

Abstract
目的
探讨一期后路经单侧骶棘肌髂骨瓣入路手术治疗腰骶椎结核的安全性和疗效。
方法
2011 年 8 月—2014 年 10 月,收治 13 例腰骶椎结核患者。采用一期后路保留后方韧带复合体,经单侧骶棘肌髂骨瓣入路行病灶清除、植骨融合、内固定治疗。其中男 8 例,女 5 例;年龄 22~57 岁,平均 35 岁。病程 2~19 个月,平均 6.7 个月。术前美国脊髓损伤协会(ASIA)分级为 B 级 2 例、C 级 4 例、D 级 5 例、E 级 2 例;Oswestry 功能障碍指数(ODI)为(36.4±5.7)分;腰骶角为(20.7±0.7)°;红细胞沉降率(erythrocyte sedimentation rate,ESR)为(63.4±8.4)mm/1 h,C 反应蛋白为(38.8±5.2)mmol/L。记录手术时间和术中出血量;末次随访时 ODI、ASIA 分级、腰骶角及 ESR;采用 Bridwell 标准判断椎间植骨融合情况。
结果
手术时间 150~240 min,平均 190 min;术中出血量 420~850 mL,平均 610 mL。术中未出现大血管、硬膜囊、神经根及腰骶丛损伤。3 例切口延迟愈合,其余患者切口均 Ⅰ 期愈合;未见切口感染及窦道形成。13 例患者均获随访,随访时间 1.5~6.1 年,平均 2.8 年。随访期间无结核中毒症状,无脑脊液漏、内固定物松动断裂;8 例男性患者均未出现逆行射精、勃起障碍等并发症。患者椎间植骨均融合,融合时间 4.2~9.9 个月,平均 6.4 个月;髂骨瓣均骨性愈合。末次随访时,ODI 为(7.2±3.5)分,腰骶角为(31.2±0.5)°,ESR 为(9.8±2.5)mm/1 h,均较术前显著改善(P<0.05);ASIA 分级为 D 级 2 例、E 级 11 例,较术前显著改善(Z=–3.168,P=0.002)。
结论
一期后路经单侧骶棘肌髂骨瓣入路手术治疗腰骶椎结核安全、有效。
Keywords: 腰骶椎结核, 后路手术, 骶棘肌髂骨瓣
Abstract
Objective
To evaluate the safety and effectiveness of one-stage posterior surgery via unilateral musculussacrospinalis iliac flap approach in treatment of lumbosacral tuberculosis.
Methods
Between August 2011 and October 2014, 13 patients with lumbosacral tuberculosis were treated by one-stage posterior reserved posterior ligament complex, lesion debridement, bone graft fusion, and internal fixation via unilateral musculussacrospinalis iliac flap approach. There were 8 males and 5 females, aged from 22 to 57 years, with an average age of 35 years. The disease duration ranged from 2 to 19 months, with an average of 6.7 months. According to the American Spinal Injury Association (ASIA) classification criteria, the patients were graded as grade B in 2 cases, grade C in 4 cases, grade D in 5 cases, and grade E in 2 cases before operation. The preoperative Oswestry disability index (ODI) was 36.4±5.7; the preoperative lumbosacral angle was (20.7±0.7)°; the preoperative erythrocyte sedimentation rate (ESR) was (63.4±8.4) mm/1 h; and the preoperative C-reactive protein (CRP) was (38.8±5.2) mmol/L. The operation time and intraoperative blood loss were recorded. The ODI, ASIA grade, lumbosacral angle, and ESR were recorded at last follow-up. Bridwell criterion was used to judge the interbody fusion.
Results
The operation time was 150-240 minutes (mean, 190 minutes), and the intraoperative blood loss was 420-850 mL (mean, 610 mL). No major blood vessel, dural sac, nerve root, and lumbosacral plexus injuries occurred during the operation. Delayed wound healing occurred in 3 cases, and primary wound healing achieved in the other patients. No wound infection or sinus formation was found. All 13 patients were followed up 1.5-6.1 years (mean, 2.8 years). During the follow-up period, there was no tubercular symptom, cerebrospinal fluid leakage, loosening and rupture of internal fixator; and no complications such as retrograde ejaculation and erectile dysfunction occurred in 8 male patients. Solid spinal fusion obtained in all patients with the mean fusion time of 6.4 months (range, 4.2-9.9 months); and all iliac osteotomies healed. At last follow-up, the ODI was 7.2±3.5, the lumbosacral angle was (31.2±0.5)°, and ESR was (9.8±2.5) mm/1 h, all of which improved significantly when compared with pre-operative ones (P<0.05). The patients were classified as grade D in 2 cases and grade E in 11 cases, which improved significantly when compared with preoperative ones (Z=–3.168, P=0.002).
