

Abstract
Objective:
Sexual aggression remains a significant public health problem, with the majority of sexual assaults involving alcohol. Founded upon an experimental medicine approach to behavior change, the current study used a proximal change experiment to target and test emotion regulation (ER) as a mechanism underlying alcohol-involved sexual aggression.
Methods:
Heavy episodic drinking men aged 21–30 with a sexual assault perpetration history (N = 209) were randomly assigned to a brief, online, ER-focused cognitive restructuring or mindfulness intervention or to control. Intervention effects were evaluated during sober and intoxicated states through laboratory-based alcohol administration (target BrAC = .08%). Intoxicated and sober participants completed a proximal change protocol that included implementing ER skills during a sexual aggression analogue that assessed relevant emotions and intentions.
Results:
Path analysis demonstrated that relative to control, the cognitive restructuring intervention improved emotional modulation and emotional clarity, resulting in lower sexual arousal and anger, respectively, followed by decreased sexual coercion intentions. The mindfulness intervention yielded mixed results, predicting decreased sexual aggression intentions compared to control but also predicting stronger coercive tactic intentions in intoxicated men with more severe sexual aggression histories. Both interventions improved emotional acceptance relative to control, but only for sober men.
Conclusions:
Overall, the current study demonstrated that ER-focused interventions improved proximal ER skills associated with reduced sexual aggression intentions, signifying ER as an important mechanism for changing sexually aggressive behavior. Because intervention efficacy varied by intoxication state, further research is needed to assess the effectiveness of ER interventions targeting real-world alcohol-involved sexual aggression.
Despite the proliferation of sexual assault prevention programs, rates of sexual assault continue to present a significant public health problem in the U.S. Nationally, over 1 in 3 women (36.3%) of women have experienced sexual violence in their lifetimes, primarily by male perpetrators (Smith et al., 2017). Because the majority of sexual assaults involve alcohol consumption by the perpetrator, the victim, or both (Testa, 2002), continued efforts to reduce alcohol-involved sexual aggression are essential.
Evidence-based approaches to reducing sexually aggressive behavior are limited, however. A systematic review of primary prevention strategies for sexual assault perpetration found only three effective prevention approaches, noting that studies in this field are plagued by a lack of rigor and replication (DeGue et al., 2014). Additionally, even in studies that demonstrate changes in sexually aggressive behavior, the mechanisms underlying these changes are typically not identified (Salazar et al., 2014). To address some of these deficiencies, the current study utilized the Science of Behavior Change (SOBC) experimental medicine approach (Nielsen et al., 2018) to test two interventions for reducing sexually aggressive behavior. Commensurate with the tenets of the SOBC approach, we first identified a malleable intervention target (emotion regulation) supported by both theory and empirical literature as having promise for influencing sexually aggressive behavior. We then developed two interventions to target this specified mechanism, implemented the interventions using experimental methods, and assessed intervention effects on the target mechanism of emotion regulation. Finally, we tested whether changes in the target mechanism of emotion regulation resulted in changes in intentions to engage in sexually aggressive behavior utilizing a proximal change experiment (Babcock et al., 2011; Gottman et al., 2005). Similar to drug development proof of concept studies, proximal change experiments test interventions that focus on “small, specific, measurable behavior changes” in order to provide initial empirical evidence regarding the proximal effects of the intervention (Gottman et al., 2005, p. 165). Proximal change experiments not only demonstrate that an intervention target is a mechanism of behavior change (Kazdin & Nock, 2003) but also provide data that can serve as the empirical foundation for conducting more resource-intensive, large-scale clinical trials (Gottman et al., 2005). Given our interest in alcohol-involved sexual assault, another critical benefit of the proximal change experimental approach is that it enables a randomized, rigorous evaluation of intervention efficacy during both sober and intoxicated states using an alcohol administration paradigm. Such an approach provides evidence regarding the necessity of adapting intervention content such that it specifically and differentially targets putative mechanisms of behavior change during intoxicated and sober states. To our knowledge, investigation of intervention effects on target mechanisms during randomly assigned states of intoxication/sobriety is a unique contribution to the SOBC field.
Emotion Regulation and Sexually Aggressive Behavior
Behavioral research studies have demonstrated that difficulties in emotion regulation (ER) may be an important mechanism underlying men’s sexual aggression against women. ER difficulties refer to “the inability, even when one’s best efforts are applied, to change or regulate emotional cues, experiences, actions, verbal responses, and/or nonverbal expression” (Linehan et al., 2007, p. 583). ER difficulties play a prominent role in many explanatory theories of sexual aggression, in which problems coping with negative emotions are postulated to result in attempts to use alcohol or sex to satisfy or reduce negative affect (Ward & Beech, 2006). Of note, studies have consistently demonstrated a positive association between ER difficulties and aggressive behavior at both distal and daily levels (Pond et al., 2012; Stappenbeck & Fromme, 2014; Tager et al., 2010), suggesting that sexually aggressive men have more pronounced difficulties than other men regulating their negative emotions. Moreover, sexually aggressive men report greater tendencies towards anger and hostility, particularly towards women, compared to other men (Logan-Greene & Davis, 2011; Lyn & Burton, 2007), and sexually aggressive men with poor emotion regulation skills are more likely to behave aggressively towards women following provocation (Pickett et al., 2016). Thus, the dysregulation of anger may represent an especially important mechanism underlying sexual aggression, particularly for more severe perpetrators (Ward & Beech, 2006). Additionally, research indicates that emotion regulation abilities may transfer to regulatory ability in other emotional domains, such as the regulation of sexual arousal (Winters et al., 2009), in that differential use of emotion regulation is associated with modulation of physiological and subjective sexual arousal (Both et al., 2011). Based on these findings, we investigated intervention effects on ER skills and whether these ER skills subsequently influenced the emotional domains of anger and sexual arousal.
Importantly, acute alcohol intoxication impairs the higher order cognitive functions necessary for effective ER, thus potentially resulting in greater sexual aggression likelihood (Stappenbeck & Fromme, 2014). Alcohol intoxication plays a critical role in moderating the effects of distal trait anger/hostility on both in-the-moment anger and aggressive responses. For example, alcohol’s effects on proximal in-the-moment anger expression (Eckhardt, 2007) and aggression after provocation are typically the strongest for men with greater hostile tendencies (Parrott & Giancola, 2004). Moreover, intoxicated men with greater trait hostility report feeling more justified in coercing nonconsensual sex than do sober men (Abbey et al., 2009). Similarly, alcohol intoxication can disrupt men’s ability to regulate their sexual arousal (George et al., 2006), and men with greater sexual arousal report stronger intentions to engage in sexual aggression (Ariely & Lowenstein, 2006). Finally, ER difficulties moderate the relationship between men’s alcohol consumption in sexual situations and sexual assault perpetration (Kirwan et al., 2019). In sum, research indicates that both intoxication and emotional factors play key roles in sexual aggression. It follows then that interventions which improve ER skills can potentially increase men’s ability to regulate their emotions even after alcohol consumption, further reducing their sexual aggression likelihood.
Emotion Regulation Interventions.
