

Abstract
Background
The interventional cardiac magnetic resonance imaging suite combines a cardiac catheterization x-ray laboratory with a magnetic resonance imaging suite. At the study institution, interventional cardiac magnetic resonance imaging procedures (ie, magnetic resonance imaging–guided cardiac catheterizations) have been performed under institutional review board–approved research protocols since 2015. Because the workplace incorporates x-ray and magnetic resonance imaging in a highly technical environment, education about the importance of magnet safety is crucial to ensure the safety of patients and staff.
Objective
To promote magnetic resonance imaging safety and staff preparedness to respond in emergency situations in a specialized interventional cardiac magnetic resonance imaging environment.
Methods
Quarterly in situ evacuation drills with a live volunteer were implemented. A retrospective participant survey using a Likert scale was conducted. Evacuations were timed from the cardiac arrest code alert to safe evacuation or defibrillation if appropriate.
Results
Over 4 years, 14 drills were performed. Twenty-nine of 48 participants responded to the survey, a 60% response rate. Most participants agreed or strongly agreed that the drills were a positive experience (90%) and that the drills increased their confidence in their ability to perform in an evacuation scenario (100%). Room evacuation times improved from 71 to 41 seconds. No patient or staff safety events occurred in the interventional cardiac magnetic resonance imaging environment.
Conclusion
Magnetic resonance imaging–guided cardiac catheterization evacuation drills promote preparedness, ensure patient and staff safety, and improve evacuation time in the interventional cardiac magnetic resonance imaging environment.
Pediatric patients with complex congenital and acquired heart disease often require multiple cardiac catheterizations with x-ray, accruing significant radiation exposure throughout their lifespan.1 Magnetic resonance imaging (MRI) provides an alternative to conventional x-ray–guided catheterization by eliminating patient and staff exposure to ionizing radiation while also providing improved soft-tissue and structural imaging in multiple planes.2 Additionally, MRI provides volumetric analysis of cardiac function and flow measurements of stroke volume and cardiac output, and MRI shows promise in detecting fibrosis and edema.3 Magnetic resonance imaging–guided cardiac catheterization was first described by Razavi et al4 in 2003 and has continued to evolve. This innovative procedure is now being performed successfully in adult and pediatric populations internationally.1,2,5
Patients undergoing diagnostic cardiac catheterization, including MRI-guided procedures, are at risk for life-threatening arrhythmias such as complete heart block and ventricular fibrillation.6 These arrhythmias require immediate action, which can be challenging to implement in the interventional cardiac MRI (iCMR) environment. Other unique safety issues that are added to the procedural environment when MRI is used include the need for fastidious exclusion of unsafe metal objects and team understanding of emergency procedures unique to MRI.
The iCMR suite combines a cardiac catheterization x-ray laboratory with an MRI suite. At our institution we have performed iCMR procedures (ie, MRI-guided cardiac catheterizations) under institutional review board–approved research protocols since 2015. Because the work described in this article was of a quality improvement nature, additional institutional review board approval was not required. Given the unique work environment that incorporates x-ray and MRI in a highly technical environment, it is crucial for our team to provide education and stress the importance of magnet safety to ensure that our patients and staff remain safe. Also of significant importance is training staff members from multiple disciplines on how to handle emergency evacuations in the iCMR suite. Creating a safety protocol using quarterly in situ evacuation drills led by advanced practice and research nurses is necessary to prevent serious adverse events in the iCMR suite. The primary aim of this quality improvement initiative was to promote MRI safety and staff preparedness to respond in emergency situations in the specialized iCMR environment.
MRI-Guided Cardiac Catheterization Workflow
At our institution, the iCMR suite consists of a 1.5-T MRI scanner (MAGNETOM Aera, Siemens Healthineers) in a room that is connected via automatic doors to a separate biplane fluoroscopy catheterization room (Figure 1). The MRI side of the suite is outfitted for cardiac catheterization with a real-time cardiac MRI console (Interactive Front End, Siemens Healthineers), wireless operator noise-canceling communication headsets (IMROC, Optoacoustics), hemodynamic recording system interface (Physiological Recording in MRI Environment [PRiME], Centers for Information Technology, National Institutes of Health),7 and in-room shielded liquid crystal display projectors (GJJ-PRO shielding, Gaven Industries) for a rear-projection screen that can slide to the head or foot of the patient as needed.6 Further details regarding equipment and room setup can be found in our previously published work.1,2
Figure 1.

Interventional cardiac magnetic resonance imaging suite with adjoining magnetic resonance imaging room and biplane x-ray fluoroscopy room.