Conclusion
One-stage posterior surgery via unilateral musculussacrospinalis iliac flap approach in treatment of lumbosacral tuberculosis is effective and safe.
Keywords: Lumbosacral tuberculosis, posterior approach surgery, musculussacrospinalis iliac flap
世界卫生组织(WHO)2018 年全球结核报告显示,结核病是全球十大致死疾病之一,2017 年全球结核死亡病例超过 130 万[1]。脊柱结核是一种常见的肺外结核,占肌骨系统结核的 44.3%~50%[2-3];可导致后凸畸形、神经症状甚至脊髓压迫瘫痪[4-5]。脊柱结核是系统性疾病,除正规抗结核治疗外,对并发脊柱畸形或神经症状患者还需手术治疗[6-7]。
脊柱腰骶段是非常特殊的应力集中节段,腰骶椎活动度差,前方有大血管分叉,同时侧方有髂骨阻挡[8]。腰骶椎结核比较少见,仅占所有脊柱结核的 2%~3%[9],由于其特殊的解剖学和生物力学特征,关于腰骶椎结核手术入路一直存在争议。前路手术解剖结构复杂,容易出现大血管神经损伤,同时前方固定困难且固定强度欠佳。前后联合入路手术时间长、创伤大,理论上存在将主要位于前方的感染播散至后方的风险。近年来,后路手术受到部分学者青睐,并取得良好疗效[10-14],但存在手术暴露及操作空间有限、病灶清除不彻底、破坏后方韧带复合体等脊柱稳定结构的问题。
2011 年 8 月—2014 年 10 月,我们采用一期后路保留后方韧带复合体,经单侧骶棘肌髂骨瓣入路行病灶清除、植骨融合、内固定治疗 13 例腰骶椎结核患者,取得较好疗效。现回顾分析患者临床资料,分析此入路的适应证及技术要点,为临床治疗腰骶椎结核提供一种手术入路选择。报告如下。
1. 临床资料
1.1. 患者选择标准
纳入标准:① 术后病原菌诊断确诊为腰骶椎结核;② 破坏范围≤1 个椎体+2 个相邻椎间隙;③ 腰大肌脓肿相对局限;④ 术前抗结核治疗有效。排除标准:① 合并窦道;② 合并严重内科疾病无法接受手术;③ 开放性活动性肺结核;④ 使用免疫抑制剂或合并 HIV 感染导致免疫力低下;⑤ 多发及跳跃性脊柱结核。本研究通过贵州省人民医院医学伦理委员会批准。
1.2. 一般资料
