

Summary
Affordances offered by new media platforms are perceived as revolutionary instruments for removing the inequities of access to health promotion and communication. However, the production and dissemination of health promotional material on digital platforms does not necessarily translate into uniform access across diverse demographics. This article addresses the lacuna when it comes to analyzing Health Promotion initiatives in India, with a specific focus on the governmental publicity carried out on social media during the four phases of COVID-19 national lockdown between 24 March and 31 May 2020. Our intervention examines how governmental social media health promotion in India played a key role in shaping the ‘outbreak narrative’ during the lockdown across different levels of social and economic privilege. Through a combination of quantitative data analysis and qualitative interview methods, this article analyzes the circulation and impact of official publicity in online and offline spaces, during the COVID-19 lockdown in India. Resultant findings allow for a comprehensive assessment of whether such publicity contributed to democratized citizen science discourses: enabling social protection measures for vulnerable majorities or potentially reified the existing privileges of the economically and socially affluent minority. We find that health promotion campaigns during a pandemic must focus on reaching the widest possible audience in the most efficient manner. Specifically, in the Indian context, health promotion through mass-media like Television and Radio, and participatory media platforms needed to be implemented in tandem with new media platforms, to achieve required engagement with vulnerable communities on key health issues.
Keywords: community health promotion, media, governance, health education, ICT
Lay Summary
This article examines the impact of governmental publicity carried out on social media during the four phases of COVID-19 lockdown in India, between 24 March and 31 May 2020. Through a combination of quantitative data analysis and qualitative interview methods, both online and offline spaces are analyzed. The findings interrogate if such publicity contributed to democratic scientific knowledge and social protection measures or potentially reified the privileges of already affluent populations. The analysis reveals that a combination of mass and new media platforms in health promotion initiatives must be implemented to ensure maximum reach and participation from underprivileged communities.
INTRODUCTION
The global disruption of health, economic and social systems by the COVID-19 pandemic requires a reassessment of Health Promotion initiatives in underprivileged locations. Especially in postcolonial spaces like India—where inequitable distributions of power, wealth, and resources are quotidian phenomena—pandemics can reorder social relations (Das, 1995; Hoppe, 2003; Lynteris, 2014; Poleykett, 2018). This narrative was especially visible in colonial India during serious disease outbreaks, when dominant colonial subjectivities exploited vulnerable colonized subalterns under the guise of servicing scientific modernity (Arnold, 1993; Echenberg, 2002; Keck et al., 2019; Prince, 2019). The emergence of a truncated Indian state in 1947 saw a concerted effort to alleviate poverty and improve opportunities for all citizens through a welfare economy model that promoted universal education and health services. However, many such policies catalyzed through Nehruvian socialism failed to find effective on-ground success due to sub-par execution (Rao, 2018). Resultantly, even after seven decades of independence from colonial rule numerous issues remain in the healthcare sector including the lack of primary healthcare services, insufficient funding, lack of uniformity across federal and state jurisdictions in healthcare access and policy, and the severe scarcity of qualified health professionals in rural areas where much of India's population resides (Joumard and Kumar, 2015). Pertinently, the COVID-19 crisis has laid bare the vertiginous divides in health access, policy and promotion in India, which simultaneously enhance and impede literacy, motivation, and ability of different groups (and individuals) within the populace (Bodie and Dutta, 2008; Musahar, 2020).
In its first and only ranking of health systems in 2000, The World Health Organization (WHO) ranked India, 112 out of 191 countries. More recently in the 2015 Healthcare Access and Quality Index, India also ranked a lowly 154 out of 195 countries, which highlighted how ‘heightened healthcare access and quality is not an inevitable product of increased development’ (AFP, 2017). This is a crucial consideration particularly during the ongoing COVID Crisis since 70% of the Indian population do not have access to any form of institutionalized health insurance (Islam, 2020). Such disparities imply that health promotion initiatives in India during this unprecedented crisis must continually work to address the privileges separating offline and online sites and not further reify them. Since pandemics demand democratic health promotion, the affordances of new media platforms are often seen as revolutionary instruments: for removing the inequities of access (Viswanath and Finnegan, 1996). However, mere production and dissemination of health promotional material on digital platforms does not necessarily equate into uniform access across diverse demographics. What must be noted here is that our analysis does not flatten the problems of digital divide across the world. Instead, we emphasize that digital platforms are not established sites of health promotion in postcolonial spaces and unlike the Global North not an intrinsic part of the national sociotechnical imaginary (Jassanof and Kim, 2013). Especially since the digital divide is often compounded by linguistic barriers as well as the disparities of class, caste and gender identities in a country like India, health promotion must function on a different register as compared to the Global North.
By operationalizing Ruth Prince’s coinage ‘postcolonial pandemic publics’ in the Indian context—as populations that are realized through the ‘interplay of visibility and presentation, voice and audience’ [(Prince, 2019), p. 135]—this intervention examines governmental health promotion and communication on social media platforms during the four phases of COVID-19 lockdown (24 March to 31 May 2020). Our consequent analysis interrogates the nature of postcolonial pandemic publics that were self-reflexively produced through these communicative practices to understand how structural inequities reinforced themselves and contributed to healthcare disparities. We conclude by assessing the efficacy of social (new) media centric governmental pandemic publicity and offering concrete policy suggestions for participatory models of health promotion.
Governmental publicity on social media can play a key role in shaping the ‘outbreak narrative’ during a pandemic (Keck et al., 2019) across various levels of social and economic privilege. Following the adoption of social media initiatives and the interactivity offered by Web 2.0, which is in line with the long-term objectives of the Ottawa Charter (WHO, 1986), health promotion initiatives have begun to examine the potential of citizens’ engagement in knowledge production and inclusive health policy making by drawing from Citizen science [Den Broeder et al., 2018; by King et al. (King et al., 2016)]. However, one of the crucial issues for citizen engagement in health policy and promotion in the Indian context remains the lack of a sustained dialogue between Science and Technology (S&T) policy stakeholders (such as the various government ministries, scientific bodies and research scientists) and the common populace. A key reason for this failure is the percolation of the colonial imaginary for S&T into the postcolonial space: one that saw scientific (colonial) experts as privileged bodies thriving in exceptionalism and an active shunning of discussion with supposedly inexpert (colonized) subjects. In postcolonial India such an ideology translates into policy stakeholders perceiving themselves ‘as privileged holders of knowledge beyond the reach of popular movements, who therefore ought to accept the experts’ superior knowledge’ (Raghunandan and Jayaprakash, 2020). This privileged perception when perpetuated over time leads to the collapse of any possibility for a critical public sphere, as it systematically silences all those deemed unfit to be part of the discussion (Jansen, 1983). Such disparities in health communication and promotion amongst the health rich and the poor have been acknowledged by culture-centered approaches to health that focus on the dire need to reconfigure existing health promotion infrastructures (Marshall and McKeon, 1996; Viswanath and Finnegan, 1996; Dutta-Bergman, 2004a). Thus, this paradigm has not allowed even citizen science initiatives such as the People’s Science Movement Network in India, the Delhi Science Forum and various regional Non-Governmental Organizations to develop critical counterpublic discourses: and challenge the normative hegemony of governmental and institutionalized practices (Warner, 2002).
