

Abstract
Objectives
This study aimed at examining health sufferings of readymade garments (RMG) workers, the factors that affect their health sufferings, their healthcare seeking pattern, knowledge about health insurance and health related rights in Bangladesh.
Methods
A cross‐sectional study was conducted among 486 RMG workers recruited randomly from eight garments factories located on the periphery of Dhaka, Bangladesh. The prevalence of musculoskeletal pain, headache, fever and abdominal pain was estimated and multivariable logistic regression analysis was performed to examine association between these illnesses of workers and their socio‐demographic characteristics and other work related information. We also explored their healthcare seeking patterns, knowledge about health insurance and health related rights.
Results
The prevalence of musculoskeletal pain, headache, fever and abdominal pain was found to be 78.1%, 57.9%, 52.2% and 24.6%, respectively, among the RMG workers. Factors that increased the odds of: musculoskeletal pain were working for more than 10 h per day (adjusted odds ratio [AOR]: 2.3, 95% confidence interval [CI]: 1.1–4.7) and being female [AOR: 4.6, 95% CI: 2.0–10.6]; fever was living in slums [AOR: 1.9, 95% CI: 1.1–3.5]; and abdominal pain was being female [AOR: 3.6, 95% CI: 1.4–9.3]. The workers commonly reported visiting drug sellers in local pharmacies for reported illnesses. They also had better knowledge of health related rights but poor knowledge of health insurance.
Conclusion
In order to address the overall health and well‐being of the RMG workers, it is imperative to lay out a blueprint for a safe and healthy workplace.
Keywords: Bangladesh, health rights, health status, healthcare seeking behavior, readymade garments workers
1. BACKGROUND
Readymade garments (RMG) sector is the most important and contributing industrial sector of Bangladesh’s economy. In the past fiscal year (2018–2019), Bangladesh earned US$40.53 billion through export, of which 84.21% came from the RMG sector. Started back in 1980 with only 12 garment factories, the sector now encompasses 4621 factories employing around 4.0 million workers of which more than 60% are women.1 Because of the enormous job creation, steady growth, poverty reduction and female empowerment, it is often argued that the RMG sector is the lifeline of Bangladesh economy and the country’s economic development largely depends on the growth and sustainability of this sector.2, 3, 4
Despite significant achievement of the RMG sector in the past decades and its bright prospects in the future, many challenges remain that are yet to be solved. Some of these challenges are related to deprivations of its workers which include poor working conditions, non‐compliance with minimum wages, weak legal provisions and lack of provision of essential service benefits for the workers.5, 6, 7 Previous research has indicated that the informal nature of job coupled with poor working conditions, prolonged working hours and inadequate dietary intake are some of the factors associated with worse health outcomes of RMG workers.8, 9, 10 On average, more than half of the RMG workers work for 10 h per day whereas standard working hours as per International Labour Organization (ILO) recommendation are 8 h.11 A recent study by Oxfam Australia in 2019 among 384 RMG workers revealed that 90% of the workers cannot afford food for themselves and their families and about two thirds (72%) cannot afford medical treatment when they get sick or injured.9 Another study found a very high prevalence (79%) of illness among the RMG workers. Out of 522 RMG workers participated in the study, 40.5% reported suffering from diarrhea, 22.5% from common cold and 15.1% from respiratory tract infection in the last 2 months preceding the survey. Surprisingly, more than half (56%) of the sufferers sought treatment from Local Medical Assistant and Family Welfaredoctors followed by 21% from local drug shops and 10% from herbal medicine practitioners locally known as kabiraj.5
Overall, there is a lack of research evidence on the health suffering of RMG workers, their healthcare seeking pattern, knowledge about health rights, attitudes towards health insurance and barriers to formal healthcare utilization in Bangladesh. The studies described above explored some of these issues; however to our knowledge there has not been any study conducted in Bangladesh that comprehensively explored all the issues faced by them. This study aimed to fill this knowledge gap by presenting results obtained from a cross‐sectional study conducted among a representative sample of RMG workers in Bangladesh.
2. METHODS
The study uses data from a cross‐sectional study conducted between August and December, 2018 in Gazipur, Savar and Tongi areas of Bangladesh where BRAC Urban Development Program (UDP) is implementing a project titled “Empowering the Ready‐Made Garments Workers Living in Urban Slums (ERMG)”. More detail about the ERMG project and BRAC UDP program is available at http://www.brac.net/program/urban‐development/.