Interventions directed toward teaching adaptive ER skills have been effective in reducing alcohol use (Stappenbeck et al., 2015) and treating several psychological disorders (Moses & Barlow, 2006), suggesting promise in their ability to target a potential mechanism of behavior change for reducing sexual aggression. Skills that enable individuals to modify emotions or to accept and tolerate undesirable emotions have been identified as important targets for interventions (Berking et al., 2008). Cognitive restructuring and mindfulness are two techniques well-suited to address these ER skills. Cognitive restructuring is included in many cognitive behavioral therapies and involves actively challenging and modifying one’s thoughts as a way to change how one feels about a given situation or experience that influences subsequent behavior. Further, cognitive restructuring has been effectively implemented in brief single-session interventions to reduce substance use (Stappenbeck et al., 2015) and attenuate physiological and subjective sexual arousal in the presence of sexual stimuli (Shafir et al., 2018; Winters et al., 2009). Mindfulness as an ER skill promotes nonjudgmental acceptance and tolerance of emotions, which is thought to reduce the distress associated with upsetting emotions rather than modifying the emotions per se (Gratz & Tull, 2010). Notably, high levels of dispositional mindfulness appear to serve as a protective factor in the association between men’s alcohol use and sexual aggression (Gallagher et al., 2010). Despite the promise of these ER intervention approaches, research is still needed to determine whether such ER interventions can effectively be applied to reduce men’s sexual aggression. Although some work with incarcerated sexual offenders has incorporated ER skills training into their interventions (Gillespie et al., 2012; Stinson & Becker, 2013), ER has not been a focus of sexual aggression prevention work with non-incarcerated populations.
ER techniques may be especially effective at reducing aggression while intoxicated (Giancola et al., 2009); however, this supposition has not yet been tested. As noted, sexually aggressive men often engage in heavy alcohol consumption which has demonstrated associations with both sexual aggression severity (Testa, 2002) and ER deficits (Stappenbeck & Fromme, 2014), and ER moderates the relationship between alcohol consumption in sexual situations and sexual aggression perpetration (Kirwan et al., 2019). Such findings indicate that it is important to understand whether or not ER interventions that are efficacious during states of sobriety also maintain their efficacy after individuals have consumed alcohol to the point of intoxication. Thus, this study investigated the effects of acute alcohol intoxication on ER intervention efficacy for sexual aggression reduction.
The Current Study and Hypotheses
Using proximal change experimental procedures, young men with elevated risk of perpetrating alcohol-involved sexual aggression were randomly assigned to either 1) a brief, online, cognitive restructuring ER skills training; 2) a brief, online mindfulness ER skills training; or 3) an attention control condition. Next, participants were randomly assigned to consume either an alcoholic or non-alcoholic beverage after which they read and responded to a hypothetical nonconsensual sexual scenario with a woman. We hypothesized that, relative to men in the control condition, men in both ER intervention conditions would report improved ER skills across four domains of ER (Figure 1). We also predicted that both ER intervention conditions would be indirectly predictive of decreased sexual aggression intentions (i.e., intentions to use coercive tactics and intentions to engage in nonconsensual sex) through improved ER skills and subsequent reductions in sexual arousal and anger. Additionally, we expected that alcohol intoxication would moderate the effects of the interventions on ER such that sober men who received either ER intervention would report greater ER skill improvement than intoxicated men who received an intervention and sober or intoxicated men in the control condition. We also hypothesized that alcohol intoxication would predict increased sexual aggression intentions directly as well as indirectly through poorer emotion regulation, greater sexual arousal, and greater anger when the female partner does not consent to sexual activity. Finally, sexual aggression history severity was expected to predict greater sexual aggression intentions both directly and indirectly through poorer emotion regulation, greater sexual arousal, and greater anger (Ward & Beech, 2006). Given the novelty of the study and the lack of data on which to base a priori hypotheses, comparisons of the two interventions as well as the two-way and three-way interactions of beverage condition, intervention condition, and sexual aggression history severity on ER skills, sexual arousal, anger, coercive tactics intentions, and nonconsensual sex intentions were explored.
Figure 1:
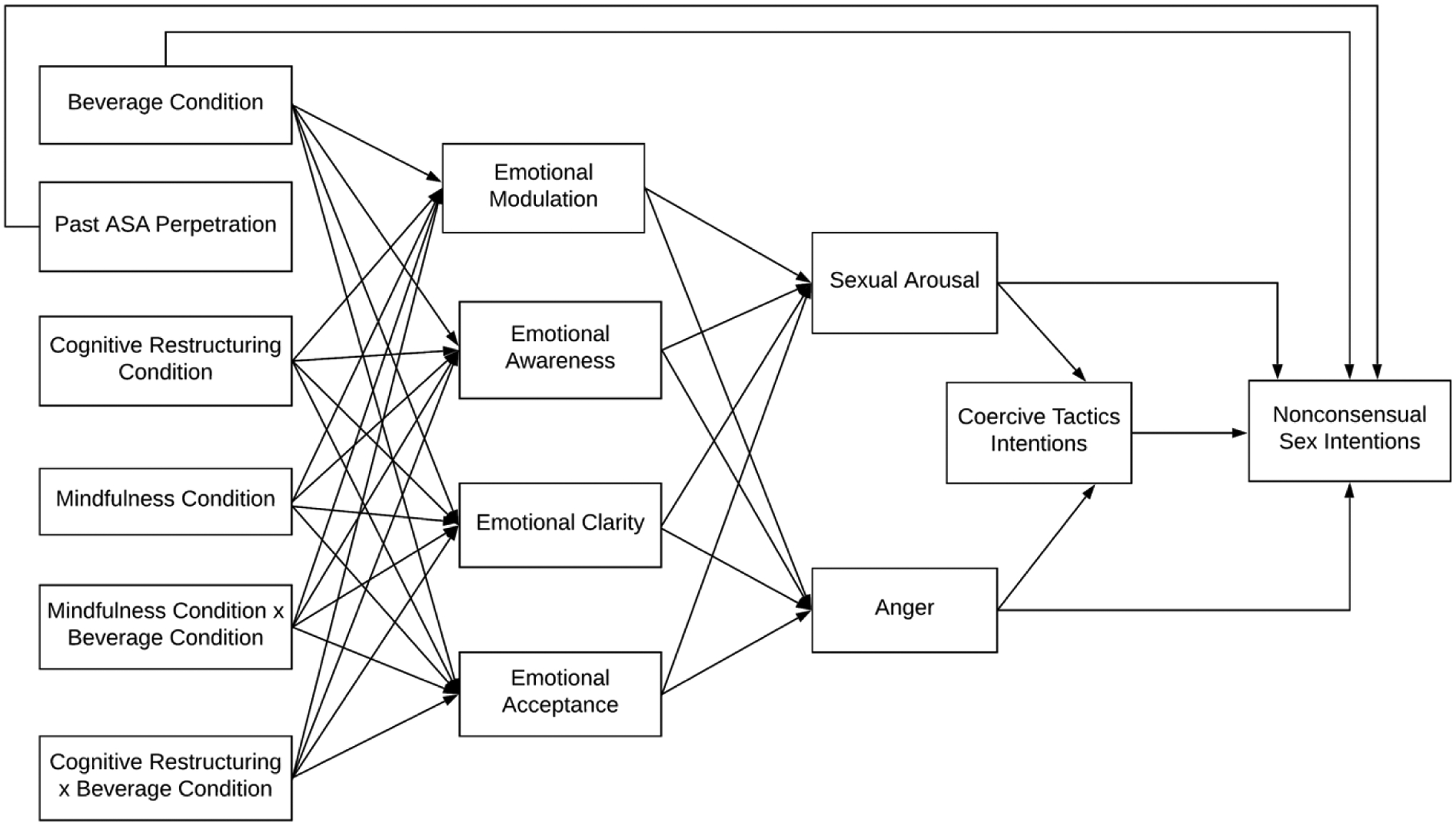
Hypothesized Model
Note: Exploratory two- and three-way interactions are not depicted in the model
Methods
Participants were recruited through online and print advertisements, as well as the university registrar’s student list. The advertisements solicited 21–30 year old single male drinkers who were interested in dating women. Interested men completed an online screening survey to determine eligibility, then were called to confirm eligibility and schedule an appointment.
