

Abstract
The purpose was to examine and compare the longer-term generalization between 2 different practice dosages for a single-session treadmill slip-perturbation training when reexposed to an overground slip 6 months later. A total of 45 older adults were conveniently assigned to either 24 or 40 slip-like treadmill perturbation trials or a third control group. Overground slips were given immediately after initial training, and at 6 months after initial training in order to examine immediate and longer-term effects. The performance (center of mass stability and vertical limb support) and fall percentage from the laboratory-induced overground slips (at initial posttraining and at 6 mo) were measured and compared between groups. Both treadmill slip-perturbation groups showed immediate generalization at the initial posttraining test and longer-term generalization at the 6-month retest. The higher-practice-dosage group performed significantly better than the control group (P < .05), with no difference between the lower-practice-dosage and the control groups at the 6-month retest (P > .05). A single session of treadmill slip-perturbation training showed a positive effect for reducing older adults’ fall risk for laboratory-induced overground slips. A higher-practice dosage of treadmill slip perturbations could be more beneficial for further reducing fall risk.
Keywords: dosage, longer-term generalization, older adults, stability
Falling is one of the most common and significant health threats faced by older adults.1 Approximately 30% of older adults over age 65 and 50% of older adults over age 80 fall annually.2–4 Most falls among community-dwelling healthy older adults occur due to external perturbations (ie, slips and trips), leading to devastating fall-related injuries.1,5 Specifically, slips are responsible for about 40% of all environmental falls that can lead to severe consequences, such as hip fractures and traumatic brain injuries, which can also cause prolonged hospitalization or even death.6,7
Recent studies indicated that perturbation training is an emerging paradigm to reduce idiopathic falls (without clinical signs or symptoms) among community-dwelling older adults.8 Such perturbation training involves enhancing protective limb responses, such as stepping or grasping, in order to control individuals’ dynamic stability. Dynamic stability is simultaneously affected by the center of mass (COM) position and its velocity relative to the base of support (BOS) (ie, COM state) to prevent environmental-induced falls.9 Specifically, slip-perturbation training is induced by a sudden forward displacement of the BOS relative to the COM. Previous studies have reported that overground slip training induced by a vinyl floor and a low-friction movable platform can significantly reduce the rate of falls within the first several trials through immediate (ie, <5 min) improvements in COM state stability via the process of motor adaptation.10–12 Moreover, the improvements in COM state stability (more anterior relative COM position and greater relative COM velocity), vertical limb support (net extensor force), and fall incidence (lower rate of falls) obtained from a single session of 24 overground induced slips were retained for 12 months.13 Overground slip training has also been shown to possibly transfer/generalize to real-life situations in order to reduce annual falls by 50% in community-dwelling older adults.8 While overground slip-perturbation training might be considered more task specific in relation to real-life fall risk during ambulation, there are some advantages of treadmill-based training paradigms. The treadmill is relatively portable in comparison to the complex laboratory setting of an overground walkway and can be easily translated into rehabilitation clinics. Furthermore, the use of treadmills could be broadly applied to both healthy and frail older adults because the intensity and repetition can be easily modulated. Therefore, it is important to develop a better understanding of the short- and long-term effects of treadmill slip-perturbation training.
Recently, a few studies have reported immediate improvements in stability control resulting from treadmill slip-perturbation training through the process of adaptation.14–16 For example, Patel and Bhatt15 found that the central nervous system adapts to repeated slip-like treadmill perturbations by improving reactive control of stability (ie, the ability to control COM in order to resist fall after the slip onset) through increased compensatory step length and reduced trunk extension. Also, Wang et al16 reported that treadmill slip-perturbation training showed immediate improvements in proactive and reactive control of stability in community-dwelling older adults. Given the similar mechanisms of adaptive improvement in stability control between overground and treadmill slip-perturbation training, it is probable that the stability gained by participants during treadmill slip-perturbation training can be generalized to overground slips.
Emerging studies have provided evidence of immediate generalization such that, after receiving a single session of treadmill-perturbation training of both slip and trip (ie, sudden backward displacement of the BOS relative to the COM),17,18 the likelihood of falls during laboratory-induced slip or trip while overground walking is reduced.13,19 For example, recent studies in young adults found that improvement in fall-resisting skills after computerized treadmill slip-perturbation training generalized immediately to overground slips.20–22 In addition, it has been reported that treadmill slip-perturbation training can be beneficial for older adults, and the improvements in reactive stability control were maintained when they were immediately exposed to a novel overground slip, leading to a reduced fall incidence compared with older adults who received no training.17,23 However, all of these previous studies only examined the transfer of immediate effects from treadmill to overground gait-slip perturbations; longer-term effects of such generalization have yet to be determined.
Besides insufficient evidence of longer-term generalization from a single session of treadmill slip-perturbation training to overground slips, the other major gap yet to be addressed is whether practice dosage would affect such longer-term generalization. It was reported that a 24-slip repetition dosage in a single overground training session outperforms several sessions of single slips delivered over weeks to resist falling over a longer term in a similar environment.24 However, studies on how the practice dosage of treadmill slip training relates to longer-term generalization of performance are very limited. Theoretically, the neuroplasticity induced within the central nervous system from any motor practice is based on the process of consolidation, wherein the long-term memory becomes more stable as time passes.25 It is postulated that overlearning resulting from a higher-practice dosage improves long-term retention.13,24 While such phenomenon has been shown for overground perturbation training, literature from treadmill perturbation training demonstrates some conflicting evidence, albeit limited. König et al26 compared 8 trials, with 1 trial consisting of trip-like perturbation during treadmill walking in middle-aged adults. At the 14-week posttraining retest, they found that subjects who received a higher-practice dosage had a better margin of stability in comparison with those who received a lower-practice dosage. However, Lee et al23 reported that there was no difference in the immediate overground generalization between a higher dosage (40 trials) of treadmill slip-perturbation training and a lower-practice dosage (24 trials), with both dosage groups having better stability on the overground slip trial compared with the control group. This can be explained by the notion that better consolidation of memory usually occurs 24 hours after training.27 Though the benefits of higher repetitions might not be apparent immediately after the initial training, they might appear later and could lead to longer-term generalization effects.
The purpose of this study was to examine the immediate and longer-term generalization to overground slip-perturbation after treadmill slip-perturbation training for 2 different practice dosages. The authors hypothesized that there would be longer-term generalization from the treadmill slip to the overground slip for both dosages (24 and 40 repetitions) of treadmill slip-perturbation training. Both dosages would result in better performance (greater proactive and reactive stability and vertical limb support) and fewer falls on the 6-month overground slip in comparison to the control group (Hypothesis 1). The authors further hypothesized that the higher-practice-dosage treadmill slip-training group would show significantly better performance and fewer falls on the overground slip occurring at 6 months than the lower-practice-dosage group (Hypothesis 2).
Methods
Participants
A total of 45 community-dwelling older adults (age = 74.5 [6.9] y, female = 34) participated in the present study. They were conveniently assigned to 3 groups with equivalent treadmill walking durations: the treadmill training group with 24 slip perturbations (TM_24, n = 15), the treadmill training group with 40 slip perturbations (TM_40, n = 15), and the control group without slip perturbations (Control, n = 15).23 One group of the experiment (TM_24) was finished before the second group (TM_40). Twenty-four repetitions of treadmill slips was chosen as the standard dosage for the first group because many previous overground slip-training studies used this dosage.13 The second set of experiments involved verifying whether the additional treadmill slips (ie, 40 repetitions) would provide better outcomes than the standardized 24 repetitions of the treadmill slip. The addition of around two-thirds more dosage could serve to enhance the longer-term generalization of the gains in performance during overground slip exposure.
All participants were prescreened for neurological, musculo-skeletal, cardiopulmonary, or any other systemic disorders. Older adults with cognitive impairments (score < 25 on the Folstein Mini-Mental State Exam),28 poor mobility (score > 13.5 s on the Timed Up and Go test),29 or symptomatic postural hypotension were excluded. Six subjects in TM_24, 4 subjects in TM_40, and 4 subjects in the control group dropped out. Consequently, a total of 31 subjects (TM_24: n = 9, TM_40: n = 11, Control: n = 11) completed the 6-month retest session (Figure 1A). All participants provided written informed consent, and this study was approved by the institutional review board at the University of Illinois at Chicago.
