

Abstract
Objective
To explore the distribution of constitution types of diabetes mellitus (DM) in traditional Chinese medicine (TCM) and to provide evidence-based medicine basis for the prevention and treatment of diabetes.
Methods
PubMed, Embase, Web of Science, and three Chinese databases were searched to include research literature on the relationship between diabetes and TCM constitution. The single rate study of cross-sectional literature was conducted with RStudio software, and the control meta-analysis of the diabetic and nondiabetic population was performed with Review Manager 5.3 software. Two independent reviewers assessed the methodological quality of the studies' data. The main outcomes included the distribution of constitutional types in the diabetic population and the odds ratio (OR) between the two. Effect sizes are expressed as proportions or ORs with 95% confidence intervals (CI).
Results
A total of 28,781 diabetic cases were included in 87 articles. Yin-deficiency, phlegm-dampness, and qi-deficiency accounted for 18% (95% CI (15%, 20%), P < 0.01), 17% (95% CI (15%, 19%), P < 0.01), and 13% (95% CI (11%, 15%), P < 0.01) of the total diabetic cases. The risk of diabetes in people with yin-deficiency and phlegm-dampness was 3.06 (95% CI (1.38–6.78), P=0.006) and 1.89 (95%CI (1.05–3.42), P=0.03) times higher than that in those with other constitutions, respectively. The distribution of TCM constitution of DM patients varied significantly in different regions and ages.
Conclusion
Yin-deficiency and phlegm-dampness are the common constitution types of diabetic people, and they may also be the risk factors of diabetes. Balanced constitution may be a protective factor of diabetes. More high-quality cohort and case-control studies need to be designed to provide more valuable evidence-based basis for assessing the correlation between DM and TCM constitution.
1. Introduction
Diabetes mellitus is a common chronic metabolic disease. With the development of society and the change of people's lifestyles, the incidence of DM has increased year by year, and it has become the most harmful noncommunicable disease on human health after tumor and cardiovascular disease [1]. According to the data released by the International T2DM Federation in 2013, there were 387 million diabetes patients in the world in 2013. China has the largest number of T2DM patients in the world, with 98 million T2DM patients, which is expected to increase to 143 million by 2035 [2]. The high incidence of chronic diseases and the rapid increase in medical costs highlight the importance of public health. In the face of the current high prevalence of diabetes, it is particularly important to carry out effective prevention and treatment measures. Traditional Chinese medicine (TCM) has been used for thousands of years of history as a form of health management, and this health care system has been widely used in many countries of the world [3]. TCM regards that everyone is different from others, so there is no recognized diagnosis and treatment model in the TCM treatment of diabetes, but more emphasis on individual treatment. Different constitution types make individuals suffer from different diseases. Individualized prevention and treatment measures for different types of constitution personalized treatment, so as to achieve a better effect than conventional treatment. The constitution of traditional Chinese medicine is the grasp of “preventive treatment of the disease” [4]. In April 2009, the Constitution in Chinese Medicine Questionnaire (CCMQ) was published and recommended by the China Association of Chinese Medicine as a standard for constitution measurement because of its good reliability and validity [5]. According to the CCMQ, the body constitutions of Chinese population are divided into nine basic types, namely balanced, qi-deficiency, yang-deficiency, yin-deficiency, phlegm-dampness, dampness-heat, blood stasis, qi stagnation, and inherited special. Among them, the balanced constitution is normal, while the other eight are biased and prone to relevant diseases [6]. TCM constitution identification has been widely used in nondisease treatment centers and community health service centers all over the country because of its simple operation, easy to understand, and easy to accept. In recent years, a large number of clinical studies on the relationship between diabetes and TCM constitution have been carried out in various regions, which provides data support for analyzing the distribution law of the TCM constitution of diabetic patients.
This study aims to obtain a larger sample of data on the distribution of TCM constitution types of diabetic patients, to determine the types of constitution prone to diabetes, and to provide evidence-based medical evidence for the effective prevention and treatment of diabetes for “preventive treatment of disease.” This was achieved by a meta-analysis of the current clinical research literature on the TCM constitution of diabetes.
2. Materials and Methods
2.1. Retrieval Strategy
Clinical studies on the correlation between body constitution and diabetes were searched in PubMed, Embase, Web of Science, China National Knowledge Infrastructure (CNKI), VIP Database (VIP), and Wanfang Database from April 2009 (the CCMQ's publication time) to March 31, 2021. The search terms included “diabetes mellitus,” “tangniaobing” (Chinese pinyin of diabetes), “tizhi” (Chinese pinyin of constitution), and “constitution.” No language, nationality, or publication restrictions were applied. As an example of one specific strategy, the search terms for PubMed were as follows: (diabetes mellitus [Title/Abstract]) AND constitution [Title/Abstract]).
2.2. Inclusion/Exclusion Criteria
All clinical literature on the relationship between diabetes and TCM constitution types (including cross-sectional studies, case-control studies, and cohort studies) were included, without limiting the type of research and the form of publication. The details are as follows: (1) Research object: the research object is the diabetic patients with a definite diagnosis; (2) Research tool: the measurement tool used for the constitution identification of the research object is the standard of Classification and Judgment of TCM Constitution issued by the China Institute of TCM in 2009; and (3) the sample size of the study is clear, and the data of the constitution composition are complete.
Exclusion criteria: (1) literature lacking in basic information reports or without statistics of constitution composition; (2) included subjects combined with other systematic serious diseases that may affect their TCM constitution types; (3) the study is limited to a certain kind of constitution population, such as simple phlegm-dampness constitution research; and (4) repeatedly published literature.
2.3. Data Extraction and Quality Evaluation on Methodology
Make a data extraction form, including the literature title, the type of research design, the area of the study, the sex of the object of study, the average age, the number of people of each type of constitution, the total sample size, and so on.
The Newcastle-Woodward scale (NOS) [7] was used to assess the methodological quality of the cohort study and case-control study. The scale was compared with 8 items from three aspects: the selection of the study population, the comparability between groups, and the measurement of exposure factors, with a total score of 9 points. The cross-sectional study adopted the standard (referred to as AHRQ standard) recommended by the Agency for Healthcare Research and Quality (AHRQ) [8]. It is divided into 11 items, including data sources, inclusion criteria, observation time, continuity of research objects, subjective factors of evaluators, quality control, and so on, with a total score of 11 points.
2.4. Data Analysis
The meta-analysis of the individual rate of each constitution type was carried out by using RStudio-1.1.463 software [9]. Analysis models were chosen by the results of heterogeneity tests. The percentage of 8 different biased constitution types of diabetic people and their 95% confidence interval (CI) were calculated. When the heterogeneity was too large, subgroup analysis was carried out according to regional and age factors, and the inverted funnel chart was used to analyze the degree of publication bias assessed by funnel plot analysis. The Review Manager 5.3 software provided by the Cochrane collaboration network was used to analyze the data synthesis between the diabetic group and nondiabetic group, and the odds ratio (OR) and its 95% CI were used to describe the effect value of a single study. The effect model was selected according to heterogeneity: the fixed effect model was used when heterogeneity was less than 50%, and the random effect model was used when heterogeneity was greater (I2 > 50%).
3. Results
3.1. Retrieval Process and Results
Duplicate references were excluded. All titles and abstracts were then screened to eliminate duplicates and obviously irrelevant citations. Following screening of 1240 citations found in the literature search, 93 papers potentially met the inclusion criteria and were examined in full text. 87 studies were included in the final review. The literature screening process and results are shown in Figure 1.
Figure 1.

Flow chart of study searching and selection.
3.2. Basic Characteristics and Quality Evaluation of the Inclusion Study
Among all the studies we included, 1 was a Chinese-Malaysian constitution fitness study, and 86 were domestic clinical studies, including 22 provinces, autonomous regions, and municipalities directly under the central government. The study was published in 2009 at the earliest, and the number of studies is increasing year by year. A total of 28,581 patients with diabetes were included in each study, with an average sample size of 329. According to the NOS (9 items) and AHRQ cross-sectional study evaluation criteria (11 items), 7 case-control studies and 80 cross-sectional studies were evaluated. The scores of cross-sectional studies were all 3–7, which were medium- and low-quality literatures, which did not have high research quality and had a high risk of bias. See Table 1 for details.
Table 1.
