

Abstract
OBJECTIVE:
To compare energy expenditure rates in children playing the physically active video games, Dance Dance Revolution (DDR) and Nintendo’s Wii Sports in relation to treadmill walking.
METHODS:
Energy expenditure, heart rate, step rate, and perceived exertion were measured in 14 boys and 9 girls (ages 10–13 years; BMI at 3–98th percentile for age and gender) while watching television at rest, playing DDR at 2 skill levels, playing Wii bowling and boxing, and walking at 2.6, 4.2, and 5.7 km/h. Arterial elasticity was measured at rest and immediately after gaming.
RESULTS:
Compared with watching television, energy expenditure while gaming or walking increased 2- to 3-fold. Similarly, high rates of energy expenditure, heart rate, and perceived exertion were elicited from playing Wii boxing, DDR level 2, or walking at 5.7 km/h. This occurred despite variations in step rate among activities, reflecting greater use of upper body during Wii play (lowest step rate) than during walking (highest step rate) or DDR play. Wii bowling and beginner level DDR elicited a 2-fold increase in energy expenditure compared to television watching. Large-artery elasticity declined immediately after both DDR and Wii. The change was inversely related to the increment in energy expenditure above rest achieved during the activity.
CONCLUSIONS:
Energy expenditure during active video game play is comparable to moderate-intensity walking. Thus, for children who spend considerable time playing electronic screen games for entertainment, physically active games seem to be a safe, fun, and valuable means of promoting energy expenditure.
Keywords: indirect calorimetry, video games, physical activity
The prevalence of overweight children in the United States, defined as those at >85th percentile of age- and gender-specific norms for BMI (kg/m2), has reached ~32%.1,2 Increased childhood adiposity is associated with a higher risk of developing adulthood obesity1 and metabolic complications such as type 2 diabetes.2 Obesity is often associated with low rates of physical activity and daily energy expenditure3 and time spent in sedentary activities such as watching television or working at a computer.4,5 Traditional exercise programs can be effective for making improvements in body composition,6 arterial elasticity,7 insulin sensitivity,8 and spontaneous physical activity9 in obese adolescents. Unfortunately, obese children are less likely to participate in traditional volitional exercise or sports programs than their healthy-weight peers.10
Recently, a new generation of video games that requires interactive physical activity, known as exergaming, has become popular. Exergaming could help some children increase their physical activity by integrating play with exercise. It was reported that a popular dance-simulation game, Dance Dance Revolution (DDR) (Konami Digital Entertainment, Redwood City, CA), increased energy expenditure in 10-year-olds to a level similar to low-to-moderate intensity (2.4 km/hour) walking.11 More importantly, energy expenditure during DDR was 172% greater than when watching television or playing traditional video games while seated. The newest commercially available active video game system, the Nintendo Wii (Nintendo, Redmond, WA), allows individuals to play simulated sports games and other activities by using handheld motion sensors. Although this new gaming device has been described in the lay media as a popular form of entertainment and has potential to provide an exercise stimulus, there is little information available on the physiologic responses to playing the Wii game system. Two small studies showed that adolescents expend ~50% more energy while playing the Wii sports-simulation games of tennis, boxing, and bowling than playing traditional video games.12,13 DDR and Wii games rely mainly on leg versus arm activity, respectively, but their impact on energy expenditure has not been compared. As the number of active game systems used by children increases, a more detailed assessment of physiologic responses to this form of activity is needed. Thus, the purpose of the current investigation was to use indirect calorimetry to compare the rates of energy expenditure in children playing 2 popular physically active video games, DDR and Wii Sports, in relation to walking. Physiologic and perceptual responses to these activities were also assessed by measuring heart rate (HR), arterial elasticity, and perceived exertion.
METHODS
Subjects
Twenty-three healthy children (14 boys, 9 girls) aged 10 to 13 years were recruited from the local community. Informed written consent and assent from the parent and child were obtained. The study was conducted under the approval of the University of Oklahoma’s institutional review board. A brief medical screening was performed before data collection. Body mass and body fat content were measured by using bioelectrical impedance (model BC-418 [Tanita, Arlington Heights, IL]), and height was measured to the nearest 0.5 cm. BMI (kg/m2) and age-adjusted percentile were calculated by using Centers for Disease Control and Prevention charts.14
Protocol and Procedures
Each child completed 2 visits to the laboratory within 4 weeks. Testing order was fixed with DDR performed on visit 1 and Wii play and treadmill walking performed on visit 2. Participants fasted except for water for 4 hours before arrival. Testing was performed in a well-lit room at consistent temperature (22°C–24°C) and relative humidity (45%–54%). Each visit began with an initial 20-minute rest phase, during which the child watched nonviolent cartoons while supine on a padded table with his or her head and shoulders supported by pillows. After the rest phase, the subjects played either the DDR (visit 1) or Wii (visit 2) games for 30 minutes.
