 66% of pediatrician participants completed the 2018 surveys (1,192 of 1,796; analytic sample = 1,069). Three-fourths reported EHR documentation as a major or moderate burden. Half reported such burden for billing and insurance and 42.7% for quality and performance measurement. Most pediatricians reported satisfaction with their jobs (86.7%), careers (84.5%), and lives (66.2%). Many reported work–life balance challenges (52.5% reported stress balancing work and personal responsibilities). In multivariable analysis, higher reported EHR burden was associated with lower scores on career and life satisfaction measures and on all three measures of work–life balance. Open-ended responses ( n = 467) revealed several themes. Two predominant themes especially supported the quantitative findings—poor EHR functionality and lack of support for administrative burdens.
Conclusion Most early to midcareer pediatricians experience administrative burdens with EHRs. These experiences are associated with worse work–life balance including more stress in balancing responsibilities and less career and life satisfaction.
Keywords: electronic health record, work–life balance, satisfaction
Background and Significance
Clinical documentation has been digitized substantially over the last decade. In 2015, 96% of hospitals used certified electronic health records (EHRs), 1 and EHR use by office-based pediatricians increased from 58% in 2009 to 79% in 2012 and to 94% in 2016. 2 3 Although EHRs are standard practice, pediatricians must adhere to clinical documentation requirements developed in 1997 when nearly all pediatric offices documented on paper. 4 Electronic documentation and team-based charting created conflicts with outdated regulations and introduced new problems including documentation burden, chart bloat, and information overload. 5 6 7
Concerns are growing about physician burnout and the negative impact on patient care, including increased medical errors. 2 3 4 Use of EHRs has been linked to higher risk for physician burnout. 8 Recent studies indicate that a large portion of physician time is spent on EHR documentation. A study of adult physicians in ambulatory settings found for every hour in patient encounters, physicians work 2 additional hours on EHRs and administrative tasks during office hours, plus 1 to 2 hours nightly from home. 9 A study of primary care physicians reported that they spent 6 hours interacting with the EHR on work days, 10 and physicians in an academic faculty group spent up to 3 hours on the EHR on days without any appointments. 11 Increased self-reported physician workload was associated with increased asynchronous alerts or inbox notifications, 12 13 and high volumes of patient call messages have been linked to burnout. 14 Less research has focused on pediatricians or the association of EHR use and work–life balance and satisfaction.
Objectives
Our goals were to examine (1) early and midcareer pediatricians' perspectives on administrative tasks, including EHR documentation burden; (2) existing approaches to reduce burden; (3) variation of perspectives by specialization (e.g., generalist, subspecialist, or hospitalist); and (4) the effect of EHR burden on work–life balance and satisfaction with work.
Methods
Participants
We analyzed survey data collected in 2018 from the national American Academy of Pediatrics (AAP) Pediatrician Life and Career Experience Study (PLACES). PLACES is a cohort study tracking the work and life experiences of pediatricians across their career continuums. 15 16 Pediatricians who agreed to participate in this longitudinal study are surveyed twice annually by email and mail, depending on preference. The PLACES extensive annual survey covers several domains (e.g., work characteristics, satisfaction, work–life balance, life experiences). A shorter annual survey covers a single topic selected by the participants. In 2018, “administrative tasks” was chosen.
Study cohorts graduated from residency between 2002 and 2004 or 2009 and 2011. PLACES participants were randomly selected from an AAP database that included all pediatricians who completed U.S. pediatric residency programs, both AAP members and nonmembers. Four in 10 pediatricians (1,925 out of 4,677) invited to participate in PLACES initially signed up for the longitudinal study in 2012. Of these, 93.7% (1,804) completed the first survey and were thereafter considered PLACES participants; eight of these participants either passed away or asked to be dropped from the study.
Compared with the target population of pediatricians (all pediatricians who graduated residency between 2002 and 2004 or 2009 and 2011), study participants were significantly more likely to be female, AAP members, and graduates of U.S. medical schools. Therefore, two types of weights were calculated to adjust for differences in study and target cohorts. The first weight was a nonresponse weight to adjust for differences between participants and the target sample of pediatricians for sex and AAP membership status. The second weight was a poststratification weight to adjust for differences between medical school location of participants and information on pediatricians from the American Board of Pediatrics. Adjusted weights were applied to all analyses presented in this study. Additional details regarding PLACES methodology, including target population, sample size analysis, and nonresponse and poststratification weights have been described previously. 15 The AAP Institutional Review Board approved the study and all surveys.
Measures
After a literature review, the AAP PLACES Project Advisory Committee and other practicing pediatricians advised on development of the questions, which were primarily fixed-response questions.
In the shorter 2018 survey, we queried participants about their perceived burden for three administrative tasks, including (1) EHR documentation; (2) billing, preauthorization, and other insurance tasks; and (3) quality and performance measurements (survey questions provided as Appendix A ). Response options included no, minor, moderate, and major burden. We asked fixed-response questions regarding seven approaches that might reduce administrative burdens, the level of input participants had on EHR documentation practices at their workplace, and experiences with scribes assisting with documentation. The survey included one open-ended question asking about additional experiences with administrative tasks.
Appendix A. Survey questions asked to AAP PLACES participants in 2018 on administrative tasks.
