

Abstract
This study examines the independent, relative, and additive associations between both parent and peer role models and longitudinal patterns of smoking across adolescence and early adulthood. An analysis of data from the National Longitudinal Study of Adolescent to Adult Health (N=10,166) reveals at least four distinct trajectories of smoking across ages 13–35: (1) non-smokers; (2) late peak (almost 10 cigarettes per day around age 30); (3) an early peak group that reached roughly 10 cigarettes per day around age 20 and declined; and (4) a high group that increased during adolescence and early adulthood and then remained high. Parent and peer smoking behaviors were associated with trajectory group membership net of controls for sociodemographic characteristics, parental SES, parent-child relations, and the availability of cigarettes in the family home. Parents and peers appear to have at least some independent associations net of each other, but their combined effects are powerful.
Keywords: Family, Friends, Socialization, Substance Abuse, Add Health, Longitudinal
INTRODUCTION
Cigarette smoking continues to be an important public health concern in the United States (US Department of Health and Human Services, 2014). There are many factors influencing the likelihood that an individual will engage in smoking behaviors. A life course perspective suggests that individual lives are embedded in social contexts, and that human development is a lifelong process (Brook, Brook, Gordon, Whiteman, & Cohen, 1990; Elder, 2008; Sudhinaraset, Wigglesworth, & Takeuchi, 2016). When applied to cigarette use, this suggests that smoking habits arise, in part, from social conditions starting early in life (Audrain-McGovern et al., 2004; Bernat, Erickson, Widome, Perry, & Forster, 2008; Mays et al., 2014). Therefore, identifying early-life factors that are associated with smoking among adolescents and young adults may help prevent premature mortality and health problems throughout the life course (Danaei et al., 2009).
Both parent and peer smoking behaviors are associated with smoking among adolescents and those in early adulthood, and these shape tobacco use patterns through a variety of mechanisms (Fuemmeler et al., 2013; Vitaro, Wanner, Brendgen, Gosselin, & Gendreau, 2004). A simple explanation is that children and adolescents obtain cigarettes from family and friends (Meyers, Delucchi, & Halpern-Felsher, 2017; Widome, Forster, Hannan, & Perry, 2007). However, individuals often observe and imitate the behavior of those around them, and research indicates that modeling of smoking is common (Akers, 1985; Akers & Lee, 1996). Associating with individuals who smoke makes it a more normative practice, and these processes may be even more powerful when positive and negative reinforcement is involved, such as encouragement, coercion, teasing, and punishment (Flay et al., 1994; Harakeh, Scholte, Vermulst, de Vries, & Engels, 2004; Simons-Morton, Chen, Abroms, & Haynie, 2004; Simons-Morton, Haynie, Crump, Eitel, & Saylor, 2001). Additionally, people tend toward homogeneity in social settings. Individuals commonly conform to the norms and expectations of social groups so they can fit in and feel accepted, and this almost certainly applies to smoking habits (Alexander, Allen, Crawford, & McCormick, 1999; Arnett, 2007; Baumeister, 1990; Kobus, 2003). Despite progress in understanding these phenomena, there are still gaps in the literature.
First, relatively few studies in this area have used latent group-based trajectory models, in which clusters of individuals who follow similar pathways of smoking across adolescence and early adulthood are identified (Abroms, Simons-Morton, Haynie, & Chen, 2005; Audrain-McGovern et al., 2004; Bernat et al., 2008; Chassin, Curran, Presson, Sherman, & Wirth, 2009; Karp, O’loughlin, Paradis, Hanley, & Difranza, 2005; Mays et al., 2014; Orlando, Tucker, Ellickson, & Klein, 2004; Riggs, Chou, Li, & Pentz, 2007; White, Pandina, & Chen, 2002). Only three studies have analyzed nationally-representative data (Costello, Dierker, Jones, & Rose, 2008; Fuemmeler et al., 2013; Pollard, Tucker, Green, Kennedy, & Go, 2010). This work broadly suggests there are several possible trajectories of smoking across time (e.g., non-smokers, light smokers, early-life users who eventually reduce their smoking habits, late users who smoke more over time, a group that starts in adolescence and continues smoking in adulthood, etc.). While informative, this relative dearth of research makes it challenging to draw firm conclusions at this time.
Second, even though research has simultaneously examined the roles of both parents and peers (Allen, Donohue, Griffin, Ryan, & Turner, 2003; Geckova, Stewart, van Dijk, Orosova, Groothoff, & Post, 2005; Vitaro et al., 2004), only a few studies have done so using a group-based trajectory approach (Abroms et al., 2005; Bernat et al., 2008; Fuemmeler et al., 2013; Orlando et al., 2004; Pollard et al., 2010; White, Pandina, & Chen, 2002). No published research to date has examined how parent and peer role models might work together to shape trajectories of smoking, so we do not know: (a) whether they have independent associations (net of each other) on different trajectories of smoking; (b) if one is more important relative to the other; and (c) whether they combine in an additive manner (where both parents and peers smoke). Research using techniques other than the group-based approach employed here suggests that peers may be relatively more important than parents (Flay et al., 1994; Simons-Morton et al., 2004; 2001; Vitaro et al., 2004). Examining this possibility using group-based models will provide information on the characteristics of individuals who follow different trajectories of smoking across adolescence and adulthood.
Third, we do not fully understand why parent and peer smoking behaviors are associated with the tobacco consumption patterns of adolescents and early adults. Having parents and friends who smoke could simply make cigarettes readily available (Meyers et al., 2017; Widome et al., 2007), but attitudes about smoking, knowledge of cigarettes, and social sanctions may be important as well (Arnett, 2007; Flay et al., 1994; Harakeh et al., 2004; Simons-Morton et al., 2001, Simons-Morton et al., 2004). Simultaneously examining the roles of both parent and peer role models while controlling for the availability of cigarettes during adolescence may help address these issues. Also, analyzing the independent and additive effects of both parents and peers may shed light on the social and cultural aspects of smoking habits. If the combined effects of having both parents and peers who smoke is larger than having one or the other (controlling for access), this could suggest that having multiple role models in one’s life that smoke makes it more normative to do so, thus increasing the likelihood of smoking.
