

ABSTRACT
Objective:
To measure peak inspiratory flow (PIF) and assess dynamic lung function in children and adolescents with asthma, as well as to determine the association of PIF with dynamic lung function and clinical variables.
Methods:
This was a cross-sectional study of children and adolescents with asthma using dry powder inhalers (DPIs) regularly. The control group included sex-, age-, weight-, and height-matched individuals without lung disease. Socioeconomic and clinical variables were collected. PIF and dynamic lung function variables were obtained with a specific device. Between-group comparisons were made with the Student’s t-test and ANOVA. Multiple linear regression analysis was performed, and Pearson’s correlation coefficients were calculated to assess associations between PIF and the other variables.
Results:
A total of 88 individuals (44 asthma patients and 44 controls) participated in the study. PIF and respiratory muscle strength (S-index) values were lower in the asthma patients than in the controls. PIF correlated positively with age, weight, height, and S-index in the asthma group. After controlling for height, we found an increase of 0.05 units in PIF associated with an increase of 1 unit in the S-index in the asthma group.
Conclusions:
PIF appears to be lower in children and adolescents with asthma than in those without asthma, correlating positively with age, height, weight, and respiratory muscle strength.
Keywords: Dry powder inhalers, Asthma, Muscle strength, Child, Adolescent
RESUMO
Objetivo:
Analisar o pico de fluxo inspiratório (PFI) e a função pulmonar dinâmica de crianças e adolescentes asmáticos e verificar sua associação com variáveis clínicas.
Métodos:
Estudo transversal com crianças e adolescentes asmáticos que faziam uso regular de inaladores de pó. O grupo controle foi composto por participantes sem doença pulmonar, pareados por sexo, idade, peso e altura. Foram coletadas variáveis socioeconômicas e clínicas. O PFI e variáveis de função pulmonar dinâmica foram obtidos através de um dispositivo específico. As associações entre os dois grupos foram estudadas utilizando-se o teste t de Student e ANOVA. Realizou-se um modelo de regressão linear múltipla e foram calculados os coeficientes de correlação de Pearson para estimar associações entre o PFI e as demais variáveis.
Resultados:
Foram incluídos no estudo 88 participantes (44 em cada grupo). Nos asmáticos, os valores do PFI e de força muscular respiratória (S-índex) foram menores que os dos controles. O PFI nos asmáticos apresentou correlações positivas com as variáveis idade, peso, altura e S-índex. Controlando-se a altura, houve um aumento de 0,05 unidades no PFI associado ao aumento de 1 unidade de S-índex nos asmáticos.
Conclusões:
O PFI é menor em crianças e adolescentes com asma em comparação àqueles sem asma com características antropométricas semelhantes e apresenta correlações positivas com idade, altura, peso e força dos músculos respiratórios.
Descritores: Inaladores de pó seco, Asma, Força muscular, Criança, Adolescente
INTRODUCTION
The prevalence of asthma is high during childhood and adolescence; the disease results in a high number of emergency department visits and is associated with a significant economic burden related to hospitalizations for uncontrolled asthma. 1 - 3 Providing asthma education and reducing asthma triggers are essential to reduce the number of emergency department visits and the economic burden of asthma, as is the use of inhaled medications in some cases. 4
Dry powder inhalers (DPIs) have been increasingly used to deliver inhaled medication, correct inhaler technique and inhalation flow being required for treatment success. In addition, inspiratory flow must be sufficient to overcome the internal resistance of the device and allow the delivery of the correct medication dose, so that the desired therapeutic effect is achieved. 5 - 7
Studies have shown that peak inspiratory flow (PIF) varies widely across patients, especially in those with severe airflow obstruction (such as severe asthma patients), and depends on respiratory muscle strength. 8 - 10 Inspiratory flow decreases during acute exacerbations of asthma and increases during periods of disease remission. 11 There are difficulties in measuring PIF, and only a few centers routinely assess it. The In-Check DIAL (Clement Clarke International Ltd., Harlow, UK) is the only device that simulates the resistance characteristics of different DPIs; however, it is not currently available in all countries. Inhaler devices are often prescribed on the basis of intuition and common sense rather than careful evaluation. 12 Factors influencing drug deposition include inhaler technique, the shape of the inspiratory flow curve, and inspiratory volume. 11 , 12
In 2010, the POWERbreathe® K5 (HaB International Ltd., Southam, UK) was launched, with software that allows analysis of lung function variables, including PIF. In addition to measuring PIF, the POWERbreathe® K5 assesses variables such as the S-index (dynamic muscle strength), inhaled air volume, and duration of inhalation, as well as allowing real-time graphical analysis of the inhalation pattern. 13 - 15 The POWERbreathe® K5 is currently the only device available in Brazil to assess the aforementioned variables. 13
Given the large number of inhaler devices currently available, the differences among manufacturers regarding PIF rates, and the lack of validated guidelines for prescribing an inhaler device, the objective of the present study was to measure PIF and assess dynamic lung function in children and adolescents with asthma using DPIs, as well as to determine the association of PIF with dynamic lung function and clinical variables.
