

Abstract
Depression constitutes one of the greatest sources of morbidity and mortality for United States (U.S.) adolescents. Latinx are the fastest growing U.S. adolescent population, particularly in rural communities, and suffer from depression at higher rates than other racial/ethnic groups. Informed by community perspectives on adolescent health, we examined factors associated with depression among Latinx early adolescents in an agricultural community. We surveyed 599 predominantly Latinx 8th graders (12 to 15 years old) recruited from middle schools in Salinas, California. Depression was measured cross-sectionally with the Patient Health Questionnaire-8. Exposures included environmental, cultural, and family factors, assessed using validated measures. We used hierarchical logistic regression guided by Garcia Coll’s Model for the Study of Developmental Competencies in Minority Children to examine associations between protective factors within each domain and depression. Eighty-six of the 599 youth (14%) scored above the clinical threshold for depression, with higher prevalence among females (19%) than males (10%), p=0.001. Environmental (school connectedness and neighborhood social cohesion) and family factors were associated with a lower odds of depression (all p≤0.01). Increased language assimilation was associated with an increased odds of depression (p=0.007). Social cohesion in neighborhoods and family communication offered similarly strong protective associations with depression.
Keywords: depression, adolescent, Latinx, protective factors, schools, family
Introduction
The Latinx population is growing in all regions of the United States (U.S.), with Latinx youth projected to comprise almost one-third of US adolescents aged 10 to 19 years by 2050 (United States Department of Health and Human Services, 2016). Latinx youth experience more depressive symptoms and are at greater risk of attempting suicide than white or black youth (Kann et al., 2018). As among adolescents nationally, rates of depression in Latinx adolescents vary by sex with females experiencing higher rates than males (Scott, Wallander, & Cameron, 2015). Depression among Latinx youth may be further exacerbated by personal or family immigration status and barriers to care (Potochnick & Perreira, 2010; Raymond-Flesch, Siemons, Pourat, Jacobs, & Brindis, 2014). Rural and agricultural regions are among the fastest growing populations of Latinx and Latinx immigrants in the U.S. (Lichter, 2012), but little is known about the factors associated with risk of depression among youth in these communities and how they may differ from youth in large urban centers.
A Crecer: The Salinas Teen Health Study is a prospective cohort study designed to examine social and structural influences on the health and wellbeing of youth in Salinas, California, a small urban center in California’s agricultural central coast. The study was initiated in collaboration with community co-investigators to investigate the intersection of community violence and reproductive health among adolescents; however, our formative interviews with community advisors, parent groups, and educators highlighted the community’s concerns about adolescent mental health (Comfort, Raymond-Flesch, Auerswald, McGlone, Chavez, & Minnis, 2018) and stressors tied to community violence and other sources of structural disadvantage. Thus, this examination, motivated by community priorities for adolescent health needs, focuses on identifying promising directions for addressing mental health in early adolescence (Raymond-Flesch, Auerswald, McGlone, Comfort, & Minnis, 2017).
Model.
This analysis is guided by the Integrative Model for the Study of Developmental Competencies in Minority Children (Figure One) which postulates that the psychological development of minority children is a function of proximal (e.g., family) and distal (e.g., school, neighborhood) ecologies (Coll Garcia & Lamberty, 1996). According to this model each child begins with a particular social position defined by characteristics such as race/ethnicity, economic status and/or immigrant generation. Their social position is further influenced by promoting and inhibiting environments, such as schools and neighborhoods, as well as the effects of cultural adaptations, family, and individual factors that give rise to psychological development (Coll Garcia & Lamberty, 1996).
Social position.
Social position influences both proximal and distal factors within the Garcia Coll model. Parent education level is a measure of social position and proxy for socioeconomic status that is well documented to impact a variety of health outcomes for minority youth, including mental health (Larson, Russ, Crall, & Halfon, 2008). As noted above, another measure of social position, racial and ethnic minority status, is associated with higher rates of depression for Latinx youth (Kann et al., 2018). Specific to immigrant communities, research on the effects of immigrant generation on adolescent mental health is limited. The “immigrant paradox” or the hypothesis that Latinx, particularly first-generation immigrants, have a protective advantage for some health outcomes, has been widely described in some adult health conditions (Fuentes-Afflick, Hessol, & Pérez-Stable, 1999; Markides & Coreil, 1986). However, studies on the impact of immigrant generation on adolescent depression show mixed results (Cervantes, Padilla, Napper, & Goldbach, 2013; Harker, 2001; Perreira et al., 2019). Some data suggest that first generation adolescent immigrants may experience high rates of depression, while those who have been in the U.S. longer or who receive adequate support from family and teachers are less likely to experience depression (Potochnick & Perreira, 2010). In keeping with Garcia Coll’s description of social position as determined by race, social class, and ethnicity we incorporated immigrant generation as a facet of ethnicity.
Promoting and inhibiting environments: Neighborhoods.
Neighborhoods are environments outside of the home that Latinx youth navigate regularly and that have the potential to buffer the impact of social position on their wellbeing and reduce both internalizing and externalizing behaviors (White, Zeiders, & Safa, 2018). Supporting this, among urban Latinx adolescents higher rates of neighborhood belonging are associated with lower rates of depression (Maurizi, Ceballo, Epstein-Ngo, & Cortina, 2013; Donnelly et al., 2016; Vega, Ang, Rodriguez, & Finch, 2011). Higher levels of neighborhood social cohesion may protect Latinx adolescents by buffering youth from stressors that are associated with depression (Lee & Liechty, 2015; Lorenzo-Blanco et al., 2019; Nair, White, Roosa, & Zeiders, 2013). First generation immigrant youth may particularly benefit from living in more ethnically homogeneous neighborhoods (Roosa et al., 2009). Conversely higher levels of parent-reported neighborhood disorder as well as youth and parent reported neighborhood safety concerns are associated with higher levels of youth depressive symptoms (Behnke, Plunkett, Sands, & Bámaca-Colbert, 2011; Dawson et al., 2019). Importantly, none of these studies focused on the impact of neighborhood cohesion on Latinx adolescent mental health in rural or agricultural settings where neighborhood structure may markedly differ from urban settings, and few of these studies measure neighborhood cohesion from the youth’s perspective.
Promoting and inhibiting environments: Schools.
School is the primary place outside of the home where adolescents spend time. The school and neighborhood environments can interact as a result of economic resources and social conditions such as community violence to reduce academic achievement, but positive school climate may promote academic achievement (Ruiz, McMahon, & Jason, 2018; Boxer, Drawve, & Caplan, 2020). The school environment also has a complex relationship with depression symptoms for Latinx adolescents. While some factors within the school environment, such as concerns for safety, have been associated with higher levels of depression symptoms among Latinx adolescents, support within schools has been associated with lower depression symptoms for this group (Arora & Wheeler, 2018; Cupito, Stein, Gonzalez, & Supple, 2016; Scott et al., 2015; Maurizi, et al., 2013). Similarly, data from the National Longitudinal Study of Adolescent Health (Add Health) have demonstrated that higher school connectedness and perceptions of feeling cared for by teachers are associated with fewer depressive symptoms, though these associations are less protective for Latinx and Black youth than white youth (Joyce & Early, 2014). While the association between school connectedness and depression is well documented, no studies have focused on school connectedness and depression among rural Latinx adolescents.
Adaptive culture: Spirituality and church attendance.
In the wider literature religious beliefs and participation in religious activities are being examined with increasing frequency as potential protective factors for wellbeing and mental health (Koenig, 2009). Measures of religious engagement range from frequency of church attendance, to broader measures of spirituality, or the degree that spirituality-based beliefs influenced the respondent’s life, sometimes referred to as religious salience (“Positive Indicators Project: Spirituality,” 2018; Yonker, Schnabelrauch, & DeHaan, 2012). There is growing evidence that church attendance and even more so, spirituality, may reduce the risk of depressive symptoms in adolescents, though the effect appears weaker for minority adolescents than white adolescents in one recent meta-analysis (Scott et al., 2015; Yonker et al., 2012). Some studies suggest that religious engagement may moderate exposures to other risk factors for depression such as neighborhood socioeconomic disadvantage and community violence (Hull, Kilbourne, Reece, & Husaini, 2008; Scott et al., 2015). There remains a paucity of data about the relationship between spirituality or church attendance and depression for Latinx adolescents in rural communities.