| 1. For each area, to what extent do you feel that the following administrative tasks are a burden to you at your primary job? | |||||
| Not a burden | Minor burden | Moderate burden | Major burden | NA | |
| EHR documentation | □ | □ | □ | □ | □ |
| Billing, preauthorization, and other insurance | □ | □ | □ | □ | □ |
| Quality and performance measurement | □ | □ | □ | □ | □ |
| Other (please specify): | □ | □ | □ | □ | □ |
| 2. For each area, how much input do you have regarding procedures and staffing in these administrative areas? | |||||
| No input | Minor input | Moderate input | Major input | NA | |
| EHR documentation | □ | □ | □ | □ | □ |
| Billing, preauthorization, and other insurance | □ | □ | □ | □ | □ |
| Quality and performance measurement | □ | □ | □ | □ | □ |
| 3. How much do you agree or disagree with the following statements? | |||||
| Strongly disagree | Disagree | Agree | Strongly agree | ||
| I have adequate time to spend with my patients during typical visits | □ | □ | □ | □ | |
| I have freedom to make clinical decisions that meet my patients' needs | □ | □ | □ | □ | |
| I have adequate time and support to address administrative tasks | □ | □ | □ | □ | |
| Physicians at my work place have adequate voice in decisions regarding administrative structures and tasks | □ | □ | □ | □ | |
| 4. How much do you agree or disagree that the following approaches might reduce administrative tasks on physicians at your work place? | |||||
| Strongly disagree | Disagree | Agree | Strongly agree | ||
| Increase time scheduled for patient visits | □ | □ | □ | □ | |
| Provide more protected time in physician's schedule for administrative work | □ | □ | □ | □ | |
| Shift administrative work to other team members | □ | □ | □ | □ | |
| Add scribes to the team | □ | □ | □ | □ | |
| Improve the functionality of the EHR | □ | □ | □ | □ | |
| Provide training to physicians on efficient ways to use your EHR | □ | □ | □ | □ | |
| Obtain physician input on administrative structures and tasks | □ | □ | □ | □ | |
| Other (please specify): | □ | □ | □ | □ | |
| 5. One of the most specific strategies that have been suggested to reduce administrative tasks for physicians is scribes. Do you have a scribe at your work place to assist you in EHR documentation? | |||||
| □ Yes → How would you rate the services of the scribe(s) at your work place? | |||||
| □ Poor □ Fair □ Good □ Very good □ Excellent | |||||
| □ No → Has the use of scribes been discussed at your work place? | |||||
| □ No □ Yes □ Not sure | |||||
| 6. What more should we know about your experiences with administrative tasks? | |||||
Abbreviation: EHR, electronic health record.
In the 2018 larger PLACES survey, we asked participants about their specialty (generalist, hospitalist, subspecialist, other), work hours (full-time, part-time), practice ownership (owner, employee, or other), work–life balance (three measures), and satisfaction (three measures). Work–life balance measures included (1) perceived stress balancing work and personal responsibilities; (2) satisfaction with time for personal interests or hobbies; and (3) frequency of work performed at home, such as patient charting. Satisfaction measures included agreement that (1) work is personally rewarding; (2) career as a physician is satisfying; and (3) satisfaction with overall life. Response options are described below.
Data Analysis
Quantitative Data
We linked data from two PLACES surveys conducted in 2018 with information collected during study recruitment in 2012 on age, sex, race and ethnicity, and medical school location.
We used chi-square tests to examine variations in pediatrician perceptions of (1) burden from administrative tasks (major or moderate vs. minor or no burden) and (2) approaches to reduce burdens (strongly agree vs. agree, disagree, strongly disagree) by career specialty (generalist, subspecialist, hospitalist). We used McNemar tests to identify which of the three administrative tasks were rated as most burdensome (moderate or major burden) for each specialty.
We used chi-square tests to examine associations of pediatrician-reported EHR burden (major or moderate vs. minor or no burden) with work–life balance and satisfaction measures. Work–life balance responses were dichotomized as follows: (1) perceived stress balancing work and personal responsibilities (very or moderately vs. little or not at all stressed); (2) satisfaction with time for personal interests or hobbies (very satisfied or satisfied vs. neutral, dissatisfied, or very dissatisfied); and (3) frequency of work performed at home, such as patient charting (every work day vs. more than once a week but less than every day, about once a week, about once a month, or a few times a year or never). Satisfaction measures were dichotomized as follows: (1) work is personally rewarding (strongly agree or agree vs. neither agree nor disagree, disagree, or strongly disagree); (2) career as a physician is satisfying (strongly agree or agree vs. neither agree nor disagree, disagree, or strongly disagree); and (3) satisfaction with overall life (completely or very vs. somewhat, not very, or not at all satisfied).
For the work–life balance and satisfaction measures that varied significantly by EHR burden, we used multivariable logistic regression to examine the independent effect of burden controlling for pediatrician self-reported level of input on EHR implementation and staffing, age cohort (between 2009 and 2011 or 2002 and 2004 residency graduate), sex, race and ethnicity, medical school location, married or partnered, children, career specialty (generalist, subspecialist, or hospitalist), practice ownership, and part-time hours. Characteristics included in the models were based on prior work 17 18 and a priori hypotheses that they would be related to work–life balance and satisfaction.
The number of cases in each analysis varied slightly because of missing values for specific questions. All data presented are weighted as described above. Analyses were conducted with IBM SPSS Statistics 25 (SPSS Inc., Chicago, Illinois, United States), with p ≤ 0.05.
Qualitative Data
Two authors (M.P.F. and C.A.S.) reviewed all open-ended responses to the following question: “What more should we know about your experiences with administrative tasks?” They created a list of codes and used a conventional content analysis approach 19 and ATLAS.ti to tag and assess all comments. Codes were updated during iterative readings as part of the coding process. Coding agreement was 86%; discrepancies between the authors were resolved through discussion. Themes were identified to help illustrate the data.
Results
Sixty-six percent of PLACES participants completed both 2018 surveys (1,192 of 1,796). The analytic sample was restricted to 1,069 participants, who completed at least one question on administrative tasks and worked in general pediatrics ( n = 481), subspecialty care ( n = 481), and hospitalist care ( n = 107) in 2018. The 123 participants excluded were either not working or not providing direct patient care in 2018, reported another nonclinical position, or were in fellowship training.
Respondent Characteristics
Two-thirds of responding pediatricians were women (64.6%) and white, non-Hispanic (64.9%), with a mean age of 43 years (median = 43; standard deviation = 4.7). Most were graduates of U.S. medical schools (78.4%), married (88.4%), and had children (86.0%). Eight in 10 (78.5%) were employees, 17.4% were full- or part-owners, and 4.1% reported other (e.g., independent contractor). Twenty-three percent were working part-time, including 34.7% of women and 1.9% of men.
Sixty-five pediatricians (6.1%) reported using a scribe. Among scribe users, 0% rated their service as poor, 18.2% as fair, 35.1% as good, 22.1% as very good, and 24.7% as excellent. One-third or fewer of pediatricians reported having moderate or major input in procedures and staffing for administrative tasks, including EHR documentation (25.9%); billing, preauthorization, and other insurance (15.3%); and quality and performance measurement (33.7%).
Administrative Tasks—Burden and Approaches to Reduce Burden
Three-quarters of pediatricians (73.6%) reported EHR documentation was a major or moderate burden. Half (49.0%) reported such burden for billing and insurance and 42.7% for quality and performance measurement (QI). General pediatricians and subspecialists were more likely than hospitalists to report that EHR documentation (74.5, 75.3, and 62.3%, respectively, p < 0.05) and billing and insurance (51.9, 50.7, and 28.4%, p < 0.001) tasks were major or moderate burdens ( Fig. 1 ). For each specialty group, McNemar tests comparing responses to each of three tasks found more pediatricians in each group reported EHR documentation as more burdensome than billing and insurance and QI tasks ( p < 0.001 for all comparisons). For example, among generalists, 75.5% reported EHR documentation as a major or moderate burden compared with billing and insurance (51.9%, p < 0.001) or quality and performance measurement (47.7%, p < 0.001).