Figure 1 —
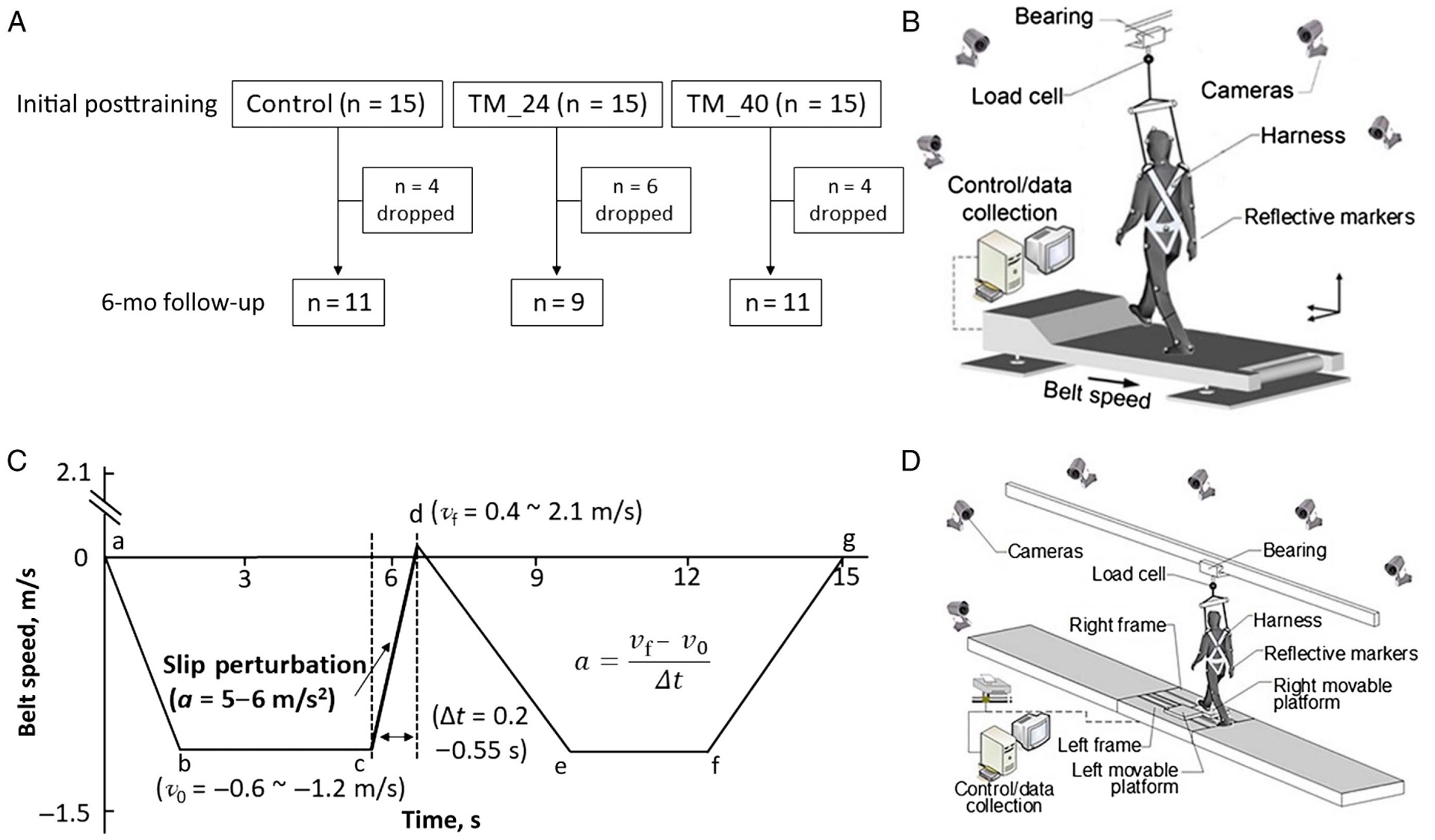
(A) Flow chart of participants in the study; schematics of (B) the treadmill that was used to produce the slip perturbation; (C) the profile of the treadmill slip perturbation; a–b indicates ramping-up duration, b–c indicates steady state of walking duration, c–d indicates slip-perturbation duration, d–e indicates returning duration to steady state of walking, e–f indicates steady state of walking duration, and f–g indicates ramping-down duration; (D) the overground walkway with movable platforms to test the generalization of the treadmill slip-perturbation training.
Experimental Setup
A computer-controlled treadmill (Active Step; Simbex, Lebanon, NH) was used to induce slip perturbations during walking (Figure 1B). The characteristics of the treadmill slip perturbations were designed to induce a forward displacement of each subject’s BOS relative to their COM by a sudden forward acceleration of the previously backward-moving belt. The participants selected their preferred walking speed (v0) on the treadmill from 4 speed options (−1.2, −1.0, −0.8, or −0.6 m/s, Figure 1C).23 The participants were asked to walk on the treadmill at 0.8 m/s for about 30 seconds, and then they were asked if the speed was their most comfortable speed for the training. If not, they were further asked to choose whether to increase or to decrease the walking speed. Once they chose their preferred walking speed, they were asked to walk another 30 seconds for familiarization of treadmill walking. The intensity of each perturbation was determined by 2 factors, the acceleration of the belt (at 2 levels, a: 5 or 6 m/s2) and the duration of its application (at 8 levels, Δt: 0.2, 0.25, 0.3, 0.35, 0.4, 0.45, 0.5, or 0.55 s).23 The final velocity (vf: range 0.4–2.1 m/s) and slip distance (d: range 0.1–0.91 m) were obtained, respectively, using the following equations:
The immediate generalization (ie, initial posttraining) test and the retention (longer-term generalization) test were conducted on an overground walkway. A sliding device was embedded in the middle section of a 7-m walkway to induce slips during overground walking (Figure 1D). This device consisted of a pair (ie, right and left) of low friction, passively movable platforms. Each platform was mounted to an aluminum track via ball bearings and placed on top of 2 tandem force plates (AMTI, Newton, MA) bolted to the ground for recording ground reaction forces. The movable platforms were originally locked and were only unlocked during a slip trial by a computer-controlled release mechanism. The slip trials were induced without alerting the subject and at the instance of the participant’s right heel strike on the right-side platform. Once released, both right and left platforms could slide up to 90 cm.13 To protect the participants from injuries, all subjects wore walking shoes and a full-body safety harness, which was attached to a load cell via a pair of shock-absorbing ropes and further secured to a low-friction ceiling-mounted track.30
Protocol
Every session for all groups began with 3 overground baseline walking trials (Figure 2). Next, the TM_24 and TM_40 groups received 24 and 40 repeated “slips” on the treadmill, respectively. The trial sequence followed the principle of block-and-mixed practice.31 Each block included 4 slip-perturbation trials, and the subjects in the training groups received progressively graded slip perturbation.23 If the subjects could not tolerate a higher threat dosage level during this progression, their remaining “slips” would stay at their highest tolerable level. The TM_40 group had further reinforcement trials (more practice dosage trials at levels 3, 4, and 5) before a cool-down session. The control group completed the same amount of walking time on the treadmill, without any perturbations. Finally, all subjects returned to the same overground walkway and experienced a novel overground slip after 3 to 5 natural walking trials. The subjects were not informed where, when, or how the slip would occur during the test. Six months later, the subjects were asked to come back to the laboratory and were exposed to the same overground slip during walking.