Adaptive culture: Acculturation.
Garcia Coll and colleagues describe that adaptive cultural responses, “largely reflect culturally defined coping mechanisms to the demands placed by the promoting and inhibiting environments” (Coll Garcia & Lamberty, 1996). They note that these adaptive responses can include traditions and cultural legacies as well as the ways that groups adapt, including migration and acculturation. Acculturative stress is well documented to be associated with depression among Latinx adolescents (Perreira et al., 2019; Sirin, Ryce, Gupta, & Rogers-Sirin, 2013). The acculturation gap between parents and adolescents may further place youth at risk for depression (Nair, Roche, & White, 2018). Language assimilation is one long-standing measure of unidirectional acculturation which may be related to other factors influencing depression such as connectedness within community, school, and family (Stella, Huang, Schwalberg, Overpeck, & Kogan, 2003). We had particular interest in linguistic assimilation because youth in the formative phase of our work identified a lack of linguistic assimilation as a source of bullying and ostracism for new immigrants in the community. Here we use the Short Acculturation Scale for Hispanics (Marin, Sabogal, VanOss Marin, Otero-Sabogal, & Perez-Stable, 1987) to explore the relationship between linguistic assimilation and depression in rural adolescents.
Family.
The relationship between adolescent depression and family structure and function have been well studied for Latinx youth. Single parent families are associated with higher rates of depression for minority adolescents though this finding may be related to other factors such as childhood trauma associated with parental separation, economic constraints of a single-income household, or lack of adequate structural supports for single-parent families (Costello, Swendsen, Rose, & Dierker, 2008). Factors such as parental support, parental closeness, family cohesion (a component of familism), and family function, have been associated with lower depression symptom burden in single and dual parent households, though data are somewhat mixed (Arora & Wheeler, 2018; Costello, et al., 2008; Perreira et al., 2019; Scott et al., 2015). Parental support has been shown to decrease the risk of depressive symptoms for Latinx adolescents, even in the face of significant challenges such as migration (Potochnick & Perreira, 2010). Here we build on this work by exploring the association between depression and family structure through both traditional measures of family composition as well as factors more specific to families in rural communities such as parents working in agriculture or moving for work.
Multiple research questions guided our analysis, including: are school connectedness and neighborhood cohesion associated with lower risk of depression? Are adaptive cultural factors such as higher levels of spirituality, church attendance, or acculturation associated with lower risk of depression? Are family factors such as parental communication, monitoring, and presence in the home associated with lower risk of depression? Drawing from the Garcia Coll model contextualized in the literature above, we hypothesize that school connectedness, neighborhood cohesion, family function (communication, cohesion, parental monitoring), religion and spirituality will be associated with lower odds of depression while linguistic assimilation and female sex will be associated with higher odds of depression. We hypothesize that critical promoting environment factors, including school connectedness and neighborhood cohesion, will be associated with a lower odds of depression, independent of adaptive cultural and family factors. This analysis build on findings from our formative work (Raymond-Flesch, et al., 2017) to examine the relationships between social position (socioeconomic status and immigrant generation), promoting and inhibiting environments (neighborhoods and schools), adaptive cultural practices (spirituality, church attendance, and linguistic assimilation), family structure and function, and sex with depression in an understudied population of Latinx adolescents in a Californian agricultural community.
Methods
Study population and design.
This analysis includes baseline data from A Crecer. The primary goal of A Crecer is to identify protective factors that promote positive youth development as well as factors that heighten youth’s risk for violence and adverse sexual health outcomes during the transition from early to middle adolescence. The study cohort includes primarily Latinx youth recruited from all four of the public middle schools in Salinas, California. Between November 2015 and March 2017, our team enrolled 599 youth (approximately 150 per school), representing about one-third of the total eighth grade population of approximately 1,800 youth in the school district. Bilingual research assistants recruited participants using strategies developed in partnership with leadership at each school, with the study’s Community Advisory Board, and through our formative research (Comfort et al., 2018). These included approaching youth during lunchtime and through afterschool programs, classroom presentations, and presenting during school assemblies and meetings of established parent groups (“Cafecitos”). Eligible youth were in 8th grade, between 12 and 15 years old, spoke English or Spanish, and intended to live in Salinas for at least one year after enrollment. In accordance with A Crecer’s community-engaged approach and in partnership with community advisors in the Salinas Unified School District and Health Department, the study included youth of all racial and ethnic backgrounds to provide useful and representative data to our community partners. Questionnaires were interviewer-administered with data collected via computers, with sensitive topics assessed using audio computer-assisted self-interviewing. The study team obtained parent permission by telephone using a structured protocol. Adolescents provided written assent at the time of their baseline study visit. The Institutional Review Board at RTI approved the study procedures and consent documents (parent permission and youth assent). Participants received a $20 payment for the visit.
Study setting.
The Salinas Valley is at the heart of California’s agricultural central coast. The agricultural sector is the largest employer in the county. The city of Salinas is 77% Latinx (Deloitte and MIT, 2019). Migrants and immigrants make up 38% of the local population and 17% of the population lives below the federal poverty line (“Data USA: Salinas, CA,” 2019).
Measures.
Factors of child development hypothesized to be associated with depression were adapted from the Integrative Model for Developmental Competencies in Minority Children (Coll Garcia & Lamberty, 1996; Marks & Garcia Coll, 2018) (Figure 1).
Figure 1.
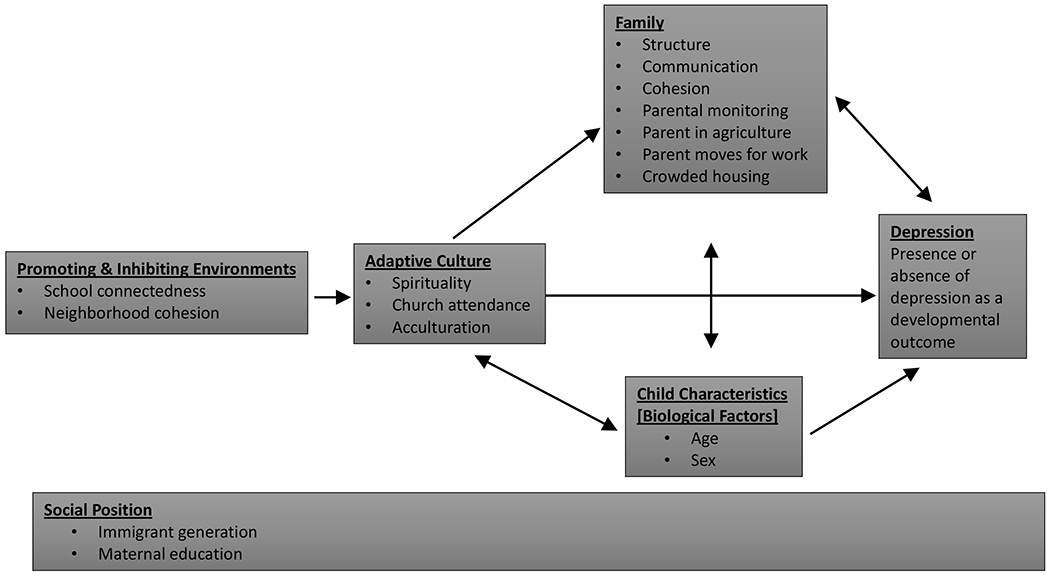
Factors influencing the Development of Depression, an Adapted Model of Developmental Competencies in Minority Children. Adapted from Garcia Coll, et al 1996. Bulleted factors are the measures specific to the A Crecer study chosen to represent each construct.
Outcome.