The patient is moved via a transfer system consisting of an x-ray table and an MRI table (Combi Dockable Table, Siemens Healthineers) into the MRI scanner via the automatic door that separates the 2 suites. The automatic door is open only during times of patient transfer between the catheterization room and the MRI room. When the door is open during patient transfer, the entire iCMR suite is considered MRI zone IV.8 Upon completion of safe patient transfer, the doors are immediately closed and the catheterization side of the suite and the control rooms revert to MRI zone III (Figure 2).
Figure 2.
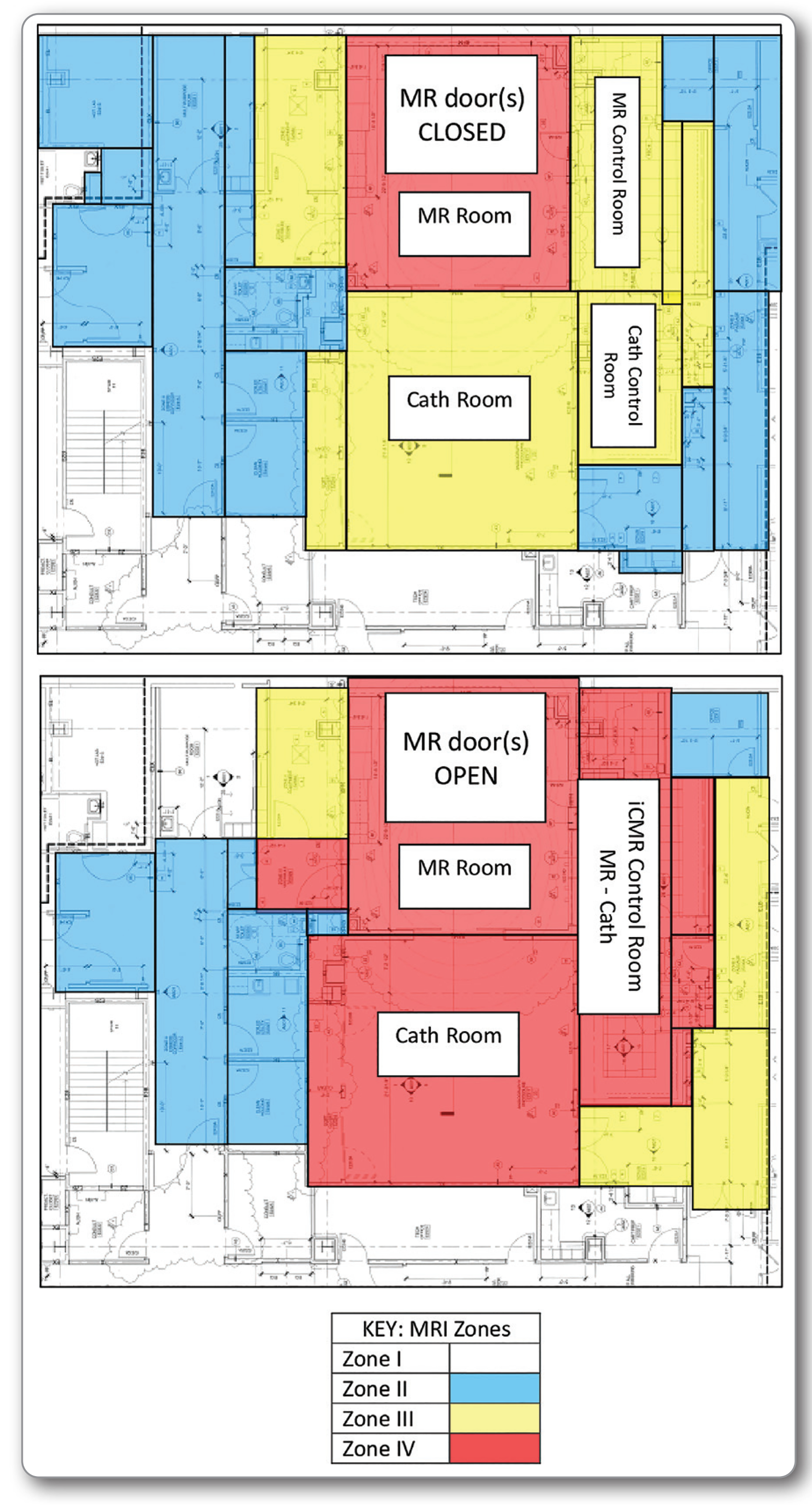
Magnetic resonance imaging (MRI) zones for interventional cardiac MRI (iCMR). Top image depicts the MRI zones in and around the iCMR suite when the automated dividing doors are closed. The MRI room is designated as zone IV (red), and the adjacent rooms (MRI/catheterization control rooms and catheterization room) are zone III (yellow). Bottom image depicts the MRI zones in and around the iCMR suite when the automated dividing doors are open. The MRI room and adjacent rooms (MRI/catheterization control rooms and catheterization room) become zone IV (red).