Figure 2 —
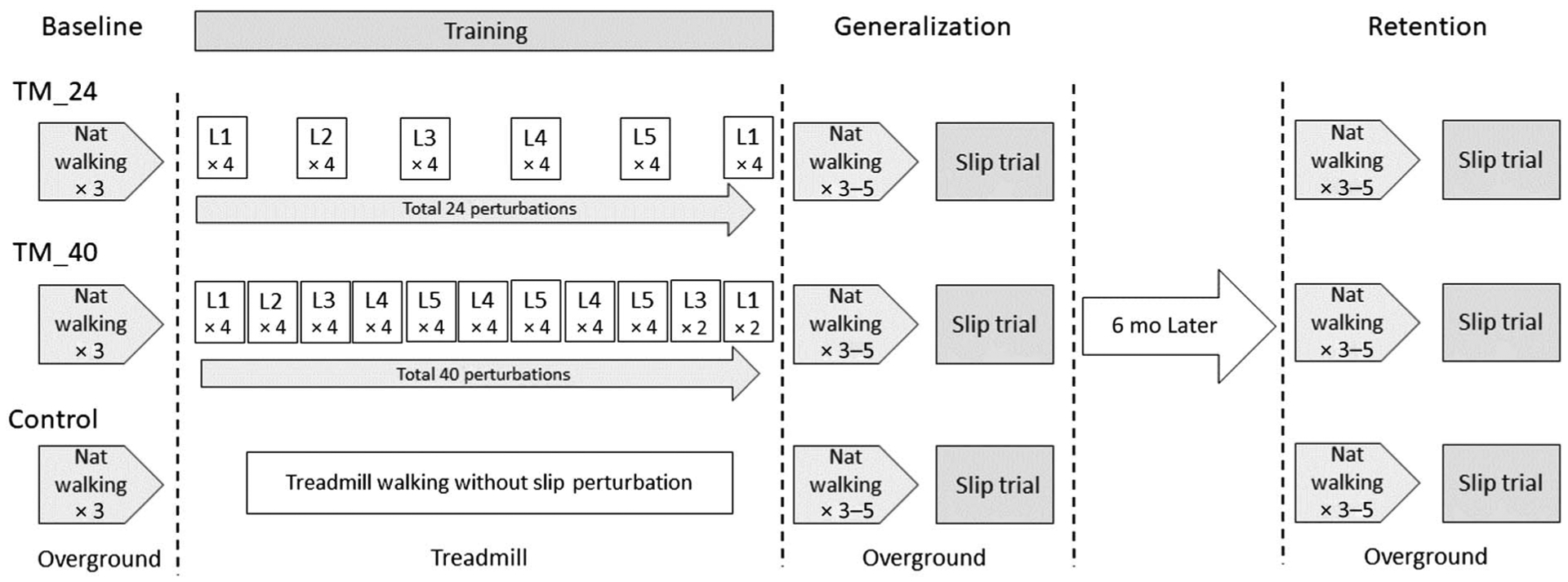
Study protocol for the 3 groups from initial test to retest. TM_24 indicates the treadmill training group with 24 slip perturbations; TM_40, the treadmill training group with 40 slip perturbations.
Data Collection
Thirty reflective markers were placed on the subjects’ bodies and the movable platforms. Kinematic data were recorded using an 8-camera motion capture system (Motion Analysis Corporation, Santa Rosa, CA and Qualisys, Gothenburg, Sweden) at 120 Hz. The marker paths were low-pass filtered at marker-specific cutoff frequencies (ranging from 4.5 to 9 Hz) using fourth-order, zero-lag Butterworth filters.32 The 3-dimensional locations of joint centers, heels, and toes were computed from the filtered marker positions. Force plates, load cells, and platform trigger-release onset signals were collected at 600 Hz and synchronized with motion data at the time of data collection.
Outcome Measure
A fall was determined when the load cell value exceeded 30% of the subject’s body weight.30 The COM state stability in the present study was computed based on the theory of dynamic feasible stability regions.9 The COM state stability was composed of 2 factors, COM position and COM velocity, which were both quantified to examine the contribution of each factor to any stability changes following training (Figure 3A). The COM position and COM velocity were calculated relative to the rear edge of the BOS (ie, the right heel) and were normalized to a dimensionless unit by foot length (lBOS) and , respectively, where g is gravitational acceleration and bh is body height. Stability was defined as the shortest distance from the below boundary of the feasible stability region to the COM state and was assessed at 2 gait events to identify proactive (ie, immediately before slip onset [right touch down]: 85 [30] ms) and reactive (ie, immediately after slip onset [left liftoff]: 100 [50] ms) control.33 A previous study has demonstrated a linear relationship between the change in vertical ground reaction force and change in hip height.34 When the body is unable to generate sufficient vertical supporting force against body gravity (ie, ground reaction force < body weight), limb collapse ensues with the associated downward movement of the pelvis. The collapse can be easily measured by the change of hip height (Figure 3B). Along with stability, hip height is a significant predictor of laboratory falls during overground slips.34 The hip height was calculated as the distance from the bilateral hip midpoint of the 2 hip joint centers to the platform after slip onset.
Figure 3 —
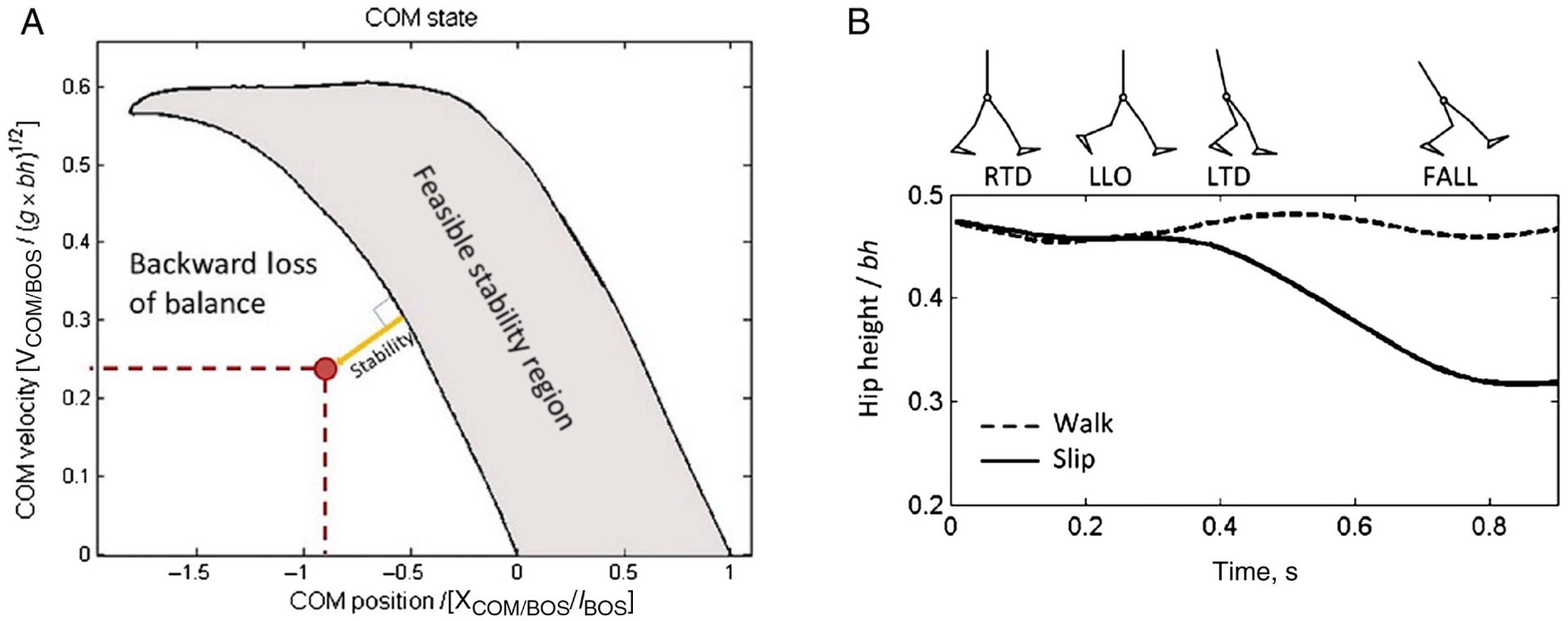
(A) Schematic illustration of the FSR: the LOS against backward balance loss. LOS represents the below boundary of FSR for backward loss of balance. The dynamic stability indicates the magnitude of the instantaneous stability of the COM against backward balance loss and is defined as the shortest distance from the instantaneous COM motion state (circle) to the corresponding LOS. The x-coordinates represent the COM anteroposterior position and the y-coordinates represent the COM velocity. (B) Schematic illustration of the time history of midhip point height during natural walking (dashed line) and gait-slip (solid line). This includes slipping (right) limb touchdown (RTD), recovery step (left) liftoff (LLO), and recovery step (left) touchdown (LTD).34 The actual fall time is identified as the instant the fall-arrest force exerted on the load cell exceeds 30% body weight. COM indicates center of mass; FSR, feasible stability region; LLO, left liftoff; LOS, limits of stability; LTD, left touchdown; RTD, right touchdown.
