

Abstract
The concept of social cohesion has been indicated to be a critical social determinant of health in recent literature. Inconsistencies surrounding the conceptualization and operationalization have made utilizing these findings to inform health intervention and policy difficult. The objective of this article is to provide a theoretical clarification of the concept “social cohesion,” as it relates to health behaviors and outcomes by using the Rodgers’ evolutionary method for concept analyses. This article uncovers the critical attributes, antecedents, and consequences of social cohesion and provides reflection on future use of social cohesion in health literature.
Keywords: concept analysis, health, social cohesion, social environment
Given the important role that social factors have in an individual’s well-being, nursing and related disciplines have been increasingly interested in understanding how social cohesion, a concept characterized as person’s trust and solidarity among a group of people, relates to health.1,2 The concept has been investigated frequently in recent health literature3 and has been found to be associated with several health outcomes, including obesity, diabetes, depression, cardiovascular disease, cancer, and all-cause mortality.4–7 However, because the conceptualization and operationalization of social cohesion in health literature has profound inconsistences, these findings have a modest chance to influence health policy and interventions to improve health outcomes.
Social cohesion is nested within the larger domain of the social environment, which consists of 5 dimensions: (1) socioeconomic position and income inequality, (2) discrimination, (3) neighborhood factors, (4) social support and social networks, and (5) social capital and social cohesion.8 These dimensions are interrelated, often overlap, and are used interchangeably in health literature, contributing to the misunderstanding and uncertainty on the impact of singular dimensions, such as social cohesion.3,9 Moreover, the lack of clarity surrounding these dimensions creates inconsistency in the definition, use, and measurement of these concepts, which in turn makes conclusions regarding the implications of social cohesion on health difficult to establish.10
A deeper understanding of the concept social cohesion is crucial in elucidating its relationship and association with disease development and progression. Moreover, a theoretical clarification will help determine the mechanisms in which social cohesion may be beneficial in health promotion and understanding how social cohesion differs from other social environment dimensions. Such clarifications can be utilized to influence intervention design and health policy to improve community and population health. Thus, this concept analysis aims to provide a clearer understanding of the concept of social cohesion in the context of health behavior and health outcomes.
METHODS
Concept analysis method
This concept analysis was executed following the recommendations outlined in Rodgers’ evolutionary method.11 The method includes 7 steps intended to clarify a concept of interest. These steps include (1) identifying the concept of interest, (2) identifying relevant uses and surrogate terms of the concept, (3) identifying the data sources and sample, (4) identifying attributes of the concept, (5) determining references, antecedents, and consequences of the concept, (6) identifying concepts closely related to the one of interest, and (7) establishing a model case/exemplar of the concept of interest. Further details about these steps appear in Table 1.11 Using the tenants of the 7-step Rodgers’ evolutionary method as a framework, this article organizes these steps in an approach that best offers clarity to the concept social cohesion. In addition to these steps, this concept analysis compares the various operationalizations of the term “social cohesion.”
Table 1.
Components and Definitions of Core Analysis Phasea
| Concept identification | Identify a concept for which a definition and deep exploration is relevant and necessary |
| Surrogate and related terms | Alternative expressions of the concept or terms that heavily overlap with (but do not substitute for) the concept |
| Relevant uses | Uses of the concept that pertains to the field of study |
| Attributes | Characteristics that identify situations that define the concept |
| References | The range of events, situations, or phenomena where the concept is appropriately applied |
| Antecedents | Events or phenomena that have been previously related to the concept and occur previous to the manifestation of the concept |
| Consequences | Events or outcomes that occur as a result of the concept |
| Establishing a model case | An exemplar illustrating application of all components of the concept in action |
From Tofthagen and Fagerstrøm.11
Data sources and sample
A literature search using the key words “social cohesion” and “health” was performed with consultation from a health science librarian. Four databases—PubMed, PyscINFO, Embase, and CINAHL—were searched. A total of 506 articles were identified after the removal of duplicates. Titles and abstracts were screened by one author to determine relevance to this review. Articles were retained if the purpose of the article was to examine the relationship between social cohesion and a health outcome or health behavior. Afterward, full-text articles (n = 90) were screened for eligibility, based on predetermined inclusion and exclusion criteria set by the authorship team. Full-text screening was completed by one author and confirmed by a second. Discrepancies (n = 3) were discussed and resolved with assistance from a third author. To be included, articles must have been an original research article, be no more than 10 years old, identified social cohesion as the predictor/independent variable of interest, identified a health outcome or health behavior as the outcome of interest, and be peer reviewed. The choice to include articles only published within the past 10 years was made to account for current uses of the definition and to allow for examination of the concept in modern environments. Articles were excluded from this analysis if they did not provide a conceptual definition of social cohesion or if they identified social capital as the primary concept of interest, as this was not the focus of the analysis. Twenty-four research articles, all of which were quantitative, met the eligibility criteria to be included in this concept analysis. Additional details of the search summary are provided in the Figure.12
Figure.
