

Abstract
Objective: To investigate the effects of modified Buzhong Yiqi decoction combined with Gangtai ointment on the wound healing and anal function of circumferential mixed hemorrhoid patients. Methods: Patients (n=120) with circumferential mixed hemorrhoids were recruited as the research cohort. All the patients underwent surgical treatment and were randomly divided into a control group and a research group. The control group was administered chitosan hydrogels for wound healing, once a day. The research group was administered modified Buzhong Yiqi decoction (1 dose a day, orally) combined with Kangtai ointment for external application (twice a day, for two consecutive weeks). We compared the two groups’ effective rates, their pain indexes, their perianal edema scores, their quality of life scores, their wound healing times, their pain resolution times, their anal functions, their wound exudate scores, and their adverse reactions. Results: Compared with the control group, the research group had a higher effective rate (P<0.01), a lower pain index, and a lower perianal edema score (both P<0.001), a higher quality of life score (P<0.001), a shorter wound healing time, a shorter pain resolution time, and fewer adverse reactions than the control group (both P<0.001). The lengths of the anal canals in the research group were shorter than they were in the control group (P<0.01), and the resting pressure, maximum diastolic blood pressure, and maximum systolic blood pressure were higher than they were in the control group (all P<0.001). The wound exudate scores at 7 and 14 days after the treatment in the research group were lower than they were in the control group (all P<0.001). There were fewer adverse reactions in the research group than there were in the control group (P<0.05). Conclusion: Modified Buzhong Yiqi decoction combined with Gangtai ointment for patients with circumferential mixed hemorrhoids has good short-term efficacy. It helps to promote wound healing, improves anal function, and does not increase the incidence of adverse reactions. It is worthy of promotion and application.
Keywords: Gangtai ointment, circumferential mixed hemorrhoids, effective rate, modified Buzhong Yiqi decoction, wound healing, anal function
Introduction
In the field of anorectal diseases, hemorrhoids are a chronic disease. They are venous clusters formed by the congestion, expansion, and flexion of the venous plexus in the lower part of the rectum [1]. Mixed hemorrhoids are a common type, and they arise both above and below the dentate line and are covered by the anal skin and rectal mucosa [2]. The formation of circumferential mixed hemorrhoids involves the formation of mixed hemorrhoids around the rectum and anal canal, and they are the final stage of hemorrhoidal development [3]. When edema incarceration accompanies the hemorrhoids, the traditional treatment using external stripping and internal ligation is usually performed [4]. However, some symptoms will occur after surgery, such as anal swelling and pain, difficulty urinating, incision pain, and the slow healing of the incision. In the past, anti-inflammatories, analgesics, and physical barrier protection were used as the main treatments after surgery in western medicine, but the effects were unsatisfactory [5].
Traditional Chinese medicine believes that the anal swelling and pain after hemorrhoidal surgery is mostly due to the prolonged course of the disease, the deficiency of Qi and blood, and damp-heat betting. The trauma after surgery will cause meridian damage, blood clotting, further causing swelling and pain after the meridian is blocked. Modified Buzhong Yiqi decoction includes White peony root, Atractylodes rhizome, Angelica, Ginseng, Bupleurum, Cimicifuga, Tangerine peel, Roasted licorice, and Astragalus. It has the effects of raising Yang, improving muscle tone, and strengthening the spleen and stomach. At the same time, depending on the severity of the symptoms, the dosage can be adjusted to achieve the desired therapeutic effect. Qian et al. used Buzhong Yiqi decoction to treat 86 patients experiencing pain after getting circumferential mixed hemorrhoids, a treatment that significantly shortened the time for wound healing and reduced the incidence of complications, suggesting that modified Buzhong Yiqi decoction has beneficial effects [6].
However, there is still a lack of clinical data on the treatment of circular mixed hemorrhoids with modified Buzhong Yiqi decoction combined with Gangtai ointment. In this study, the application of modified Buzhong Yiqi decoction combined with Gangtai ointment was found to have good results.