METHODS
Study design
This was a cross-sectional analytical study conducted between March of 2018 and September of 2019 at the Pediatric Pulmonology Outpatient Clinic of the Instituto de Medicina Integral Prof. Fernando Figueira (IMIP, Professor Fernando Figueira Institute of Integrative Medicine), which is a tertiary referral hospital for pediatric respiratory diseases and which is located in the city of Recife, Brazil. The study was approved by the local research ethics committee (CAAE no. 84171618.3.0000.5201). Eligible individuals were directly invited to participate, and all participants gave written informed consent or assent, as applicable.
Study population
The study population consisted of 88 children/adolescents in the 6- to 18-year age bracket. Participants were divided into two groups: the asthma group (n = 44) and the control group (n = 44). The decision to include a control group was based on the lack of reference values for dynamic lung function in the literature. The eligibility criteria were as follows:
asthma group-children/adolescents with a clinical diagnosis of asthma 4 followed at the IMIP Pediatric Pulmonology Outpatient Clinic and using DPIs regularly for at least three months. Those who were unable to understand or perform the required maneuvers were excluded, as were those with any chronic lung disease other than asthma.
control group-children/adolescents without asthma or any other lung disease matched to those in the asthma group for sex, age, weight, and height. All of the individuals included in the control group were selected from among those enrolled in a public school in the city of Recife and were able to understand and perform the required maneuvers.
The sample size was calculated with the use of the free, Web-based, open-source program OpenEpi, version 3.01, differences in mean PIF between asthma patients and controls being taken into account. A sample size of 92 (46 per group) was calculated to be required for a significance level of 95% and a power of 80%.
Procedures
Weight and height were measured on the day of the evaluation and recorded on a data collection form, which included the Asthma Control Test, a five-item questionnaire for assessing asthma control (controlled, partly controlled, or uncontrolled). 16 , 17 The BMI was calculated with the use of the BVS online calculator for children, the percentiles being determined on the basis of the Centers for Disease Control and Prevention charts. 18 The total daily dose of inhaled corticosteroids (in µg) was classified as low, intermediate, or high on the basis of the GINA guidelines. 19
The level of physical activity was assessed with an adapted version of the habitual level of physical activity (HLPA) score developed by Santuz et al. 20 The HLPA score used in the present study was as follows: 1, sedentary lifestyle; 2, regular physical activity (≤ 2 h/week); and 3, competitive physical activity or physical activity > 2 h/week. 20 With regard to environmental control, participants/legal guardians were asked about exposure to dust, mold, and pet dander, as well as active/passive exposure to cigarette smoke. Environmental control was considered inadequate if participants/legal guardians reported exposure to any of the aforementioned exposure items.
Participants were asked about the type of inhaler device used and were asked to demonstrate their inhaler technique using placebo devices. Patient inhaler technique was evaluated on the basis of the manufacturer instructions. Patients were instructed to inhale as usual, with or without the assistance of their companions, but without any input from the examiners. Inhaler technique was evaluated by two trained assessors, who evaluated dose preparation, exhalation (exhalation into the device constituting a technique error), inhalation (failure to inhale as rapidly and deeply as possible constituting a technique error), and inspiratory pause (failure to hold breath for 10 seconds constituting a technique error). There are differences across device types regarding dose preparation, which should follow the manufacturer instructions. 21
PIF was measured with the POWERbreathe® K5, which is an electronic inspiratory loading device. The device includes the Breathe-Link live feedback software, which allows real-time graphical analysis of the breathing pattern.