Participants
Men (N = 209) were eligible if they were between 21–30 years old, had sexual intercourse with a woman at least once in the past year, and reported at least one incidence of sexual coercion or aggression perpetration in their lifetime (i.e., nonconsensual sexual contact or intercourse; Struckman-Johnson, Struckman-Johnson, & Anderson, 2003). To comply with guidelines for ethical alcohol administration (NIAAA, 2005), eligibility criteria also included no history of alcohol problems as assessed by the Brief Michigan Alcoholism Screening Test (Pokorny et al., 1972), no medical conditions or medications that contraindicated alcohol consumption, and weekly consumption of at least 3 alcoholic drinks. To target higher risk drinkers, at least one instance of heavy episodic drinking in the past year was also required for eligibility (Davis, 2010).
Participants (Mage = 24.76, SD = 2.77) self-identified as: White and/or European American (61.9%), Asian American (18.3%), Black and/or African American (6.9%), Multi-racial (11.4%), and “Other race” (1.5%), with 10.1% of the sample identifying as Hispanic/Latino. Over 60% of the sample indicated they were full-time undergraduate or graduate students, and 44.2% reported that they had a college degree.
Procedures
All procedures and measures were approved by the University’s Human Subject Division. Participants were not allowed to drive to their appointment, eat or drink caloric beverages for three hours prior to their appointment, or drink alcohol or use any over-the-counter or recreational drugs for 24 hours before their appointment. Upon arrival, a trained male research assistant verified their identification and age and ensured that they had a breath alcohol concentration (BrAC) of 0.00 through a breath test using an Alco-Sensor IV (Intoximeters, Inc.). After providing informed consent, participants were weighed to calculate their correct beverage dose and completed background measures on a computer in a private room. Based on the severity of their sexual aggression history, participants were block randomized to a computerized five-to-ten minute ER-focused cognitive restructuring (CR) intervention, a computerized five-to-ten minute ER-focused mindfulness intervention, or an attention control condition and then were block randomized to either the alcohol condition or no-alcohol condition. Participants in the intervention conditions were told they would learn and practice a skill for coping with negative emotions. Consistent with the ABC model of cognitive restructuring (Ellis, 2008), participants in the CR condition (n = 69) were taught to 1) identify their initial thought in response to an interpersonal situation (seeing a friend on the street who does not acknowledge them); 2) notice their emotions after having that thought; 3) list alternative thought responses; 4) choose an alternate thought response; and 5) identify their emotional response to the alternative thought. In the mindfulness intervention, developed from Dialectical Behavior Therapy (Linehan, 2014), participants (n = 69) learned to 1) observe their thoughts, feelings, and reactions to the same interpersonal situation as above; 2) describe their emotions and bodily sensations; 3) take a nonjudgmental and accepting position regarding their emotions; and 4) allow their emotions to come and go like waves. The attention control condition (n = 71) provided basic nutritional information and was of a similar length and style to the ER interventions. Next, participants were provided with a hypothetical situation that described a day of frustrating events and, if in an intervention condition, practiced using the skills they just learned in order to regulate their emotional responses. After practicing the skill, participants indicated the extent to which they were able to implement the ER skills (1 = Not at all to 7 = Extremely; M = 4.35, SD =1.58). There was no significant difference between intervention conditions regarding participants’ reported ability to implement the ER skills [t(135) = −1.24, p > .20].
After the skills practice, alcohol condition participants were given .816 ml ethanol per pound of body weight designed to reach a peak BrAC of .08%. Alcoholic beverages consisted of one part 100-proof vodka to three parts juice; non-alcoholic beverages consisted of one part water and three parts juice. Participants paced their consumption evenly over nine minutes and were informed as to whether they were consuming alcoholic or non-alcoholic beverages. Alcohol participants were breathalyzed every four minutes until they reached a criterion BrAC of at least .05%, at which point they began the post-beverage measures. Each no-alcohol participant was yoked to a prior alcohol participant, receiving breathalyzer tests at the same intervals as their yoked participant to in order to reduce error variance (Schacht et al., 2010).
After beverage administration, participants read and projected themselves into a sexually explicit story as the protagonist (Davis, 2010). Participants who received the intervention were instructed to use the skill they learned while reading the story. In the story, the protagonist experiences a frustrating day before heading to a party where he encounters a casual sex partner named “Kim”. The protagonist has a conversation with Kim at the party, after which they go to Kim’s apartment. They engage in consensual kissing, during which Kim states that she does not want to have sex that night. Kissing and sexual activity continues, with Kim again clearly stating that she does not want to have sexual intercourse while pushing the protagonist away, after which the story ends. Participants rated their in-the-moment emotion regulation, current levels of sexual arousal and anger, and their likelihood of using coercive tactics and having sexual intercourse with Kim. All participants were compensated $15 per hour they spent in the laboratory, and the participants who consumed alcohol stayed in the lab until their BAC was below .03%.
Measures
Past Adult Sexual Aggression (ASA) Perpetration.
During the background questionnaire session, participants completed the revised Sexual Experiences Survey (SES; Koss et al., 2007) and the Sexual Strategies Scale (SSS; Struckman-Johnson et al., 2003) to assess perpetration of sexual aggression since the age of 14. The SES assesses a range of sexually aggressive acts (nonconsensual sexual contact, attempted rape, rape) and tactics (coercion, threats, intoxication, and force). Participants indicated the number of times (0 – 3 times) that a tactic was used for each act. For the SSS, participants completed 17 items assessing whether they have ever (Yes/No) engaged in behaviors consistent with five levels of sexual aggression: sexual enticement, verbal coercion, use of older age or authority, use of intoxication, and threats or force “to have sexual activity with a woman when she did not want to”. Past research has suggested that while men may report their use of intoxication and physical force strategies consistently between the two measures, men report more verbal strategies on the SSS (Testa et al., 2015). Moreover, the items on the SES enabled participants to differentiate between the types of sexual activity obtained through each tactic. Thus, a three-level composite variable of past ASA perpetration severity based upon participants’ most severe tactic used was created from responses to both scales: Non-Perpetrators = Participants who did not endorse any tactics on either scale (19.6% of the sample); Moderate = Endorsement of having perpetrated nonconsensual sexual contact on the SES or endorsement of sexual enticement or verbal coercion on the SSS (40.2% of the sample); and Severe = Endorsement of having perpetrated attempted or completed rape regardless of tactic on the SES or endorsement of manipulation of authority, intoxication, or threats or physical force on the SSS (40.2% of the sample). Notably, despite all participants having endorsed at least one incidence of sexual aggression in their lifetime when completing the SSS via web-based eligibility survey, 19.6% of the sample denied a history of perpetration on both the SSS and SES when in the laboratory.
Emotion Regulation Skills.