Materials and methods
General data
Patients (n=120) with circumferential mixed hemorrhoids from May 2018 to January 2020 were recruited as the research cohort. All the patients underwent surgical treatment and were randomly divided into a control group and a research group, with 60 cases in each group. This study was reviewed and approved by the medical ethics committee of our hospital.
Inclusion criteria: (1) Patients who were diagnosed with circumferential mixed hemorrhoids through anoscopies, rectal examinations, their medical histories, and digital anorectal examinations. (2) Patients with good compliance. (3) Patients who had ineffective intermittent treatment or ineffective continuous conservative treatment. (4) Patients who signed the consent forms voluntarily. (5) Patients who successfully completed the surgery.
Exclusion criteria: (1) Patients who suffered from serious dysfunction in their major organs such as their kidneys, lungs, liver, heart, or who were intolerant to the surgery and who failed to take care of themselves. (2) Patients who were ineligible for the surgery because of diabetes and high blood pressure. (3) Patients who suffered from combined malformations, fissures, incontinence, fistulas, stenosis, etc. (4) Patients had rectal occupied lesions, acute infections, or specific infections.
Methods
The patients in the both groups underwent minimally invasive hemorrhoid surgery (PPH). Each patient was placed in a lying position with the left knee bent and anesthetized. After the anesthesia took effect, the patient was placed in a lithotomy position. The anus was disinfected, a sterile hole towel was placed and the anus was expanded. PPH03 (Johnson and Johnson, USA) was used. Axternal hemorrhoidectomies were performed on the patients with obvious external hemorrhoids. Titanoreine suppositories were used and fixed in the anal canal. After the PPH was completed, hemostasis, anti-infection treatment, and defaecation were carried out. The patient orally took a single dose of 100 mg Tramadol (Shenzhen Hai Wang Pharmaceutical Co., Ltd., China). The gauze was pulled out and the following treatments were carried out the next day after surgery.
The control group was treated with chitosan gel (Boda Lean Biopharmaceutical Company, Shenyang, China) after the surgery. After the wound was cleaned and disinfected every morning, the gel was applied to and completely covered the wound surface, once a day for two consecutive weeks [7].
The research group was given Kangtai ointment for external application (twice a day, for two consecutive weeks) combined with modified Buzhong Yiqi decoction. The Buzhong Yiqi decoction consisted of 10 g White peony root, Atractylodes, Angelica, Ginseng, 9 g Bupleurum, Cimicifuga, 6 g Tangerine Peel, 5 g Roasted licorice, 20 g Astragalus. Eucommia, Dipsacus, and Morus alba needed to be added for the patients with kidney deficiencies. Rhizoma sparganii and Motherwort need to be added for the patients with blood stases. Curcuma, Neem seed and Silktree albizia bark were added for the patients with liver-qi stagnation. Alisma and Phellodendron were added for the patients with dampness-heat. All the medicinal materials were soaked for 30 minutes. The first dose of the medicine was decocted to 200 mL, and the second was decocted to 100 mL. The patients were instructed to combine these two solutions into one and take the combination after meals, twice a day, in the morning and evening.
Outcome measures
The main outcome measure was the effective rate, and the secondary outcome measures included the quality of life scores, the wound healing times, the pain resolution times, the pain indexes, and the perianal edema scores.
The two groups’ effective rates were compared after the treatment. The wound healing and the changes in the patient’s vital signs were observed. Ineffective was defined as no improvement in the patient’s signs and symptoms, or when they even become more severe.
Effective was defined as an improvement in the patient’s signs and symptoms, and the wound healed partly. Markedly effective was defined as no signs and symptoms, and the wound healed completely [7]. Total effective rate = number of (markedly effective cases + effective)/total number of cases ×100%.
The patients’ pain levels and their perianal edemas were observed before the treatment and at 14 days after the treatment. The perianal edema score system was used. Three points indicated the tissues were severely bulged, without skin lines. Two points indicated the tissues were moderately bulged, with unobvious lines. One point indicated the tissues were slightly bulged, with lines. Zero stood for no edema. The visual analog scale measurements were used for the pain assessment. Seven to ten points were regarded as severe pain, 4-6 points were regarded as moderate pain, 1-3 points were regarded as mild, and 0 points was regarded as pain free [8].
