

Abstract
Background
There is a debate regarding the safety of etomidate. We evaluated the effects of etomidate on mortality in a large cohort of critical care patients.
Methods
This retrospective matched-cohort study was performed using the Medical Information Mart for Intensive Care version 3 (MIMIC-III) database. Among 12,526 adult patients who were prescribed etomidate or propofol on the first day of mechanical ventilation, 625 patients administered etomidate were statistically matched with 6,250 patients administered propofol. The primary outcome measures were all-cause in-hospital mortality, 48-hour survival, cardiovascular morbidity, and infectious morbidity. Logistic regression analysis with stepwise selection of variables was performed to examine the dose–mortality relationship of etomidate.
Results
All-cause in-hospital mortality was 1.84 times higher in the etomidate cohort (OR: 1.84, 98.75% CI: 1.42, 2.37). Compared to the propofol cohort, the etomidate cohort showed 57% lower odds of 48-hour survival (0.43 [0.27, 0.73]), no difference in odds of cardiovascular morbidity (0.86 [0.66, 1.12]), and 1.77 times higher odds of infectious morbidity (1.77 [1.35, 2.31]). Additionally, the odds of mortality increased by 1.36 times per 0.1 mg/kg of etomidate (1.36 [95% CI: 1.23, 1.49]).
Conclusions
Etomidate is a poor choice as a hypnotic drug on the first day of mechanical ventilation, as it is associated with a dose-dependent increase in all-cause mortality, and does not improve survival for the first 48 h.
Keywords: Dose-response relationship, Etomidate, Intensive care unit, Mortality, Propofol, Ventilator
Introduction
The use of etomidate for tracheal intubation in septic patients has been reported to show no association with an increased mortality rate [1]. However, some meta-analyses indicated a strong association between mortality and the use of etomidate for tracheal intubation in patients with sepsis [2]. Further, a higher mortality rate has been reported in critically ill patients administered etomidate in comparison to other anesthetic induction agents [3]. Etomidate has also been reported to be associated with increased 30-day mortality when administered during anesthesia in patients undergoing non-cardiac surgery [4]. Conversely, Wagner et al. [5] reported no association between etomidate exposure and poor outcomes, including mortality, in patients undergoing cardiac surgery. The reasons for these discrepancies regarding the safety of etomidate are unclear.
This retrospective study was performed to determine the dose-response relationship between etomidate exposure and mortality using the vast amount of data from the Medical Information Mart for Intensive Care version 3 (MIMIC-III), a database of combined real-world health records, prescriptions, dictionaries, diagnostic information (including disease-related groups), and complete survival and mortality information for patients admitted to the intensive care unit (ICU) of a large tertiary care hospital located in Boston, MA, USA.
Materials and Methods
Construction of cohorts
MIMIC-III is an open database of electronic health records of 38,597 adult critical care patients (>16 years) at the Beth Israel Deaconess Medical Center, a tertiary care hospital in Boston, MA, USA, from 2001 to 2012 [6]. The use of de-identified MIMIC-III data in the present study was not deemed research in human subjects by the Institutional Review Board (IRB) of the University of Massachusetts Medical School, which waived the requirement for informed consent. After completing the required training, all co-authors were granted access to MIMIC-III for free use of the data without additional IRB approval. The selection of patients in the etomidate and propofol cohorts was based on the following criteria.
Common inclusion criteria: adult patients treated with a mechanical ventilator for at least 1 h.
Etomidate cohort: patients prescribed etomidate (≤ 20 mg) on the first day of mechanical ventilation (cohort start date).
Propofol cohort: patients prescribed propofol instead of etomidate on the first day of mechanical ventilation. These patients were never prescribed etomidate during admission.
Patients with a history of previous hospitalization within 7 days and body weight or height above or below the respective upper and lower 0.1 percentile were excluded. A total of 12,526 patients were enrolled in the study before matching cohorts (etomidate, n = 625; propofol, n = 11,901).