To summarize, this study uses group-based trajectory models to identify unique longitudinal pathways of smoking across adolescence and early adulthood using nationally-representative data. It then links parent and peer smoking behaviors to these trajectories. This is the first study to examine the relative importance of parents versus peers, and whether having both parents and peers who smoke makes it more likely that individuals will follow trajectories of increased smoking. It also sheds light on the mechanisms that link parent and peer behaviors to smoking by examining access to cigarettes and the role of normative processes including multiple role models for smoking.
METHODS
Data
Data come from the National Longitudinal Study of Adolescent to Adult Health (Add Health), a nationally-representative, probability-based survey of American adolescents who were in grades 7 to 12 during the 1994–1995 school year. The baseline sample was drawn from 80 high schools selected from a national random sample with probabilities proportional to size, and an additional 52 feeder middle schools. The overall response rate among schools was 79 percent. Over 90,000 students completed in-school surveys in 1994–1995 and 20,745 of these 7th-12th graders were interviewed at Wave I, of which 12,118 formed a “core” nationally-representative sample. Additional respondents comprised strategic oversamples of minority racial/ethnic groups. In addition to Wave I, two subsequent waves of data collected in 2001–2002 and 2007–2008 were used in this analysis. Further methodological details for Add Health can be found elsewhere (Resnick et al., 1997).
Cases were lost for several reasons. First, respondents who did not answer the smoking question at all three time points were dropped. Second, those missing sampling weights were removed (14,800 had weights - for more information on why some cases do not have weights see http://www.cpc.unc.edu/projects/addhealth/faqs/aboutdata/). Third, respondents who were age 12 at the time of Wave 1 or 36 at the time of Wave 4 were removed since they were too few in number to be considered representative of their age groups in the age-based design (see analytic strategy). Finally, those missing data on gender or race were removed. Additional missing data on independent and control variables accounted for the loss of a further 14.4% of cases (N=1,468), which were multiply imputed after data were identified as missing at random (MAR) (Acock, 2005; Sterne et al., 2009). This resulted in a final analytic sample of 10,166, with results based on 20 imputed datasets (Schafer, 1999). Findings were comparable to a listwise deletion strategy as well as the use of five imputed datasets (Royston, 2004).
Measures
Dependent Variable
Number of cigarettes smoked daily was measured with the following question: “During the past 30 days, on the days you smoked, how many cigarettes did you smoke each day?” Extreme outliers above 30 were recoded to 30, but the results were substantively the same when these individuals were recoded to the mean or dropped from the analysis, so this did not appear to bias the results. Alternative coding schemes, including measuring the average number of cigarettes smoked per day (Costello et al., 2008; Pollard et al., 2010), produced similar results.
Independent Variables
Parents ever smoked cigarettes was measured with the following questions: (a) “Has your residential mother figure (i.e., mother, adoptive mother, stepmother, foster mother, etc.) ever smoked cigarettes?” and (b) “Has your residential father figure (i.e., father, adoptive father, stepfather, foster father, etc.) ever smoked cigarettes?” Both questions were coded 0=no and 1=yes. Two variables were created from these items: (a) having any mother / father figure who ever smoked cigarettes (coded 0=no parent figure who ever smoked, 1=at least one smoked at some point); and (b) the number of mother / father figures who ever smoked cigarettes (coded 0=neither smoked, 1=at least one smoked, and 2=both smoked). Preliminary analyses showed that having any parent who ever smoked compared with none explained just as much variation in the dependent variable as the count measure, so it was used in all analyses. One residential parent was also asked (0=no and 1=yes): “Do you smoke?” The findings were comparable when this measure was used, so results are only reported for the measure that included information on the smoking habits of both residential parents.
Peer cigarette smoking was measured with the following question: “Of your three best friends, how many smoke at least 1 cigarette a day?” Response categories ranged from 0=no friends to 3=three friends. The key distinction for the dependent variable was having any friends who smoke not necessarily the number of friends who smoke, so a dichotomous variable indicating those who have at least one friend who smokes (coded 1) was compared with having no friends who smoke (coded 0) was used in all analyses.
To examine the independent, relative, and additive effects of parent and peer role models for smoking, a four-category variable was created: (a) having neither parents nor peers who smoke (the reference category); (b) having parents who smoke but peers who do not; (c) having parents who do not smoke but peers who do; and (d) having both parents and peers who smoke.
Control Variables
Sociodemographic control variables included: gender (female=1); race / ethnicity (dummy system for black, Hispanic, Asian, Native American, and other compared with whites); and urbanicity (e.g., living in a rural town, farm, or other non-urban area compared with larger urban areas).
Mother’s education and father’s education were both measured with a series of dummy variables indicating: less than high school, high school (the reference category), some college, college degree, and graduate degree. Total parental income during adolescence was measured in dollars. Poor neighborhood quality during adolescence was measured with a mean index composed of the following two questions (α=0.863): “How well kept: (a) is the building in which the respondent lives; and (b) are most of the buildings on the street?” Response categories ranged from 1=very well kept to 4=very poorly kept. The questions were answered by the interviewer.
Relations with mother were measured with a mean index composed of the following five questions (α=0.849): (a) “How close do you feel to your residential mother figure (i.e., mother, adoptive mother, stepmother, foster mother, etc.)?” (b) “How much do you think she cares about you?” (c) “Most of the time, your mother is warm and loving toward you.” (d) “You are satisfied with the way your mother and you communicate with each other.” and (e) “Overall, you are satisfied with your relationship with your mother.” The first two questions were coded 1=not at all to 5=very much, and the last three were coded 1=strongly disagree to 5=strongly agree. Relations with father were created using analogous questions (α=0.886). In this sample, 5.3% of the respondents had missing data for their residential mother / mother figure and 27.5% had missing data for their residential father figure because these individuals did not reside in the family home. To address this issue, three dummy variables were made for relations with mother: (a) no residential mother figure; (b) poor relations with mother figure (~25th percentile of individuals with a residential mother-figure); and (c) good relations with mother figure (top three quartiles). The same coding scheme was used for fathers. In all models, the first two categories were compared with the last.