本组男 8 例,女 5 例;年龄 22~57 岁,平均 35 岁。病程 2~19 个月,平均 6.7 个月。病变节段: L4、5 5 例,L5、S1 4 例,L4~S1 4 例。既往病史:腰椎管狭窄 2 例,肺结核 5 例,消化道结核 1 例。合并腰大肌脓肿 2 例,椎管内脓肿 11 例。均存在下腰痛;伴有神经压迫症状 11 例,根据美国脊髓损伤协会(ASIA)分级为 B 级 2 例、C 级 4 例、D 级 5 例、E 级 2 例。术前 Oswestry 功能障碍指数(ODI)为(36.4±5.7)分,腰骶角为(20.7±0.7)°,红细胞沉降率(erythrocyte sedimentation rate,ESR)为(63.4±8.4)mm/1 h,C 反应蛋白(C-reactive protein,CRP)为(38.8±5.2)mmol/L。
1.3. 治疗方法
1.3.1. 术前准备
术前所有患者行腰椎 CT 检查,了解椎体冠状位及矢状位、横断位破坏范围,亚健康骨质残留椎弓根及附件情况;MRI 检查了解炎性区域位置及范围,有无椎管内脓肿、腰大肌脓肿、髂窝脓肿、骶前脓肿及范围;CT 血管造影了解髂血管分叉情况。术前正规抗结核治疗 4 周,改善全身情况,纠正贫血(血红蛋白>100 g/L),无发热(体温<38℃);ESR 及 CRP 升高不作为手术禁忌。
1.3.2. 手术方法
患者于全麻下取俯卧位,胸部及髂前上棘垫枕避免腹部受压。取腰骶部后正中 L 形切口,尾部呈弧形至病变较严重侧髂后上棘。切开皮肤、皮下组织,剥离椎板上附着的骶棘肌,保留棘上韧带、棘间韧带及对侧椎板并行椎弓根固定。肌骨瓣侧剥离骶棘肌至骶髂关节水平,筋膜下游离其外侧缘至髂后上棘水平。将骶棘肌内侧部分于 S2 水平横行切断,剥离骶骨外板,髂骨瓣横断面与后正中线垂直,位于髂后上棘以远 3 cm;纵断面与骶棘肌外侧缘平行,位于髂后上棘外侧 4 cm,向近端翻起骶棘肌髂骨瓣,并用盐水纱布保护固定于切口近端,使术野充分暴露。对固定节段椎弓根进行开口、扩大、攻丝、骨蜡填塞,暂不植钉。咬除 L4 下关节突及椎板,部分 L5 上关节突及椎板;必要时咬除 S1 上关节突及部分骶骨,如果 L5 椎体大部分破坏,则切除 L5 椎弓根。切除 L5 横突,此时上位神经下行及腰骶丛主干和分支清晰可见。游离上位及下位神经根至腰骶干处,注意保护腰骶丛及分支,必要时用双极电凝止血。保护硬膜及神经根,根据术前 CT 或 MRI 显示范围清除病灶。小心剥离前纵韧带与椎体前缘,勿突破前纵韧带。剥离椎体侧方,如无死骨形成,一般情况下尽可能保留部分椎体侧壁,以减少节段性血管出血可能;一旦出血,用双极电凝及明胶海绵予以止血。根据术前 MRI 显示的椎旁及腰大肌脓肿范围,从腰大肌的后侧面避开腰骶丛进行穿刺,然后进行钝性分离,吸除脓腔脓液及干酪样组织。彻底清除病灶后,修整椎体健康骨面。