

Abstract
Background
Botulinum toxin A can be used to eliminate dynamic wrinkles by relaxing the muscles involved in facial expressions. Therefore, it is essential to know the location, origin, insertion, function, and changes of the facial expression muscles according to their contraction.
Methods
After drawing the muscles on the face of a model, pictures were taken at rest. The model was then asked to make facial expressions that cause facial wrinkles. All images were taken with the Vectra H1 camera system (Canfield Scientific, Inc., Fairfield, New Jersey). Each expression image was aligned to its respective static image to compute the differences in skin position, so as to calculate the skin displacement vectors. The values for local changes in skin displacement were calculated by applying the automated algorithms of the Vectra Software Mirror Suite and visualized using the color and size of the arrow.
Results
Face painting and 3D skin vector displacement analyses enabled visualization of all the facial muscles involved in facial expressions working dynamically, allowing us to visualize the effect of each muscle in the creation of hyperkinetic wrinkles. Face painting and 3D skin vector displacement analyses can be combined to determine the location of the wrinkles, extent of the muscle, part of the muscle that contracts, presence of asymmetry, direction in which the muscle contracts, and correlation between the antagonists and synergistic muscles.
Conclusion
The botulinum toxin A injection educational model using body painting and 3D skin vector displacement analyses can provide a deeper understanding of actual moving muscle anatomy.
Level of Evidence
4.
Keywords: 3D skin vector, botulinum toxin, dynamic anatomy, education, face painting
1. INTRODUCTION
Increasing numbers of people worldwide are opting to undergo nonsurgical facial aesthetic procedures, owing to their safety and effectiveness in reducing the signs of facial aging.1 In particular, botulinum toxin A is an effective method for non‐surgically eliminating facial wrinkles and may play a role in the cosmetic enhancement of the aging face.2, 3
Muscle paralysis/weakness is the ultimate goal of the cosmetic use of botulinum toxin A, but it may also lead to unintended effects on neighboring muscles through local diffusion of up to a diameter of 3 cm from the injection point.4 Therefore, a complete understanding of facial anatomy is essential to ensure proper injection technique, obtain safe and predictable results, and anticipate any complications, all of which can be significantly reduced through education and training.5
Cadaver anatomy training has been shown to improve facial anatomy knowledge for the majority of aesthetic practitioners. It may also enhance their confidence in performing nonsurgical facial aesthetic procedures.6 Unfortunately there are limited correlations to be obtained between facial expression muscles and dynamic facial expressions from cadaveric anatomy because it is very static.7
An assessment of botulinum toxin treatment includes anatomical and functional analyses of the musculature in the context of facial morphology, for which a full understanding of muscle relationships is required.8 Comprehensive facial assessments encompass both static and dynamic observation.9 However, until now, the curriculum has mainly used cadavers to teach static anatomy, and consequently, many doctors lack an understanding of dynamic anatomy.10
An objective quantification of minute skin movement has been shown to be provided by 3D skin vector displacement analysis.11 This study aimed to investigate skin movement using state‐of‐the‐art 3D skin vector displacement analyses and relate the measurements to the shape of facial wrinkles. The results of this investigation led to the formation of more individualized neuromodulator injection schemata.12 Therefore, in this study, we sought to develop educational materials that could be used to teach physicians the shape and function of individual muscles. To this end, we drew muscles on the face of a volunteer using body painting and employed 3D skin vector displacement analysis to quantify the movement of the muscles.
2. MATERIALS AND METHODS
This study was approved by the Institutional Review Board of Chosun University Hospital, Gwangju, Korea (2020‐11‐012‐001).
A 32‐year‐old Korean woman who had not previously been treated for wrinkles using botulinum toxin A, was selected as the model for this study. She was educated until she fully understood how to make facial expressions related to facial wrinkles. The patient voluntarily applied to become a model and consented to the use of her images for the purposes of research and education. She was briefed on the study, aim, scope, and procedures; and provided written informed consent for the use of her data and associated images prior to her inclusion in the study.
The model washed her face and removed her makeup, and a professional makeup artist drew muscles associated with facial expressions on her face. The location of the facial muscles was verified by one anatomist and one facial plastic surgeon.
