

Abstract
Background
The use of circulating tumor DNA (ctDNA) to reflect clinical benefits of advanced non-small cell lung cancer (NSCLC) patients during immune checkpoint inhibitor (ICI) therapy remains controversial. This study aimed to determine the association of pre-treatment and early dynamic changes of ctDNA with clinical outcomes in advanced NSCLC patients treated with ICIs.
Methods
Electronic databases (PubMed, Embase, Web of Science, and Cochrane) were systematically searched to include relevant studies published in English up to November 2020. The primary outcomes were overall survival (OS) and progression-free survival (PFS) and the secondary outcome was objective response rate (ORR) with RECIST criteria.
Results
A total of 1017 patients from 10 studies were identified. The baseline ctDNA levels (detected versus not detected) showed no significant association with clinical outcomes regarding OS (hazard ratio [HR], 1.18; 95% confidence interval [CI], 0.93-1.51), PFS (HR, 0.98; 95% CI, 0.80-1.21), and ORR (odds ratio [OR], 0.89; 95% CI, 0.54-1.46). Interestingly, when taken early longitudinal assessment of ctDNA into consideration, the early reduction of the concentration of ctDNA was associated with significant improvements of OS (HR, 0.19; 95% CI, 0.10-0.35), PFS (HR, 0.30; 95% CI, 0.22-0.41) and ORR (OR, 0.07; 95% CI, 0.03-0.18). Further subgroup analyses revealed that the reduction magnitude did not significantly impact the association between ctDNA and clinical outcomes, suggesting that both patients with decreased ctDNA or a ≥50% reduction of ctDNA was associated with improved OS, PFS and ORR.
Conclusion
Early reduction of ctDNA was associated with improved OS, PFS and ORR in advanced NSCLC patients treated with ICIs.
Systematic Review Registration
https://www.crd.york.ac.uk/PROSPERO, CRD42021226255.
Keywords: non-small-cell lung cancer, immune checkpoint inhibitor, circulating tumor DNA, biomarker, survival
Introduction
Over the past decade, immunotherapy, targeting immune checkpoint molecules, programmed-death-1(PD-1)/PD ligand-1 (PD-L1) axis, has turned into one of the most important breakthroughs in cancer treatment, including non-small cell lung cancer (NSCLC) (1). Although treatment of NSCLC with immune checkpoint inhibitors (ICIs) can produce remarkably durable responses, a considerable proportion of patients cannot derive meaningful benefits from ICI therapy owing to drug resistance (2), disease hyper-progression (3), or immune-related adverse events (irAEs) (4).
Currently, several promising biomarkers for ICI therapy have been widely investigated, such as tumor mutation burden (TMB), PD-L1 expression, germline genotype of HLA-I, the molecular profiling of the tumor microenvironment, mutations in DNA mismatch repair and replication genes (1, 5, 6). However, most of these biomarkers are far from perfect biomarkers owing to being invasive, not always feasible, and its spatial and temporal heterogeneity (6, 7).
In response to the demand for genetic predictive and non-invasive molecular biomarkers in NSCLC, liquid biopsy, including circulating tumor DNA (ctDNA), have been developed. ctDNA, referring to a sub-set of cell-free DNA, is released by tumor cells undergoing apoptosis, necrosis, and in extracellular vesicles (exosomes) secreted from tumor cells and can be found in plasma. ctDNA is highly fragmented and ranges between 100 and 200 base pairs in size and represents genetic material from the primary tumor as well as metastases (8). ctDNA can be quantified using multiple metrics, such as mutant allele fraction or mutant allele concentration (that is, copies per milliliter) (9). The level of ctDNA in plasma has been demonstrated to correlate with tumor size (10, 11), disease stage (12), the clinical responses and prognosis of patients receiving anti-tumor treatment (13–16). The short half-life of ctDNA (17, 18), as well as the reduced and ease risk of repeating liquid biopsies relative to tissue biopsies (19) or imaging (20), enables ctDNA to be used for real-time monitoring of tumor burden in response to treatment. Although NSCLC is the cancer type for which plasma ctDNA testing has the most comprehensive and compelling evidence (21), it is still controversial regarding the role of ctDNA in predicting survival and clinical response.
ctDNA assays for the evaluation of cancers that harbor EGFR-sensitizing or EGFR-resistance mutations have already entered into clinical practice (22). A recent prospective study using ctDNA to guide matched targeted therapy in lung cancers supported the incorporation of plasma ctDNA into clinical practice (23). In addition to the direction of molecular targeted treatment, ctDNA could also potentially help monitor ICI response as the quantitative level in plasma has been demonstrated to reflect the tumor burden in patients even earlier than clinical detection (17, 24–27) and might identify response earlier than clinical detection (28, 29). However, these studies are mostly retrospective design, lacking high-level medical evidence, and some results were even inconsistent. Therefore, we conducted this meta-analysis to comprehensively investigate the predictive value of ctDNA for advanced NSCLC patients who received ICI therapy.
Method
The authors declare that all supporting data, study materials and analytic methods within the article and the online supporting information are available to other researchers. This systematic review was performed in adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (30). The PRISMA checklist is provided in Supplementary Table S1 .
Search Strategy
The systematic search of the scientific literature was performed. The search was conducted up to November 2020 in PubMed, EMBASE, Web of Science, and the Cochrane Library database. The main keywords used for the online search were “Circulating Tumor DNA,” “Carcinoma, Non-Small Cell Lung,” “Immune Checkpoint Inhibitor.” The full online search strategies were demonstrated in Supplementary Text S1 . We also manually examined the references of each screened study until no additional articles could be added.
Exclusion and Inclusion Criteria
Studies were selected if they met the following inclusion criteria (1): patients with advanced NSCLC; (2) patients received ICIs alone or ICI-based therapy; (3) ctDNA was analyzed in these groups; (4) information on the clinical response or prognosis of these patients were provided; (5) if multiple studies from the same populations were available, to avoid repetition information, only the one with the largest sample size was included. Reviews, case reports, conference reports, abstracts, phase I studies and non-English publications were excluded. Endnote (Thomson Research Soft; Stanford, Connecticut, the United States) was used to select and screen the literature.