Matching
The patients were matched based on the propensity to use etomidate. By preparing statistically matched cohorts, we minimized the heterogeneity of the patients due to the retrospective design. The matching procedure used a total of 43 variables consisting of 9 physical characteristics, 4 clinical features, and 30 disease components of the Elixhauser comorbidity index [7,8] as covariates for calculating the propensity scores. The nine physical characteristics were sex, three age groups (younger than 65, 65–86, and older than 86), four BMI groups (body mass index, <18.5, 18.5–25.0, 25.0–30.0, and >30 kg/m2), and ethnicity (white vs. non-white). The four clinical features were hypothalamic adrenal insufficiency as a primary diagnosis, previous history of treatment with adrenal suppressants (ketoconazole, metyrapone, suramin, aminoglutethimide, carbamazepine, phenobarbital, phenytoin, rifampin, and mitotane), admission before mid-2008, and a sequential organ failure assessment (SOFA) score > 5.0. Adopting the nearest neighbor matching method, a 1 : 10 matching ratio, and targeting absolute values of standardized differences < 0.1, a total of 6,875 patients were assigned after matching to the etomidate cohort (n = 625) or the propofol cohort (n = 6,250) (Supplementary Table 1).
Primary outcome measures
The four primary outcome variables were all-cause in-hospital mortality, survival for the first 48 h, cardiovascular morbidity, and infectious morbidity. Unless otherwise noted, in this manuscript mortality refers to all mortalities except those occurring within 48 h since sedative administration. Cardiovascular morbidity and infectious morbidity were judged using the ICD-9 code for diagnosis; the numbers in parentheses indicate the dotless version of the ICD-9 code. Cardiovascular morbidity was related to hypovolemia (27652), dialysis hypotension (45821), other iatrogenic hypotension (45829), atypical shock (78550), cardiogenic shock (78551), shock unrelated to trauma (78559), and cardiac and peripheral complications, unclassified (9971/9972). Infectious morbidity was due to ventilator-associated pneumonia (99731); infection of the central catheter (99931), bladder, or urological organs (99664 and 99665); infection of the stoma (tracheostomy, 51901; esophagostomy, 53086; gastrostomy, 53641; and colostomy or enterostomy, 56961); infection of the implanted prosthesis (99660, 99661, 99662, 99663, 99666, 99667, 99668, and 99669); and other postoperative infections (99859).
After the finding by Vinclair et al. [9] that adrenal inhibition was full-blown in 48-hour, we adopted a 48-hour interval after the day of etomidate administration as the guarantee period. Acute deaths after etomidate administration were excluded because they would generally have causes other than etomidate administration. Therefore, deaths that occurred within the initial 48 h after the cohort start date were excluded when counting all-cause in-hospital mortality.
Secondary outcome measures including dose–mortality relationship with the exploration of other factors
The secondary outcomes were supplementation with corticosteroids (n), vasopressor therapy (n), cortisol blood concentration measured in the morning after the cohort start date (μg/dl), accumulated time of vasopressor therapy (h) summed after the cohort start date, duration of ICU stay (days), total duration of hospitalization (days), and dose–mortality relationship of etomidate.
To check the dose-mortality relationship that may exist in the etomidate cohort, factors that may influence mortality were explored in the post-matching cohorts. We removed all variables that contributed little to the overall regression model. Variables were selected by the Akaike’s Information Criterion (AIC)-based stepwise selection method in pursuit of the most parsimonious model. All variables used for calculating the propensity score were used again in the logistic regression analysis, and a stepwise selection of the variables was performed. In the regression model using only the selected variables, a relationship was established between the administered dose (every 0.1 mg/kg) of etomidate and all-cause in-hospital mortality. In the dataset, neither LD50 nor LD95 was extrapolated as the observed dose ranges were not far beyond 0.5 mg/kg.
Blood pressure profile on the cohort start date
Systolic blood pressure (SBP) and mean blood pressure (MBP) on the cohort start date were compared between the two cohorts.
Data manipulation and analytical tools
After obtaining the rights to handle MIMIC-III, the entire dataset was imported and rebuilt as a copy of the SQL database on a personal computer having a 64-bit Darwin operating system. The codes for MIMIC-III shared by The Laboratory of Computational Physiology of the Massachusetts Institute of Technology (https://github.com/MIT-LCP/mimic-code/tree/main/mimic-iii/concepts), that included patients’ comorbidities, vasopressor use, ventilator days, body weight, and height were utilized. Temporary tables were created using SQL and batch-queried into R version 3.5.5 (R: A language and environment for statistical computing. R Foundation for Statistical Computing, Austria. 2019). We employed the R software for all subsequent manipulations and analyses. We applied all statistical inferences, focusing on the size of the effect (odds ratio [OR] or Cohen’s d) and its associated uncertainty (CI), which complied with the American Statistical Association’s 2016 Statement on P values [10]. ORs were calculated using the conditional maximum likelihood method in the primary outcome and secondary measures, except the dose–response estimation from the log-odds in logistic regression analysis. To calculate the intervals, the alpha was adjusted to 98.75% (= (1 − [0.05/4]) × 100) for the four primary outcome measures, or 95% for other measures. To address the size of the effect, the OR was adopted for incidence data and Cohen’s d was used for interval data.