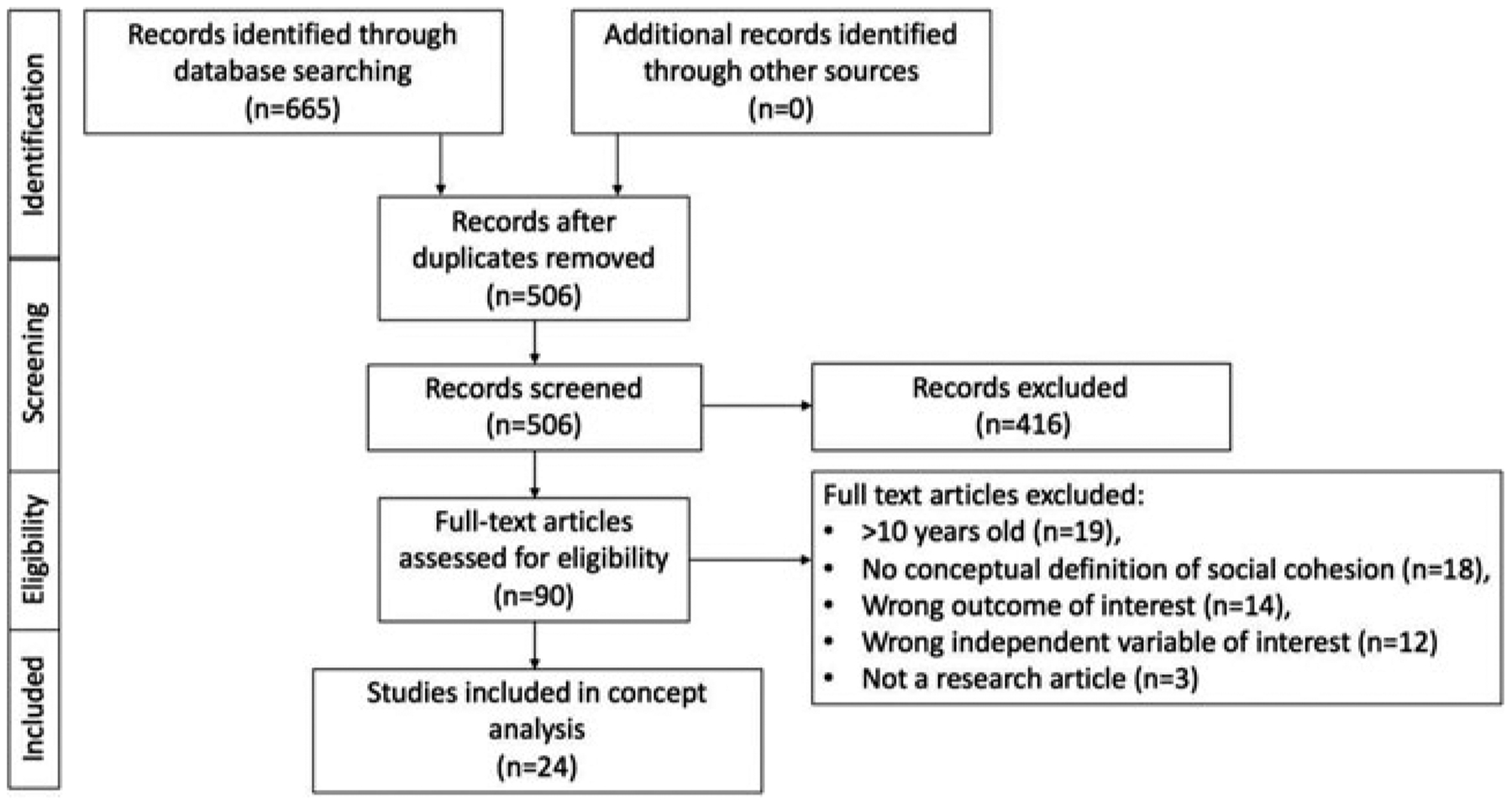
PRISMA flowchart.
Data extraction
After identifying the data sources and sample, data extraction was completed by 3 authors. Each author completed their assignment independently, with a subsequent check completed by a second author. Components were extracted and are presented in the results in the following order: (1) relevant uses of social cohesion, (2) surrogate terms and related concepts of social cohesion, (3) attributes of social cohesion, (4) conceptual definitions of social cohesion, (5) operationalization of social cohesion, and (6) references, antecedent, and health-related consequences of social cohesion. Any discrepancies were resolved through discussion with a minimum of 2 authors.
RESULTS
Relevant uses
The measured health-related behaviors and outcomes in this sample of articles varied. These included health promotion behaviors, such as walking (n = 1)13 and physical activity (n = 2)14,15; activities related to sexual behaviors, such as condom use (n = 1),16 concurrent partner use (n = 1),17 HIV testing (n = 1)17; and health-risk behaviors, such as smoking (n = 1)18 and alcohol use (n = 2).17,19 Health outcomes evaluated included frailty (n = 1),20 violence victimization (n = 1),18 child neglect/abuse (n = 1),21 number of chronic conditions (n = 2),22,23 glycemic control (n = 1),24 myocardial infarction (n = 1),25 posttraumatic stress disorder (n = 1),26 mental/psychological health (n = 7),15,22,23,27–30 body mass index/obesity (n = 2),31,32 self-rated health (n = 5),22,23,33–35 and mortality (n = 1).6 The mechanisms by which social cohesion were hypothesized to affect these behaviors and outcomes are discussed later.
Surrogate terms and related concepts
A common surrogate term for social cohesion identified in this analysis was social capital. Although related, these concepts are different. A concept analysis on social capital suggested the following definition: “social capital is intangible assets, including trust, personal networks, and social norms of reciprocity possessed by a society with a specific culture.”36 To elucidate the relationship between social cohesion and social capital, Berkman and Kawachi37 detailed that socially cohesive communities have a large amount of social capital. Inasmuch, social capital should be regarded as a subset of the concept social cohesion. Other reoccurring related concepts identified in this analysis were social control/disorder,19,20,28 collective efficacy,17,33 community attachment and connectiveness,17 and neighborhood safety.30 These concepts are closely related to, or potentially a consequence of, the attributes and antecedents of social cohesion discussed later.