A team huddle is held before each MRI-guided cardiac catheterization. All members involved in the case are required to be present. The patient’s case is presented and the procedure is reviewed. Any additional testing, interventions, and imaging are identified. The evacuation plan and provider roles are reviewed.
Patients enrolled in the MRI-guided cardiac catheterization study protocol are placed under either general anesthesia or deep sedation by our cardiac anesthesia team in the catheterization room. After induction of anesthesia, the patient is prepared and draped, and access to the femoral or neck catheter site is obtained. The access site is secured with a transparent film dressing or sutured in place. All metal is cleared from the table. The MRI/catheterization nurses and technologists perform a metal time-out and final metal sweep. A second sterile drape is placed over the patient to maintain sterility in preparation for transfer. The automated doors separating the MRI and x-ray suites are opened. Baseline images are obtained and reference images are created. Magnetic resonance imaging–guided cardiac catheterization is performed using the reference images as guidance. Additional MRI images may be obtained. Another drape is placed on the patient to maintain sterility in preparation for transfer. The patient is transferred back to the x-ray room for additional interventions. Catheter sheaths are removed and hemostasis is obtained. The patient is extubated, if applicable, and transferred to the cardiac procedure recovery room or the cardiac intensive care unit.
Methods
To help prepare our team for emergency situations, we implemented quarterly evacuation drills with a live volunteer. The drills are performed in situ because this method provides a sense of realness to the simulation and an opportunity to better identify environmental or system issues that could compromise patient and staff safety.9 The drills are led by the iCMR nurse practitioner and research nurse. Simulation drills have been shown to be effective for preparing staff members for emergency situations. They allow all team members to actively engage in the scenarios and collaborate as a team.10 Institutional safety policies are available on the intranet so that all iCMR staff members can access them at any time. Additionally, all iCMR staff members are required to maintain basic life support and pediatric advanced life support certifications.
Safety Drill Workflow
All staff members involved in specialized iCMR cases (interventional cardiologist, MRI cardiologist, anesthesiologist, fellows, catheterization/MRI nurses, catheterization/MRI technologist, and research staff) are required to attend. Two to 4 simulations are performed for team members in rotation. The acting interventional cardiologist leads the drill, simulating an MRI-guided cardiac catheterization and announcing a cardiac arrest code or a need to evacuate. Supporting staff members are responsible for assisting in resuscitation (anesthesiologist, fellows, and catheterization/MRI nurse and technologist), removing the patient from the MRI scanner to the catheterization room (catheterization/MRI nurse and technologist), and crowd control (MRI cardiologist and research staff). Drilled scenarios include shockable arrhythmias, table or door malfunction, and environmental emergencies such as water intrusion or fire (Figure 3). Evacuations are timed from the cardiac arrest