The quality of life scores, the wound healing times, and the pain resolution times in the two groups were compared. The quality of life and the wound healing times were observed, and the duration of the pain was recorded from the right after time for surgery. Severe anorexia, emotional stress and anxiety, time for inability to fall asleep, poor physical activity, and anal pain were clearly recorded as 1 point. Emotional tension, anal pain, frequent insomnia, frequent anorexia, and poor physical activity were recorded as 2 points. Minor insomnia, poor physical activity, emotional disturbances, anal pain, and anorexia were recorded as 3 points. Occasional insomnia, anorexia, anal pain, emotional discomfort, and poor physical activity were recorded as 4 points. No emotional discomfort, no anal pain, no anorexia, better sleep quality, and better physical activity were recorded as 5 points [9].
The anal function was compared between the two groups. The length, resting pressure, maximum diastolic pressure, and maximum systolic pressure of the anal canal were measured three times, and the average was calculated [10]. A ZCJ-CII anorectal pressure detector (Medike Electronics Company, Hefei, China) was used. Before it was used, empty stools, no enema, no digital rectal examination, and no rectoscopy were carried out. The application of a microcomputer was used to provide for the production of a ZCJ-CII type pressure detector for testing, the detection of the front empty stool, no enema, no rectal fingering, and a rectal mirror examination.
The wound exudates in the two groups were observed and compared before the treatment, and at 7 and 14 days after the treatment, respectively. The wound exudate score system was adopted. Three points indicated that the amount of wound exudate wet through more than 12 layers of gauzes, two stood for 8-11 layers, 1 meant 4-7 layers and 0 represented fewer than 4 layers [11].
The adverse reactions during the treatment were compared, including fevers, bleeding, wound exudate, and perianal edemas. The incidence of adverse reactions = number of cases of (fever + bleeding + wound exudate + perianal edema)/total number of cases ×100%.
Statistical anaysis
SPSS 22.0 was used for the data analysis. The measurement data was expressed as the mean ± standard deviation (x̅ ± sd). Independent sample t-tests were used for the comparisons between the two groups, and paired sample t-tests were used for the comparisons before and after the surgeries. The data at three time points used repeated measures analysis of variance combined with post-hoc Bonferroni tests. Chi-square test were used to analyze the count data, which were expressed as percentages. Statistical significance was defined as P<0.05.
Results
Comparison of baseline data
There was no statistically significant differences in the basic data between the two groups, so they were comparable (P>0.05). See Table 1.
Table 1.
Comparison of the baseline data (x̅ ± sd)
| Group | Gender (n) | Average age (year) | Average course (month) | |
|---|---|---|---|---|
|
| ||||
| Male | Female | |||
| Control group (n=60) | 43 | 17 | 43.4±2.7 | 134.3±3.5 |
| Research group(n=60) | 40 | 20 | 42.8±2.4 | 135.1±3.7 |
| χ2/t | 0.352 | 0.858 | 1.217 | |
| P | 0.553 | 0.393 | 0.226 | |
Comparison of the effective rates
The research group had a higher effective rate than the control group (P<0.01). See Table 2.
Table 2.
Comparison of the effective rates (n, %)
| Group | Markedly effective | Effective | Ineffective | Effective rate |
|---|---|---|---|---|
| Control group (n=60) | 32 (53.3) | 18 (30.0) | 10 (16.7) | 83.3% |
| Research group (n=60) | 38 (63.3) | 21 (35.0) | 1 (1.7) | 98.3% |
| χ2 | 8.107 | |||
| P | 0.004 | |||
Comparison of the pain indexes and the perianal edema scores
No significant differences were found in the pain indexes or the perianal edema scores between the two groups before the treatment. (both P>0.05). 14 days after the treatment, the pain indexs and perianal edema scores in the two groups were significantly lower than they were before the treatment, and the above indicators in the study group were lower than they were in the control group (both P<0.001). See Table 3.
Table 3.