Attributes
There were 4 primary attributes of social cohesion that emerged from the literature: (1) trust, (2) solidarity, (3) connectedness, and (4) sense of belonging. The most commonly identified of these was trust; it was discussed as the individual’s belief that the people in their community or neighborhood will do good.25 It was often measured through the statement “People in this neighborhood can be trusted,” or similarly-worded question prompts.17,18,20,21,30,32,33,35 Other scales asked respondents to rate their agreement on statements like “local residents watch out that children are safe”28 or “when I’m away from home I know that my neighbors will keep their eyes open for possible trouble.”29 The second attribute, solidarity, refers to the neighborhood’s ability to act together based on a shared value to achieve a goal or provide aid.4,25,33 This was often measured by the statement “people in this neighborhood do not share the same values,”17,18,20,21,30,32,33,35 but also in more direct statements such as, “local residents work together to deal with community problems.”28 In several articles, either connectedness or sense of belonging was used in tandem with trust and solidarity to describe the attributes of social cohesion. These attributes encompass an individual’s feeling of attachment and placement for and within a given community.25,26 They were often measured through the statements, “this is a close-knit neighborhood” and “people in this area generally get along with each other.”17,18,20,21,30,32,33,35 Other scales asked questions regarding knowledge of neighbor’s names, frequency of conversation with neighbors, and interactions with other residents in the area.13
Conceptual definitions
Table 2 displays the conceptual definitions of social cohesion provided by each study. The majority of studies defined social cohesion as a combination of the previously discussed attributes, in addition to some others, including social support, social ties, reciprocity, social tolerance, and social order. The definition provided in Healthy People 2020 by the Office of Disease Prevention and Health Promotion is, “the extent of connectedness and solidarity among groups in society,” which was originally described by Berkman and Kawachi.37,38 One of the studies26 included in this analysis utilized this definition.
Table 2.
Social Cohesion Conceptual Definitions
| Author | Conceptual Definition Provided |
|---|---|
| Caldwell et al20 | Mutual trust and solidarity among residents |
| Chen et al33 | State of affairs concerning vertical and horizontal interactions among members of society; characterized by norms of trust, sense of belonging, willingness to participate and help, and related behaviors |
| Choi and Matz-Costa30 | Perceptions of the extent to which people in one’s community are willing to help each other and can be trusted; an aspect of social competence |
| Chuang et al34 | Attitudes, behaviors, institutional, and structural dimensions that bind citizens together for better life quality |
| de Leon et al13 | Mutual trust and solidarity among neighbors along with the extent of supportive social connections, interactions, and exchange-based behavior |
| Duff et al16 | Perceptions of peer supportiveness, trust, and mutual aid |
| Greif and Nii-Amoo Dodoo28 | Trust, familiarity, values, and neighborhood network ties shared among residents, which serve as the basis from which social capital can be formed |
| Guilcher et al32 | Degree of trust, respect, and participation within a community |
| Hikichi et al26 | Extent of social connectedness and solidarity among groups in a society |
| Inoue et al6 | Characterization of closely-knit social relationships among residents with strong mutual trust and reciprocity |
| Kim et al25 | Perceived degree of connectedness between and among neighbors and their willingness to intervene for the common good; the degree to which one feels secure, connected to the area, and trusts its inhabitants |
| Kingsbury et al29 | Presence of shared values, sense of social order, solidarity, availability of social networks and support, and a sense of community, belonging, or identity |
| Kuipers et al19 | Indicator of attachment to and satisfaction with the neighborhood and its residents |
| Lippman et al17 | Shared trust, connectedness, or unit experienced by members of a residential area or social group |
| Maguire-Jack and Showalter21 | Mutual trust among neighbors |
| Mmari et al18 | Degree to which neighbors share instrumental and emotional support with one another |
| Olamijuwon et al35 | Encompasses trust, social support, tolerance, and quality/quantity of social connections |
| Pabayo et al14 | How harmoniously students, teachers, principals, and other staff relate to each other within a school |
| Perez et al15 | Characterized by the presence of trusting relationships with individuals in one’s community |
| Ruiz et al27 | Presence of communal bonds characterized by altruism, reciprocity, and shared norms and values |
| Smalls et al24 | [Respondents] ability to trust and relate to those in their neighborhood |
| Tang et al22 | Neighborhood social resources in the form of mutual trust and solidarity and expectations for action |
| Wen et al23 | Social relational resources of an area characterized by some degree of homogeneity |
| Yu31 | Strong social ties, mutual trust, and reciprocity within the social network |
Operationalization
Table 3 details the operationalization of social cohesion in each study, which varied greatly. In the 24 studies in this analysis, social cohesion was measured using 16 different scales. It was most frequently measured via the scale introduced by Sampson et al39 (n = 9). This scale is a 5-item Likert-style scale asking respondents to rate their level of agreement or disagreement to the prompts “This is a close-knit area,” “People around here are willing to help neighbors,” “People in the area generally get along with each other,” “People in this area share same values,” and “People in this area can be trusted”. The responses to this scale range from strongly disagree (1) to strongly agree (5). Studies using other scales varied in number of items (range: 2–37) and types of questions and some authors devised their own scale or measurement of social cohesion for the purpose of their study. There was a single study that utilized indicators of social cohesion, rather than an instrument.34
Table 3.