After drawing the muscle, pictures were taken at rest (static images) using a Vectra H1 camera system (Canfield Scientific, Inc., Fairfield, New Jersey). The model was then asked to make facial expressions that cause facial wrinkles (forehead lines, glabellar frown lines, lateral orbital lines, and nasal dorsal lines), to make an excessive gingival display (gummy smile), and to pull down the corners of her mouth with maximal effort (expression image). Each image was taken with the Vectra H1 camera system. Using Vectra Software Mirror Suite two‐dimensional (Video Graphic 1) and three‐dimensional facial expression videos (Video Graphic 2) were created utilizing before and after facial expression images.
Each expression image was aligned to its respective static image to compute the differences in skin position so as to calculate the skin displacement vectors. The degree of the skin displacement is gradually increases as it goes toward blue, green, yellow, orange, red, and the degree of the skin displacement is proportional to the length of the arrow on arrows of the same color.
The values for local changes in skin displacement were calculated by applying the automated algorithms of the Vectra Software Mirror Suite, and visualized using the color and size of the arrow (Video Graphic 3).
Through these studies, we were able to determine the location of the wrinkles, the extent of the muscle, which part of the specific muscle contracts during expression, the presence of asymmetry, the direction in which the muscle contracts, and the correlation between muscle antagonists and agonists.
3. RESULTS
Face painting and 3D skin vector displacement analyses enabled the visualization of all the facial muscles involved in facial expressions working dynamically, and allowed us to visualize the effect of each muscle in the creation of hyperkinetic wrinkles. With this method, we learned various morphological features related to the contraction of facial expression muscles that had been previously overlooked.
The outer boundary of the skin that moves in response to muscle contraction is outside the muscle insertion area. Therefore, the range of skin displacement due to muscle contraction was wider than that of the muscle. Even in one muscle, the size of the skin displacement was different, depending on the part. Differences in the extent and size of skin displacement were observed between the same muscle groups on the left and right sides. Although wrinkles occur mainly in areas where skin displacement appears, they may also occur in areas with no skin displacement. In most cases, multiple synergistic muscles contract to make one wrinkle or one expression. When synergistic muscles contract to form a facial expression, the antagonists relax and lengthen. Furthermore, the vector of skin displacement developed by muscle contraction for each muscle has a characteristic direction.
The above‐mentioned contents are summarized by indication as follows.
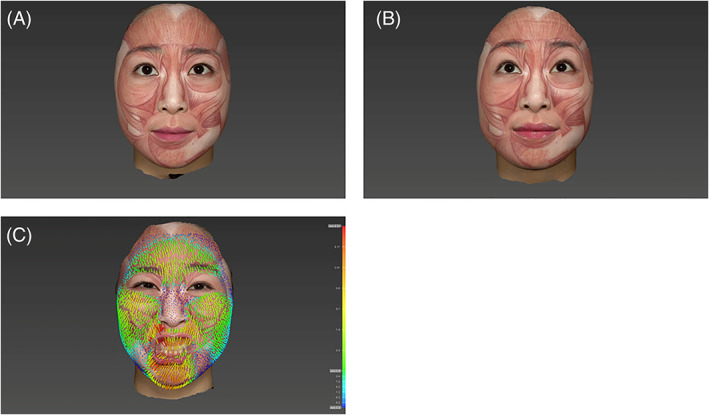
Horizontal Forehead lines (Figure 1A‐C)
FIGURE 1.
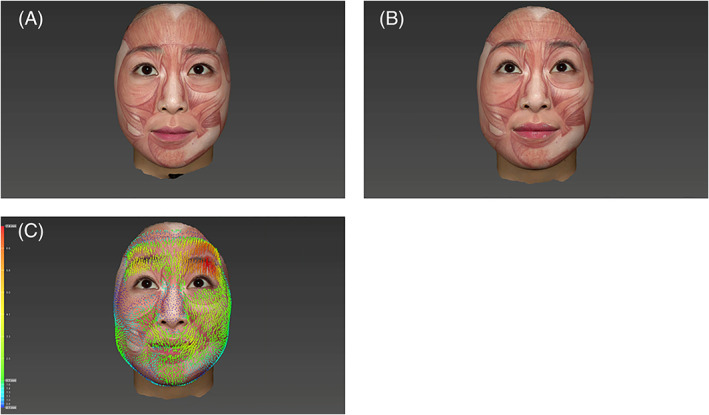
Horizontal forehead wrinkle lines. When the frontalis muscle is contracted to raise the eyebrows, the lower part of the frontalis muscle contracts. When the frontal muscle contracts, skin displacement is also observed on the medial side of the temporal region. A, Static status. B, Dynamic status. C, Skin displacement amount shown by arrows
Related muscles are the frontalis muscle. When the frontalis muscle contracts to raise the eyebrows, skin displacement occurs primarily in the lower forehead. In other words, when the frontalis muscle is contracted to raise the eyebrows, the lower part of the frontalis muscle contracts. Wrinkles were also observed in the upper forehead with slight skin displacement caused by contraction of the frontalis muscle. The direction in which the frontalis muscle contracts, rises obliquely to the side.