Characteristics of included studies.
| Study ID | Area | Study design | Sample size | Average age (years) | Gender ratio | Quality evaluation |
|---|---|---|---|---|---|---|
| Li [10] | Jiangxi | CSS | 398 | 75.42 ± 8.65 | 206/192 | 5 |
| Zhong and Xue [11] | Guangdong | CSS | 50 | 62.99 ± 3.49 | 25/25 | 6 |
| Liu et al. [12] | Henan | CSS | 109 | 57.94 ± 8.69 | 58/51 | 4 |
| Zhang et al. [13] | Shanghai | CSS | 120 | 56.88 ± 2.42 | 65/55 | 4 |
| Wu et al. [14] | Ningxia | CSS | 100 | 41.6 ± 4.5 | 68/32 | 5 |
| Wang et al. [15] | Shanghai | CSS | 112 | 55.8 ± 6.2 | 54/58 | 5 |
| Shen et al. [16] | Shanghai | CSS | 395 | 73.81 | 172/223 | 4 |
| Lin et al. [17] | Guangdong | CSS | 500 | 61.2 ± 5.3 | 258/242 | 6 |
| Li et al. [18] | Guizhou | CSS | 663 | 59.12 ± 6.57 | 411/252 | 3 |
| Hang et al. [19] | Guangdong | CSS | 250 | 71.01 ± 5.82 | 133/117 | 4 |
| Guan [20] | Jiangsu | CSS | 200 | U | 105/95 | 3 |
| Guan [21] | Sichuan | CSS | 195 | 69.36 ± 3.41 | 109/86 | 7 |
| Zhang et al. [22] | Zhejiang | CCS | 1315 | U | 890/425 | 6 |
| Zhou [23] | Fujian | CCS | 285 | 56.98 ± 6.75 | U | 5 |
| Wei and Yang [24] | Guangdong | CSS | 300 | U | U | 5 |
| Wang [25] | Neimongol | CSS | 270 | 66.8 ± 10.5 | 136/134 | 6 |
| Lin et al. [26] | Beijing | CSS | 122 | U | U | 4 |
| Li et al. [27] | Beijing | CSS | 119 | U | 71/48 | 5 |
| Lang [28] | Heilongjiang | CSS | 100 | 75.12 ± 6.34 | 56/44 | 7 |
| Jiang et al. [29] | Shanghai | CSS | 700 | 60.14 ± 4.55 | 350/350 | 5 |
| Hu et al. [30] | Tianjin | CSS | 200 | 61.32 ± 8.24 | 96/104 | 5 |
| Gao et al. [31] | Shandong | CSS | 75 | 69.92 | 33/42 | 4 |
| Chen et al. [32] | Zhejiang | CSS | 700 | 74.1 ± 13.1 | 242/458 | 5 |
| Zhou et al. [33] | Shanghai | CSS | 442 | U | 187/255 | 7 |
| Wang [34] | Shandong | CSS | 436 | 58.12 ± 9.63 | 255/181 | 7 |
| Shen et al. [35] | Beijing | CCS | 461 | 70.68 ± 10.41 | 202/259 | 6 |
| Shen et al. [36] | Beijing | CSS | 333 | 57.80 ± 10.91 | 133/200 | 6 |
| Qiu [37] | Xinjiang | CSS | 141 | 61.89 ± 11.37 | 86/55 | 5 |
| Lv [38] | Tianjin | CSS | 1003 | U | U | 7 |
| Liu et al. [39] | Jiangxi | CSS | 208 | 52.1 ± 3.4 | 107/91 | 5 |
| Li [40] | Beijing | CSS | 60 | U | 31/29 | 4 |
| Jing et al. [41] | Beijing | CSS | 160 | 56.35 ± 12.82 | 74/86 | 4 |
| Jing [42] | Guangxi | CSS | 297 | 57.59 ± 11.12 | 176/121 | 5 |
| Huang [43] | Guangdong | CSS | 497 | 67.94 ± 8.64 | 200/297 | 4 |
| Huang et al. [44] | Guangdong | CSS | 367 | 67.57 ± 8.77 | 137/230 | 4 |
| Huang et al. [45] | Zhejiang | CSS | 630 | U | 236/394 | 4 |
| Zhu et al. [46] | Nationwide | CSS | 412 | 52.54 ± 13.92 | U | 7 |
| Feng [47] | Jiangsu | CSS | 200 | 61.4 | 103/97 | 7 |
| Zou and Wang [48] | Sichuan | CSS | 320 | 52.11 ± 11.32 | 167/153 | 4 |
| Zhu et al. [49] | Beijing | CSS | 136 | U | U | 4 |
| Xue et al. [50] | Shanghai | CCS | 879 | U | 425/454 | 5 |
| Xu and Liu [51] | Shanxi | CSS | 251 | 59.666 | 114/133 | 4 |
| Xie et al. [52] | Henan | CSS | 426 | U | 258/198 | 5 |
| Wang et al. [53] | Guangdong | CSS | 112 | 86.61 ± 13.39 | 45/67 | 5 |
| Wang et al. [54] | Jiangsu | CSS | 300 | U | 144/156 | 6 |
| Wang [55] | Sichuan | CSS | 57 | 39.04 ± 12.09 | 10/17 | 7 |
| Ren et al. [56] | Shandong | CSS | 151 | 63.8 | 83/68 | 6 |
| Li [57] | Guangdong | CSS | 120 | 51.9 ± 4.7 | 68/52 | 5 |
| Li et al. [58] | Guangxi | CSS | 302 | 65.60 ± 10.96 | 130/172 | 6 |
| Huang [59] | Malaysia | CSS | 68 | 64.16 ± 10.03 | 30/38 | 5 |
| Hua et al. [60] | Shanghai | CSS | 931 | 73.45 ± 7.37 | 353/578 | 4 |
| Zou and Wang [61] | Beijing | CSS | 296 | 49.70 ± 12.28 | 173/123 | 4 |
| Zhao [62] | Inner Mongolia | CCS | 139 | U | 84/55 | 7 |
| Zhang [63] | Henan | CSS | 90 | 40 | 71/19 | 5 |
| Yu [64] | Liaoning | CSS | 372 | 60.9 l ± 11.557 | 173/199 | 6 |
| Yang [65] | Shandong | CSS | 192 | 63.4 ± 8.0 | 80/112 | 7 |
| Xiang and Qian [66] | Jiangsu | CSS | 835 | 63.4 | 343/492 | 5 |
| Wu and Hao [67] | Shanxi | CSS | 354 | U | 196/158 | 5 |
| Wu et al. [68] | Fujian | CSS | 476 | U | 188/288 | 4 |
| Wei et al. [69] | Shanghai | CSS | 400 | 59.8 ± 11.6 | 211/189 | 6 |
| Wang et al. [70] | Guangdong | CSS | 320 | 47.2 | 175/145 | 5 |
| Lu [71] | Shanghai | CSS | 1420 | 69.2 | 574/846 | 3 |
| Liu et al. [72] | Tianjin | CSS | 200 | U | U | 4 |
| Li [73] | Guangdong | CCS | 483 | 42.03 ± 12.68 | 263/220 | 6 |
| Li [74] | Fujian | CSS | 250 | 70.12 ± 11.92 | 204/261 | 5 |
| Hu et al. [75] | Jiangxi | CSS | 500 | 57.1 ± 11.4 | 188/312 | 6 |
| Chen and Zhou [76] | Zhejiang | CSS | 119 | 57.6 | 65/54 | 6 |
| Xiao et al. [77] | Guangdong | CSS | 300 | 65.6 ± 12.6 | 160/140 | 5 |
| Zhu et al. [78] | Shandong | CSS | 135 | 55.69 ± 9.87 | 56/79 | 6 |
| Yang and Wang [79] | Yunnan | CSS | 427 | U | U | 6 |
| Xiang and Ran [80] | Jiangsu | CSS | 270 | U | 116/154 | 5 |
| Xiang [81] | Jiangsu | CSS | 478 | 63.1 ± 9.1 | 201/277 | 5 |
| Wang et al. [82] | Beijing | CSS | 213 | 56.55 ± 12.14 | 99/104 | 6 |
| Li et al. [83] | Zhejiang | CSS | 300 | 56.57 ± 7.91 | 152/148 | 5 |
| Chen et al. [84] | Henan | CSS | 300 | 52.12 ± 12.19 | 152/148 | 5 |
| Zheng and Jian [85] | Guangdong | CCS | 89 | U | 54/35 | 6 |
| Wu et al.[86] | Guangdong | CSS | 147 | U | U | 6 |
| Tang [87] | Guangxi | CSS | 200 | 52.78 ± 6.62 | 99/101 | 3 |
| Ma [88] | Guangdong | CSS | 48 | 56.9 ± 6.7 | 35/13 | 4 |
| Liu [89] | Guangdong | CSS | 98 | 56.6 ± 4.8 | 55/43 | 6 |
| Li et al. [90] | Guangdong | CSS | 74 | 62.6 | 39/35 | 5 |
| Zhang et al. [91] | Hong Kong | CSS | 239 | 59 ± 10.33 | 119/120 | 5 |
| Han [92] | Beijing | CSS | 206 | 65 ± 12 | 91/115 | 6 |
| Han et al. [93] | Beijing | CSS | 52 | 58.14 ± 8.2 | 41/11 | 4 |
| Zhang [94] | Fujian | CSS | 534 | 57.67 ± 11.17 | 258/276 | 5 |
| Yan et al. [95] | Henan | CSS | 571 | 51.69 ± 8.81 | 284/287 | 6 |
| Cui [96] | Shanxi | CSS | 476 | U | 188/288 | 4 |
CSS, cross-sectional study; CCS, case-control study; U, unclear, indicating no report.