DDR was performed by using the Sony Playstation 2 game system (Sony Computer Entertainment, San Marco, CA). The game requires participants to move their feet on a pressure-sensitive mat to match step patterns displayed on the television screen. Feedback is provided for matching timing and accuracy of footsteps. Participants selected a single song from the game menu for use during the entire session; song choices were from popular television shows familiar to the age group tested. The skill level was set to beginner (DDR1) for the first 15 minutes and basic (DDR2, higher rate of stepping versus DDR1) for the next 15 minutes. Approximately 1 to 2 minutes were taken between levels to reset the game and allow participants to take a drink of water if needed.
Wii gaming consisted of 15 minutes each of bowling and boxing from the Wii Sports package. A familiarization session was performed at the end of visit 1. Bowling and boxing games are played with handheld controllers that contain motion sensors to transmit player actions to an on-screen character. Each participant began his or her game session at the beginner skill level. Between the bowling and boxing games, a 1- to 2-minute break was allowed.
After completing the 30-minute game sessions, subjects returned to the resting position for 10 to 15 minutes for postactivity measurements of arterial elasticity. On visit 2, after the recovery period, participants walked on a motor-driven treadmill for 6 minutes at each of 3 velocities (2.6, 4.2, and 5.7 km/hour) while watching cartoons. Preliminary testing showed that these walking velocities were appropriate for children and would approximate the range of outcome responses measured during the gaming activities.
Throughout the study energy expenditure was measured by indirect calorimetry by using an expired breath analyzer (Ultima Cardi02 [Medgraphics, St Paul, MN]). A neoprene mask was worn over the mouth and nose with an open pneumotach for breath-by-breath analysis of expired ventilation and oxygen and carbon dioxide concentration. Certified gases were used for calibration before every test. HR was measured by using a surface electrode chest strap (Polar [PolarElectro Oy, Helsinki, Finland]) interfaced by telemetry with the metabolic measurement software. Footstep rate was recorded by using an accelerometer worn above the right ankle (StepWatch 3 [OrthoCare Innovations, Mountlake Terrace, WA]). During the gaming and walking phases the participants were asked to subjectively gauge their level of effort by using a standard Borg scale15 for rating of perceived exertion (RPE) (eg, 6 = very easy; 20 = very difficult). During the rest phases before and at 10 minutes after the gaming activities, blood pressure and arterial elasticity were measured in triplicate by using diastolic pulse waveform analysis (HDI/Pulsewave CR-2000 [Hypertension Diagnostics, Eagan, MN]). Arterial pulse waves were acquired by using a surface pressure transducer placed over the radial artery.
Statistical Analysis
Indirect calorimetry, HR, and step-rate data were collected at 30-second intervals and averaged over the last 6 minutes of the rest, DDR, and Wii phases and the last 4 minutes of each treadmill velocity. Repeated-measures analysis of variance was used to test the effects of exercise mode, time of measurement, and gender of the participant, with Bonferroni posthoc tests used to locate pairwise differences as appropriate. Comparisons of descriptive data according to gender were made by using Student’s t test. Associations between variables were measured by using Pearson’s correlations. For all tests, significance was accepted at P < .05. Summary data are presented as mean (SEM) except for subject characteristics as noted.
RESULTS
Participant characteristics are shown in Table 1. The mean height, weight, and BMI were within the normal range, although the BMI percentile range was 3% to 98%. On the basis of BMI category, most participants (n = 17) were considered healthy weight (5th–84th percentile), with 3 overweight (85th–94th percentile), 2 obese (≥95th percentile), and 1 underweight (<5th percentile).16 The only difference in physical characteristics between boys and girls was percent body fat, which was 6% higher in girls. Blood pressure and arterial elasticity values shown in Table 1 were recorded at rest before exercise; all subjects had normal resting blood pressure.17
TABLE 1.