When the frontal muscle contracts, skin displacement is also observed on the medial side of the temporal region.
Since the degree and width of skin displacement of the left and right frontalis muscle are different, the width and contraction force of the left and right frontalis muscle may also differ; in this case, the height or shape of both eyebrows was asymmetric.
When the frontalis muscle contracts, its antagonists, the orbicularis oculi muscle, corrugator supercilii muscle, depressor supercilii muscle, and procerus muscle, are relatively relaxed, and these muscles tend to elongate.
Glabellar frown lines (Figure 2 A, B, C)
FIGURE 2.
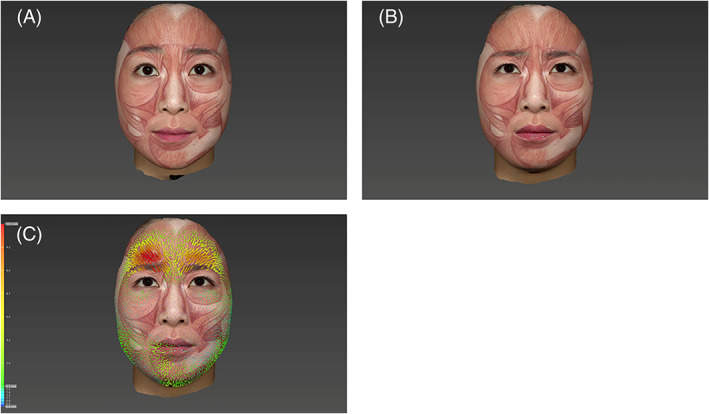
Glabellar frown lines. When glabellar wrinkles are made, the entire eyebrow moves downward and inward. In other words, all muscles involved pull the eyebrow medial down. The inner third of the eyebrow is pulled the most, while the degree of outward pulling is weak. A, Static status. B, Dynamic status. C, Skin displacement amount shown by arrows
The orbicularis oculi muscle, corrugator supercilii muscle, depressor supercilii muscle, and procerus muscle are involved in the formation of glabellar lines; among which, the corrugator supercilii muscle causes skin displacement. When glabellar wrinkles are made, the entire eyebrow moves downward and inward. In other words, all muscles involved pull the eyebrow medial down. The inner third of the eyebrow is pulled the most, while the degree of outward pulling is weak. The outer eyebrows are also pulled down, mainly by the sphincteric action of the orbicularis oculi muscle. The height of the procerus muscle on the center line remains unchanged; in other words, the procerus muscle does not pull the central part of the face, but mainly pulls the inner side of the eyebrow downward. As the related muscles contract, the antagonist of these muscles, the frontalis muscle, is observed to relax and lengthen.
Lateral canthal lines (crow's feet) (Figure 3 A, B, C)
FIGURE 3.
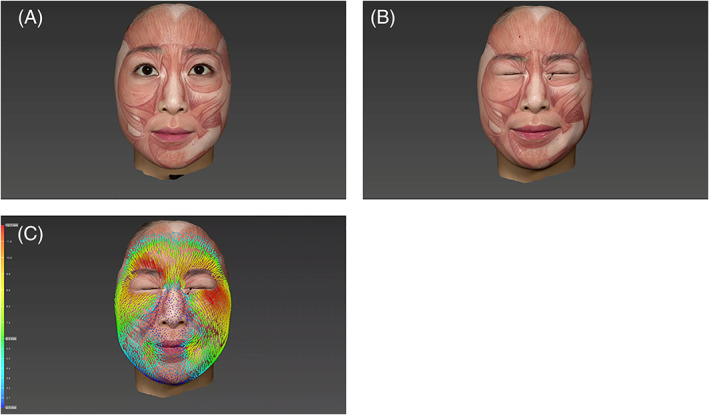
Crow's feet. The corrugator supercilii muscle, depressor supercilii muscle, procerus muscle, and nasalis muscle are synergistic. The labii superioris alaeque nasi (LLSAN) muscle and others contract together, while the antagonist, the frontalis muscle, relaxes and lengthens. The direction of the vector in which the orbicularis oculi muscle contracts is toward the inner canthal angle; this vector is radial, similar to the spokes of a wheel. A, Static status. B, Dynamic status. C, Skin displacement amount shown by arrows
The target muscle is the orbicularis oculi muscle.