Social cohesion instrument descriptions
| Author | Measurement Scale Description/Origination | Individual Items |
|---|---|---|
| Caldwell et al20
Chen et al33 Guilcher et al32 Lippman et al17a Maguire-Jack and Showalter21 Mmari et al18a Olamijuwon et al35 Perez et al15 Smalls et al24 |
Sampson Cohesion Scale39
5-point Likert scale, responses ranged from “strongly agree” to “strongly disagree” Cronbach α = 0.68–0.84 Validity was not reported |
This is a close-knit area People around here are willing to help neighbors People in this area share same values People in this area can be trusted People in the area generally get along with each other |
| Choi and Matz-Costa30 | Source citation not provided 3-point Likert scale; responses included “strongly agree,” “agree,” and “disagree” Cronbach α = 0.70 Validity was not reported |
People in the neighborhood are willing to help each other People in the neighborhood can be trusted |
| Chuang et al34 | Author-created index based upon Berger-Schmitt and Noll’s framework to measure social cohesion40
Measured 5 factors (derived from exploratory factor analysis): social equality, social inclusion, social development, social capital, and social diversity Cronbach α ranging between 0.57 and 0.80 for 5 factors Measures demonstrated content and construct validity |
Ratio of female/male employment rates and gender wage gap Social, educational, and health expenditures Physician density Government responsibility Household income inequality Social club/organization membership Social trust and quality of social relations Quality of social institutions |
| de Leon et al13 | Author-created scale developed from several established scales13
Cronbach α = 0.71 Validity was not reported |
Do you know neighbors by name? Neighbors with whom you can have a friendly talk Neighbors taking care of each other Neighbors and friends talking outside (Remaining items not provided) |
| Duff et al16 | Community organization and empowerment subscale: Social Cohesion Scale41
Previously adapted and validated in population of interest (sex workers)42 Cronbach α = 0.81 |
You can count on your colleagues if you need to borrow money You can count on your colleagues to accompany you to the doctor or hospital You can count on your colleagues if you need to talk about your problems In general, your colleagues in the area where you work only worry about themselves You can count on your colleagues if you need advice You can count on your colleagues if you need somewhere to stay You can count on your colleagues to help deal with a violent or difficult client You can count on your colleagues to help you find clients You can count on your colleagues to support the use of condoms The group of women/men with whom you work in an integrated group In general, the people you work with are always arguing among each other You can trust the majority of the people working in your area In general, the people you work with get along well |
| Greif and Nii-Amoo Dodoo28 | Source citation not provided 5-point Likert scale, responses ranged from “strongly agree” to “strongly disagree” Cronbach α = 0.60 Validity was not reported |
If there is a problem in the community, neighbors get together to deal with it There are adults in the community that youth can look up to as a role model You can count on adults in this community to watch out that children are safe and do not get into trouble |
| Hikichi et al26 | Scale devised from Kawachi and Berkman’s description of social cohesion37
Evaluated 3 factors: trust, mutual help, and community attachment 5-point Likert scale, responses ranged from 1 “not at all” to 5 “very much” Scale reliability or validity was not reported |
Do you think that people living in your community can be trusted in general? Do you think people living in your community try to help others in most situations? How attached are you to the community in which you live? |
| Inoue et al6 | Author created index from the Shizuoka cohort survey6
Responses included “yes” and “no” Cronbach α = 0.90 Validity was not reported |
Do you get along with the people around you? Are you satisfied with your friendships? Do you have someone you can ask for a favor? Are you satisfied with your relationships with the people around you? |
| Kim et al25 | Utilized scale developed and tested in the English Longitudinal Study of Aging43
Based upon other widely used scales, including Sampson’s39 7-point Likert scale, response options not disclosed Cronbach α = 0.83 Validity was not reported |
I really feel part of this area If you were in trouble, there are lots of people in this area who would help you Many people in this area can be trusted Most people in this area are friendly |
| Kingsbury et al29 | Source citation not provided Scale previously utilized to assess cohesion in children and adolescence44,45 To be completed by the person most knowledgeable about the child 4-point Likert scale, responses ranged from “strongly disagree” to “strongly agree” Internal consistency of 0.86–0.90 in current sample Citation provided for validity46 |
If there is a problem around here, the neighbors get together to deal with it There are adults in the neighborhood that children can look up to People around here are willing to help their neighbors You can count on adults in this neighborhood to watch out that children are safe and do not get in trouble When I am away from home I know that my neighbors will keep their eyes open for possible trouble |
| Kuipers et al19 | Scale items retrieved from the 2006 Netherlands Housing Research questionnaire47
5-point Likert scale, responses included “totally agree,” “agree,” “equal,” “disagree,” and “totally disagree” Cronbach α = 0.83 Validity was not reported |
It is unpleasant to live in this neighborhood I feel attached to this neighborhood I feel at home in this neighborhood I am in touch with my direct neighbors I am in touch with other neighbors In this neighborhood, people treat each other nicely I live in a social neighborhood with a high level of solidarity In this neighborhood, people hardly know each other I am satisfied with the population composition of this neighborhood |
| Pabayo et al14 | Scale devised of 7 subscales. These include relationships between students, relationships between students and teachers, education, security, justice, equity, and membership or belonging14
Cronbach α = 0.92 Principal component analysis demonstrated acceptable construct validity |
Full scale (37 items) not reported |
| Ruiz et al27 | Source citation not provided Utilized items from the English Longitudinal Study of Aging and the Health, Alcohol and Psychosocial factors in Eastern Europe studies Scale reliability and validity was not reported |
Most people in this area cannot be trusted If you were in trouble, there is nobody in this area who would help you |
| Tang et al22 | Scale items extracted from the questions asked in the Chicago Neighborhood and Disability study22
Items aimed to measure social integration and social cohesiveness48 Response scales varied by item Cronbach α = 0.86 Validity was not reported |
Do you see neighbors and friends talking outside in the yard or on the street? Do you see neighbors taking care of each other, such as doing yard work or watching children? Do you see neighbors watching out for each other, such as calling if they see a problem? How many neighbors do you know by name? How many neighbors do you have a friendly talk with at least once a week? Could you call on assistance in doing something around your home or yard to “borrow a cup of sugar” or some other small favor? |
| Wen et al23 | Scale developed based on principal component factor analysis Cronbach α = 0.81 Response scale not disclosed |
People in this neighborhood are willing to help each other People in this neighborhood get along well with each other People in this neighborhood are trustworthy Most people in this neighborhood know each other |
| Yu31 | Source citation does not match scale (modifications not justified)49 4-point Likert scale, responses ranging from “definitely disagree” to “definitely agree” Scale reliability and validity was not provided |
People in this neighborhood help one another People in this neighborhood can be counted on People in this neighborhood can be trusted This is a close-knit neighborhood |
Used a modified version of the Sampson Cohesion Scale.
References, antecedents, and health-related consequences
Antecedents necessary in order for social cohesion to develop were discussed by 14 of the included publications. When mentioned, the antecedents that were described often overlapped with the attributes of social cohesion including trust and connectedness. A single article discussed the built environment as an antecedent to social cohesion.32 These authors suggested that socially cohesive communities exist among places with safe spaces for interactions and connectivity, such as having streets and sidewalks available for neighbors to use to interact with each other.