测量所需钛网高度,选择 19 mm 大直径钛网,修整钛网与椎体亚健康骨面相匹配,钛网内植入自体骨或添加同种异体骨(商品名:拜欧金;北京大清生物技术股份有限公司)填充中心。撑开椎弓根螺钉扩大间隙,从侧后方将钛网斜行放入椎体间,放置过程中避免损伤内侧的硬膜及外侧的上下位神经根。可进一步调整钛网位置,必要时植入双钛网。C 臂 X 线机透视下确认钛网位置后,植棒进行加压、固定,测试钛网稳定程度。冲洗切口,病灶区植入链霉素加异烟肼 2 g。复位并用椎弓根螺钉固定骶棘肌髂骨瓣,严密缝合骨板附着处肌肉筋膜层,修补骶棘肌内侧部分,置负压引流管,逐层缝合关闭切口。
1.4. 术后处理及疗效评价指标
术后负压引流量<50 mL/d 后拔除引流管。采用 3HREZ+xHRE 的抗结核治疗方案,即 3 个月的异烟肼、利福平、吡嗪酰胺、乙胺丁醇四联强化治疗,根据患者病情采用 12~15 个月的个体化异烟肼、利福平、吡嗪酰胺三联巩固治疗。综合患者腰痛症状、术中稳定性重建、术后影像学复查采取个体化康复锻炼方案。
记录手术时间和术中出血量;末次随访时 ODI、ASIA 分级、腰骶角及 ESR;采用 Bridwell 标准[15]判断椎间植骨融合情况。
1.5. 统计学方法
采用 SPSS18.0 统计软件进行分析。计量资料以均数±标准差表示,手术前后比较采用配对 t 检验;等级资料比较采用秩和检验;检验水准 α=0.05。
2. 结果
本组手术时间 150~240 min,平均 190 min;术中出血量 420~850 mL,平均 610 mL。术中未出现大血管、硬膜囊、神经根及腰骶丛损伤。3 例切口延迟愈合,经换药或清创后于术后 3 周左右愈合;其余患者切口均 Ⅰ 期愈合。未见切口感染及窦道形成。13 例患者均获随访,随访时间 1.5~6.1 年,平均 2.8 年。随访期间无低热、盗汗、乏力等结核中毒症状,无脑脊液漏、内固定物松动断裂;8 例男性患者均未出现逆行射精、勃起障碍等并发症。 患者椎间植骨均融合,融合时间 4.2~9.9 个月,平均 6.4 个月;末次随访时根据 Bridwell 标准,植骨达 Ⅰ 级融合 12 例、Ⅱ 级融合 1 例,髂骨瓣均骨性愈合。末次随访时,ODI 为(7.2±3.5)分,腰骶角为(31.2±0.5)°,ESR 为(9.8±2.5)mm/1 h,均较术前显著改善(t=18.650,P=0.018;t=62.540,P=0.034;t=33.280,P=0.007);ASIA 分级为 D 级 2 例、E 级 11 例,较术前显著改善(Z=–3.168,P=0.002)。见图 1。
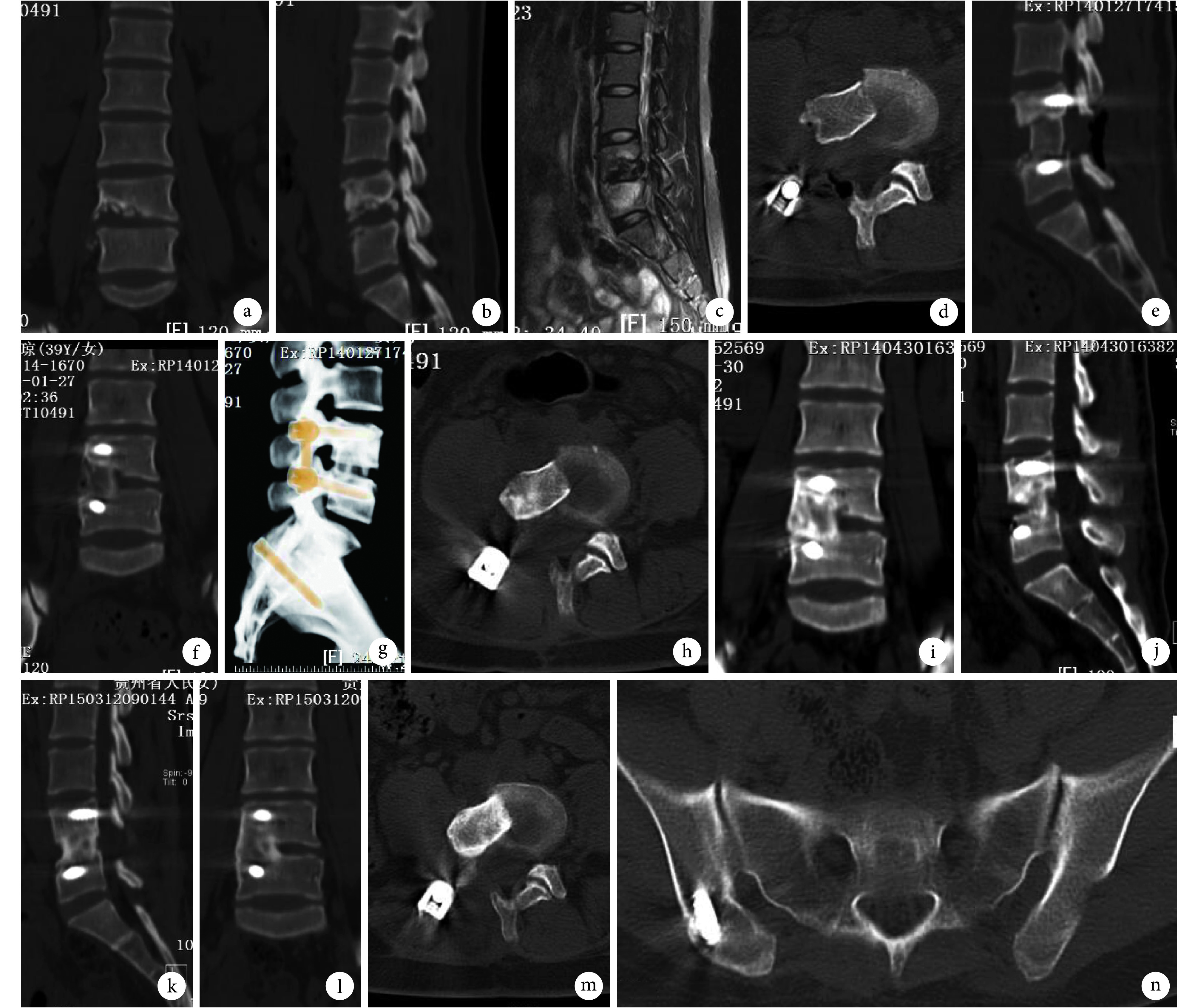
图 1.