Parental monitoring / supervision was measured with the following questions: “Do your parents let you make your own decisions about: (a) the time you must be home on weekend nights; (b) the people you hang around with; (c) what you wear; (d) how much television you watch; (e) which television programs you watch; (f) what time you go to bed on week nights; and (g) what you eat?” Each item was coded: 1=parents do not allow them to make this decision, and 0=they do allow them. The seven yes responses were then summed to create an additive score. Family fun was measured with the following question: “How much do you feel that you and your family have fun together?” Response categories ranged from 1=not at all to 5=very much. Frequency of dinner with parents was measured with the following question: “On how many of the past 7 days was at least one of your parents in the room with you while you ate your evening meal?” Response categories ranged from 0=no days to 7=7 days.
Cigarettes available at home was measured with the following question: “Are cigarettes easily available to you in your home?” The variable was coded 0=no and 1=yes. In addition, the interviewer answered the following question during data collection with each respondent: “Was there any evidence of smoking in the household—for example, ashtrays, people smoking, cigarettes, the smell of cigarettes?” This question was used to create a second measure of the availability of cigarettes called evidence for smoking in the household (coded 0=no and 1=yes).
Analytic Strategy
Latent growth curve models are commonly used to examine trajectories (Bollen, 1989), but this technique may not be adequate if multiple trajectories are followed by subgroups in the population (Xie, Drake, & McHugo, 2006). An alternative strategy is the group-based approach, which assumes that patterns of repeated measures (e.g., smoking) across time reflect a finite number of longitudinal trajectory groups that correspond to unobserved, latent classes in the population (Bauer & Curran, 2003; Nagin, 2005; Nagin & Odgers, 2010). The objective is to determine if multiple groups exist in the population, whether they follow distinct growth curves, and how many groups exist. This approach was chosen because different trajectory groups of cigarette smoking have been identified in previous research (Costello et al., 2008; Fuemmeler et al., 2013; Pollard et al., 2010).
Trajectory models were estimated using zero inflated Poisson regression and the “traj” procedure in Stata 15 (Jones & Nagin, 2012). The Bayesian Information Criterion (BIC) was used to evaluate model fit, the optimal number trajectory groups, and the functional form of each trajectory (e.g., intercept-only, linear, quadratic, cubic). Respondents were placed in trajectory groups based on their maximum posterior probability assignment, and average posterior probabilities for each trajectory group were 0.70 or greater (Nagin, 2005; Xie et al., 2006).
Prior to estimating trajectory groups, the data was converted into an age-based structure (Costello et al., 2008; Fuemmeler et al., 2013; Pollard et al., 2010; Windle, Mun, & Windle, 2005). To ensure adequate numbers of individuals at each age, categories were constructed for the following age groups, which have more than 1,000 individuals in each: 13–14, 15–16, 17–18, 19–20, 21–22, 23–24, 25–26, 27–28, 29–30, 31–32, and 33–35. This provided eleven different points, which allowed for the examination of non-linear trajectories of smoking. Independent variables were linked to trajectory groups using a multinomial logit model.