Statistical Analysis
The authors conducted the preliminary analyses to compare the baseline characteristics of the participants in the TM_24, TM_40, and Control groups using t tests for continuous variables and a chi-square test for the categorical variable to identify confounding variables that could emerge from the baseline sample demographics and dropout status. A generalized estimating equations model (PROC GENMOD) was used to determine if the within-group change (the time factor, initial posttraining vs 6-mo retest) differed as a result of training dosage (the between-group factor) for fall incidence, COM stability, and hip height. The authors used the chi-square test to compare the rate of falls in the 3 groups for the retest data, and the authors used a 1-way analysis of variance to compare COM stability and hip height between the 3 groups for the retest measurements. Gabriel pairwise post hoc tests were conducted to compare differences among the groups. All analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC) with a significance level of .05.
Results
The participants in all 3 groups had comparable ages, heights, body weights, cognitive scores, balance confidences, histories of falls, and Berg Balance Scores (Table 1). There were no significant between-group differences in the variables for both the initial and retest measurements (P > .05), except for the Timed Up and Go test score during the initial test (P < .05). The Timed Up and Go test score was significantly different between the TM_24 and Control groups (P = .007). This confounding variable was adjusted in the generalized estimating equations model. There were no significant between-group differences in the perturbation intensity (slip acceleration and duration, P > .05) and the walking speed (P > .05) on the treadmill. Also, there were no significant between-group differences in the variables after sample size attrition at 6 months (P > .05).
Table 1.
Sample Demographics and Confounding Factors by Groups, Means (SD)
| Group | Pooled | ||||||
|---|---|---|---|---|---|---|---|
| TM_24 (n = 15) | TM_40 (n = 15) | Control (n = 15) | P value | Returned (n = 31) | Not returned (n = 14) | P value | |
| Age, y | 76.8 (6.1) | 72.9 (6.7) | 73.9 (7.7) | .30 | 74.5 (6.9) | 75 (5.4) | .77 |
| Height, m | 1.6 (0.1) | 1.6 (0.1) | 1.6 (0.1) | .75 | 1.6 (0.1) | 1.7 (0.1) | .06 |
| Weight, kg | 64.3 (10.7) | 68.1 (12.0) | 71.0 (13.5) | .30 | 68.1 (12.0) | 70.3 (9.3) | .40 |
| MMSE | 27.8 (1.8) | 28.6 (1.7) | 27.3 (1.8) | .14 | 27.8 (1.9) | 27.8 (2.0) | .97 |
| ABC | 92.0 (8.7) | 89.5 (8.7) | 92.0 (7.0) | .63 | 90.6 (7.9) | 92.3 (7.8) | .52 |
| Fall hx/y,a % | 38 | 38 | 43 | .96 | 40 | 25 | .20 |
| BBS | 64.3 (10.7) | 68.1 (12.0) | 71.0 (13.5) | .30 | 55.3 (1.3) | 54.5 (2.2) | .22 |
| TUG, s | 7.2 (1.5) | 9.4 (1.9) | 7.9 (1.8) | .01 | 8.1 (1.9) | 8.2 (2.0) | .92 |
| Walking speed on TM, m/s | 0.9 (0.2) | 0.9 (0.1) | 0.9 (0.2) | .96 | 0.8 (0.2) | 0.9 (0.2) | .09 |
Abbreviations: ABC, activities-specific balance confidence scale; BBS, Berg Balance Scores; hx, history; MMSE, Mini-Mental State Examination; TM, treadmill; TUG, Timed Up and Go test; TM_24, the treadmill training group with 24 slip perturbations; TM_40, the treadmill training group with 40 slip perturbations.
Number of falls within past year.
The Rate of Falls
At the initial posttraining test, 13%, 33%, and 60% of the participants fell, while 9%, 44%, and 73% fell during the 6-month retest for the TM_40, TM_24, and Control groups, respectively. There was no significant difference in fall rates between the initial posttraining test and the 6-month follow-up test in the 3 groups (main effect, P = .420; TM_24, P = .607; TM_40, P = .732; Control, P = .457, Table 2, Figure 4). In addition, there were overall group effects for the rate of falls (ie, the combination of initial posttraining and 6-mo follow-up test) between the TM_40 and Control groups (P = .020), while there were no significant differences between the TM_24 and Control groups (P = .510) or between the TM_24 and TM_40 groups (P = .089). Also, there was a significant difference in the falling rate between groups for the 6-month follow-up test (X2 [2, n = 31] = 9.18, P = .010). The post hoc test indicated that the rate of falls for TM_40 was significantly less than for Control (P = .002); however, there were no significant differences between TM_24 and Control (P = .199) or between TM_40 and TM_24 (P = .069).
Table 2.
Generalized Estimating Equations Model for Change in Rate of Falls, Proactive Control of Stability, Reactive Control of Stability, and Hip Height in 3 Groups (Control, TM_24, and TM_40) With Initial Posttraining and 6-Month Follow-Up Test
| Predictor: rate of falls | OR | 95% CI | P value |
|---|---|---|---|
| Time (initial vs retest) | 0.57 | −0.81 to 1.95 | .420 |
| Group (Control vs TM_24) | −0.52 | −2.10 to 1.04 | .510 |
| Group (Control vs TM_40) | −2.19 | −4.03 to −0.35 | .020 |
| Group (TM_24 vs TM_40) | −1.66 | −3.58 to 0.25 | .089 |
| Group (Control vs TM_24) × time (initial vs retest) | −0.30 | −2.61 to 2.02 | .803 |
| Group (Control vs TM_40) × time (initial vs retest) | −0.99 | −3.94 to 1.97 | .513 |
| TUG score | −0.18 | −0.45 to 0.11 | .238 |
| Predictor: proactive control of stability | Estimate | 95% CI | P value |
| Time (initial vs retest) | 0.02 | −0.02 to 0.05 | .375 |
| Group (Control vs TM_24) | −0.01 | −0.05 to 0.03 | .668 |
| Group (Control vs TM_40) | 0.04 | 0.00 to 0.07 | .046 |
| Group (TM_24 vs TM_40) | 0.05 | 0.01 to 0.09 | .022 |
| Group (Control vs TM_24) × time (initial vs retest) | 0.01 | −0.05 to 0.06 | .822 |
| Group (Control vs TM_40) × time (initial vs retest) | 0.00 | −0.04 to 0.04 | .860 |
| TUG score | 0.01 | −0.00 to 0.01 | .092 |
| Predictor: reactive control of stability | Estimate | 95% CI | P value |
| Time (initial vs retest) | 0.04 | −0.51 to 0.11 | .336 |
| Group (Control vs TM_24) | 0.13 | 0.00 to 0.26 | .049 |
| Group (Control vs TM_40) | 0.20 | 0.10 to 0.21 | <.001 |
| Group (TM_24 vs TM_40) | 0.08 | −0.04 to 0.09 | .211 |
| Group (Control vs TM_24) × time (initial vs retest) | −0.06 | −0.20 to 0.09 | .453 |
| Group (Control vs TM_40) × time (initial vs retest) | −0.04 | −0.16 to 0.07 | .446 |
| TUG score | 0.00 | −0.01 to 0.03 | .418 |
| Predictor: hip height | Estimate | 95% CI | P value |
| Time (initial vs retest) | 0.01 | −0.01 to 0.04 | .258 |
| Group (Control vs TM_24) | −0.00 | −0.03 to 0.03 | .876 |
| Group (Control vs TM_40) | 0.04 | 0.01 to 0.07 | .013 |
| Group (TM_24 vs TM_40) | 0.04 | 0.01 to 0.08 | .006 |
| Group (Control vs TM_24) × time (initial vs retest) | −0.00 | −0.04 to 0.04 | .883 |
| Group (Control vs TM_40) × time (initial vs retest) | −0.01 | −0.05 to 0.03 | .636 |
| TUG score | 0.01 | 0.00 to 0.01 | .001 |
Abbreviations: 95% CI, 95% confidence interval; OR, odds ratio; TUG, Timed Up and Go test; TM_24, the treadmill training group with 24 slip perturbations; TM_40, the treadmill training group with 40 slip perturbations.