PIF was measured with participants sitting in a chair with a backrest, wearing a nose clip, and facing a computer screen for visual feedback, which assisted in performing the inhalation maneuver. The assessor put the device mouthpiece in place and instructed participants to keep their lips sealed tightly around the mouthpiece in order to prevent leaks. Participants were then instructed to exhale to RV and then inhale as rapidly and deeply as possible. PIF rates were expressed in liters per second. Because PIF is a dynamic measure, participants performed 8-10 consecutive maneuvers. The highest PIF rate was selected for analysis, provided that the curve was reproducible and acceptable. For a reproducible curve, the three highest PIF rates must differ by no more than 20%. For an acceptable curve, all maneuvers must be performed with no leaks noted (graphical analysis) and the highest PIF rate must be achieved within the first few seconds, without evidence of decrease prior to the highest PIF rate achieved. All participants were able to perform the maneuver correctly, and no test was stopped because of respiratory distress or at the request of the participant.
In addition to PIF measurements, the following lung function variables were obtained: the S-index, which is a dynamic measure of inspiratory muscle strength (in cmH2O); total VT (in L); and time to PIF (in s).
Statistical analysis
Statistical analyses were performed with the Stata statistical software package, version 12.1 SE (StataCorp LP, College Station, TX, USA). Between-group comparisons were made with the Student’s t-test and ANOVA. Potential confounders were controlled for in a multiple linear regression model, which included all of the variables that differed significantly between the groups in the univariate analysis. Pearson’s correlation coefficient was used in order to estimate the strength of association between PIF and the other variables. The level of significance was set at 5%.
RESULTS
A total of 109 individuals were considered eligible for the study. The asthma group comprised 44 children and adolescents who had asthma and who were not experiencing an exacerbation, the mean age, weight, and height of the patients being 14.3 ± 3.5 years, 52.3 ± 13.0 kg, and 156.4 ± 12.2 cm, respectively. The control group comprised 44 children and adolescents who did not have asthma and who were matched to the asthma patients for sex, age, weight, and height, the mean age, weight, and height of the controls being 14.0 ± 3.46 years, 55.85 ± 12.92 kg, and 1.60 ± 0.11 cm, respectively. Therefore, a total of 88 individuals participated in the study (Figure 1). There were no differences between the groups regarding baseline characteristics. Table 1 shows the general characteristics of the patients with asthma.
Figure 1. Flow chart of the patient selection process. IMIP: Instituto de Medicina Integral Prof. Fernando Figueira (Professor Fernando Figueira Institute of Integrative Medicine); and DPI: dry powder inhaler.
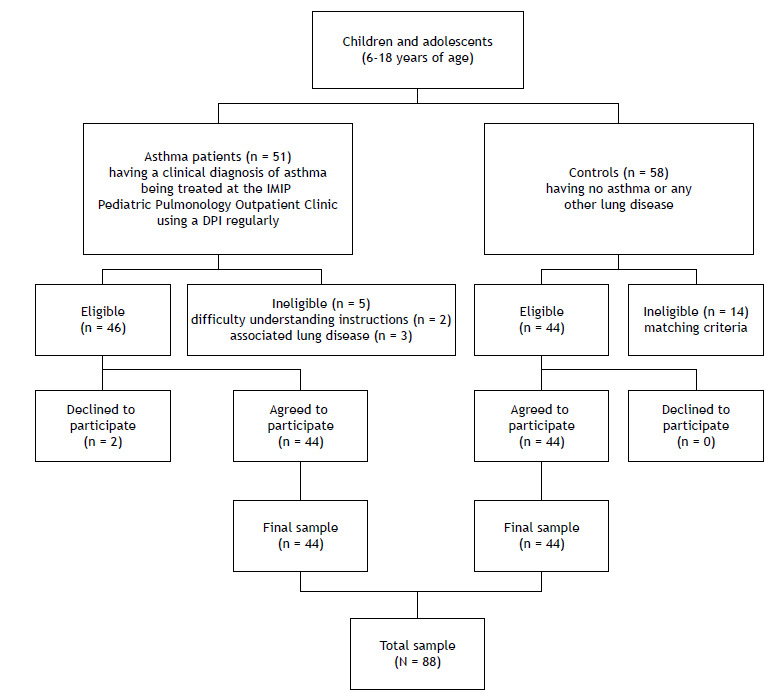
Table 1. Biological and clinical characteristics of the patients with asthma (n = 44), as well as level of environmental control and type of inhaler device.