Depression was measured using the validated Patient Health Questionnaire-8 (PHQ-8) (Kroenke et al., 2009) with a score of ≥10 validated as correlated with the diagnosis of depression in national samples and Latinx populations (Alpizar, Plunkett, & Whaling, 2018; Kroenke et al., 2009). Established translations are available in English and Spanish. In addition, this brief 8-item version was selected to minimize participant burden, a particularly important consideration for this study’s young cohort. (Cronbach alpha, α=0.78).
Promoting and inhibiting environments: School connectedness and neighborhood cohesion.
We measured school connectedness using the 5-item scale from the National Longitudinal Study of Adolescent to Adult Health as well as 3-items to expand on the assessment of relationships with teachers (Bond et al., 2007; Resnick et al., 1997). The school connectedness score was created by taking the mean of the eight items (α=0.79). Neighborhood social cohesion was based on a 5-item subscale of a collective efficacy measure (Sampson, Raudenbush, & Earls, 1997) in which participants indicated agreement with each statement on a 4-point Likert scale. A composite score was created from the average of the five items (α=0.76). For both measures, higher scores indicate greater connectedness or cohesion.
Adaptive culture: Spirituality, church attendance, and language acculturation.
Religiosity consisted of two measures: frequency of religious service attendance in the past six months and spirituality. Attendance at church or other religious service was categorized as “never or rarely,” “about 1-2 times per month,” and “about once a week or more.” The 7-item Spirituality Scale for Adolescents (“Positive Indicators Project: Spirituality,” 2018) assessed to what degree spirituality-based beliefs influenced the respondent’s life on a 5-point Likert scale that ranged from 1 (“not at all”) to 5 (“completely”). The spirituality score was created by taking the mean of seven items (α=0.90).
The language acculturation measure was adapted from the Short Acculturation Scale for Hispanics (Marin, Sabogal, VanOss Marin, Otero-Sabogal, & Perez-Stable, 1987). The scale included 10-items, and responses were given on a 5-point bipolar scale from 1 (“only Spanish”) to 5 (“only English”), with 3 meaning “both equally.” Example questions included “what language(s) do you usually speak in your home?” and “in what language(s) do you think?” A composite score was created from the mean of the ten items (α=0.88), with a higher score indicating higher level of linguistic acculturation.
Family: Structure and support.
Family exposures included measures of both family structure and support from family members. Family structure included whether the participant lived with his/her mother or father (at least part-time), had a parent who worked in agriculture, and, in order assess parental migration for labor, we asked “Does your mother/father have to move during part of the year because of her/his job?” Crowded housing conditions were based on the US Census Bureau definition of more than one person per room in the home (Blake, Kellerson, & Simic, 2007). Family support was assessed using four measures: parental monitoring, maternal and paternal communication (assessed individually), and family cohesion. Parental monitoring was measured by three questions that asked youth to indicate how often parents “make sure they know who you are spending your time with,” “try to get to know who your friends are,” “make sure they know where you are when you are not in school” (Cottrell et al., 2007; Gorman-Smith, Henry, & Tolan, 2004). Response options ranged from 1 (“almost never”) to 4 (“almost always”). The parental monitoring score was created from the mean of these items (α=0.67). For the other three measures, participants indicated agreement with each item on a scale of 1 (“strongly disagree”) to 4 (“strongly agree”). Parent-adolescent communication was measured separately for fathers and mothers using 10-items that assess communication ease, parental attentiveness and satisfaction (Miller, Forehand, & Kotchick, 2000). Each score was created from the mean of the 10 items (α=0.84 and α=0.85, respectively). Family cohesion was measured using 6-items that assess emotional closeness, dependability and support (Tolan, Gorman-Smith, Huesmann, & Zelli, 1997). The score was created from the mean of six items (α=0.79). Higher scores on all three measures represent greater monitoring, stronger communication, and greater cohesion.
Child characteristics.
Participant’s age and sex were characteristics included in the conceptual model, for their known relationship with child development. Sex was determined by asking participants “What is your sex?”
Social position: Socioeconomic status, race/ethnicity, and immigrant generation.
The following sociodemographic characteristics described the study sample: maternal education level, government assistance in the past 6 months, food insecurity, ethnicity, immigrant generation, and years lived in the US. Immigrant generation was based on participants’ self-reported country of birth and his/her parents’ country of birth and categorized as 1st (participant not born in US), 2nd (participant born in US and at least one parent born outside US), or 3rd + (participant and both parents born in US). Likewise, ethnicity was based on self-identification and the participant’s parents’ and grandparents’ reported country of birth. Food insecurity was assessed for the past six months (Spanish-Language Current Population Survey Food Security Supplement, 2013).
Statistical analysis.
All measures were summarized using means and standard deviations (for continuous variables) or counts and percentages (for categorical variables). Cronbach alpha’s were calculated for each scale measure to assess its internal consistency and reliability. If a participant was missing a response to one of the scale items, the response was imputed using the average response of the other scale items. For each of the scale measures, there were fewer than 5 participants (<1%) with missing data. Participants who did not have contact with their father did not have a paternal communication score and were therefore not included in analyses with that measure; same for those without contact with their mother. We conducted preliminary analyses to explore the association between each measure of the conceptual model and depression using chi-square tests (categorical) or t-tests (continuous). We also explored correlations among measures of the conceptual model using Spearman rank correlation. Each measure was included in individual logistic regression models, adjusting for age and sex and controlling for recruitment school to account for the clustered structure of the data. Hierarchical logistic regression was then used to build successive regression models that examined associations between factors comprising each domain of the conceptual model and depression. Only variables with a p-value< 0.05 in the bivariable analyses were included in the final modelling (except for biological measures of age and sex which were included in all models). Factors were assessed by increasing proximity to the outcome, added as blocks based on domains in the Garcia Coll framework. Model 1 included promoting and inhibiting environments measures, then adaptive culture variables were added (model 2), and finally family measures (model 3). The Bonferroni correction was used to adjust for multiple tests, and a p-value < 0.003 was considered statistically significant. All analyses were performed using Stata 15.0 (StataCorp LP, College Station, Texas).
Results
The characteristics of the study sample (n=599) are described in Table 1. About half (53%) were female, most were aged 13 years (70%), and nearly all (94%) identified as Latinx. The majority were born in the United States (87%), primarily in Salinas, California (74%). Slightly more than half (53%) received government assistance in the past 6 months. Forty-two percent had a mother with less than high school education.
Table 1.
Characteristics of adolescents in 8th grade enrolled in A Crecer: The Salinas Teen Health Study, 2015-2017.
| Total | ||
|---|---|---|
| N | % | |
| Sociodemographic characteristics | 599 | (100) |
| Mean age, years (SD) | 13.2 | (1) |
| Female | 316 | (53) |
| Immigrant generation | ||
| 1st: born outside of the US | 71 | (12) |
| 2nd: US born/immigrant parents | 422 | (70) |
| 3rd+: US born and parents US born | 97 | (16) |
| US born; generation unknown | 9 | (2) |
| Latinxa | 566 | (94) |
| Mexican origin | 531 | (89) |
| Central American origin | 64 | (11) |
| Unknown origin | 20 | (3) |
| Years lived in US | ||
| Entire life | 525 | (88) |
| More than 5 years | 55 | (9) |
| 5 years or less | 19 | (3) |
| Mother’s education | ||
| Less than high school | 255 | (42) |
| High school/GED | 177 | (30) |
| More than high school | 149 | (25) |
| (Unknown) | 18 | (3) |
| Received government assistanceb past 6 months | 320 | (53) |
| At least one parent works in agriculture | 292 | (49) |
| Food insecurity (hunger) | 46 | (8) |
GED= general equivalency diploma; SD= standard deviation; US = United States
Percentages add to >100% as participants may have more than one origin
Includes Medi-Cal, unemployment benefits, food stamps
Depression: Primary developmental outcome.
Eighty-six of the 599 youth (14%; 95% confidence interval [CI]: 12%, 17%) scored above the threshold for depression, with two (<1%) scoring above the threshold for severe major depression. Depression was higher among females than males (19% vs. 10%, p=0.002). There was no statistically significant association with age. Spearman correlations for all exposures in the Garcia Coll model can be found in Table 2.
Table 2.