3.3. Meta-Analysis of Biased Constitution Distribution in TCM
According to the number of diabetic patients reported in each study, meta-analysis was carried out. A total of 87 studies reported these data, with a total sample size of 28,581 cases. The results showed that the distribution of 8 biased constitution types in patients with diabetes was yin-deficiency, phlegm-dampness, and qi-deficiency in the highest proportion, and the results of meta-analysis were shown in a forest map. The proportion of the other five types of constitution is less than 10%. The results of the meta-analysis are described in a table.
3.3.1. Yin-Deficiency Constitution
86 studies involving 28,342 cases reported the proportion of yin-deficiency constitution in DM patient population. The random effects model was adopted due to the great heterogeneity of included studies. The results showed that the proportion of yin-deficiency constitution in DM patients was 18% (95% CI (15%, 20%), P < 0.01) (Figure 2).
Figure 2.
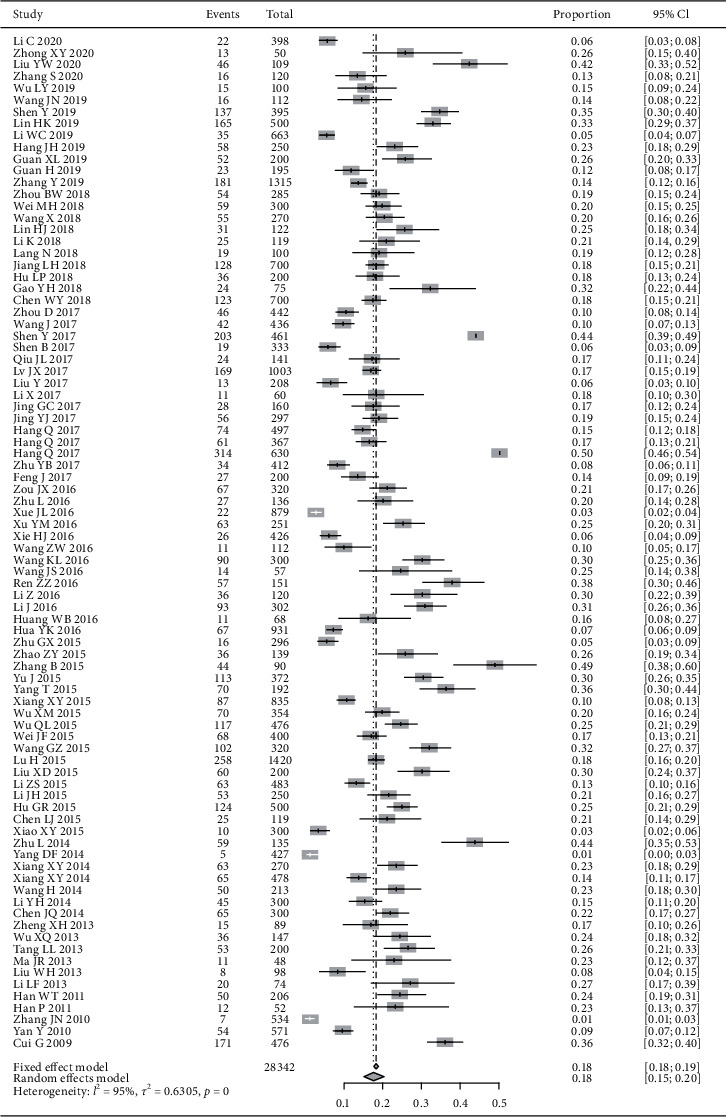
Meta-analysis of the proportion of yin-deficiency constitution in DM patients.
3.3.2. Phlegm-Dampness Constitution
86 studies involving 28,342 cases reported the proportion of phlegm-dampness constitution in DM patient population. The random effects model was adopted due to the great heterogeneity of included studies. The results showed that the proportion of phlegm-dampness constitution in DM patients was 17% (95% CI (15%, 19%), P < 0.01) (Figure 3).
Figure 3.
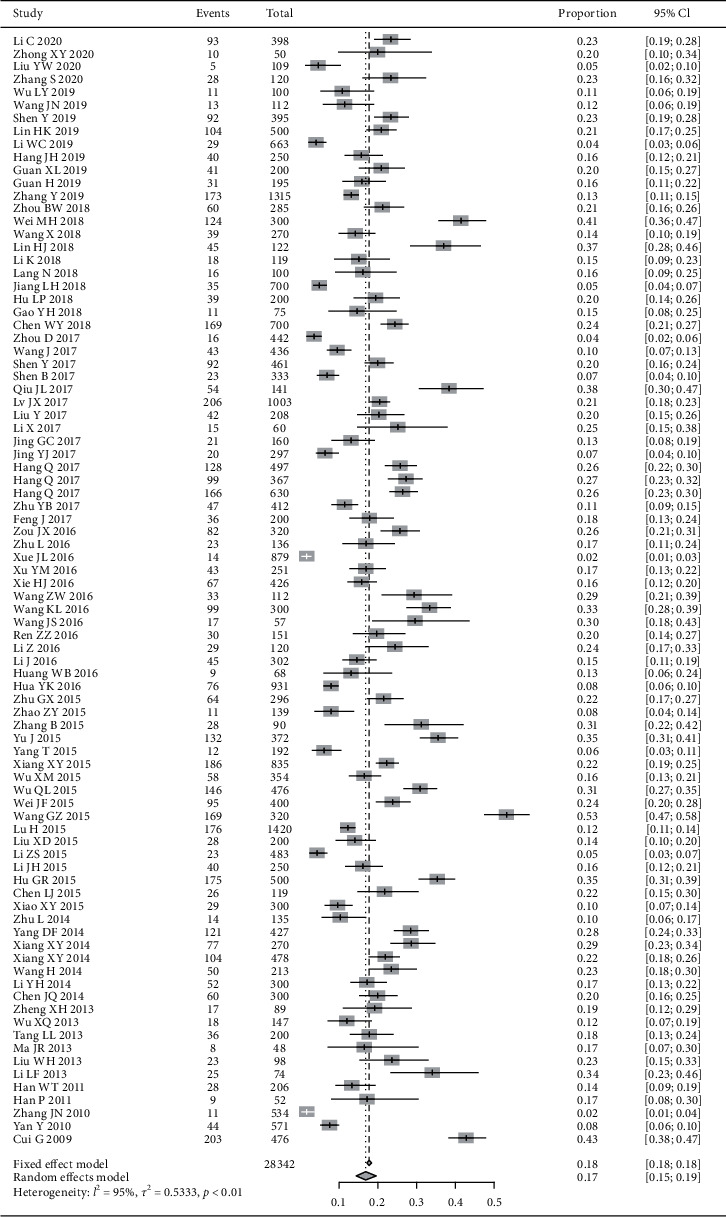
Meta-analysis of the proportion of phlegm-dampness constitution in DM patients.
3.3.3. Qi-Deficiency Constitution
84 studies involving 27,608 cases reported the proportion of qi-deficiency constitution in DM patient population. The random effects model was adopted due to the great heterogeneity of included studies. The results showed that the proportion of qi-deficiency constitution in DM patients was 13% (95% CI (11%, 15%), P < 0.01) (Figure 4).
Figure 4.