A 40-year-old female patient with lumbosacral tuberculosis at L4, 5
患者,女,40 岁,L4、5脊柱结核
a~c. 术前 CT 及 MRI;d~g. 术后即刻 CT 及三维重建;h~j. 术后 3 个月 CT;k~n. 术后 14 个月 CT
a-c. Preoperative CT and MRI; d-g. CT and three-dimensional reconstruction at immediate after operation; h-j. CT at 3 months after operation; k-n. CT at 14 months after operation
3. 讨论
腰骶椎应力集中,故此部位结核病灶清除、充分减压后,必须进行确定的植骨融合内固定,重建其稳定性。腰骶椎结核手术入路是逐渐从前路向后路演变的。腰骶椎结核大部分从椎间隙开始,主要侵犯脊柱的前中柱,可形成骶前或椎管内脓肿。故前路手术可以获得病灶区域的直接暴露,更有利于彻底清除病灶及修复骨缺损。前路手术由 Hodgson 等[16]于 1960 年提出。Song 等[17]报道可以用前外侧入路治疗腰骶椎结核,得到平均 9.5° 的腰骶角改善和脊柱的骨性融合。Li 等[18]回顾性分析了 43 例腰骶椎结核接受前正中腹膜外入路行病灶清创、2 块三皮质同种异体髂骨植骨融合、内固定术,平均随访 34 个月,未发现明显矫形丢失、结核复发、结核性腹膜炎、勃起障碍及逆行射精。他们认为前路手术可提供直接、充分的暴露,对于腰骶椎结核是一种有效的手术入路。但前路固定存在生物力学上的先天不足,Hirano 等[19]及 Weinstein 等[20]均证实椎弓根为椎弓根螺钉提供至少 60% 拔出强度和 80% 的轴向强度,而椎体松质骨只能提供 15%~20% 的拔出强度,提示后路固定强度强于前路。再加上椎体骨质疏松和炎性改变导致内固定物与骨质界面的潜在不稳,使得前路固定强度欠佳,同时不能很好地纠正畸形及防止畸形发生。同时,腰骶椎前方解剖结构复杂,分布有大血管分叉及腰骶神经丛,而结核炎性病灶又导致软组织增厚粘连,故前路手术损伤大血管、神经、输尿管等致命性重要结构的风险更高[21-22],甚至出现无法进行有效内固定的情况。
前后联合入路可以解决单一前路手术内固定强度不足及神经根彻底减压的问题。前后联合入路是治疗腰骶椎结核的主流入路,其优势包括前路直接而彻底的病灶清除、充分的前柱植骨融合获得长期腰骶椎稳定性,以及后路坚强固定恢复腰骶椎序列及稳定性[23-24]。He 等[25]报道前后联合入路可以有效治愈腰骶椎结核,但平均手术时间、出血量及住院时间均高于前路手术。另外前后联合入路往往先行后路固定,导致植骨为嵌入式,不能有效加压。
近年来单一后路手术治疗腰骶椎结核受到了部分学者的青睐,其具有手术创伤小、不易出现致命性大血管神经损伤、可完成 360° 环形减压、可向近远端延伸手术范围来重建严重破坏的责任节段、可获得坚强的三柱固定等优势。Zhang 等[26]报道了 28 例脊柱结核通过单纯后路清创、内固定、用钛合金笼重建,患者均获骨性融合,未见内固定失效,感染均治愈。Jain 等[27]回顾性分析了 28 例腰椎及腰骶椎结核患者,其中 13 例在抗结核治疗后症状无缓解,接受了单纯后路减压椎弓根螺钉后外侧融合,抗结核治疗持续至影像、神经功能恢复正常(9~16 个月)。已有大量关于一期后路手术成功治愈腰骶椎结核的报道[28-33]。对于单一后路手术与前后联合入路手术的对比研究也表明,前者在手术时间、术中出血量、住院时间、手术相关并发症方面更有优势,而且未牺牲植骨融合率、畸形矫正率等方面的指标[34-37]。
本研究小组周焯家等[38]认为,通过单一后路手术即可治疗腰骶椎结核,但大部分主要涉及前中柱的脊柱结核行单一后路手术需要将全椎板切除,这意味着切除了后方正常的骨性及韧带复合体,完全破坏了后柱的稳定机制,易出现顽固腰痛等并发症,一旦出现复发,翻修手术难度明显提高。鉴于此,本研究提出一期后路保留后方韧带复合体,经单侧骶棘肌髂骨瓣入路行病灶清除、椎间椎骨融合、内固定治疗严重腰骶椎结核。近期随访结果显示无结核复发、植骨融合均成功、神经功能保留或恢复满意,未发现严重并发症。该术式优势包括:① 最大限度地保护了脊柱后方结构,对侧植钉也可以通过微创方式进行。② 骶棘肌髂骨瓣截骨操作容易,髂骨瓣血供丰富,容易愈合。③ 骶棘肌髂骨瓣向近端翻起后,临时去除了对术野的阻挡,可直视下处理 L4~S1 横突下的神经、椎弓根外侧节段性血管,便于游离,不易损伤,使清除椎体病灶相对容易。这类似于胸椎后路手术,肋横突关节及部分肋骨切除术后的胸廓塌陷后效应。④ 便于椎间植骨,上下位相邻神经根游离后给予足够的操作通道,钛网或植骨块从侧后方植入,无需更多地牵拉硬膜。⑤ 骶棘肌髂骨瓣向近端翻起,保证了骶棘肌在手术过程中无张力状态,肌肉得到更好保护,髂骨血供丰富,复位固定后愈合速度快,发生不愈合概率低。存在的不足:① 在截骨获取髂骨瓣时,如骨瓣过小会影响固定的牢靠性,一旦发生不愈合,会影响单侧腰背肌的力量,造成一系列并发症;② 游离上位神经根时,椎弓根下方有大量静脉丛伴行,需要用双极电凝止血,有损伤神经根的风险;③ 神经根在与坐骨神经会合之前有吻合支形成腰骶神经丛,有损伤风险;④ 合并腰大肌脓肿时,只能从侧后方引流,没有前路手术视野开阔,腰大肌内干酪样组织清除不彻底,且有损伤腰大肌内血管风险,一旦损伤只能电凝或明胶海绵压迫,无法结扎;⑤ 即便反复冲洗,也不容易彻底清除骶前脓肿,脓肿较大或形成干酪样组织时,需另行切口引流;⑥ 对医生的技术要求高,必须熟悉腰骶部后路的神经、血管解剖结构;⑦ 本组患者切口愈合不良比例较高,考虑可能为切口呈 L 形,早期经验不足,转角位置选择及转角处皮瓣处理欠佳,牵拉较重导致。
综上述,经后路一期保留后方韧带复合体,经一侧经骶棘肌髂骨瓣入路病灶清除、植骨融合、内固定治疗严重的腰骶椎结核,取得了满意的近期疗效。该术式尽可能地保留了脊柱后方韧带复合体结构,很好地显露了病灶区域,病灶清除较彻底,术中出血较少,减少了大血管损伤的风险。术后椎体间植骨相对容易,即刻加压,使植骨块或钛网更加稳定,可促进移植骨融合并防止后凸畸形的发生。注意事项:① 严格掌握手术适应证,适用于后柱椎板破坏<1/2,前柱破坏≤1 个椎体+2 个相邻椎间盘范围,且椎旁脓肿局限;② 术者应具备后路全脊椎切除的技术能力;③ 剥离椎板上附着的骶棘肌,要尽量做到骨膜下剥离,减少因剥离导致的肌肉坏死;④ 在后外侧手术窗内充分游离上下位神经根至腰骶干处,在进行病灶清除及椎间融合时注意保护神经根;⑤ 如无死骨形成,剥离椎体侧方时尽可能保留部分椎体侧壁,以减少节段性血管出血。下一步仍需增加样本量并延长随访时间,进一步研究该术式远期疗效。
志谢:国家卫生健康委员会肺脏免疫性疾病诊治与推广重点实验室
References
- 1.Laura A, Annabel B, Hannah MD, et al Global tuberculosis report 2018. World Health Organization. 2018:1. [Google Scholar]