Characteristics of Study Participants
| All (n = 23), Mean (SD) | Boys (n = 14), Mean (SD) | Girls (n = 9), Mean (SD) | |
|---|---|---|---|
| Age, y | 11.9 (1.2) | 11.9 (1.0) | 11.8 (1.5) |
| Height cm | 150.5 (8.9) | 150.9 (9.2) | 149.8 (8.9) |
| Weight kg | 43.4 (8.8) | 42.4 (9.6) | 44.8 (7.8) |
| BMI, kg/m2 | 19.1 (3.1) | 18.5 (3.4) | 19.9 (2.5) |
| BMI percentile | 54 (31) | 49 (35) | 62 (21) |
| Total body fat, % | 20.6 (6.2) | 18.1 (6.1) | 24.5 (4.0)a |
| Systolic blood pressure, mm Hg | 110 (8) | 110 (5) | 111 (11) |
| Diastolic blood pressure, mm Hg | 56 (6) | 57 (5) | 55 (7) |
| Large-artery elasticity, mL/mm Hg × 10 | 11.8 (2.7) | 11.9 (2.9) | 11.5 (2.6) |
| Small-artery elasticity, mL/mm Hg × 10 | 7.9 (2.2) | 8.4 (2.4) | 7.2 (2.0) |
Higher in girls than in boys (P < .01).
Energy expenditure adjusted for body mass is shown Fig 1. A similar response pattern was evident for energy expenditure expressed in kJ/min (data not shown). We opted to present energy expenditure relative to body mass because most activities were weight-bearing; therefore, body weight and energy expenditure were strongly associated (r = 0.71–0.86 for walking, r = 0.51–0.57 for DDR). The association between body weight and energy expenditure during bowling and boxing games was lower (r = 0.37–0.42), reflecting greater reliance on upper-body movement. Walking and exergaming resulted in significant elevations in energy expenditure (Fig 1), expired ventilation, , and HR (Table 2) compared with these measures for children watching television at rest. The highest rate of energy expenditure was recorded for DDR2 (3.3-fold increase above rest), although energy expenditure when playing the boxing game was nearly as high (2.9- and 3.3-fold increase above rest for boys and girls, respectively) and not different from DDR2. Walking at 5.7 km/hour elevated energy expenditure 3-fold on average, which was less than that for DDR2 (P < .05) but not boxing. For , the highest value was recorded during DDR2 (3.3-fold increase above rest on average), with lower values during boxing and walking at 5.7 km/hour (both 3.0-fold higher than rest). Ventilatory rate was not different during DDR2 versus boxing but higher during these activities than the other study phases. HR was higher during boxing than all other activities. RPE values were numerically highest during DDR2, while both the 5.7 km/hour walk and boxing were rated as 1 arbitrary unit lower (P < .05) and not different from one another. The highest step rates were recorded during walking, with all 3 walking velocities eliciting faster step rates than any of the gaming activities (Fig 2). Step rates were lowest when playing either of the Wii games.
FIGURE 1.
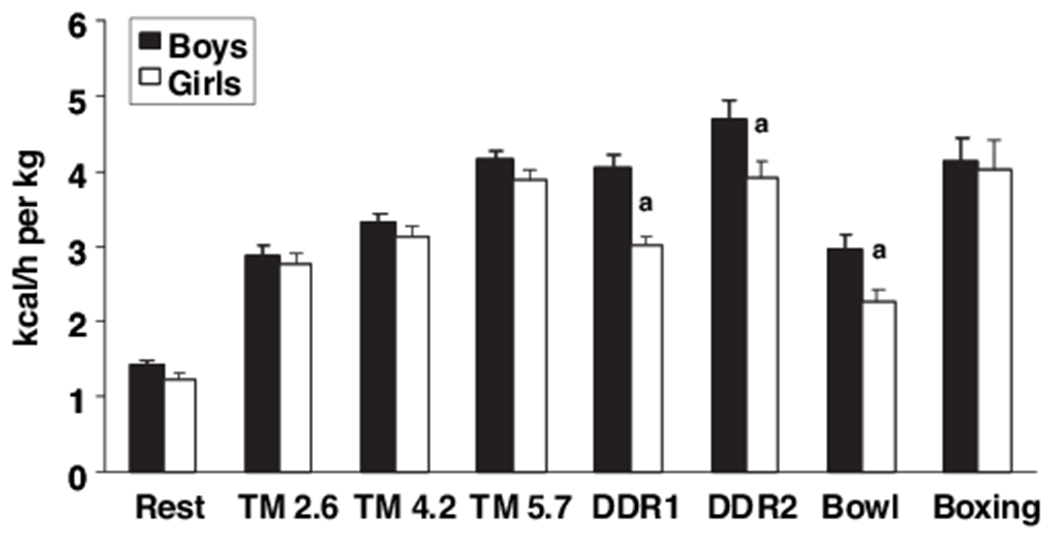
Energy expenditure at rest and during treadmill walking, DDR, and Wii bowling and boxing games. Treadmill (TM) walking velocities were 2.6, 4.2, and 5.7 km/hour, respectively. a Higher in boys than girls (P < .05).