RESULTS
Figure 1 shows mean levels of the number of cigarettes smoked per day by age. There was an increase starting at age 13 and continuing until the early 20s. The number peaked at slightly less than 4 cigarettes per day around age 21–22, and then fluctuated up and down slightly until the early 30s. Table 1 shows additional descriptive statistics. Roughly 23.3% of the sample had no parents or friends who smoked, 12.4% had only parents who smoked, 34.0% had only friends who smoked, and 30.4% had both parents and friends who smoked.
Figure 1:
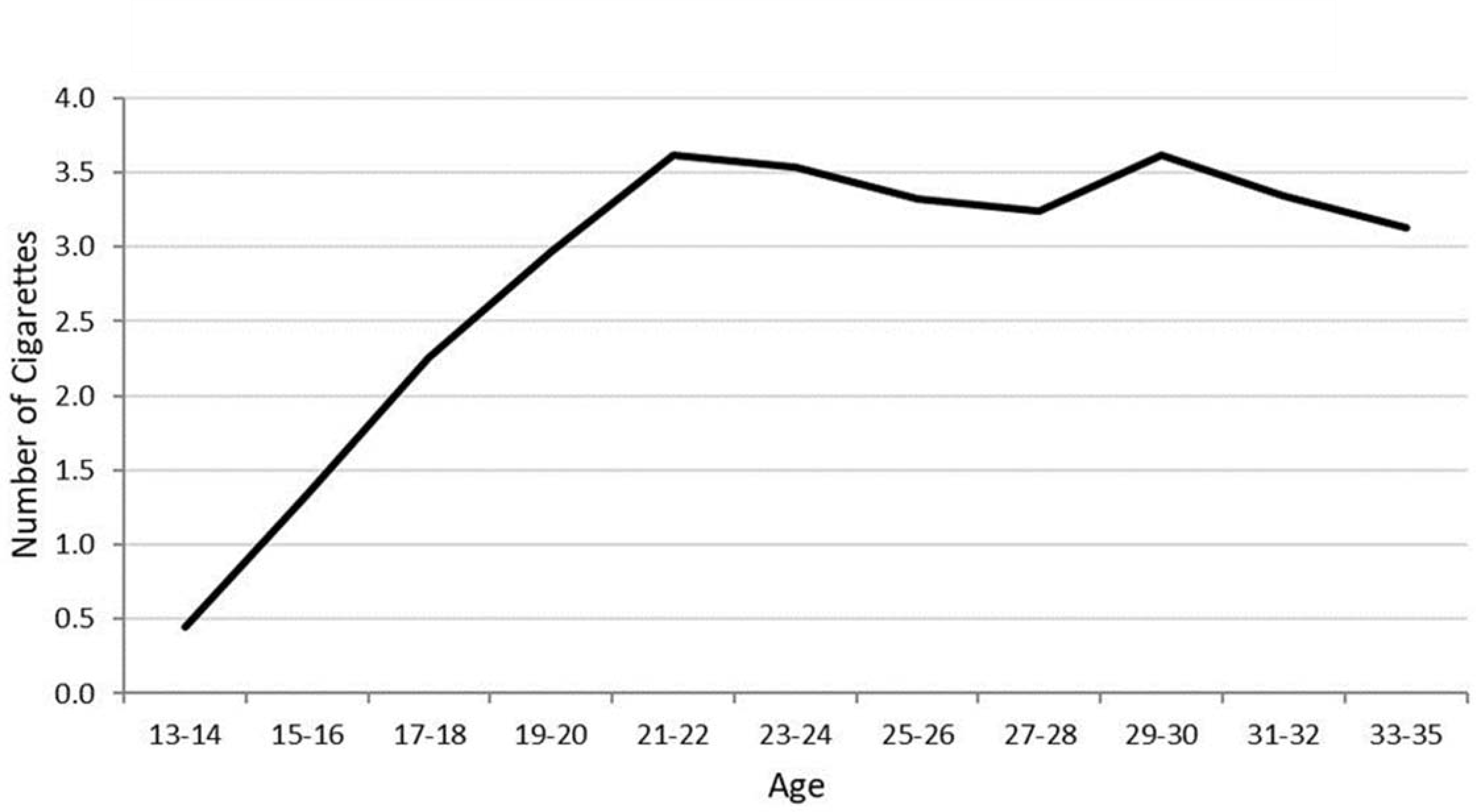
Average Number of Cigarettes per Day by Age
Table 1:
Descriptive Statistics
| Mean/Proportion | Std. Dev. | Min. | Max. | |
|---|---|---|---|---|
|
|
||||
| Parent and Peer Smoking Behaviors | ||||
| Neither Parents Nor Peers Smoke | 0.233 | - | 0 | 1 |
| Parents Smoke/Peers Do Not Smoke | 0.124 | - | 0 | 1 |
| Parents Do Not Smoke/Peers Smoke | 0.340 | - | 0 | 1 |
| Both Parents and Peers Smoke | 0.304 | - | 0 | 1 |
| Gender | ||||
| Female | 0.544 | - | 0 | 1 |
| Male | 0.456 | - | 0 | 1 |
| Race/Ethnicity (ref=White) | ||||
| White | 0.595 | - | 0 | 1 |
| Black | 0.185 | - | 0 | 1 |
| Hispanic | 0.068 | - | 0 | 1 |
| Asian | 0.052 | - | 0 | 1 |
| Native American | 0.018 | - | 0 | 1 |
| Other Race | 0.081 | - | 0 | 1 |
| Urban/Rural Residence | ||||
| Urban | 0.343 | - | 0 | 1 |
| Rural | 0.267 | - | 0 | 1 |
| Suburban | 0.375 | - | 0 | 1 |
| Other Rural/Urban | 0.015 | - | 0 | 1 |
| Mother’s Education | ||||
| <HS | 0.145 | - | 0 | 1 |
| HS | 0.315 | - | 0 | 1 |
| Some College | 0.188 | - | 0 | 1 |
| College Degree | 0.193 | - | 0 | 1 |
| Graduate Degree | 0.079 | - | 0 | 1 |
| Do Not Know | 0.039 | - | 0 | 1 |
| Mother Non-Resident | 0.041 | - | 0 | 1 |
| Father’s Education | ||||
| <HS | 0.107 | - | 0 | 1 |
| HS | 0.221 | - | 0 | 1 |
| Some College | 0.130 | - | 0 | 1 |
| College Degree | 0.149 | - | 0 | 1 |
| Graduate Degree | 0.084 | - | 0 | 1 |
| Do Not Know | 0.042 | - | 0 | 1 |
| Father Non-Resident | 0.268 | - | 0 | 1 |
| Parental Income | 47629 | 52340 | 0 | 999 |
| Poor Neighborhood Quality | 1.607 | 0.753 | 1 | 4 |
| Relations with Mother | ||||
| No Mother | 0.041 | - | 0 | 1 |
| Poor | 0.214 | - | 0 | 1 |
| Good | 0.745 | - | 0 | 1 |
| Relations with Father | ||||
| No Father | 0.268 | - | 0 | 1 |
| Poor | 0.239 | - | 0 | 1 |
| Good | 0.493 | - | 0 | 1 |
| Parental Monitoring/Supervision | 1.853 | 1.549 | 0 | 7 |
| Family Fun | 3.724 | 1.011 | 1 | 5 |
| Frequency of Dinner with Parents | 4.676 | 2.461 | 0 | 7 |
| Cigarettes Available at Home | 0.305 | - | 0 | 1 |
| Evidence of Cigarette Use (Interviewer) | 0.205 | - | 0 | 1 |
n=10,166
Figure 2 shows the findings from the trajectory analysis. For the number of cigarettes smoked per day, the best-fit model included four trajectories: “non-smokers” (63.4% of the sample), “late peak” at about age 30 (13.2%), “early peak” in the teenage years (9.9%), and consistent “high” usage from the teenage years on (13.6%). The model included one intercept term and three cubic terms. The BIC was −67106.02. The average posterior probability for each trajectory group was very high (ranging from 0.940–0.993), suggesting that these are distinct and clean groups in the data.