In the articles included, social cohesion was found to be associated with several health-related consequences. One study identified that neighborhoods with more residential stability and higher levels of social cohesion had lower rates of frailty in older adults20 and another found a direct relationship between social cohesion and improved ability to perform activities of daily living, reports of quality of life, and higher self-related happiness and health.33 Other investigations found correlations between social cohesion and overall improvements in psychological health,30 increased rates of regular walking,13 higher incidence of condom use,16 lower depression,4,15 better glycemic control,24 and reduced rates of smoking.4 Findings from additional literature indicate that social cohesion is associated with lower rates of overweight and obesity,32 less all-cause mortality,6 reduced incidence of myocardial infarction,25 lower rates of child neglect,21 and overall improved status in those with chronic conditions.23
As a result of social cohesion, studies suggest that individuals may be at a better position to receive advice, support, and news, and to act together toward a common goal if they live in a more socially cohesive environment.26,28,34 For example, this might be investing in the school system or passing a new tax to benefit a community center. Initiatives like these have the potential to impact health through safe spaces to exercise, receive services, convene with community members, and share healthy habits. The mechanism through which social cohesion was able to influence these health behaviors and outcomes is suggested in articles. For example, Chen et al33 recommended that social cohesion maintains public order through individuals being willing to participate and intervene for the common good. Similarly, Greif and Dodoo28 believed that social cohesion may prevent crime and neighborhood disorder.
Exemplar
Utilizing the results above, consider the following as an exemplar of how social cohesion can positively influence health behaviors and outcomes. Anthony is an 11-year-old boy who has struggled with being overweight. His family has recently relocated to a new city due to his parent’s employment. His family formerly lived in an urban development with very few children. His parents work into the evening and are unable to transport Anthony to afterschool programs to increase his activity and socialization. The neighborhood in which they now live has other children Anthony’s age that he interacts with regularly (connectedness). Because the children’s parents believe that the children should remain active, the parents created a community soccer league that the children play in after school (solidarity). Since moving there and becoming connected to the other children, Anthony joined the soccer team with neighborhood peers (sense of belonging). When his parents are working after school, a reliable neighbor assists with transporting Anthony to and from soccer practice (trust). Facilitated by the attributes of social cohesion italicized earlier, Anthony has increased physical activity, and in turn, better management of his weight.
DISCUSSION
Our findings reiterated the need for a clarification of the concept of social cohesion. The report of social cohesion in health literature has had a significant increase in the last decade and has been found to be an important social determinant of health. However, a lack of theoretical development and consensus surrounding the conceptualization and operationalization of social cohesion has resulted in the inability to compare and synthesize results from studies that focus on this concept.50 Furthermore, it has inhibited investigators’ ability to utilize these findings to inform intervention and policy. As work progresses to better understand the social determinants of health in individuals and communities, there is a strong need for theoretical development and consensus among social cohesion and its related terms.
A first step in utilizing social cohesion in intervention is understanding its key characteristics (attributes) and what is needed for it to exist (antecedents).11 The most common terms identified for attributes and antecedents were trust, solidarity, connectedness, and sense of belonging. However, among the articles included, a clear distinction between the 2 did not present itself. For example, were trust and solidarity necessary for a socially cohesive society to exist, or were they a result of social cohesion existing within the society? Although distinguishing these might seem trivial, they are important distinctions to make for future intervention science, for one intervention might have the primary aim to foster social cohesion, while another to utilize existing social cohesion to change behavior. To optimize the effectiveness of interventions and create meaningful change in communities, understanding these nuances remains an important area for future research.
The term “social capital” appeared several times in the studies included in this review. “Social capital” and “social cohesion” are used interchangeably in current literature, contributing to the difficulty in delineating place-based effects on health. In a recent of review of literature on the relationship between social capital and obesity, the authors noted that social capital is most often examined through 2 approaches: social cohesion and social support/networks.10 A separate review examining social capital and health described similar trends.9 The latter review took a deeper dive into the utilization of social capital through history and described that “social capital can be understood as a contextual attribute that manifests through social cohesion via mechanisms such as mutual trust, social norms, and reciprocity.”9 Considering this, it is likely that a common error in conceptualizing/operationalizing the 2 concepts is that authors are not identifying that they are measuring social capital as a proxy or construct of social cohesion. Instead, they use the terms synonymously, perpetuating the confusion surrounding the most appropriate conceptualization and distinct operationalization of the 2 terms.
In majority of the included articles, social cohesion was measured at the neighborhood or community level.6,13,15,17–23,25–33,35 Other articles measured social cohesion within larger geographic boundaries, such as the country,34 or within a specific setting, such as work16 and school.14 Given the purpose of this article, it is possible that we missed articles that may include these relevant settings and the benefit of social cohesion within them. For example, a recent concept analysis, discussing the related term social capital, found that increased social capital improves the nursing work environment.51 In those articles measuring social cohesion within a geographic boundary, it was not clear what defined those boundaries (perceived neighborhood, zip code, etc). Currently, there is not an agreed-upon tool to best measure social cohesion, nor an understanding at which level of the population social cohesion can be measured. A previous article discussing the concept of social cohesion supported that social cohesion is a societal construct and therefore should be measured at a national or state level.34 Nonetheless, as noted in our results, a majority of the literature does not do so. A further concern is the point at which a population loses homogeneity is not understood and measuring the concept at the neighborhood, city, county, or state level may influence health differently. To compare results in the future, it is important that articles distinguish the level of measurement (work, school, neighborhood, city, state, etc) to the research participants who are completing the social cohesion survey and to the reader. This conceptualization will also be important in testing mediators of these relationships, as the mechanisms in which social cohesion may influence health may differ at these levels. In addition, key attributes and antecedents of social cohesion, like the built environment, may also differ based on the level at which it is measured.