| Socioeconomic variable | n | % |
|---|---|---|
| Male sex | 24 | 54.5 |
| BMI Underweight Normal weight Overweight Obese |
4 24 9 7 |
9.1 54.5 20.4 16 |
| Environmental control Adequate Inadequate |
10 34 |
22.73 77.27 |
| Level of physical activity (HLPA score) Sedentary lifestyle Regular physical activity (≤ 2 h/week) Physical activity > 2 h/week |
13 16 15 |
30.2 37.2 32.6 |
| Type of inhaler device Aerolizer Aerocaps Turbohaler CDM Haler Diskus |
19 17 2 3 3 |
43.18 38.64 4.54 6.82 6.82 |
| Daily inhaled corticosteroid dose Low Intermediate High |
22 14 8 |
50 31.8 18.2 |
| Inhaler technique Correct Incorrect |
25 19 |
56.8 43.2 |
| Asthma control (ACT) Controlled asthma Partly controlled asthma Uncontrolled asthma |
27 11 6 |
61.36 25 13.64 |
HLPA: habitual level of physical activity; and ACT: Asthma Control Test.
Table 2 shows a comparison of mean lung function values between the asthma and control groups. There were significant differences between the groups regarding PIF and S-index values.
Table 2. Comparison of mean lung function values between the asthma and control groups.a .
| Variable | Group | p* | |
|---|---|---|---|
| Asthma (n = 44) | Control (n = 44) | ||
| PIF, L/s | 4.34 ± 0.87 | 4.86 ± 1.33 | 0.03 |
| Volume, L | 1.72 ± 0.65 | 1.78 ± 0.78 | 0.70 |
| S-index | 78.27 ± 15.21 | 87.10 ± 23.32 | 0.04 |
| Time to PIF, s | 0.20 ± 0.09 | 0.18 ± 0.11 | 0.85 |
PIF: peak inspiratory flow. aValues expressed as mean ± SD. *Student’s t-test.
Table 3 shows the mean PIF rates in the asthma group, by clinical characteristics. A higher level of physical activity translated to a higher PIF rate in the asthma group. In addition, PIF correlated positively with age (r = 0.56, p ≤ 0.001), weight (r = 0.32; p = 0.032), height (r = 0.56, p ≤ 0.001), and the S-index (r = 0.96; p ≤ 0.001) in the asthma group.
Table 3. Mean peak inspiratory flow rates in the asthma group, by clinical characteristics.a .
| Variable | p* | ||||
|---|---|---|---|---|---|
| PIF, L/s | BMI | ||||
| Underweight | Normal weight | Overweight | Obese | ||
| 4 (4.4 ± 1.2) | 24 (4.6 ± 0.8) | 9 (4.2 ± 1.0) | 7 (3.8 ± 0.6) | 0.165 | |
| Level of physical activity (HLPA score) | |||||
| Sedentary lifestyle | Regular physical activity (≤ 2 h/week) | Physical activity > 2 h/week | |||
| 14 (4.2 ± 0.6) | 16 (4.0 ± 0.7) | 14 (4.8 ± 1.1) | 0.045 | ||
| Asthma control (ACT) | |||||
| Controlled asthma | Partly controlled asthma | Uncontrolled asthma | |||
| 27 (4.5 ± 0.9) | 11 (4.3 ± 0.7) | 6 (3.6 ± 0.6) | 0.060 | ||
| Sex | |||||
| Female | Male | ||||
| 24 (4.28 ± 0.61) | 20 (4.42 ± 1.12) | 0.60 | |||
| Daily inhaled corticosteroid dose | |||||
| Low | Intermediate | High | |||
| 22 (4.46 ± 0.87) | 14 (4.46 ± 0.85) | 8 (4.44 ± 0.89) | 0.74 | ||
| Inhaler technique | |||||
| Correct | Incorrect | ||||
| 25 (4.30 ± 0.93) | 19 (4.40 ± 0.81) | 0.70 | |||
PIF: peak inspiratory flow; HLPA: habitual level of physical activity; and ACT: Asthma Control Test. aValues expressed as n of participants and (mean ± SD) PIF. *ANOVA.
Table 4 shows that height and the S-index correlated positively with PIF, a higher height and a higher S-index translating to a higher PIF rate. The adjusted multiple regression model showed an adjusted r2 of 93.4% (F [2.40] = 325.64; p < 0.001). After controlling for height, we found an increase of 0.05 units in PIF (in L/s) associated with an increase of 1 unit in the S-index; likewise, after controlling for the S-index, we found an increase of 0.012 units in PIF (in L/s) associated with an increase of 1 cm in height in the asthma group (Table 4).