After the intervention and alcohol administration, participants completed a modified version of the State-Difficulties in Emotion Regulation Scale (S-DERS; Lavender et al., 2015) to assess emotion regulation during the scenario. The S-DERS measures four facets of emotion regulation and asks participants to rate the extent to which the statements apply to their emotions in the present moment (1 = Not at all to 5 = Completely). Participants completed two items to assess each facet, and mean scores were created, with higher scores indicating better emotion regulation: emotional acceptance (“I feel embarrassed for feeling this way,” reverse-scored; α = .81), emotional awareness (“I am acknowledging my emotions,” α = .72), emotional modulation (“My emotions feel out of control,” reverse-scored; α = .85), and emotional clarity (“I am confused about how I feel,” reverse-scored; α = .68).
Anger.
Participants rated the extent (1 = Not at all to 7 = Extremely) to which they felt three anger-related emotions (irritated, angry, frustrated; α = .89) while reading the scenario (Davis, 2010).
Sexual Arousal.
Participants rated the extent (1 = Not at all to 7 = Extremely) to which they felt three sexual arousal-related emotions (horny, aroused, turned on; α = .98) while reading the scenario (Davis, 2010).
Coercive tactic intentions.
While reading the scenario, an 11-item, modified version of the revised SES assessed sexual coercion intentions within the scenario (α = .88; Koss et al., 2007). Participants indicated the likelihood (1 = Not at all likely to 7 = Extremely likely) that they would engage in a spectrum of coercive tactics to have sex with Kim after she refused. The tactics ranged from emotional (i.e., “tell Kim how upset you would be if you did not have sex”) and relationship manipulation (i.e., “promise to have a relationship with Kim so she will have sex with you”) to intoxication (i.e., “get Kim another drink so that she has sex with you.”), and threats/use of physical force (i.e., “use physical restraint or force to get Kim to have sex with you”). A mean score was computed.
Nonconsensual Sex Intentions.
During the scenario, a single item assessed intentions to have sexual intercourse with Kim despite her lack of consent. Participants indicated the likelihood (1 = Not at all likely to 7 = Extremely likely) that they would “have vaginal sex with Kim” after she refused to engage in sexual activity (Davis, 2010).
Data Analysis Plan
Beverage condition was coded (0 = no-alcohol condition; 1 = alcohol condition) and intervention condition was dummy coded with control group as the reference group. Path analysis was conducted using MPlus 8 (Muthén & Muthén, 1998–2017) using maximum likelihood estimation.1 Acceptable model fit was determined by a non-significant χ2 statistic, SRMR < .08, TLI > .95, CFI > .95, and RMSEA < .06 (West et al., 2012). Models were also compared using the Bayesian Information Criterion (BIC), in which smaller relative scores indicate improved model fit (Kass & Raftery, 1995). Significant interactions were probed at each level of beverage, intervention, and sexual aggression history severity. Because all interaction terms were comprised of categorical variables, the estimated marginal means were also examined. All possible indirect effects from beverage to nonconsensual sex intentions and from intervention to nonconsensual sex intentions were examined. Indirect effects were calculated using 10,000 bootstrap resamples (Hayes, 2013), and statistical significance was determined by a bias-corrected bootstrap 95% confidence interval that did not include zero.
Results
Three participants withdrew before beverage administration and one participant had missing data on the outcome, leaving a final sample of 205. Pearson chi-square analyses indicated that ASA severity history was comparable across groups in both beverage and intervention conditions (χ2(2) = 1.30, p = .52 and χ2(4) = 3.90, p = .42, respectively), indicating randomization was successful. Table 1 contains means, standard deviations, skewness, and correlations for all variables in the model. The pattern of bivariate associations indicated that all continuous variables except anger were significantly associated with nonconsensual sex intentions.
Table 1.
Means, Standard Deviations, and Bivariate Correlations of Model Variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Beverage Conditiona | -- | |||||||||||
| 2. CR Dummy Codeb | −.01 | -- | ||||||||||
| 3. Mindfulness Dummy Codec | −.01 | −.50** | -- | |||||||||
| 4. ASA Group | .04 | −.06 | −.06 | -- | ||||||||
| 5. Emotional Acceptance | .02 | .08 | .06 | −.01 | -- | |||||||
| 6. Emotional Awareness | .12 | −.12 | .14* | −.14* | .06 | -- | ||||||
| 7. Emotional Clarity | .−.01 | .18* | .00 | .−.07 | .47** | .27** | -- | |||||
| 8. Emotional Modulation | −.06 | .19* | −.01 | −.16* | .33** | .11 | .45** | -- | ||||
| 9. Anger | −.06 | −.06 | .00 | .11 | −.12 | −.05 | −.23** | −.12 | -- | |||
| 10. Arousal | .18* | −.12 | .03 | .34** | −.05 | −.10 | −.09 | −.33** | .08 | -- | ||
| 11. Coercive Tactic Intentions | .17* | −.10 | .03 | .27** | −.16* | −.12 | .16* | −.45** | .18* | .47** | -- | |
| 12. Nonconsensual Sex Intentions | .13+ | −.13 | −.02 | .20** | −.23** | −.18* | −.15* | −.42** | −.03 | 52** | .68** | -- |
| Mean | N/A | N/A | N/A | N/A | 4.48 | 3.84 | 4.44 | 4.52 | 2.58 | 3.30 | 1.39 | 1.99 |
| SD (Skewness) | N/A | N/A | N/A | N/A | .82 (−1.93) | .99 (−.76) | .76 (−1.46) | .80 (−2.03) | 1.55 (.87) | 2.13 (.44) | .71 (2.65) | 1.57 (1.69) |
1 = intoxicated; 0 = sober;
1 = cognitive restructuring = 1; 0 = control;
1 = mindfulness; 0 = control
p < .07
p < .05
p < .01
Model Fit
The hypothesized model (Figure 1) fit the data well. Non-significant interactions were dropped from the model, and the model was rerun. This final model (Figure 2) was an excellent fit for the data, χ2(41) = 29.94, p = .90, SRMR = .02, TLI = 1.00, CFI = 1.00, and RMSEA = .00 (95% CI: .00, .02), and BIC reflected a better fitting model compared to the hypothesized model. Model variables accounted for 58.5% of the variance of nonconsensual sex intentions (R2 = .585, p < .001), 45.0% of the variance of coercive tactic intentions (R2 = .450, p < .001), 25.4% of the variance of sexual arousal (R2 = .254, p < .001), 6.6% of the variance of anger (R2 = .066, p < .05), 7.0% of the variance of emotional modulation (R2 = .070, p < .05), and 10.8% of the variance of emotional acceptance (R2 = .108, p < .05). The model did not account for a significant amount of variance of any other variables. Figure 2 depicts the final model with standardized path coefficients.