Spearman correlations between child development factors.
| School connectedness |
Neighborhood cohesion |
Language acculturation |
Church attendance |
Spirituality | Parental monitoring |
Maternal communication |
Family cohesion |
Paternal communication |
|
|---|---|---|---|---|---|---|---|---|---|
| School connectedness | 1.00 | ||||||||
| Neighborhood cohesion | 0.26 | 1.00 | |||||||
| Language acculturation | −0.04 | 0.07 | 1.00 | ||||||
| Church attendance | 0.16 | 0.12 | −0.15 | 1.00 | |||||
| Spirituality | 0.32 | 0.14 | −0.03 | 0.35 | 1.00 | ||||
| Parental monitoring | 0.18 | 0.10 | −0.04 | 0.13 | 0.19 | 1.00 | |||
| Maternal communication | 0.38 | 0.21 | 0.00b | 0.14 | 0.30 | 0.29 | 1.00 | ||
| Family cohesion | 0.38 | 0.24 | −0.06 | 0.18 | 0.40 | 0.31 | 0.57 | 1.00 | |
| Paternal communication a | 0.31 | 0.23 | 0.08 | 0.10 | 0.25 | 0.13 | 0.43 | 0.44 | 1.00 |
n=539
exact estimate: −0.0008
Environment.
The average school connectedness and neighborhood cohesion scores for those with and without depression are presented in Figure 2. On a scale of 1 to 4, with 4 meaning high connectedness or cohesion, those with depression had a lower average school connectedness score (3.3) and neighborhood cohesion score (2.8) compared to those without depression (mean scores 3.5 and 3.1, respectively). Indeed, higher school connectedness and neighborhood cohesion were associated with lower odds of depression (all p<0.001, Table 4). For each one-point increase in the school connectedness mean score, the odds of depression decreased 85% (95% CI: 71%, 92%). The odds of depression were 0.41 times lower for each one-point increase in neighborhood cohesion mean score (95% CI: 0.26, 0.65; p<0.001).
Figure 2.
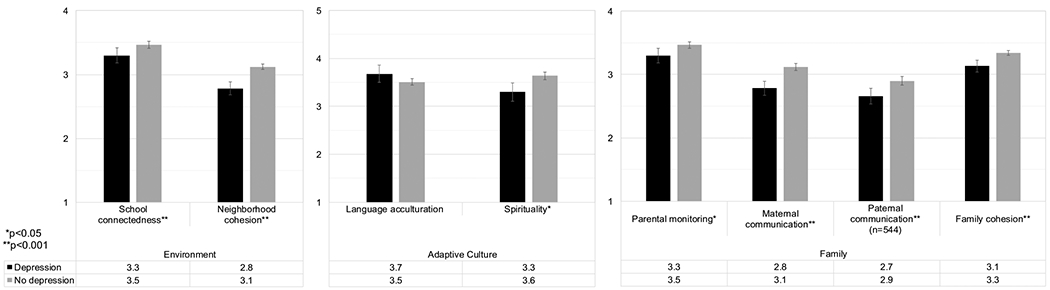
The mean, with 95% confidence interval, of child development factors by adolescents with and without current depression (N=599). Depression was assessed by PHQ-8 (score≥10); 1=low score. Mean differences tested using t-tests.
Table 4.
Estimating the association of each child development factor with depression; A Crecer: The Salinas Teen Health Study, 2015-2017 (n=599).
| Factor | OR | 95% CI | p-value | Adj ORa | 95% CI | p-value |
|---|---|---|---|---|---|---|
| Promoting and Inhibiting Environments | ||||||
| School connectedness (score 1-4) | 0.15 | (0.08, 0.28) | <0.001 | 0.15 | (0.08, 0.29) | <0.001 |
| Neighborhood cohesion (score 1-4) | 0.41 | (0.26, 0.64) | <0.001 | 0.41 | (0.26, 0.65) | <0.001 |
| Adaptive Culture | ||||||
| Language acculturation (score 1-5) | 1.39 | (1.02 - 1.90) | 0.04 | 1.48 | (1.08, 2.04) | 0.02 |
| Church attendance | 0.04 | 0.03 | ||||
| Never/rarely | Ref | - | - | Ref | - | - |
| About 1-2 times/month | 0.51 | (0.28, 0.94) | 0.03 | 0.48 | (0.26, 0.89) | 0.02 |
| About once a week or more | 0.60 | (0.35, 1.02) | 0.06 | 0.56 | (0.33, 0.97) | 0.04 |
| Spirituality (score 1-5) | 0.68 | (0.54, 0.86) | 0.002 | 0.67 | (0.52, 0.85) | 0.001 |
| Family | ||||||
| Parental monitoring (score 1-4) | 0.65 | (0.46, 0.92) | 0.01 | 0.58 | (0.41, 0.83) | 0.002 |
| Maternal communication (score 1-4) | 0.28 | (0.17, 0.44) | <0.001 | 0.30 | (0.19, 0.48) | <0.001 |
| Paternal communication (score 1-4)b | 0.42 | (0.27, 0.67) | <0.001 | 0.46 | (0.29, 0.73) | 0.001 |
| Family cohesion (score 1-4) | 0.35 | (0.21, 0.59) | <0.001 | 0.36 | (0.21, 0.61) | <0.001 |
| Lives with mother, at least part time | 0.69 | (0.22, 2.13) | 0.52 | |||
| Lives with father, at least part timeb | 1.24 | (0.71, 2.16) | 0.46 | |||
| At least one parent in agriculture | 0.65 | (0.40, 1.05) | 0.08 | |||
| At least one parent moves for work | 1.54 | (0.85, 2.77) | 0.15 | |||
| Crowded housing conditions | 0.77 | (0.48, 1.23) | 0.28 | |||
| Individual Characteristics | ||||||
| Age, years | 1.13 | 0.71 - 1.79 | 0.61 | |||
| Female | 2.19 | 1.34 - 3.57 | <0.001 | 2.20 | (1.35, 3.59) | 0.002 |
CI=confidence interval; OR=odds ratio
Each model adjusted for age and sex
Limited to participants who reported having contact with their father in the previous six months (n=544)
Adaptive culture.
The mean language acculturation score was 3.6, and the mean score was modestly higher among those with depression (Figure 2). Similarly, there was a trend in increased odds of depression with increased language acculturation scores (adjusted odds ratio 1.46, 95% CI: 1.06, 2.01), but this did not reach the level of statistical significance adjusted for multiple comparisons. Most youth (60%) reported attending religious services, either 1-2 times per month (26%) or at least once a week (34%), see Table 3. Regular religious service attendance was less common among youth who were depressed (52% of youth with depression never or rarely attended compared with 38% of those without depression, p=0.04). Spirituality mean scores were modestly higher among those without depression (3.6 versus 3.3, Figure 2), and having a higher spirituality-based belief mean score was associated with lower odds of depression (Adjusted odds ratio [AOR] 0.67, 95% CI: 0.52, 0.85, p=0.001; Table 4).
Table 3.
Distribution of factors of child development by current depression in adolescents enrolled in A Crecer: The Salinas Teen Health Study, 2015-2017.
| Depressiona | ||||||
|---|---|---|---|---|---|---|
| Yes | No | Total | ||||
| N | (%) | N | (%) | N | (%) | |
| 86 | (100) | 513 | (100) | 599 | (100) | |
| Adaptive Culture | ||||||
| Church attendance | ||||||
| Never/rarely | 45 | (52) | 197 | (38) | 242 | (40) |
| About 1-2 times/month | 17 | (20) | 139 | (27) | 156 | (26) |
| About once a week or more | 24 | (28) | 177 | (35) | 201 | (34) |
| Family | ||||||
| Lives with mother, at least part time | 82 | (95) | 498 | (97) | 580 | (97) |
| Lives with father, at least part timeb | 68 | (79) | 388 | (76) | 456 | (76) |
| At least one parent works in agriculture | 35 | (41) | 259 | (50) | 294 | (49) |
| At least one parent moves for work | 17 | (20) | 70 | (14) | 87 | (15) |
| Crowded housing conditionsc | 48 | (56) | 316 | (62) | 364 | (61) |
| Individual Characteristics | ||||||
| Female* | 59 | (69) | 257 | (50) | 316 | (53) |
GED= general equivalency diploma; SD= standard deviation; US = United States
Depression was measured using the PHQ-8, with a score >=10 indicating depression.