The corrugator supercilii muscle, depressor supercilii muscle, procerus muscle, and nasalis muscle are synergistic. Levator labii superioris alaeque nasi (LLSAN) muscle and others contract together, while the antagonist, the frontalis muscle, relaxes and lengthens. The direction of the vector in which the orbicularis oculi muscle contracts is toward the inner canthal angle; this vector is radial, similar to the spokes of a wheel.
Nasal dorsal lines (bunny lines) (Figure 4 A, B, C)
FIGURE 4.
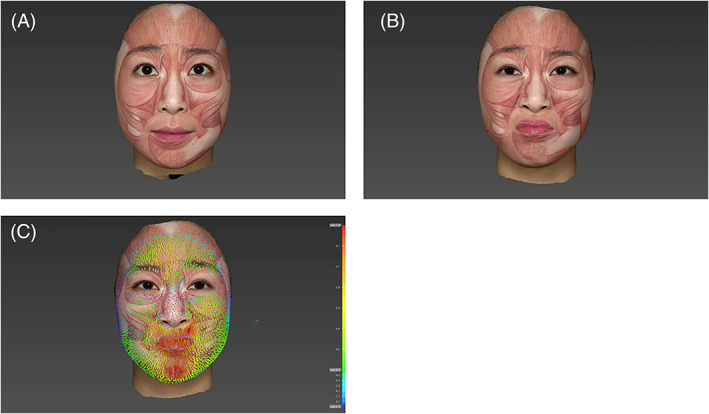
Nose. The wrinkles of the nasal dorsum are mainly caused by the nasalis muscle. However, in the current study, there was little skin displacement on the nasalis of the model, with the majority of the contractions found in the LLSAN muscle. A, Static status. B, Dynamic status. C, Skin displacement amount shown by arrows
The wrinkles of the nasal dorsum are mainly caused by the nasalis muscle and LLSAN muscle. However, in the current study, there was little skin displacement on the nasalis muscle of the model, with the majority of the contractions found in the LLSAN muscle.
Excessive gingival show (gummy smile) (Figure 5 A, B, C)
FIGURE 5.
Gummy smile. The target muscles to improve excessive gingival display were the zygomaticus minor muscle, LLSAN muscle, and levator labii superioris (LLS) muscle. The muscles involved in raising the upper lip were the zygomaticus minor muscle, LLSAN muscle, and LLS muscle. A, Static status. B, Dynamic status. C, Skin displacement amount shown by arrows
The target muscles to improve excessive gingival display were the zygomaticus minor muscle, LLSAN muscle, and levator labii superioris (LLS) muscle. The muscles involved in raising the upper lip were the zygomaticus minor muscle, LLSAN muscle, and LLS muscle.
The muscles that raise the upper lip are involved in exposing the gums when laughing. Of these muscles, the LLSAN muscle raises the upper lip the most when exposed to the gingiva.
Drooping of the mouth corner (Figure 6 A, B, C)
FIGURE 6.