- 2.Trecarichi EM, Di Meco E, Mazzotta V, et al Tuberculous spondylodiscitis: epidemiology, clinical features, treatment, and outcome. Eur Rev Med Pharmacol Sci. 2012;16(Suppl 2):58–72. [PubMed] [Google Scholar]
- 3.Mor Z, Pinsker G, Cedar N, et al Epidemiology of extra-pulmonary tuberculosis in Israel, 1999-2010. Int J Tuberc Lung Dis. 2013;17(2):229–233. doi: 10.5588/ijtld.12.0375. [DOI] [PubMed] [Google Scholar]
- 4.García-Rodríguez JF, Álvarez-Díaz H, Lorenzo-García MV, et al Extrapulmonary tuberculosis: epidemiology and risk factors. Enferm Infecc Microbiol Clin. 2011;29(7):502–509. doi: 10.1016/j.eimc.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 5.Pigrau-Serrallach C, Rodríguez-Pardo D Bone and joint tuberculosis. Eur Spine J. 2013;22(Suppl 4):556–566. doi: 10.1007/s00586-012-2331-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rajasekaran S Kyphotic deformity in spinal tuberculosis and its management. Int Orthop. 2012;36(2):359–365. doi: 10.1007/s00264-011-1469-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jain AK Tuberculosis of the spine: a fresh look at an old disease. J Bone Joint Surg (Br) 2010;92(7):905–913. doi: 10.1302/0301-620X.92B7.24668. [DOI] [PubMed] [Google Scholar]
- 8.Shah SP, Kulkarni AG S1 tuberculosis treated with segmental lumbopelvic fixation: a case report. Spine (Phila Pa 1976) 2012;37(14):E866–E869. doi: 10.1097/BRS.0b013e3182540579. [DOI] [PubMed] [Google Scholar]
- 9.Rajasekaran S, Shanmugasundaram TK, Prabhakar R, et al Tuberculous lesions of the lumbosacral region. A 15-year follow-up of patients treated by ambulant chemotherapy. Spine (Phila Pa 1976) 1998;23:1163–1167. doi: 10.1097/00007632-199805150-00018. [DOI] [PubMed] [Google Scholar]
- 10.彭琪琪, 欧云生, 朱勇, 等 后路病灶清除植骨内固定联合不同入路腰大肌脓肿清除局部化疗治疗胸腰椎结核. 中国修复重建外科杂志. 2018;32(7):912–919. [Google Scholar]
- 11.Zhang H, Sheng B, Tang M, et al One-stage surgical treatment for upper thoracic spinal tuberculosis by internal fixation, debridement, and combined interbody and posterior fusion via posterior-only approach. Eur Spine J. 2013;22(3):616–623. doi: 10.1007/s00586-012-2470-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rawall S, Mohan K, Nene A Posterior approach in thoracolumbar tuberculosis: a clinical and radiological review of 67 operated cases. Musculoskelet Surg. 2013;97(1):67–75. doi: 10.1007/s12306-012-0235-y. [DOI] [PubMed] [Google Scholar]
- 13.Wu P, Wang XY, Li XG, et al One-stage posterior procedure in treating active thoracic spinal tuberculosis: a retrospective study. Eur J Trauma Emerg Surg. 2015;41(2):189–197. doi: 10.1007/s00068-014-0421-8. [DOI] [PubMed] [Google Scholar]
- 14.Zhang HQ, Lin MZ, Li JS, et al One-stage posterior debridement, transforaminal lumbar interbody fusion and instrumentation in treatment of lumbar spinal tuberculosis: a retrospective case series. Arch Orthop Trauma Surg. 2013;133(3):333–341. doi: 10.1007/s00402-012-1669-2. [DOI] [PubMed] [Google Scholar]