Considering the challenges discussed previously, identifying a concrete definition of social cohesion remains difficult. There are several different contexts (ie, work, community, and school) in which social cohesion is measured and a lack of clarity surrounding what precedes social cohesion versus the characteristics of social cohesion. Despite these challenges, we offer a working definition of social cohesion based upon our results. Specifically, we suggest that social cohesion is “the degree to which an individual finds trust, solidarity, connectedness, and sense of belonging within a group in society.” This working definition encompasses the most commonly identified attributes and antecedents from the included articles. To accommodate specific settings, such as a school or workplace, the phrase “a group in society” can be replaced.
As this concept analysis has acknowledged the several benefits of social cohesion on health behaviors and outcomes, it is important to also recognize the potential negative implications of social cohesion.52 Assuming healthy habits can be spread and shared in socially cohesive communities, unhealthy habits can be as well. For example, a study examining binge drinking in adolescents found adolescents reporting an increase in community/neighborhood social cohesion were 3.3 times more likely to binge drink than those who did not.52 It is important that future work take this into consideration in the conceptualization of social cohesion and the mechanisms through which it may influence the health behavior or outcome of interest.
This concept analysis has limitations. First, the articles analyzed in this sample assessed social cohesion primarily within one geographic setting, the neighborhood. Because of this, the working definition we provided may not be applicable in other geographic settings that social cohesion is measured, such as the city or state. Second, articles that did not provide a conceptual definition of social cohesion were excluded, leaving several articles examining the concept of social cohesion as a predictor variable out of the analysis. Despite these limitations, this concept analysis has several strengths. To the best of our knowledge, it is the first concept analysis of social cohesion to be completed in the context of health behavior and health outcomes and provides an initial definition for the concept of social cohesion. Providing a standard definition of the concept is significant because it will allow future research on the topic to be conducted with standardized and shared vocabulary. Offering a definition for a concept is important so that future investigations ensure they are examining the same phenomenon and will aid in making comparisons between studies on social cohesion. This analysis included studies that examined social cohesion in relation to both physiological and Psychological behaviors and outcomes, providing a holistic perspective of the potential use of social cohesion in relation to health. Lastly, it enhances the current understanding of both the conceptualization and operationalization of social cohesion, offering a direction for future nurse scientists and researchers to utilize social cohesion in their research.
CONCLUSION
In summary, utilizing a consistent definition of social cohesion is important to strengthening the theoretical conceptualization and operationalization of social cohesion, as it is applied to understanding the social determinants of health. This analysis provided a working definition of social cohesion as the degree to which an individual finds trust, solidarity, connectedness, and sense of belonging within a group in society. In addition, this analysis highlighted the antecedents, attributes, and consequences of social cohesion, which can be utilized to inform future hypotheses surrounding the mechanisms of action in which social cohesion may influence health behaviors or health outcomes. Because nurses play a pivotal role in holistic health among many settings (ie, inpatient, out-patient, community, and schools), they are in a unique position to improve and consider the social determinants of health in their practice. More specifically, with a better theoretical understanding of social cohesion and its related health consequences, nurses and nurse practitioners can consider the influence of social cohesion when developing educational tools and recommending lifestyle changes for their patients. Future research should continue to investigate the most relevant uses of social cohesion and how these can be applied to inform intervention and policy.
Statement of Significance.
What is known or assumed to be true about this topic:
As a dimension of the social environment, social cohesion, or the trust and solidarity among a group of people, has been of increasing interest in health literature. In the past decade, it has been found to be associated with several health behaviors and outcomes. However, due to its lack of conceptual and operational clarity, the findings related to social cohesion and health are difficult to compare and utilize to inform future science.
What this article adds:
This article utilizes Rodgers’ evolutionary method to explore the concept of social cohesion, as it relates to health behaviors and outcomes. This article identifies key attributes, antecedents, and consequences of social cohesion, offers a working conceptual definition of social cohesion, and provides thoughtful commentary for future investigators to consider when examining this dimension of the social environment.
Acknowledgments
HNM was supported by the National Institute of Nursing Research (T32NR012704). RJT was supported by the National Institute on Aging (K02AG059140) and the National Institute on Minority Health and Health Disparities (U54MD000214).
Footnotes
The authors have disclosed that they have no significant relationships with, or financial interest in, any commercial companies pertaining to this article.
REFERENCES
- 1.Healthy People 2020. Social Determinants of Health. https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health. Accessed November 25, 2019.