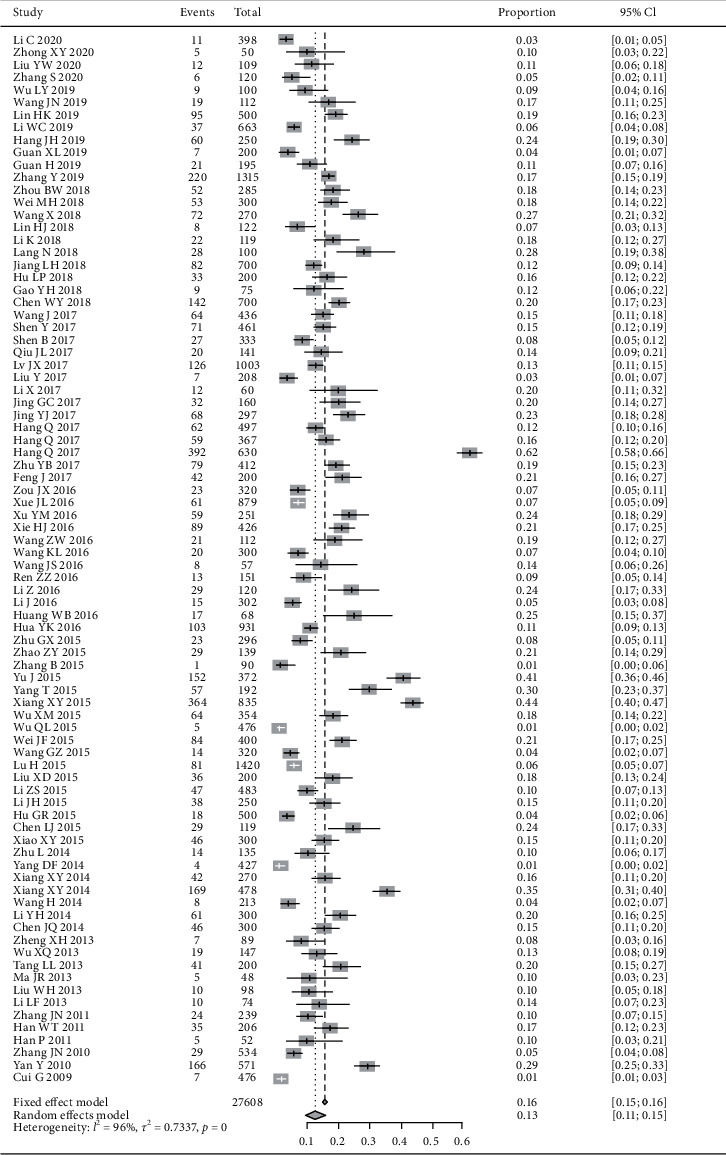
Meta-analysis of the proportion of qi-deficiency constitution in DM patients.
3.3.4. Other TCM Constitutions
The distribution proportion of the other five biased constitution in DM patients is less than 10%, and the order from high to low is yang-deficiency, dampness-heat, blood stasis, qi stagnation, and inherited special constitution. The statistical results show that the I2 values of all types of constitution are more than 50%, suggesting that there is a large heterogeneity, so the random effect model should be used for meta-analysis (Table 2).
Table 2.
Meta-analysis of the proportion of other five constitutions in DM patients.
| Constitution | Studies | Participants | Proportion (%) | 95% CI | P | I2(%) |
|---|---|---|---|---|---|---|
| Yang-deficiency | 79 | 26025 | 8 | 7%–9% | <0.01 | 91 |
| Dampness-heat | 78 | 26209 | 7 | 6%–9% | <0.01 | 96 |
| Blood stasis | 83 | 27290 | 6 | 5%–7% | <0.01 | 90 |
| Qi stagnation | 73 | 24692 | 4 | 3%–5% | <0.01 | 90 |
| Inherited special | 62 | 21295 | 2 | 1%–2% | <0.01 | 76 |
3.4. Subgroup Analysis of Distribution of TCM Constitution by Region and Age
3.4.1. Region
According to the regions included in the literature, all but one of the reports were conducted in China. Divided by the seven major regions of China, the majority of the literature included in this study is from North China, East China, and South China, with a large sample size, and other regions have smaller literature and smaller sample sizes. Therefore, all the literature was divided into three groups according to North China, East China, and South China to compare the proportions of yin-deficiency, phlegm-dampness, and qi-deficiency reported in the literature from the three regions. The results are shown in Table 3.
Table 3.
Meta-analysis of common constitution proportion of DM in three regions.
| Constitution | Region | Studies | Number of occurrence | Total sample size | Proportion (%) | 95% CI | P |
|---|---|---|---|---|---|---|---|
| Yin-deficiency | East China | 32 | 2472 | 14386 | 16 | 13%–20% | <0.01 |
| South China | 20 | 944 | 4793 | 17 | 13%–21% | <0.01 | |
| North China | 18 | 961 | 4575 | 20 | 16%–25% | <0.01 | |
|
| |||||||
| Phlegm-dampness | East China | 32 | 2351 | 14386 | 15 | 12%–19% | <0.01 |
| South China | 19 | 980 | 4554 | 20 | 15%–26% | <0.01 | |
| North China | 18 | 812 | 4575 | 17 | 14%–20% | <0.01 | |
|
| |||||||
| Qi-deficiency | East China | 31 | 2241 | 13991 | 11 | 7%–16% | <0.01 |
| South China | 20 | 690 | 4793 | 13 | 11%–16% | <0.01 | |
| North China | 18 | 662 | 4575 | 13 | 9%–17% | <0.01 | |
3.4.2. Age
According to the average age of participants reported in each study, all the studies were divided into 3 subgroups by average age (≤45, 46–60, and >60). The random effects model was adopted due to the great heterogeneity of included studies. Meta-analysis showed that among the population of DM patients, the distribution of yin-deficiency, phlegm-dampness, and qi-deficiency constitution over 45 years old was significantly higher than that of adults under 45 years old (Table 4).
Table 4.
Meta-analysis of distribution of TCM constitutions by age in DM patients.
| Constitution | Age | Studies | Participants | Proportion (%) | 95% CI | P |
|---|---|---|---|---|---|---|
| Yin-deficiency | ≤45 | 4 | 136 | 23 | 12%–38% | <0.01 |
| 46–60 | 31 | 1352 | 14 | 11%–19% | <0.01 | |
| >60 | 29 | 1916 | 19 | 15%–23% | <0.01 | |
|
| ||||||
| Phlegm-dampness | ≤45 | 4 | 79 | 15 | 7%–31% | <0.01 |
| 46–60 | 30 | 1356 | 15 | 11%–19% | <0.01 | |
| >60 | 29 | 1846 | 18 | 16%–21% | <0.01 | |
|
| ||||||
| Qi-deficiency | ≤45 | 4 | 65 | 8 | 4%–14% | ≤0.01 |
| 46–60 | 31 | 1173 | 12 | 9%–15% | <0.01 | |
| >60 | 28 | 1699 | 16 | 13%–20% | <0.01 | |
3.5. Meta-Analysis of Distribution of TCM Constitution in DM and General Population
The three most common types of constitution including yin-deficiency, phlegm-dampness, and qi-deficiency were identified in the meta-analysis of the proportion of constitution in DM patients. Then, we further compared it with general population. Seven studies [22, 35, 49, 50, 62, 73, 85] involving 36,546 participants reported the relevant data, so they were included in the meta-analysis.
Meta-analysis showed that the OR value of yin-deficiency, phlegm-dampness, and balanced constitution's distribution in DM patients and general population was 3.06 (95%CI: 1.38–6.78), 1.89 (95%CI: 1.05–3.42), and 0.48 (95%CI: 0.32–0.71), respectively. The difference was statistically significant. There was no significant difference in the proportion of qi-deficiency between the DM and general populations, with an OR of 1.82 (95%CI: 0.68–4.81). More details are shown in Figure 5.
Figure 5.
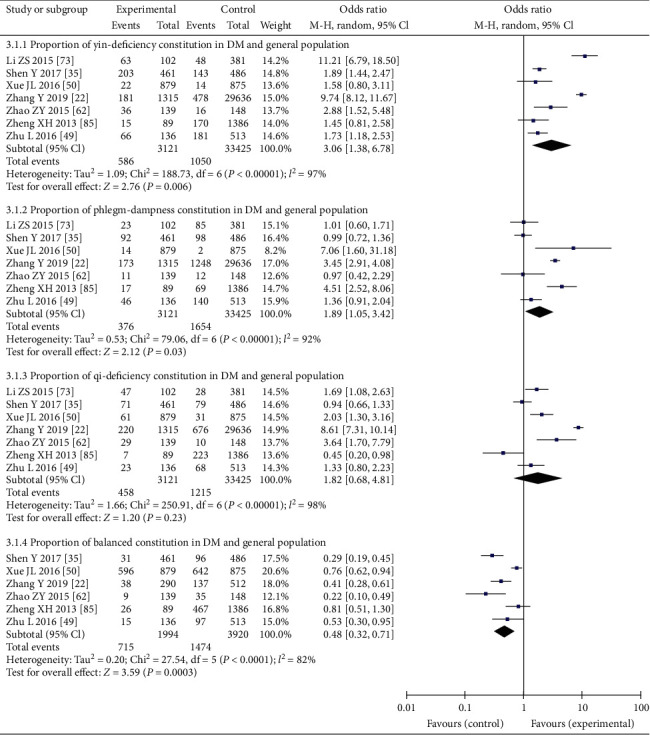
Comparison of distribution of three common traditional Chinese medicine constitutions and balanced constitution between DM patients and general population.