Comparison of the pain indexes and the perianal edema scores (score, x̅ ± sd)
| Group | Pain index | Perianal edema score | ||
|---|---|---|---|---|
|
|
|
|||
| Before treatment | 14 d after treatment | Before treatment | 14 d after treatment | |
| Control group (n=60) | 6.73±1.52 | 2.23±0.34*** | 2.35±0.46 | 1.47±0.31*** |
| Research group (n=60) | 6.56±1.33 | 1.26±0.37*** | 2.23±0.34 | 0.96±0.22*** |
| t | 0.652 | 14.953 | 1.625 | 10.392 |
| P | 0.516 | 0.000 | 0.108 | 0.000 |
Note: Compared with the same group before the treatment;
P<0.001.
Comparison of the quality-of-life scores, the wound healing times and the pain resolution times
The research group had higher quality-of-life scores (P<0.001), shorter wound healing times, and shorter pain resolution times than the control group (both P<0.001). See Table 4.
Table 4.
Comparison of the quality of life scores, the wound healing times, and the pain resolution times (x̅ ± sd)
| Group | Quality of life score (score) | Time for wound healing (d) | Time to pain resolution (d) |
|---|---|---|---|
| Control group (n=60) | 3.32±0.23 | 24.68±4.54 | 8.06±1.35 |
| Research group (n=60) | 4.86±0.63 | 18.96±3.75 | 6.73±1.04 |
| t | 17.786 | 7.524 | 6.054 |
| P | 0.000 | 0.000 | 0.000 |
Comparison of the anal function
Before the treatment, there were no significant differences in terms of the lengths, resting pressures, maximum diastolic pressures, and maximum systolic pressures of the anal canal between the groups (all P>0.05). 14 days after the treatment, the anal canal lengths in the two groups were lower than they were before the treatment (P<0.001), and the resting pressures, maximum diastolic blood pressures, and maximum systolic blood pressures were higher than they were before the treatment (all P<0.001). Also, the above indicators in the research group were better than they were in the control group at 14 days after the treatment (P<0.01). See Table 5 and Figure 1.
Table 5.
Comparison of the anal functions (x̅ ± sd)
| Group | Control group (n=60) | Research group (n=60) | t | P |
|---|---|---|---|---|
| Length of anal canal (cm) | ||||
| Before treatment | 3.57±0.76 | 3.61±0.82 | 0.278 | 0.782 |
| 14 d after treatment | 2.97±0.88*** | 2.51±0.69*** | 3.186 | 0.002 |
| Anal canal resting pressure (mmHg) | ||||
| Before treatment | 45.21±7.14 | 46.88±6.84 | 1.308 | 0.193 |
| 14 d after treatment | 49.31±8.05*** | 54.64±8.13*** | 3.609 | 0.000 |
| Maximum diastolic pressure of anal canal (mmHg) | ||||
| Before treatment | 81.36±7.22 | 80.95±7.58 | 0.303 | 0.762 |
| 14 d after treatment | 137.61±40.91*** | 168.47±39.22*** | 4.218 | 0.000 |
| Maximum systolic pressure of anal canal (mmHg) | ||||
| Before treatment | 95.32±13.67 | 96.81±11.53 | 0.645 | 0.520 |
| 14 d after treatment | 109.48±11.24*** | 125.66±15.09*** | 6.661 | 0.000 |
Note: Compared with the same group before the treatment;
P<0.001.
Figure 1.