code alert to safe evacuation or defibrillation if appropriate. Observing staff members note what the team did well and what could be improved. The drills adjourn with a debriefing session to highlight and discuss what was done well and identify areas for improvement. Action plans are made and tasks are delegated. The entire team receives a follow-up email providing a summary of the drill and action plans for the areas needing improvement. Updates and changes developed from the previous drill are presented at the beginning of the next drill to reinforce learning.
Figure 3.
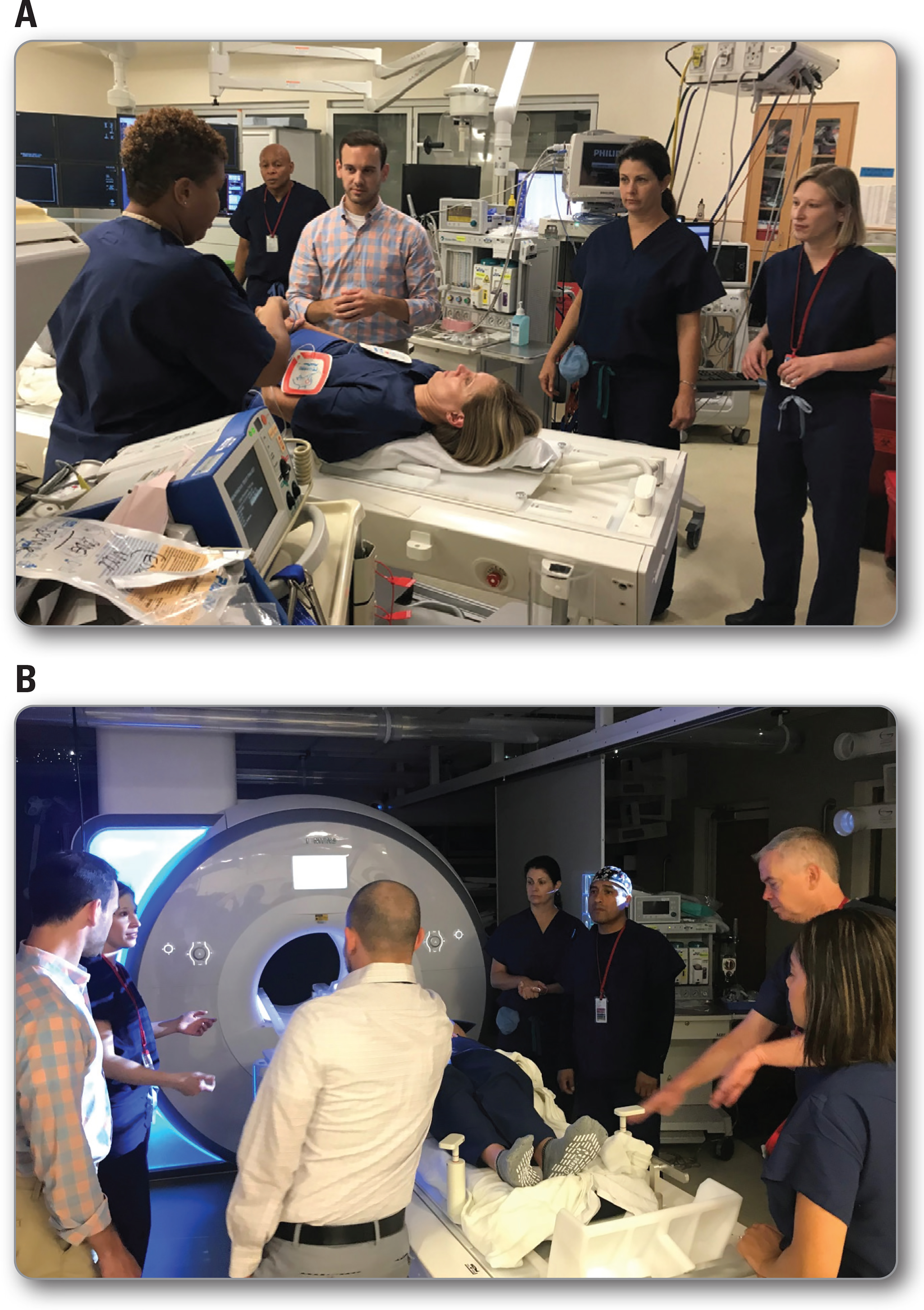
A. Evacuation drill with members of the interventional cardiac magnetic resonance imaging (iCMR) team on the x-ray side of the iCMR suite: interventional cardiologist, anesthesiologist, cardiac fellow, catheterization laboratory technologist, catheterization laboratory nurse, and research staff member. B. Evacuation drill with members of the iCMR team on the magnetic resonance imaging (MRI) side of the iCMR suite: interventional cardiologist, anesthesiologist, cardiac MRI physician, cardiology fellow, MRI technologist, MRI nurse, and research staff member.
Because we have rotating staff, especially with our cardiology and anesthesiology trainees, we strategically schedule an evacuation drill near the beginning of the academic year (ideally at the beginning of August before the new fellows rotate through the catheterization laboratory). This schedule guarantees that all new staff members have received the mandatory MRI safety education course provided by our hospital physicist and are properly oriented to the iCMR environment. After this initial drill, the iCMR nurse practitioner schedules the drills on a quarterly basis.
Measurements and Definitions
To quantitatively measure the effectiveness of these drills, we conducted a retrospective participant survey. The survey consisted of 6 questions. The participants used a Likert scale from 1 (strongly disagree) to 5 (strongly agree) to rank their attitudes toward the evacuation drills. Additionally, the drills were timed (in seconds) from the interventional cardiologist’s announcement of a cardiac arrest code alert or a need to evacuate to the first defibrillation or safe evacuation to the catheterization side of the suite.
Results
The evacuation drills were implemented in March 2015 and performed on a quarterly basis. Fourteen drills were performed over 4 years (March 2015 through July 2019). A mean (range) of 17 (11–25) iCMR staff members, including at least 1 representative from each discipline, participated in each drill. All individuals who had ever participated in a drill received the retrospective participant survey. Twenty-nine of 48 total participants responded, a response rate of 60%. An overall majority agreed or strongly agreed that the evacuation drills were a positive experience (90%) and that the drills helped clarify their roles and responsibilities during an emergency evacuation (Figure 4). All participants agreed or strongly agreed that the evacuation drills helped boost confidence in their ability to safely evacuate a patient from the iCMR suite in an emergency or cardiac arrest event. In comparison, 28% of participants indicated that they were not confident in their ability to safely evacuate a patient before participating in a drill (Figure 4). One participant commented that “evacuation drills are a necessity.”
Figure 4.