Figure 2:
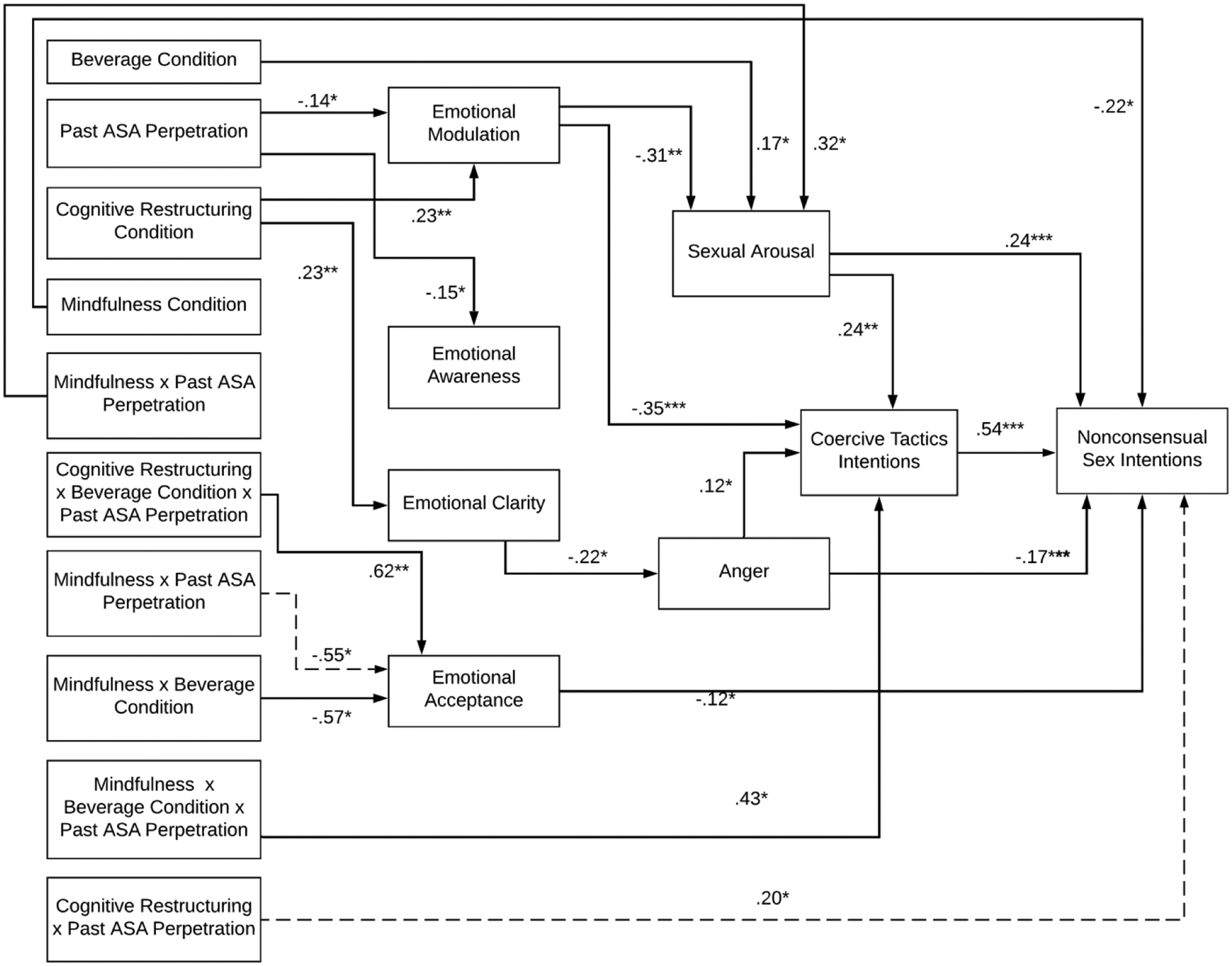
Final Model
* p < .05 ** p < .01 *** p < .001
Note: Only relations meeting statistical significance and not subsumed by two- or three-way interactions are depicted in the final model. Significant interactions with no significant differences in estimated marginal means are depicted in the figure by dashed lines.
Beverage main effects.
There were two significant indirect paths between beverage condition and nonconsensual sex intentions via sexual arousal. Intoxicated men reported greater sexual arousal than sober men, which was in turn associated with stronger nonconsensual sex intentions [ß = .04, 95% CI: (.01, .08)]. The full path from beverage condition to nonconsensual sex intentions via sexual arousal and coercive tactic intentions was also significant [ß = .02, 95% CI: (.01, .05)].
Intervention main effects.
There was a significant positive effect of the CR intervention condition relative to control on the emotional modulation and emotional clarity subscales. There were two significant indirect paths from the CR intervention condition to nonconsensual sex intentions via emotional modulation. Specifically, those who received the CR intervention relative to control reported stronger emotional modulation, which in turn was associated with lower sexual arousal, which was associated with lower nonconsensual sex intentions [ß = −.02, 95% CI: (−.03, −.01)]. The second indirect association followed a similar path, with stronger emotion modulation predicting lower intentions to use coercive tactics, which was associated with lower nonconsensual sex intentions for those who received the CR intervention relative to control [ß = −.04, 95% CI: (−.08, −.01)]. Relative to control, the CR intervention resulted in greater emotional clarity which then predicted lower anger, and anger was subsequently positively associated with coercive tactics intentions and negatively associated with nonconsensual sex intentions; however this indirect pathway was not significant. Finally, receiving the mindfulness intervention resulted in lower nonconsensual sex intentions compared to control.
Perpetration main effects.
ASA perpetration severity was negatively associated with emotional awareness and emotional modulation. There was a significant indirect effect from past ASA perpetration severity to nonconsensual sex intentions via emotional modulation and coercive tactics. That is, men who reported a more severe ASA perpetration history reported less emotional modulation, which was associated with greater intentions to use coercive tactics, which in turn predicted nonconsensual sex intentions [ß = .03, 95% CI: (.01, .05)].
Moderated effects.
There were several significant interactions in the final model. Regarding the CR intervention, there was a three-way interaction between beverage condition, CR intervention, and past ASA perpetration on emotional acceptance. For sober men who had low or moderate ASA histories, those in the CR intervention condition reported greater emotional acceptance than those in the control condition [t(199) = 2.69, p < .01; MCR/Sober/Low = 4.68, vs. MCon/Sober/Low = 3.45]. For intoxicated men and men with high ASA histories, there were no differences. Greater emotional acceptance was in turn associated with lower nonconsensual sex intentions. Additionally, there was a significant two-way interaction between CR intervention and past ASA on nonconsensual sex intentions; for men with low or moderate ASA histories, those who received the CR intervention reported lower nonconsensual sex intentions than those in the control condition. While the simple slope analyses were significant [t(199) = −2.53, p < .05; t(199) = −2.04, p < .05], examination of marginal means indicated no significant mean differences.
For the mindfulness intervention, there was a two-way interaction between mindfulness condition and past ASA on sexual arousal; men in the mindfulness condition with high ASA histories reported greater sexual arousal than men with moderate or low ASA histories [t(199) = 5.49, p < .001; MMind/High = 4.75 vs. MMind/Mod = 2.97 vs. MMind/Low = 1.82). Second, there was also a two-way interaction between the mindfulness intervention and beverage condition such that sober men who received the mindfulness intervention reported more emotional acceptance than sober men in the attention control condition [t(199) = 3.02, p < .01; MMind/Sober = 4.70 vs. MCon/Sober = 4.20], with no significant difference between intoxicated men (MMind/Intox = 4.43 vs. MCon/Intox = 4.48). Third, there was a significant three-way interaction between mindfulness, beverage condition, and ASA on coercive tactic intentions, such that intoxicated men with high ASA histories reported stronger coercive tactic intentions if they had received the mindfulness condition relative to control condition (t(199) = 4.22, p < .001; MMind/Intox/High = 2.58 vs. MCon/Intox/High = 1.83). Finally, there was a two-way interaction between mindfulness intervention and ASA history such that for those with low or moderate ASA histories, the mindfulness intervention was associated with greater emotional acceptance; however, examination of the marginal means suggested that these differences were not significantly different than men with high ASA histories who received the mindfulness intervention.