TABLE 2.
HR, Expired Ventilatory Rate, Oxygen Uptake (), and RPE
| Rest | Treadmill, 2.6 km/h | Treadmill, 4.2 km/h | Treadmill, 5.7 km/h | DDR1 | DDR2 | Bowl | Boxing | |
|---|---|---|---|---|---|---|---|---|
| HR, bpm | ||||||||
| Boys | 66 (2) | 98 (3) | 102 (2) | 111 (2) | 111 (3) | 121 (4) | 101 (4) | 127 (5) |
| Girls | 69 (3) | 101 (4) | 105 (3) | 113 (3) | 106 (5) | 124 (6) | 98 (3) | 140 (8) |
| Expired ventilatory rate, L/min | ||||||||
| Boys | 6.3 (0.3) | 11.3 (0.7) | 12.9 (0.7) | 16.0 (0.7) | 15.9 (0.8) | 18.9 (1.0) | 11.9 (0.9) | 17.9 (1.4) |
| Girls | 5.8 (0.3) | 11.7 (0.7) | 13.2 (0.9) | 16.3 (0.9) | 13.0 (0.8)a | 17.6 (1.5) | 9.6 (0.5)a | 18.7 (1.9) |
| , mL/kg per min | ||||||||
| Boys | 4.8 (0.3) | 9.8 (0.5) | 11.2 (0.4) | 14.0 (0.4) | 13.7 (0.6) | 15.8 (0.9) | 10.0 (0.7) | 13.8 (1.1) |
| Girls | 4.1 (0.3) | 9.3 (0.5) | 10.5 (0.6) | 13.0 (0.5) | 10.2 (0.4)a | 13.2 (0.7)a | 7.7 (0.6)a | 13.5 (1.4) |
| RPE | ||||||||
| Boys | — | 8 (1) | 10 (1) | 12 (1) | 9 (1) | 13 (1) | 9 (1) | 12 (1) |
| Girls | — | 11 (1)a | 13 (1) | 15 (1) | 12 (1)a | 16 (1)a | 11 (1) | 15 (1)a |
Values shown are mean (SEM).
P < .05 between boys and girls.
FIGURE 2.
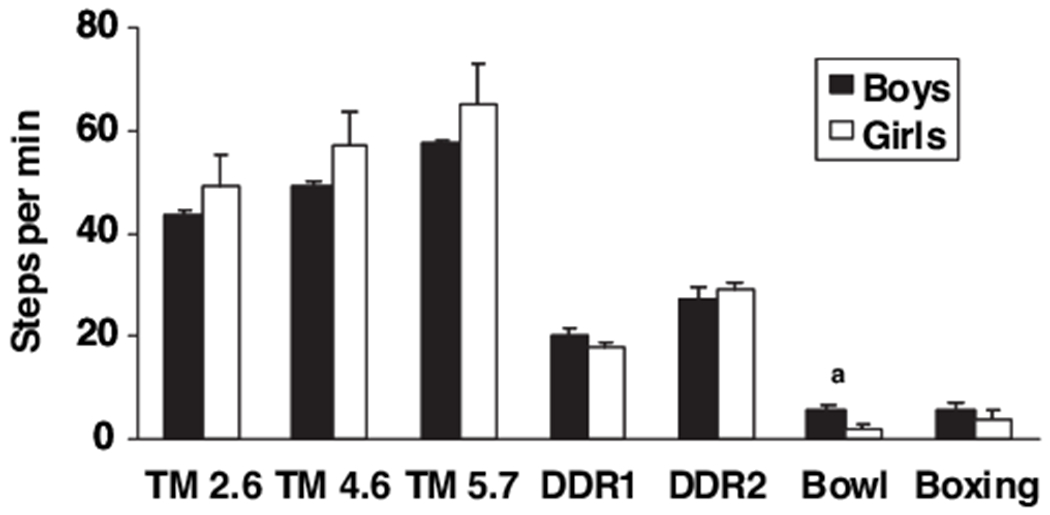
Step rate during treadmill walking, DDR, and Wii bowling and boxing games. Treadmill (TM) walking velocities were 2.6, 4.2, and 5.7 km/hour, respectively. a Higher in boys than girls (P < .05).