Our interrogation begins with Ministry of Health and Family Welfare’s (MoHFW) online health promotion initiatives during the COVID-19 lockdown. As the key organization handling the Government of India’s COVID-19 publicity, we surmise that the intention of MoHFW may also have been to catalyze citizen scientists (Den Broeder et al., 2018)—or ideal pandemic publics—who would play an active role as community participants in appropriate disease prevention behavior and also contribute to the broader goals of research and policy making. However, contrary to such intentions the major focus on online, specifically social media health promotion, was potentially counterintuitive, especially in a country like India where there are systemic disparities in health communication and promotion (NITI Aayog, 2017). Arising from the above premises this intervention asks if health promotion initiatives on social (new) platforms can contribute to democratized citizen science discourse and social protection measures for vulnerable communities in the Global South; or do they on the contrary reify the existing privileges of the economically and socially affluent minority populace in postcolonial spaces like India.
MATERIALS AND METHODS
Addressing the research question required a combination of quantitative data analysis and qualitative interview methods. Our methods of inquiry reflect previous research in the field of health promotion and education (Andrade et al., 2018; Dadich and Khan, 2020) that approach health promotion on social media using quantitative and qualitative tools. While our methods of inquiry could have solely focused on the analysis of data collected online from representative social media platforms, where the Indian MoHFW publicizes governmental COVID-19 documentation, the researchers in this study agreed that this approach would lead to little new insight: as the digital divide is an established fact in India (The Economic Times, 2020). Considering that only 294 million Indians out of a population of 1.32 billion people are active on social media (McKinsey Digital India Report, 2019) of which a disproportionate (98%) of users are in urban areas, we decided to implement a dual-pronged approach. Therefore, online data collection and quantitative computational analysis was complemented with offline phone interviews with respondents from marginalized populations, across both rural and urban locations, to understand the effects of primarily social-media centric health promotion, in a landscape which has considerable informational inequality.
Online data collection and quantitative analysis
For the online data collection stage, Twitter was chosen as the representative platform. The importance of Twitter within public health communication discourses has been established (Dadich and Khan, 2020) since it is a decentralized space that allows for the rapid creation of a public sphere through hashtag-based ad hoc publics (Ahmed et al., 2017; Bruns and Burgess, 2011; Holmes and Lussos, 2018; Merchant et al., 2011) Significantly, in the Indian context, Twitter lags substantially behind Facebook in the total number of registered users (Pragati, 2019). However, the official MoHFW on Facebook has only 4299 followers (see figures below) and in comparison, the official account of the MoHFW on twitter has 1.9 Million followers (as of July 2019) with a high followers ratio (Twitter Analytics by Foller.Me).
For this study, all tweets released on the official handle of the MoHFW (@MoHFW_INDIA) across all the four phases of the COVID-19 lockdown in India (24 March−31 May) were collected and analyzed. A total of 1389 tweets were released from the official MoHFW Twitter handle. Further, the top two hashtags related to the COVID-19 lockdown, during this period were identified using publicly available Twitter data (#indiafightscorona; #coronaupdatesinindia) and 10 000 tweets for each of these hashtags was extracted from Twitter. Consequently, text mining and data visualization of the twitter datasets were carried out by using two applications: Voyant Tools and Orange (Figures 1 and 2).
Fig. 1:

Official FB page of MoHFW with number of followers noted.
Fig. 2:

Source: Foller.me’s analysis of MoHFW’s Twitter followers.
Offline data collection and qualitative analysis
For the offline portion of our study, we decided upon purposive sampling to produce the sample of interview respondents for this study. (Battaglia, 2008). Fifteen respondents were interviewed from five different locations in India. Five from Kolkata (West Bengal), two from New Delhi (Delhi NCR) and two from Mumbai (Maharashtra) three of the major metropolitan cities in India; four were from Pilani, a small town in the state of Rajasthan and two from Indore (Madhya Pradesh) a Tier 2 city in India. The rationale for choosing these locations was to represent a sample showing a diversity of responses from marginalized collectivities across India. Coding of the qualitative data from the interviews was done following a three-cycle structure where the first (descriptive coding) cycle considered the structural characteristics of the data itself, the second (topic/thematic coding) cycle focused on contextual data to decipher its key meaning and relation to our research question (Saldanña, 2008; Maietta et al., 2018) and the third (analytic) coding cycle led to the emergence of core categories and discussion themes discussed below. All three researchers individually and manually coded for every cycle. The matrix that emerged allowed for the development of the codes into categories and discussion themes, following the Framework Method, that allows for an appropriate summarization of qualitative data in multi-disciplinary health research (Gale et al., 2013). Principles of inter-coder reliability were adhered to and researchers followed a comprehensive inductive approach to code and analyze the data. The varying agreement rates helped to locate the key problems in the coding schema and were used to develop a more nuanced coding schema, which helped in the emergence of comprehensive analytical themes (Sharma and Chaudhary, 2021) (Table 1).
Table 1:
Respondents’ profiles (n = 15)
| R1 | R2 | R3 | R4 | R5 | R6 | R7 | R8 | R9 | R10 | R11 | R12 | R13 | R14 | R15 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | Female | Female | Female | Female | Male | Female | Female | Female | Female | Female | Female | Female | Female | Female | Female |
| Age (approx imately) | 39 | 42 | 35 | 50 | 45 | 46 | 55 | 45 | 30 | 38 | 40 | 50 | 65 | 45 | 39 |
| Employ ment (Unorg/ Org Sector) | Housemaid (Unorgan ized) | Housemaid (Unorgani zed) | Housemaid (unorgani zed) | Housemaid (unorgani zed) | Security guard (unorga nized) | Housemaid (unorgani zed) | Housemaid (unorgani zed) | Housemaid (unorgani zed) | Housemaid (unorgani zed) | Housemaid (unorgan ized) | Housemaid (unorgani zed) | Housemaid (unorgani zed) | Housemaid (unorgani zed) | Housemaid (unorgan ized) | Housemaid (unorgani zed) |
| Monthly income in INR*a | 20 000 (268 USD) | 13 000 (174 USD) | 10 000 (134 USD) | 10/12 000 (134 − 161 USD) | 4/5000 (67 − 80 USD) | 13 000 (174 USD) | 10 000 (134 USD) | 16 000 (214 USD) | 16 000 (214 USD) | 14 000 (187 USD) | 20 000 (268 USD) | 18 000 (248 USD) | 10 000 (134 USD) | 20 000 (268 USD) | 19 000 (262 USD) |
| Location | Pilani, Rajas than | Pilani, Rajas than | Kolkata, WB | Kolkata, WB | Kolkata, WB | Indore, Madhya Pradesh | Kolkata, WB | Pilani, Rajas than | Indore, Madhya Pradesh | Kolkata, WB | Mumbai, Mahara shtra | Mumbai, Mahara shtra | Kolkata, WB | New Delhi | New Delhi |
Rough equivalent in US dollars provided on the basis of current currency exchange rates.