Exploratory Analyses: CR compared to Mindfulness
Exploratory analyses were conducted to compare the effects of the CR intervention to the mindfulness intervention within the final model shown in Figure 2. Dummy codes were re-computed with CR serving as the reference group (e.g., mindfulness vs. CR; control vs. CR). The final model was rerun, using the same procedures as above. The magnitude, direction, and significance of all associations between ER skills, anger, arousal, coercive tactic intentions, and nonconsensual sex intentions were the same as in the final model.
Intervention main effects.
Men who received the mindfulness condition reported greater emotional awareness than men who received the CR condition (ß = .17, p < .05), whereas men who received the mindfulness condition reported less emotional modulation than men who received the CR condition, although this difference was not significant (ß = −.13, p = .055).
Moderated effects.
There was a significant three-way interaction between mindfulness, ASA perpetration, and beverage condition on coercive tactic intentions (ß = .54, p < .01). For intoxicated men with high levels of past ASA perpetration, those who received the mindfulness condition reported higher intentions to engage in coercive tactics relative to those who received the CR intervention [t(199) = 4.31, p < .001); MMind/Intox/High = 2.58, MCR/Intox/High = 1.39]. Notably, the mean coercive tactic intentions reported by intoxicated men with high ASA perpetration histories who received the mindfulness condition was significantly higher than those reported by any other group (Range: 1.03 to 1.68). The moderated indirect effect was also significant; for intoxicated men with high past ASA perpetration, those who received the mindfulness intervention reported greater coercive tactic intentions and subsequently greater nonconsensual sex intentions relative to those who received the CR intervention [ß = .29 (95% CI: .04, .53)]. Similar to findings comparing mindfulness to control, there was a significant two-way interaction between mindfulness and past ASA severity on sexual arousal (ß = .28, p < .05), such that there was a positive association between past ASA severity and sexual arousal only for men who received the mindfulness intervention [t(199) = 3.45, p < .001].
Discussion
The present study addresses a critical need for brief evidence-based interventions targeting the reduction of sexual aggression. Evidence from behavioral science has demonstrated that deficiencies in ER may serve as an underlying mechanism for sexually aggressive behavior (Picket et al., 2016). Thus, we employed an experimental medicine approach to behavior change (Neilsen et al., 2018) to test the efficacy of two ER-focused interventions for reducing alcohol-involved sexual aggression intentions using a proximal change experiment approach that enabled testing intervention efficacy during both sober and intoxicated states. Many of the hypotheses were supported, although some unexpected findings emerged. Overall, results demonstrate that ER is a malleable intervention target that holds promise for reducing sexually aggressive behavior. Importantly, because proximal intervention effects varied by states of intoxication versus sobriety, our findings highlight the necessity of considering state-related factors when intervening in behaviors that occur during “hot” states (Yang et al., 2012).
Our findings demonstrate that emotional modulation is a critical mechanism underlying sexual aggression intentions, and that ER-focused CR interventions may be an effective means of improving emotion modulation skills, resulting in decreases in sexual aggression. As predicted, participants in the CR intervention condition demonstrated improved emotional modulation relative to participants in the attention control condition, resulting in decreased nonconsensual sex intentions through lower intentions to engage in sexual coercion. Moreover, a key piece of emotional modulation’s effectiveness in reducing sexual aggression may lie in its association with lower feelings of sexual arousal which predicted lower coercive tactic intentions and nonconsensual sex intentions. Notably, alcohol intoxication was predictive of stronger sexual arousal, which in turn was associated with greater coercive tactic and nonconsensual sex intentions. Considered together, these results demonstrate that sexual arousal-related emotion is not only a key predictor of engagement in sexual coercion and aggression but also that it is an important intervention target, particularly for men who drink before sexual situations. Further, because men with more severe past sexual aggression histories reported difficulty modulating their emotions in the moment, they may benefit from targeted ER-focused CR interventions. Our results indicate that CR interventions are a promising tool for reducing feelings of sexual arousal during nonconsensual sexual situations through increased emotional modulation; future larger scale trials could assess the effectiveness of targeting CR interventions focused on emotional modulation towards men at higher risk of committing alcohol-involved sexual aggression.
The CR intervention also resulted in greater emotional clarity relative to control. Emotional clarity was associated with reduced feelings of anger, which in turn was positively associated with intentions to use coercive tactics and negatively associated with nonconsensual sex intentions. Given these contradictory associations, the possible role of anger in sexual aggression situations needs further research. That noted, our results suggest that if in-the-moment feelings of anger are indeed associated with increases in sexual coercion, CR interventions that improve emotional clarity may be of benefit.
Emotional acceptance may also be a key mechanism for reducing sexual aggression. The CR intervention was associated with greater emotional acceptance, however this was only observed for sober men with less severe sexual aggression histories. Similarly, the mindfulness intervention resulted in greater emotional acceptance relative to control, but only for sober men regardless of their sexual aggression histories. Greater emotional acceptance then predicted lower nonconsensual sex intentions. This pattern of findings suggests that both CR and mindfulness interventions targeting emotional acceptance may work particularly well for men with lower distal (i.e., less aggressive history) and proximal (i.e., sober) risk factors for sexual aggression perpetration. These results are consistent with findings from prior investigations of sexual assault interventions (e.g., Stephens & George, 2009) demonstrating greater intervention efficacy with men at lower risk of sexual assault perpetration. As such, it would behoove continued research in this area to develop and test interventions that target and tailor their approaches to individual sexual assault risk levels, with an emphasis on those at greatest risk of future perpetration.
The finding that the mindfulness intervention resulted in greater emotional acceptance for sober men, coupled with its direct effect of reducing nonconsensual sex intentions relative to control, indicates that mindfulness approaches may have some utility in reducing sexual aggression. However, the overall pattern of results suggests caution regarding the use of brief, ER-focused, mindfulness interventions with men who have more severe perpetration histories. First, men with more severe perpetration histories who received the mindfulness intervention reported greater sexual arousal relative to men with low or moderate perpetration severity, which was in turn associated with stronger coercive and nonconsensual sex intentions. Notably, the association between perpetration severity and sexual arousal was significant among men who received the mindfulness condition, however such a relationship was not observed among those who received the CR condition. Second, among intoxicated men with the most severe perpetration histories, those who received the mindfulness intervention reported stronger intentions to use coercive tactics relative to the control and the CR groups. These findings may reflect the focus on nonjudgmental acceptance of emotions in our mindfulness intervention in contrast to the focus on modifying emotions via alternative thoughts in our CR intervention. That is, participants in the mindfulness condition were instructed to become aware of their feelings and then experience them without modification or judgment, consistent with typical mindfulness-based approaches (Gillespie et al., 2012). The mindfulness intervention did indeed result in greater emotional awareness relative to CR overall and greater emotional acceptance relative to control among sober participants. However, because sexually aggressive men demonstrate greater sexual arousal in response to nonconsensual sexual stimuli relative to other men (Bernat et al., 1999), the mindfulness intervention may have inadvertently succeeded in teaching these men to allow and accept such feelings. While this may reduce any potential emotional distress in response to these feelings, it may also unintentionally increase their intentions to obtain sexual intercourse despite the woman’s lack of consent. Such findings demonstrate the negative potential outcomes of mindfulness approaches that do not include explicit ethical components in their instruction (Monteiro et al., 2015). Although there is debate regarding the most appropriate and effective ways to include a consideration of ethics into mindfulness interventions (Baer, 2015), mindfulness approaches that incorporate self-identified prosocial values (e.g., Acceptance and Commitment Therapy Hayes et al., 2012) may be useful to consider, particularly when working with men with more severe perpetration histories.