Data Extraction
Data extraction and analyses were performed by 2 independent reviewers (HW and FZ). Any disagreement was discussed with the senior author (XC). Extracted study characteristics included: first author, publication year, country of the study, number of patients who underwent ICIs alone or combined therapy, gender, median/mean age, histological types, stage, smoking history, PD-L1 expression, ECOG PS, follow up duration, drugs, sample, extraction method, detection method, platform, detection time, most mutated genes.
Outcomes
The primary outcomes were overall survival (OS) and progression-free survival (PFS), then the secondary outcome included objective response rate (ORR) with RECIST criteria.
Risk of Bias Assessment
To assesses the quality of non-randomized studies (31), the Newcastle-Ottawa scale was used to assess the risk of bias. The scale assesses risk of bias in the following 3 aspects: selection of the study which include adequate definition and representation of the case, comparability of groups, and ascertainment of exposure and outcome for cases and controls. Studies with score less than 4 were considered as a high risk of bias, those with scores of 4 to 6 were regarded to have an intermediate risk of bias, and scores of 7 or more represented a low risk of bias. The results displayed in Supplementary Table S2
Statistical Analysis
The heterogeneity of different studies was tested by using the Q test. The HRs and ORs with 95% CIs were directly extracted from the research article or calculated using previously published methods, as proposed by Tierney et al. (32). We calculated the I2 to assess the extent of variability attributable to statistical heterogeneity across studies. I2 < 50% and P > 0.10 were interpreted as signifying low-level heterogeneity. Across the studies, if no significant heterogeneity was found, the results were combined with the fixed-effects model (Mantel–Haenszel) (33); otherwise, the random-effects model (DerSimonian-Laird) was used (34). Publication bias was assessed by visual inspection of a funnel plot, Begg’s and Egger’s tests. A sensitivity analysis was performed by serially excluding each study to determine its influence. P values were two-sided and considered significant if less than 0.05. STATA 15.1 software for Mac was used to evaluate the outcomes.
Subgroup Analysis
The following subgroup analyses were performed. Firstly, as already assessed, the patients were stratified with two groups depending on different cutoff value of longitudinal ctDNA dynamic. Then, we also performed subgroup analysis considering that different platforms in studies might provide heterogeneity. The details of groups and outcomes were provided in the results of subgroup analysis.
Results
Study Selection
Of the 427 articles retrieved by the literature search, 97 duplicates were removed, left 330 studies available for screening. 50 studies underwent full-text review, after screening the title and abstract. Of these studies,10 pieces of literature met the inclusion criteria and were chose for the current meta-analysis (7, 35–43). The detailed flow chart is shown in Figure 1 .
Figure 1.

Flow diagram of the study selection.
Study Characteristics
The basic characteristics of the studies are summarized in Table 1 . A total of 1017 patients were included in the study. Data from 3 studies (7, 36, 43) analyzed the PFS, 3 studies (36, 37, 43) considered OS and 4 studies (35, 36, 39, 43) discussed the ORR with the association of baseline ctDNA. 7 studies (37–43) presented PFS, 4 studies (37–39, 43) reported OS and 6 (35, 37–39, 41, 43) studies treated ORR as one of the results in early dynamic assessment of ctDNA. There were 2 studies (36, 38), both of which had 2 independent cohorts, so we used (1) and (2) to distinguish them.
Table 1.
Basic characteristics of the included studies in the present meta-analysis.
| First author | Year | Country | Total cases | Female(%) | Age | Histological types | Stage | Smoking history | PD-L1 Expression | ECOG PS | Follow up duration median or up to(M) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NSCC | SCC | III | IV | current | former | never | positive | negative | unknown | 0 | ≥1 | ||||||||
| Iijima, Y. | 2017 | Japan | 14.00 | 5 (36) | 66 | 10 | 4 | 0 | 14 | 0 | 10 | 4 | 2 | 0 | 12 | 10 | 4 | 10 | |
| Gandara, D. R (1) | 2018 | US | 144.00 | 51 (35) | 62 | 95 | 49 | advanced | 25 | 92 | 27 | NA | NA | NA | 48 | 96 | 27 | ||