Figure 4 —
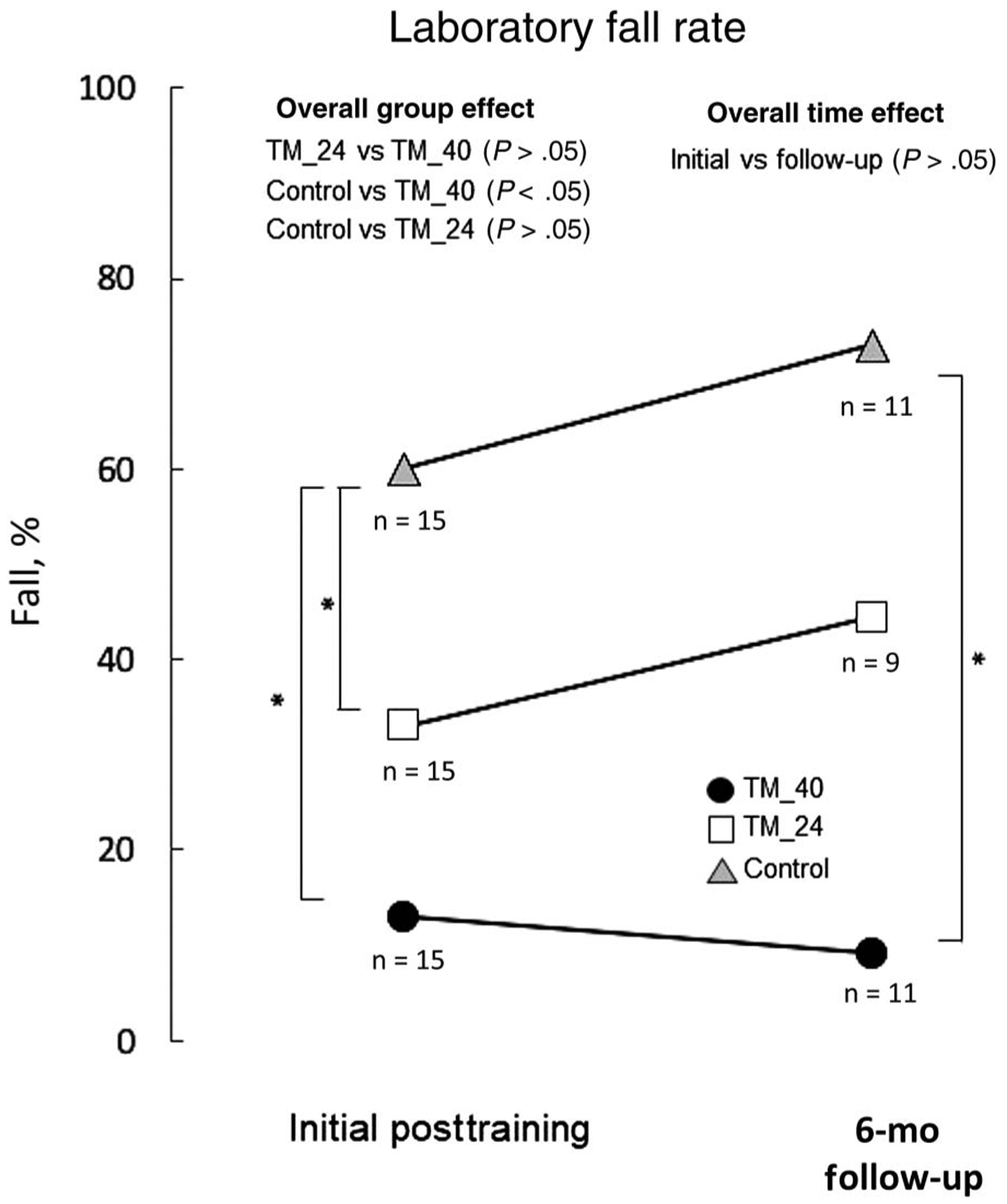
Rate of falls between the 3 groups (TM_40, TM_24, and Control) upon their novel overground slip (ie, initial posttraining generalization test) and 6-month retest during overground walking. TM_24 indicates the treadmill training group with 24 slip perturbations; TM_40, the treadmill training group with 40 slip perturbations. *P < .05.
Proactive Control
There was no significant difference in proactive control of stability between the initial posttraining test and the 6-month retest (main effect, P = .375; TM_24, P = .437; TM_40, P = .094; Control, P = .462, Table 2, Figure 5A). However, there were overall effects for proactive control of stability between the experimental groups. TM_40 exhibited significantly better proactive control of stability in comparison to Control (P = .046) and TM_24 (P = .022), but there was no significant group effect between TM_24 and Control (P = .668). During the 6-month follow-up test, no difference in proactive control was found between groups (F2,30 = 2.40, P = .110).
Figure 5 —
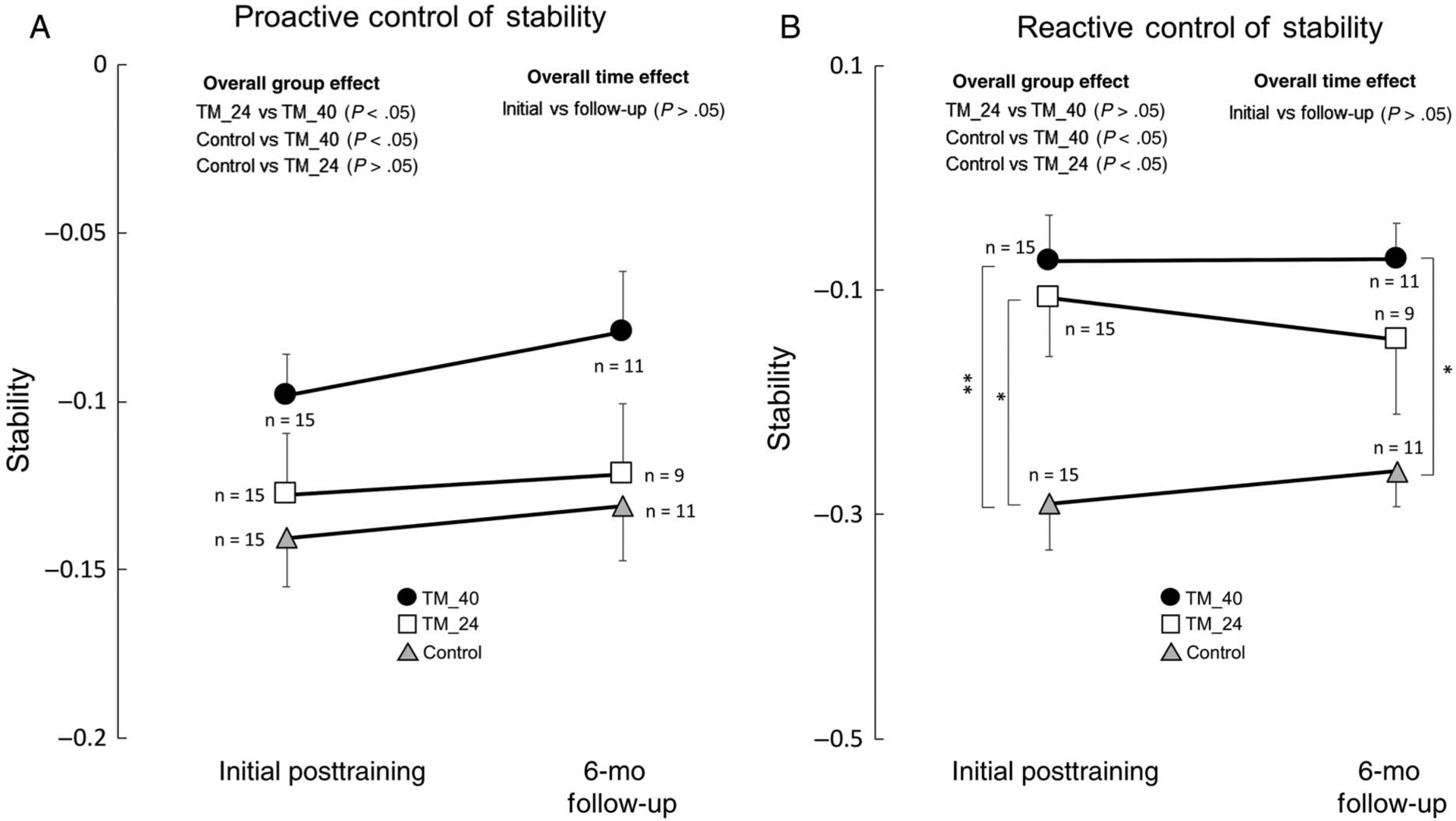
(A) Proactive control (ie, immediately prior to the novel slip onset) comparisons of stability at right foot (ie, slipping foot) touchdown between the 3 groups (ie, Control, TM_24, and TM_40) upon their novel overground slip (ie, initial posttraining generalization test) and 6-month retest during overground walking. (B) Reactive control (ie, immediately after the slip onset) comparisons of stability between the 3 groups (ie, Control, TM_24, and TM_40) upon their novel overground slip (ie, initial posttraining generalization test) and 6-month retest during overground walking. TM_24 indicates the treadmill training group with 24 slip perturbations; TM_40, the treadmill training group with 40 slip perturbations. *P < .05 and **P < .01.