3.6. Publication Bias
Taking the proportion of yin-deficiency constitution of participants with DM as an index, the inverted funnel diagram was analyzed in the included literature. Considering that TCM constitution research is mostly carried out in different regions and people, and the differences in climate, environment, and lifestyle lead to obvious heterogeneity of each research, so it presents a relatively scattered state, which is related to the particularity of TCM constitution research (Figure 6).
Figure 6.

Funnel plot analysis of the distribution of yin-deficiency constitution.
4. Discussion
4.1. Analysis of the Correlation between DM and the Constitution of TCM
Prevention is the one of the most important essences of TCM, indicating the preventive treatment of diseases. The body constitution in TCM could indicate the patients' overall condition and could form the basis of prevention theory; thus, it has attracted much attention from researchers and clinicians [97]. The TCM constitution refers to the comprehensive, relatively stable, and inherent characteristics of the morphological structure, physiological function, and psychological state formed on the basis of innate endowment and acquired disposition in the course of human life [98]. It can reflect an individual's current health status and future health trends in constitution differences, life processes, psychological condition, and adaptability to natural and social environments. The specificity of individual constitution often causes body's susceptibility to a specific pathogenic factor. For instance, people with phlegm-dampness constitution easily suffer from disease such as diabetes mellitus, metabolic syndrome, and other diseases, with weak adaptability to rainy season and moist environment [99]. The TCM constitution scale provided an objective, generally recognized technical tool and professional standard. Through the constitution classification of TCM, we can determine the individual constitution type of the population and guide the individualized treatment and disease prevention. Correlative studies on constitution and clinical disease have promoted the application of TCM in public health. Relevant research shows that yin-deficiency constitution of hypertension, diabetes, constipation, female menopause, and osteoporosis showed high distribution [100]. This is also consistent with our research results.
A total of 87 articles were included in this study, with a total of 28,781 large samples. It was found that yin-deficiency, phlegm-dampness, and qi-deficiency constitution accounted for 18% (15%–20%), 17% (15%–19%), and 13% (11%–15%) of the total number of people with diabetes, respectively. The results of meta-analysis showed that balanced constitution may be a protective factor of diabetes (OR = 0.48, 95% CI: 0.32–0.71), while yin-deficiency and phlegm-dampness constitution may be the risky factors of it (OR = 3.06, 95% CI: 1.38–2.78 and OR = 1.89, 95% CI: 1.05–3.42).
The constitution distribution of DM patients was significantly different from that of the general population. In 2009, Zhu and Wang published a nationwide cross-sectional study [101] on the constitution of 21,948 general populations in TCM. The results showed that balanced constitution (32.14%) was the most common type of TCM constitution. Qi-deficiency (13.42%), yang-deficiency (9.08%), and phlegm-dampness (9.04%) were common biased constitution. In this study, yin-deficiency constitution was the most common (18%) followed by phlegm-dampness (17%) and qi-deficiency (13%). The proportion of yin-deficiency and phlegm-dampness constitution is much higher than that in general population, while qi-deficiency was close to that of general population. This could illustrate the specificity of constitution characteristics in patients with DM and may also confirm the association between DM and TCM constitution. It is suggested that in the process of prevention and treatment of diabetes in the future, we should identify and focus on the people with yin-deficiency and phlegm-dampness constitution as soon as possible and take corresponding intervention measures in exercise, diet, and so on, to promote the return of biased constitution to balanced constitution.
The results of meta-analysis showed that the proportion of yin-deficiency was the highest in North China followed by South and East China, and the proportion of phlegm-dampness was the highest in South China followed by North China and East China, which may be related to the climatic characteristics of different regions. The climate in North China is cool and dry, the humidity of the air is insufficient, and the body fluid is deficient and dry, so that there are more people with yin-deficiency. The climate in South China is warm and humid, which may easily generate phlegm, dampness, and heat inside the bodies of local residents, which may lead to more people with phlegm-dampness. East China runs through the north and south areas, and the climate contains dry and wet, so people with yin-deficiency and phlegm-dampness account for more. The age subgroup showed that the number of people with diabetes over 45 years old was significantly more than that under 45 years old. Some studies have shown that age is one of the most important factors affecting diabetes [102], advanced age is a risk factor for diabetes, and the prevalence rate of diabetes increases with age. Hence, efforts should be made to adjust the constitution in middle‐aged and elderly populations about diabetes mellitus to reduce the incidence of type 2 diabetes.
4.2. Limitations of the Study
From the perspective of the methodology of research design, the literature reports on the basic information related to the research is incomplete, such as the time of inclusion of the research object, basic data, and the original data of each constitution. In the aspect of data statistical analysis, some studies only describe the number and proportion of various constitution types and there is a lack of research on the correlation between constitution types and family heredity, external environment, illness and other factors.
The causes of diabetes are complex, but due to the lack of reported data in the original literature, the analysis angle has some limitations, so it is difficult to deeply analyze the various factors that affect the constitution of people with diabetes. This study is different from other types of meta-analysis. The articles included are mainly observational studies, which can only hint but not prove the causal relationship between disease and constitution. The results of this study need to be confirmed by more high-quality prospective cohort studies and case-control studies. Therefore, there may be a certain risk of deviation in the result.
The included studies are heterogeneous. Due to the large amount of literature, there are significant differences in research time, measurement methods, sample size, age, gender, region, and other aspects. Different from intervention research, individual differences have a great impact on TCM constitution, which is also the characteristic of TCM constitution. Therefore, this study conducted subgroup analyses of the original data by region and age in order to better understand. It is suggested that clinical research methods with higher quality and more standardized contents should be adopted in the future to further explore the relationship between various TCM constitutions and chronic diseases.
4.3. Implications for Future Clinical Practice
Referring to the methods of evidence-based medicine in the previous study [103] on the relationship between constitution and disease, this study analyzed the people with high incidence of diabetes from the perspective of TCM constitution. Combined with published studies [103, 104], we have found that phlegm-dampness constitution is closely related to various metabolic diseases, which is of great significance to guide the accurate prevention and treatment of metabolic diseases. In the future clinical practice, we can determine the target of early intervention of diabetes by screening the high-risk groups of yin-deficiency and phlegm-dampness and carry out targeted drug and nondrug intervention according to the constitution and syndrome of TCM, in order to adjust biased constitution and reduce the risk of disease.
5. Conclusion
The current systematic review of 87 included studies found that yin-deficiency, phlegm-dampness, and qi-deficiency are the main types of constitution in diabetes patients, of which yin-deficiency and phlegm-dampness are associated with the occurrence of diabetes. They are also risk factors for the incidence of diabetes, while balanced constitution is a protective factor for diabetes. It is suggested that in the future, we should focus on people over 45 years old with yin-deficiency in North China and phlegm-dampness people over 45 years old in South China and increase TCM constitution intervention measures as soon as possible to improve biased constitution and reduce the incidence of diseases. More high-quality observational studies should be designed in the future to provide a more scientific evidence-based basis for the use of personalized diagnosis and treatment of TCM in the prevention and treatment of diabetes.
Acknowledgments
This research was financially supported by the National Natural Science Foundation of China (no. 81874413), Science and Technology Nova Plan of Beijing City (no. Z201100000820027), Young Talent Promotion Project of China Association of Chinese Medicine (no. CACM-2018-QNRC2-C02), and Youth Innovation Team Project of Beijing University of Traditional Chinese Medicine (no. 2019-JYB-TD-010).
Contributor Information
Yanfei Zheng, Email: yanfei_z@163.com.
Lingru Li, Email: lilingru912@163.com.
Data Availability
The relevant data used to support the results of this study are included in this article.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Authors' Contributions
Fan Bai and Hui Luo contributed equally to this work. Fan Bai and Hui Luo put forward the idea of this study and designed the method of this systematic review. Fan Bai, Liying Wang, Linghui Zhu, and Yuanyuan Guan searched the articles, conducted data collection and extraction, and analyzed the data. Lingru Li, Yanfei Zheng, and Qi Wang provided guidelines for this systematic review and meta-analysis. The authors approved the final version of the manuscript.