ANALYSIS AND DISCUSSION
Quantitative analysis
Total 1389 tweets collected from the official handle of the MoHFW (@MoHFW_INDIA) were visualized using content clouds, a common methodological tool in exploratory data analysis (Cidell, 2010). As the content cloud visualization indicates, there was a heavy recurrence of political personas in the tweets from the MoHFW, which include the names of the current Prime Minister of India (Mr Narendra Modi) Minister of Health and Family Welfare (Dr Harshvardhan) and Mr Ashwini Kumar Choubey (Minister of State for Health and Family Welfare). In their analysis of the health promotion campaigns Wakefield et al. surmise that social media messages affect behavior change among audiences by directly causing a cognitive or emotional response and indirectly by creating avenues of discussion amongst publics (Wakefield et al., 2010). Thus, health promotion campaigns that use new media platforms for information dissemination have the potential to create the necessary dialogue, which enables the creation of safe environments for vulnerable populations (Figures 3 and 4).
Fig. 3:
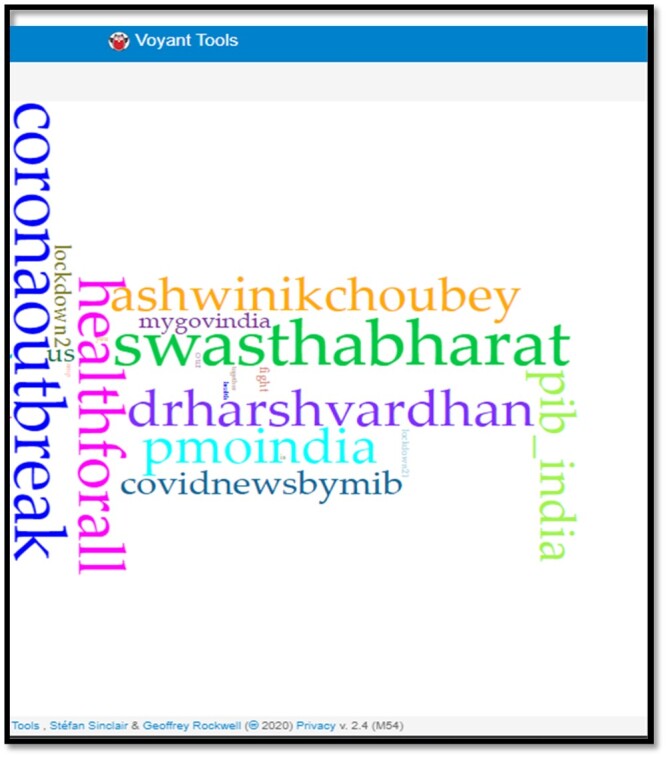
Content cloud generated from MoHFW tweets between 24 March and 31 May 2020.
Fig. 4:

Corpus summary of MoHFW tweets.
Contextually, new media platforms like Twitter can produce informed citizen scientists, through directed health-related information (Aharony, 2012; Enli and Simonsen, 2018). However, in uneven socio-economic landscapes the potential to orient uninformed individuals into discerning pandemic publics is often limited when tweets address and amplify privileged identities. For example, the corpus summary of the MoHFW’s tweets shows the dominant presence of the Indian PM as the third most frequently occurring word and evidences his importance in the discursive formation of MoHFW’s health promotion and communication, during the COVID-19 lockdown. This phenomenon can be expected since Prime Minister Modi has a significant social media following (with 60.4 million followers on Twitter) and any mention or tagging of his name offers impressive purchase in Twitterverse. But the reliance on the charismatic authority of a single actor amongst a greater population carries the risk of eliding the health protection measures, which should have been the primary intent of these communicative practices (von Klimó, 2004; Cocker and Cronin, 2017). In fact, contrary to expectations these tweets remain largely devoid of ‘better knowledge about the fundamental epidemiology of disease transmission (Den Broeder et al., 2018), the role of the local environment, and the interaction with the local healthcare infrastructure’ (Das, 2020), which would be vital in creating citizen science publics. Instead, the continued focus on particular personalities as noted in the visualization raises crucial questions regarding the role of such social media platforms during a pandemic, which scholars note can also be easily utilized for political propaganda (Uysal and Schroeder, 2019).
With exploratory insights from analyzing MoHFW’s tweets, the second logical step was to analyze how such messages create discourse communities on Twitter (Swales, 1990; Borg, 2003), defined as ‘as groups that have goals or purposes and use [written] communication to achieve this goal’ [(Borg, 2003), p. 398]. Central to the functioning of such discourse communities is the concept of genre or ‘patterns of written communication’ which allow for the operationalization of the goals for discourse communities. Twitter is a potent example of such a purposive genre of written communication, especially during moments of crisis, emergencies and disasters (Cameron et al., 2012; Ahmed et al., 2017). More specifically trending hashtags that are ‘platform convention for user-defined topics [are]…intended to identify a topic of communication’ [(Ahmed et al., 2017), p. 4] and allow for a centralized understanding of how different discourse communities approach issue-based communication goals on Twitter (Navar-Gill and Stanfill, 2018). Consequently, 10 000 tweets each were collected for each of the top two trending hashtags (#coronaupdatesindia; #indiafightscorona) and Topic modeling was used to analyze the tweets (Table 2; Figures 5 and 6).
Table 2:
Thematic distribution of topics emerging from the topic modeling of tweets using the top two hashtags during the COVID-19 lockdown in India
| Trending hashtag | Topics related to critical awareness of the pandemic | Topics related to socio-political environment |
|---|---|---|
| #coronaupdatesindia | Topics 1 − 3, 7 − 13, 17, 20 | Topics 4 − 6, 14 − 16, 18, 19 |
| #indiafightscorona | Topics 3 − 6, 8 − 16, 20 | Topics 1, 2, 7, 17 − 19 |
Fig. 5:

Topics found by analyzing 10 000 tweets with the hashtag #coronaupdatesinindia from Twitter during the COVID lockdown in India.
Fig. 6:

Topics found by analyzing 10 000 tweets with the hashtag #indiafightscorona from Twitter during the COVID lockdown in India.