Reactive Control
There was no significant difference in reactive control of stability between the initial posttraining test and the 6-month retest (main effect, P = .336; TM_24, P = .590; TM_40, P = .903; Control, P = .314, Table 2, Figure 5B). However, there were overall group effects for reactive control of stability. TM_40 and TM_24 both demonstrated significantly better reactive control of stability in comparison to Control (P < .001 and P = .049, respectively), but TM_40 was not significantly different from TM_24 (P = .211). During the 6-month follow-up test, there were main effects between groups (F2,30 = 4.21, P = .025). Post hoc tests indicated that TM_40 displayed significantly higher reactive control of stability than Control (P = .003), while no significant differences were found between TM_24 and Control (P = .154) or between TM_40 and TM_24 (P = .314).
Furthermore, there was no significant difference in hip height between the initial posttraining test and the 6-month retest (main effect, P = .258; TM_24, P = .647; TM_40, P = .684; Control, P = .143, Table 2, Figure 6). However, there were overall group effects for hip height. TM_40 exhibited a significantly higher hip height in comparison to Control (P = .013) and TM_24 (P = .006), but there was no significant group effect between TM_24 and Control (P = .876). During the 6-month follow-up test, there was a main effect of hip height (F2,30 = 3.78, P = .035). Post hoc tests demonstrated that hip height for TM_40 was significantly higher than for Control (P = .006), while there were no significant differences between TM_24 and Control (P = .340) or between TM_40 and TM_24 (P = .129).
Figure 6 —
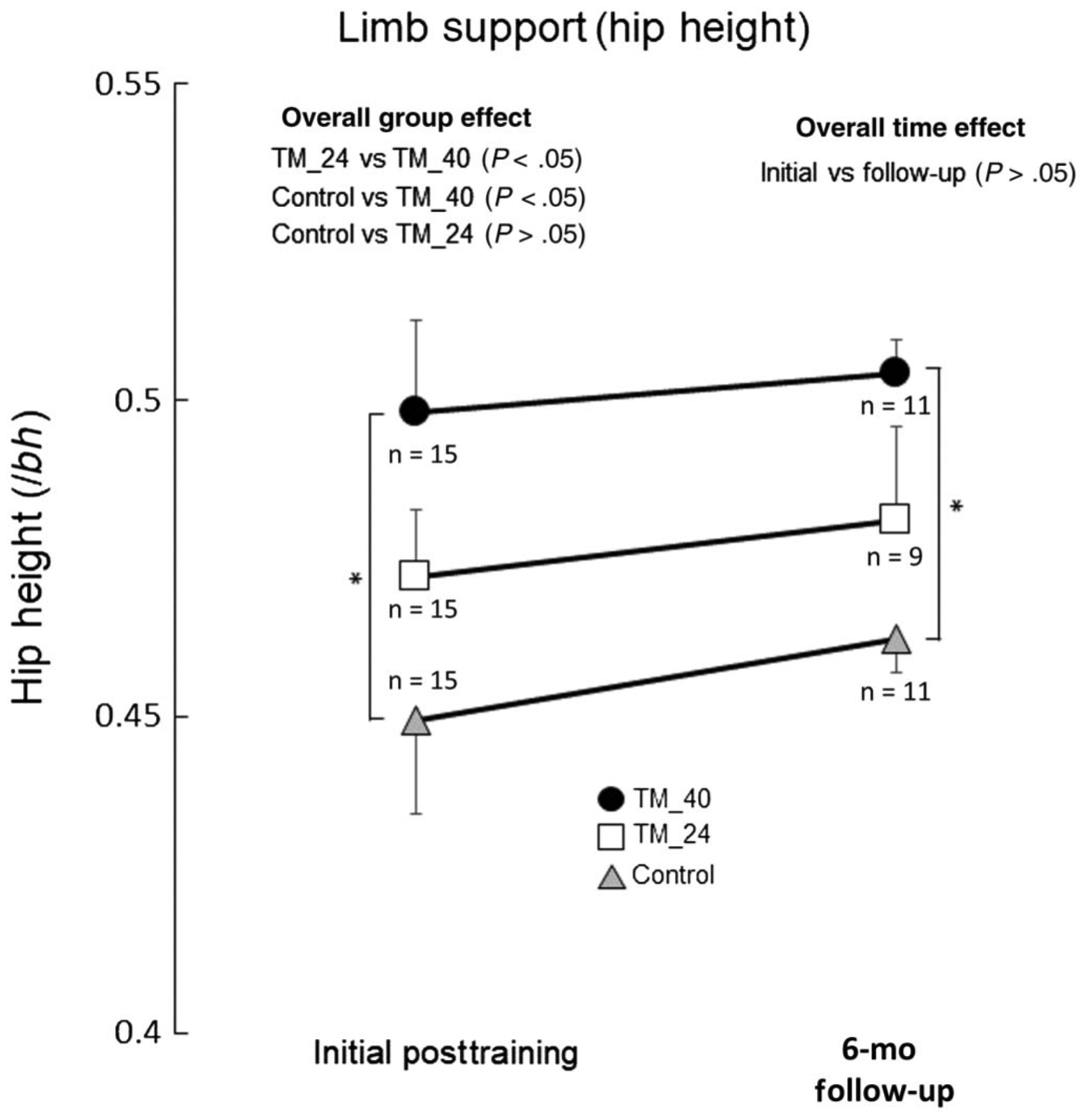
Limb support (hip height) at left foot (ie, recovery foot) touchdown comparisons between the 3 groups (ie, Control, TM_24, and TM_40) upon their novel overground slip (ie, initial posttraining generalization test) and 6-month retest during overground walking. TM_24 indicates the treadmill training group with 24 slip perturbations; TM_40, the treadmill training group with 40 slip perturbations *P < .05, **P < .01, and ***P < .001.