Data are presented separately for boys and girls because there were differential responses between genders for several outcomes. Energy expenditure was 19% to 33% higher (P < .05) for boys when playing DDR1, DDR2, and bowling. Similarly, was 20% to 34% higher in boys (P < .05) during DDR1, DDR2, and bowling, whereas ventilatory rate was ~22% higher in boys (P < .05) for DDR1 and bowling. In contrast, boys consistently reported lower RPE values, reaching significant differences (P < .05) during the 2.6 km/hour walk, DDR1, DDR2, and boxing or a trend to be lower (P < .08) for the other activities. However, HR did not differ between boys and girls during rest or any activity. The only significant difference between boys and girls for step rate was observed during the bowling game, with boys taking more than twice as many steps as girls (5.5 vs 2.4 steps/minute, respectively).
Systolic blood pressure increased significantly above the resting value (P < .01) after both the DDR (4 [2] mm Hg) and Wii (6 [1] mm Hg) game sessions, with trends (P < .07) for higher diastolic values after both game sessions (average increase of 2–4 mm). The average decrease in large-artery elasticity from baseline to postactivity was 17% (DDR) to 20% (Wii) (both P < .05) (Fig 3). This decline was greater in boys (25%) than girls (5%) after the DDR session (P < .02) but not after the Wii session (25% and 17% decline in girls and boys, respectively). The change in large-arterial elasticity was inversely associated with the increase in energy expenditure above rest during DDR2 (r = −0.52) and Wii boxing (r = −0.72), respectively. The average decline in small-artery elasticity was 18% after DDR (P < .05) and approached significance for boys only (P = .052). The average (for boys and girls combined) 9% decline in small-arterial elasticity after Wii gaming did not reach significance. There were no differences between boys and girls in small-arterial elasticity for either activity.
FIGURE 3.
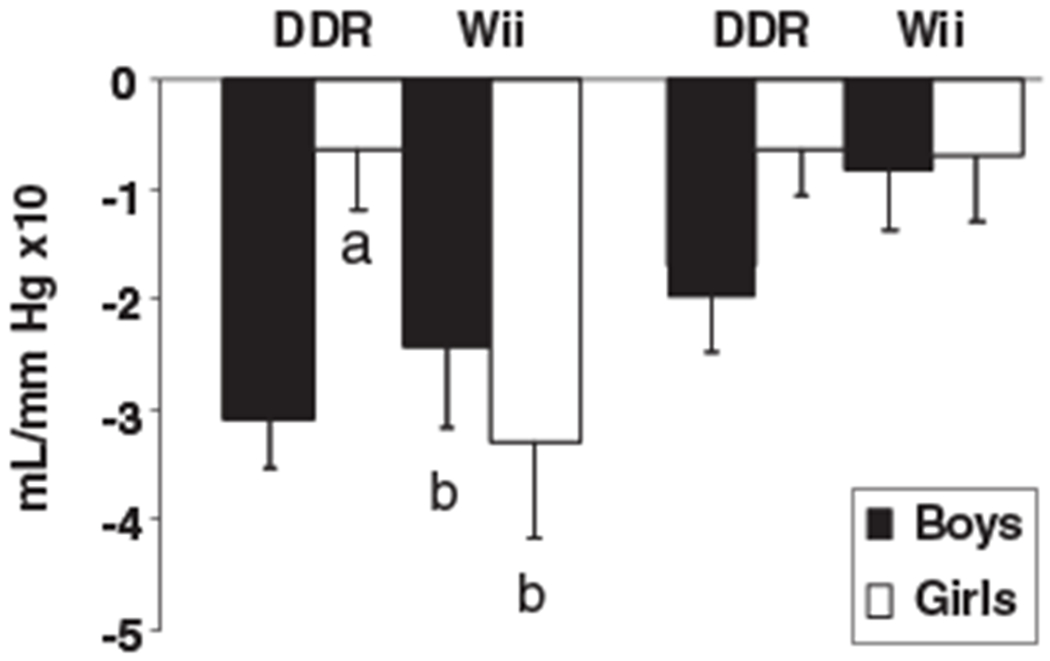
Change in arterial elasticity after DDR and Wii game play. Left, Large-artery elasticity declined in boys after playing both games, but only after Wii gaming for girls. Right, There was a trend for lower small-arterial elasticity in boys after DDR (P = .052). a Greater decline in boys versus girls after playing DDR (P < .02). b Postexercise value lower than baseline (P < .02).