Strengths, Limitations, and Conclusions
The strengths of this study also highlight its limitations. We recruited heavy episodic drinkers in order to obtain a sample at greater risk of alcohol-involved sexual aggression; however, findings may not generalize to lighter drinkers. Additionally, all participants reported a sexual aggression history during eligibility screening; however, a minority of participants denied a history of sexual aggression during data collection. Other studies have also demonstrated suboptimal test-retest reliability in sexual aggression measures (e.g., Anderson et al., 2017), indicating a need for further research. While our lab-based alcohol administration procedures enabled rigorous testing of ER mechanisms and causal attributions for alcohol intoxication and intervention effects, they preclude our ability to test our hypotheses in real-world conditions that may include higher levels of alcohol consumption and different sexual/relationship contexts. Finally, the use of a proximal change experimental approach allowed us to test intervention effects on the targeted mechanism of ER. However, outcomes could only include behavioral intentions rather than actual behavior. Given these limitations and the promising findings, next steps in this line of research include expansion to a randomized controlled trial that tests intervention effects on real-world alcohol-involved sexually aggressive behavior across a more diverse sample (e.g., lighter drinkers, men with specific ER difficulties).
Through an experimental medicine approach to behavior change, this study sought to translate findings from behavioral research regarding the role of emotions and emotion regulation in alcohol-involved sexual aggression into interventions designed to target these mechanisms with an eye toward reducing such behavior. This research conforms to SOBC principles by demonstrating target engagement and validity and advances the field by assessing intervention efficacy during behavior-relevant states. This study bridges the gap between lab-based behavioral science and applied behavior change intervention research, serving as a first step towards creating effective, mechanisms-focused, evidence-based approaches to reduce alcohol-involved sexual aggression.
Acknowledgments
Funding (R21AA023811) was provided by the National Institute on Alcohol Abuse and Alcoholism to the first author.
Footnotes
Path analysis was originally conducted using maximum likelihood estimation with robust standard errors (MLR), which is a preferable estimation method when an outcome variable is skewed. MPlus 8 does not allow for the use of MLR concurrently with bootstrap resampling. Analyses were run with a model using MLR and bootstrap resamples. The coefficients for both models were similar, with the model using bootstrap resampling resulting in more conservative p-values and 95% confidence intervals for all estimates. Thus the models using bootstrap resamples was selected.
References
- Abbey A, Parkhill MR, Jacques-Tiura AJ, & Saenz C (2009). Alcohol’s role in men’s use of coercion to obtain unprotected sex. Substance Use & Misuse, 44, 1329–1348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson RE, Cahill SP, & Delahanty DL (2017). Initial evidence for the reliability and validity of the Sexual Experiences Survey-Short Form Perpetration (SES-SFP) in college men. Journal of Aggression, Maltreatment & Trauma, 26(6), 626–643. [Google Scholar]
- Ariely D, & Loewenstein G (2006). The heat of the moment: The effect of sexual arousal on sexual decision making. Journal of Behavioral Decision Making, 19, 87–98. [Google Scholar]
- Babcock JC, Graham K, Canady B, & Ross JM (2011). A proximal change experiment testing two communication exercises with intimate partner violent men. Behavior Therapy, 42, 336–347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baer R (2015). Ethics, values, virtues, and character strengths in mindfulness-based interventions: A psychological science perspective. Mindfulness, 6(4), 956–969. [Google Scholar]
- Berking M, Wupperman P, Reichardt A, Pejic T, Dippel A, & Znoj H (2008). Emotion-regulation skills as a treatment target in psychotherapy. Behaviour Research and Therapy, 46, 1230–1237. [DOI] [PubMed] [Google Scholar]
- Bernat JA, Calhoun KS, & Adams HE (1999). Sexually aggressive and nonaggressive men: Sexual arousal and judgments in response to acquaintance rape and consensual analogues. Journal of Abnormal Psychology, 108(4), 662–673. [DOI] [PubMed] [Google Scholar]
- Both S, Laan E, & Everaerd W (2011). Focusing “hot” or focusing “cool”: Attentional mechanisms in sexual arousal in men and women. The Journal of Sexual Medicine, 8, 167–179. [DOI] [PubMed] [Google Scholar]
- Cloitre M, Koenen KC, Cohen LR, & Han H (2002). Skills training in affective and interpersonal regulation followed by exposure: A phase-based treatment for PTSD related to childhood abuse. Journal of Consulting and Clinical Psychology, 70(5), 1067–1074. [DOI] [PubMed] [Google Scholar]
- Davis KC (2010). The influence of alcohol expectancies and intoxication on men’s aggressive unprotected sexual intentions. Experimental & Clinical Psychopharmacology, 18, 418–428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeGue S, Valle LA, Holt MK, Massetti GM, Matjasko JL, & Tharp AT (2014). A systematic review of primary prevention strategies for sexual violence perpetration. Aggression and Violent Behavior, 19, 346–362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eckhardt CI (2007). Effects of alcohol intoxication on anger experience and expression among partner assaultive men. Journal of Consulting and Clinical Psychology, 75, 61–71. [DOI] [PubMed] [Google Scholar]
- Ellis A (2008). Cognitive restructuring of the disputing of irrational beliefs. In O’Donohue WT & Fisher JE (Eds.), Cognitive Behavior Therapy: Applying Empirically Supported Techniques in your Practice (2nd ed., pp. 91–95). Hoboken, NJ: Wiley. [Google Scholar]
- Gallagher KE, Hudepohl AD, & Parrott DJ (2010). Power of being present: The role of mindfulness on the relation between men’s alcohol use and sexual aggression toward intimate partners. Aggressive Behavior, 36, 405–413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- George WH, Davis KC, Norris J, Heiman JR, Schacht RL, Stoner SA, & Kajumulo KF (2006). Alcohol and erectile response: The effects of high dosage in the context of demands to maximize sexual arousal. Experimental and Clinical Psychopharmacology, 14, 461–470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giancola PR, Josephs RA, Dewall CN, & Gunn RL (2009). Applying the attention-allocation model to the explanation of alcohol-related aggression: Implications for prevention. Substance Use & Misuse, 44(9–10), 1263–1279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillespie SM, Mitchell IJ, Fisher D, & Beech AR (2012). Treating disturbed emotional regulation in sexual offenders: The potential applications of mindful self-regulation and controlled breathing techniques. Aggression and Violent Behavior, 17, 333–343. [Google Scholar]
- Gottman J, Ryan K, Swanson C, & Swanson K (2005). Proximal change experiments with couples: A methodology for empirically building a science of effective interventions for changing couples’ interaction. The Journal of Family Communication, 5, 163–190. [Google Scholar]
- Gratz KL & Tull MT (2010). Emotion regulation as a mechanism of change in acceptance- and mindfulness-based treatments. In Baer RA (Ed.), Assessing Mindfulness & Acceptance Processes in Clients (pp. 107–133), Oakland, CA: New Harbinger Publications. [Google Scholar]