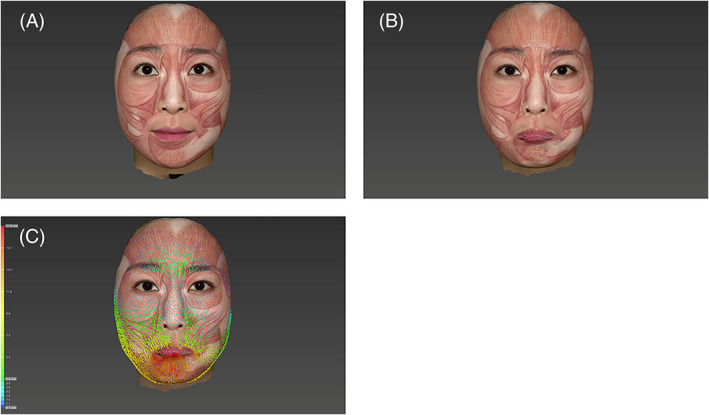
Both the depressor anguli oris (DAO) muscle and mentalis muscle work synergistically to pull down the corner of the mouth. The mentalis muscle pulls the tail of the mouth down and inward, while the DAO muscle pulls the corner of the mouth in a downward direction perpendicular to the mandibular border. Furthermore, the mentalis muscle contracts strongly to lower the tail of the mouth
Both the depressor anguli oris (DAO) muscle and mentalis muscle work synergistically to pull down the corner of the mouth. The mentalis muscle pulls the tail of the mouth down and inward, while the DAO muscle pulls the corner of the mouth in a downward direction perpendicular to the mandibular border. Furthermore, the mentalis muscle contracts strongly to lower the tail of the mouth.
4. DISCUSSION
The development of facial expression wrinkles are part of a natural aging process caused by repetitive facial muscle contraction and skin damage. Botulinum toxin A can be used to eliminate dynamic wrinkles by affecting the muscles involved with facial expressions. It is, therefore, essential to know the location, origin, insertion, function, and changes of the facial expression muscles according to their contraction. Existing anatomical knowledge based on cadaver dissection has limitations in that the dynamic changes caused by muscle contraction have not been determined.
Face painting and 3D skin vector displacement analyses can be combined to determine the location of the wrinkles, extent of the muscle, part of the muscle that contracts, presence of asymmetry, direction in which the muscle contracts, and correlation between the antagonists and synergistic muscles. To determine the dynamic characteristics of each muscle, it is more effective to view the muscle as a moving image rather than as a still photo.
In this study, the frontalis muscle was found to contract mainly in the lower part, while the upper part was fixed with limited movement. Since the lower half of the frontalis muscle is mainly responsible for eyebrow lifting, if botulinum toxin is injected in the lower half of the forehead in wrinkle treatment, it may be difficult to raise the eyebrows, or the eyebrows may begin to droop. When treating the upper face with neuromodulators, eyebrow ptosis is an undesired effect that can result in patient dissatisfaction.13 Another matter of concern is the lateral extent of the frontalis muscle effect. Since skin displacement is also observed outside the temporal line, the outer boundary of the frontalis muscle will be located further lateral to the temporal line. Therefore, in the treatment of forehead wrinkles, botulinum toxin must be injected along the temporal line to prevent aesthetically unappealing outcomes such as the “Spock eyebrow” or “Mephisto sign.”14 Increased muscle activity caused by increased muscle mass results in larger skin displacement; thus the stronger side requires a higher dose of a neuromodulator to achieve a comparable clinical effect.15, 16
Moreover, the contraction intensity and width between the left and right frontalis muscle may be different. This may lead to an asymmetric height or shape of the eyebrows. To correct asymmetry, it is necessary to inject more points or doses on the stronger and wider side. For example, our study volunteer showed left side dominant forehead activity, therefore, to correct her forehead wrinkles, a greater amount of botulinum toxin would have to be injected to the left side.
According to our study on glabellar frown lines, when the associated muscles (orbicularis oculi muscle, corrugator supercilii muscle, depressor supercilii muscle, procerus muscle) contract, vertical wrinkles on the inside of the eyebrows, depressions around the pupil line above the eyebrows, horizontal wrinkles between the glabella, and depressions inside the eyebrows occur. The vertical folds are divided into the orbital and glabellar portions.
Vertical wrinkles on the inside of the eyebrows are caused by contraction of the orbicularis oculi muscle, corrugator supercilii muscle, and depressor supercilii muscle. Lateral depression is caused by contraction of the corrugator supercilia muscle oblique part.
Before the procedure, it is necessary to check whether the abovementioned components are present, and the injection point and dosage should be determined accordingly. When glabellar wrinkles are made, the entire eyebrow moves downward and inward. According to our study, the inner third of the eyebrow is pulled downward to the greatest extent, while the degree of outward pulling is less. The outer part of the eyebrows was also pulled down as a result of the sphincteric action of the orbicularis oculi muscle. The height of the procerus muscle on the center line remains unchanged. In other words, the procerus muscle does not pull the central part of the face, but mainly pulls the inner side of the eyebrow downward. As a result, dents appear on the inside of the eyebrows and the pulled skin tissue overlaps, resulting in horizontal wrinkles.