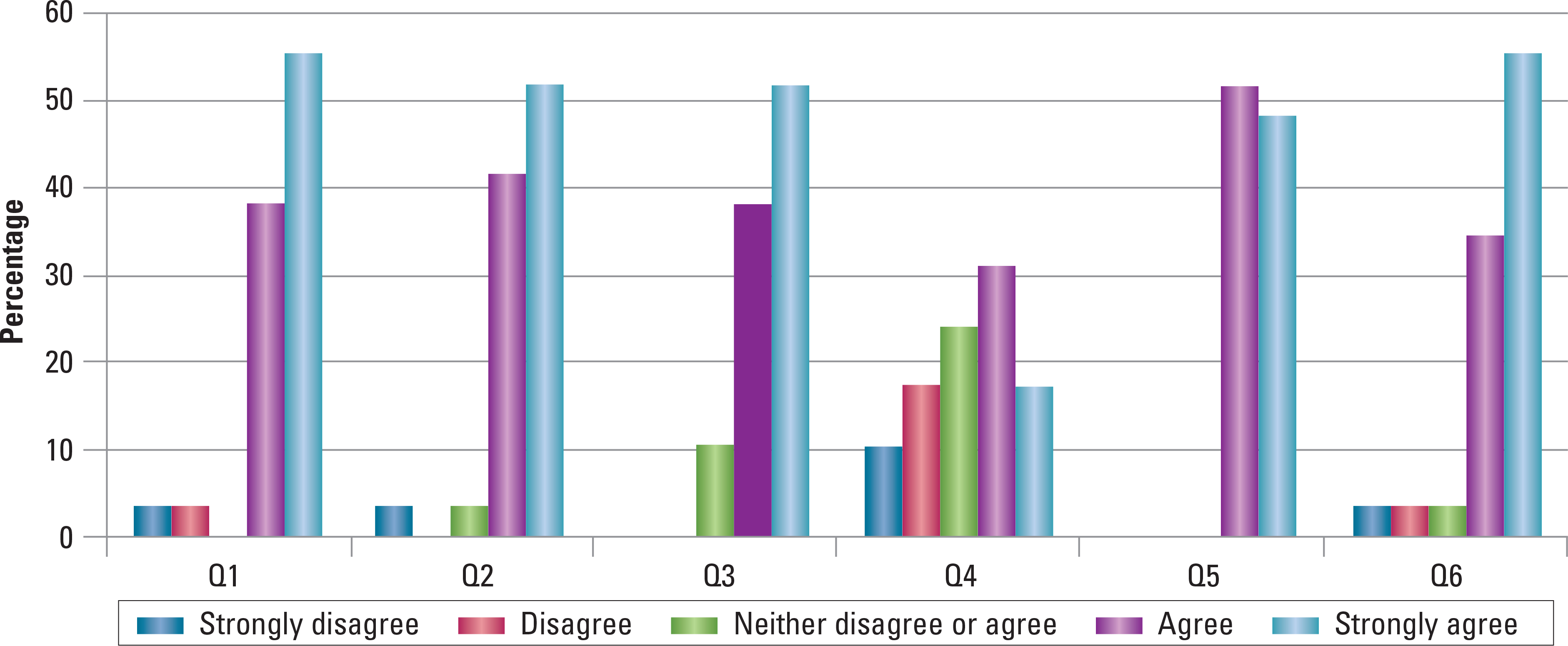
Retrospective participant survey results. Q1. Evacuation drills have clarified my role and responsibilities in an emergency evacuation. Q2. Evacuation drills have increased my awareness of MRI safety. Q3. Evacuation drills have helped identify emergency release buttons on the MRI Combi table. Q4. Before participating in an evacuation drill I was confident in my ability to safely evacuate a patient from the iCMR suite in an emergency/code situation. Q5. After participating in an evacuation drill I was confident in my ability to safely evacuate a patient from the iCMR suite in an emergency/code situation. Q6. Overall the evacuation drills are a positive experience.
Abbreviations: iCMR indicates interventional cardiac magnetic resonance imaging; MRI, magnetic resonance imaging.
Room evacuation times improved from 71 to 41 seconds after the drills. We attribute this result mainly to the hands-on experience the drills provide. This improvement in response time helped boost the staff ’s confidence in performing in an evacuation scenario. Performing the drills in situ also helped staff members identify safety features of the equipment to allow for a swift and seamless evacuation (eg, in case of table failure; Figure 5). No patient and/or staff member safety events occurred in the iCMR environment.
Figure 5.