A representative survey was conducted among 486 RMG workers (190 males and 296 females) recruited from eight garments factories in Savar, Gazipur and Tongi areas. Savar is a small sub‐district (Upazila) of Dhaka district with a population of 1 385 910 and an area of 280.13 square kilometers. Gazipur is a district adjacent to Dhaka district with a population of 34 03 912 and an area of 1806.4 square kilometers. Tongi is a major township in Gazipur district with an area of 32.1 square kilometers and a population of 4 06 424.12 Sample size for the survey was calculated to be 486 assuming that the prevalence of different health sufferings, healthcare seeking behavior, knowledge about health insurance and health related rights ranges from 30% to 70% and with 95% confidence level, 5% level of significance and with a design effect of 1.5.13 For randomly recruiting the 486 RMG workers, we developed a comprehensive list of workers by collecting employee lists from 8 RMG factories where BRAC UDP had access at the time of the survey. From the list, 190 male and 296 female RMG workers were proportionately selected and asked to participate in the survey. The survey questionnaire included 10 sections in total, such as characteristics of the RMG workers, their housing characteristics and families, their job/work related information, health sufferings and healthcare service utilization, financial behavior, skills training, communicative literacy and barriers in using online digital support platform, legal aid support need, owner‐employee relationships, government and non‐government organizations (NGOs) service utilization. On average, each survey interview took about 45 min. The survey questionnaire was pretested before final data collection. A group of 16 field research assistants were involved in the survey data collection process. All of them received training before the survey. The topics covered in the training included different aspects of research ethics, rapport building with the respondents, understanding the research objectives, sampling methodology and survey questionnaire.
Survey data were analyzed using statistical software Stata (Stata version 13). Both descriptive and multivariable analyses were performed. Descriptive analyses findings are presented in statistical tables and graph. The prevalence of different health sufferings was calculated by using the data on whether the respondents had suffered from any illnesses in the last 3 months preceding the survey. Four common illnesses—musculoskeletal pain, headache, fever and abdominal pain were considered as outcomes for multivariable logistic regression analysis. In this study, musculoskeletal pain referred to back pain, neck pain, wrist pain, shoulder pain, knee pain or external chest pain.14 Headache was defined as a condition that causes pain in any region of the head.15 Fever was defined as a condition of having a temperature above the normal range of body temperature.16 Abdominal pain was defined as pain that occurs between the chest and pelvic region.17 For logistic regression analysis, each of the outcome variables (musculoskeletal pain, headache, fever and abdominal pain) was considered as dichotomous with “1” indicating the presence of the illness and “0” indicating the absence of the illness among the respondents. The predictor variables considered were: age and gender of the respondents, educational attainment, working hours in a day, years of experience in the RMG sector, status of current job (either first job or not) and types of households (slum or non‐slum). A slum household was defined as a dwelling unit where one or a group of individuals live under the same roof with insufficient living area, inadequate access to water supply, sanitation facility and a lack of secure tenure and durable housing.18 These variables were chosen as they were deemed to be epidemiologically important that may influence the outcomes mentioned earlier. In addition to exploring the health sufferings of the respondents, we also explored their healthcare seeking behavior, knowledge about health insurance and health related rights. The respondents were asked several questions related to health insurance such as “do you know about health insurance?” and if a respondent answered “yes,” she/he was further asked “what do you know about health insurance?”. Similarly, they were asked “do you know the right to get sick leave?” and if someone answered “yes” she/he was further asked “from whom you learned about this right?”.
3. RESULTS
3.1. Characteristics of the survey respondents
Table 1 shows demographic characteristics of the 486 RMG workers interviewed in the survey. Most of the respondents (61%) were female. About 30% of them were from the age group 31 years and above followed by 24.5% from the age group 23–26 years. Only one‐fifth (20.1%) completed their secondary level education. Majority of them (86.2%) were married and almost two‐thirds (63.6%) were from Savar area (Table 1).
TABLE 1.
Characteristics of the 486 respondents interviewed in the survey
| Background characteristics | Frequency | Percentage (%) |
|---|---|---|
| Gender | ||
| Male | 190 | 39.1 |
| Female | 296 | 60.9 |
| Age in years | ||
| 18–22 years | 105 | 21.6 |
| 23–26 years | 119 | 24.5 |
| 27–30 years | 117 | 24.1 |
| 31 Years and above | 145 | 29.8 |
| Education | ||
| No education | 57 | 11.7 |
| Primary incomplete | 39 | 8.0 |
| Primary complete | 105 | 21.6 |
| Secondary incomplete | 187 | 38.5 |
| Secondary complete and above | 98 | 20.1 |
| Marital status | ||
| Married | 419 | 86.2 |
| Never married | 67 | 13.8 |
| Living area | ||
| Gazipur | 136 | 27.9 |
| Savar | 309 | 63.6 |
| Tongi | 41 | 8.4 |
3.2. Health suffering of the RMG workers
Among the 486 survey respondents, 228 (47%) mentioned that they have suffered from at least one illness in the preceding three months of the date of survey. Of these 228 respondents, 70 were male and 158 were female. Figure 1 shows frequency of different types of illnesses suffered by the respondents. Female RMG workers reported suffering more from musculoskeletal pain than the male workers and the difference in prevalence was found to be statistically significant (P value < .05). For the other types of illnesses such as headache, fever, abdominal pain, eye and breathing problem, the trend was similar, ie, female workers reported suffering more from these conditions than male workers although the differences in prevalence were not statistically significant (Figure 1).