In total, 91% (n=544) had contact with their father currently
Definition per US Census Bureau as ≥1 person per room
p-value from Chi-square test <0.05
Family.
Nearly all participants (97%) lived with their mother at least part-time (Table 3). Three-quarters (76%) lived with their father at least part of the time, and 91% had contact currently. About half (49%) had at least one parent working in agriculture. There were no statistically significant associations between any family structure measures and depression (Table 4). As depicted in Figure 2, the mean scores for each family support factor (range 1 to 4) were higher for those without depression than for those youth who screened positive for depression. Likewise, the odds of depression were lower among participants with greater parental monitoring, stronger parent communication, and higher family cohesion (Table 4, all p<0.003). As evidenced by both the mean differences presented in Figure 2 and the adjusted odds ratios (Table 4), maternal communication appeared to exert the greatest protective association with depression among the family support measures evaluated (AOR 0.30, 95% CI: 0.19, 0.48, p<0.001).
Hierarchical regression.
Table 5 also presents the adjusted odds ratios from the multiple hierarchical logistic regression models. More distal measures such as school connectedness had a strong association with decreased odds of depression. There were also trends in associations across measures within each model domain, with neighborhood cohesion, language assimilation, and maternal communication associated with depression, although at a p≤0.01. Maternal communication was moderately correlated with school connectedness (Spearman’s rho 0.38, p<0.001) and parental monitoring (Spearman’s rho 0.29, p<0.001) and strongly correlated with family cohesion (Spearman’s rho 0.56, p<0.001) (Table 2).
Table 5.
Estimating the association of each child development factor with depression; A Crecer: The Salinas Teen Health Study, 2015-2017 (n=599).
| Individual Models | Hierarchical Modelling | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Model 1 | Model 2 | Model 3 | ||||||||||
|
| ||||||||||||
| Factor | Adj ORa | 95% CI | p-value | Adj ORa | 95% CI | p-value | Adj ORa | 95% CI | p-value | Adj ORa | 95% CI | p-value |
| Promoting and Inhibiting Environments | ||||||||||||
| School connectedness (score 1-4) | 0.15 | (0.08, 0.29) | <0.001 | 0.17 | (0.09, 0.32) | <0.001 | 0.19 | (0.10, 0.37) | <0.001 | 0.22 | (0.12, 0.43) | <0.001 |
| Neighborhood cohesion (score 1-4) | 0.41 | (0.26, 0.65) | <0.001 | 0.50 | (0.30, 0.82) | 0.006 | 0.49 | (0.30, 0.81) | 0.006 | 0.48 | (0.28, 0.81) | 0.007 |
| Adaptive Culture | ||||||||||||
| Language assimilation (score 1-5) | 1.48 | (1.08, 2.04) | 0.02 | 1.56 | (1.11, 2.20) | 0.01 | 1.63 | (1.15, 2.32) | 0.007 | |||
| Church attendance | 0.04 | 0.43 | 0.70 | |||||||||
| Never/rarely | Ref | - | - | Ref | - | - | ||||||
| About 1-2 times/month | 0.48 | (0.26, 0.89) | 0.02 | 0.65 | (0.33, 1.27) | 0.21 | 0.74 | (0.38, 1.47) | 0.39 | |||
| About once a week or more | 0.56 | (0.33, 0.97) | 0.04 | 0.86 | (0.47, 1.59) | 0.64 | 0.91 | (0.49, 1.69) | 0.76 | |||
| Spirituality (score 1-5) | 0.67 | (0.52, 0.85) | 0.001 | 0.85 | (0.64, 1.13) | 0.27 | 0.93 | (0.68, 1.27) | 0.64 | |||
| Family | ||||||||||||
| Parental monitoring (score 1-4) | 0.58 | (0.41, 0.83) | 0.002 | 0.88 | (0.57, 1.35) | 0.56 | ||||||
| Maternal communication (score 1-4) | 0.30 | (0.19, 0.48) | <0.001 | 0.47 | (0.26, 0.84) | 0.01 | ||||||
| Family cohesion (score 1-4) | 0.36 | (0.21, 0.61) | <0.001 | 1.12 | (0.55, 2.27) | 0.76 | ||||||
| Paternal communication (score 1-4)b | 0.46 | (0.29, 0.73) | 0.001 | |||||||||
| Lives with mother, at least part time | 0.67 | (0.21, 2.10) | 0.49 | |||||||||
| Lives with father, at least part timeb | 1.28 | (0.73, 2.25) | 0.39 | |||||||||
| At least one parent in agriculture | 0.64 | (0.39, 1.03) | 0.07 | |||||||||
| At least one parent moves for work | 1.53 | (0.84, 2.78) | 0.16 | |||||||||
| Crowded housing conditions | 0.75 | (0.47, 1.21) | 0.25 | |||||||||
| Individual Characteristics | ||||||||||||
| Age, years | 1.16 | (0.72, 1.87) | 0.54 | 1.09 | (0.66, 1.80) | 0.74 | 1.13 | (0.67, 1.89) | 0.64 | 1.13 | (0.67, 1.92) | 0.64 |
| Female | 2.20 | (1.35, 3.59) | 0.002 | 2.12 | (1.27, 3.56) | 0.004 | 2.31 | (1.36, 3.91) | 0.002 | 2.28 | (1.32, 3.94) | 0.003 |
CI=confidence interval; OR=odds ratio
Each model adjusted for age, sex, and recruitment school
Limited to participants who reported having contact with their father in the previous six months (n=544); not included in hierarchical modelling because of loss of sample
Discussion
This study adds to the limited literature about depression in the US’s growing population of rural Latinx youth. Guided by Garcia Coll’s model we assessed the contributions of environmental, cultural, and family factors to depression. In this large sample of predominantly Latinx youth from an agricultural community, 14% scored positive for depression, higher than national data for U.S. adolescents aged 13-14 (Merikangas et al., 2010). Distal environmental factors including school connectedness and neighborhood cohesion, as well as more proximal factors such as language assimilation and parental communication, were all associated with lower odds of depression in this understudied community
Promoting and inhibiting environments.
Environmental measures were associated with depression in all analyses. As anticipated, our findings indicate that school connectedness may be a particularly powerful protective factor for rural Latinx youth. This aligns with findings on the protective effects of school connectedness among urban Latinx youth (Arora & Wheeler, 2018; Cupito et al., 2016; Scott et al., 2015). These benefits extend from education to mental health. Latinx teens who are well connected in school are more likely to disclose suicidal ideation to an adult and seek adult help (De Luca & Wyman, 2012). Education literature suggests that collectivist cultural norms make school connectedness more critical for Latinx youth than their white peers (Espinoza & Juvonen, 2011). Latinx youth may particularly benefit from mentoring relationships with teachers, a finding that was also supported by our formative focus groups in the community (Raymond-Flesch, et al., 2017), and that has been shown to be of heightened benefit for Latinx youth relative to other racial or ethnic groups (Crosnoe, Johnson, & Elder Jr, 2004),. This suggests that future research could focus on developing and testing school-based interventions that promote adult mentoring and connection to peers to reduce the burden and sequela of depression among Latinx youth in immigrant, agriculture-based settings.
Higher neighborhood cohesion was also associated with lower odds of depression in our sample as we expected. This aligns with research showing that neighborhood cohesion is associated with lower rates of depression in urban Latinx populations (Donnelly et al., 2016; Vega et al., 2011). However, the structure and make up of neighborhoods in agricultural communities are markedly different from urban settings. The California Department of Housing (2020) notes that agricultural communities are characterized by high rates of poverty, extremely high levels overcrowding, and disproportionately poor housing conditions. The proportion of farmworkers living doubled-up with families has been increasing since 1990, giving rise to more children who are growing up in these adverse conditions (California Department of Housing & Community, 2020). It is possible that extended family networks and strong social ties in immigrant enclaves, which have been described in urban settings, are among the factors contributing to protective impacts of neighborhood cohesion (Cardoso & Thompson, 2010; Lee & Liechty, 2015; Roosa et al., 2009). Future research could further explore this hypothesis in rural settings.