Table 4. Descriptive statistics, correlation coefficients, and multiple regression coefficients for the peak inspiratory flow rates and explanatory variables (height and S-index) in the asthma group.a .
| Variable | n | Mean | SD | r* | Regression coefficient (95% CI) | p** |
|---|---|---|---|---|---|---|
| PIF, L/s | 44 | 4.3 | 0.9 | - | - | - |
| Height, cm | 44 | 156.4 | 12.2 | 0.56 | 0.012 (0.006-0.019) | < 0.001 |
| S-index | 44 | 51.9 | 15.2 | 0.96 | 0.05 (0.05-0.06) | < 0.001 |
PIF: peak inspiratory flow. aThe initial explanatory variables were those showing a p < 0.20 in Tables 2 and 3 (age, height, weight, S-index, BMI, level of physical activity, and level of asthma control). Multiple regression constant = −0.19. *Pearson’s correlation coefficient. **Student’s t-test.
DISCUSSION
The present study is the first to analyze PIF and dynamic lung function variables in children and adolescents with asthma using an electronic inspiratory loading device, demonstrating that PIF is lower in asthma patients than in controls.
It is known that factors related to patient experience with the inhalation maneuver are related to changes attributable to a learning effect. 21 , 22 Nevertheless, PIF values were significantly lower in the children and adolescents with asthma, who had to perform the inhalation maneuver on a daily basis, than in the healthy controls, who had never had to perform such a maneuver. This can be explained by the pathophysiology of asthma, which is associated with airway obstruction (particularly small airway obstruction), airway remodeling, or a combination of the two. There is an increase in the negative intrathoracic pressure needed to overcome inhaler device resistance, resulting in narrowing of the airway lumen and decreased inspiratory flow. 23 - 25 A lower PIF rate in asthma patients might also be related to flattening of the diaphragm from hyperinflation secondary to airway obstruction. 26
In the present study, children and adolescents with asthma achieved a mean PIF of 4.34 L/s, which is equivalent to 260.4 L/min and higher than the reported rate for children and adolescents with asthma (a mean PIF of ~ 91.1 L/min). 11 This difference can be attributed to the different internal resistances used during the tests. In the aforementioned study, 11 PIF was measured by simulating the internal resistance of the Accuhaler (GlaxoSmithKline, Bretford, UK), which is a medium-resistance inhaler device, whereas, in our study, PIF was measured against a standardized resistance of 3 cmH2O, which is the minimum resistance imposed by the POWERbreathe® K5, being required in order to actuate the loading valve. In addition, as is well established in the literature, a higher internal resistance translates to a lower PIF rate. 27 The mean PIF rate achieved in the present study (260.4 L/s) is similar to that reported by Kamps et al. (i.e., 186.8 L/s), 8 who measured PIF without simulating the internal resistance of inhaler devices. Our finding of a higher PIF rate might be due to the fact that the mean height was higher in our study population. Kamps et al. 8 found a positive correlation between height and PIF, as we did in our study.
In our study, each participant performed 10 maneuvers for PIF measurement, the highest PIF rate being selected for analysis. This is in contrast with other studies, in which participants perform 1-3 maneuvers. Our decision to have participants perform up to 10 maneuvers was based on a study by Silva et al. 15 and was made in order not to underestimate PIF, given that most of the participants in the study 15 achieved the highest PIF rate in the eighth maneuver, because of the learning effect.
Studies have shown that PIF is reduced during acute exacerbations of asthma; however, we found no correlation between PIF and the level of asthma control, with most of the asthma patients in our study being classified as having controlled asthma. 8 , 28
We found a difference between the asthma and control groups regarding the relationship between PIF and the level of physical activity. This can be explained by the fact that respiratory muscle strength is decreased in children with asthma, and decreased respiratory muscle strength can lead to a decrease in PIF not only by obstructing airflow but also by reducing the number of diaphragm muscle fibers. Aerobic activity is known to improve asthma, whereas a sedentary lifestyle can worsen it; this is consistent with our finding that a higher level of physical activity translates to a higher PIF rate. 29
In the present study, age correlated positively with PIF in children and adolescents; this might be due to a better understanding and execution of the inhaler technique, resulting in higher PIF values, or to the process of muscle growth and development. 8 , 30 In adults, age correlates negatively with PIF, the aging process leading to loss of muscle strength and mass and resulting in lower PIF values. 31 - 33
In the present study, VT and time to PIF were similar between the asthma and control groups. In a study by Seheult et al., 31 mean VT was slightly lower than in the present study (1.1 L vs. 1.72 L). In a study of children trained in using DPIs, time to PIF was found to change as resistance changed. 34 Mean time to PIF was found to be 0.16 s when high-resistance devices were used and 0.19 s when low-resistance devices were used. 34 These findings are consistent with those of the present study, in which time to PIF was approximately 0.20 s.