Results
The top 20 diagnoses for the admitted patients were obtained and are listed according to the after-matching cohorts in Supplementary Table 2. The maximum blood pressure was higher, while the minimum blood pressure was lower in the etomidate cohort than in the propofol cohort (Table 1).
Table 1.
Blood Pressure Profiles of the Cohorts on the First Day of Mechanical Ventilation
| Etomidate (n = 625) | Propofol (n = 6,250) | Cohen’s d | 95% CI |
||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| SBP (mmHg) | |||||
| Average | 117.8 | 118.9 | −0.1 | −0.2 | 0.0 |
| Minimum | 78.7 | 86.1 | −0.3 | −0.3 | −0.2 |
| Maximum | 160.3 | 153.9 | 0.3 | 0.3 | 0.3 |
| MBP (mmHg) | |||||
| Average | 77.7 | 78.8 | −0.1 | −0.1 | 0.0 |
| Minimum | 51.4 | 57.0 | −0.4 | −0.4 | −0.3 |
| Maximum | 116.9 | 109.1 | 0.2 | 0.1 | 0.3 |
Cohen’s d = (etomidate mean − propofol mean)/SD. SBP: systolic blood pressure, MBP: mean blood pressure.
Primary outcome measures
Overall, 6,690 of the 6,875 patients survived for the first 48 h after administration of the study drug. The patients receiving etomidate showed 1.84 times higher odds of hospital mortality (OR: 1.84 [98.75% CI: 1.42, 2.37]), 57% lower odds of survival for the first 48 h (0.43 [0.27, 0.73]), no significant difference in the odds of cardiovascular morbidity (0.86 [0.66, 1.12]), and 1.77 times higher odds of infectious morbidity (1.77 [1.35, 2.31]) than the propofol cohort (Fig. 1).
Fig. 1.
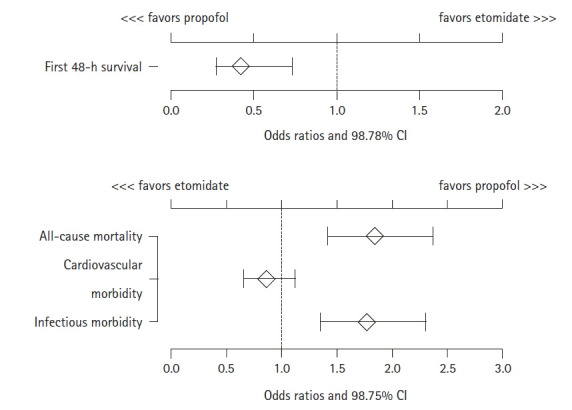
Four primary outcome measures in the after-matching cohorts (n = 625 vs. 6,250). Odds ratios and 98.75% CI.
Secondary outcome measures
The frequencies of corticosteroid replacement and vasopressor therapy were 1.82 times and 1.39 times higher in the etomidate cohort than in the propofol cohort, respectively. A total of 3,399 cortisol measurements were made in 1,341 patients (195 and 1,146 patients in the etomidate and propofol cohorts, respectively). Etomidate was associated with a trivial decrease in the morning blood cortisol level (95% CI, Cohen’s d = −0.30 μg/dl). In comparison to the propofol cohort, the etomidate cohort showed a longer cumulative vasopressor duration (42.7 vs. 68.1 h), total ICU stay (8.9 vs. 14.9 days), and number of hospital days (16.7 vs. 23.1 days) (Table 2).
Table 2.
Additional Outcome Measures
| Etomidate (n = 625) | Propofol (n = 6,250) | OR | Cohen’s d* | 95% CI |
||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Steroid replacement (n) | 41 | 232 | 1.82 | - | 1.26 | 2.58 |
| Vasopressor (n) | 436 | 3901 | 1.39 | - | 1.16 | 1.67 |
| Cortisol level (μg/dl)† | 24.2 | 26.3 | - | −0.12 | −0.30 | 0.06 |
| Vasopressor duration (h) | 68.1 | 42.7 | - | 0.26 | 0.17 | 0.34 |
| ICU stay (days) | 14.9 | 8.9 | - | 0.60 | 0.51 | 0.68 |
| Hospital stay (days) | 23.1 | 16.7 | - | 0.42 | 0.34 | 0.51 |
Cohen’s d = (etomidate mean − propofol mean)/SD.