References
- 1.Yu L., Liu N. W., Zhang L., et al. An epidemiological survey of diabetes mellitus and prediabetes in adults in Tianjin. Chinese Journal of Prevention and Control of Chronic Diseases. 2017;25(7):511–513. [Google Scholar]
- 2.Guariguata L., Whiting D. R., Hambleton I., et al. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Research and Clinical Practice. 2017;103:137–149. doi: 10.1016/j.diabres.2013.11.002. [DOI] [PubMed] [Google Scholar]
- 3.Li L., Yao H., Wang J., Li Y., Wang Q. The role of Chinese medicine in health maintenance and disease prevention: application of constitution theory. The American Journal of Chinese Medicine. 2019;47(3):495–506. doi: 10.1142/S0192415X19500253. [DOI] [PubMed] [Google Scholar]
- 4.Wang Q. Physical identification is “Treat the disease” of ‘Gripper’. Global Traditional Chinese Medicine. 2008;4(3):5–6. [Google Scholar]
- 5.Zhu Y. B., Wang Q., Origasa H. Evaluation on reliability and validity of the constitution in Chinese medicine questionnaire (CCMQ) Chinese Journal of Behavioral Medicine Science. 2007;16(7):651–654. [Google Scholar]
- 6.Wang Q. Individualized medicine, health medicine, and constitutional theory in Chinese medicine. Frontiers of Medicine. 2012;6(1):1–7. doi: 10.1007/s11684-012-0173-y. [DOI] [PubMed] [Google Scholar]
- 7.Wells G., Shea B., O’Connell D., Peterson J. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-randomized Studies in Meta-Analysis. Ottawa, Canada: Ottawa Hospital Research Institute; 2000. [Google Scholar]
- 8. A. Rostom, C. Dube, and A. Cranney, Summary, Evidence Report/technology Assessment No 104 (Prepared by the University of Ottawa Evidence-Based Practice Center, under contract, No. 290-02-0021), 2004.
- 9.Luo M. L., Tan H. Z., Zhou Q. Realizing the meta-analysis of single rate in R. The Journal of Evidence-Based Medicine. 2013;13:181–184. [Google Scholar]
- 10.Li C. Identification and analysis of TCM constitution of diabetic population in lujiang community of zhangshu city. The Medical Forum. 2020;24(31):4579–4580. [Google Scholar]
- 11.Zhong X. Y., Xue L. Effects of TCM biased constitution on type 2 diabetes mellitus and impaired glucose regulation. Chinese and Foreign Medical Research. 2020;18(16):126–127. [Google Scholar]
- 12.Liu Y. W., Zhang K. W., Ji H. Y., et al. Correlation between the constitution of type 2 diabetes mellitus and the twelve meridians was discussed based on palmar meridians detection instrument. Henan Traditional Chinese Medicine. 2020;40(1):120–122. [Google Scholar]
- 13.Zhang S., Zhang S. X., Ling Y., et al. Investigation of traditional Chinese medicine constitution types in 120 patients with type 2 diabetes and comparison of different constitution-related glucose metabolism indexes. Shanghai Journal of Traditional Chinese Medicine. 2020;54(1):7–10. [Google Scholar]
- 14.Wu L. Y., Liu W., Liu X. X. The intervention study of TCM constitution identification on hypertension and type 2 diabetes mellitus. Nei Mongol Journal of Traditional Chinese Medicine. 2019;38(8):77–80. [Google Scholar]
- 15.Wang J. N., Du L. Y., Zhao Y. W., et al. Correlation and mechanism between constitution in traditional Chinese medicine and mild cognitive impairment of patients with type 2 diabetes mellitus. Shandong Journal of Traditional Chinese Medicine. 2019;38(11):1031–1036. [Google Scholar]
- 16.Shen Y., Tang H., Zhou D., et al. Association of TCM constitution with gene polymorphisms of interleukin-6, interleukin-10, and interleukin-10 receptor 1 in patients with type 2 diabetes. Journal of Anhui University of Chinese Medicine. 2019;38(3):6–11. [Google Scholar]
- 17.Lin H. K., Huang W. F., Zhan W. B., et al. Investigation on the constitution type of Chinese medicine in middle-aged and old patients with type 2 diabetes. Shenzhen Journal of Integrated Traditional Chinese and Western Medicine. 2019;29(8):59–60. [Google Scholar]
- 18.Li W. C., Feng J., Liu L. L. Analysis of constitution identification of type 2 diabetes mellitus. Yiyaojie. 2019;6:p. 40. [Google Scholar]
- 19.Huang J. H., Zhu W. X., Xia Q., et al. Study on the relationship between sympathetic activity of autonomic nervous system and vagal activity, their balances and coordination in patients with diabetes mellitus with different constitutions of traditional Chinese medicine. Guangzhou Medical Journal. 2019;3:84–87. [Google Scholar]
- 20.Guan X. L. Analysis and discussion on constitution of traditional Chinese medicine in community patients with type 2 diabetes mellitus. Journal of Community Medicine. 2019;17(9):529–531. [Google Scholar]
- 21.Guan H. The Implementation and Effect Evaluation of Constitution Intervention in the Health Management of Type 2 Diabetes Mellitus. Luzhou, China: Southwest Medical University; 2019. [Google Scholar]
- 22.Zhang Y., Zhang Y. Y., Yang R. W., et al. Establishment and verification of diabetes risk assessment model based on TCM constitution identification. Chinese General Practice. 2020;23(637):68–73. [Google Scholar]
- 23.Zhou B. W. Study on the Relationship between the Constitution Type and the Main Risk Factors of Cardiovascular System in Type 2 Diabetic Patients. Fujian, China: Fujian University of traditional Chinese Medicine; 2018. [Google Scholar]
- 24.Wei M. H., Yang Y. J. Investigation on the constitution of traditional Chinese medicine of type 2 diabetes mellitus and prediabetes at Panyu District, Guangzhou. International Medicine and Health Guidance News. 2018;24(4):480–482. [Google Scholar]
- 25.Wang X. Relationship between body type and correlation index of diabetic patients in Baotou area. Journal of Baotou Medical College. 2018;34(6):85–87. [Google Scholar]
- 26.Lin H. J., Jiang Y., Liu Y. J., et al. Influence of family health guidance on blood glucose of diabetic patients based on constitution identification of traditional Chinese Medicine. Guide of China Medicine. 2018;16(16):196–197. [Google Scholar]
- 27.Li K., Lin Y. X., Ma L. R., et al. Yuan identification of TCM constitution and function of islet β cells in patient with newly onset type 2 diabetes. Journal of Traditional Chinese Medicine. 2018;33(9):48–50. [Google Scholar]
- 28.Lang N. Study on the relationship between different constitution of traditional Chinese medicine and endothelial function in the elderly with diabetes mellitus. Journal of Clinical Medical Literature Electronic Edition. 2018;5(89):p. 21. [Google Scholar]
- 29.Jiang L. H., Wong Z. F., Hu X. Y. The influence of prevention and treatment of integrated traditional Chinese and Western Medicine on the constitution of community diabetes patients. Chinese Journal of Information on Traditional Chinese Medicine. 2018;25(2):20–25. [Google Scholar]
- 30.Hu L. P., Wang D. H., Li J. H. Correlation between socioeconomic status and TCM constitution in 200 patients with Type 2 diabetes mellitus. Hebei Journal of Traditional Chinese Medicine. 2018;40(2):187–191. [Google Scholar]
- 31.Gao Y. H., Zhang A. L., Yang H. B., et al. Study on the constitution identification and syndrome differentiation of the elderly patients with diabetes and hypertension. Hebei Journal of Traditional Chinese Medicine. 2018;40(11):46–49. [Google Scholar]
- 32.Chen W. Y., Cheng B. X., Wang L. Q. Observation on the effect of TCM Constitution Differentiation on community management of type 2 diabetes in the elderly. Modern Medicine and Health Research. 2018;2(17):p. 144. [Google Scholar]
- 33.Zhou D., Lin N. S., Wang F., et al. Correlation analysis of Traditional Chinese medicine Constitution type and blood glucose control in type 2 diabetes patients. Health Education and Health Promotion. 2017;12(3):200–203. [Google Scholar]
- 34.Wang J. Relationship between lifestyle and Traditional Chinese medicine Constitution in patients with chronic disease diabetes. Chinese Practical Medicine. 2017;9:187–188. [Google Scholar]