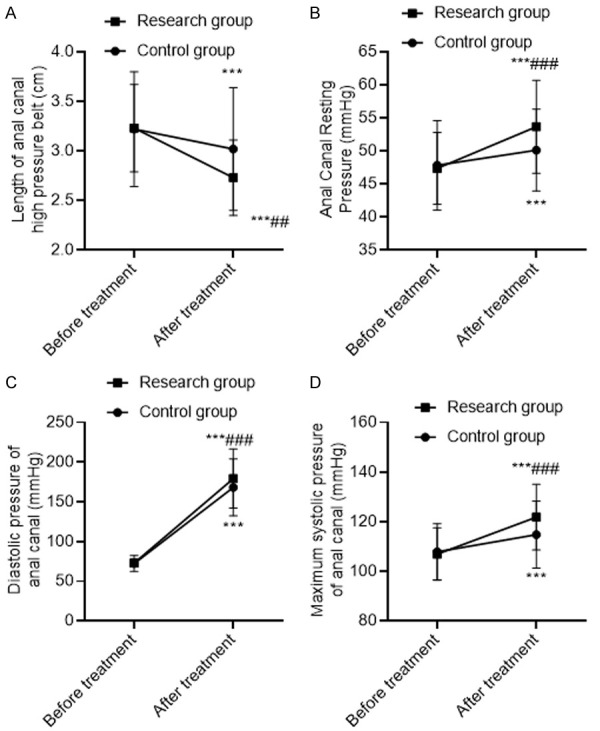
Comparison of the anal function. A: Length of the anal canal; B: Anal canal resting pressure; C: Maximum diastolic pressure of the anal canal; D: Maximum systolic pressure of the anal canal. Compared with the same group before the treatment, ***P<0.001; compared with the control group after the treatment, ##P<0.01, ###P<0.001.
Comparison of the wound exudate scores
Before the treatment, there was no statistically significant difference in the wound exudate scores between the two groups (P>0.05). At 7 and 14 days after the treatment, the wound exudate scores in the two groups were significantly lower than they were before the treatment (all P<0.001), and the wound exudate scores in the research group were lower than the wound exudate scores in the control group at the same time (all P<0.001). See Table 6.
Table 6.
Comparison of the wound exudate scores (score, x̅ ± sd)
| Group | Before treatment | 7 d after treatment | 14 d after treatment |
|---|---|---|---|
| Control group (n=60) | 2.93±0.33 | 1.53±0.22*** | 1.03±0.19*** |
| Research group (n=60) | 2.88±0.37 | 0.96±0.11*** | 0.76±0.14*** |
| t | 0.781 | 17.950 | 8.862 |
| P | 0.436 | 0.000 | 0.000 |
Note: Compared with the same group before the treatment;
P<0.001.
Comparison of the adverse reactions
The research group had fewer adverse reactions than the control group (P<0.05). See Table 7.
Table 7.
Comparison of the adverse reactions (n, %)
| Group | Fever | Wound exudate | Bleeding | Perianal edema | Incidence |
|---|---|---|---|---|---|
| Control group (n=60) | 2 (3.3) | 3 (5.0) | 2 (3.3) | 3 (5.0) | 16.7 |
| Research group (n=60) | 1 (1.7) | 0 (0.0) | 0 (0.0) | 1 (1.7) | 3.3 |
| χ2 | 6.211 | ||||
| P | 0.013 |
Discussion
The clinical incidence of hemorrhoids reaches 38% in China, and accounts for about 91% of all anorectal diseases, of which, circumferential mixed hemorrhoids is a common type. Mixed hemorrhoids arise both above and below the dentate line and are covered by the anal skin and rectal mucosa at the final stage of hemorrhoidal development. The Department of Intestinal Surgery of the Chinese Medical Association has formulated new principles for the treatment of hemorrhoids, to alleviate and eliminate the symptoms and protect the anal function [12].
After hemorrhoidal excisions, the wounds cause severe pain in patients, leading to stress changes in the neuroendocrine and cardiovascular systems, and that can accelerate the heart rate and raise the blood pressure, resulting in a certain psychological impact and prolonged recovery time [13]. Anal swelling becomes a major complication after circumferential mixed surgery. Most patients will have significant pain symptoms and edema; in addition, detoxion can lead to sphistate spasm contraction, which causes stool dry knot, feces retention, and drainage difficulties, resulting in long-term pain [14,15]. Clinically, nonsteroidal anti-inflammatory drugs, and opioids are used after surgery to relieve pain, but significant complications may occur that lower patient compliance [16]. Chitosan antibacterial gel for hemorrhoids, mainly composed of shell polysaccharides, has good adsorption, is film-forming, has permeability, is fiber-forming, and allows for moisture absorption and moisturizing, which can inhibit the growth of E. coli, Staphylococcus aureus, streptococcus and other pathogenic microorganisms. It is a common drug for wound healing after hemorrhoidal surgery in the clinic. But because it has no effect on pain relief, for the patients who have significant wound healing, the therapeutic efficacy is not ideal [17].