- 15.Bridwell KH, Lenke LG, McEnery KW, et al Anterior fresh frozen structural allografts in the thoracic and lumbar spine. Do they work if combined with posterior fusion and instrumentation in adult patients with kyphosis or anterior column defects? Spine (Phila Pa 1976) 1995;20(12):1410–1418. [PubMed] [Google Scholar]
- 16.Hodgson AR, Stock FE, Fang HS, et al Anterior spinal fusion. The operative approach and pathological findings in 412 patients with Pott’s disease of the spine. Br J Surg. 1960;48:172–178. doi: 10.1002/(ISSN)1365-2168. [DOI] [PubMed] [Google Scholar]
- 17.Song JF, Jing ZZ, Chen B, et al One-stage anterolateral surgical treatment for lumbosacral segment tuberculosis. Int Orthop. 2012;36(2):339–344. doi: 10.1007/s00264-011-1378-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Li JH, Zhang ZH, Shi T, et al Surgical treatment of lumbosacral tuberculosis by one-stage debridement and anterior instrumentation with allograft through an extraperitoneal anterior approach. J Orthop Surg Res. 2015;10:62. doi: 10.1186/s13018-015-0204-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hirano T, Hasegawa K, Takahashi HE, et al Structural characteristics of the pedicle and its role in screw stability. Spine (Phila Pa 1976) 1997;22(21):2504–2509. doi: 10.1097/00007632-199711010-00007. [DOI] [PubMed] [Google Scholar]
- 20.Weinstein JN, Rydevik BL, Rauschning W Anatomic and technical considerations of pedicle screw fixation. Clin Orthop Relat Res. 1992;(284):34–46. [PubMed] [Google Scholar]
- 21.Bateman DK, Millhouse PW, Shahi N, et al Anterior lumbar spine surgery: a systematic review and meta-analysis of associated complications. Spine J. 2015;15(5):1118–1132. doi: 10.1016/j.spinee.2015.02.040. [DOI] [PubMed] [Google Scholar]
- 22.Lindley EM, McBeth ZL, Henry SE, et al Retrograde ejaculation after anterior lumbar spine surgery. Spine (Phila Pa 1976) 2012;37(20):1785–1789. doi: 10.1097/BRS.0b013e31825752bc. [DOI] [PubMed] [Google Scholar]
- 23.廖烨晖, 叶入裴, 李广州, 等 一期后前联合入路与单纯后路手术治疗下腰椎结核的疗效比较. 中国修复重建外科杂志. 2017;31(5):534–540. doi: 10.7507/1002-1892.201609083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ekinci S, Akyildiz F, Ersen O, et al Tuberculosis of ultralong segmental thoracic and lumbar vertebrae treated by posterior fixation. Spine J. 2015;15(10):2298–2299. doi: 10.1016/j.spinee.2015.03.050. [DOI] [PubMed] [Google Scholar]
- 25.He Q, Xu J Comparison between the antero-posterior and anterior approaches for treating L5-S1 vertebral tuberculosis. Int Orthop. 2012;36(2):345–351. doi: 10.1007/s00264-011-1307-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zhang H, Zeng K, Yin X, et al Debridement, internal fixation, and reconstruction using titanium mesh for the surgical treatment of thoracic and lumbar spinal tuberculosis via a posterior-only approach: a 4-year follow-up of 28 patients. J Orthop Surg Res. 2015;10:150. doi: 10.1186/s13018-015-0292-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jain A, Jain R, Kiyawat V Evaluation of