- 35.Shen Y., Tang H., Zhou D. Research on distribution characteristics of TCM constitution of patients with type 2 diabetes mellitus and related risk factors. World Chinese Medicine. 2017;12(10):2487–2491. [Google Scholar]
- 36.Shen B., Yu C., Yu W., et al. Investigation and analysis of TCM constitution of 333 patients with type 2 diabetes in beijing pinggu district. Chinese medicine Modern Distance Education of China. 2017;15(16):58–60. [Google Scholar]
- 37.Qiu J. L. Effect of Characteristic Health Education Based on Constitution Recognition of Traditional Chinese Medicine on Metabolic Control of Diabetic Patients. Wulumuqi, China: Xinjiang Medical University; 2017. [Google Scholar]
- 38.Lv J. X. Study on the Relationship between the Constitution of Traditional Chinese Medicine and Risk Factors in Type 2 Diabetes Mellitus. Tianjin, China: Tianjin University of traditional Chinese Medicine; 2017. [Google Scholar]
- 39.Liu Y., Zhu H. Y., Wu Q. S. Study on the level of inflammatory factors in diabetic patients with different constitution of traditional Chinese Medicine. Heilongjiang Medicine and Pharmacy. 2017;40(3):p. 121. [Google Scholar]
- 40.Li X. Analysis of the effect of TCM Constitution identification on the treatment and intervention of elderly diabetes patients in the community. Health and Nutrition in China. 2017;27(1):p. 383. [Google Scholar]
- 41.Jing G. C., Gu W. J., Zhang M. R. Study on relationship between constitution of TCM and personality characteristics of patients with type 2 diabetes mellitus. China Journal of Traditional Chinese Medicine and Pharmacy. 2017;32(11):4946–4948. [Google Scholar]
- 42.Jing Y. J. Correlation Analysis of Multiple Factors in Type 2 Diabetes Patients with Qi-Deficiency Constitution. Kunming, China: Yunnan College of Traditional Chinese Medicine; 2017. [Google Scholar]
- 43.Huang Q. Study on TCM Constitution Intervention of “2394” Chronic Disease Management Model in Type 2 Diabetes Patients. Guangzhou, China: Southern Medical University; 2017. [Google Scholar]
- 44.Huang Q., Zhao X. S., Sun S. N., et al. TCM constitutional types and cardiovascular risk factors on 367 type 2 diabetic patients. Chinese Archives of Traditional Chinese Medicine. 2017;35(1):229–232. [Google Scholar]
- 45.Huang Q., Wang W. R., Tan J. F., et al. Observation of TCM constitutions in patients with different stroke risks in type 2 diabetes mellitus. Zhejiang Medical Education. 2017;16(5):46–48. [Google Scholar]
- 46.Zhu Y. B., Shi H. M., Wang Q., et al. Association between nine types of TCM constitution and five chronic diseases: a correspondence analysis based on a sample of 2660 participants. Evidence-Based Complementary and Alternative Medicine. 2017;2017:7. doi: 10.1155/2017/9439682.9439682 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Feng J. Application of TCM Constitution identification in health management of community diabetes. Health Care Guide. 2017;5:46–48. [Google Scholar]
- 48.Zou J. X., Wang W. P. Investigation of TCM syndrome type and Constitution type in type 2 diabetes patients. Health Nutrition in China. 2016;26(25):p. 149. [Google Scholar]
- 49.Zhu L., Liu L. G., Zhu L. Study on relationship between type 2 diabetes mellitus and constitution of inhabitants in community. Journal of Inhabitants in Community,” Clinical And Experimental Medicine. 2016;26(12):1169–1174. [Google Scholar]
- 50.Xue J. L., Li M. Z., Gong Y. Z. The characteristics of TCM constitution in type 2 diabetes patients in Baoshan District, Shanghai. Shanghai Preventive Medicine. 2016;28(7):453–459. [Google Scholar]
- 51.Xu Y. M., Liu D. Investigation and Analysis on the constitution type of traditional Chinese medicine in the elderly patients with type 2 diabetes in the community. Shanxi Journal of Traditional Chinese Medicine. 2016;32(2):45–46. [Google Scholar]
- 52.Xie H. J., Zhang G. F., Peng Y. J., et al. Investigation and analysis of TCM constitution characteristics of 426 elderly patients with type 2 diabetes in Zhengzhou city. Clinical Research of Traditional Chinese Medicine. 2016;8(13):27–29. [Google Scholar]
- 53.Wang Z. W., yang J. Y., Lei B., et al. Effect of TCM constitution regulation on treatment effect and life quality of elder patients with type 2 diabetes mellitus. World Chinese Medicine. 2016;11(8):1606–1609. [Google Scholar]
- 54.Wang K. F., Yan Q., Li C. M. Characteristics and correlation analysis of Traditional Chinese medicine constitution in 300 diabetic patients in Qitaihe Area. Diet Care. 2016;3(12) [Google Scholar]
- 55.Wang J. S. The Correlation Study of Efficacy of Exenatide or Saxapliptin in Type 2 Diabetes and Plasma GC, Chinese Medicine Body Constitution. Chengdu, China: Chengdu University of Traditional Chinese Medicine; 2016. [Google Scholar]
- 56.Ren Z. Z., Zhao H., Yang L., et al. Research on application of TCM constitution identification and individual health management guidance in type 2 diabetes of community. Guangming Journal of Chinese Medicine. 2016;31(18):2603–2604. [Google Scholar]
- 57.Li Z. A clinical analysis of TCM constitution distribution of hypertension and diabetes and treating different diseases by the same method. Clinical Journal of Chinese Medicine. 2016;8(4):70–71. [Google Scholar]
- 58.Li J., Zhu Y., Chen Y. S., et al. Distribution of TCM constitutions in 302 patients with type 2 diabetes in Kunming. Chinese Medicine Research. 2016;29(1):11–13. [Google Scholar]
- 59.Huang W. B. Preliminary Research on Diabetic Patients’ TCM Body Constitution Among Malaysian Chinese in Klang Valley. Chengdu, China: Chengdu University of Traditional Chinese Medicine; 2016. [Google Scholar]
- 60.Hua Y. K., Yuan W., Be Y. P., et al. Investigation and analysis of TCM constitution among 931 patients with diabetes in yangpu district of shanghai. Guiyang College of Traditional Chinese Medicine. 2016;38(3):71–74. [Google Scholar]
- 61.Zou J. X., Wang W. P. Investigation on TCM syndrome type and constitution type of type 2 diabetes mellitus. China Health Nutrition. 2016;26(25):p. 149. [Google Scholar]
- 62.Zhao Z. Y. The Correlation Research of Dangerous TCM Constitution and Type 2 Diabetes Mellitus in Inner Mongolia Region. Neimongol, China: Inner Mongolia Medical University; 2015. [Google Scholar]
- 63.Zhang B. Discussion on the relationship between the onset of diabetes and the constitution of traditional Chinese Medicine. Biotech World. 2015;10:268–269. [Google Scholar]
- 64.Yu J. Traditional Chinese Medical Body Constitution, its Related Clinical Characteristics, and Diabetes-Associated Chronic Complications in Patients with Type 2 Diabetes. Dalian, China: Dalian Medical University; 2015. [Google Scholar]
- 65.Yang T. Studies on Building Platform of Type Diabetes Management in Qingdao Area Based on the Constitution Identification of Traditional Chinese Medicine. Qingdao, China: Qingdao University; 2015. [Google Scholar]
- 66.Xiang X. Y., Qian J. Q. Study on the relationship between TCM constitution characteristics and body mass index, fasting blood glucose in type 2 diabetes mellitus. Asia-Pacific Traditional Medicine. 2015;11(16):91–92. [Google Scholar]
- 67.Wu X. M., Hao Z. H. TCM constitution analysis of type 2 diabetic patients with different body mass index. Journal of Hubei University for Nationalities. 2015;32(3):21–23. [Google Scholar]
- 68.Wu Q. L., Guo S. R., Ke J. H., et al. Clinical investigation on the constitution of diabetes mellitus patients in Jinjiang area. Journal of Clinical Medical Literature. 2015;2(21):4486–4487. [Google Scholar]
- 69.Wei J. F., Liu Q., Chen J. G. Analysis on application effect of TCM constitution identification and intervention in the management of type 2 diabetes patients in community. Guiding Journal of Traditional Chinese Medicine and Pharmacy. 2015;21(13):35–38. [Google Scholar]
- 70.Wang G. Z., Zeng J. L., Zeng S., et al. Investigation report on constitution condition of type 2 diabetes patients in Meizhou Hospital of traditional Chinese Medicine. Guiding Journal of Traditional Chinese Medicine and Pharmacy. 2015;21(2):88–89. [Google Scholar]