| Gandara, D. R (2) | 425.00 | 164 (39) | 63 | 313 | 112 | advanced | 59 | 282 | 84 | NA | NA | NA | 155 | 270 | 27 | ||||
| Goldberg, S. B | 2018 | US | 49.00 | 31 (63) | 67 | 47 | 2 | advanced | 1 | 43 | 5 | NA | NA | NA | NA | NA | 20 | ||
| Raja, R (1) | 2018 | US | 28.00 | 8 (29) | 62 | 10 | 18 | 3 | 25 | 22 | 6 | 13 | 13 | 2 | 10 | 18 | 15 | ||
| Raja, R (2) | 72.00 | 30 (42) | 61 | 57 | 15 | 16 | 56 | 59 | 13 | 58 | 11 | 3 | 27 | 45 | 9 | ||||
| Anagnostou, V. | 2019 | US | 24.00 | 12 (50) | 64 | 16 | 8 | 0 | 24 | 3 | 18 | 3 | NA | NA | NA | NA | NA | 12.7 | |
| Guibert, N | 2019 | French | 97.00 | 37 (38) | NA | 76 | 21 | 11 | 86 | 22 | 63 | 7 | 35 | 40 | 22 | 87(0-2) | 4(≥2) | 24 | |
| Chen, Y. | 2020 | China | 22.00 | 5 (23) | 62 | 10 | 12 | 5 | 17 | 15 | 7 | 11 | 4 | 7 | NA | NA | 15 | ||
| Jia, Q | 2020 | China | 9.00 | 1 (11) | 65 | 6 | 3 | 0 | 9 | 0 | 8 | 1 | NA | NA | NA | NA | NA | 10 | |
| Nabet, B. Y. | 2020 | US | 99.00 | 51 (52) | 65 | 85 | 14 | advanced | 13 | 64 | 22 | 58 | 24 | 17 | NA | NA | 50 | ||
| Zulato, E | 2020 | Italy | 34.00 | NA | 68 | NA | NA | advanced | NA | NA | NA | NA | NA | NA | NA | NA | 13.1 | ||
| First author | Year | Drugs (number) | Previous therapy lines | Sample | Detection method | Platform | Detection time (weeks) | Most mutated genes | |||||||||||
| 0-1 | >1 | ||||||||||||||||||
| Iijima, Y. | 2017 | Nivolumab (14) | NA | plasma | NGS | Ion Proton | baseline, 1, 2, 4, 6,8 | TP53 | |||||||||||
| Gandara, D. R (1) | 2018 | Atezolizumab (144) | 93 | 51 | plasma | NGS | Illumina HiSeq 4000 | baseline | KRAS | ||||||||||
| Gandara, D. R (2) | Atezolizumab (425) | 320 | 105 | plasma | NGS | Illumina HiSeq 4000 | baseline | EGFR | |||||||||||
| Goldberg, S. B | 2018 | anti–PD-1 (36); anti–PD-L1 (2) anti-PD-L1+ID01 inhibitor (2) anti-CTLA-4+anti PD-L1 (7) anti-CTLA-4+anti PD-1 (2) |
40 | 9 | plasma | NGS | Illumina HiSeq 2500 | baseline, 2 | KRAS | ||||||||||
| Raja, R (1) | 2018 | Durvalumab (28) | 11 | 17 | plasma | NGS | Guardant360 | baseline, 6 | TP53 | ||||||||||
| Raja, R (2) | Durvalumab (72) | 0 | 72 | plasma | NGS | Guardant360 | baseline, 6 | TP53 | |||||||||||
| Anagnostou, V. | 2019 | Nivolumab (14); Pembrolizumab (5) Nivolumab+anti-LAG3 (1) Nivolumab+Ipilimumab (1) Pembrolizumab+chemotherapy (3) |
NA | plasma | NGS | Illumina HiSeq 2500 | baseline, 4 or 8, the time of disease progression |
KRAS | |||||||||||
| Guibert, N | 2019 | Nivolumab (90); Pembrolizumab (7) | 57 | 40 | plasma | NGS | Illumina NextSeq 500 | baseline, 4 | KRAS | ||||||||||
| Chen, Y. | 2020 | Camrelizumab + Apatinib (22) | 14 | 8 | plasma | NGS | Illumina Novaseq 6000 | baseline | TP53 | ||||||||||
| Jia, Q | 2020 | Durvalumab (4) Tremelimumab+Durvalumab (5) |
NA | plasma | NGS | Illumina Novaseq 6000 | baseline, 8 | TTN | |||||||||||
| Nabet, B. Y. | 2020 | anti–PD-L1 (1); anti–PD-1 (31) anti–PD-1+anti–CTLA-4 (5) anti–PD-1+Chemotherapy (5) |
41 | 58 | plasma | NGS | Illumina HiSeq4000 | baseline, the time of the second infusion |
TP53 | ||||||||||
| Zulato, E | 2020 | Nivolumab (12) Pembrolizumab (18) Atezolizumab (4) |
NA | plasma | ddPCR | Bio-Rad QX200 | baseline, first radiological restaging |
KRAS | |||||||||||
NSCC, Non-squamous cell carcinoma; SCC, Squamous cell carcinoma; NA, not applicable; NGS, Next-generation sequencing; ddPCR, Droplet Digital PCR; M, months.
The Association of Baseline (Pre-ICI Therapy) ctDNA and Clinical Outcomes
4 cohorts from 3 studies (36, 37, 43) were included for analyzing the association between baseline ctDNA and OS ( Figure 2A ). Considering that the results were not heterogeneous, we chose fixed effects models. There was no statistical significance between the two groups regarding OS (HR, 1.18; 95% CI, 0.93-1.51; I2<0.1%; p=0.181). Data from 3 studies (7, 36, 43) and 4 cohorts were pooled for the analysis of PFS ( Figure 2B ), with a total of 625 patients. Considering that the results were homogeneous, we also used fixed-effects models. There was still no evident difference between the groups in terms of PFS (HR,0.98; 95% CI, 0.80-1.21; I2 = 38.1%; p=0.865) The results of 4 studies (35, 36, 39, 43) and 5 cohorts were pooled to examine the relationship of baseline detected ctDNA and ORR ( Figure 2C ), with a sample size of 641 patients. The pooled OR in the detected group with ORR (OR,0.89; 95% CI,0.54-1.46; I2 = 7.6%; p=0.641) showed no significant difference between the two groups.
Figure 2.