DISCUSSION
The goal of this study was to quantify and compare rates of energy expenditure and related physiologic responses in children while playing 2 new-generation physically active video games. The primary new findings were that both the Wii Sports and DDR games elicit increases in energy expenditure, HR, and perceived exertion that are similar to, or even higher than, moderate-intensity walking. Because video and computer gaming is increasing in popularity, it is likely that spending time playing active video games could help counter the effects of sedentary behavior. Thus, there may be some benefit to people who are overweight or obese incorporating active video games into their physical activity plans.
The most notable findings were that Wii boxing and both skill levels of DDR tested (DDR1 and DDR2) elicited energy expenditure, HR, and ventilatory responses that were similar to or greater than moderate-intensity walking (4.2–5.7 km/hour). Energy expenditure during these activities was 3-fold greater than during resting. This increase occurred despite clearly different reliance on upper- versus lower-body movements, with predominant use of the arms for Wii games and greater leg activity for walking and DDR.
An important feature of exergaming is the entertainment factor, which may motivate some users more than traditional exercise modes. Active games such as DDR or Wii may offer an alternative to sedentary screen games and could be incorporated into more structured exercise programs as a complement to activities such as walking and cycling. Current recommendations are that children participate in ≥60 minutes of moderate-to-vigorous physical activity most days of the week.16,18 Playing Wii boxing, DDR at DDR2, or walking at 5.7 km/hour can be considered moderately intense on the basis of physiologic and perceptual responses. Children engaging in these activities for 30 minutes would expend ~360 to 390 kJ. Although this represents a small fraction of total daily energy turnover, daily energy imbalance of this magnitude, when occurring as energy excess, has been demonstrated to account for much of the current increase in obesity19 and, therefore, is important to body-weight regulation.
Rates of energy expenditure measured during DDR (~11 and ~13 kJ/min for DDR1 and DDR2, respectively) were consistent with values of ~12 kJ/min in previous studies11,20 in which the game was played at a single intensity level by children of similar age (10–12 years old) as the present study. Higher energy expenditure is possible as players gain experience and increase the skill setting, as shown in college-aged men.21 Wii bowling and boxing were selected, after preliminary testing, to represent light and moderate-intensity exercise, respectively. Energy expenditure during boxing (12 kJ/min) was 50% greater than in the bowling game (8 kJ/min). Previously, Graves et al13 reported energy expenditure values of ~12 kJ/min for both bowling and boxing, although a motion-detection system used to predict energy expenditure likely underestimated upper-body activity. More recent work by those authors, however, showed that energy expenditure was indeed higher for boxing than bowling, and this was reflected by corresponding differences in arm motion.12 In the present study, energy expenditure, HR, ventilatory rate, and perceived exertion all reflected the higher metabolic intensity of the boxing versus bowling games.
We found that boys expended more energy than girls when playing DDR and bowling.This suggests that some activities may engage boys more than girls, because energy expenditure did not differ during rest, walking, or boxing. Graves et al13 reported higher energy expenditure in boys versus girls when playing Wii tennis. The reason for these differences is not presently clear, especially in light of the fact that we found no differences in HR, and boys perceived their level of effort as lower than girls across activities. We reasoned that energy cost was similar among participants when walking because the treadmill speed was fixed and, therefore, activity intensity was largely obligatory. The Wii boxing game requires that participants remain consistently engaged to compete successfully, whereas game progression and movement during bowling is self-paced and potentially more variable. The DDR game requires participants to complete foot steps at a fixed pace to master the game, so differences between boys and girls may reflect differences in either motivation or exercise economy.