Figure 2:
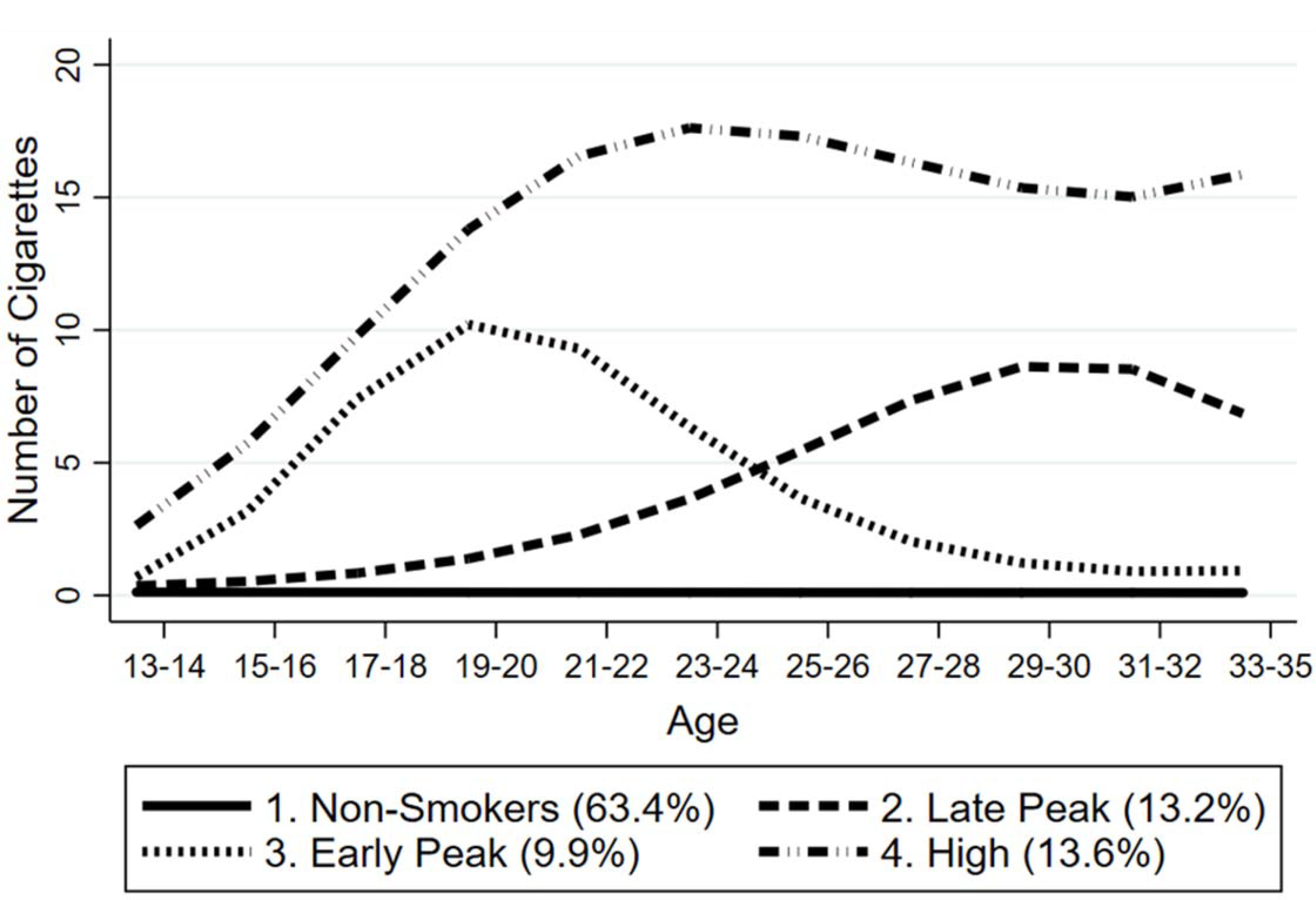
Trajectories of Number of Cigarettes per Day by Age
Table 2 shows the associations between parent and peer smoking behaviors and trajectory group membership. Compared with having neither parent nor peer role models for smoking (the reference category), having only a parent who smoked made it more likely that one would follow all three trajectories of increased smoking compared with non-smokers (RRR=1.848, 1.743, and 2.349 for the late peak, early peak, and high trajectories, respectively; all were significant at p<0.001). Having peers that smoked but parents who did not also increased the risk for belonging to the late peak, early peak, and high groups (RRRs=2.058, 3.818, and 5.760, respectively; all significant at p<0.001). Having both parents and peers made it even more likely that one would follow any of the three trajectories of cigarette use compared with non-smokers. The RRRs for having both parents and peers were larger than the ones for having one or the other for all three trajectories of cigarette use, and this was especially true for the high trajectory. Models 2 and 3 show that these results are robust even when controls for gender, race / ethnicity, rural / urban residence, parental SES, neighborhood conditions, and parent-child relations are included.