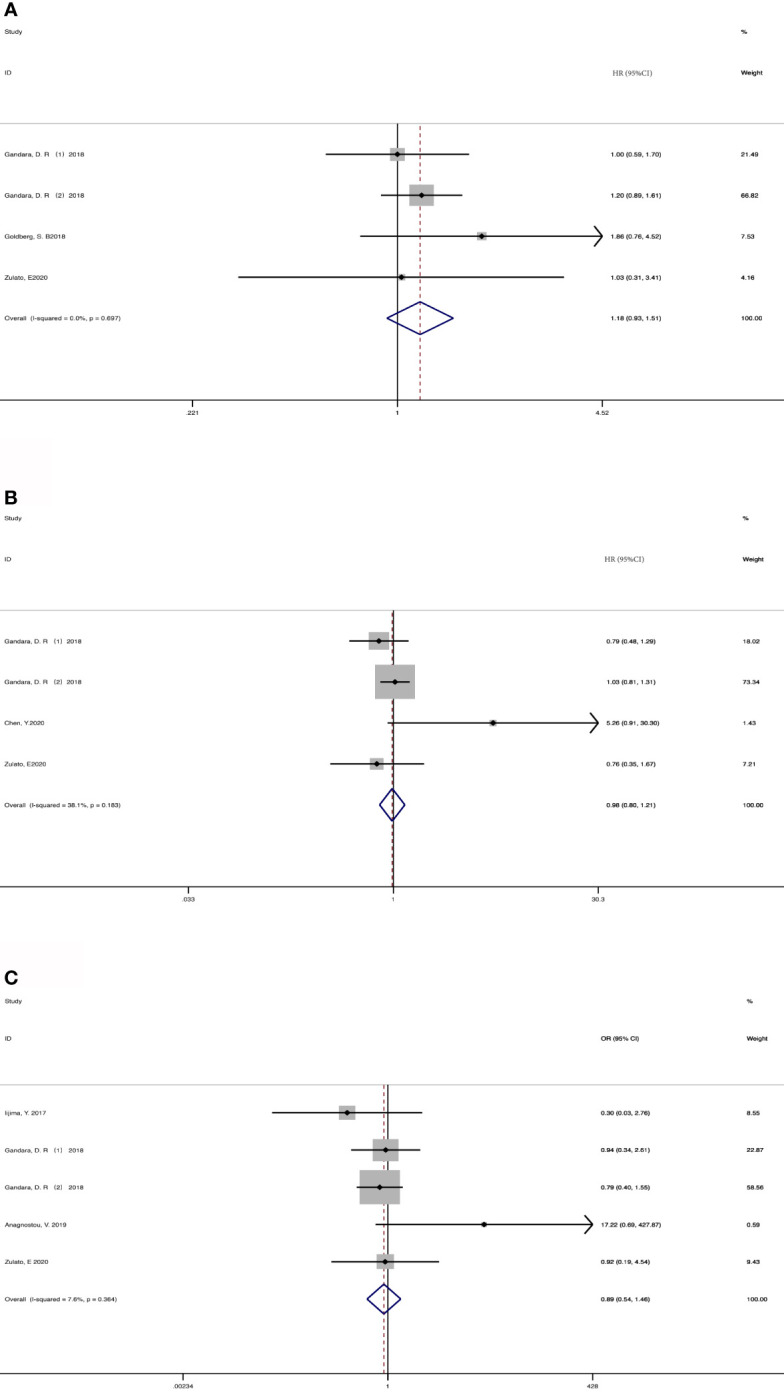
Meta-analysis of the associations between baseline ctDNA and (A) overall survival, (B) progression-free survival, (C) objective response rate. HR, hazard ratio; OR, odds ratio.
The Association of Early Reduction of ctDNA and Clinical Outcomes
207 patients from 5 cohorts in 4 studies (37–39, 43) were included to investigate the pooled association between early reduction of ctDNA and OS. Eight cohorts from 7 studies (37–43) were included to survey the relation between early assessment of ctDNA and PFS, with a sample size of 412 patients. The pooled HR for OS with the fixed-effects model ( Figure 3A ) was 0.19 (95%CI, 0.10-0.35; I2<0.1%; p<0.001); the HR for PFS with random-effects model ( Figure 3B ) was 0.25 (95%CI, 0.16-0.40; I2 = 44.8%; p<0.001); Sensitivity analysis and Star Plot were performed because of the significant heterogeneity ( Figure 4 ). When excluding group 1 in the study by Raja et al. (38), the heterogeneity decreased to I-squared<0.1%; with a pooled HR ( Figure 3C ) of 0.30 (95%CI, 0.22-0.41; p<0.001). In the early reduction ctDNA group, the pooled OR ( Figure 3D ) for ORR in 6 studies (35, 37–39, 41, 43) with 230 patients with fixed-effect models was 0.07 (95% CI,0.03-0.18; I2<0.1%; p<0.001).
Figure 3.

Meta-analysis of the associations between early reduction of ctDNA and (A) overall survival, (B, C) progression-free survival, (D) objective response rate.
Figure 4.

Sensitivity analysis (A) and Star Plot (B) of the included literatures on the reduction of ctDNA with PFS as the result.
Subgroup Analysis in Longitudinal Observation of Patients With ICIs Therapy and Platform
Taking into account these studies, the authors selected different degrees of the reduction of ctDNA during treatment as the cutoff to define the positive group. Therefore, we further adopted subgroup analysis to divide the studies that dropped into the positive group and those with different degrees of decline into two subgroups: a decline of >50% as the threshold to define ctDNA response (subgroup 1) vs others; decreased vs others (subgroup 2). 73 patients from two studies (37, 39) were included in subgroup 1 with a HR ( Figure 5A ) of 0.16 for OS (95%CI, 0.06-0.43; I2 <0.1%, p<0.001), 106 patients from two studies were included in subgroup 2 with a HR ( Figure 5A ) of 0.21 for OS (95%CI, 0.10-0.46; I2 <0.1%, p<0.001). 181 patients from 4 studies (37, 39, 41, 42) were included in subgroup 1 with a HR ( Figure 5B ) of 0.33 for PFS (95%CI, 0.20-0.54; I2 <0.1%, p<0.001). 203 patients from 3 studies (38, 40, 43) were included in subgroup 2 with a HR ( Figure 5B ) of 0.28 for PFS (95% CI, 0.18-0.41; I2 <0.1%, p<0.001). When regarding ORR, 73 patients from 2 studies (37, 39) were included in subgroup 1 with an OR ( Figure 5C ) of 0.03 (95%CI,0.01-0.25; I2<0.1%, p=0.001), and 157 patients from 4 studies (35, 38, 41, 43) in subgroup 2 with an OR ( Figure 5C ) of 0.09 (95%CI,0.03-0.26 I2 <0.1%, p<0.001). Considering that most studies included used illumina platform, the subgroup was utilized to analyze the difference of illumina platform vs other platforms ( Supplement Figure S1 ). The results still maintained coherence in different platforms both in baseline detection and dynamic observation, showing consistent with previous research (44).
Figure 5.

Subgroup analysis the associations between early decrease of ctDNA and (A) overall survival, (B) progression-free survival, (C) objective response rate.
Publication Bias
As shown in Figure 6 , the funnel plots were almost symmetrical and the test results indicated that no publication bias existed regarding the HRs for OS (Begg’s test, p=1.000; Egger’s test, p=0.802), PFS (Begg’s test, p=0.734; Egger’s test, p=0.699) and OR for ORR (Begg’s test, p= 0.806; Egger’s test, p=0.493) in baseline detected ctDNA. However, there are inconsistent results when taking early ctDNA dynamics into consideration, with HRs for OS (Begg’s test, p=0.308; Egger’s test, p=0.023) or PFS (Begg’s test, p=0.230; Egger’s test, p=0.160) and OR for ORR (Begg’s test, p= 0.548; Egger’s test, p=0.009), suggesting that publication bias might exist among these studies.