Analysis of the tweets associated with the two hashtags shows two clear division of topics emerging, which are (i) Topics related to a Critical Awareness of the Pandemic and (ii) Topics related to India’s Socio-Political Environment during the COVID-19 lockdown. The results reflect conventional assumptions about Twitter being a public sphere that reflects the empowering role played by individuals with internet access in democratic societies (Jackson and Welles, 2015). Some of the common words and phrases in tweets using the hashtags #coronaupdatesinindia and ‘#indiafightscorona’, include ‘pandemic’, ‘masks’, ‘infections’, ‘doctors’, ‘test’, ‘stayhomestaysafe’, ‘quarantine’, ‘lockdown’, ‘recovery’ and ‘transmission’, which indicates the clear theme of both a factual and critical awareness of the COVID-19 crisis. These words indicate that Twitter users as a discourse community were able to reflect on the crisis and come together to ‘actively share goals and communicate with other members to pursue those goals’ [(Borg, 2003), p. 3]. These goals included both strategies like staying home during the lockdown, being under quarantine, testing of patients, as well as advanced inferences like those about the Aarogya Setu Mobile Application (a mobile app launched by the Indian government for contact tracing of COVID-19), and the possibilities of community transmission. Similarly, a clear theme also emerged from the topics that reflected Twitter users discussing their socio-political environment with the mention of political parties and figures, popular film stars as well as the ban on aviation, which has significantly affected white collar workers in the Indian economy.
What is significant is the lexical absence of words/phrases related to the migrant workers crisis as only a few topics mention the words ‘migrant’ or ‘rural’. Due to the ban on public transport during COVID-19 lockdown millions of migrant workers were forced to walk thousands of miles from their sites of employment in urban spaces to reach their homes in rural India. This led to many deaths and has since been a dominant global topic of discussion in mainstream media and academic discussions (Infante, 2020; Slater and Masih, 2020). The relative apathy shown to the migrant worker crisis on Twitter challenges the notion that social media can give rise to counterpublic discourses and resist hegemonic and privileged cultural conversations (Brock, 2012). Instead by highlighting the privileges and ad hoc nature of hashtag-based publics (Bruns and Burgess, 2011) the analysis indicates how digital inequality in the Global South genuinely affects inclusive social media discussions, which can create much needed public trust during a pandemic and promote conversations on health-related issues for marginalized populations (Park et al., 2016; Siegrist and Zingg, 2014).
QUALITATIVE ANALYSIS AND DISCUSSION THEMES
Factual knowledge of the pandemic
Pandemics interpellate different forms of publics through mediated encounters depending on their social and economic locations. Ideally, informed pandemic publics should democratically emerge through both dialogue and debate in both offline and online public spheres. However, in recent years it has been seen that dominant discursive publics, especially in the health promotion context, are brought into being by being addressed on/through social media (Marsland, 2013; Prince, 2019). Although most respondents in the qualitative dataset had a satisfactory understanding of the symptoms of the pandemic (as highlighted in the attached table) there was a complete lack of clarity when it came to a critical awareness about the nature of the COVID-19 virus as well as the reasons behind its rapid spread. For example, one of the respondents’ noted ‘When you stay in the dirt, it spreads’ while another stated that ‘I have heard more people are dying now. One who is going to the hospital is never returning (sic)’. These comments reflect some of the on-ground realities facing vulnerable communities in India during the COVID crisis (Limaye et al., 2020) but also an increasing paranoia amongst vulnerable populations about the disease being an immediate signified for certain death. Such fear amongst a vast majority of the Indian population from lower socio-economic backgrounds is justified considering the genuine difficulty with social distancing measures and personal hygiene, given their residence in congested locations with irregular access to clean running water (Mathur, 2020) (Table 3).
Table 3:
Discussion themes and quotes from respondents (translated into English from regional language)
| Discussion themes | Respondents’ quotes |
|---|---|
| Factual awareness of COVID-19/Coronavirus (knowledge of the pandemic) | Quotes from respondents
|
| Information conduit/channel utilized for COVID-19 awareness |
|
| Socio-economic distress (community and individual) |
|
The challenges for such vulnerable populations were also compounded by the lack of directed public health information that which should have considered the in situ obstacles for underprivileged communities (Guilmoto and Thomas, 2020). On the other end of this paranoia, were respondents who denied the serious nature of the pandemic by stating ‘Nobody in my locality has got it. I have not seen it happen. Therefore, I cannot understand’. Often a denial of the disease is a coping mechanism for marginalized communities who have neither the economic or social capital to deal with pandemic’s fallout, which reflect similar strategies used by vulnerable populations in West Africa during the 2014 Ebola crisis (Keck et al., 2019). Some of the responses also foreground that while vital health promotion messages were largely limited to new media platforms, the virality of the ongoing India−China military crisis on mass media, and India’s aggressive response had ignited strong xenophobic sentiments. As one respondent noted ‘I know that it has come from China (chin se aya hai)’ while another asserted that ‘There is a war. With China. Corona they only started’. Overall, we infer that while the discourse communities emerging on Twitter were mostly able to critically reflect upon factual information to draw crucial health-based social insights, the qualitative dataset reflects a xenophobia based in hearsay. A clear understanding of the pandemic, its imminent harm as well as contextual preventive measures is understandably overshadowed by the fear of death, loss of employment, scarcity of food than a critical understanding of the pandemic.
Information conduit/channel
While the Indian government’s MoHFW twitter handle tweeted 1389 times during the time period analyzed (24 March−31 May 2020), this social media information was uniformly inaccessible to all the participants in the qualitative sample. More importantly a majority of the respondents were also unaware of the existence of such a platform (Twitter). While social media’s inherent characteristics of instantaneity and high levels of interactivity can create awareness and initiate meaningful conversations, India’s digital divide complicated at multiple levels—by gender, class, caste, levels of education, technical knowhow—created barriers to accessing social media centric health information, which is brought to the fore by the qualitative data (Selwyn, 2004). Most respondents received their information about the outbreak, its spread and the declaration of the pandemic from four primary sources. Through mass-media platforms, primarily the Television; through messages on messaging platforms like SMS or Whatsapp; through a recorded message on their mobile phones before they attempted to make call; or through the word of mouth from people they viewed as ‘opinion leaders’ (Katz, 1957) in their everyday lives.