S-index values were significantly different between the asthma patients and controls in the present study. The diaphragm is the major inspiratory muscle, and the fact that it is at a biomechanical disadvantage in patients with asthma might be a factor contributing to lower S-index values in this population. In addition, the S-index correlated positively with PIF, a finding that is consistent with those of Kamps et al., 8 who found a positive correlation between PIF and MIP in children with asthma using DPIs. Like the S-index, MIP is a measure of inspiratory muscle strength. Therefore, the S-index is a dynamic lung function measure that can indicate reduced PIF.
Although Kamps et al. 8 showed a correlation between PIF and a static measure of respiratory muscle strength, no studies have shown a correlation between PIF and a dynamic measure of lung function (the S-index). Given that this is the first study to show a correlation between PIF and S-index values in children and adolescents with and without asthma, there are currently no reference values for this population. We found mean S-index values of 87.10 cmH2O and 78.27 cmH2O for controls and asthma patients, respectively. Although the mean S-index was higher in a study by Silva et al. (i.e., 102 cmH2O), 15 the study population consisted of healthy adults.
One of the limitations of the present study is that the device used in order to measure PIF does not simulate the internal resistance of the inhaler devices used in clinical practice. Another limitation is that symptoms of upper airway involvement were not evaluated, and they could have an impact on pulmonary function.
In summary, PIF measurement proved to be a practical method that provides important additional information on which to base prescription decisions regarding the use of DPIs. Despite the positive outcomes of inhalation therapy, it should be prescribed on a case-by-case basis after careful patient evaluation. PIF appears to be lower in children and adolescents with asthma using DPIs than in controls without lung disease. Age, weight, height, and respiratory muscle strength appear to correlate positively with PIF.
DPIs should be prescribed on a case-by-case basis after careful patient evaluation, with anthropometric characteristics and lung function variables being taken into account. Patients should be instructed on how to perform the inhalation maneuver correctly and should be encouraged to participate in supervised physical activity or in a pulmonary rehabilitation program.
ACKNOWLEDGMENTS
We thank PULMOCARDIO Fisioterapia Ltda. for the loan of the POWERbreathe® K5, which made the present study possible.
Footnotes
Financial support: None.
Study carried out in the Serviço de Pneumologia Pediátrica, Instituto de Medicina Integral Prof. Fernando Figueira - IMIP - Recife (PE) Brasil.
REFERENCES
- 1.Solé D, Camelo-Nunes IC, Wandalsen GF, Mallozi MC. Asthma in children and adolescents in Brazil contribution of the International Study of Asthma and Allergies in Childhood (ISAAC) [Article in Portuguese]. Rev Paul. Pediatr. 2014;32(1):114–125. doi: 10.1590/S0103-05822014000100018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pizzichini MMM, Cruz ÁA. Celebrating World Asthma Day in Brazil is the glass half full or half empty?. J Bras. Pneumol. 2019;45(3):e20190130. doi: 10.1590/1806-3713/e20190130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cardoso TA, Roncada C, Silva ERD, Pinto LA, Jones MH, Stein RT. The impact of asthma in Brazil a longitudinal analysis of data from a Brazilian national database system. J Bras Pneumol. 2017;43(3):163–168. doi: 10.1590/s1806-37562016000000352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Global Initiative for Asthma - GINA . Pocket Guide for Asthma Management and Prevention in Children. Bethesda: Global Initiative for Asthma; 2018. https://ginasthma.org/archived-reports [Google Scholar]