The use of a conventional botulinum toxin injection cannot affect the position of the eyebrow. Instead, to raise the lateral eyebrows, it is necessary to paralyze the orbicularis oculi muscle, located in the lateral one‐third part of the eyebrow. At this point, botulinum toxin should be injected into the intradermal or subcutaneous layer to prevent blepharoptosis.
Nasal wrinkles on the dorsum of the nose are frequently treated with the injection of botulinum toxin type A into the nasalis muscle.17 However, there was little movement of the nasalis muscle in the model in our study. Depending on individual differences, it is thought that muscles associated with wrinkles on the nasal dorsum will contract either the nasalis muscle or LLSAN muscle or both muscles. Before the procedure, the patient should be asked to make wrinkles on the nasal dorsum to determine the predominant muscles, so that the botulinum toxin is injected properly.
Of the muscles that raise the upper lip (zygomaticus minor, LLSAN muscle, LLS muscle), the LLSAN muscle contracts the most strongly when exposed to the gums. Therefore, the LLSAN muscle can be injected with botulinum toxin to effectively treat a gummy smile.18, 19, 20
The muscles that lower the tail of the mouth are known as the DAO muscle. However, the muscle that contracts strongly to lower the tail of the mouth is the mentalis, which pulls the tail of the mouth down and inward. The DAO muscle pulls down the corner of the mouth in a direction perpendicular to the mandibular border. Both the DAO muscle and mentalis muscle can be injected with botulinum toxin to effectively alleviate sagging of the mouth. Mouth corner lifting performed by botulinum toxin injections should target both the DAO muscle and the mentalis muscle.21, 22
5. CONCLUSION
The botulinum toxin A injection educational model using face painting and 3D skin vector displacement analyses can provide a deeper understanding of actual moving muscle anatomy and, consequently, lead to a more practical and safe treatment.
ACKNOWLEGEMENT
This study was supported by research fund from Chosun University Hospital, 2020.
CONFLICT OF INTEREST
None of the authors have conflicts of interest nor financial interest in any of the products, devices, or drugs mentioned in this article.
Supporting information
Video S1 Graphic 1: 2‐dimensional facial expression video of face painting face.
Video S2 Graphic 2: 3‐dimensional facial expression video of face painting face.
Video S3 Graphic 3: Each expression image was aligned to its respective static image to compute the differences in skin position to calculate the skin displacement vectors. The values for local changes in skin displacement were calculated by applying the automated algorithms, and visualized using the color and size of the arrow.
Moon H‐J, Lee W, Choi JY. Dynamic evaluation of facial muscles: 3D skin displacement vector analysis using a facial painting model. Laryngoscope Investigative Otolaryngology. 2021;6(4):650–656. 10.1002/lio2.590
BIBLIOGRAPHY
- 1.De Aquino MS, Haddad A, Ferreira LM. Assessment of quality of life in patients who underwent minimally invasive cosmetic procedures. Aesthetic Plast Surg. 2013;37(3):497‐503. [DOI] [PubMed] [Google Scholar]
- 2.Keen M, Blitzer A, Aviv J, et al. Botulinum toxin A for hyperkinetic facial lines: results of a double‐blind, placebo‐controlled study. Plast Reconstr Surg. 1994;94(1):94‐99. [DOI] [PubMed] [Google Scholar]
- 3.Carruthers JD, Lowe NJ, Menter MA, et al. Double‐blind, placebo‐controlled study of the safety and efficacy of botulinum toxin type for patients with glabellar lines. Plast Reconstr Surg. 2003;112:21S. [DOI] [PubMed] [Google Scholar]
- 4.Huang W, Foster JA, Rogachefsky AS. Pharmacology of botulinum toxin. J Am Acad Dermatol. 2000;43:249‐259. [DOI] [PubMed] [Google Scholar]
- 5.Wieder JM, Moy RL. Understanding botulinum toxin. Surgical anatomy of the frown, forehead, and periocular region. Dermatol Surg. 1998;24(11):1172‐1174. [PubMed] [Google Scholar]