Responses about sources of information, ranged from the simplistic ‘It is told every day, on news’; or ‘TV, I can see it on the television on the news’ to more complex ones like; ‘There are many messages, stay safe from coronavirus. It is dangerous, there are no medicine for it’. SMS or Text Messages on mobiles, as communicative media also have their limitations to accessibility as they require the recipient to be able to read and decode the said message. A domestic laborer in Mumbai said, ‘We got information from news about fever, cold, pain in foot and hands and other symptoms of COVID. Otherwise, how would we know?’ This quote reiterates that the only credible and accessible source of information about the virus for this population were TV news channels. While a health promotion initiative that delivers the message to everyone who dials a number or makes a call seems far-reaching, the compromises of the approach become evident when the delivery of the messages is examined. Limited time to deliver the message combined with the overwhelming need to disburse as much information as possible implies a possibility where the intended message never registers, nor is comprehended by the receiver. As is evident from the lamentations of a respondent ‘No I don’t quite know. Cause I can't see SMS by myself…It only states … ‘stay safe from coronavirus’.—I don’t understand mostly…it is too fast’. Thus, the inability of the government’s machinery to reach large segments of its population becomes increasingly apparent in this analysis forcing people to look elsewhere for their information. Most participants found the news broadcast on their televisions to be the only way to receive crucial information. One respondent was explicit by stating ‘We got to know everything from news only, that’s all we know’. Similarly, the word of mouth or the role of the opinion leader as a source of information (Katz, 1957); a paradigm that has been heavily critiqued (Gitlin, 1978) in communication studies is seen to re-emerge: since there is a paucity/inability to access factual information. This consequently leads to the creation of new binaries between people who have the requisite information and those who don’t. Respondents in the study acknowledge this development when they observe: ‘I work (as a domestic help) in the houses, the madams tell me. The madams tell about the spread of coronavirus and about taking precautions’. However, such interactions are not devoid of class and caste dynamics as perceived opinion leaders can frame and disseminate information to meet their specific agendas (a possibility that exists with news media as well). Fundamental to the creation of a citizens’ science publics is the creation of repositories and sources of information that are democratic and easily available to the population. The health promotion strategy used by the Indian MoFHW was found wanting in overcoming the various barriers that inhibit the flow of essential/critical information during a pandemic. It also caused underprivileged publics to look elsewhere, to less-trusted sources, as is apparent in the analysis. Free, accurate, unbiased and easy to understand information that is a prerequisite for allowing the maximum number of people to make conscious, fundamental decisions during a health crisis was denied by the deployment of a social-media centric health promotion campaign.
Socio-economic distress (community and individual)
‘So many people kid, elderly people are walking (on feet) for hours on the road, in the hot sun, without food, without water’ said a 45-year-old domestic worker in Pilani, Rajasthan. The respondent here narrated the hard-hitting reality of the Indian lockdown during the COVID-19 pandemic in India. Thousands of migrant workers were stranded without food, housing and employment in their places of work as factories, shops and construction sites shut down mid-March due to the nationwide lockdown. Supporting our data, a 27-year-old worker from Bihar stuck in Mumbai noted on ruralindia.org, ‘Not a rupee has come from anywhere. What are we to eat? How are we to live?’ Some of the other stories addressed the tale of migrant workers who had to travel by foot without any smart phone or GPS support. As migrant workers and their families started their journey home by foot to cover an unattainable distance of 200 km, the rising concern along with the rehabilitation of the workers was to abate the spread of the virus. Although the government of India facilitated the migration by initiating the Shramik (worker) special trains, the mass exodus completely defied the norms of social distancing and other parameters needed to prevent community transmission of the virus (Vaz, 2020) For the vast majority of Indian population social distancing was a new normal that did not synchronize with their quotidian economic and social location. The qualitative data shows that workers from the unorganized sectors and the lower socio-economic strata living in congested settings often shared common living spaces and bathrooms. A significant part of the health promotion by the Indian government promoted ideals of social distancing, constant personal hygiene including sanitizing/washing hands and wearing masks. Unfortunately, many of these preventive measures while available to the new media publics could not translate to lower socio-economic populations. As a female domestic worker pointed out in her interview, ‘We have to physically go to the ration shop and collect the samaan (groceries), it is crowded, but what to do! The government never came to our doorstep to deliver food. We got no help from them’ (the government). Thakur et al. (Thakur et al., 2016) claim that health promotion should ideally focus on achieving equitable health and therefore the major role of the government during a health crisis like the pandemic is to amplify health communication in a way that ‘enables people to increase control over and improve their health’. However, during the interviews it was discovered that social media centric health promotion did not effectively reach the lowest strata of Indian society. On the contrary they experienced massive economic and social affliction as evidenced by long waiting periods in crowded Public Distribution System Channels (ration shops) as pointed above, which amplified the chances of contracting the virus. Although they were aware of the merits of social distancing, the dilemma facing vulnerable populations lay in daily food and sustenance for which they had to be mobile, even at the cause of contracting the virus (Rukmini, 2020). Health promotion initiatives in these pandemic situations should ideally collaborate with human welfare practices, which were also found wanting. For example, a respondent noted, ‘We did not get any money on the bank account only the people with Jan-Dhan account got 500 rupees (INR) in their account’. However, other respondents mentioned that it was pointless to have a bank account because they had no tangible savings and whatever they earned was spent to support the essentials of the entire family. Importantly, not all the respondents were aware of the Pradhan Mantri Jan-Dhan Yojana (2014): a scheme under Government of India that is meant to promote financial inclusion. It may be inferred that if crucial information for the economic sustenance of underprivileged populations (e.g. the Jan-Dhan scheme) failed to reach the intended populations in pre-pandemic times, the possibility of social media centric health promotion initiatives of reaching them during a pandemic would be particularly bleak.
CONCLUSION
Emerging scholarship on the COVID-19 crisis has seen several approaches trying to understand best practices for crucial health information dissemination. An approach particularly relevant to our intervention is the culture centered approach (CCA) (Dutta et al., 2020a) which operationalizes communities at the ‘margins of margins’ as sites where challenges to health and well-being can be identified and new solutions developed (Dutta et al., 2020b). CCA’s conceptualization is deeply rooted in a participatory communication framework that is willing to ‘learn from the below’ [(Dutta et al., 2020a), p. 2] and resonates with our analysis that subaltern communities cannot find effective empowerment through a primarily social (new) media centric health promotion paradigm. Instead, the voices of marginalized collectivities must be amplified through community owned media networks, which would allow them to be informed, engaged and active participants in the transition to a new normal (Habersaat et al., 2020). Our findings and analysis offer a unique intervention into official governmental COVID-19 publicity and contributes to emergent scholarship, which indicates how India’s health information dissemination approach eschewed the establishment of participatory spaces: for both shaping COVID-19 aware communities and sites where community and culturally based solutions could be developed.