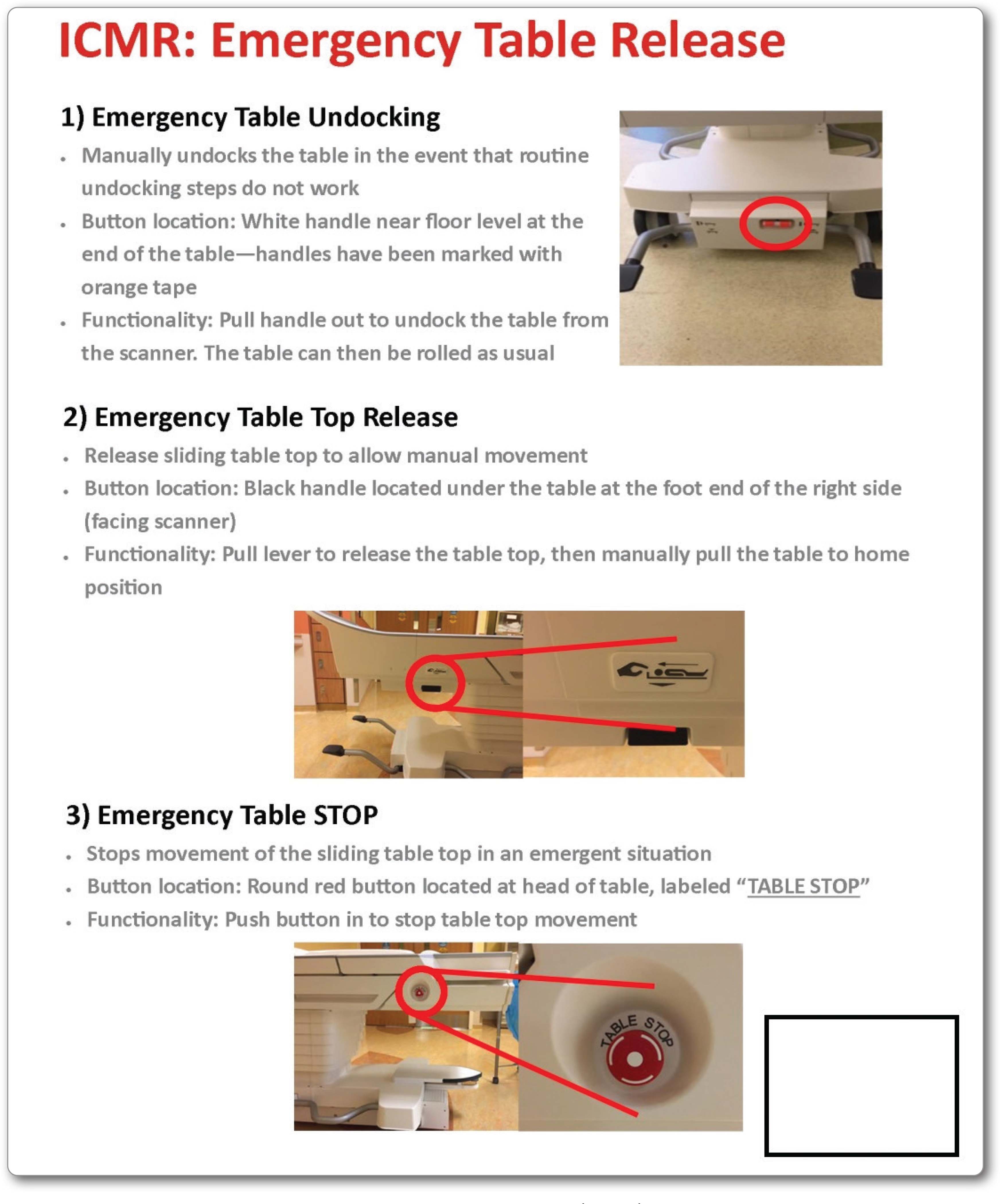
Interventional cardiac magnetic resonance imaging (ICMR) safety poster depicting location of emergency release buttons. Poster is displayed in the magnetic resonance imaging control room for easy viewing.
Discussion
This article describes our institution’s creation of a safety protocol using quarterly in situ evacuation drills in the iCMR environment. This protocol has proven to be an effective tool for improving and maintaining the safety of our patients and staff. With the ever-growing interest in iCMR, it is crucial to highlight the importance of MRI safety training. One of the responsibilities of the catheterization laboratory nurse is assistance in resuscitation efforts, which includes making sure the defibrillator is readily available and ready for use. Currently standard defibrillators are not approved for use in an MRI setting.6 Magnetic resonance imaging–conditional defibrillators are currently being tested but have yet to obtain regulatory approval.11 This situation poses a huge challenge for high-risk iCMR procedures. Implementing a safety protocol such as the one described in this article provides a solution to this challenge and makes performing these innovative procedures safe and feasible.