A total of 3,399 cortisol measurements in 1,341 patients (195 and 1,146 patients in the etomidate and propofol cohorts, respectively). OR: odds ratio, ICU: intensive care unit.
The administered dose of etomidate ranged from 0.02 to 0.50 mg/kg, with a mean of 0.19 mg/kg and median of 0.19 mg/kg, and Q1 and Q3 of 0.14 and 0.24, respectively. The estimated odds of mortality increased by 1.36 times per 0.1 mg/kg of etomidate (1.36 [95% CI: 1.23, 1.49]). These estimated OR of dose-mortality relationship did not change before and after the removal of other variables using the AIC-based stepwise selection method (Figs. 2 and 3). Male sex, age < 86 years, BMI > 18.5, SOFA score < 5.0, and absence of pre-existing adrenal insufficiency were associated with a better in-hospital survival rate. Non-elective admission and admission before mid-2008 were associated with poor in-hospital survival. The effects of all other potential factors are shown in Fig. 3.
Fig. 2.
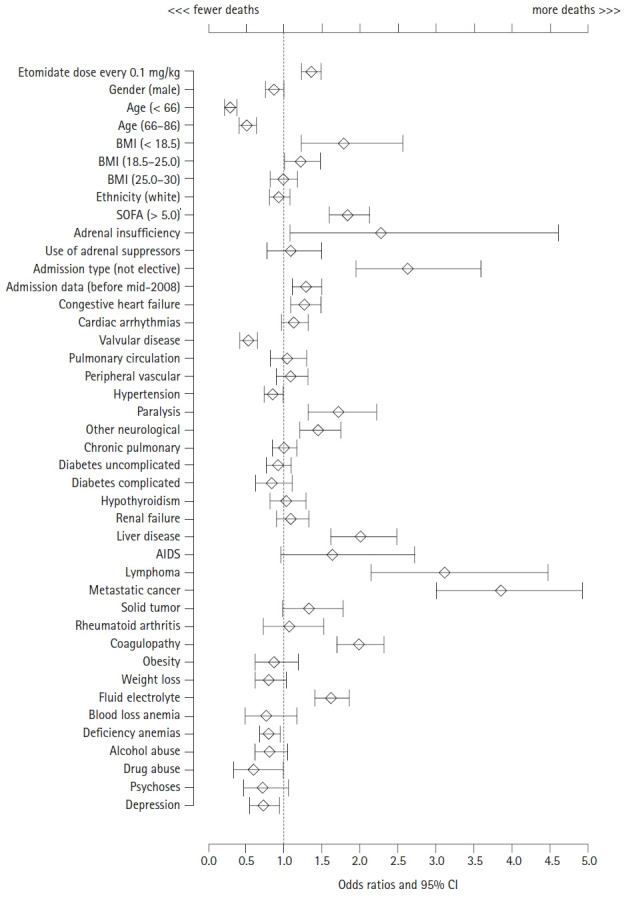
Etomidate dose-effect on mortality before the variable selection. All variables were included tentatively to explain the mortality with the dose of etomidate. BMI: body mass index, SOFA: sequential organ failure assessment, AIDS: acquired immune deficiency syndrome.
Fig. 3.
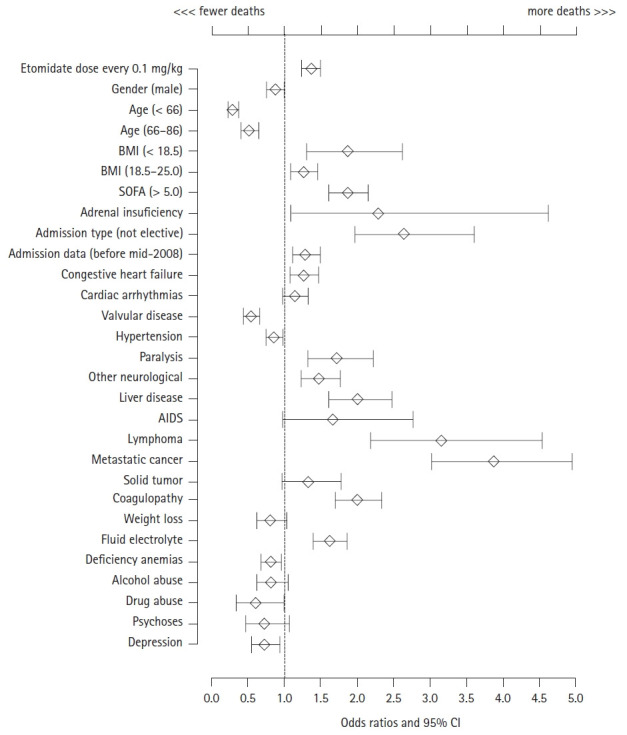
Dose-mortality relationships with the selection of factors. The effects of the dose of etomidate on mortality were adjusted after a stepwise selection of variables. BMI: body mass index, SOFA: sequential organ failure assessment, AIDS: acquired immune deficiency syndrome.