Gangtai ointment is an external medicine compound that contains papaverine hydrochloride, borneol, carbonized sanguisorba root, hydrochloric acid nicotine, sapindales, etc. Carbonized sanguisorba root can stop the bleeding. The containing geosaccharides A, B, E, steroids, and geosaccharides I., II. can help to shrink the blood vessels, shorten external bleeding time, and have antibacterial effects [18,19]. Sapindales has the effect of resolving toxins and dispersing swelling, and its tannin content can shrink wound microvessels, avoid wound inflammation, reduce pain, and inhibit bacteria [20,21]. Borneol clears heat evil and detoxifies, and it has antibacterial effects on Staphylococcus aegylomic, E. coli, etc.
Buzhong Yiqi decoction has the effects of raising Yang, improving muscle tone, and strengthening the spleen and stomach. Bupleurum and Cimicifuga should be added for patients with spleen dysfunction. Although licorice, ginseng, and Astragalus taste bitter, they play a role in treating spleen dysfunction [22,23]. The combined use of the above drugs has a complementary effect [24,25]. Roasted licorice can be reconciled with all the drugs, to help rise Qingyang, strengthen the Yang and Qi, restore spleen and stomach function, replenish energy, and eliminate disease [26]. In modern pharmacology, white atractylodes rhizome can relieve pain. It has a protective effect on endothelial cells, on immunity, and is anti-inflammatory. Cimicifuga can inhibit the intestinal cramps caused by acetylcholine and histamines, as well as the inflammatory cytokines produced by the endoblast cells in the blood vessels. Buzhong Yiqi decoction has anti-viral, anti-bacterial, immunity enhancing, anti-tumor, and anti-allergy effects. In this study, the research group had a better effective rate, lower incidences of fever, bleeding, pain, wound exudation, and perianal edemas than the control group. This was because both the modification of Buzhong Yiqi decoction according to the patient’s symptoms and the combination with Gangtai ointment treatment, can effectively alleviate the patient’s clinical symptoms to achieve better patient recovery. It suggested depending on the severity of the symptoms, increasing or decreasing the dosage of modified Buzhong Yiqi decoction can target and treat the disease. Meanwhile, the combination of Gangtai ointment effectively relieved the clinical symptoms and helped the recovery better.
The research group had higher quality of life scores, shorter wound healing times, shorter pain resolution times, lower pain indexes, and lower perianal edema scores than the control group. Also at 7 and 14 days after the treatment, the wound exudate scores in the research were lower than they were in the control group. This was because Buzhong Yiqi decoction had the effects of raising Yang, improving the muscle tone, and strengthening the spleen and stomach. After the combination of hemostatic drugs, it can effectively reduce edema, anal pain, shorten the wound healing times and the pain resolution times, and reduce wound exudation, therefore helping patients improve their quality of life, so it is worthy of wide application.
The lengths of the anal canals in the research group were shorter than they were in the control group, and the resting pressures, maximum diastolic blood pressures, and the maximum systolic blood pressures were higher than they were in the control group. Gangtai ointment can stop the bleeding, relieve the swelling and pain, and has significant effects on fissures and hemorrhoids. Depending on the severity of the symptoms, increasing or decreasing the dosage of modified Buzhong Yiqi decoction can help the targeted treatment be carried out, remove the distress caused by the diseases and restore related functionality.
This study has some shortcomings. The study cohort was small, and this may lead to errors in the results. We will conduct in-depth research and discussion, to ensure that the results have greater accuracy in our later research.
In summary, modified Buzhong Yiqi Decoction combined with Gangtai ointment for circumferential mixed hemorrhoids can improve anal function. It is worthy of promotion and application.
Disclosure of conflict of interest
None.