Although these safety drills are not true simulations with computerized manikins, the underlying concept of these drills is modeled after simulation-based learning techniques. The rise of simulation-based learning in the health care community has grown exponentially over the years, especially after the Institute of Medicine report To Err Is Human in 1999.12–14 This report estimated that up to 98 000 preventable health care–related deaths occurred annually in the United States,14 and follow-up studies estimated that annual preventable deaths would increase to 400 000 in 2013.15
Studies from The Joint Commission suggest that medical errors leading to preventable deaths are commonly caused by poor teamwork and communication.13 Simulation-based training has proven to be effective in improving the communication and performance of multidisciplinary teams.16 From critical care and surgical settings to medical school training, simulation-based learning has been integrated into technical and safety training sessions across the medical field. Providing hands-on experience helps familiarize medical practitioners with complex scenarios, build team members’ confidence in executing expected responsibilities, and eliminate situation and role confusion.16 These benefits are especially true in high-stress situations like cardiac resuscitations, where timeliness, coordination, and safety are critical.
Because of the novelty of iCMR procedures, specifically MRI-guided cardiac catheterization, no comparative studies are available. Similarly, literature describing emergency simulation drills in the MRI environment is scarce. However, a common theme throughout MRI safety publications is the dire importance of continuing staff education to avoid adverse events.17 The simulation drills described in this article take education a step further by providing staff members with real-life experience. One group from the University of Munich had a similar approach to emergency training. Muehling et al18 used in situ code drills with a live volunteer as a means of safety training for dobutamine stress MRI. They performed 30 drills with similar results regarding improved evacuation times. They concluded that repetitive practice significantly improved their rescue times. Although our group has not achieved this number of evacuation drills, our data to date suggest that focused in situ emergency response drills are an important component to minimizing rescue time.
Limitations
Challenges encountered have been related to scheduling. To ensure attendance and efficient timing for these drills, an hour-long block in the iCMR suite is necessary. The drills require the use of both the x-ray and MRI rooms, which function independently of each other when no iCMR procedures are scheduled. As a result, case start times on drill days are delayed by an hour and a half. Over 4 years of performing these drills, we have canceled a handful of drills because of miscommunication. Communicating the date and time of these drills among the various disciplines that use these spaces is required to prevent further case delays and unnecessary cancellations of the safety drills.
Conclusions
Along with the overwhelmingly positive response from the retrospective survey, these drills led to identification of several safety improvements that have been incorporated into standard operations. Practice recommendations include the following: (1) properly identifying emergency release latches and buttons for the MRI table in case of table failure, (2) posting illustrations of the location of emergency release buttons in the iCMR suite for easy viewing (Figure 5), (3) creating signage outlining staff roles in an emergency evacuation, (4) performing a metal time-out and room sweep before patient transfer to or from the MRI side of the suite, (5) placing all anesthesia ventilation tubing and intravenous catheter access on the right side of the patient to prevent ventilator or intravenous tube dislodgment, and (6) performing personal metal checks and announcing “I am safe” before entering the MRI side of the suite.
As driving forces behind evacuation drills and staff education, nurses in this specialized environment are crucial for promoting patient and staff safety. It is imperative that other institutions embarking on the iCMR journey implement similar precautions to ensure patient and staff safety.
Magnetic resonance imaging–guided cardiac catheterization evacuation drills promote preparedness, ensure patient and staff safety, and improve evacuation time in the iCMR environment. Our institution’s approach to iCMR safety can be used as a model for other iCMR programs.
Acknowledgments
Tacy Downing, MD, Karen Thompson, MD, Brad Ralston, MD, Christopher Hairston, RCIS, Keisha Grant, RCIS, Simon Vargas, RTR, Shena Phillips, RTR, were photographed during an evacuation drill.
Footnotes
Financial Disclosures
This study was funded by National Heart, Lung, and Blood Institute, National Institutes of Health, grant/award numbers HHSN268201500001C,Z01-HL005062, and 1R01-HL144494–01.
See also
To learn more about cardiovascular care, read “Impact of CPR Quality and Adherence to Advanced Cardiac Life Support Guidelines on Patient Outcomes in In-Hospital Cardiac Arrest” by Kaplow et al in AACN Advanced Critical Care, 2020;31(4):401–409. Available at www.aacnacconline.org.
Contributor Information
Ileen F. Cronin, Department of Anesthesiology, Perioperative and Pain Medicine, Lucile Packard Children's Hospital Stanford, Palo Alto, California..
Joshua P. Kanter, George Washington University School of Medicine, Washington, District of Columbia, and Director of the cardiac catheterization laboratory and an interventional cardiologist, Division of Cardiology, Children's National Hospital, Washington, District of Columbia..
Nina Deutsch, George Washington University School of Medicine, and Director of cardiac anesthesiology, Division of Cardiology, Children's National Hospital..