Discussion
We found a relation between the dose of etomidate administered and mortality in ICU patients on ventilator support. Although we observed that an increase in etomidate dose was associated with a higher mortality rate, it was difficult to determine the presence of a causal link; randomized controlled trials are required to infer such a relation.
Etomidate seemed to be used selectively in patients with wide blood pressure fluctuations. However, the use of etomidate did not rescue patients in the first 48 h after its administration. Cardiovascular morbidity was not diminished despite the use of etomidate. Moreover, the etomidate cohort received vasopressor therapy more frequently and had a longer cumulative vasopressor duration. Further, the use of etomidate was associated with a higher rate of infectious morbidity and a higher incidence of subsequent corticosteroid replacement, which in turn was associated with a higher mortality rate.
The Bradford Hill criteria of causation indicate that when greater exposure leads to a greater incidence of the effect or an inverse proportion is observed, it can be taken to suggest a causal relationship. However, it should be noted that most previous studies examining the relationship between etomidate and a high mortality rate ignored the dose-mortality relationship. In this study, in addition to the application of a propensity score matching procedure, we calculated the dose-mortality relationship rather than using randomization. We established a relationship between etomidate dose and mortality, but our results by themselves cannot confirm the existence of a causal relationship. However, this is an important finding considering the miscellaneous and multifactorial characteristics of deaths of patients undergoing respiratory therapy. Moreover, our results may be useful as a basis for future research regarding mortality in ICU patients administered etomidate.
There were two additional notable aspects of the dose-mortality relationship indicated in this study. First, the estimates of the calculated OR of dose-mortality relationship remained consistent up to two decimal places in a vigorous stepwise selection of the variables (1.36 [1.23, 1.49] vs. 1.36 [1.23, 1.49] for before and after the variable-selection), thereby indicating that the dose-effect of etomidate on mortality was independent of other factors. Second, the calculated OR of dose-mortality relationship is 1.85 for the well-accepted dose regimen of the etomidate (0.2 mg/kg), which comes from the squared OR 1.36 of dose-mortality relationship for every 0.1 mg/kg etomidate dose. It indicates that the odds of death will be increased by 1.85 times for every 0.2 mg/kg increment in dose of etomidate. It is very cautious to compare the calculated OR 1.85 of dose-mortality relationship with the OR 1.84 for mortality of the etomidate cohort presented in Fig. 1, as the dose range of etomidate in current study was very wide from 0.02 to 0.5 mg/kg. Considering the fact that other variables had little influences on the derivation of the OR 1.36 of dose-mortality relationship for etomidate use, however, it would be worth studying further sensitivity analysis.
This study had some limitations due to its retrospective nature. First, the MIMIC-III dataset does not clearly mention the reason for prescribing the sedatives. We only gathered information on the prescription of etomidate and propofol and selected patients who were prescribed sedatives on the first day of mechanical ventilation. It was unclear whether the sedatives were used to facilitate intubation or for other purposes. We just assumed that the intensivists used sedatives in patients who required mechanical ventilation.
Second, the MIMIC-III dataset does not explain the physicians’ intentions in choosing etomidate over other drugs. We assumed that the intensivists utilized etomidate because of the benefit that it provides hemodynamic stability in patients in an unfavorable condition. Blood pressure fluctuations were not included in the initial list of variables for the matching procedure. This significant factor is emphasized by the fact that, as presented in Table 1, the average SBP and average MBP of the two cohorts were almost the same. However, fluctuations were observed in SBP, which were wider in the etomidate cohort than in the propofol cohort (82 vs. 68 mmHg, respectively). Although the etomidate cohort showed more severe SBP fluctuations, the MBP was almost the same in the two cohorts, and the difference in the extent of fluctuation between the two groups was 14 mmHg. This greater blood pressure fluctuation indicates an unstable hemodynamic state, which may have affected the decisions of the intensivists in selecting the etomidate which has minimal effect on vital signs.