FIGURE 1.
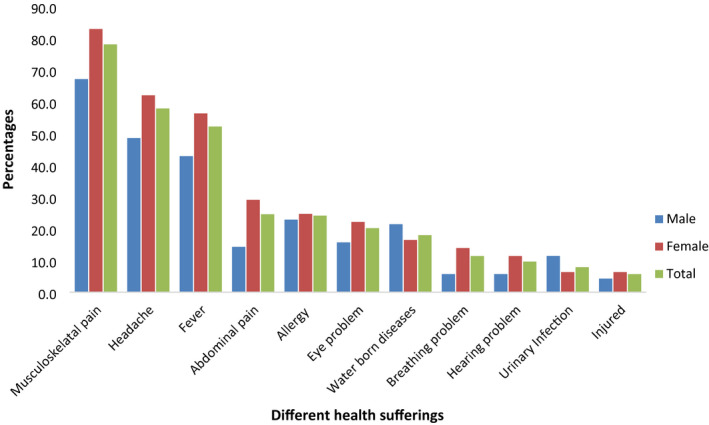
Different types of illnesses suffered by RMG workers in the last 3 months preceding the survey. Chi‐square tests were performed to examine the association between different types of illnesses suffered by the RMG workers and their gender status in the last 3 months preceding the survey. Only difference in prevalence of musculoskeletal pain was found to be statistically significant at 5% level of significance (P value < .05)
3.3. Factors associated with illnesses suffered by the RMG workers
Table 2 reports logistic regression analysis findings that examined the association between different illnesses (musculoskeletal pain, headache, fever and abdominal pain) of the RMG workers and their socio‐demographic characteristics and other work related information. In the adjusted model where musculoskeletal pain was considered as an outcome variable, female workers were found 4.6 times more likely (adjusted odds ratio [AOR]: 4.6, 95% confidence interval [CI]: 2.0–10.6) to report suffering from musculoskeletal pain than their male counterparts. Respondents who worked for more than 10 h in a day were found 2.3 times more likely [AOR: 2.3, 95% CI: 1.1–4.7] to report suffering from various musculoskeletal pain than those worked for ≤10 h. For the outcome variable headache, workers who have been working in the RMG sector for more than 10 years were found 0.2 times less likely [AOR: 0.2, 95% CI: 0.1–0.7] to report suffering from headache than those working for <2 years. Female workers were found 3.6 times more likely [AOR: 3.6, 95% CI: 1.4–9.3] to report suffering from abdominal pain than their male counterparts. Finally, for the outcome variable fever, RMG workers who reported living in the slums were found two times more likely [AOR: 1.9; 95% CI: 1.1–3.5] to suffer from fever than those living in non‐slum areas (Table 2).
TABLE 2.