A novel finding was that large-artery elasticity was reduced 10 minutes after the DDR and Wii gaming sessions. We are not aware of previous observations on acute effects of physical activity on arterial elasticity in children, although in adults arterial elasticity was reported to decrease in response to isometric hand griping,22 resistance training,23 and moderate-intensity bicycling.24 The change in arterial elasticity may be related to the intensity of the exercise mode preceding the measurement because the magnitude of change after the DDR session was greater in boys, who also expended more energy playing that game than girls. In comparison, during the Wii game session boys and girls had similar energy expenditure when playing boxing and similar changes in large-artery elasticity. Collectively, the decline in elasticity was inversely associated with the increment in energy expenditure above rest during DDR2 and boxing, respectively. It is important to note that although arterial elasticity decreased acutely in response to exergaming, it is not clear from the current study how long this change persists. With repeated exercise training, higher elasticity at rest would be expected, because aerobic fitness and a history of high physical activity are positively associated with arterial compliance in children 9 to 11 years old.25,26 It is not yet known whether regular use of DDR or Wii games could elicit prospective changes in resting arterial elasticity in children or how this would compare to other forms of activity.
CONCLUSIONS
Activity-promoting video games increase energy expenditure equivalent to moderate-intensity walking. These new video games have the potential to attract children to become more physically active and could have particular value for extremely sedentary individuals or those who may shun traditional forms of exercise. Although there are case studies that have reported injuries incurred while using these new game systems,27,28 these injuries are similar to the overuse or accidental injuries that could occur with any form of physical activity. With increasing numbers of overweight children, it is important to promote daily exercise in various forms. Additional research is needed on the impact on body composition and cardiometabolic control from incorporating active video games into an exercise program for overweight or obese children.
WHAT’S KNOWN ON THIS SUBJECT:
Physical activity levels in children are declining, whereas obesity rates are increasing. Fun, alternate forms of physical activity may help some children become more active. Active video games such as DDR stimulate energy expenditure similar to walking.
WHAT THIS STUDY ADDS:
This study provides the first objective measurement of physiological responses in children playing a new physically active video game, Nintendo Wii. Comparisons with DDR and treadmill walking show that these games result in significant increases in energy expenditure.
ACKNOWLEDGMENTS
This project was supported by National Center for Research Resources grant P20RR024215 (to Dr Short). Additional support was provided by the Children’s Medical Research Institute Brann Summer Scholar program (to Dr Graf) and the Harold Hamm Oklahoma Diabetes Center.
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
ABBREVIATIONS
- DDR
Dance Dance Revolution
- HR
heart rate
- DDR1
DDR beginner level
- DDR2
DDR basic level
- RPE
rating of perceived exertion
Footnotes
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
REFERENCES
- 1.Power C, Lake JK, Cole TJ. Measurement and long-term health risks of child and adolescent fatness. Int J Obes Relat Metab Disord. 1997;21(7):507–526 [DOI] [PubMed] [Google Scholar]
- 2.Fagot-Campagna A, Pettitt DJ, Engelgau MM, et al. Type 2 diabetes among North American children and adolescents: an epidemiologic review and a public health perspective. J Pediatr. 2000;136(5):664–672 [DOI] [PubMed] [Google Scholar]
- 3.Ekelund U, Sjöström M, Yngve A, et al. Physical activity assessed by activity monitor and doubly labeled water in children. Med Sci Sports Exerc. 2001;33(2):275–281 [DOI] [PubMed] [Google Scholar]
- 4.Bouten CV, Verboeket-van de Venne WP, Westerterp KR, Verduin M, Janssen JD. Daily physical activity assessment: comparison between movement registration and doubly labeled water. J Appl Physiol. 1996;81(2):1019 –1026 [DOI] [PubMed] [Google Scholar]
- 5.Hoos MB, Plasqui G, Gerver WJM, Westerterp KR. Physical activity level measured by doubly labeled water and accelerometry in children. Eur J Appl Physiol. 2003;89(6):624–626 [DOI] [PubMed] [Google Scholar]