- 5.Salvi S, Gogtay J, Aggarwal B. Use of breath-actuated inhalers in patients with asthma and COPD - an advance in inhalational therapy a systematic review. Expert Rev Respir Med. 2014;8(1):89–99. doi: 10.1586/17476348.2014.854168. [DOI] [PubMed] [Google Scholar]
- 6.Pepper AN, Cooke A, Livingston L, Lockey RF. Asthma and chronic obstructive pulmonary disease inhalers Techniques for proper use [published correction appears in Allergy Asthma. Proc. 2016;37(5):122–122. doi: 10.2500/aap.2016.37.3954. [DOI] [PubMed] [Google Scholar]
- 7.Farkas Á, Jókay Á, Balásházy I, Füri P, Müller V, Tomisa G. Numerical simulation of emitted particle characteristics and airway deposition distribution of Symbicort((r)) Turbuhaler((r)) dry powder fixed combination aerosol drug. Eur J Pharm Sci. 2016;93:371–379. doi: 10.1016/j.ejps.2016.08.036. [DOI] [PubMed] [Google Scholar]
- 8.Kamps AW, Brand PL, Roorda RJ. Variation of peak inspiratory flow through dry powder inhalers in children with stable and unstable asthma. Pediatr Pulmonol. 2004;37(1):65–70. doi: 10.1002/ppul.10410. [DOI] [PubMed] [Google Scholar]
- 9.Taylor TE, Holmes MS, Sulaiman I, Costello RW, Reilly RB. Influences of gender and anthropometric features on inspiratory inhaler acoustics and peak inspiratory flow rate. Annu Int Conf IEEE Eng Med Biol Soc. 2015;2015:2227–2230. doi: 10.1109/EMBC.2015.7318834. [DOI] [PubMed] [Google Scholar]
- 10.Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde . Portaria no. 1317 de 25 Nov 2013. Aprova o Protocolo Clínico e Diretrizes Terapêuticas da Asma. Brasília: Ministério da Saúde; http://bvsms.saude.gov.br/bvs/saudelegis/sas/2013/prt1317_25_11_2013.html [Google Scholar]
- 11.Bentur L, Mansour Y, Hamzani Y, Beck R, Elias N, Amirav I. Measurement of inspiratory flow in children with acute asthma. Pediatr Pulmonol. 2004;38(4):304–307. doi: 10.1002/ppul.20109. [DOI] [PubMed] [Google Scholar]
- 12.Sanders MJ. Guiding Inspiratory Flow Development of the In-Check DIAL G16, a Tool for Improving Inhaler Technique. Pulm Med. 2017;2017:1495867–1495867. doi: 10.1155/2017/1495867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Langer D, Jacome C, Charususin N, Scheers H, McConnell A, Decramer M. Measurement validity of an electronic inspiratory loading device during a loaded breathing task in patients with COPD. Respir Med. 2013;107(4):633–635. doi: 10.1016/j.rmed.2013.01.020. [DOI] [PubMed] [Google Scholar]
- 14.Minahan C, Sheehan B, Doutreband R, Kirkwood T, Reeves D, Cross T. Repeated-sprint cycling does not induce respiratory muscle fatigue in active adults measurements from the powerbreathe(r) inspiratory muscle trainer. J Sports Sci Med. 2015;14(1):233–238. [PMC free article] [PubMed] [Google Scholar]
- 15.Silva PE, de Carvalho KL, Frazão M, Maldaner V, Daniel CR, Gomes-Neto M. Assessment of Maximum Dynamic Inspiratory Pressure. Respir Care. 2018;63(10):1231–1238. doi: 10.4187/respcare.06058. [DOI] [PubMed] [Google Scholar]
- 16.Diretrizes da Sociedade Brasileira de Pneumologia e Tisiologia para o Manejo da Asma - 2012 J Bras. Pneumol. 2012;38(Suppl 1):S1–S46. [Google Scholar]
- 17.Roxo JP, Ponte EV, Ramos DC, Pimentel L, D'Oliveira A, Júnior, Cruz AA. Portuguese-language version of the Asthma Control Test validation for use in Brazil. J Bras Pneumol. 2010;36(2):159–166. doi: 10.1590/S1806-37132010000200002. [DOI] [PubMed] [Google Scholar]
- 18.Biblioteca Virtual em Saúde (BVS) Tede Telessaúde Brasil [homepage on the Internet] São Paulo: BVS; https://aps.bvs.br/apps/calculadoras/?page=7 [Google Scholar]
- 19.Global Initiative for Asthma (GINA) 2019 GINA Report: Global Strategy for Asthma Management and Prevention. Bethesda: GINA; https://ginasthma.org/2019-gina-report-global-strategy-for-asthma-management-and-prevention [Google Scholar]