Factors associated with musculoskeletal pain, headache, fever and abdominal pain suffered by the survey respondentsa
| Variables | Musculoskeletal pain | Headache | Fever | Abdominal pain | ||||
|---|---|---|---|---|---|---|---|---|
| AOR (95% CI) | P‐value | AOR (95% CI) | P‐value | AOR (95% CI) | P‐value | AOR (95% CI) | P‐value | |
| Gender | ||||||||
| Male | Ref. | |||||||
| Female | 4.6 (2.0 10.6) | 0.00 | 1.5 (0.7 3.1) | 0.26 | 1.8 (0.9 3.7) | 0.11 | 3.6 (1.4 9.3) | 0.01 |
| Education status | ||||||||
| No education | Ref. | |||||||
| Primary incomplete | 0.4 (0.1 1.6) | 0.18 | 0.6 (0.2 2.1) | 0.41 | 0.8 (0.2 3.0) | 0.77 | 2.4 (0.6 10.4) | 0.23 |
| Primary complete | 0.8 (0.3 2.8) | 0.77 | 0.7 (0.3 1.8) | 0.45 | 0.7 (0.2 1.7) | 0.39 | 1.9 (0.6 6.7) | 0.30 |
| Secondary incomplete | 1.2 (0.4 3.5) | 0.78 | 0.8 (0.3 2.1) | 0.71 | 0.9 (0.4 2.2) | 0.78 | 2.2 (0.7 7.0) | 0.17 |
| Secondary complete and above | 2.3 (0.5 9.4) | 0.26 | 0.5 (0.2 1.7) | 0.26 | 0.7 (0.2 2.4) | 0.62 | 5.1 (1.2 22.0) | 0.03 |
| Age in years | ||||||||
| 18–22 years | Ref. | |||||||
| 23–26 years | 0.6 (0.2 1.9) | 0.39 | 1.1 (0.4 2.9) | 0.86 | 1.0 (0.4 2.7) | 0.93 | 0.9 (0.3 2.7) | 0.90 |
| 27–30 years | 1.0 (0.3 3.3) | 0.97 | 1.2 (0.4 3.4) | 0.76 | 1.3 (0.5 3.5) | 0.64 | 0.8 (0.3 2.6) | 0.76 |
| Above 30 years | 1.0 (0.3 3.4) | 0.96 | 0.8 (0.3 2.4) | 0.72 | 1.3 (0.5 3.7) | 0.61 | 0.7 (0.2 2.2) | 0.48 |
| Marital status | ||||||||
| Unmarried | Ref. | |||||||
| Married | 0.6 (0.2 2.2) | 0.46 | 1.6 (0.6 4.5) | 0.37 | 0.4 (0.1 1.1) | 0.09 | 1.1 (0.3 3.7) | 0.85 |
| Type of residence | ||||||||
| Non‐slum | Ref. | |||||||
| Slum | 1.0 (0.5 2.0) | 0.92 | 1.1 (0.6 2.0) | 0.79 | 1.9 (1.1 3.5) | 0.03 | 1.5 (0.7 2.9) | 0.27 |
| Working hours in a day | ||||||||
| Less than 10 h | Ref. | |||||||
| More than 10 h | 2.3 (1.1 4.7) | 0.03 | 1.4 (0.8 2.6) | 0.23 | 0.9 (0.5 1.6) | 0.68 | 1.4 (0.7 2.7) | 0.37 |
| First job or not | ||||||||
| First job | Ref. | |||||||
| Not first job | 1.3 (0.6 2.9) | 0.53 | 1.5 (0.8 2.8) | 0.26 | 1.1 (0.6 2.0) | 0.88 | 1.0 (0.5 2.2) | 0.92 |
| Year of experience in RMG sectors | ||||||||
| Less than 2.0 years | Ref. | |||||||
| 2.0–5.0 years | 1.7 (0.6 4.6) | 0.33 | 1.0 (0.4 2.5) | 0.95 | 1.0 (0.4 2.3) | 0.99 | 1.2 (0.5 3.2) | 0.67 |
| 5.0–10.0 years | 1.4 (0.5 4.2) | 0.53 | 0.4 (0.1 1.0) | 0.04 | 0.8 (0.3 2.0) | 0.64 | 1.8 (0.6 5.2) | 0.28 |
| More than 10.0 years | 1.9 (0.5 7.4) | 0.38 | 0.2 (0.1 0.7) | 0.01 | 0.3 (0.1 1.1) | 0.06 | 0.9 (0.2 3.8) | 0.90 |
AOR, adjusted odds ratio; CI, confidence interval; Ref, reference category
Results from multivariable logistic regression analysis adjusted for gender, education, age, marital status, residence, working hours, first job and year of experience of the respondents.
3.4. Healthcare seeking pattern for reported illnesses
Among the 228 survey respondents who reported suffering from at least one illness, only 193 sought healthcare. Of these`193 respondents, 138 were female and 55 were male. Figure 2 shows choice of providers according to the gender of the respondents. It is clear that irrespective of being male or female, respondents’ first choice of provider was a drug seller in local pharmacy. However, about one‐fifth (18.1%) of females also reported visiting private clinic (18.1%) followed by factory clinic (13.8%) for healthcare. Among the males, many (18.2%) visited NGO run health clinic followed by 14.6% reported visiting factory clinic for healthcare. The differences in proportion of males and females visiting different health facilities were not found to be statistically significant except for government Upazila health complexes (Figure 2). Upazila health complexes are primary level health care facilities located at the sub‐districts in all geographical regions of Bangladesh.19
FIGURE 2.