- 6.Watts K, Beye P, Siafarikas A, et al. Exercise training normalizes vascular dysfunction and improves central adiposity in obese adolescents. J Am Coll Cardiol. 2004;43(10):1823–1827 [DOI] [PubMed] [Google Scholar]
- 7.Watts K, Beye P, Siafarikas A, et al. Effects of exercise training on vascular function in obese children. J Pediatr. 2004;144(5):620–625 [DOI] [PubMed] [Google Scholar]
- 8.Shaibi GQ, Cruz ML, Ball GD, et al. Effects of resistance training on insulin sensitivity in overweight Latino adolescent males. Med Sci Sports Exerc. 2006;38(7):1208 –1215 [DOI] [PubMed] [Google Scholar]
- 9.Schlumpf M, Eiholzer U, Gygax M, et al. A daily comprehensive muscle training programme increases lean mass and spontaneous activity in children with Prader-Willi syndrome after 6 months. J Pediatr Endocrinol Metab. 2006;19(1):65–74 [DOI] [PubMed] [Google Scholar]
- 10.Dowda M, Ainsworth BE, Addy CL, Saunders R, Riner W. Environmental influences, physical activity, and weight status in 8- to 16-year-olds. Arch Pediatr Adolesc Med. 2001;155(6):711–717 [DOI] [PubMed] [Google Scholar]
- 11.Lanningham-Foster L, Jensen TB, Foster RC, et al. Energy expenditure of sedentary screen time compared with active screen time for children. Pediatrics. 2006;118(6). Available at:www.pediatrics.org/cgi/content/full/118/6/e1831 [DOI] [PubMed] [Google Scholar]
- 12.Graves LE, Ridgers ND, Stratton G. The contribution of upper limb and total body movement to adolescents’ energy expenditure whilst playing Nintendo Wii. Eur J Appl Physiol. 2008;104(4):617– 623 [DOI] [PubMed] [Google Scholar]
- 13.Graves L, Stratton G, Ridgers ND, Cable NT. Comparison of energy expenditure in adolescents when playing new generation and sedentary computer games: cross sectional study. BMJ. 2007; 335(7633):1282–1284 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000. CDC growth charts for the United States: methods and development. Vital Health Stat 11. 2002;(246):1–190 [PubMed] [Google Scholar]
- 15.Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc. 1982;14(5):377–381 [PubMed] [Google Scholar]
- 16.Barlow SE; Expert Committee. Expert Committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007;120(suppl 4):S164–S192 [DOI] [PubMed] [Google Scholar]
- 17.National High Blood Pressure Education Program, Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(2):555–576 [PubMed] [Google Scholar]
- 18.Institute of Medicine. Preventing Childhood Obesity: Health in the Balance. Washington, DC: National Academies Press; 2005 [PubMed] [Google Scholar]
- 19.Hill JO, Wyatt HR, Reed GW, Peters JC. Obesity and the environment: where do we go from here? Science. 2003;299(5608):853– 855 [DOI] [PubMed] [Google Scholar]
- 20.Unnithan VB, Houser W, Fernhall B. Evaluation of the energy cost of playing a dance simulation video game in overweight and nonoverweight children and adolescents. Int J Sports Med. 2006; 27(10):804–809 [DOI] [PubMed] [Google Scholar]
- 21.Sell K, Lillie T, Taylor J. Energy expenditure during physically interactive video game playing in male college students with different playing experience. J Am Coll Health. 2008;56(5):505–511 [DOI] [PubMed] [Google Scholar]
- 22.Lydakis C, Momen A, Blaha C, et al. Changes of elastic properties of central arteries during acute static exercise and lower body negative pressure. Eur J Appl Physiol. 2008;102(6):633– 641 [DOI] [PubMed] [Google Scholar]
- 23.Heffernan KS, Collier SR, Kelly EE, Jae SY, Fernhall B. Arterial stiffness and baroreflex sensitivity after bouts of aerobic and resistance exercise. Int J Sports Med. 2007;28(3):197–203 [DOI] [PubMed] [Google Scholar]
- 24.Sharman JE, McEniery CM, Campbell RI, et al. The effect of exercise on large artery haemodynamics in healthy young men. Eur J Clin Invest. 2005;35(12):738 –744 [DOI] [PubMed] [Google Scholar]
- 25.Reed KE, Warburton DER, Lewanczuk RZ, et al. Arterial compliance in young children: the role of aerobic fitness. Eur J Cardiovasc Prev Rehabil. 2005;12(5):492– 497 [DOI] [PubMed] [Google Scholar]
- 26.Schack-Nielsen L, Mølgaard C, Larsen D, Martyn C, Michaelsen KF. Arterial stiffness in 10-year-old children: current and early determinants. Br J Nutr. 2005;94(6):1004 –1011 [DOI] [PubMed] [Google Scholar]
- 27.Cowley AD, Minnaar G. Watch out for Wii shoulder. BMJ. 2008;336(7636):110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Peek AC, Ibrahim T, Abunasra H, Waller D, Natarajan R. White-out from a Wii: traumatic haemothorax sustained playing Nintendo Wii. Ann R Coll Surg Engl. 2008;90(6):W9–10 [DOI] [PMC free article] [PubMed] [Google Scholar]