Fig. 1.
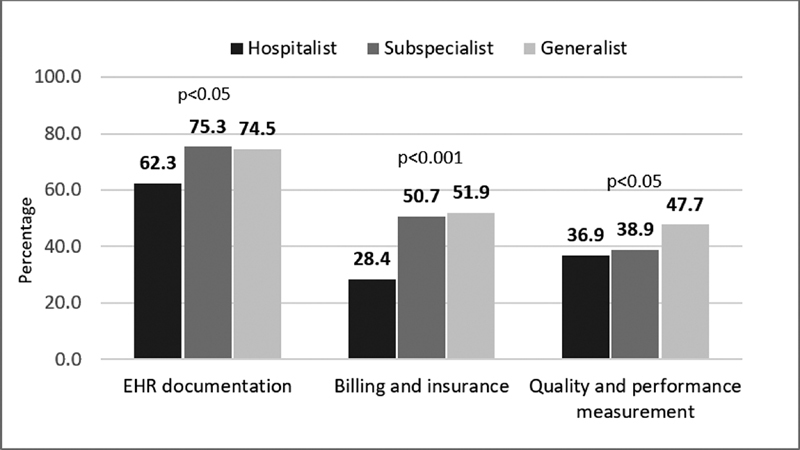
Administrative burden among early and midcareer pediatricians by specialty: percentage of pediatricians reporting major or moderate burden at work. Source: AAP PLACES 2018 (between 2002 and 2004 or 2009 and 2011 Residency Graduates Cohort). Weights were applied; n = 1,050. Chi-square examined burden (major or moderate vs. minor or no burden) for each area by specialty ( p -value represents result).
Regarding approaches pediatricians endorsed to help reduce physician administrative burdens, 90% strongly agreed (44.7%) or agreed (45.5%) with improving EHR functionality ( Fig. 2 ). Nine in 10 pediatricians also strongly agreed or agreed that providing protected time for tasks (89.9%), shifting tasks to other team members (86.5%), and obtaining physician input on administrative structures and tasks (92.9%) would reduce burden.
Fig. 2.
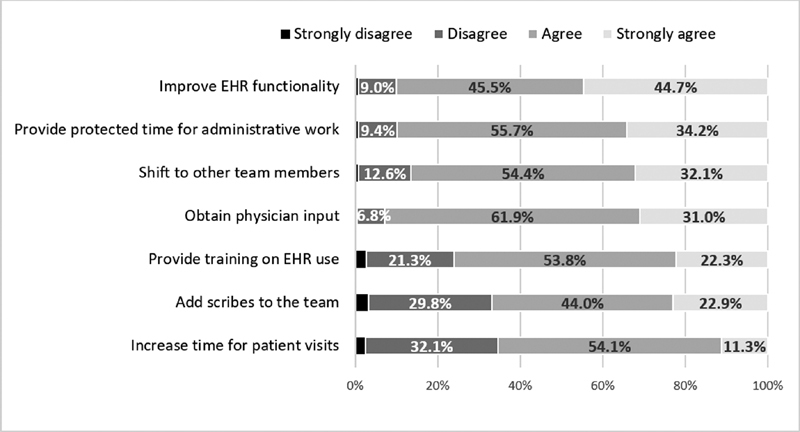
Agreement among early and midcareer pediatricians regarding approaches to reduce administrative burden. Source: AAP PLACES 2018 (between 2002 and 2004 or 2009 and 2011 Residency Graduates Cohort). Weights were applied; n = 1,063.
Pediatrician views on top approaches to reduce administrative burden varied across specialty, with five of seven approaches varying modestly. When examining “strongly agree” responses, subspecialists were most likely to strongly agree that improved EHR functionality (50.0% compared with 40.4% of generalists and 39.6% of hospitalists, p < 0.01), adding scribes to the team (27.8, 18.6, and 19.0%, p < 0.01), and shifting work to other team members (36.2, 31.4, and 28.1%, p < 0.05) might reduce burden. Hospitalists were most likely to strongly agree that protected time in schedules for administrative tasks might help (44.3% compared with 31.5% of generalists and 34.7% of subspecialists, p < 0.05). While few pediatricians (11.2%) strongly agreed that increased patient time might help, generalists were most likely to strongly agree with this approach (15.7 vs. 6.6% of hospitalists and 7.7% of subspecialists, p < 0.001).
Association of EHR Documentation Burden with Work–Life Balance and Satisfaction
Over half of pediatricians (52.5%) reported being very or moderately stressed balancing work and personal responsibilities. Only 32.2% were very satisfied or satisfied with their personal time, and 28.1% brought work home daily. Pediatricians reporting EHR documentation as a major or moderate burden were more likely to report stress balancing responsibilities and bringing work home daily and less likely to report satisfaction with their personal time ( Fig. 3 ). Sixty-one percent of pediatricians reporting EHR documentation as a major or moderate burden compared with 30.1% of those reporting less burden reported being very or moderately stressed balancing work and personal responsibilities, p < 0.001.
Fig. 3.
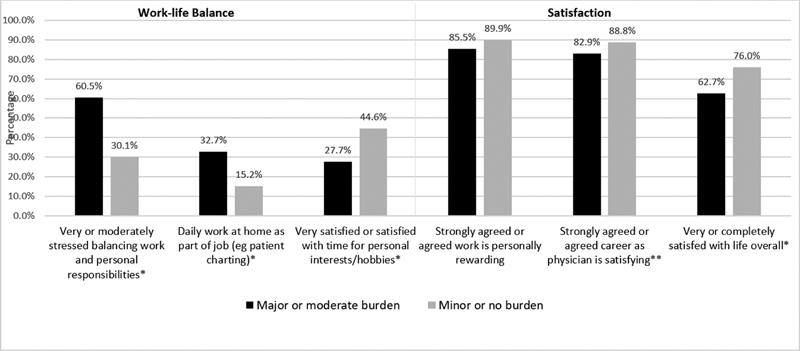
Early and midcareer pediatrician work–life balance and satisfaction by perceived EHR documentation burden. Source: AAP PLACES 2018 (between 2002 and 2004 or 2009 and 2011 Residency Graduates Cohort). Weights were applied; n = 1,052. * p < 0.001; ** p < 0.05 for chi-square test that examined EHR burden (major/moderate vs. minor/no burden) and work–life balance and satisfaction measures. EHR, electronic health record.