Discussion
Our results indicated that there was significantly greater stability control and fewer falls in the group receiving treadmill slip-perturbation training compared with the control group when exposed to an overground slip minutes after the initial session. Furthermore, such improvement was retained 6 months after training, suggesting positive longer-term generalization. There was no significant difference between the higher-practice-dosage (40 slips) group and the lower-practice-dosage (24 slips) group at the 6-month retest. However, only the higher-practice dosage showed a significant lower fall rate compared with the control group, with no significant difference between the low-practice dosage group and the control group, suggesting greater performance gains led by the higher-practice dosage in the longer term.
Consistent with our first hypothesis, the subjects exhibited immediate and longer-term generalization from the treadmill slip perturbation to the overground slip. These generalizations are evident by the absence of statistically significant differences in the rate of falls at the 6-month retest compared with the initial posttraining test and the lower number of falls than the control group. Such a generalization is possible, as treadmill slip-perturbation training has been shown to cause changes within the reactive balance control, resulting in improved fall-resisting skills similar to those required to recover from overground slips.12,16,17 For example, it has been previously shown in older adults that treadmill slip-perturbation training (using a protocol and instrumentation similar to this study) allows for the development of implicit motor strategies via a trial-and-error learning process to improve COM state stability control (ie, larger compensatory stepping against slip).16 After several trials of the treadmill slip perturbation, this process may result in updates to the internal representation of stability limits within the central nervous system.35,36 The updated stability limits may be stored within motor memory and could be retrieved when encountering a similar environmental threat (ie, novel over-ground slip).10
The results in the present study partially support our second hypothesis. Although there were no significant differences between the higher (40 slips)- and lower (24 slips)-practice-dosage groups, only the higher-practice-dosage group showed significant better outcomes in comparison with the control group, while the lower-dosage group was not significantly different. It has been established that overtraining (ie, high repetitions) is an essential factor to lead to longer-term changes in performance. The results that the lower-dosage group did not show any significant difference from the control group at the 6-month period suggest that the lower dosage might not be enough to elicit overlearning. The improved retention of immediate performance gains at 6 months for the higher-dosage group might suggest that the greater number of exposures (two thirds more) could suffice and might be required to consolidate motor memory for later retrieval. Moreover, Karamanidis et al11 reviewed the practice-dose–response relationship by applying perturbation training during gait based on the recent data in older adults. They reported that a lower-practice dosage might limit the longer-term changes in balance responses, which are generalizable to real daily life perturbation (eg, slip and trip) situations.
In the present study, the higher-practice-dosage group (TM_40) demonstrated significantly better performance than the control group on the immediate generalization test and maintained that improvement at 6 months, whereas the TM_24 group exhibited a slight motor memory decay in reactive stability. This difference could have led to a higher fall incidence for the TM_24 group at 6 months compared with their own initial generalization test. Also, the higher-practice-dosage group showed overall group differences (ie, combining initial posttraining and 6-mo follow-up tests) in proactive control of stability and limb support in comparison to the lower-practice-dosage group, while there were no overall group differences in reactive control or fall rates between the 24- and 40-practice-dosage groups.
Although the overall performance in the control group was worse than the treadmill slip-perturbation training groups, its performance was maintained at that level with no further decay in stability, limb support, and falls incidence. Our findings are in accordance with a previous study, which reported a remarkable “single-trial” effect of overground-slip exposure on long-term retention.37 That study applied a single overground novel slip to healthy community-dwelling older adults and found that the single slip trial experience was sufficient to reduce the rate of falls by about 20% at the 6-month retest. Along with this effect, the subjects demonstrated a significant improvement in reactive stability control that lasted as long as 12 months. It is possible in the present study that the effects of fall reduction and improvement in the dynamic stability after the control group’s exposure to a single overground slip was due to familiarization and anticipatory mechanisms affecting reactive responses.37 While both the previous and the present studies showed that the “single-trial” of overground slip is effective on long-term retention, additional trials would be more beneficial for reducing falls of daily living. Specifically, the previous results have indicated that, even though a single slip exposure could lead to fall reduction when exposed to the same laboratory environment 12 months later, it could not significantly reduce real-life fall risk, which was seen in the group that received repeated slip training.8,37
This study was able to produce valuable insight to perturbation training; however, it has a few limitations. For example, it is still unknown whether a further reduced practice dosage than the “low dosage” used in this study (ie, number of trials < 24) could affect the results of longer-term generalization. Along with that, the small sample size, especially at the 6-month retest, and the convenient sample assignment of the present study may limit its broad application. Also, there were only 4 options to determine self-selected treadmill walking speed (0.6, 0.8, 1.0, and 1.2 m/s) for the participants, and increments in walking speed at 0.2 m/s intervals could be considered to be set at a lower resolution. In addition, the lack of baseline over-ground-slip response data is a limitation of the study. However, a “baseline” overground slip trial was not included to prevent the “first trial” effect,38–40 which could lead to changes in participant behavior and introduce a bias. Furthermore, this study did not report the participants’ performance improvement (ie, learning curve) during treadmill slip-perturbation training, as results of the treadmill slip-perturbation training led improvements on COM state stability in older adults, which have been previously published.16 However, the 3-group posttest-only design was sufficient to demonstrate immediate and longer-term performance on overground slips after receiving different dosages of treadmill slip-perturbation training versus the control group.
Conclusion
Our results demonstrated that community-dwelling older adults can reduce both immediate and longer-term fall risk from laboratory-induced overground slips after a single session of treadmill slip-perturbation training of at least 24 slips compared with those who receive no training. Moreover, our results suggest that providing more practice by increasing the dosage to 40 treadmill slip perturbations may further assist in maintaining the performance improvements over the longer term.
Acknowledgments
This work was supported by the National Institutes of Health (R01-AG029616 to [Clive] Y.-C.P. and R01-AG044364 to [Clive] Y.-C.P. and T.B.). The authors thank Dr Edward Wang for his consultation in statistical data analysis and Ms Alison Schenone, Ms Shamali Dusane, and Ms Julia Lerman for assisting in editing the manuscript. The authors have no conflicts of interest to disclose.