Table 2:
Relative Risk Ratios from the Multinomial Regression of Age-Based Trajectories of Number of Cigarettes per Day on Parent and Peer Smoking Behaviors
| Ref=Non-Smokers | |||
|---|---|---|---|
| Late Peak | Early Peak | High | |
|
|
|||
| 1. No Controls | |||
| Ref=Neither Parents Nor Peers Smoke | |||
| Parents Smokes/Peers Do Not Smoke | 1.848 *** | 1.743 *** | 2.349 *** |
| Parents Does Not Smoke/Peers Smoke | 2.058 *** | 3.818 *** | 5.760 *** |
| Both Parents and Peers Smoke | 3.084 *** | 5.625 *** | 12.420 *** |
| 2. Sociodemographic Controls | |||
| Ref=Neither Parents Nor Peers Smoke | |||
| Parents Smokes/Peers Do Not Smoke | 1.756 *** | 1.709 *** | 1.862 *** |
| Parents Does Not Smoke/Peers Smoke | 1.952 *** | 3.943 *** | 5.112 *** |
| Both Parents and Peers Smoke | 2.871 *** | 5.573 *** | 9.056 *** |
| 3. Sociodemographic Controls and Parent-Child Relations | |||
| Ref=Neither Parents Nor Peers Smoke | |||
| Parents Smokes/Peers Do Not Smoke | 1.827 *** | 1.706 *** | 1.978 *** |
| Parents Does Not Smoke/Peers Smoke | 1.877 *** | 3.662 *** | 4.500 *** |
| Both Parents and Peers Smoke | 2.931 *** | 5.161 *** | 8.832 *** |
| 4. Sociodemographic Controls, Parent-Child Relations, and Availability of Cigarettes | |||
| Ref=Neither Parents Nor Peers Smoke | |||
| Parents Smokes/Peers Do Not Smoke | 1.807 *** | 1.540 ** | 1.435 * |
| Parents Does Not Smoke/Peers Smoke | 1.878 *** | 3.627 *** | 4.333 *** |
| Both Parents and Peers Smoke | 2.891 *** | 4.551 *** | 6.024 *** |
n=10,166
P<0.001
P<0.01
p<0.05
p<0.10
Model 4 shows the full model, which includes additional controls for the availability of cigarettes in the home and evidence for cigarette use in the household. Most of the relationships between parent and peer smoking behaviors and trajectories of number of cigarettes smoked remained significant, but some of the RRRs were reduced. This was true for the association between having parents but not peers who smoked (compared with neither) and the early peak and high trajectories (compared with non-smokers). In these cases, the RRRs were reduced from 1.706 to 1.540 and 1.978 to 1.435, respectively, for the early peak and high trajectories. For the relationship between having both parents and peers who smoked, the RRR for the early peak group was reduced from 5.161 to 4.551 for the early peak group, and from 8.832 to 6.024 for the high trajectory. This suggests that at least part of the association between having parents (and both parents and peers) and increased risk of adolescent and early adult smoking is due to the availability of cigarettes in the family home.
DISCUSSION
This study provides evidence for four distinct trajectories of smoking across adolescence and early adulthood: (1) non-smokers; (2) another that increases slowly and peaks at around 10 cigarettes per day at the age of 30; (3) one that peaks in late adolescence / emerging adulthood and then declines; and (4) a final group that increases during adolescence and emerging adulthood and then remains high (see Figure 2). Consistent with a growing number of studies (Bernat et al., 2008; Chassin et al., 2009; Karp et al., 2005; Mays et al., 2014; Riggs, Chou, Li, & Pentz, 2007; White et al., 2002), these findings suggest that modeling average growth curves like the one depicted in Figure 1 would miss important variation in the population since multiple trajectories appear to exist. This is one of the main contributions and strengths of the group-based approach, and here it highlights the life course perspective and varying etiologies of cigarette use. Rather than identifying smoking status at a single point in time or change in cigarette use from one time point to another, this age-based design across 11 age categories in a nationally-representative sample sheds light on patterns of smoking as well as cessation. While 9.9% of the sample has an appreciably high rate of smoking in the teen and emerging adult years, this groups appears to largely eliminate smoking as time goes on. There is also suggestive evidence of a possible decline in smoking in the late peak group, though follow-up data are necessary to evaluate this possibility.
The primary findings on family and peer smoking behaviors indicate how important these context-specific factors are as correlates of long-term trajectories of smoking (Audrain-McGovern et al., 2004; Geckova et al., 2005; Harakeh et al., 2004; Simons-Morton et al., 2004; 2001; Vitaro et al., 2004). Peers appear to be relatively more important than parents (Allen et al., 2003), but the combined effects of having both parents and peers who smoke are larger than having one or the other. A possible explanation for the link between parent / peer behaviors and smoking among adolescents and early adults is simply the provision of cigarettes (Meyers et al., 2017; Widome et al., 2007). However, including controls for the availability of cigarettes at home and interviewer ratings of evidence of smoking only reduced the correlations between parent / peer smoking behaviors and trajectories by a small amount. Other mechanisms are obviously at work.
Given that the combined effects of having both parents and peers who smoke appear to be larger than having one or the other (net of availability), it may be much more normative to smoke if you have multiple role models in your lives, demonstrating that there is more to the story than simple access to cigarettes. Individuals routinely model the behavior of their parents and peers, and they may respond to rewards and punishments as well (Akers, 1985; Akers & Lee, 1996; Flay et al., 1994; Harakeh et al., 2004; Simons-Morton et al., 2004; 2001). Norms regarding cigarette smoking may be powerful in social circles and having multiple role models for smoking places individuals at high risk for initiating and sustaining cigarette use. Also, it was noted above that the results for having at least one residential parent who ever smoked were similar to the findings when a different variable (having a residential parent who currently smokes) was used. If past smoking matters just as much as associating with a current smoker, this may provide additional evidence for a social learning process, and against a provision argument.
This study has several strengths. First, it is one of the few studies to date that has used group-based trajectory models to examine longitudinal pathways of smoking across adolescence and early adulthood, and to link parent and peer smoking behaviors to trajectory membership (Audrain-McGovern et al., 2004; Bernat et al., 2008; Colder et al., 2001; Mays et al., 2014). Second, the findings reported here are based on a large, nationally-representative sample. Most of the published research on this topic has used small, regional, or non-representative samples. Third, this study shows that early-life social conditions are associated with trajectories that span adolescence and early adulthood, adding to evidence from a life course perspective and indicating that prevention programs need to target both adolescents and young adults (Elder, 2008).
This study has weaknesses as well. First, some have argued that the group-based modeling approach over-extracts latent trajectory classes (Bauer & Curran, 2003). This is a valid concern, but using the BIC, which penalizes unnecessary parameters, may help to guard against identifying too many groups. The fact that the posterior probabilities were high for each trajectory also suggests that these are distinct groups. Second, this study employed data from a large, national study, so it relied on variables that were not developed by the authors. Several key measures like parental attitudes toward smoking, whether parents talk to their kids about smoking, and whether peers provide access to cigarettes are not present in the data. Third, the current data are not well-suited to disentangling causal from selection effects. In other words, parents and peers are assumed to be the cause of the adolescent and early adult smoking in this study, but that does rule out the possibility that individuals also choose to be around friends who smoke so that they will fit in (Arnett, 2007). It is likely that both processes are occurring to some degree, and future research should be devoted to this issue. Fourth, there may be gender, race / ethnic, and socioeconomic differences in smoking. Fifth, while the length of time assessed here is appreciably lengthy, it will be important to reassess trajectories with updated data as they become available, particularly to evaluate if the late peak trajectory group continues on a downward trend. These issues are beyond the scope of this study, but they merit attention in future research.