- 6.Klein AW. Complications and adverse reactions with the use of botulinum toxin. Semin Cutan Med Surg. 2001;20:109‐120. [DOI] [PubMed] [Google Scholar]
- 7.Kumar N, Rahman E. Effectiveness of teaching facial anatomy through cadaver dissection on aesthetic physicians' knowledge. Adv Med Educ Pract. 2017;8:475‐480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lorenc ZP, Smith S, Nestor M, et al. Understanding the functional anatomy of the frontalis and glabellar complex for optimal aesthetic botulinum toxin type a therapy. Aesthetic Plast Surg. 2013;37:975‐983. [DOI] [PubMed] [Google Scholar]
- 9.Sundaram H, Signorini M, Liew S, et al. Global aesthetics consensus: botulinum toxin type A—evidence‐based review, emerging concepts, and consensus recommendations for aesthetic use, including updates on complications. Plast Reconstr Surg. 2016;137:518e‐529e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Monheit G, Lin X, Nelson D, Kane M. Consideration of muscle mass in glabellar line treatment with botulinum toxin type A. J Drugs Dermatol. 2012;11:1041‐1045. [PubMed] [Google Scholar]
- 11.Cotofana S, Freytag DL, Frank K, et al. The bidirectional movement of the frontalis muscle: introducing the line of convergence and its potential clinical relevance. Plast Reconstr Surg. 2020;145(5):1155‐1162. [DOI] [PubMed] [Google Scholar]
- 12.Frank K, Freytag DL, Schenck TL, et al. Relationship between forehead motion and the shape of forehead lines‐A 3D skin displacement vector analysis. J Cosmet Dermatol. 2019;8. 10.1111/jocd.13065. [DOI] [PubMed] [Google Scholar]
- 13.King M. Management of ptosis. J Clin Aesthet Dermatol. 2016;9:E1‐E4. [PMC free article] [PubMed] [Google Scholar]
- 14.Cho ES, Hwang JY, Kim ST. A proposal to prevent the “Mephisto Sign” side effect of botulinum toxin type A injection in chronic migraine. Yonsei Med J. 2013;54(6):1542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Janssen I, Heymsfield SB, Wang ZM, Ross R. Skeletal muscle mass and distribution in 468men and women aged 18–88 yr. J Appl Physiol (1985). 2000;89:81‐88. [DOI] [PubMed] [Google Scholar]
- 16.Weeden JC, Trotman CA, Faraway JJ. Three‐dimensional analysis of facial movement in normal adults: influence of sex and facial shape. Angle Orthod. 2001;71:132‐140. [DOI] [PubMed] [Google Scholar]
- 17.Tamura BM, Odo MY, Chang B, Cucé LC, Flynn TC. Treatment of nasal wrinkles with botulinum toxin. Dermatol Surg. 2005;31:271‐275. [DOI] [PubMed] [Google Scholar]
- 18.Polo M. Botulinum toxin type A (Botox) for the neuromuscular correction of excessive gingival display on smiling (gummy smile). Am J Orthod Dentofacial Orthop. 2008;133:195‐203. [DOI] [PubMed] [Google Scholar]
- 19.Suber JS, Dinh TP, Prince MD, Smith PD. OnabotulinumtoxinA for the treatment of a "gummy smile". Aesthet Surg J. 2014;34(3):432‐437. [DOI] [PubMed] [Google Scholar]
- 20.Hwang WS, Hur MS, Hu KS, et al. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. Angle Orthod. 2009;79(1):70‐77. [DOI] [PubMed] [Google Scholar]
- 21.Bae GY, Na JI, Park KC, Cho SB. Nonsurgical correction of drooping mouth corners using monophasic hyaluronic acid and incobotulinumtoxinA. J Cosmet Dermatol. 2020;19(2):338‐345. [DOI] [PubMed] [Google Scholar]
- 22.Qian W, Zhang YK, Lv W, Hou Y, Cao Q, Fan JF. Application of local injection of botulinum toxin A in cosmetic patients with congenital drooping mouth corner. Aesthetic Plast Surg. 2016;40(6):926‐930. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video S1 Graphic 1: 2‐dimensional facial expression video of face painting face.
Video S2 Graphic 2: 3‐dimensional facial expression video of face painting face.
Video S3 Graphic 3: Each expression image was aligned to its respective static image to compute the differences in skin position to calculate the skin displacement vectors. The values for local changes in skin displacement were calculated by applying the automated algorithms, and visualized using the color and size of the arrow.