In conclusion, etomidate usage showed a significant dose-dependent relationship with mortality in ICU patients undergoing mechanical ventilation for a variety of diagnoses. Etomidate was not helpful in improving the initial survival of ICU patients showing unstable vital signs; the etomidate cohort showed 57% lower odds of survival in the first 48 h than the propofol cohort. Although etomidate provides favorable hemodynamics, it failed to improve survival in the first 48 h after administration, and showed a dose-dependent association with increased overall mortality rate (Supplementary Digital Content 3).
Footnotes
Funding
Younsuk Lee and Chi-Yeon Lim has been receiving 2018–2020 R&D Fund from the Korean Government (Ministry of Trade, Industry, and Energy).
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Ha Yeon Park (Conceptualization; Data curation; Investigation; Resources; Writing – original draft; Writing – review & editing)
Younsuk Lee (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Supervision; Visualization)
Chi-Yeon Lim (Data curation; Formal analysis; Software)
Mina Kim (Data curation; Resources; Software)
Jieun Park (Data curation; Investigation; Resources)
Teakseon Lee (Data curation; Formal analysis; Software)
Supplementary Materials
Patient characteristics and pre-existing conditions before and after propensity score matching
Top 20 Admission Diagnoses in After-Matching Cohorts
The full analytical code was developed by the authors and is freely available at https://github.com/ylee03/etomidate_kja
References
- 1.McPhee LC, Badawi O, Fraser GL, Lerwick PA, Riker RR, Zuckerman IH, et al. Single-dose etomidate is not associated with increased mortality in ICU patients with sepsis: analysis of a large electronic ICU database. Crit Care Med. 2013;41:774–83. doi: 10.1097/CCM.0b013e318274190d. [DOI] [PubMed] [Google Scholar]
- 2.Chan CM, Mitchell AL, Shorr AF. Etomidate is associated with mortality and adrenal insufficiency in sepsis: a meta-analysis*. Crit Care Med. 2012;40:2945–53. doi: 10.1097/CCM.0b013e31825fec26. [DOI] [PubMed] [Google Scholar]
- 3.Albert SG, Sitaula S. Etomidate, adrenal insufficiency and mortality associated with severity of illness: a meta-analysis. J Intensive Care Med. doi: 10.1177/0885066620957596. 2020. Advance Access published on Sept 10, 2020. doi: 10.1177/0885066620957596. [DOI] [PubMed] [Google Scholar]
- 4.Komatsu R, You J, Mascha EJ, Sessler DI, Kasuya Y, Turan A. Anesthetic induction with etomidate, rather than propofol, is associated with increased 30-day mortality and cardiovascular morbidity after noncardiac surgery. Anesth Analg. 2013;117:1329–37. doi: 10.1213/ANE.0b013e318299a516. [DOI] [PubMed] [Google Scholar]
- 5.Wagner CE, Bick JS, Johnson D, Ahmad R, Han X, Ehrenfeld JM, et al. Etomidate use and postoperative outcomes among cardiac surgery patients. Anesthesiology. 2014;120:579–89. doi: 10.1097/ALN.0000000000000087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Johnson AE, Pollard TJ, Shen L, Lehman LW, Feng M, Ghassemi M, et al. MIMIC-III, a freely accessible critical care database. Sci Data. 2016;3:160035. doi: 10.1038/sdata.2016.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Simard M, Sirois C, Candas B. Validation of the combined comorbidity index of Charlson and Elixhauser to predict 30-day mortality across ICD-9 and ICD-10. Med Care. 2018;56:441–7. doi: 10.1097/MLR.0000000000000905. [DOI] [PubMed] [Google Scholar]
- 8.Thompson NR, Fan Y, Dalton JE, Jehi L, Rosenbaum BP, Vadera S, et al. A new Elixhauser-based comorbidity summary measure to predict in-hospital mortality. Med Care. 2015;53:374–9. doi: 10.1097/MLR.0000000000000326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Vinclair M, Broux C, Faure P, Brun J, Genty C, Jacquot C, et al. Duration of adrenal inhibition following a single dose of etomidate in critically ill patients. Intensive Care Med. 2008;34:714–9. doi: 10.1007/s00134-007-0970-y. [DOI] [PubMed] [Google Scholar]
- 10.Wasserstein RL, Lazar NA. The ASA’s statement on p-values: context, process, and purpose. Am Stat. 2016;70:129–33. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Patient characteristics and pre-existing conditions before and after propensity score matching
Top 20 Admission Diagnoses in After-Matching Cohorts
The full analytical code was developed by the authors and is freely available at https://github.com/ylee03/etomidate_kja