In the context of the global north and the first world where access to the internet is part of the national socio technical imaginary and an everyday phenomenon (Jassanof and Kim, 2009; Boyd, 2012) the potential of intersections between health promotion and the formulation of citizen science publics are many. In the global south however, where the digital divide is compounded with social stratification, online-focused health promotion campaigns create a substantial difference in impact amongst a populace having stark contrasts in intersectional privileges. The challenges for health promotion activities in a country like India are several as they can face a lack of availability, lack of interest, constraints of time and a disinterest that is rooted in the societal construction of gender (Dutta-Bergman, 2004b; Gaiha and Gådin, 2020). The need for a health promotion campaign that focuses on the dissemination of awareness information in times of pandemics is to reach the widest possible audience and in the most efficient manner. Therefore, the adoption of an internet-centric, social media focused health promotion campaign (as in the case of the COVID-19 pandemic in India) does not take into account the country’s various ICT4D initiatives and participatory development approaches, which taps into the reach of conventional mass-media and alternative media platforms.
In the Indian context, the rise of the people’s science movement (Jaffry et al., 1983; Kannan, 1990) especially after specific incidents like the Bhopal gas tragedy (Raghunandan and Jayaprakash, 2020) has served as the first of several precedents where the use of mass-media channels like Television and Radio, participatory media platforms like community radio (Pavarala & Malik, 2007; Malik & Pavarala, 2020) and IVRS platforms (Marathe et al., 2015; Moitra et al., 2018) have been successful in achieving both the dissemination of messages and fostering required engagement with their communities on key issues. However, despite numerous such instances where mass-media and alternate media channels have helped disseminate crucial information successfully, governments and designers of health promotion initiatives have failed to tap into the benefits of either the mass media or grassroot level networks. In the case of COVID-19, the approach chosen by the MoFHW when examined critically, as done by this study; raises pertinent questions as to why a tried and tested approach was eschewed in favor of a primarily online, social-media centric campaign.
The existence but non-utilization of existent infrastructure including a free to air public broadcasting system (for both TV and radio) which could have served as focal points of the health promotion initiative remains questionable. Further, the democratic nature of community and alternative media platforms (Pavarala and Malik, 2007) would have provided the necessary framework to synchronize with the benefits of an established citizens science publics. Lastly, the creation, implementation and use of the Arogya Setu app to inform the publics of the pandemic’s spread in their vicinity and its positioning as a tool for participatory disease surveillance (Garg et al., 2020) further magnifies the differential impact that this study highlights: where marginalized publics on the wrong side of the digital divide are deprived of fundamental health information in the times of a once in a generation pandemic.
ETHICAL APPROVAL
Interviews with respondents in this study were done telephonically because of the COVID-19 crisis. The respondents were informed of the purpose of the interviews and that their participation in the project was voluntary. Further, it was delineated that if the respondents’ consented to provide interviews their responses would be recorded and that they had full autonomy to ask the researchers to stop recording or withdraw consent if they so desired. Respondents were assured that their responses and identities would remain confidential unless they preferred otherwise.
ACKNOWLEDGMENT
The authors would like to acknowledge Ms. Sayantani Saraswati for her help during the data collection and transcription of interviews.
FUNDING
No external or internal institutional funding was received by the authors for this project.
REFERENCES
- Arnold D. (1993) Colonizing the Body: State Medicine and Epidemic Disease in Nineteenth Century India. Univ of California Press. [Google Scholar]
- Aharony N. (2012) Twitter use by three political leaders: an exploratory analysis. Online Information Review, 36, 587–603. [Google Scholar]
- AFP. (2017) India Ranks 154 in Global Healthcare Rankings for 2015, Switzerland Tops List. Livemint, 19 May 2017, www.livemint.com/Politics/b9c6cJFhzDHfubCfXEEIoJ/India-ranks-154-in-global-healthcare-rankings-for-2015-Swit.html (last accessed 04 June 2021).
- Bodie G. D., Dutta M. J. (2008) Understanding health literacy for strategic health marketing: eHealth literacy, health disparities, and the digital divide. Health Marketing Quarterly, 25(1-2), 175–203. [DOI] [PubMed] [Google Scholar]
- Economic Times Blogs. (2020) Let Lockdown Not Grow Digital Divide. The Economic Times, 9 April 2020. https://economictimes.indiatimes.com/blogs/et-editorials/let-lockdown-not-grow-digital-divide/ (last accessed 04 June 2021).
- Ahmed W., Bath P. A., Demartini G. (2017) Using twitter as a data source: an overview of ethical, legal, and methodological challenges. In Woodfield K. (ed.) The Ethics of Online Research. Advances in Research Ethics and Integrity (2). Emerald, pp. 79−–107.. [Google Scholar]
- Andrade E. L., Evans W. D., Barrett N., Edberg M. C., Cleary S. D. (2018) Strategies to increase Latino immigrant youth engagement in health promotion using social media: mixed-methods study. JMIR Public Health and Surveillance, 4, e71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Battaglia M. P. et al. (2008) A comparison of address-based sampling (ABS) versus random-digit dialing (RDD) for general population surveys. Public Opinion Quarterly, 72, 6–27. [Google Scholar]
- Borg E. (2003) Discourse community. ELT Journal, 57, 398–400. [Google Scholar]
- Boyd D. (2012) Participating in the always-on lifestyle. The Social Media Reader, 71–76. [Google Scholar]
- Brock A. (2012) From the blackhand side: twitter as a cultural conversation. Journal of Broadcasting & Electronic Media, 56, 529–549. [Google Scholar]
- Bruns A., Burgess J. E. (2011, August) The use of Twitter hashtags in the formation of ad hoc publics. In Proceedings of the 6th European Consortium for Political Research (ECPR) General Conference 2011.
- Cameron M. A., Power R., Robinson B., Yin J. (2012, April) Emergency situation awareness from twitter for crisis management. In Proceedings of the 21st International Conference on World Wide Web, pp. 695 − 698.
- Cidell J. (2010) Content clouds as exploratory qualitative data analysis. Area, 42, 514–523. [Google Scholar]
- Cocker H. L., Cronin J. (2017) Charismatic authority and the YouTuber: unpacking the new cults of personality. Marketing Theory, 17, 455–472. [Google Scholar]
- Dadich A., Khan A. (2020) Using Twitter to promote a youth mental health agenda. Health Promotion International, 36, 235–249. [DOI] [PubMed] [Google Scholar]
- Das V. (1995) Critical Events: An Anthropological Perspective on Contemporary India, Vol. 7. Oxford University Press, Oxford, New York. [Google Scholar]
- Das V. (2020) Corona Policy Must Factor in Scientific Uncertainty. Deccan Chronicle [online], May 24. https://www.deccanchronicle.com/opinion/columnists/240520/veena-das-corona-policy-must-factor-in-scientific-uncertainty.html (last accessed 04 June 2021).