Figure 6.

Publication bias for the association of detected baseline ctDNA with (A) overall survival, (B) progression-free survival, (C) objective response rate and (D) the relationship of early decreased ctDNA with OS; (E) PFS; (F) ORR.
Discussion
To our knowledge, this was the first meta-analysis to comprehensively investigate predictive significance of ctDNA in advanced NSCLC patients treated with ICI therapy. The current study found that early reduction of ctDNA was associated with improved PFS, OS and ORR while there was no significant association between baseline ctDNA and clinical outcomes.
The concept of monitoring tumor burden and therefore biological effects of treatment by analyzing circulating biomarkers has been known for long, but only recently the availability of techniques able to detect ctDNA has opened new perspectives (17, 45). In lung cancer, the first experience concern EGFR-mutated disease (46). The use of ctDNA as a quantitative biomarker for assessment of ICI response has been investigated in prior studies (47–50), most of which have focused on tracking driver mutations in patients using digital PCR or allele-specific PCR. Even previous studies concluded that pretreatment ctDNA level appears to be an independent, inversely prognostic variable across tumor types, characterized by an association with OS and other known prognostic variables, but not with ORR (51). In this meta-analysis, we did not find a significant association between baseline ctDNA and clinical outcomes. Compared with tumor tissue, the abundance of tumor DNA in plasma samples is relatively low, which poses a great challenge to the sensitivity of plasma detection. False-negative results may occur due to insufficient plasma ctDNA content or lacking of inclusion of altered genes in the targeted NGS panel (21). On the other hand, false-positive results may also occur because of germline variants or the presence of somatic mutations in hematopoietic stem cells owing to clonal hematopoiesis, although most plasma ctDNA assays use matched sequencing of white blood cells (52–54), there still be sequencing errors and artifacts (55). A recent study found that high allele frequency blood TMB was strongly correlated with the ctDNA amount (56). However, high allele frequency blood TMB was a negative prognostic factor rather than a predictive factor (56), this may partially explain that there was no significant association between baseline ctDNA and clinical outcomes.
Interestingly, in this meta-analysis, patients with the reduced dynamic ctDNA obviously obtained more clinical benefits from ICI therapy. The early reduction of ctDNA may reflect an early response of tumors to effective treatment. This was consistent with previous studies, the amount of ctDNA may be an independent factor to predict the efficacy of patients receiving ICIs, and combined with other predictive indicators can better distinguish potential benefit populations (42). Subgroup analysis also indicated that a decline of >50% as a threshold to define ctDNA response and even achievement of undetectable ctDNA may prove to be a stronger predictor of long-term response, compared with just defining ctDNA response as decrease during ICIs therapy, and may identify patients who comprise the “tail” of the survival curve (57). Nevertheless, it still needs prospective studies to confirm these findings. Interestingly, some studies report a transient spike preceding a decline in ctDNA levels in a subset of patients, likely reflecting DNA release as tumor cells are killed. It would be important to avoid misinterpreting such a spike as disease progression (37, 58, 59).
There still were some limitations in our analysis. Firstly, all data were extracted from retrospective or post-hoc analysis studies. Secondly, the quality of data was heterogeneous as several pieces of important information such as prior therapy were not consistently reported. Finally, a high proportion of patients in these studies had KRAS and TP53 mutations. As TP53 and KRAS mutations showed remarkable clinical benefits from ICIs (60), it remains undermined that whether detecting TP53 and KRAS in ctDNA for predicting the response to ICIs was as effective as total ctDNA.
In summary, this current study suggested that early reduction of ctDNA was associated with improved PFS, OS and ORR in advanced NSCLC patients treated with ICIs. Further large-scale and rigorously designed prospective studies are still warranted to verify its clinical value. In the future, clinical trials will be conducted in NSCLC patients to determine whether ctDNA could be selected as a significant factor to monitor clinical response to ICI therapy.
Data Availability Statement
The original contributions presented in the study are included in the article/ Supplementary Material . Further inquiries can be directed to the corresponding authors.
Author Contributions
HW and FZ collected the relevant papers and data and drafted the manuscript text. HW, MQ and XL performed statistical analyses. HW, CZ, and LC performed the quality assessment. XC and CCZ gave critical comments and revised the paper. All authors contributed to the article and approved the submitted version.
Funding
This study was supported in part by grants from the Shanghai “Rising Stars of Medical Talent” Youth Development Program (to FZ) National Natural Science Foundation of China (No. 81703020), Medical Guidance Project of Shanghai Science and Technology Commission (No. 17411969200), and Shanghai Innovative Collaboration Project (No. 2020CXJQ02).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.671874/full#supplementary-material
Subgroup analysis of the different platforms in baseline detection with (A) overall survival, (B) progression-free survival, (C) objective response rate and in dynamic ctDNA with (D) overall survival, (E) progression-free survival, (F) objective response rate. HR, hazard ratio; OR, odds ratio.