References
- 1.Wilson MZ, Swarup A, Wilson LRT, Ivatury SJ. The effect of nonoperative management of chronic anal fissure and hemorrhoid disease on bowel function patient-reported outcomes. Dis Colon Rectum. 2018;61:1223–1227. doi: 10.1097/DCR.0000000000001193. [DOI] [PubMed] [Google Scholar]
- 2.Zienkiewicz M, Krupnik T, Drozak A, Wasilewska W, Golke A, Romanowska E. Deletion of psbQ’ gene in cyanidioschyzon merolae reveals the function of extrinsic PsbQ’ in PSII. Plant Mol Biol. 2018;96:135–149. doi: 10.1007/s11103-017-0685-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tong F, Dannaway J, Enke O, Eslick G. Effect of preoperative psychological interventions on elective orthopaedic surgery outcomes: a systematic review and meta-analysis. ANZ J Surg. 2020;90:230–236. doi: 10.1111/ans.15332. [DOI] [PubMed] [Google Scholar]
- 4.Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American society of colon and rectal surgeons clinical practice guidelines for the management of hemorrhoids. Dis Colon Rectum. 2018;61:284–292. doi: 10.1097/DCR.0000000000001030. [DOI] [PubMed] [Google Scholar]
- 5.Liu ZC, Wu SP, Fan YQ, Chen ZH. Absorbable thread prevents 50 cases of postoperative complications of circular mixed hemorrhoids. Chin J Integr Tradit Chin West Med Surg. 2017;23:189–191. [Google Scholar]
- 6.Qian ZJ. Efficacy observation on 86 cases of postoperative complications of mixed hemorrhoid treated by Jiawei Buzhong Yiqi decoction. Gansu Tradit Chin Med. 2001;14:46. [Google Scholar]
- 7.Li XP, Huang ZH, Hu LC. The effect of chitosan gel (Type lll) on wounds after hemorrhoidectomy. Chin J New Drugs Clin. 2015;34:233–235. [Google Scholar]
- 8.Orangio GR. Expert commentary on the evaluation and management of hemorrhoids. Dis Colon Rectum. 2020;63:424–426. doi: 10.1097/DCR.0000000000001643. [DOI] [PubMed] [Google Scholar]
- 9.Rørvik HD, Styr K, Ilum L, McKinstry GL, Dragesund T, Campos AH, Brandstrup B, Olaison G. Hemorrhoidal disease symptom score and short health scaleHD: new tools to evaluate symptoms and health-related quality of life in hemorrhoidal disease. Dis Colon Rectum. 2019;62:333–342. doi: 10.1097/DCR.0000000000001234. [DOI] [PubMed] [Google Scholar]
- 10.Kothari TH, Shivangi K, Krystle B, Vivek K. Su1720 Prospective evaluation of the hemorrhoidal energy treatment procedure for the management of bleeding internal hemorrhoids. Gastrointest Endosc. 2018;87:AB384–AB385. [Google Scholar]
- 11.Arunabha M, Tanushree H, Sourabh B, Witte JS. An efficient bayesian meta-analysis approach for studying cross-phenotype genetic associations. PLoS Genetics. 2018;14:e1007139–e1007140. doi: 10.1371/journal.pgen.1007139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fang ZX, Xiao ZG. Minutes of the 14th national symposium on new technologies and advances in colorectal and anal surgery. Colorectal Anal Surg. 2020;26:3. [Google Scholar]
- 13.Quaglio AEV, Cruz VM, Almeida-Junior LD, Costa CARA, Di Stasi LC. Bidens Pilosa (Black Jack) standardized extract ameliorates acute tnbs-induced intestinal inflammation in rats. Planta Med. 2020;86:319–330. doi: 10.1055/a-1089-8342. [DOI] [PubMed] [Google Scholar]
- 14.Ali SA, Rizk MZ, Hamed MA, Aboul-Ela EI, El-Rigal NS, Aly HF, Abdel-Hamid Z. Assessment of titanium dioxide nanoparticles toxicity via oral exposure in mice: effect of dose and particle size. Biomarkers. 2019;24:1–33. doi: 10.1080/1354750X.2019.1620336. [DOI] [PubMed] [Google Scholar]