To conclude, when teen-agers are asked why they initially started smoking, they often say that they “just wanted to try it” or that they thought it was “cool” to smoke (American Cancer Society, 2015). Feelings like these arise during social interaction, and parents and peers are powerful influences. Adolescents and early adults may initiate and sustain smoking because their friends (and perhaps even parents) provide access to cigarettes, encourage them to smoke, and respond with attitudes of approval (or a failure to show disapproval or concern). Simons-Morton and colleagues (2001:105) offered important advice for prevention programs: “The finding that peer influences are associated with substance use confirms the importance of social skills training approaches to intervention. While no studies have shown that peer group affiliation can be systematically altered, numerous studies have shown that teens’ social skills can be improved, and improved social skills protects teens from early initiation of smoking and drinking.” The key to preventing the initiation of smoking may lie in our ability to reduce tendencies to “want to try it” and eliminate social circles where smoking is viewed as “cool.” This task involves not only parents, but also teachers, religious leaders, health care professionals, community organizations, and the media, among others.
Acknowledgments
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis. The authors thank Baylor University for providing financial support for data access, statistical software, data analysis, and writing the manuscript.
Contributor Information
Matt Bradshaw, Baylor University.
Blake Victor Kent, Harvard University.
James Clark Davidson, Baylor University.
Stacy De Leon, Baylor University.
REFERENCES
- Abroms L, Simons-Morton B, Haynie DL, & Chen RS (2005). Psychosocial predictors of smoking trajectories during middle and high school. Addiction, 100, 852–861. [DOI] [PubMed] [Google Scholar]
- Acock AC (2005). Working with missing values. Journal of Marriage and Family, 67, 1012–1028. [Google Scholar]
- Akers RL (1985). Deviant Behavior: A Social Learning Approach. Wadsworth Press. [Google Scholar]
- Akers RL, & Lee G (1996). A longitudinal test of social learning theory: Adolescent smoking. Journal of Drug Issues, 26, 317–343. [Google Scholar]
- Alexander CS, Allen P, Crawford MA, & McCormick LK (1999). Taking a first puff: Cigarette smoking experiences among ethnically diverse adolescents. Ethnicity and Health, 4, 245–257. [DOI] [PubMed] [Google Scholar]
- Allen M, Donohue WA, Griffin A, Ryan D, & Turner MMM (2003). Comparing the influence of parents and peers on the choice to use drugs: A meta-analytic summary of the literature. Criminal Justice and Behavior, 30, 163–186. [Google Scholar]
- American Cancer Society. (2015). Retrieved December 27, 2018, from https://www.cancer.org/cancer/cancer-causes/tobacco-and-cancer/why-people-start-using-tobacco.html.
- Arnett JJ (2007). The myth of peer influence in adolescent smoking initiation. Health Education & Behavior, 34, 594–607. [DOI] [PubMed] [Google Scholar]
- Audrain-McGovern J, Rodriguez D, Tercyak KP, Cueva J, Rodgers K, & Patterson F (2004). Identifying and characterizing adolescent smoking trajectories. Cancer Epidemiology, Biomarkers & Prevention, 13, 2023–2034. [PubMed] [Google Scholar]
- Bauer DJ, & Curran PJ (2003). Overextraction of latent trajectory classes: Much ado about nothing? Reply to Rindskopf (2003), Muthén (2003), and Cudeck and Henly (2003).Psychological Methods, 8, 384–393. [DOI] [PubMed] [Google Scholar]
- Baumeister R (1990). Meanings of Life. Guilford. [Google Scholar]
- Bernat DH, Erickson DJ, Widome R, Perry CL, & Forster JL (2008). Adolescent smoking trajectories: Results from a population-based cohort study. Journal of Adolescent Health, 43, 334–340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bollen KA (1989). Structural Equations with Latent Variables. Wiley Series in Probability and Mathematical Statistics. Wiley, 1989. [Google Scholar]
- Brook JS, & Brook DW, Gordon AS, Whiteman M, & Cohen P (1990). The psychosocial etiology of adolescent drug use: A family interactional approach. Genetic, Social, and General Psychology Monographs, 116, 111–267. [PubMed] [Google Scholar]
- Chassin L, Curran PJ Presson CC, Sherman SJ, & Wirth R, editors. (2009). Developmental Trajectories of Cigarette Smoking from Adolescence to Adulthood. US Department of Health and Human Services, National Institutes of Health, National Cancer Institute; Bethesda, MD. [Google Scholar]
- Colder CR, Mehta P, Balanda K, Campbell RT, Mayhew KP, Stanton WR, Pentz MA, & Flay BR (2001). Identifying trajectories of adolescent smoking: An application of latent growth mixture modeling. Health Psychology, 20, 127–135. [DOI] [PubMed] [Google Scholar]
- Costello DM, Dierker LC, Jones BL, & Rose JS (2008). Trajectories of smoking from adolescence to early adulthood and their psychosocial risk factors. Health Psychology, 27, 811–818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Danaei G, Ding EL, Mozaffarian D, Taylor B, Rehm J, Murray CJL, & Ezzati M (2009). The preventable causes of death in the United States: Comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Medicine, 6, 1–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elder GH (2008). The life course as developmental theory. Child Development, 69, 1–12. [PubMed] [Google Scholar]
- Flay BR, Hu FB, Siddiqui O, Day LE, Hedeker D, Petraitis J, ... & Sussman S (1994). Differential influence of parental smoking and friends’ smoking on adolescent initiation and escalation and smoking. Journal of Health and Social Behavior, 35, 248–265. [PubMed] [Google Scholar]