- Den Broeder L., Devilee J., Van Oers H., Schuit A. J., Wagemakers A. (2018) Citizen science for public health. Health Promotion International, 33, 505–514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dutta‐Bergman M. J. (2004a) The unheard voices of Santalis: communicating about health from the margins of India. Communication Theory, 14, 237–263. [Google Scholar]
- Dutta-Bergman M. J. (2004b) Health attitudes, health cognitions, and health behaviors among Internet health information seekers: population-based survey. Journal of Medical Internet Research, 6, e15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dutta M. J., Moana-Johnson G., Elers C. (2020a) COVID 19 and the pedagogy of culture-centered community radical democracy: a response from Aotearoa New Zealand. Journal of Communication Pedagogy, 3, 11–19. [Google Scholar]
- Dutta M., Agarwal D., Sivakami M. (2020b) The “invisible” among the marginalised: do gender and intersectionality matter in the Covid-19 response? Indian Journal of Medical Ethics, 05, 302–308. [DOI] [PubMed] [Google Scholar]
- Echenberg M. (2002) Pestis redux: The initial years of the third bubonic plague pandemic, 1894–1901. Journal of World History, 429–449. [DOI] [PubMed] [Google Scholar]
- Enli G., Simonsen C. A. (2018) ‘Social media logic’ meets professional norms: twitter hashtags usage by journalists and politicians. Information, Communication & Society, 21, 1081–1096. [Google Scholar]
- Gale N. K., Heath G., Cameron E., Rashid S., Redwood S. (2013) Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Medical Research Methodology, 13, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gaiha S. M., Gådin K. G. (2020) ‘No time for health:’ exploring couples’ health promotion in Indian slums. Health Promotion International, 35, 70–81. [DOI] [PubMed] [Google Scholar]
- Garg S., Bhatnagar N., Gangadharan N. (2020) A case for participatory disease surveillance of the COVID-19 pandemic in India. JMIR Public Health and Surveillance, 6, e18795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gitlin T. (1978) Media sociology. Theory and Society, 6, 205–253. [Google Scholar]
- Guilmoto C. Z., Thomas L. (2020) India and Coronavirus: Lack of Access to Handwashing Facilities among Poor Makes Fight Even Harder. The Conversation, 1 April 2020. https://theconversation.com/india-and-coronavirus-lack-of-access-to-handwashing-facilities-among-poor-makes-fight-even-harder-135087 (last accessed 04 June 2021).
- Habersaat K. B., Betsch C., Danchin M., Sunstein C. R., Böhm R., Falk A.. et al. (2020) Ten consider-ations for effectively managing the COVID-19 transition. Nature Human Behaviour, 4, 677–687. [DOI] [PubMed] [Google Scholar]
- Holmes S., Lussos R. G. (2018) Cultivating metanoia in twitter publics: analyzing and producing bots of protest in the #GamerGate controversy. Computers and Composition, 48, 118–138. [Google Scholar]
- Hoppe K. A. (2003) Lords of the Fly: Sleeping Sickness Control in British East Africa, 1900–1960. Greenwood Publishing Group, Santa Barbara. [Google Scholar]
- Infante S. (2020) India's Coronavirus Migration Crisis | JSTOR Daily, 17 June. https://daily.jstor.org/indias-migration-crisis/ (last accessed 26 March 2021).
- Islam/am (2020) Healthcare: India and US can learn from each other (Comment), Outlook THE NEWS SCROLL, 7 March. https://www.outlookindia.com/newsscroll/healthcare-india-and-us-can-learn-from-each-other-comment/175 4707 (last accessed 04 June 2021).
- Jaffry A., Rangarajan M., Ekbal B., Kannan K. P. (1983) Towards a people’s science movement. Economic and Political Weekly, 372–376. [Google Scholar]
- Jackson S. J., Welles B. F. (2015) Hijacking #myNYPD: social Media Dissent and Networked Counterpublics. Journal of Communication, 65, 932–952. [Google Scholar]
- Jansen S. C. (1983) Power and knowledge: toward a new critical synthesis. Journal of Communication, 33, 342–354. [Google Scholar]
- Jasanoff S., Kim S. H. (2013) Sociotechnical imaginaries and national energy policies. Science as Culture, 22, 189–196. [Google Scholar]
- Joumard I., Kumar A. (2015) Improving Health Outcomes and Health Care in India. OECD, Economics Department Working Papers, N. 1184, OECD Publishing, France
- Kannan K. P. (1990) Secularism and people's science movement in India. Economic and Political Weekly, 311–313. [Google Scholar]
- Katz E. (1957) The two-step flow of communication: an up-to-date report on an hypothesis. Public Opinion Quarterly, 21, 61–78. [Google Scholar]
- Keck F., Kelly A. H., Lynteris C. (2019) Introduction: the anthropology of epidemics. In Kelly, A.H., Keck, F., & Lynteris, C. (Eds.) The Anthropology of Epidemics, Routledge, London, p. 1−–24.. [Google Scholar]
- King A. C., Winter S. J., Sheats J. L., Rosas L. G., Buman M. P., Salvo D.. et al. (2016) Leveraging citizen science and information technology for population physical activity promotion. Translational Journal of the American College of Sports Medicine, 1, 30–44. [PMC free article] [PubMed] [Google Scholar]
- Lynteris C. (2014) Epidemics as events and as crises: comparing two plague outbreaks in Manchuria (1910–11 and 1920–21). The Cambridge Journal of Anthropology, 32(1), 62–76. [Google Scholar]
- Limaye Y., Yadav S., Thapar A. (2020) Overwhelmed India Hospitals Turn Covid Patients Away. BBC News, 12 June 2020. www.bbc.com/news/av/world-asia-india-53014213/coronavirus-overwhelmed-india-hospitals-turn-covid-patients-away (last accessed 04 June 2021).
- Malik K. K., Pavarala V. (eds). (2020) Community Radio in South Asia: Reclaiming the Airwaves, Routledge, London. [Google Scholar]
- Maietta R., Hamilton A., Swartout K., Petruzzelli J. (2018) ResearchTalk’s Qualitative Data Analysis Camp. Carrboro, NC. http://www.researchtalk.com/qualitative-data-analysis-camp-april-2018 (last accessed 04 June 2021). [Google Scholar]
- Marathe M., O'Neill J., Pain P., Thies W. (2015, May) Revisiting CGNet Swara and its impact in rural India. In Proceedings of the Seventh International Conference on Information and Communication Technologies and Development, pp. 1−–10..