- 2.Woolf SH, Aron L, eds. U.S. Health in International Perspective: Shorter Lives, Poorer Health. Washington, DC: National Research Council (US), Institute of Medicine (US); 2013. [PubMed] [Google Scholar]
- 3.Kepper MM, Myers CA, Denstel KD, Hunter RF, Guan W, Broyles ST. The neighborhood social environment and physical activity: a systematic scoping review. Int J Behav Nutr Phys Act. 2019;16(1):124. doi: 10.1186/s12966-019-0873-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Echeverría S, Diez-Roux AV, Shea S, Borrell LN, Jackson S. Associations of neighborhood problems and neighborhood social cohesion with mental health and health behaviors: the multi-ethnic study of atherosclerosis. Heal Place. 2008;14(4):853–865. doi: 10.1016/j.healthplace.2008.01.004. [DOI] [PubMed] [Google Scholar]
- 5.Kim ES, Park N, Peterson C. Perceived neighborhood social cohesion and stroke. Soc Sci Med. 2013;97:49–55. doi: 10.1016/j.socscimed.2013.08.001. [DOI] [PubMed] [Google Scholar]
- 6.Inoue S, Yorifuji T, Takao S, Doi H, Kawachi I. Social cohesion and mortality: a survival analysis of older adults in Japan. Am J Public Health. 2013;103(12): e60–e66. doi: 10.2105/AJPH.2013.301311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Glonti K, Mackenbach JD, Ng J, et al. Psychosocial environment: definitions, measures and associations with weight status—a systematic review. Obes Rev. 2016;17(suppl 1):81–95. doi: 10.1111/obr.12383. [DOI] [PubMed] [Google Scholar]
- 8.McNeill LH, Kreuter MW, Subramanian SV. Social environment and physical activity: a review of concepts and evidence. Soc Sci Med. 2006;63(4):1011–1022. doi: 10.1016/j.socscimed.2006.03.012. [DOI] [PubMed] [Google Scholar]
- 9.Rodgers J, Valuev AV, Hswen Y, Subramanian SV. Social capital and physical health: an updated review of the literature for 2007–2018. Soc Sci Med. 2019; 236:112360. doi: 10.1016/j.socscimed.2019.112360. [DOI] [PubMed] [Google Scholar]
- 10.Carrillo-Álvarez E, Kawachi I, Riera-Romaní J. Neighbourhood social capital and obesity: a systematic review of the literature. Obes Rev. 2019;20(1):119–141. doi: 10.1111/obr.12760. [DOI] [PubMed] [Google Scholar]
- 11.Tofthagen R, Fagerstrøm LM. Rodgers’ evolutionary concept analysis—a valid method for developing knowledge in nursing science. Scand J Caring Sci. 2010;24(suppl 1):21–31. doi: 10.1111/j.1471-6712.2010.00845.x. [DOI] [PubMed] [Google Scholar]
- 12.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009; 6(7):e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.de Leon C, Cagney K, Bienias J, et al. Neighborhood social cohesion and disorder in relation to walking in community-dwelling older adults: a multilevel analysis. J Aging Heal. 2009;21(1):155–171. doi: 10.1177/0898264308328650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pabayo R, Janosz M, Bisset S, Kawachi I. School social fragmentation, economic deprivation and social cohesion and adolescent physical inactivity: a longitudinal study. PLoS One. 2014;9(6):e99154. doi: 10.1371/journal.pone.0099154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Perez LG, Arredondo EM, McKenzie TL, Holguin M, Elder JP, Ayala GX. Neighborhood social cohesion and depressive symptoms among Latinos: does use of community resources for physical activity matter? J Phys Act Health. 2015;12(10):1361–1368. doi: 10.1123/jpah.2014-0261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Duff P, Shoveller J, Dobrer S, et al. The relationship between social, policy and physical venue features and social cohesion on condom use for pregnancy prevention among sex workers: a safer indoor work environment scale. J Epidemiol Community Heal. 2015;69(7):666–672. doi: 10.1136/jech-2014-204427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lippman SA, Leslie H, Neilands T, et al. Context matters: community social cohesion and health behaviors in two South African areas. Health Place. 2018; 50:98–104. doi: 10.1016/j.healthplace.2017.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mmari K, Lantos H, Blum RW, et al. A global study on the influence of neighborhood contextual factors on adolescent health. J Adolesc Heal. 2014;55(6):S13–S20. doi: 10.1016/j.jadohealth.2014.08.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kuipers M, van Poppel M, van den Brink W, Win-gen M, Kunst A. The association between neighborhood disorder, social cohesion and hazardous alcohol use: a national multilevel study. Drug Alcohol Depend. 2012;(1/2):27–34. doi: 10.1016/j.drugalcdep.2012.04.008. [DOI] [PubMed] [Google Scholar]
- 20.Caldwell JT, Lee H, Cagney KA. Disablement in context: neighborhood characteristics and their association with frailty onset among older adults. J Gerontol Ser B Psychol Sci Soc Sci. 2019;74(7):e40–e49. doi: 10.1093/geronb/gbx123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Maguire-Jack K, Showalter K. The protective effect of neighborhood social cohesion in child abuse and neglect. Child Abuse Negl. 2016;52:29–37. doi: 10.1016/j.chiabu.2015.12.011. [DOI] [PubMed] [Google Scholar]
- 22.Tang F, Xu L, Chi I, Dong X. Health in the neighborhood and household contexts among older Chinese Americans. J Aging Heal. 2017;29(8):1388–1409. doi: 10.1177/0898264316661829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wen M, Fan J, Jin L, Wang G. Neighborhood effects on health among migrants and natives in Shanghai, China. Health Place. 2010;16(3):452–460. doi: 10.1016/j.healthplace.2009.12.001. [DOI] [PubMed] [Google Scholar]
- 24.Smalls BL, Gregory CM, Zoller JS, Egede LE. Conceptualizing the effect of community and neighborhood factors on type 2 diabetes health outcomes. Environ Behav. 2017;49(5):560–582. doi: 10.1177/0013916516652440. [DOI] [Google Scholar]