Large majorities of pediatricians strongly agreed or agreed that their work was personally rewarding (86.7%) and their career as a physician was satisfying (84.5%). Two-thirds (66.2%) reported they were completely or very satisfied with their overall life. Pediatricians who reported that EHR documentation was a major or moderate burden were less likely to agree that their career as a physician was satisfying and to report that they were completely or very satisfied with their overall life ( Fig. 3 ). Only 62.7% of pediatricians reporting EHR documentation was a major or moderate burden also reported being completely or very satisfied with their life compared with 76.0% of those reporting less burden ( p < 0.001).
Similar patterns were found in the multivariable logistic regression models ( Table 1 ). Pediatricians reporting more EHR documentation burden were more likely to be stressed balancing work and personal responsibilities and to bring work home daily (adjusted odds ratio [aOR] = 3.79, 95% confidence interval [CI] = 2.76–5.19 and aOR = 3.05, 95% CI = 2.08–4.47, respectively). They reported less satisfaction with personal time (aOR = 0.43, 95% CI = 0.32–0.59), career (aOR = 0.63, 95% CI = 0.41–0.98), and life overall (aOR = 0.49, 95% CI = 0.35–0.69). EHR burden was related to all five measures of work–life balance and satisfaction and was a bigger factor in the models than any of the pediatrician characteristics (gender, race, medical school, marital status, and having children).
Table 1. Factors associated with pediatrician work–life balance and satisfaction: results of multivariable logistic regression models.
| Adjusted odds ratio (aOR), 95% confidence interval (CI) | |||||
|---|---|---|---|---|---|
| Work–life balance | Satisfaction | ||||
| Very or moderately stressed balancing work and personal responsibilities | Daily work at home as part of job (e.g., patient charting) | Very satisfied or satisfied with time for personal interests/hobbies | Strongly agreed or agreed career as physician is satisfying | Very or completely satisfied with life overall | |
| EHR documentation burden | |||||
| Minor or no burden | Reference | Reference | Reference | Reference | Reference |
| Major or moderate burden | 3.79, 2.76–5.19 | 3.05, 2.08–4.47 | 0.43, 0.32–0.59 | 0.63, 0.41–0.98 | 0.49, 0.35–0.69 |
| Level of input in decisions regarding EHR | |||||
| Minor or no input | Reference | Reference | Reference | Reference | Reference |
| Major or moderate input | 0.87, 0.62–1.21 | 1.27, 0.89–1.81 | 0.92, 0.65–1.31 | 1.19, 0.76–1.89 | 1.25, 0.88–1.76 |
| Study cohort | |||||
| Between 2002 and 2004 Residency Graduates | Reference | Reference | Reference | Reference | Reference |
| Between 2009 and 2011 Residency Graduates | 1.57, 1.20–2.06 | 0.80, 0.60–1.06 | 0.72, 0.54–0.95 | 1.01, 0.71–1.45 | 0.79, 0.60–1.04 |
| Sex | |||||
| Male | Reference | Reference | Reference | Reference | Reference |
| Female | 1.55, 1.14–2.11 | 1.35, 0.97–1.89 | 0.66, 0.48–0.92 | 0.76, 0.50–1.16 | 0.80, 0.58–1.09 |
| Race and ethnicity | |||||
| White, not Hispanic | Reference | Reference | Reference | Reference | Reference |
| Hispanic | 1.47, 0.90–2.39 | 0.89, 0.53–1.50 | 0.91, 0.55–1.52 | 1.59, 0.77–3.29 | 1.54, 0.92–2.58 |
| Black or African American | 1.89, 0.98–3.61 | 0.98 0.48–1.99 | 1.13, 0.59–2.15 | 4.01, 1.05–15.37 | 0.58, 0.31–1.08 |
| Asian | 0.94, 0.65–1.35 | 1.45, 0.99–2.13 | 0.81, 0.55–1.19 | 0.83, 0.52–1.31 | 0.79, 0.55–1.14 |
| Other | 0.86, 0.33–2.29 | 0.56, 0.17–1.81 | 0.89, 0.32–2.51 | 2.06, 0.44–9.72 | 1.29, 0.46–3.61 |
| Medical school location | |||||
| United States or Canada | Reference | Reference | Reference | Reference | Reference |
| Outside United States or Canada | 0.68, 0.48–0.97 | 0.75, 0.51–1.11 | 1.21, 0.84–1.73 | 1.55, 0.92–2.59 | 0.67, 0.47–0.96 |
| Married | |||||
| No | Reference | Reference | Reference | Reference | Reference |
| Yes | 1.30, 0.81–2.09 | 1.75, 1.03–2.99 | 0.68, 0.42–1.10 | 0.78, 0.41–1.49 | 1.39, 0.87–2.23 |
| Have children | |||||
| No | Reference | Reference | Reference | Reference | Reference |
| Yes | 1.42, 0.90–2.23 | 0.65, 0.40–1.04 | 0.34, 0.22–0.53 | 1.43, 0.80–2.54 | 1.51, 0.97–2.37 |
| Career specialty | |||||
| Generalist | Reference | Reference | Reference | Reference | Reference |
| Subspecialist | 1.65, 1.21–2.25 | 1.30, 0.93–1.83 | 0.77, 0.56–1.06 | 1.21, 0.80–1.82 | 1.06, 0.77–1.45 |
| Hospitalist | 1.50, 0.93–2.41 | 2.01, 1.23–3.29 | 0.64, 0.38–1.06 | 1.01, 0.55–1.84 | 1.41, 0.86–2.31 |
| Full or part owner | |||||
| No (employee or other) | Reference | Reference | Reference | Reference | Reference |
| Yes | 1.07, 0.72–1.61 | 1.11, 0.72–1.72 | 0.99, 0.65–1.31 | 1.56, 0.87–2.82 | 1.47, 0.95–2.27 |
| Work hours | |||||
| Full-time | Reference | Reference | Reference | Reference | Reference |
| Part-time | 0.61, 0.43–0.88 | 1.18, 0.81–1.71 | 1.86, 1.28–2.71 | 0.83, 0.53–1.29 | 0.95, 0.67–1.37 |
Abbreviation: EHR, electronic health record.