- 20.Santuz P, Baraldi E, Zaramella P, Filippone M, Zacchello F. Factors limiting exercise performance in long-term survivors of bronchopulmonary dysplasia. Pt 1Am J Respir Crit Care Med. 1995;152(4):1284–1289. doi: 10.1164/ajrccm.152.4.7551383. [DOI] [PubMed] [Google Scholar]
- 21.Aguiar R, Lopes A, Ornelas C, Ferreira R, Caiado J, Mendes A. Terapêutica inalatória Técnicas de inalação e dispositivos inalatórios. Rev Port Imunoalerg. 2017;25(1):9–26. [Google Scholar]
- 22.Dal Negro RW, Povero M. Dry-powder inhalers in patients with persistent airflow limitation usability and preference. Multidiscip Respir Med. 2016;11(1):31–31. doi: 10.1186/s40248-016-0068-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Oliveira CM, Lanza Fde C, Solé D. Respiratory muscle strength in children and adolescents with asthma similar to that of healthy subjects?. J Bras. Pneumol. 2012;38(3):308–314. doi: 10.1590/S1806-37132012000300005. [DOI] [PubMed] [Google Scholar]
- 24.Gelfand EW, Kraft M. The importance and features of the distal airways in children and adults. J Allergy Clin Immunol. 2009;124(6 Suppl):S84–S87. doi: 10.1016/j.jaci.2009.07.062. [DOI] [PubMed] [Google Scholar]
- 25.World Allergy Organ J Manifesto on small airway involvement and management in asthma and chronic obstructive pulmonary disease an Interasma (Global Asthma Association - GAA) and World Allergy Organization (WAO) document endorsed by Allergic Rhinitis and its Impact on Asthma (ARIA) and Global Allergy and Asthma European Network (GA2LEN) World Allergy Organ J. 2016;9(1):37–37. doi: 10.1186/s40413-016-0123-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Weiner P, Suo J, Fernandez E, Cherniack RM. The effect of hyperinflation on respiratory muscle strength and efficiency in healthy subjects and patients with asthma. Am Rev Respir Dis. 1990;141(6):1501–1505. doi: 10.1164/ajrccm/141.6.1501. [DOI] [PubMed] [Google Scholar]
- 27.Cegla UH. Pressure and inspiratory flow characteristics of dry powder inhalers. Respir Med. 2004;98(A):S22–S28. doi: 10.1016/j.rmed.2004.02.003. [DOI] [PubMed] [Google Scholar]
- 28.Selroos O. Dry-powder inhalers in acute asthma. Ther Deliv. 2014;5(1):69–81. doi: 10.4155/tde.13.132. [DOI] [PubMed] [Google Scholar]
- 29.Andrade LB, Britto MC, Lucena-Silva N, Gomes RG, Figueroa JN. The efficacy of aerobic training in improving the inflammatory component of asthmatic children Randomized trial. Respir Med. 2014;108(10):1438–1445. doi: 10.1016/j.rmed.2014.07.009. [DOI] [PubMed] [Google Scholar]
- 30.Vogelberg C, Kremer HJ, Ellers-Lenz B, Engel M, Maus J, Conrad F. Clinical evaluation of the peak inspiratory flow generated by asthmatic children through the Novolizer. Respir Med. 2004;98(10):924–931. doi: 10.1016/j.rmed.2004.03.024. [DOI] [PubMed] [Google Scholar]
- 31.Seheult JN, Costello S, Tee KC, Bholah T, Al Bannai H, Sulaiman I. Investigating the relationship between peak inspiratory flow rate and volume of inhalation from a Diskus(tm) Inhaler and baseline spirometric parameters a cross-sectional study. Springerplus. 2014;3:496–496. doi: 10.1186/2193-1801-3-496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Janssens JP, Pache JC, Nicod LP. Physiological changes in respiratory function associated with ageing. Eur Respir J. 1999;13(1):197–205. doi: 10.1183/09031936.99.14614549. [DOI] [PubMed] [Google Scholar]
- 33.Janssens W, VandenBrande P, Hardeman E, De Langhe E, Philps T, Troosters T. Inspiratory flow rates at different levels of resistance in elderly COPD patients. Eur Respir J. 2008;31(1):78–83. doi: 10.1183/09031936.00024807. [DOI] [PubMed] [Google Scholar]
- 34.Kondo T, Hibino M, Tanigaki T, Cassan SM, Tajiri S, Akazawa K. Appropriate use of a dry powder inhaler based on inhalation flow pattern. J Pharm Health Care Sci. 2017;3:5–5. doi: 10.1186/s40780-017-0076-9. [DOI] [PMC free article] [PubMed] [Google Scholar]