References
- 1. Zhou F, Qiao M, Zhou CC. The Cutting-Edge Progress of Immune-Checkpoint Blockade in Lung Cancer. Cell Mol Immunol (2020) 18(2):279–93. 10.1038/s41423-020-00577-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Sharma P, Hu-Lieskovan S, Wargo JA, Ribas A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell (2017) 168(4):707–23. 10.1016/j.cell.2017.01.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kato S, Goodman A, Walavalkar V, Barkauskas DA, Sharabi A, Kurzrock R. Hyperprogressors After Immunotherapy: Analysis of Genomic Alterations Associated With Accelerated Growth Rate. Clin Cancer Res Off J Am Assoc Cancer Res (2017) 23(15):4242–50. 10.1158/1078-0432.CCR-16-3133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Friedman CF, Proverbs-Singh TA, Postow MA. Treatment of the Immune-Related Adverse Effects of Immune Checkpoint Inhibitors: A Review. JAMA Oncol (2016) 2(10):1346–53. 10.1001/jamaoncol.2016.1051 [DOI] [PubMed] [Google Scholar]
- 5. Hallqvist A, Rohlin A, Raghavan S. Immune Checkpoint Blockade and Biomarkers of Clinical Response in non-Small Cell Lung Cancer. Scand J Immunol (2020) 92(6):e12980. 10.1111/sji.12980 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Galon J, Bruni D. Approaches to Treat Immune Hot, Altered and Cold Tumours With Combination Immunotherapies. Nat Rev Drug Discov (2019) 18(3):197–218. 10.1038/s41573-018-0007-y [DOI] [PubMed] [Google Scholar]
- 7. Chen Y, Li XB, Liu GF, Chen SF, Xu MY, Song LL, et al. ctDNA Concentration, MIKI67 Mutations and Hyper-Progressive Disease Related Gene Mutations Are Prognostic Markers for Camrelizumab and Apatinib Combined Multiline Treatment in Advanced NSCLC. Front Oncol (2020) 10:1706–17. 10.3389/fonc.2020.01706 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Pessoa LS, Heringer M, Ferrer VP. ctDNA as a Cancer Biomarker: A Broad Overview. Crit Rev Oncol Hematol (2020) 155:103109. 10.1016/j.critrevonc.2020.103109 [DOI] [PubMed] [Google Scholar]
- 9. Parkinson CA, Gale D, Piskorz AM, Biggs H, Hodgkin C, Addley H, et al. Exploratory Analysis of TP53 Mutations in Circulating Tumour DNA as Biomarkers of Treatment Response for Patients With Relapsed High-Grade Serous Ovarian Carcinoma: A Retrospective Study. PloS Med (2016) 13(12):e1002198. 10.1371/journal.pmed.1002198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Thierry AR, Mouliere F, Gongora C, Ollier J, Robert B, Ychou M, et al. Origin and Quantification of Circulating DNA in Mice With Human Colorectal Cancer Xenografts. Nucleic Acids Res (2010) 38(18):6159–75. 10.1093/nar/gkq421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Kamat AA, Bischoff FZ, Dang D, Baldwin MF, Han LY, Lin YG, et al. Circulating Cell-Free DNA: A Novel Biomarker for Response to Therapy in Ovarian Carcinoma. Cancer Biol Ther (2006) 5(10):1369–74. 10.4161/cbt.5.10.3240 [DOI] [PubMed] [Google Scholar]
- 12. Bettegowda C, Sausen M, Leary R, Kinde I, Wang Y, Agrawal N, et al. Detection of Circulating Tumor DNA in Early- and Late-Stage Human Malignancies. Sci Trans Med (2014) 6:224ra24. 10.1126/scitranslmed.3007094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Yi X, Ma J, Guan Y, Chen R, Yang L, Xia X. The Feasibility of Using Mutation Detection in ctDNA to Assess Tumor Dynamics. Int J Cancer (2017) 140(12):2642–7. 10.1002/ijc.30620 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Ossandon MR, Agrawal L, Bernhard EJ, Conley BA, Dey SM, Divi RL, et al. Circulating Tumor DNA Assays in Clinical Cancer Research. J Natl Cancer Inst (2018) 110(9):929–34. 10.1093/jnci/djy105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Pantel K, Alix-Panabières C. Liquid Biopsy and Minimal Residual Disease - Latest Advances and Implications for Cure. Nat Rev Clin Oncol (2019) 16(7):409–24. 10.1038/s41571-019-0187-3 [DOI] [PubMed] [Google Scholar]
- 16. Cabel L, Proudhon C, Romano E, Girard N, Lantz O, Stern MH, et al. Clinical Potential of Circulating Tumour DNA in Patients Receiving Anticancer Immunotherapy. Nat Rev Clin Oncol (2018) 15(10):639–50. 10.1038/s41571-018-0074-3 [DOI] [PubMed] [Google Scholar]
- 17. Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, et al. Circulating Mutant DNA to Assess Tumor Dynamics. Nat Med (2008) 14(9):985–90. 10.1038/nm.1789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Yao W, Mei C, Nan X, Hui L. Evaluation and Comparison of In Vitro Degradation Kinetics of DNA in Serum, Urine and Saliva: A Qualitative Study. Gene (2016) 590(1):142–8. 10.1016/j.gene.2016.06.033 [DOI] [PubMed] [Google Scholar]
- 19. Overman MJ, Modak J, Kopetz S, Murthy R, Yao JC, Hicks ME, et al. Use of Research Biopsies in Clinical Trials: Are Risks and Benefits Adequately Discussed? J Clin Oncol (2013) 31(1):17–22. 10.1200/JCO.2012.43.1718 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Fazel R, Krumholz HM, Wang Y, Ross JS, Chen J, Ting HH, et al. Exposure to Low-Dose Ionizing Radiation From Medical Imaging Procedures. N Engl J Med (2009) 361(9):849–57. 10.1056/NEJMoa0901249 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Cheng ML, Pectasides E, Hanna GJ, Parsons HA, Choudhury AD, Oxnard GR. Circulating Tumor DNA in Advanced Solid Tumors: Clinical Relevance and Future Directions. CA Cancer J Clin (2020) 71(2):176–90. 10.3322/caac.21650 [DOI] [PubMed] [Google Scholar]
- 22. Rolfo C, Mack PC, Scagliotti GV, Baas P, Barlesi F, Bivona TG, et al. Liquid Biopsy for Advanced Non-Small Cell Lung Cancer (NSCLC): A Statement Paper From The IASLC. J Thorac Oncol (2018) 13(9):1248–68. 10.1016/j.jtho.2018.05.030 [DOI] [PubMed] [Google Scholar]