Qualitative Data
Among the 1,069 study participants, 467 responded to the question, “What more should we know about your experiences with administrative tasks?” Table 2 lists major categories used to summarize participants' comments as well as example quotes. Two predominant themes that supported the quantitative findings were (1) documenting the patient visit in the EHR, including EHR functionality and (2) ways that might help physicians reduce their administrative burdens, such as designated time in physician schedules, dictation software and training on EHR systems, and support by administrators. Many commented on support staff and scribes taking on some documentation tasks which might allow physicians to work at the top of their license. Participants provided both positive and negative comments about scribes. Negative comments focused on costs associated with adding scribes to the team and interruptions to the workflow. One participant commented, “ A scribe has been offered to physicians in my practice, but each physician is responsible for that cost. That is not much of an incentive! I would prefer more time to be built into my schedule for EHR documentation than having a scribe.” Pediatricians expressed that patient documentation in the EHR is a huge burden, including the time needed to adequately document visits and number of documentation requirements. They commented on the functionality of the EHR (e.g., system is not user-friendly, customizable, or developed for pediatrics) and how documentation burden negatively affects their well-being, including work–life balance. One pediatrician commented, “It is an incredible burden to finish working a 10-hour day, 4–5 days per week, with at least 20 EHR charts to finish (about 2 hours of work). I leave the office as soon as all the tasks are done that have to be done at the office, so I can spend 30–60 minutes with my son before he goes to bed. Then, I chart for 2 hours. This is not sustainable.”
Table 2. Themes identified in pediatricians' open-ended responses to “What more should we know about your experiences with administrative tasks?” and illustrative quotes.
| Patient documentation in the electronic health record (EHR), including the functionality of the EHR |
| Pediatricians often commented on documentation issues including time needed to adequately document patient visits, volume of requirements, and negative effect on patient encounters. • “Use of an EHR has added significantly to work burden (that is not accommodated for in our documenting after work hours and on nights/weekends at home). If I try to document while in the room, it really detracts from the visit, taking away from that interpersonal experience. Scribes are a luxury that a small private practice cannot afford.” • “I don't mind some administrative tasks, particularly the ones that benefit the patient in front of me. What I resent, is the weaponization of the EMR and the shift of required data entry to the clinician so every committee in the hospital can have data streaming in that suits their particular needs. As soon as a new CMS requirement is pronounced, committees jump to see how they can manipulate the EMR to capture new data or process information that they care about by compelling certain fields of the clinician. They all justify it as “just a few more clicks.” Importantly, no one is keeping track of these ever-expanding demands/clicks so more and more of the work day is about checking the boxes. Patients are noticing too.” • “I would say that almost the entirety of my work outside of work hours is documentation in the EHR. This is not just writing progress notes for the patients I've seen in a day, but also updating discharge summaries for patients I'm signing out to another physician and updating a written handoff tool in the EHR. This is triple documentation and it is exhausting and a big 'dissatisfier'.” • “Administrative tasks especially EHR are burdensome and painstaking. Just looking at past medications takes multiple clicks. Not all the physicians document the same so seeing another physician's note is even more challenging. Yes, it is legible and easer to access but that is where the positivity ends.” |
| Functionality of the EHR |
| Many pediatricians commented on the functionality of the EHR, expressing that the system is not user-friendly, customizable, or developed for pediatrics. Billing issues and constant changes in procedures and updates related to the EHR were also voiced. • “EHRs are not user-friendly or customizable and do not decrease time spent charting, actually the opposite.” • “The EHR has significantly reduced the number of patients I can see in a day. In addition, it removes the personal nature of the note causing it to seem very generic. At some point in the future, I can see how and EHR may become beneficial to both the patient and the provider but we are not there yet.” • “Our EHR also needs improvement. People keep adding to it but not taking away. Now it's mostly a series of meaningless click boxes. It has some great, time saving features (vaccine decision support, for example), but there is also too much clutter.” • “Also, no one has talked about how billing in the EMR takes up more time. We used to just circle items that we had done on the paper bill and someone else would input all that. Now, the doctor has to do it and pick all the correct diagnosis codes to attach, etc., when signing off on a note. My providers are resenting all this.” A few PLACES pediatricians commented that the EHR improves their work and responsiveness to patients: • “I have made a lot of workarounds with EHR, (my major administrative task), so have ready-made note templates, etc. The initial time investment was definitely worth it.” • “I actually feel the EHR has improved my work and responsiveness to patients. Before the EHR it would take days to share lab results and respond to patients.” |
| Supporting physicians with administrative burdens |
| Pediatricians frequently commented on ways that might help physicians reduce their administrative burdens, mostly related to patient documentation. Topics included designated time in physician schedules to complete documentation, dictation software and training on EHR system, financial-related issues, and support by administrators. Many commented on support staff and scribes taking on some documentation tasks, which would allow physicians to work at the top of their license. Both positive and negative comments were provided about scribes. • “A scribe has been offered to physicians in my practice, but each physician is responsible for that cost. That is not much of an incentive! I would prefer more time to be built into my schedule for EHR documentation than having a scribe. All of us in my practice are either staying in office for several hours at end of day or finishing documentation at home. I do administrative tasks during the days off, as there is no other time to do it.” • “Scribes are a luxury that a small private practice cannot afford.” • “I had a scribe for 6–9 months, though adm. burden was decreased there was a lot of “down time” for the scribe. I have changed her role to more adm/medical assistant. Prepping my day, immunization needed, previous recent visit + last CPE [complete physical exam] documentation brought into visit. Post visit documentation routine + ins. [insurance] regulation such as care plans, referrals, documentation, etc. call back for normal laboratories.” • “Scribes are the exact opposite of what we really need. I need to write/dictate my own notes. This helps me to remember the patient and review the case and my own thought process, i.e., important to decision making.” • I personally have thought of scribes, but I actually feel that it would interfere with the intimate nature of the exam room. I think scribes would not decrease our workload as we would still need to review each chart and correct any errors that we found. I think in the long run it would actually increase our work than decrease our work.” • “Dragon Medically Speaking” is a program with voice recognition that substantially reduces documentation time. I highly recommend this. Scribes increase labor costs.” • “Being trained on an EHR in a way that truly matches how you prefer to work is important.” |
| Physician autonomy |
| Some pediatrician commented that their input is not considered, and decisions about issues that result in more administrative tasks for physicians are made by nonphysicians and/or those not aware of local issues. Comments again often focused on the EHR. • “EHR is a necessity, but doctors should have a lot more autonomy in guiding how they are delivered and modified.” • “Doctors do not have much control and/or say in the ridiculous amount of administrative/secretarial work they are required to do. Many other professions would not put up with this uncompensated time (e.g., lawyers).” • “More physician input is critical. Administrators who don't even use the EMR make all the decisions and are mostly oblivious to the repercussions of their decisions. I see a movement to improve this but we still have a long way to go.” |
| Physician health and wellness |
| Pediatricians commented that administrative tasks require them to bring work home such as charting or stay at work late. Some specifically raised the effect on work–life balance, physical and mental health, and satisfaction with their career. • “I am having a very difficult time balancing work and personal life. I am up until 1:30 a.m. at night to complete my documentational notes. It is a struggle. The lack of adequate sleep is so unhealthy. I worry about my health.” • “Less than half of what I do on a daily basis requires my brain. Much of it just occupies my fingers and eyeballs. It is repetitive, contributes little to meaningful patient care, and deadening and a major contributor to burnout.” • “It is an incredible burden to finish working a 10-hour day, 4–5 days per week, with at least 20 EHR charts to finish (about 2 hours of work). I leave the office as soon as all the tasks are done that have to be done at the office, so I can spend 30–60 minutes with my son before he goes to bed. Then, I chart for 2 hours. This is not sustainable.” |
| Other patient care responsibilities |
| Another topic raised by pediatricians included other patient care responsibilities that are time-consuming, burdensome, and interrupt their work flow including forms (e.g., school, daycare, camp) and other paper work, responding to patients (via calls, email, and patient portals), prescription renewals, and laboratory result inquiries. • “Patient messages are a huge administrative burden. We do not get compensated for essentially doing mini visits over EHR messaging. We should either bill for this service or get RVUs or both.” • “I have to complete a lot of forms for my patients, especially special-needs patients. Forms for school, asthma and allergy action plans, therapy prescriptions, nutrition forms, supplies, disability parking, and more. There is no reimbursement but they have to get done. I typically spend at least 1/2 day per week on forms. It is ridiculous.” |
Abbreviations: EHR, electronic health record; EMR, electronic medical record.
