

To the Editor,
I am a professor and attending pharmacist and writer or co-author of at least 5 manuscripts about different aspects of COVID-19 pharmacotherapy (1-3). More than 18 months from the first report of COVID-19, over 179 million people all over the world infected by this virus, and more than 3.89 million of them have died. Although different treatment approaches have been proposed but management of the COVID-19 patients is steal remained controversial. In this regard, I want to share my personal experience from the exposure to the coronavirus and the consequence of this infection on my health status. I am a 51 years old male, known case of hypertension and dyslipidemia. During working hours of colleagues in the Faculty of Pharmacy, I visited one of my colleagues in his office for 30 minutes. During this conversation both of us wore three-layer medical mask, the widow and door of the room were opened and at least 2-meter distance between us was regarded. After leaving the Faculty, my colleague declares that his RT-PCR test of COVID-19 is positive. It took 3 days for me to experience the first sign of the COVID-19 as fever. Other signs of the disease including arthralgia, myalgia, headache, gastrointestinal (GI) symptoms also appear during this period on day 5th from the exposure to the COVID-19 positive case. Nausea was persistent, especially in the morning. I had a positive RT-PCR test on day 5th after exposure. During the follow-up of the disease within the Shahid-Faghihi Hospital as a referral center for COVID-19 patients, a high-resolution computed tomography (HRCT) scan of the lung was performed but no considerable involvement of the lung was seen (Fig. 1.A) but pulse oximetry revealed that the PO2 saturation rate is about 93% at the same day. In this regard, consulting with infectious disease subspecialist and his recommendation, favipiravir was scheduled with a loading dose of 1600 mg bid and maintenance dose of 800 mg bid for 5 days. Up to day 7th no sign of improvement in my health condition was seen and most of the signs of the infection were worsen during this period and insomnolence and breathing disorders including tachypnea and sporadic cough were other complications. In this regard, another HRCT scan 5 days later from the first scan was scheduled and according to the results 20 % involvement of lung was detected and the bilateral multifocal peripheral patchy ground-glass opacity was highly suggestive for COVID-19 infection. (Fig. 1.B). Another consult with infectious diseases subspecialist and a pulmonologist was taken and anti-inflammatory treatment with prednisolone 10 mg per day and colchicine 1 mg BID were considered and rivaroxaban 10 mg per day as a preventive dose of the anticoagulant agent was taken. On day 3rd from the anti-inflammatory treatment and day 10 from the involvement respiratory signs were improved. PO2 saturation levels according to daily assessment from 88 % was increased to 93 or 94% although during this period fever and myalgia and headache were suppressed but periodic fever and palpitation exist. Due to the severe diarrhea colchicine taking was stop on the day 4th but my general conditioning was profoundly improved about 3 days after initiation of anti-inflammatory therapies.
Figure 1.
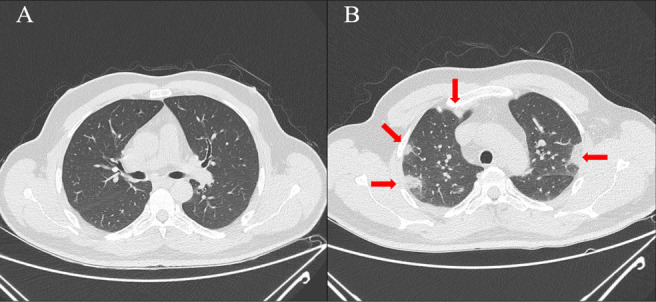
A: HRCT of the lung 5th day after coronavirus exposure, and B: HRCT of the lung on the 10th day after coronavirus exposure.
Different strategies to COVID-19 management can be divided into 5 categories including of pre-exposure prophylaxis, post-exposure prophylaxis, treatment in the outpatient setting, treatment of patients admitted to hospital wards, and treatment of critically ill patients admitted to intensive care unit (ICU) (4). Although, several vaccines have been approved and are available around the world, accessibility and affordability of all people and nations around the world to the COVID-19 vaccine would be challenging. When COVID-19 infection occurred, early patient monitoring and initiation of suitable therapy based on the stages of disease would be essential. After COVID-19 progression to the inflammatory phase, prompt initiation of anti-inflammatory agents including oral or intravenous corticosteroids would be lifesaving to prevent acute respiratory distress syndrome (ARDS).
So, we want to emphasize the necessity of early initiation of anti-inflammatory agents including corticosteroids (5) and colchicine (6) in high-risk patients with mild-to-moderate COVID-19 who shows respiratory system involvement, in order to prevent progression to the severe and critical stages of this disease.
References
- Ghasemiyeh P, Borhani-Haghighi A, Karimzadeh I, Mohammadi-Samani S, Vazin A, Safari A, et al. Major Neurologic Adverse Drug Reactions, Potential Drug–Drug Interactions and Pharmacokinetic Aspects of Drugs Used in COVID-19 Patients with Stroke: A Narrative Review. Ther Clin Risk Manag. 2020;16:595. doi: 10.2147/TCRM.S259152. doi: 10.2147/TCRM.S259152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ghasemiyeh P, Mohammadi-Samani S. Iron Chelating Agents: Promising Supportive Therapies in Severe Cases of COVID-19? Trends Pharmaceut Sci. 2020;6(2):65–6. doi: 10.30476/tips.2020.86274.1047. [Google Scholar]
- Ghasemiyeh P, Mohammadi-Samani S. COVID-19 outbreak: Challenges in pharmacotherapy based on pharmacokinetic and pharmacodynamic aspects of drug therapy in patients with moderate to severe infection. Heart Lung. 2020;49(6):763–773. doi: 10.1016/j.hrtlng.2020.08.025. doi: 10.1016/j.hrtlng.2020.08.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park JJ, Decloedt EH, Rayner CR, Cotton M, Mills EJ. Clinical trials of disease stages in COVID 19: complicated and often misinterpreted. Lancet Glob Health. 2020;8(10):e1249–e50. doi: 10.1016/S2214-109X(20)30365-X. doi: 10.1016/S2214-109X(20)30365-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sterne JA, Murthy S, Diaz JV, Slutsky AS, Villar J, Angus DC, et al. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. JAMA. 2020;324(13):1330–41. doi: 10.1001/jama.2020.17023. doi: 10.1001/jama.2020.17023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deftereos S, Giannopoulos G, Vrachatis DA, Siasos G, Giotaki SG, Cleman M, et al. Colchicine as a potent anti-inflammatory treatment in COVID-19: can we teach an old dog new tricks? Eur Heart J Cardiovasc Pharmacother. 2020;6(4):255. doi: 10.1093/ehjcvp/pvaa033. doi: 10.1093/ehjcvp/pvaa033. [DOI] [PMC free article] [PubMed] [Google Scholar]