- 23. Sabari JK, Offin M, Stephens D, Ni A, Lee A, Pavlakis N, et al. A Prospective Study of Circulating Tumor DNA to Guide Matched Targeted Therapy in Lung Cancers. J Natl Cancer Inst (2019) 111(6):575–83. 10.1093/jnci/djy156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Forshew T, Murtaza M, Parkinson C, Gale D, Tsui DW, Kaper F, et al. Noninvasive Identification and Monitoring of Cancer Mutations by Targeted Deep Sequencing of Plasma DNA. Sci Transl Med (2012) 4(136):136ra68. 10.1126/scitranslmed.3003726 [DOI] [PubMed] [Google Scholar]
- 25. Dawson SJ, Tsui DW, Murtaza M, Biggs H, Rueda OM, Chin SF, et al. Analysis of Circulating Tumor DNA to Monitor Metastatic Breast Cancer. N Engl J Med (2013) 368(13):1199–209. 10.1056/NEJMoa1213261 [DOI] [PubMed] [Google Scholar]
- 26. Newman AM, Bratman SV, To J, Wynne JF, Eclov NC, Modlin LA, et al. An Ultrasensitive Method for Quantitating Circulating Tumor DNA With Broad Patient Coverage. Nat Med (2014) 20(5):548–54. 10.1038/nm.3519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Gray ES, Rizos H, Reid AL, Boyd SC, Pereira MR, Lo J, et al. Circulating Tumor DNA to Monitor Treatment Response and Detect Acquired Resistance in Patients With Metastatic Melanoma. Oncotarget (2015) 6(39):42008–18. 10.18632/oncotarget.5788 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Schreuer M, Meersseman G, Van Den Herrewegen S, Jansen Y, Chevolet I, Bott A, et al. Quantitative Assessment of BRAF V600 Mutant Circulating Cell-Free Tumor DNA as a Tool for Therapeutic Monitoring in Metastatic Melanoma Patients Treated With BRAF/MEK Inhibitors. J Transl Med (2016) 14:95. 10.1186/s12967-016-0852-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Marchetti A, Palma JF, Felicioni L, De Pas TM, Chiari R, Del Grammastro M, et al. Early Prediction of Response to Tyrosine Kinase Inhibitors by Quantification of EGFR Mutations in Plasma of NSCLC Patients. J Thorac Oncol (2015) 10(10):1437–43. 10.1097/JTO.0000000000000643 [DOI] [PubMed] [Google Scholar]
- 30. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Int J Surg (2010) 8(5):336–41. 10.1016/j.ijsu.2010.02.007 [DOI] [PubMed] [Google Scholar]
- 31. Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. Ottawa: Ottawa Hospital Research Institute; (2011). Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp [Google Scholar]
- 32. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical Methods for Incorporating Summary Time-to-Event Data Into Meta-Analysis. Trials (2007) 8:16. 10.1186/1745-6215-8-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Overton R. A Comparison of Fixed-Effects and Mixed (Random-Effects) Models for Meta-Analysis Tests of Moderator Variable Effects. Psychol Methods (1998) 3:354–79. 10.1037/1082-989X.3.3.354 [DOI] [Google Scholar]
- 34. DerSimonian R, Kacker R. Random-Effects Model for Meta-Analysis of Clinical Trials: An Update. Contemp Clin Trials (2007) 28(2):105–14. 10.1016/j.cct.2006.04.004 [DOI] [PubMed] [Google Scholar]
- 35. Iijima Y, Hirotsu Y, Amemiya K, Ooka Y, Mochizuki H, Oyama T, et al. Very Early Response of Circulating Tumour–Derived DNA in Plasma Predicts Efficacy of Nivolumab Treatment in Patients With Non–Small Cell Lung Cancer. Eur J Cancer (2017) 86:349–57. 10.1016/j.ejca.2017.09.004 [DOI] [PubMed] [Google Scholar]
- 36. Gandara DR, Paul SM, Kowanetz M, Schleifman E, Zou W, Li Y, et al. Blood-Based Tumor Mutational Burden as a Predictor of Clinical Benefit in non-Small-Cell Lung Cancer Patients Treated With Atezolizumab. Nat Med (2018) 24(9):1441–8. 10.1038/s41591-018-0134-3 [DOI] [PubMed] [Google Scholar]
- 37. Goldberg SB, Narayan A, Kole AJ, Decker RH, Teysir J, Carriero NJ, et al. Early Assessment of Lung Cancer Immunotherapy Response via Circulating Tumor DNA. Clin Cancer Res (2018) 24(8):1872–80. 10.1158/1078-0432.Ccr-17-1341 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Raja R, Kuziora M, Brohawn PZ, Higgs BW, Gupta A, Dennis PA, et al. Early Reduction in ctDNA Predicts Survival in Patients With Lung and Bladder Cancer Treated With Durvalumab. Clin Cancer Res (2018) 24(24):6212–22. 10.1158/1078-0432.Ccr-18-0386 [DOI] [PubMed] [Google Scholar]
- 39. Anagnostou V, Forde PM, White JR, Niknafs N, Hruban C, Naidoo J, et al. Dynamics of Tumor and Immune Responses During Immune Checkpoint Blockade in Non–Small Cell Lung Cancer. Cancer Res (2019) 79(6):1214–25. 10.1158/0008-5472.CAN-18-1127 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Guibert N, Jones G, Beeler JF, Plagnol V, Morris C, Mourlanette J, et al. Targeted Sequencing of Plasma Cell-Free DNA to Predict Response to PD1 Inhibitors in Advanced Non-Small Cell Lung Cancer. Lung Cancer (2019) 137:1–6. 10.1016/j.lungcan.2019.09.005 [DOI] [PubMed] [Google Scholar]