Discussion
Among a national sample of early and midcareer pediatricians, three-quarters reported being highly burdened by EHR documentation. Ninety percent believed that improving the functionality of the EHR, protecting time in physician's schedules for administrative tasks, shifting tasks to other team members, and obtaining physician input might help reduce the burden of administrative tasks on physicians. We also found consistent, statistically significant negative associations between self-reported EHR burden and measures of pediatricians' work–life balance and work and life satisfaction. More than half reported stress balancing work and personal responsibilities. Those who reported more burden with EHR documentation were twice as likely as those reporting less burden to report stress-balancing responsibilities and bringing work home daily. They were less likely to report satisfaction with their personal time, career as a physician, and overall life.
The impact of EHRs on work–life balance might be particularly salient in pediatrics. The majority of early and midcareer pediatricians are women with children. 15 Research on physicians at academic medical centers found that women spend more time on EHRs each day than men. 20 21 Other studies found that women are more likely to report burnout, 22 23 24 and have more household and childcare responsibilities 25 26 27 and report more challenges with work–life balance. 17 27 28 29 30
Most pediatricians in our study reported that improving EHR functionality might reduce administrative burdens for physicians. This also emerged as a theme in our qualitative analysis. One participant suggested that preparing “ready-made note templates” was worth the initial time investment. Participants noted frustration with the high number of clicks they needed to make in the EHR. Lack of pediatric functionalities in EHRs has been extensively documented. 3 31 32 33 EHRs require time-consuming, granular data documentation, and it is a reasonable expectation that entered data can be reused to complete forms required in pediatrics (e.g., school and administrative documents). However, lack of standardized data requests and forms and the need to enter these data in an EHR can be time-consuming and burdensome and result in duplicate documentation. Creation of essential clinical documentation components 34 and including ideal and accessible pediatric EHR functions 35 might reduce burden on pediatricians.
While pediatricians in our study believed that obtaining physician input would reduce administrative burdens, only a quarter of these pediatricians reported they have any input related to their EHRs. One of the consequences of EHR use has been the redistribution of work to physicians, such as through asynchronous messaging (“the burden of the inbox”) 13 without the addition of allotted time. Prior to EHRs with patient portals, patients would call the office and most needs would be addressed by office staff. While portals allow some self-service by patients reducing pediatrician work load, they can also be set-up to allow patients to reach physicians directly, adding to pediatrician's workload—a feature that has been shown to increase burnout. 14 Organizations have started to address this issue. Reliant Medical Group reduced physician inbox messages by 25% through rules that routed new messages to the appropriate staff or team member. 36
A recent AAP policy statement highlighted the different electronic documentation needs for pediatricians and a lack of best practices in pediatric populations. 35 It points out that “[m]ultiple stakeholders with differing priorities […] have contributed to increased documentation burden and physician burnout.” It also discusses several tools to reduce provider documentation burden, including speech recognition software, scribes, and new technologies. Half of our study participants thought adding a scribe to the team would help reduce documentation burden but only 6% reported using a scribe. While these participants had high ratings of their scribes, we found mixed results in the qualitative data, with cost and workflow being raised as issues. The Centers for Medicare and Medicaid Services (CMS) and American Medical Association (AMA) are working on changes to decrease administrative documentation burdens and credit providers for the total time spent on outpatient encounters including previsit (e.g., chart review; paperwork, forms, and letters) and postvisit (e.g., laboratory review) time, in addition to patient care, if they all occur on the same day. 37
Limitations
Study limitations include that data are self-reported and limited to early and midcareer pediatricians. Generalizability of findings to other specialties or career stages remains unclear. Although the response rate to the study survey was high, the initial project sign-up rate was 41%. 15 We made efforts to account for nonresponse bias by using a data-weighting procedure. Although PLACES is a longitudinal study, the data presented in the current study are from one year (2018) and therefore do not permit an understanding of cause and effect. For example, it is possible that being stressed about work–life balance makes documentation feel more burdensome. We did not collect data on EHR vendors, implementation, and training and support for physicians, which may have rendered some EHRs more useable for physicians than others. In addition, questions on overall categories of administrative burdens (e.g., EHR documentation; billing, preauthorization, and other insurance; quality and performance measurement) and approaches that might reduce administrative tasks (e.g., shift administrative work to other team members; improve the functionality of the EHR) were broad to understand which general types of tasks were most burdensome for pediatricians and overall solutions, respectively. Future work might focus on which EHR tasks could be successfully shifted to other team members and specific input pediatricians would like to have regarding EHRs. Also, this survey was conducted before the CMS and AMA coding and documentation changes went into effect at the beginning of 2021. 37 Lastly, the global pandemic in 2020 may have impacted pediatrician perspectives since we conducted our survey.