References
- 1.Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing. 2006;35(suppl 2):ii37–ii41. doi: 10.1093/ageing/afl084 [DOI] [PubMed] [Google Scholar]
- 2.Morris JC, Rubin EH, Morris EJ, Mandel SA. Senile dementia of the Alzheimer’s type: an important risk factor for serious falls. J Gerontol. 1987;42(4):412–417. doi: 10.1093/geronj/42.4.412 [DOI] [PubMed] [Google Scholar]
- 3.Moylan KC, Binder EF. Falls in older adults: risk assessment, management and prevention. Am J Med. 2007;120(6):493.e1–493.e6. doi: 10.1016/j.amjmed.2006.07.022 [DOI] [PubMed] [Google Scholar]
- 4.Sattin RW. Falls among older persons: a public health perspective. Annu Rev Public Health. 1992;13(1):489–508. doi: 10.1146/annurev.pu.13.050192.002421 [DOI] [PubMed] [Google Scholar]
- 5.Dijkstra BW, Horak FB, Kamsma YP, Peterson DS. Older adults can improve compensatory stepping with repeated postural perturbations. Front Aging Neurosci. 2015;7:201. doi: 10.3389/fnagi.2015.00201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Luukinen H, Herala M, Koski K, Honkanen R, Laippala P, Kivela SL. Fracture risk associated with a fall according to type of fall among the elderly. Osteoporos Int. 2000;11(7):631–634. doi: 10.1007/s001980070086 [DOI] [PubMed] [Google Scholar]
- 7.Boyé ND, Van Lieshout EM, Van Beeck EF, Hartholt KA, Van der Cammen TJ, Patka P. The impact of falls in the elderly. Trauma. 2013;15(1):29–35. doi: 10.1177/1460408612463145 [DOI] [Google Scholar]
- 8.Pai Y-C, Bhatt T, Yang F, Wang E. Perturbation training can reduce community-dwelling older adults’ annual fall risk: a randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2014;69(12):1586–1594. doi: 10.1093/gerona/glu087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pai YC, Patton JL. Center of mass velocity-position predictions for balance control. J Biomech. 1997;30(4):347–354. doi: 10.1016/S0021-9290(96)00165-0 [DOI] [PubMed] [Google Scholar]
- 10.Bhatt T, Pai Y-C. Generalization of gait adaptation for fall prevention: from moveable platform to slippery floor. J Neurophysiol. 2009;101(2):948–957. doi: 10.1152/jn.91004.2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Karamanidis K, Epro G, McCrum C, König M. Improving trip-and slip-resisting skills in older people: perturbation dose matters. Exerc Sport Sci Rev. 2020;48(1):40–47. doi: 10.1249/JES.0000000000000210 [DOI] [PubMed] [Google Scholar]
- 12.Okubo Y, Sturnieks DL, Brodie MA, Duran L, Lord SR. Effect of reactive balance training involving repeated slips and trips on balance recovery among older adults: a blinded randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2019;74(9):1489–1496. doi: 10.1093/gerona/glz021 [DOI] [PubMed] [Google Scholar]
- 13.Pai Y-C, Yang F, Bhatt T, Wang E. Learning from laboratory-induced falling: long-term motor retention among older adults. Age. 2014;36(3):9640. doi: 10.1007/s11357-014-9640-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yang F, Cereceres P, Qiao M. Treadmill-based gait-slip training with reduced training volume could still prevent slip-related falls. Gait Posture. 2018;66:160–165. doi: 10.1016/j.gaitpost [DOI] [PubMed] [Google Scholar]
- 15.Patel P, Bhatt T. Adaptation to large-magnitude treadmill-based perturbations: improvements in reactive balance response. Physiol Rep. 2015;3(2):e12247. doi: 10.14814/phy2.12247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wang Y, Wang S, Lee A, Pai Y-C, Bhatt T. Treadmill-gait slip training in community-dwelling older adults: mechanisms of immediate adaptation for a progressive ascending-mixed-intensity protocol. Exp Brain Res. 2019;237(9):2305–2317. doi: 10.1007/s00221-019-05582-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wang Y, Bhatt T, Liu X, et al. Can treadmill-slip perturbation training reduce immediate risk of over-ground-slip induced fall among community-dwelling older adults? J Biomech. 2019;84:58–66. doi: 10.1016/j.jbiomech.2018.12.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Crenshaw JR, Kaufman KR, Grabiner MD. Compensatory-step training of healthy, mobile people with unilateral, transfemoral or knee disarticulation amputations: a potential intervention for trip-related falls. Gait Posture. 2013;38(3):500–506. doi: 10.1016/j.gaitpost.2013.01.023 [DOI] [PubMed] [Google Scholar]
- 19.Wang Y, Wang S, Bolton R, Kaur T, Bhatt T. Effects of task-specific obstacle-induced trip-perturbation training: proactive and reactive adaptation to reduce fall-risk in community-dwelling older adults. Aging Clin Exp Res. 2020;32(5):893–905. doi: 10.1007/s40520-019-01268-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yang F, Bhatt T, Pai Y-C. Generalization of treadmill-slip training to prevent a fall following a sudden (novel) slip in over-ground walking. J Biomech. 2013;46(1):63–69. doi: 10.1016/j.jbiomech.2012.10.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Liu X, Bhatt T, Pai Y-C. Intensity and generalization of treadmill slip training: high or low, progressive increase or decrease? J Biomech. 2016;49(2):135–140. doi: 10.1016/j.jbiomech.2015.06.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lee A, Bhatt T, Pai Y-C. Generalization of treadmill perturbation to overground slip during gait: effect of different perturbation distances on slip recovery. J Biomech. 2016;49(2):149–154. doi: 10.1016/j.jbiomech.2015.11.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lee A, Bhatt T, Liu X, Wang Y, Pai Y-C. Can higher training practice dosage with treadmill slip-perturbation necessarily reduce risk of falls following overground slip? Gait Posture. 2018;61:387–392. doi: 10.1016/j.gaitpost.2018.01.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bhatt T, Pai Y-C. Prevention of slip-related backward balance loss: the effect of session intensity and frequency on long-term retention. Arch Phys Med Rehabil. 2009;90(1):34–42. doi: 10.1016/j.apmr.2008.06.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Krakauer JW, Shadmehr R. Consolidation of motor memory. Trends Neurosci. 2006;29(1):58–64. doi: 10.1016/j.tins.2005.10.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.König M, Epro G, Seeley J, Catalá-Lehnen P, Potthast W, Karamanidis K. Retention of improvement in gait stability over 14 weeks due to trip-perturbation training is dependent on perturbation dose. J Bomech. 2019;84:243–246. doi: 10.1016/j.jbiomech.2018.12.011 [DOI] [PubMed] [Google Scholar]
- 27.Brashers-Krug T, Shadmehr R, Bizzi E. Consolidation in human motor memory. Nature. 1996;382(6588):252–255. doi: 10.1038/382252a0 [DOI] [PubMed] [Google Scholar]
- 28.Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi: 10.1016/0022-3956(75)90026-6 [DOI] [PubMed] [Google Scholar]
- 29.Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi: 10.1111/j.1532-5415.1991.tb01616.x [DOI] [PubMed] [Google Scholar]
- 30.Yang F, Pai Y-C. Automatic recognition of falls in gait-slip training: harness load cell based criteria. J Biomech. 2011;44(12):2243–2249. doi: 10.1016/j.jbiomech.2011.05.039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bhatt T, Yang F, Pai YC. Learning to resist gait-slip falls: long-term retention in community-dwelling older adults. Arch Phys Med Rehabil. 2012;93(4):557–564. doi: 10.1016/j.apmr.2011.10.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Winter DA. Biomechanics and Motor Control of Human Movement. 4th ed. New Jersey, NJ: John Wiley & Sons; 2009. [Google Scholar]
- 33.Bhatt T, Wening J, Pai Y-C. Adaptive control of gait stability in reducing slip-related backward loss of balance. Exp Brain Res. 2006;170(1):61–73. doi: 10.1007/s00221-005-0189-5 [DOI] [PubMed] [Google Scholar]
- 34.Yang F, Bhatt T, Pai Y-C. Role of stability and limb support in recovery against a fall following a novel slip induced in different daily activities. J Biomech. 2009;42:1903–1908. doi: 10.1016/j.jbiomech.2009.05.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bhatt T, Wang E, Pai Y-C. Retention of adaptive control over varying intervals: prevention of slip-induced backward balance loss during gait. J Neurophysiol. 2006;95(5):2913–2922. doi: 10.1152/jn.01211.2005 [DOI] [PubMed] [Google Scholar]
- 36.Patel PJ, Bhatt T, DelDonno SR, Langenecker SA, Dusane S. Examining neural plasticity for slip-perturbation training: an fMRI study. Front Neurol. 2019;9:1181. doi: 10.3389/fneur.2018.01181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Liu X, Bhatt T, Wang S, Yang F, Pai Y-CC. Retention of the “first-trial effect” in gait-slip among community-living older adults. Geroscience. 2017;39(1):93–102. doi: 10.1007/s11357-017-9963-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Barajas J, Peterson D. First-trial protective step performance before and after short-term perturbation practice in people with Parkinson’s disease. J Neurol. 2018;265(5):1138–1144. doi: 10.1007/s00415-018-8821-z [DOI] [PubMed] [Google Scholar]
- 39.Goel R, Ozdemir RA, Nakagome S, Contreras-Vidal JL, Paloski WH, Parikh PJ. Effects of speed and direction of perturbation on electroencephalographic and balance responses. Exp Brain Res. 2018;236(7):2073–2083. doi: 10.1007/s00221-018-5284-5 [DOI] [PubMed] [Google Scholar]
- 40.Campbell AD, Squair JW, Chua R, Inglis JT, Carpenter MG. First trial and StartReact effects induced by balance perturbations to upright stance. J Neurophysiol. 2013;110(9):2236–2245. doi: 10.1152/jn.00766.2012 [DOI] [PubMed] [Google Scholar]