- 41. Jia Q, Chiu L, Wu S, Bai J, Peng L, Zheng L, et al. Tracking Neoantigens by Personalized Circulating Tumor DNA Sequencing During Checkpoint Blockade Immunotherapy in Non-Small Cell Lung Cancer. Adv Sci (Weinh) (2020) 7(9):1903410. 10.1002/advs.201903410 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Nabet BY, Esfahani MS, Moding EJ, Hamilton EG, Chabon JJ, Rizvi H, et al. Noninvasive Early Identification of Therapeutic Benefit From Immune Checkpoint Inhibition. Cell (2020) 183(2):363–76.e13. 10.1016/j.cell.2020.09.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Zulato E, Attili I, Pavan A, Nardo G, Del Bianco P, Bragadin AB, et al. Early Assessment of KRAS Mutation in cfDNA Correlates With Risk of Progression and Death in Advanced Non-Small-Cell Lung Cancer. Br J Cancer (2020) 123(1):81–91. 10.1038/s41416-020-0833-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Boland JF, Chung CC, Roberson D, Mitchell J, Zhang X, Im KM, et al. The New Sequencer on the Block: Comparison of Life Technology’s Proton Sequencer to an Illumina HiSeq for Whole-Exome Sequencing. Hum Genet (2013) 132(10):1153–63. 10.1007/s00439-013-1321-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Alix-Panabieres C, Pantel K. Clinical Applications of Circulating Tumor Cells and Circulating Tumor DNA as Liquid Biopsy. Cancer Discov (2016) 6(5):479–91. 10.1158/2159-8290.CD-15-1483 [DOI] [PubMed] [Google Scholar]
- 46. Sacher AG, Paweletz C, Dahlberg SE, Alden RS, O’Connell A, Feeney N, et al. Prospective Validation of Rapid Plasma Genotyping for the Detection of EGFR and KRAS Mutations in Advanced Lung Cancer. JAMA Oncol (2016) 2(8):1014–22. 10.1001/jamaoncol.2016.0173 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Lipson EJ, Velculescu VE, Pritchard TS, Sausen M, Pardoll DM, Topalian SL, et al. Circulating Tumor DNA Analysis as a Real-Time Method for Monitoring Tumor Burden in Melanoma Patients Undergoing Treatment With Immune Checkpoint Blockade. J Immunother Cancer (2014) 2(1):42. 10.1186/s40425-014-0042-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Xi L, Pham TH, Payabyab EC, Sherry RM, Rosenberg SA, Raffeld M. Circulating Tumor DNA as an Early Indicator of Response to T-Cell Transfer Immunotherapy in Metastatic Melanoma. Clin Cancer Res (2016) 22(22):5480–6. 10.1158/1078-0432.Ccr-16-0613 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Cabel L, Riva F, Servois V, Livartowski A, Daniel C, Rampanou A, et al. Circulating Tumor DNA Changes for Early Monitoring of Anti-PD1 Immunotherapy: A Proof-of-Concept Study. Ann Oncol (2017) 28(8):1996–2001. 10.1093/annonc/mdx212 [DOI] [PubMed] [Google Scholar]
- 50. Lee JH, Long GV, Boyd S, Lo S, Menzies AM, Tembe V, et al. Circulating Tumour DNA Predicts Response to Anti-PD1 Antibodies in Metastatic Melanoma. Ann Oncol (2017) 28(5):1130–6. 10.1093/annonc/mdx026 [DOI] [PubMed] [Google Scholar]
- 51. Zhang Q, Luo J, Wu S, Si H, Gao C, Xu W, et al. Prognostic and Predictive Impact of Circulating Tumor DNA in Patients With Advanced Cancers Treated With Immune Checkpoint Blockade. Cancer Discov (2020) 10(12):1842–53. 10.1158/2159-8290.CD-20-0047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Steensma DP, Bejar R, Jaiswal S, Lindsley RC, Sekeres MA, Hasserjian RP, et al. Clonal Hematopoiesis of Indeterminate Potential and its Distinction From Myelodysplastic Syndromes. Blood (2015) 126(1):9–16. 10.1182/blood-2015-03-631747 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Razavi P, Li BT, Brown DN, Jung B, Hubbell E, Shen R, et al. High-Intensity Sequencing Reveals the Sources of Plasma Circulating Cell-Free DNA Variants. Nat Med (2019) 25(12):1928–37. 10.1038/s41591-019-0652-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Coombs CC, Zehir A, Devlin SM, Kishtagari A, Syed A, Jonsson P, et al. Therapy-Related Clonal Hematopoiesis in Patients With Non-Hematologic Cancers Is Common and Associated With Adverse Clinical Outcomes. Cell Stem Cell (2017) 21(3):374–82.e4. 10.1016/j.stem.2017.07.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. El-Deiry WS, Goldberg RM, Lenz HJ, Shields AF, Gibney GT, Tan AR, et al. The Current State of Molecular Testing in the Treatment of Patients With Solid Tumors, 2019. CA Cancer J Clin (2019) 69(4):305–43. 10.3322/caac.21560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Wang ZJ, Duan JC, Wang GQ, Zhao J, Xu JC, Han JF, et al. Allele Frequency-Adjusted Blood-Based Tumor Mutational Burden as a Predictor of Overall Survival for Patients With NSCLC Treated With PD-(L)1 Inhibitors. J Thoracic Oncol (2020) 15(4):556–67. 10.1016/j.jtho.2019.12.001 [DOI] [PubMed] [Google Scholar]
- 57. Hellmann MD, Kris MG, Rudin CM. Medians and Milestones in Describing the Path to Cancer Cures: Telling "Tails". JAMA Oncol (2016) 2(2):167–8. 10.1001/jamaoncol.2015.4345 [DOI] [PubMed] [Google Scholar]
- 58. Deshpande S, Tytarenko RG, Wang Y, Boyle EM, Ashby C, Schinke CD, et al. Monitoring Treatment Response and Disease Progression in Myeloma With Circulating Cell-Free DNA. Eur J Haematol (2020) 106(2):230–40. 10.1111/ejh.13541 [DOI] [PubMed] [Google Scholar]
- 59. Husain H, Melnikova VO, Kosco K, Woodward B, More S, Pingle SC, et al. Monitoring Daily Dynamics of Early Tumor Response to Targeted Therapy by Detecting Circulating Tumor DNA in Urine. Clin Cancer Res (2017) 23(16):4716–23. 10.1158/1078-0432.Ccr-17-0454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Dong ZY, Zhong WZ, Zhang XC, Su J, Xie Z, Liu SY, et al. Potential Predictive Value of TP53 and KRAS Mutation Status for Response to PD-1 Blockade Immunotherapy in Lung Adenocarcinoma. Clin Cancer Res (2017) 23(12):3012–24. 10.1158/1078-0432.Ccr-16-2554 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Subgroup analysis of the different platforms in baseline detection with (A) overall survival, (B) progression-free survival, (C) objective response rate and in dynamic ctDNA with (D) overall survival, (E) progression-free survival, (F) objective response rate. HR, hazard ratio; OR, odds ratio.
Data Availability Statement
The original contributions presented in the study are included in the article/ Supplementary Material . Further inquiries can be directed to the corresponding authors.