- Marshall A. A., McKeon J. K. (1996) Reaching the “unreachables”: educating and motivating women living in poverty. In Ray E. B. (Ed.) Communication and Disenfranchisement: Social Health Issues and Implications, 137–155. [Google Scholar]
- Marsland R. (2013) ‘Who are the public in public health: debating crowds, populations and publics in Tanzania’. In P Ruth, M Rebecca. (eds), Making and Unmaking Public Health in Africa: Ethnographic and Historical Perspectives, pp. 75–95. Ohio University Press. [Google Scholar]
- Mathur B. (2020) Fighting COVID-19 With Hand Hygiene: Lack Of Water And Handwashing Infrastructure Pose Challenge For The Poor | News. NDTV-Dettol Banega Swasth Swachh India, 6 May 2020. https://swachhindia.ndtv.com/fighting-covid-19-with-hand-hygiene-lack-of-water-and-handwashing-infrastructure-pose-challenge-for-the-poor-44371/ (last accessed 04 June 2021).
- McKinsey Digital. (2019) Digital India: Technology to Transform a Connected Nation. McKinsey & Company, 2019. www.mckinsey.com/business-functions/mckinsey-digital/our-insights/digital-india-technology-to-transform-a-connected-nation (last accessed 04 June 2021).
- Merchant R. M., Elmer S., Lurie N. (2011) Integrating social media into emergency-preparedness efforts. New England Journal of Medicine, 365, 289–291. [DOI] [PubMed] [Google Scholar]
- Moitra A., Kumar A., Seth A. (2018) An analysis of community mobilization strategies of a voice-based community media platform in rural India. Information Technologies & International Development, 14, 18. [Google Scholar]
- Musahar N. R. (2020) India's starvation measures. New Left Review, 29–34. [Google Scholar]
- Navar-Gill A., Stanfill M. (2018) “We shouldn't have to trend to make you listen”: Queer Fan Hashtag Campaigns as Production Interventions. Journal of Film and Video, 70, 85–100. [Google Scholar]
- NITI Aayog. (2017) NITI Aayog Annual Report 2017-18. http://niti.gov.in/sites/default/files/2019-04/Annual-Report-English.pdf (last accessed 04 June 2021).
- Park H., Reber B. H., Chon M. G. (2016) Tweeting as health communication: health organizations’ use of Twitter for health promotion and public engagement. Journal of Health Communication, 21, 188–198. [DOI] [PubMed] [Google Scholar]
- Pavarala V., Malik K. K. (2007) Other Voices: The Struggle for Community Radio in India. New Delhi, India, SAGE Publications India. [Google Scholar]
- Poleykett B. (2018) Ethnohistory and the dead: cultures of colonial epidemiology. Medical Anthropology, 37, 472–485. [DOI] [PubMed] [Google Scholar]
- Pragati. (2019) Social Media Statistics in India - Talkwalker, 7 October 2019. https://www.talkwalker.com/blog/social-media-statistics-in-india (last accessed 04 June 2021).
- Prince R. et al. (2019) Pandemic publics How epidemics transform social and political collectives of public health. In Kelly A. H. (ed.), The Anthropology of Epidemics. London, Routledge, pp. 135–153. [Google Scholar]
- Rao S. L. (2018) A new paradigm. The Hindu BusinessLine, 9 March 2018. https://www.thehindubusinessline.com/opinion/a-new-paradigm/article21948342.ece1 (last accessed 04 June 2021).
- Rukmini S. (2020) Why India's ‘Migrants’ Walked Back Home. Livemint, 28 May. https://www.livemint.com/news/india/why-india-migrants-walked-back-home-11590564390171.html (last accessed 04 June 2021).
- Saldaña J. (2008) An Introduction to Codes and Coding. Sage, Thousand Oaks, CA. [Google Scholar]
- Sharma R., Chaudhary M. (2021) Perceptions of outdoor gymnasiums in National Capital Region, India: creating active environments for health promotion. Health Promotion International, 36, 89–100. [DOI] [PubMed] [Google Scholar]
- Selwyn N. (2004) Reconsidering political and popular understandings of the digital divide. New Media & Society, 6, 341–362. [Google Scholar]
- Siegrist M., Zingg A. (2014) The role of public trust during pandemics: implications for crisis communication. European Psychologist, 19, 23–32. [Google Scholar]
- Slater J., Masih N. (2020) India Coronavirus: Migrant Workers Stranded by Lockdown Walk Hundreds of Miles Home, 27 March. https://www.washingtonpost.com/world/asia_pacific/india-coronavirus-lockdown-migrant-workers/2020/03/27/a62df166-6f7d-11ea-a156-0048b62cdb51_story.html (last accessed 04 June 2021).
- Swales J. (1990) Genre Analysis: English in Academic and Research Settings. Cambridge University Press, Cambridge, UK. [Google Scholar]
- Raghunandan D., Jayaprakash N. D. (2020) Bhopal gas disaster: Delhi science forum and people’s science movement in india-in memory of Dr. Amit Sengupta. Saúde em Debate, 44, 120–134. [Google Scholar]
- Thakur J. S., Jaswal N., Grover A., Kaur R., Jeet G., Bharti B.. et al. (2016) Effectiveness of district health promotion model (Hoshiarpur Ambala model): An implementation experience from two districts from Northern part of India. International Journal of Noncommunicable Diseases, 1, 122–130. [Google Scholar]
- Twitter Analytics by Foller.Me. Foller.Me-Twitter Analytics Application, foller.me/mohfw_india. (last accessed 04 June 2021).
- Uysal N., Schroeder J. (2019) Turkey’s Twitter public diplomacy: towards a “new” cult of personality. Public Relations Review, 45, 101837. [Google Scholar]
- Vaz M. (2020) Documentary: Refugees at Home – Inside India's Migrant Crisis, May 31. https://www.thequint.com/videos/documentaries/documentary-on-india-migrant-crisis-covid-19-coronavirus-lockdown (last accessed 04 June 2021).
- Viswanath K., Finnegan J. R. Jr (1996) The knowledge gap hypothesis: twenty-five years later. Annals of the International Communication Association, 19, 187–228. [Google Scholar]
- von Klimó Á. (2004) ‘A very modest man’: Béla Illés, or how to make a career through the leader cult’. In Apor B., Behrends J. C., Jones P., Rees E. A. (eds), The Leader Cult in Communist Dictatorships. Palgrave Macmillan, New York, pp. 47–62. [Google Scholar]
- Wakefield M. A., Loken B., Hornik R. C. (2010) Use of mass media campaigns to change health behaviour. The Lancet, 376, 1261–1271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warner M. (2002) Publics and counterpublics. Public Culture, 14, 49–90. [Google Scholar]
- World Health Organization (WHO). (1986) The Ottawa Charter for Health Promotion. http://www.who.int/healthpromotion/conferences/previous/ottawa/en/ (last accessed 04 June 2021).
- World Health Organization (WHO). (2016) Shanghai Declaration on Promoting Health in the 2030 Agenda for Sustainable Development. 21 November 2016, www.who.int/healthpromotion/conferences/9gchp/shanghai-declaration/en/ (last accessed 04 June 2021). [DOI] [PubMed]