Conclusion
In summary, our study documented that three in four early and midcareer pediatricians are highly burdened by EHR documentation and these pediatricians struggle with work–life balance and are less satisfied in their careers and overall life. Nine in 10 participants felt that EHR burden would be improved with increased EHR functionality, protected time for administrative tasks, shifting tasks to other team members, and obtaining physician input. A multifactorial approach is needed to successfully reduce the burden, including improved functionality by EHR vendors and at the local level and continued advocacy by pediatricians to ensure input and feedback.
Clinical Relevance Statement
In our survey, 73.6% of pediatricians surveyed reported being highly burdened by EHR documentation. Pediatricians experiencing higher burden also reported more work–life balance issues and less career satisfaction. Nine in 10 believed improving EHR functionality would reduce administrative tasks for physicians.
Multiple Choice Questions
-
Which type of administrative task is most commonly reported by early and midcareer pediatricians as being burdensome?
Billing and insurance.
EHR documentation.
Laboratory result inquiries.
Quality and performance measurement.
Correct Answer: The correct answer is option b. Three-quarters of pediatricians (73.6%) reported EHR documentation was a major or moderate burden. Half (49.0%) reported such burden for billing and insurance and 42.7% for quality and performance measurement (QI). Majorities of general pediatricians (74.5%), subspecialists (75.3%), and hospitalists (62.3%) reported that EHR documentation was a major or moderate burden.
-
Which of the following measures were found to be negatively associated with moderate to severe EHR documentation burden on pediatrician?
Life satisfaction; work–life balance; career satisfaction.
Work–life balance; pediatrician income; patient volume.
Career satisfaction; vacation time; office staff work satisfaction.
None was negatively associated.
Correct Answer: The correct answer is option a. In multivariable analysis, controlling for pediatrician characteristics, pediatricians reporting more EHR documentation burden were more likely to be stressed balancing work and personal responsibilities and to bring work home daily (adjusted odds ratio [aOR] = 3.79, 95% confidence interval [CI] = 2.76–5.19 and aOR = 3.05, 95% CI = 2.08–4.47, respectively). They reported less satisfaction with personal time (aOR = 0.43, 95% CI = 0.32–0.59), career (aOR = 0.63, 95% CI = 0.41–0.98), and life overall (aOR = 0.49, 95% CI = 0.35–0.69). EHR burden was related to five measures of work–life balance and satisfaction and was a bigger factor in the models than any of the pediatrician characteristics.
Acknowledgments
We would like to acknowledge the contribution of the PLACES participants.
Funding Statement
Funding This study was supported by the American Academy of Pediatrics. The research presented in this article is that of the authors and does not reflect the official policy of the American Academy of Pediatrics.
Conflict of Interest None declared.
Protection of Human and Animal Subjects
The study was performed in compliance with the World Medical Association Declaration of Helsinki on Ethnical Principles for Medical Research Involving Human Subjects and was reviewed and approved by the AAP Institutional Review Board.
References
- 1.Henry J, Pylypchuk Y, Searcy T, Vaishali P.(May 2016). Adoption of Electronic Health Record Systems among U.S. Non-Federal Acute Care Hospitals: 2008–2015. ONC Data Brief, no.35 Office of the National Coordinator for Health Information Technology; Washington DC: 2016. Accessed July 5, 2021 at:https://dashboard.healthit.gov/evaluations/data-briefs/non-federal-acute-care-hospital-ehr-adoption-2008-2015.php#:~:text=Nearly%20all%20reported%20hospitals%20(96,increased%20by%2011%25%20from%202014
- 2.Lehmann C U, O'Connor K G, Shorte V A, Johnson T D. Use of electronic health record systems by office-based pediatricians. Pediatrics. 2015;135(01):e7–e15. doi: 10.1542/peds.2014-1115. [DOI] [PubMed] [Google Scholar]
- 3.Temple M W, Sisk B, Krams L A, Schneider J H, Kirkendall E S, Lehmann C U. Trends in use of electronic health records in pediatric office settings. J Pediatr. 2019;206:16400–17100. doi: 10.1016/j.jpeds.2018.10.039. [DOI] [PubMed] [Google Scholar]
- 4.Lehmann C U, Kressly S J.Commentary: a call to modernize CMS evaluation and management coding requirements. AAP NewsPublished online September 17, 2020. Accessed September 23, 2020 at:https://www.aappublications.org/news/2017/05/23/Commentary052317
- 5.Tsou A Y, Lehmann C U, Michel J, Solomon R, Possanza L, Gandhi T. Safe practices for copy and paste in the EHR. Systematic review, recommendations, and novel model for Health IT collaboration. Appl Clin Inform. 2017;8(01):12–34. doi: 10.4338/ACI-2016-09-R-0150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sittig D F, Wright A, Ash J, Singh H. New unintended adverse consequences of electronic health records. Yearb Med Inform. 2016;10(01):7–12. doi: 10.15265/IY-2016-023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Krist A H, Beasley J W, Crosson J C. Electronic health record functionality needed to better support primary care. J Am Med Inform Assoc. 2014;21(05):764–771. doi: 10.1136/amiajnl-2013-002229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shanafelt T D, Dyrbye L N, Sinsky C. Relationship between clerical burden and characteristics of the electronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. 2016;91(07):836–848. doi: 10.1016/j.mayocp.2016.05.007. [DOI] [PubMed] [Google Scholar]
- 9.Sinsky C, Colligan L, Li L. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016;165(11):753–760. doi: 10.7326/M16-0961. [DOI] [PubMed] [Google Scholar]