- 15.Okkabaz N, Esen E, Schwartzberg DM, Remzi FH, Kirat HT. Hand-crafted endoluminal vacuum-assisted drainage for anastomotic leak after IPAA. Dis Colon Rectum. 2019;62:1259–1262. doi: 10.1097/DCR.0000000000001453. [DOI] [PubMed] [Google Scholar]
- 16.Troche JMR, Franquez-Flores BJ, Amieva-Balmori M, Rojas-Loureiro G, Garcia-Garcia FD. Su1602 the effect of biofeedback therapy (BFT) on anal sphincter and puborectalis muscles in patients with fecal incontinence. Gastroenterology. 2018;154:S542–S543. [Google Scholar]
- 17.Xiao M, Li GQ. Chitosan gel in the treatment of 60 cases of hemorrhoids. Chin J Anorectal Dis. 2012;32:79. [Google Scholar]
- 18.Oketch F, Oyoko H, Amolo G. A Study of the effect of hermanson’s spatial dielectric function on the photoionization cross-section of a hydrogenic and a non-hydrogenic donor impurity in a GaAs quantum dot of cylindrical geometry in the region of finite and infinite barrier potentials. J Korean Phys Soc. 2018;73:928–933. [Google Scholar]
- 19.Zhu YF, Li SZ, Sun QZ, Yang XY. Effect of in ovo feeding of vitamin c on antioxidation and immune function of broiler chickens. Animal. 2019;13:1–7. doi: 10.1017/S1751731118003531. [DOI] [PubMed] [Google Scholar]
- 20.Chogle S, Zuaitar M, Sarkis R, Saadoun M, Mecham A, Zhao YH. The recommendation of cone-beam computed tomography and its effect on endodontic diagnosis and treatment planning. J Endod. 2020;46:162–168. doi: 10.1016/j.joen.2019.10.034. [DOI] [PubMed] [Google Scholar]
- 21.Labounty TM, Bach DS, Bossone E, Kolias TJ. Effect of race on echocardiographic measures of cardiac structure and function. Am J Cardiol. 2019;124:812–818. doi: 10.1016/j.amjcard.2019.05.049. [DOI] [PubMed] [Google Scholar]
- 22.Xia YJ, Niu Y, Cai J, Lin ZJ, Liu C, Li HC, Chen C, Song WM, Zhao ZH, Chen RJ, Kan HD. The effects of personal short-term exposure to ambient ozone on blood pressure and vascular endothelial function: a mechanistic study based on DNA methylation and metabolomics. Environ Sci Technol. 2018;52:12774–12782. doi: 10.1021/acs.est.8b03044. [DOI] [PubMed] [Google Scholar]
- 23.Alibhai S MH, Breunis H, Timilshina N, Hansen AR, Emmenegger U. The effect of docetaxel, enzalutamide, abiraterone, and radium-223 on cognitive function in older men with Metastatic Castrate-Resistant Prostate Cancer (mCRPC) J. Clin. Oncol. 2020;38:73. [Google Scholar]
- 24.Potter DD, Moir CR, Day CN, Harmsen WS, Pemberton JH. Fertility and sexual function in women following pediatric ileal pouch-anal anastomosis. J Pediatr Surg. 2020;55:59–62. doi: 10.1016/j.jpedsurg.2019.09.051. [DOI] [PubMed] [Google Scholar]
- 25.Ibares-Frías L, Gallego-Muoz P, Orive G, Anitua E, Cantalapiedra-Rodríguez R, Merayo-Lloves J, Martínez-García MC. Potential effect of plasma rich in growth factors-endoret in stromal wound healing in additive surgery. Ophthalmic Res. 2019;63:1–10. doi: 10.1159/000501507. [DOI] [PubMed] [Google Scholar]
- 26.Kober SE, Pinter D, Enzinger C, Damulina A, Duckstein H, Fuchs S, Neuper C, Wood G. Self-regulation of brain activity and its effect on cognitive function in patients with multiple sclerosis first insights from an interventional study using neurofeedback. Clin Neurophysiol. 2019;130:2124–2131. doi: 10.1016/j.clinph.2019.08.025. [DOI] [PubMed] [Google Scholar]