- 71.Lu H. Analysis on the constitution of diabetes mellitus patients over 60 years old in Anting Town. The World Clinical Medicine. 2015;9(5):10–12. [Google Scholar]
- 72.Liu X. D., Lv X. Q., Liu N. W. Investigation on TCM syndrome types and TCM constitutions of II type diabetes. Shanxi Journal of Traditional Chinese Medicine. 2015;31(1):41–42. [Google Scholar]
- 73.Li Z. S. Analysis of risk factors of type 2 diabetes base on TCM constitution differentiate. Journal of Taishan Medical College. 2015;36(11):1218–1220. [Google Scholar]
- 74.Li J. H. Analysis of the Constitution Characteristics of the Elderly Patients with Diabetes Mellitus in Dongfu Community, Xiamen. Xiamen, China: Fujian University of Traditional Chinese Medicine; 2015. [Google Scholar]
- 75.Hu G. R., Zhang L., Zeng Y. H., et al. The clinical investigation and Research on the constitution of diabetes in Nanchang area. Journal of Practical Diabetology. 2015;11(1):33–34. [Google Scholar]
- 76.Chen L. J., Zhou J. Y. Study on the Distribution of TCM Constitution of Type 2 Diabetes in Patients with Constitution Identification. Zhejiang, China: Annual Meeting of Constitution of Traditional Chinese Medicine of Chinese Medical Association; 2015. [Google Scholar]
- 77.Xiao X. Y., Li B. Y., Zhou R. Investigation and analysis of TCM Constitution of type 2 diabetes patients in Sanshui District. Global Traditional Chinese Medicine. 2015;8(S2):p. 163. [Google Scholar]
- 78.Zhu L., Tian C. Y., Lin Q., et al. Study on the constitution of traditional Chinese medicine of type 2 diabetes in Tangshan. Journal of Clinical Medical Literature Electronic Edition. 2014;1(8):1419–1420. [Google Scholar]
- 79.Yang D. F., Wang W. R. General information. Asia-Pacific Journal of Clinical Oncology. 2014;10(2):49–50. doi: 10.1111/ajco.12285. [DOI] [Google Scholar]
- 80.Xiang X. Y., Ran Y. Z. Investigation on constitution type and TCM clinical Syndrome type of 270 patients with type 2 diabetes. World Traditional Chinese Medicine. 2014;9(12):1599–1602. [Google Scholar]
- 81.Xiang X. Y. Investigation on Constitution Type and TCM Clinical Syndrome Type of Patients with Type 2 Diabetes Mellitus in Liuhe District of Taicang City. Nanjing, China: Nanjing University of Chinese Medicine; 2014. [Google Scholar]
- 82.Wang H., Zhang X. H., Liu H. F. Study on the relationship between the Constitution and family heredity of type 2 diabetes. World Chinese Medicine. 2014;36(3):201–204. [Google Scholar]
- 83.Li Y. H., Yang J. Q., Huang X. L. The application of constitution identification in “preventive treatment” health management of diabetes in community. Journal of Zhejiang Chinese Medical University. 2014;38(4):120–122. [Google Scholar]
- 84.Chen J. Q., Guo Y. D., Zhu Y. Q., et al. Studies nanyang city in type 2 diabetes patients and their constitution characteristics and the relationship between TCM. China Journal of Chinese Medicine. 2014;29:338–340. [Google Scholar]
- 85.Zheng X. H., Jian Z. Y. Logistic regression analysis of the relationship between constitution fitness, impaired glucose regulation and diabetes mellitus in 1882 middle-aged and elderly people in Guangzhou community. International Journal of Traditional Chinese Medicine. 2013;35(6):481–484. [Google Scholar]
- 86.Wu X. Q., Luo Y. Y., Xu J. H. Investigation of traditional Chinese medical constitution of type 2 diabetes mellitus patients and its relationship with insulin resistance and insulin secretion. Journal of Guangzhou University of Traditional Chinese Medicine. 2013;30(3):312–315. [Google Scholar]
- 87.Tang L. L. Analysis of the Relationship between the Constitution Type of TCM and Sex, Age, Body Mass Index in Type 2 Diabetes Mellitus. Nanning, China: Guangxi University of Traditional Chinese Medicine; 2013. [Google Scholar]
- 88.Ma J. R. A study on the relationship between biased constitution of traditional Chinese medicine and diabetes mellitus and impaired glucose regulation. Clinical Journal of Integrated Traditional Chinese and Western Medicine. 2013;13(4):56–57. [Google Scholar]
- 89.Liu W. H. Correlation analysis of TCM Constitution with obesity, blood lipid and hemagglutination index in type 2 diabetes. Guide of China Medicine. 2013;11(8):624–625. [Google Scholar]
- 90.Li L. F., Tang W. H., Wang Y. Q., et al. Relationship between TCM constitution and B-cell function in patients with type 2 diabetes. Jilin Journal of Traditional Chinese Medicine. 2013;33(1):45–47. [Google Scholar]
- 91.Zhang J. N., Zhang L., Luo R. Analysis of Related Factors of TCM Constitution in Hong Kong Diabetes Patients. Haikou, China: China Association of Chinese Medicine; 2011. [Google Scholar]
- 92.Han W. T. A Study on the Constitution of TCM in Type 2 Diabetes Mellitus. Beijing, China: Beijing University of traditional Chinese Medicine; 2011. [Google Scholar]
- 93.Han P., Bai X. Q., Lou Y. M., et al. Analysis of the relationship between the biased constitution of traditional Chinese medicine and the impairment of diabetes and glucose regulation. Beijing Journal of Traditional Chinese Medicine. 2011;30(9):656–658. [Google Scholar]
- 94.Zhang J. N. Study on the Constitution Characteristics of TCM in 534 Patients with Type 2 Diabetes Mellitus. Guangzhou, China: Southern Medical University; 2010. [Google Scholar]
- 95.Yan Y., Zhu P., Zhang F., et al. Cases of type 2 diabetes and related major. China Journal of Chinese Medicine. 2010;25(6):1154–1156. [Google Scholar]
- 96.Cui G. A Survey of the Common Constitution Types of Diabetes Mellitus in Xianyang Area and its Health Management. Xianyang, China: Shanxi University of Traditional Chinese Medicine; 2009. [Google Scholar]
- 97.Li M., Mo S., Lv Y., et al. A study of traditional chinese medicine body constitution associated with overweight, obesity, and underweight. Evidence-Based Complementary and Alternative Medicine. 2017;2017:8. doi: 10.1155/2017/7361896.7361896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.China Association of Chinese Medicine. Classification and Determination of TCM Constitution. Beijing, China: China Press of TCM; 2009. [Google Scholar]
- 99.Li L., Feng J., Yao H., et al. Gene expression signatures for phlegm-dampness constitution of Chinese medicine. Science China Life Sciences. 2017;60(1):105–107. doi: 10.1007/s11427-016-0212-9. [DOI] [PubMed] [Google Scholar]
- 100.Liang X., Wang Q., Jiang Z., et al. Clinical research linking Traditional Chinese Medicine constitution types with diseases: a literature review of 1639 observational studies. Journal of Traditional Chinese Medicine=Chung I Tsa Chih Ying Wen pan. 2020;40(4):690–702. doi: 10.19852/j.cnki.jtcm.2020.04.019. [DOI] [PubMed] [Google Scholar]
- 101.Zhu Y. B., Wang Q. Epidemiological investigation of constitution types of Chinese Medicine in general population: based on 21,948 epidemiological investigation date of nine provinces in China. Journal of Traditional Chinese Medicine and Pharmacy. 2009;24(1):7–12. [Google Scholar]
- 102.Zou D., Ye Y., Zou N., Yu J. Analysis of risk factors and their interactions in type 2 diabetes mellitus: a cross-sectional survey in Guilin, China. Journal of Diabetes Investigation. 2017;8(2):188–194. doi: 10.1111/jdi.12549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Luo H., Li L., Li T., Liao X., Wang Q. Association between metabolic syndrome and body constitution of traditional Chinese medicine: a systematic review and meta-analysis. Journal of Traditional Chinese Medical Sciences. 2020;7(4):355–365. doi: 10.1016/j.jtcms.2020.10.004. [DOI] [Google Scholar]
- 104.Ma Y. L., Yao H., Yang W. J., et al. Correlation between traditional Chinese medicine constitution and dyslipidemia: a systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine. 2017;2017:7. doi: 10.1155/2017/1896746.1896746 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The relevant data used to support the results of this study are included in this article.