- 25.Kim ES, Hawes AM, Smith J. Perceived neighbourhood social cohesion and myocardial infarction. J Epidemiol Community Health. 2014;68(11):1020–1026. doi: 10.1136/jech-2014-204009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hikichi H, Aida J, Tsuboya T, Kondo K, Kawachi I. Can community social cohesion prevent posttraumatic stress disorder in the aftermath of a disaster? A natural experiment from the 2011 Tohoku Earthquake and Tsunami. Am J Epidemiol. 2016;183(10):902–910. doi: 10.1093/aje/kwv335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ruiz M, Malyutina S, Pajak A, Kozela M, Kubi-nova R, Bobak M. Congruent relations between perceived neighbourhood social cohesion and depressive symptoms among older European adults: an East-West analysis. Soc Sci Med. 2019;237:112454. doi: 10.1016/j.socscimed.2019.112454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Greif MJ, Nii-Amoo Dodoo F. How community physical, structural, and social stressors relate to mental health in the urban slums of Accra, Ghana. Health Place. 2015;33:57–66. doi: 10.1016/j.healthplace.2015.02.002. [DOI] [PubMed] [Google Scholar]
- 29.Kingsbury M, Kirkbride JB, McMartin SE, Wick-ham ME, Weeks M, Colman I. Trajectories of childhood neighbourhood cohesion and adolescent mental health: evidence from a national Canadian cohort. Psychol Med. 2015;45(15):3239–3248. doi: 10.1017/S0033291715001245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Choi YJ, Matz-Costa C. Perceived neighborhood safety, social cohesion, and psychological health of older adults. Gerontologist. 2018;58(1):196–206. [DOI] [PubMed] [Google Scholar]
- 31.Yu CY. Racial/ethnic and income differences in obesity among older adults: the role of leisure-time physical activity and neighborhood social cohesion. J Phys Act Health. 2017;14(3):169–175. doi: 10.1123/jpah.2016-0370. [DOI] [PubMed] [Google Scholar]
- 32.Guilcher SJT, Kaufman-Shriqui V, Hwang J, et al. The association between social cohesion in the neighborhood and body mass index (BMI): an examination of gendered differences among urban-dwelling Canadians. Prev Med (Baltim). 2017;99:293–298. doi: 10.1016/j.ypmed.2017.02.022. [DOI] [PubMed] [Google Scholar]
- 33.Chen W, Okumiya K, Wada T, et al. Social cohesion and health in old age: a study in southern Tai-wan. Int Psychogeriatrics. 2015;27(11):1903–1911. doi: 10.1017/S1041610214002907. [DOI] [PubMed] [Google Scholar]
- 34.Chuang YC, Chuang KY, Yang TH. Social cohesion matters in health. Int J Equity Health. 2013;12(1):1. doi: 10.1186/1475-9276-12-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Olamijuwon E, Odimegwu C, De Wet N. Social cohesion and self-rated health among adults in South Africa: the moderating role of race. Heal Place. 2018; 51:89–96. doi: 10.1016/j.healthplace.2018.02.010. [DOI] [PubMed] [Google Scholar]
- 36.Hsieh CH. A concept analysis of social capital within a health context. Nurs Forum. 2008;43(3):151–159. doi: 10.1111/j.1744-6198.2008.00107.x. [DOI] [PubMed] [Google Scholar]
- 37.Berkman LF, Kawachi I. Social Epidemiology. New York, NY: Oxford University Press; 2000:174–190. [Google Scholar]
- 38.Office of Disease Prevention and Health Promotion. Social Determinants of Health. https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-health.
- 39.Sampson RJ, Raudenbush SW, Earls F. Neighborhoods and violent crime: a multilevel study of collective efficacy. Science. 1997;277(5328):918–924. http://www.ncbi.nlm.nih.gov/pubmed/9252316. [DOI] [PubMed] [Google Scholar]
- 40.Berger-Schmitt R, Noll H-H. Conceptual Framework and Structure of a European System of Social Indicators (EUReporting Working Paper No. 9). Mannheim, Germany: Centre for Survey Research and Methodology; 2000. [Google Scholar]
- 41.Lippman SA, Donini A, Díaz J, Chinaglia M, Rein-gold A, Kerrigan D. Social-environmental factors and protective sexual behavior among sex workers: the Encontros intervention in Brazil. Am J Public Health. 2010;100(suppl 1):216–223. doi: 10.2105/AJPH.2008.147462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kerrigan D, Telles P, Torres H, Overs C, Castle C. Community development and HIV/STI-related vulnerability among female sex workers in Rio de Janeiro, Brazil. Health Educ Res. 2008;23(1):137–145. doi: 10.1093/her/cym011. [DOI] [PubMed] [Google Scholar]
- 43.Smith J, Ryan L, Sonnega A, Weir D. Psychosocial and Lifestyle Questionnaire Documentation Report Core Section LB. https://hrs.isr.umich.edu/sites/default/files/biblio/HRS2006-2016SAQDocumentation07.06.17.pdf.
- 44.Curtis LJLJ, Dooley MDMD, Phipps SASA. Child well-being and neighbourhood quality: evidence from the Canadian National Longitudinal Survey of Children and Youth. Soc Sci Med. 2004;58(10):1917–1927. doi: 10.1016/j.socscimed.2003.08.007. [DOI] [PubMed] [Google Scholar]
- 45.Kohen DE, Brooks-Gunn J, Leventhal T, Hertzman C. Neighborhood income and physical and social disorder in Canada: associations with young children’s competencies. Child Dev. 2002;73(6):1844–1860. doi: 10.1111/1467-8624.t01-1-00510. [DOI] [PubMed] [Google Scholar]
- 46.Mujahid MS, Diez Roux AV, Morenoff JD, Raghu-nathan T. Assessing the measurement properties of neighborhood scales: from psychometrics to ecometrics. Am J Epidemiol. 2007;165(8):858–867. doi: 10.1093/aje/kwm040. [DOI] [PubMed] [Google Scholar]
- 47.CBS. Netherlands’ Housing Survey (WoON). https://www.cbs.nl/en-gb/our-services/methods/surveys/korte-onderzoeksbeschrijvingen/netherlands-housing-survey--woon.
- 48.Cagney KA, Glass TA, Skarupski KA, Barnes LL, Schwartz BS, Mendes de Leon CF. Neighborhood-level cohesion and disorder: measurement and validation in two older adult urban populations. J Gerontol B Psychol Sci Soc Sci. 2009;64(3):415–424. doi: 10.1093/geronb/gbn041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Rios R, Aiken LS, Zautra AJ. Neighborhood contexts and the mediating role of neighborhood social cohesion on health and psychological distress among Hispanic and non-Hispanic residents. Ann Behav Med. 2012;43(1):50–61. doi: 10.1007/s12160-011-9306-9. [DOI] [PubMed] [Google Scholar]
- 50.Pérez E, Braën C, Boyer G, et al. Neighbourhood community life and health: a systematic review of reviews. Health Place. 2020;61:102238. doi: 10.1016/j.healthplace.2019.102238. [DOI] [PubMed] [Google Scholar]
- 51.Westphaln KK, Fry-Bowers EK, Georges JM. Social capital: a concept analysis. ANS Adv Nurs Sci. 2020;43(2):E80–E111. doi: 10.1097/ANS.0000000000000296. [DOI] [PubMed] [Google Scholar]
- 52.Martins JG, de Paiva HN, Paiva PCP, et al. New evidence about the “dark side” of social cohesion in promoting binge drinking among adolescents. PLoS One. 2017;12(6):e0178652. doi: 10.1371/journal.pone.0178652. [DOI] [PMC free article] [PubMed] [Google Scholar]