Karin Hamann, Division of Cardiology, Children's National Hospital..
Laura Olivieri, George Washington University School of Medicine, and Director of cardiac MRI/CT and an advanced imaging cardiologist, Division of Cardiology, Children's National Hospital..
Russell R. Cross, George Washington University School of Medicine, and Medical Director of inpatient cardiology and an advanced imaging cardiologist, Division of Cardiology, Children's National Hospital..
References
- 1.Ratnayaka K, Kanter JP, Faranesh AZ, et al. Radiation-free CMR diagnostic heart catheterization in children. J Cardiovasc Magn Reson. 2017; 19(1):65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Deutsch N, Swink J, Matisoff AJ, et al. Anesthetic considerations for magnetic resonance imaging-guided right-heart catheterization in pediatric patients: a single institution experience. Paediatr Anaesth. 2019;29(1):8–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fratz S, Chung T, Greil GF, et al. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson. 2013;15(1):51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Razavi R, Hill DL, Keevil SF, et al. Cardiac catheterisation guided by MRI in children and adults with congenital heart disease. Lancet. 2003; 362(9399):1877–1882. [DOI] [PubMed] [Google Scholar]
- 5.Rogers T, Ratnayaka K, Khan JM, et al. CMR fluoroscopy right heart catheterization for cardiac output and pulmonary vascular resistance: results in 102 patients. J Cardiovasc Magn Reson. 2017;19(1):54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mazal JR, Rogers T, Schenke WH, et al. Interventional-cardiovascular MR: role of the interventional MR technologist. Radiol Technol. 2016; 87(3):261–270. [PMC free article] [PubMed] [Google Scholar]
- 7.Kakareka JW, Faranesh AZ, Pursley RH, et al. Physiological recording in the MRI environment (PRiME): MRI-compatible hemodynamic recording system. IEEE J Transl Eng Health Med. 2018;6:4100112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Expert Panel on MR Safety, Kanal E, Barkovich AJ, et al. ACR guidance document on MR safe practices: 2013. J Magn Reson Imaging. 2013;37(3): 501–530. [DOI] [PubMed] [Google Scholar]
- 9.Patterson MD, Blike GT, Nadkarni VM. In situ simulation: challenges and results. In: Henriksen K, Battles JB, Keyes MA, Grady ML, eds. Advances in Patient Safety: New Directions and Alternative Approaches. Volume 3: Performance and Tools. Agency for Healthcare Research and Quality; 2008. [PubMed] [Google Scholar]
- 10.Brown S, Nelson J. The use of interprofessional simulation among chronic pediatric populations: a review of the literature. Clin Simulation Nurs. 2014;10(4):191–197. [Google Scholar]
- 11.Schmidt EJ, Watkins RD, Zviman MM, Guttman MA, Wang W, Halperin HA. A magnetic resonance imaging–conditional external cardiac defibrillator for resuscitation within the magnetic resonance imaging scanner bore. Circ Cardiovasc Imaging. 2016;9(10):e005091. doi: 10.1161/CIRCIMAGING.116.005091 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dunn W, Dong Y, Zendejas B, Ruparel R, Farley D. Simulation, mastery learning and healthcare. Am J Med Sci. 2017;353(2):158–165. [DOI] [PubMed] [Google Scholar]
- 13.Volk MS. Improving team performance through simulation-based learning. Otolaryngol Clin North Am. 2017;50(5):967–987. [DOI] [PubMed] [Google Scholar]
- 14.Kohn LT, Corrigan JM, Donaldson MS, eds; Committee on Quality of Health Care in America, Institute of Medicine. To Err Is Human: Building a Safer Health System. National Academy Press; 1999. [PubMed] [Google Scholar]
- 15.James JT. A new, evidence-based estimate of patient harms associated with hospital care. J Patient Saf. 2013;9(3):122–128. [DOI] [PubMed] [Google Scholar]
- 16.Su L, Spaeder MC, Jones MB, et al. Implementation of an extracorporeal cardiopulmonary resuscitation simulation program reduces extracorporeal cardiopulmonary resuscitation times in real patients. Pediatr Crit Care Med. 2014;15(9):856–860. [DOI] [PubMed] [Google Scholar]
- 17.Cross NM, Hoff MN, Kanal KM. AvoidingMRI-related accidents: a practical approach to implementing MR safety.J Am Coll Radiol.2018;15(12):1738–1744. [DOI] [PubMed] [Google Scholar]
- 18.Muehling OM, Huber A, Fredrich D, Nabauer M, Reiser M, Schoenberg SO. Code blue in the MR suite—a drill to rescue a patients with cardiac arrest from the MR scanner. Int J Cardiovasc Imaging. 2006;22(2):257–261. [DOI] [PubMed] [Google Scholar]