- 10.Arndt B G, Beasley J W, Watkinson M D. Tethered to the EHR: primary care physician workload assessment using EHR event log data and time-motion observations. Ann Fam Med. 2017;15(05):419–426. doi: 10.1370/afm.2121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Saag H S, Shah K, Jones S A, Testa P A, Horwitz L I. Pajama time: working after work in the electronic health record. J Gen Intern Med. 2019;34(09):1695–1696. doi: 10.1007/s11606-019-05055-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gregory M E, Russo E, Singh H. Electronic health record alert-related workload as a predictor of burnout in primary care providers. Appl Clin Inform. 2017;8(03):686–697. doi: 10.4338/ACI-2017-01-RA-0003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Murphy D R, Meyer A ND, Russo E, Sittig D F, Wei L, Singh H. The burden of inbox notifications in commercial electronic health records. JAMA Intern Med. 2016;176(04):559–560. doi: 10.1001/jamainternmed.2016.0209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hilliard R W, Haskell J, Gardner R L. Are specific elements of electronic health record use associated with clinician burnout more than others? J Am Med Inform Assoc. 2020;27(09):1401–1410. doi: 10.1093/jamia/ocaa092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Frintner M P, Cull W L, Byrne B J. A longitudinal study of pediatricians early in their careers: PLACES. Pediatrics. 2015;136(02):370–380. doi: 10.1542/peds.2014-3972. [DOI] [PubMed] [Google Scholar]
- 16.American Academy of Pediatrics Pediatrician Life and Career Experience Study (PLACES) AAP.orgAccessed December 17, 2019. Accessed July 5, 2021 at:http://www.aap.org/en-us/professional-resources/Research/pediatrician-surveys/Pages/Pediatrician-Life-And-Career-Experience-Study-PLACES.aspx
- 17.Starmer A J, Frintner M P, Freed G L. Work-life balance, burnout, and satisfaction of early career pediatricians. Pediatrics. 2016;137(04):e20153183. doi: 10.1542/peds.2015-3183. [DOI] [PubMed] [Google Scholar]
- 18.Katakam S K, Frintner M P, Pelaez-Velez C, Chakraborty R. Work experiences and satisfaction of international medical school graduates. Pediatrics. 2019;143(01):e20181953. doi: 10.1542/peds.2018-1953. [DOI] [PubMed] [Google Scholar]
- 19.Hsieh H-F, Shannon S E. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(09):1277–1288. doi: 10.1177/1049732305276687. [DOI] [PubMed] [Google Scholar]
- 20.Gupta K, Murray S G, Sarkar U, Mourad M, Adler-Milstein J.Differences in ambulatory EHR use patterns for male vs. female physicians. NEJM CatalPublished online November 13, 2019. Accessed December 15, 2020 at:https://catalyst.nejm.org/doi/full/10.1056/CAT.19.0690
- 21.Tait S D, Oshima S M, Ren Y. Electronic health record use by sex among physicians in an academic health care system. JAMA Intern Med. 2021;181(02):288–290. doi: 10.1001/jamainternmed.2020.5036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cull W L, Frintner M P, Starmer A J, Leslie L K. Longitudinal analyses of pediatrician burnout. Acad Pediatr. 2019;19(03):256–262. doi: 10.1016/j.acap.2018.11.006. [DOI] [PubMed] [Google Scholar]
- 23.Shanafelt T D, Hasan O, Dyrbye L N. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clin Proc. 2015;90(12):1600–1613. doi: 10.1016/j.mayocp.2015.08.023. [DOI] [PubMed] [Google Scholar]
- 24.Dyrbye L N, Burke S E, Hardeman R R. Association of clinical specialty with symptoms of burnout and career choice regret among US resident physicians. JAMA. 2018;320(11):1114–1130. doi: 10.1001/jama.2018.12615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Baptiste D, Fecher A M, Dolejs S C. Gender differences in academic surgery, work-life balance, and satisfaction. J Surg Res. 2017;218:99–107. doi: 10.1016/j.jss.2017.05.075. [DOI] [PubMed] [Google Scholar]
- 26.Jolly S, Griffith K A, DeCastro R, Stewart A, Ubel P, Jagsi R. Gender differences in time spent on parenting and domestic responsibilities by high-achieving young physician-researchers. Ann Intern Med. 2014;160(05):344–353. doi: 10.7326/M13-0974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Starmer A J, Frintner M P, Matos K, Somberg C, Freed G, Byrne B J. Gender discrepancies related to pediatrician work-life balance and household responsibilities. Pediatrics. 2019;144(04):e20182926. doi: 10.1542/peds.2018-2926. [DOI] [PubMed] [Google Scholar]
- 28.Dyrbye L N, Shanafelt T D, Balch C M, Satele D, Sloan J, Freischlag J. Relationship between work-home conflicts and burnout among American surgeons: a comparison by sex. Arch Surg. 2011;146(02):211–217. doi: 10.1001/archsurg.2010.310. [DOI] [PubMed] [Google Scholar]
- 29.Cassidy-Vu L, Beck K, Moore J B. Burnout in female faculty members. J Prim Care Community Health. 2017;8(02):97–99. doi: 10.1177/2150131916669191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Colletti L M, Mulholland M W, Sonnad S S. Perceived obstacles to career success for women in academic surgery. Arch Surg. 2000;135(08):972–977. doi: 10.1001/archsurg.135.8.972. [DOI] [PubMed] [Google Scholar]
- 31.Wald J S, Haque S N, Rizk S. Enhancing health IT functionality for children: the 2015 children's EHR format. Pediatrics. 2018;141(04):e20163894. doi: 10.1542/peds.2016-3894. [DOI] [PubMed] [Google Scholar]
- 32.Dufendach K, Eichenberger J, McPheeters M.Core Functionality in Pediatric Electronic Health Records [Internet] Rockville, MD: Agency for Healthcare Research and Quality (US)2015. Apr. Report No.: 15–EHC014-EF. PMID: 25950078; 2015 [PubMed] [Google Scholar]
- 33.Council on Clinical Information Technology . Lehmann C U. Pediatric aspects of inpatient health information technology systems. Pediatrics. 2015;135(03):e756–e768. doi: 10.1542/peds.2014-4148. [DOI] [PubMed] [Google Scholar]
- 34.Sutton D E, Fogel J R, Giard A S, Gulker L A, Ivory C H, Rosa A M. Defining an essential clinical dataset for admission patient history to reduce nursing documentation burden. Appl Clin Inform. 2020;11(03):464–473. doi: 10.1055/s-0040-1713634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.COUNCIL ON CLINICAL INFORMATION TECHNOLOGY . O'Donnell H C, Suresh S. Electronic documentation in pediatrics: the rationale and functionality requirements. Pediatrics. 2020;146(01):e20201682. doi: 10.1542/peds.2020-1682. [DOI] [PubMed] [Google Scholar]
- 36.Massachusetts Medical Society Changing the EHR from a liability to an asset to reduce physician burnout. The Reliant Medical Group StoryPublished April 2019. Accessed December 15, 2020 at:www.mhalink.org/MHADocs/Resources/2019/19-04-22PR_Changing_EHR_PhysBurnout_0119_FINAL.pdf
- 37.Centers for Medicare & Medicaid Services Reducing burden | CMS. Accessed January 28, 2021 at:https://www.cms.gov/About-CMS/Components/CPI/Reducing-Burden