Adaptive Culture.
Culture, in the form of religious activities and language use, influenced the odds of depression in our study. As expected and consistent with prior research, our analyses show that greater church participation and spirituality conferred some protection from depression, despite these factors not retaining statistical significance when adjusting for other factors across the model domains. Prior studies suggest that religious engagement may reduce depression among young Latinx (Fernandez & Loukas, 2014) but results vary (Lerman et al., 2018). In other immigrant populations church attendance can function as a form of social connection to adult role models and peers, both of which may be protective (Kang & Romo, 2011). For Latinx youth, it is possible that church attendance may particularly reinforce a collectivist culture, including reinforcing family ties through shared activity, but data on this remain sparse. In addition to facilitating external connections, church attendance may also increase spirituality, an internal resource which may improve psychological wellbeing among minority adolescents (Davis & Kiang, 2016; Kang & Romo, 2011). In our study spirituality was associated with lower odds of depression regardless of church attendance, suggesting that both church attendance and interventions that cultivate spirituality could be protective for Latinx youth.
As another measure of adaptive culture, participants with greater language assimilation trended towards having increased odds of depression. The relationship between language assimilation and depression is less clear. It is possible that the impact of language assimilation was not greater in our study due to the relatively small proportion of first-generation immigrants. Additionally, language assimilation may be a proxy for youth who are experiencing an acculturation gap, or the stress that arises due to different acculturation levels and cultural expectations between first generation immigrant parents and their second-generation children (Cervantes et al., 2013). For example, there is some data to suggest that immigrant children who speak a language other than English at home are more likely to feel unsupported by their parents or bullied at school (Stella et al., 2003). In this study our measure of acculturation was limited as it is unidimensionally focused on assimilation and does not capture other possible acculturation trajectories such as separation (rejection of the dominant culture) and biculturalism (Schwartz, Unger, Zamboanga, & Szapocznik, 2010). Research with these more nuanced measures of acculturation are likely to reveal a more complex relationship between acculturation and depression. Additionally, we lacked acculturation stress and acculturation gap measures to capture these phenomena in our sample. Acculturation stress is well demonstrated to be associated with depression in Latinx youth (Perreira et al., 2019; Sirin et al., 2013). Importantly, given US immigration patterns, acculturative stress is relatively rare among white youth which may contribute to the persistent disparity in depression rates between Latinx and White adolescents. Additional research on the Acculturation Gap and its relationship to adolescent individuation across different Latinx populations is needed to further understand the impact of these adaptive cultural factors on the mental health of Latinx adolescents.
Family.
As expected, in our study, adolescents with higher scores for each family support factor had lower odds of depression. Maternal communication appeared to contribute the greatest protective association. This finding is consistent with prior literature and supports our formative focus groups which identified the important role that parents play in Latinx adolescent development, as well as the promotion of educational engagement and healthful behaviors (Potochnick & Perreira, 2010; Scott et al., 2015; Raymond-Flesch et al., 2017). These results confirm that parents play a critical role in adolescent mental health and that protective interventions at the family or environmental level could enlist parental engagement in intervention development and implementation.
Overall our findings that connections with parents, schools, and neighborhoods have the potential to protect rural Latinx adolescents from depression are critical at this juncture as Latinx youth in immigrant communities are particularly vulnerable to immigration policy that aims to disrupt their ties to the family members, neighborhoods, and school through deportation and family separation. Nationally, 27% of youth are born to immigrant parents (Immigrant Children, 2018). The proportion of immigrants in agricultural communities like Salinas is even higher (“Data USA: Salinas, CA,” 2019). Recent policy changes to deportation priorities have broadened the scope of deportation efforts, increasing the potential to separate this large group of youth from their parents extended family members who support them (Artigiga & Ubri, 2017; Kelly, 2017). Children who do experience parental deportation or detention are well documented to be at risk for significant mental health morbidity including depression and post-traumatic stress disorder (Gulbas et al., 2016; Rojas-Flores, Clements, Hwang Koo, & London, 2017). Given the potential for family separation due to migration for work or deportation in communities like Salinas, it will be important to understand more about how to support youth who are experiencing or at risk for family separation due to forced migration or deportation. This analysis points to the supportive potential of neighborhoods and schools, highlighting opportunities to strengthen mental health outcomes through multiple avenues.
While our study adds to the limited literature about depression among Latinx youth in agricultural communities, there are several limitations. Our measure of depression, the PHQ-8, is a self-reported measure that asks participants to consider their depressive symptoms for the past two weeks and may underestimate prevalence of depression in this sample compared to other data sources, such as the National Survey on Drug Use and Health, which measures depression over the past year. Our data are cross sectional hence we could not assess causal relationships or test model pathways or mediators because of the inherent temporality limitations. Likewise, we could not assess the impact of the dynamic changes of adolescent development and acculturation over time. However, our conceptual model that guided analysis allowed for consideration of domains that reflected multi-level influences on depression. Future longitudinal examinations could extend this work by identifying the most influential domains and pathways through which they operate to affect mental health. Our sample is from a single geographic area and predominantly Mexican American, limiting generalizability. However, our sample’s ethnic profile is similar to other established migration destinations for agricultural work in California and other regions that receive predominantly Mexican migration flows and relevant to the rapidly growing populations of Latinx in rural communities around the country (Lichter, 2012), populations whose perceived access to health care and mental health has been shown to be affected by the current U.S. immigration policy environment (Callaghan et al., 2019; Eskenazi et al., 2019).
To address disparities in rates of depression for Latinx adolescents it is necessary to understand what factors are associated with lower levels of depression, particularly in understudied immigrant agricultural communities where Latinx populations are rapidly growing. This study suggests that it will be critical to continue to investigate how connections with neighborhood, school, and family can be strengthened to reduce the burden of depression for Latinx youth in agricultural communities, particularly given the potential disruption of these connections related to deportation of youth or their parents with shifting public and immigration policy environments. Our findings underscore the need to preserve youths’ safe and stable connections to family members and schools in order to preserve their health and wellbeing.
Contributor Information
Marissa Raymond-Flesch, University of California San Francisco, Department of Pediatrics, Division of Adolescent and Young Adult Medicine.
Erica N. Browne, RTI International, Women’s Global Health Imperative.
Colette Auerswald, University of California, Berkeley, School of Public Health, Division of Community Health Sciences.
Alexandra M. Minnis, RTI International, Women’s Global Health Imperative, And University of California, Berkeley School of Public Health.