outcome of posterior decompression and instrumented fusion in lumbar and lumbosacral tuberculosis. Clin Orthop Surg. 2016;8(3):268–273. doi: 10.4055/cios.2016.8.3.268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sahoo MM, Mahapatra SK, Sethi GC, et al Posterior-only approach surgery for fixation and decompression of thoracolumbar spinal tuberculosis: a retrospective study. J Spinal Disord Tech. 2012;25(7):E217–E223. doi: 10.1097/BSD.0b013e31826a088e. [DOI] [PubMed] [Google Scholar]
- 29.Lee BH, Lee HM, Kim TH, et al Transpedicular curettage and drainage of infective lumbar spondylodiscitis: technique and clinical results. Clin Orthop Surg. 2012;4(3):200–208. doi: 10.4055/cios.2012.4.3.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sun L, Song Y, Liu L, et al One-stage posterior surgical treatment for lumbosacral tuberculosis with major vertebral body loss and kyphosis. Orthopedics. 2013;36(8):e1082–e1090. doi: 10.3928/01477447-20130724-28. [DOI] [PubMed] [Google Scholar]
- 31.Xu Z, Wang X, Shen X, et al One-stage lumbopelvic fixation in the treatment of lumbosacral junction tuberculosis. Eur Spine J. 2015;24(8):1800–1805. doi: 10.1007/s00586-015-3863-8. [DOI] [PubMed] [Google Scholar]
- 32.Wang YX, Zhang HQ, Liao W, et al One-stage posterior focus debridement, interbody graft using titanium mesh cages, posterior instrumentation and fusion in the surgical treatment of lumbo-sacral spinal tuberculosis in the aged. Int Orthop. 2016;40(6):1117–1124. doi: 10.1007/s00264-016-3161-z. [DOI] [PubMed] [Google Scholar]
- 33.Li W, Liu J, Gong L, et al Posterior intervertebral space debridement, annular bone grafting and instrumentation for treatment of lumbosacral tuberculosis. BMC Surg. 2017;17(1):124. doi: 10.1186/s12893-017-0310-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Campbell PG, Malone J, Yadla S, et al Early complications related to approach in thoracic and lumbar spine surgery: a single center prospective study. World Neurosurg. 2010;73(4):395–401. doi: 10.1016/j.wneu.2010.01.024. [DOI] [PubMed] [Google Scholar]
- 35.Hirakawa A, Miyamoto K, Masuda T, et al Surgical outcome of 2-stage (posterior and anterior) surgical treatment using spinal instrumentation for tuberculous spondylitis. J Spinal Disord Tech. 2010;23(2):133–138. doi: 10.1097/BSD.0b013e31819a870f. [DOI] [PubMed] [Google Scholar]
- 36.Zeng H, Wang X, Pang X, et al Posterior only versus combined posterior and anterior approaches in surgical management of lumbosacral tuberculosis with paraspinal abscess in adults. Eur J Trauma Emerg Surg. 2014;40(5):607–616. doi: 10.1007/s00068-013-0367-2. [DOI] [PubMed] [Google Scholar]
- 37.Xu Z, Wang X, Shen X, et al Posterior only versus combined posterior and anterior approaches for lower lumbar tuberculous spondylitis with neurological deficits in the aged. Spinal Cord. 2015;53(6):482–487. doi: 10.1038/sc.2014.252. [DOI] [PubMed] [Google Scholar]
- 38.周焯家, 简月奎, 李波, 等 腰骶椎结核治疗的方法选择 (附 65 例分析) 中国矫形外科杂志. 2008;16(15):1141–1143. [Google Scholar]