- Hayes AF (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Retrieved from http://www.eblib.com
- Hayes SC, Strosahl KD, & Wilson KG (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (2nd ed.). New York. NY: Guilford. [Google Scholar]
- Kass RE, & Raftery AE (1995). Bayes factors. Journal of the American Statistical Association, 90(430), 773–795. [Google Scholar]
- Kazdin AE, & Nock MK (2003). Delineating mechanisms of change in child and adolescent therapy: methodological issues and research recommendations. Journal of Child Psychology and Psychiatry, 44, 1116–1129 [DOI] [PubMed] [Google Scholar]
- Kirwan M, Lanni DJ, Warnke A, Pickett SM, Parkhill MR (2019). Emotion regulation moderates the relationship between alcohol consumption and the perpetration of sexual aggression. Violence Against Women, 25(9), 1053–1073. [DOI] [PubMed] [Google Scholar]
- Koss MP, Abbey A, Campbell R, Cook S, Norris J, Testa M, & White J (2007). Revising the SES: A collaborative process to improve assessment of sexual aggression and victimization. Psychology of Women Quarterly, 31(4), 357–370. [Google Scholar]
- Lavender JM, Tull MT, DiLillo D, Messman-Moore T, & Gratz KL (2015). Development and validation of a state-based measure of emotion dysregulation: The state difficulties in emotion regulation scale. Assessment, 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Linehan MM (2014). DBT Skills Training Manual. Guilford Publications. [Google Scholar]
- Linehan MM, Bohus M, & Lynch TR (2007). Dialectical behavior therapy for pervasive emotion dysregulation. In Gross J (Ed.), Handbook of Emotion Regulation (pp. 581–605). New York, NY: Guilford Press. [Google Scholar]
- Logan-Greene P, & Davis KC (2011). Latent profiles of risk among a community sample of men: Implications for sexual aggression. Journal of Interpersonal Violence, 26, 1463–1477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lyn TS, & Burton DL (2005). Attachment, anger and anxiety of male sexual offenders. Journal of Sexual Aggression, 11(2), 127–137. [Google Scholar]
- Monteiro LM, Musten RF, & Compson J (2015). Traditional and contemporary mindfulness: finding the middle path in the tangle of concerns. Mindfulness, 6(1), 1–13. [Google Scholar]
- Moses EB, & Barlow DH (2006). A new unified treatment approach for emotional disorders based on emotion science. Current Directions in Psychological Science, 15(3), 146–150. [Google Scholar]
- Muthén LK, & Muthén BO (1998–2017). Mplus Users guide, Eighth Edition. Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism. (2005). Recommended Council Guidelines on Ethyl Alcohol Administration in Human Experimentation. Retrieved on November 4, 2014 from http://www.niaaa.nih.gov/research/guidelines-and-resources/administering-alcohol-human-studies.
- Nielsen L, Riddle M, King JW, Aklin WM, Chen W, Clark D, … & Green P (2018). The NIH Science of Behavior Change Program: Transforming the science through a focus on mechanisms of change. Behaviour Research and Therapy, 101, 3–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parrott DJ & Giancola PR (2004). A further examination of the relation between trait anger and alcohol-related aggression: The role of anger control. Alcoholism: Clinical and Experimental Research, 28(6), 855–864. [DOI] [PubMed] [Google Scholar]
- Pickett S,M, Parkhill M,R, & Kirwan M (2016). The influence of sexual aggression perpetration history and emotion regulation on men’s aggressive responding following social stress. Psychology of Men and Masculinity, 17(4), 363–372. [Google Scholar]
- Pond RS, Kashdan TB, DeWall CN, Savostyanova A, Lambert NM, & Fincham FD (2012). Emotion differentiation moderates aggressive tendencies in angry people: A daily diary analysis. Emotion, 12(2), 326–337. [DOI] [PubMed] [Google Scholar]
- Pokorny AD, Miller BA, & Kaplan HB (1972). The brief MAST: A shortened version of the Michigan Alcoholism Screening Test. American Journal of Psychiatry, 129, 342–345. [DOI] [PubMed] [Google Scholar]
- Salazar LF, Vivolo-Kantor A, Hardin J, & Berkowitz A (2014). A web-based sexual violence bystander intervention for male college students: Randomized controlled trial. Journal of Medical Internet Research, 16(9), e203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schacht RL, Stoner SA, George WH, & Norris J (2010). Idiographically determined versus standard absorption periods in alcohol administration studies. Alcoholism: Clinical and Experimental Research, 34(5), 925–927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shafir R, Zucker L, & Sheppes G (2018). Turning off hot feelings: Down-regulation of sexual desire using distraction and situation-focused reappraisal. Biological Psychology, 137, 116–124. [DOI] [PubMed] [Google Scholar]
- Smith SG, Chen J, Basile KC, Gilbert LK, Merrick MT, Patel N, Walling M, & Jain A (2017). The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 – 2012 State Report. Atlanta, GA: Centers for Disease Control and Prevention. [Google Scholar]
- Stappenbeck CA, & Fromme K (2014). The effects of alcohol, emotion regulation, and emotional arousal on the aggression intentions of dating men and women. Psychology of Addictive Behaviors, 28, 10–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stappenbeck CA, Luterek JA, Kaysen D, Rosenthal CF, Gurrad B, & Simpson TL (2015). A controlled examination of two coping skills for daily alcohol use and PTSD symptom severity among dually diagnosed individuals. Behaviour Research and Therapy, 66, 8–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stephens KA, & George WH (2009). Rape prevention with college men: Evaluating risk status. Journal of Interpersonal Violence, 24(6), 996–1013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stinson JD & Becker JV (2013.) Treating Sex Offenders: An Evidence-Based Manual. New York, NY: Guilford Press. [Google Scholar]
- Struckman-Johnson C, Struckman-Johnson D, & Anderson PB (2003). Tactics of sexual coercion: When men and women won’t take no for an answer. Journal of Sex Research, 40, 76–86. [DOI] [PubMed] [Google Scholar]
- Tager D, Good GE, & Brammer S (2010). “Walking over ‘em”: An exploration of relations between emotion dysregulation, masculine norms, and intimate partner abuse in a clinical sample of men. Psychology of Men & Masculinity, 11(3), 233–239. [Google Scholar]
- Testa M (2002). The impact of men’s alcohol consumption on perpetration of sexual aggression. Clinical Psychology Review, 22(8), 1239–1263. [DOI] [PubMed] [Google Scholar]
- Testa M, Hoffman JH, Lucke JF, & Pagnan CE (2005). Measuring sexual aggression perpetration in college men: A comparison of two measures. Psychology of Violence, 5, 285–293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ward T & Beech A (2006). An integrated theory of sexual offending. Aggression and Violent Behavior, 11, 44–63. [Google Scholar]
- West SG, Taylor AB, Wu W (2012). Model fit and model selection in structural equation modeling. In Hoyle RH (Ed.), Handbook of Structural Equation Modeling (pp. 209–231). New York, NY: Guilford Press. [Google Scholar]
- Winters J, Christoff K, & Gorzalka BB (2009). Conscious regulation of sexual arousal in men. Journal of Sex Research, 46(4), 330–343. [DOI] [PubMed] [Google Scholar]
- Yang H, Carmon Z, Kahn B, Malani A, Schwartz J, Volpp K, & Wansink B (2012). The hot–cold decision triangle: A framework for healthier choices. Marketing Letters, 23, 457–472. [Google Scholar]