References
- Alpizar D, Plunkett SW, & Whaling K (2018). Reliability and validity of the 8-item Patient Health Questionnaire for measuring depressive symptoms of Latino emerging adults. Journal of Latina/o Psychology, 6(2), 115–130. doi: 10.1037/lat0000087 [DOI] [Google Scholar]
- Arora PG, & Wheeler LA (2018). Depressive symptoms in Mexican-Origin adolescents: Interrelations between school and family contexts. Contemporary School Psychology, 22(3), 266–278. [Google Scholar]
- Artigiga S, & Ubri P (2017). Living in an Immigrant Family in America: How Fear and Toxic Stress are Affecting Daily Life, Well-Being, & Health. Retrieved from https://www.kff.org/report-section/living-in-an-immigrant-family-in-america-issue-brief/
- Behnke AO, Plunkett SW, Sands T, & Bámaca-Colbert MY (2011). The relationship between Latino adolescents’ perceptions of discrimination, neighborhood risk, and parenting on self-esteem and depressive symptoms. Journal of Cross-Cultural Psychology, 42(7), 1179–1197. [Google Scholar]
- Blake KS, Kellerson RL, & Simic A (2007). Measuring Overcrowding in Housing Bethesda, MD: Econometrica, Inc. Retrieved from https://www.census.gov/content/dam/Census/programs-surveys/ahs/publications/MeasuringOvercrowdinginHsg.pdf. [Google Scholar]
- Bond L, Butler H, Thomas L, Carlin J, Glover S, Bowes G, & Patton G (2007). Social and school connectedness in early secondary school as predictors of late teenage substance use, mental health, and academic outcomes. Journal of Adolescent Health, 40(4), 357 e359–318. doi: 10.1016/j.jadohealth.2006.10.013 [DOI] [PubMed] [Google Scholar]
- Boxer P, Drawve G and Caplan JM (2020), Neighborhood Violent Crime and Academic Performance: A Geospatial Analysis. American Journal of Community Psychology, 65: 343–352. [DOI] [PubMed] [Google Scholar]
- California Department of Housing & Community. (2020). Farmworkers. Retrieved from https://www.hcd.ca.gov/community-development/building-blocks/housing-needs/farmworkers.shtml and https://www.hcd.ca.gov/policy-research/specific-policy-areas/farmworkers.shtml
- Callaghan T, Washburn DJ, Nimmons K, Duchicela D, Gurram A, & Burdine J (2019). Immigrant health access in Texas: policy, rhetoric, and fear in the Trump era. BMC Health Services Research, 19(1), 342. doi: 10.1186/s12913-019-4167-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cardoso JB, & Thompson SJ (2010). Common themes of resilience among Latino immigrant families: A systematic review of the literature. Families in Society, 91(3), 257–265. [Google Scholar]
- Cervantes RC, Padilla AM, Napper LE, & Goldbach JT (2013). Acculturation-related stress and mental health outcomes among three generations of Hispanic adolescents. Hispanic Journal of Behavioral Sciences, 35(4), 451–468. [Google Scholar]
- Coll Garcia C, & Lamberty G (1996). An Integrative Model for the Study of Developmental Competencies in Minority Children. Child Development, 67(5), 1891–1914. doi: 10.2307/1131600 [DOI] [PubMed] [Google Scholar]
- Comfort M, Raymond-Flesch M, Auerswald C, McGlone L, Chavez M, & Minnis A (2018). Community-engaged Research with Rural Latino Adolescents: Design and Implementation Strategies to Study the Social Determinants of Health. Gateways: International Journal of Community Research & Engagement, 11(1), 90–108. 10.5130/ijcre.v11i1.5721 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costello DM, Swendsen J, Rose JS, & Dierker LC (2008). Risk and protective factors associated with trajectories of depressed mood from adolescence to early adulthood. Journal of Consulting and Clinical Psychology, 76(2), 173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cottrell SA, Branstetter S, Cottrell L, Harris CV, Rishel C, & Stanton BF (2007). Development and validation of a parental monitoring instrument: Measuring how parents monitor adolescents’ activities and risk behaviors. The Family Journal, 15(4), 328–335. [Google Scholar]
- Crosnoe R, Johnson MK, & Elder GH Jr (2004). Intergenerational bonding in school: The behavioral and contextual correlates of student-teacher relationships. Sociology of Education, 77(1), 60–81. [Google Scholar]
- Cupito AM, Stein GL, Gonzalez LM, & Supple AJ (2016). Familism and Latino adolescent depressive symptoms: The role of maternal warmth and support and school support. Cultural Diversity and Ethnic Minority Psychology, 22(4), 517. [DOI] [PubMed] [Google Scholar]
- Data USA: Salinas, CA. (2019). Deloitte and MIT.
- Davis RF, & Kiang L (2016). Religious identity, religious participation, and psychological well-being in Asian American adolescents. Journal of Youth and Adolescence, 45(3), 532–546. [DOI] [PubMed] [Google Scholar]
- Dawson CT, Wu W, Fennie KP, Ibañez G, Cano MÁ, Pettit JW, & Trepka MJ (2019). Parental-perceived neighborhood characteristics and adolescent depressive symptoms: A multilevel moderation analysis. Journal of Community Psychology, 47(7), 1568–1590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Luca SM, & Wyman P (2012). Association between school engagement and disclosure of suicidal ideation to adults among Latino adolescents. The Journal of Primary Prevention, 33(0), 99–110. doi: 10.1007/s10935-012-0269-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donnelly L, McLanahan S, Brooks-Gunn J, Garfinkel I, Wagner BG, Jacobsen WC, Gaydosh L (2016). Cohesive neighborhoods where social expectations are shared may have positive impact on adolescent mental health. Health Affairs, 35(11), 2083–2091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eskenazi B, Fahey CA, Kogut K, Gunier R, Torres J, Gonzales NA, Deardorff J (2019). Association of Perceived Immigration Policy Vulnerability With Mental and Physical Health Among US-Born Latino Adolescents in California. JAMA Pediatrics. doi: 10.1001/jamapediatrics.2019.1475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Espinoza G, & Juvonen J (2011). Perceptions of the school social context across the transition to middle school: Heightened sensitivity among Latino students? Journal of Educational Psychology, 103(3), 749. [Google Scholar]
- Fernandez A, & Loukas A (2014). Acculturation and Religious Coping as Moderators of the Association Between Discrimination and Depressive Symptoms Among Mexican-American Vocational Students. Journal of Immigrant and Minority Health / Center for Minority Public Health, 16(6), 1290–1293. doi: 10.1007/s10903-013-9952-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuentes-Afflick E, Hessol NA, & Pérez-Stable EJ (1999). Testing the epidemiologic paradox of low birth weight in Latinos. Archives of Pediatrics & Adolescent Medicine, 153(2), 147–153. [DOI] [PubMed] [Google Scholar]
- Gorman-Smith D, Henry DB, & Tolan PH (2004). Exposure to community violence and violence perpetration: The protective effects of family functioning. Journal of Clinical Child and Adolescent Psychology, 33(3), 439–449. [DOI] [PubMed] [Google Scholar]
- Gulbas LE, Zayas LH, Yoon H, Szlyk H, Aguilar-Gaxiola S, & Natera G (2016). Deportation experiences and depression among U.S. citizen-children with undocumented Mexican parents. Child: Care, Health and Development, 42(2), 220–230. doi: 10.1111/cch.12307 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harker K (2001). Immigrant generation, assimilation, and adolescent psychological well-being. Social Forces, 79(3), 969–1004. [Google Scholar]
- Hull P, Kilbourne B, Reece M, & Husaini B (2008). Community involvement and adolescent mental health: Moderating effects of race/ethnicity and neighborhood disadvantage. Journal of Community Psychology, 36(4), 534–551. [Google Scholar]
- Immigrant Children. (2018). Retrieved from https://www.childtrends.org/indicators/immigrant-children
- Joyce HD, & Early TJ (2014). The impact of school connectedness and teacher support on depressive symptoms in adolescents: A multilevel analysis. Children and Youth Services Review, 39, 101–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kang PP, & Romo LF (2011). The role of religious involvement on depression, risky behavior, and academic performance among Korean American adolescents. Journal of Adolescence, 34(4), 767–778. [DOI] [PubMed] [Google Scholar]
- Kann L, McManus T, Harris W, Shanklin S, Flint K, Queen B, … Ethier K (2018). Youth risk behavior surveillance — United States, 2017. Morbidity and Mortality Weekly Report, 67(8), 1–114. doi: 10.15585/mmwr.ss6708a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelly J (2017). Enforcemen of the Immigration Laws to Serve the National Interest Washington, D.C. Retrieved from https://www.dhs.gov/sites/default/files/publications/170220S1Enforcement-of-the-Immigration-Laws-to-Serve-the-National-Interest.pdf.