- Fuemmeler B, Lee CT, Ranby KW, Clark T, McClernon FJ, Yang C, & Kollins SH (2013). Individual-and community-level correlates of cigarette-smoking trajectories from age 13 to 32 in a US population-based sample. Drug and Alcohol Dependence, 132, 301–308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geckova AM, Stewart R, van Dijk JP, Orosova O, Groothoff JW, & Post D (2005). Influence of socio-economic status, parents and peers on smoking behavior of adolescents. European Addiction Research, 11, 204–209. [DOI] [PubMed] [Google Scholar]
- Harakeh ZH, Scholte RHJ, Vermulst AA, de Vries H, & Engels RCME (2004). Parental factors and adolescents’ smoking behavior: An extension of the theory of planned behavior. Preventive Medicine, 39, 951–961. [DOI] [PubMed] [Google Scholar]
- Jones BL, & Nagin D (2012). A Stata plugin for estimating group-based trajectory models. Retrieved January 2016 from Carnegie Mellon University; (http://heinz.cmu.edu/research/458full.pdf). [Google Scholar]
- Karp I, O’loughlin J, Paradis G, Hanley J, & Difranza J Smoking trajectories of adolescent novice smokers in a longitudinal study of tobacco use. Annals of Epidemiology, 15, 445–452. [DOI] [PubMed] [Google Scholar]
- Kobus K (2003). Peers and adolescent smoking. Addiction, 98(Suppl. I), 37–55. [DOI] [PubMed] [Google Scholar]
- Mays D, Gilman SE, Rende R, Luta G, Tercyak KP, & Niaura RS (2014). Parental smoking exposure and adolescent smoking trajectories. Pediatrics, 133, 983–991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyers MJ, Delucchi K, & Halpern-Felsher B (2017). Access to tobacco among California high school students: the role of family members, peers, and retail venues. Journal of Adolescent Health, 61, 385–388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nagin D (2005). Group-Based Modeling of Development. Harvard University Press. [Google Scholar]
- Nagin DS, & Odgers CL (2010). Group-based trajectory modeling (nearly) two decades later. Journal of Quantitative Criminology, 26, 445–453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orlando M, Tucker JS, Ellickson PL, & Klein DJ (2004). Developmental trajectories of cigarette smoking and their correlates from early adolescence to young adulthood. Journal of Consulting and Clinical Psychology, 72 400–410. [DOI] [PubMed] [Google Scholar]
- Pollard MS, Tucker JS, Green HD, Kennedy D, & Go MH (2010). Friendship networks and trajectories of adolescent tobacco use. Addictive Behaviors, 35, 678–685. [DOI] [PubMed] [Google Scholar]
- Resnick MD, Bearman PS, Blum RW, Bauman KE, Harris KM, Jones J, & et al. (1997). Protecting adolescents from harm: Findings from the national longitudinal study on adolescent health. Journal of the American Medical Association, 278, 823–832. [DOI] [PubMed] [Google Scholar]
- Riggs NR, Chou CP, Li C, & Pentz MA (2007). Adolescent to emerging adulthood smoking trajectories: When do smoking trajectories diverge, and do they predict early adulthood nicotine dependence? Nicotine and Tobacco Research, 9, 1147–1154. [DOI] [PubMed] [Google Scholar]
- Royston P (2004). Multiple Imputation of Missing Values. The Stata Journal, 4(3), 227–241. [Google Scholar]
- Schafer Joseph L. (1999) “Multiple imputation: a primer.” Statistical Methods in Medical Research 8: 3–15. [DOI] [PubMed] [Google Scholar]
- Simons-Morton B, Chen R, Abroms L, & Haynie DL (2004). Latent growth curve analyses of peer and parent influences on smoking progression among early adolescents. Health Psychology, 23, 612–621. [DOI] [PubMed] [Google Scholar]
- Simons-Morton B, Haynie DL, Crump AD, Eitel P, & Saylor KE (2001). Peer and parent influences on smoking and drinking among early adolescents. Health Education and Behavior, 28, 95–107. [DOI] [PubMed] [Google Scholar]
- Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, ... & Carpenter JR (2009). Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. Bmj, 338, b2393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sudhinaraset M, Wigglesworth C, & Takeuchi DT (2016). Social and cultural contexts of alcohol use: Influences in a social-ecological framework. Alcohol Research: Current Reviews, 38, 35–45. [PMC free article] [PubMed] [Google Scholar]
- US Department of Health and Human Services. (2014). The health consequences of smoking—50 years of progress: a report of the Surgeon General.
- Vitaro F, Wanner B, Brendgen M, Gosselin C, & Gendreau PL (2004). Differential contribution of parents and friends to smoking trajectories during adolescence. Addictive Behaviors, 29, 831–835. [DOI] [PubMed] [Google Scholar]
- White HR, Pandina RJ, & Chen PH (2002). Developmental trajectories of cigarette use from early adolescence into young adulthood. Drug and Alcohol Dependence, 65, 167–178. [DOI] [PubMed] [Google Scholar]
- Widome R, Forster JL, Hannan PJ, & Perry CL (2007). Longitudinal patterns of youth access to cigarettes and smoking progression: Minnesota Adolescent Community Cohort (MACC) study (2000–2003). Preventive Medicine, 45, 442–446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Windle M, Mun EY, & Windle RC (2005). Adolescent-to-young adulthood heavy drinking trajectories and their prospective predictors. Journal of Studies on Alcohol, 66, 313–322. [DOI] [PubMed] [Google Scholar]
- Xie H, Drake R, & McHugo G (2006). Are there distinctive trajectory groups in substance abuse remission over 10 years? An application of the group-based modeling approach. Administration and Policy in Mental Health, 33, 423–432. [DOI] [PubMed] [Google Scholar]