- Koenig HG (2009). Research on religion, spirituality, and mental health: A review. The Canadian Journal of Psychiatry, 54(5), 283–291. [DOI] [PubMed] [Google Scholar]
- Kroenke K, Strine TW, Spitzer RL, Williams JB, Berry JT, & Mokdad AH (2009). The PHQ-8 as a measure of current depression in the general population. Journal of Affective Disorders, 114(1–3), 163–173. doi: 10.1016/j.jad.2008.06.026 [DOI] [PubMed] [Google Scholar]
- Larson K, Russ SA, Crall JJ, & Halfon N (2008). Influence of multiple social risks on children’s health. Pediatrics, 121(2), 337–344. [DOI] [PubMed] [Google Scholar]
- Lee M-J, & Liechty JM (2015). Longitudinal associations between immigrant ethnic density, neighborhood processes, and Latino immigrant youth depression. Journal of Immigrant and Minority Health, 17(4), 983–991. [DOI] [PubMed] [Google Scholar]
- Lerman S, Jung M, Arredondo EM, Barnhart JM, Cai J, Castañeda SF, … Kaplan RC (2018). Religiosity prevalence and its association with depression and anxiety symptoms among Hispanic/Latino adults. PLoS ONE, 13(2), e0185661. doi: 10.1371/journal.pone.0185661 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lichter DT (2012). Immigration and the New Racial Diversity in Rural America. Rural Sociology, 77(1), 3–35. doi: 10.1111/j.1549-0831.2012.00070.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorenzo-Blanco EI, Meca A, Unger JB, Szapocznik J, Cano MÁ, Des Rosiers SE, & Schwartz SJ (2019). Cultural stress, emotional well-being, and health risk behaviors among recent immigrant Latinx families: the moderating role of perceived neighborhood characteristics. Journal of Youth and Adolescence, 48(1), 114–131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marin G, Sabogal F, VanOss Marin B, Otero-Sabogal F, & Perez-Stable EJ (1987). Development of a short acculturation scale for Hispanics. Hispanic Journal of Behavioral Sciences, 9, 183–205. [Google Scholar]
- Markides KS, & Coreil J (1986). The health of Hispanics in the southwestern United States: an epidemiologic paradox. Public Health Reports, 101(3), 253. [PMC free article] [PubMed] [Google Scholar]
- Marks AK, & Garcia Coll C (2018). Education and developmental competencies of ethnic minority children: Recent theoretical and methodological advances. Developmental Review, 50, 90–98. doi: 10.1016/j.dr.2018.05.004 [DOI] [Google Scholar]
- Maurizi LK, Ceballo R, Epstein-Ngo Q, & Cortina KS (2013). Does neighborhood belonging matter? examining school and neighborhood belonging as protective factors for latino adolescents. American Journal of Orthopsychiatry, 83(2-3), 323–334. [DOI] [PubMed] [Google Scholar]
- Merikangas KR, He J, Burstein M, Swanson SA, Avenevoli S, Cui L, … Swendsen J (2010). Lifetime Prevalence of Mental Disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry, 49(10), 980–989. doi: 10.1016/j.jaac.2010.05.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller K, Forehand R, & Kotchick B (2000). Adolescent sexual behavior in two ethnic minority groups: a multisystem perspective. Adolescence, 35(138), 313–333. [PubMed] [Google Scholar]
- Nair RL, Roche KM, & White RM (2018). Acculturation gap distress among Latino youth: Prospective links to family processes and youth depressive symptoms, alcohol use, and academic performance. Journal of Youth and Adolescence, 47(1), 105–120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nair RL, White RM, Roosa MW, & Zeiders KH (2013). Cultural stressors and mental health symptoms among Mexican Americans: A prospective study examining the impact of the family and neighborhood context. Journal of Youth and Adolescence, 42(10), 1611–1623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perreira KM, Marchante AN, Schwartz SJ, Isasi CR, Carnethon MR, Corliss HL, Van Horn L (2019). Stress and resilience: key correlates of mental health and substance use in the Hispanic community health study of Latino youth. Journal of Immigrant and Minority Health, 21(1), 4–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Positive Indicators Project: Spirituality. (2018). Retrieved from https://www.childtrends.org/research/research-by-topic/positive-indicators-project/spirituality/
- Potochnick SR, & Perreira KM (2010). Depression and Anxiety Among First-Generation Immigrant Latino Youth: Key Correlates and Implications for Future Research. The Journal of Nervous and Mental Disease, 198(7), 470–477. doi: 10.1097/NMD.0b013e3181e4ce24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raymond-Flesch M, Auerswald C, McGlone L, Comfort M, & Minnis A (2017). Building social capital to promote adolescent wellbeing: a qualitative study with teens in a Latino agricultural community. BMC Public Health, 17(1), 177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raymond-Flesch M, Siemons R, Pourat N, Jacobs K, & Brindis CD (2014). “There is no help out there and if there is, it’s really hard to find”: a qualitative study of the health concerns and health care access of Latino “DREAMers”. Journal of Adolescent Health, 55(3), 323–328. [DOI] [PubMed] [Google Scholar]
- Resnick MD, Bearman PS, Blum RW, Bauman KE, Harris KM, Jones J, … Udry JR (1997). Protecting adolescents from harm. Findings from the National Longitudinal Study on Adolescent Health. Journal of the American Medical Association, 278(10), 823–832. [DOI] [PubMed] [Google Scholar]
- Ruiz LD, McMahon SD, & Jason LA (2018). The role of neighborhood context and school climate in school-level academic achievement. American Journal of Community Psychology, 61(3-4), 296–309. [DOI] [PubMed] [Google Scholar]
- Trauma and psychological distress in Latino citizen children following parental detention and deportation, 9 C.F.R. (2017). [DOI] [PubMed]
- Roosa MW, Weaver SR, White RM, Tein J-Y, Knight GP, Gonzales N, & Saenz D (2009). Family and neighborhood fit or misfit and the adaptation of Mexican Americans. American Journal of Community Psychology, 44(1-2), 15–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sampson RJ, Raudenbush SW, & Earls F (1997). Neighborhoods and Violent Crime: A Multilevel Study of Collective Efficacy. Science, 277(5328), 918. doi: 10.1126/science.277.5328.918 [DOI] [PubMed] [Google Scholar]
- Schwartz SJ, Unger JB, Zamboanga BL, & Szapocznik J (2010). Rethinking the concept of acculturation: implications for theory and research. The American Psychologist, 65(4), 237–251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott SM, Wallander JL, & Cameron L (2015). Protective mechanisms for depression among racial/ethnic minority youth: Empirical findings, issues, and recommendations. Clinical Child and Family Psychology Review, 18(4), 346–369. [DOI] [PubMed] [Google Scholar]
- Sirin SR, Ryce P, Gupta T, & Rogers-Sirin L (2013). The role of acculturative stress on mental health symptoms for immigrant adolescents: A longitudinal investigation. Developmental Psychology, 49(4), 736. [DOI] [PubMed] [Google Scholar]
- Spanish-Language Current Population Survey Food Security Supplement. (2013). Washington, D.C. Retrieved from https://www.ers.usda.gov/media/8287/spanishversioncpsfss.pdf. [Google Scholar]
- Stella MY, Huang ZJ, Schwalberg RH, Overpeck M, & Kogan MD (2003). Acculturation and the health and well-being of US immigrant adolescents. Journal of Adolescent Health, 33(6), 479–488. [DOI] [PubMed] [Google Scholar]
- Tolan PH, Gorman-Smith D, Huesmann LR, & Zelli A (1997). Assessment of family relationship characteristics: a measure to explain risk for antisocial behavior and depression among urban youth. Psychological Assessment, 9(3), 212–222. [Google Scholar]
- United States Department of Health and Human Services. (2016). The Changing Face of America’s Adolescents. Retrieved from www.hhs.gov/ash/oah/facts-and-stats/changing-face-of-americas-adolescents/index.html
- Vega WA, Ang A, Rodriguez MA, & Finch BK (2011). Neighborhood protective effects on depression in Latinos. American Journal of Community Psychology, 47(1-2), 114–126. [DOI] [PubMed] [Google Scholar]
- White RMB, Zeiders KH, & Safa MD (2018). Neighborhood structural characteristics and mexican-origin adolescents’ development. Development and Psychopathology, 30(5), 1679–1698. [DOI] [PubMed] [Google Scholar]
- Yonker JE, Schnabelrauch CA, & DeHaan LG (2012). The relationship between spirituality and religiosity on psychological outcomes in adolescents and emerging adults: A meta-analytic review. Journal of Adolescence, 35(2), 299–314. [DOI] [PubMed] [Google Scholar]