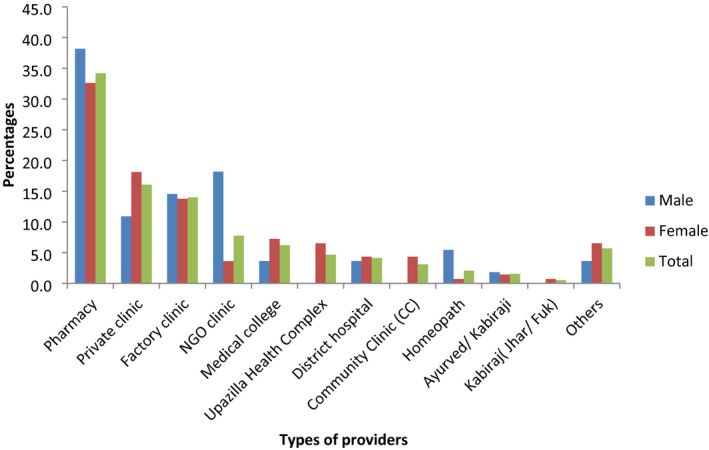
Healthcare seeking pattern of the RMG workers for reported illnesses. Chi‐square tests were performed to examine the association between gender of the respondents and their healthcare seeking pattern. The association was found to be statistically significant only for the category Upazila Health Complex (P value < .05)
3.5. Health insurance
Figure 3 presents health insurance related knowledge of the survey respondents. Surprisingly, only 51 respondents (10.5%) knew about health insurance. Of these 51 respondents, 33 were male and 18 were female. Among the 33 male respondents, 18 reported having a health insurance plan whereas among the 18 female respondents, 14 reported having a health insurance plan (Figure 3).
FIGURE 3.

Knowledge about health insurance and having health insurance plan of the RMG workers
3.6. Knowledge about health rights
Figure 4 shows awareness of health related rights among the survey respondents. Almost all the female respondents (99.3%) reported that they are aware of the right to enjoy maternity leave. They were also aware of the right to get sick leave (95.3%) and medical allowance (87.4%). Among the males, 96.8% were aware of the right to get sick leave and 79.1% were aware of the right to receive medical allowance. The differences in knowledge of health related rights among the male and female respondents were not found to be statistically significant (Figure 4).
FIGURE 4.
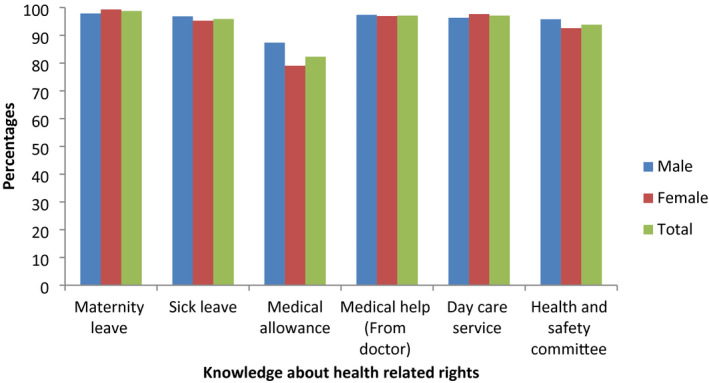
Knowledge about health related rights among the RMG workers. Chi‐square tests were performed to examine the association between gender of the respondents and their knowledge about different health rights. No statistically significant differences were observed
4. DISCUSSION
The study found that the prevalence of different types of illnesses such as musculoskeletal pain, headache fever and abdominal pain is high among the study respondents and varies according to gender. Overall, female RMG workers reported suffering more from different illnesses than male RMG workers. This finding is consistent with previous study findings.5, 20 The factors that increased the odds of musculoskeletal pain among the respondents were being female and engagement in prolong working hours. It is important to note that women are more susceptible to develop musculoskeletal disorder then men when performing repetitive work for longer period of time such as the work done in the garment factories.21 However, research has shown that if working conditions can be improved, this difference in experience of musculoskeletal disorder can be minimized.22, 23, 24 Overall, it can be recommended that there is a need to provide healthy tips and implementing some changes so that workers can maintain healthy posture at the workplace, such as changing posture at a regular interval, periodic short breaks for stretching out to minimize the burden of musculoskeletal disorder among the RMG workers, etc.
The study findings suggest that RMG workers living in informal settlements or slums are more likely to report suffering from fever than those living in non‐slum areas. This is reasonable since it is well known that slum dwellers do not adequately enjoy the benefits of urban living and quite often they have poor access to health services and basic facilities or amenities such as water, sanitation and waste management services than son‐slum dwellers which make them more susceptible to suffer from different health ailments.25, 26 The poor wage structures of the RMG sector often place no choice to the workers but to live in slums, which are lower in rent but with little basic services. The workers often struggle to meet the basic needs of their families with their meager average monthly income of BDT 8000 (USD 120). It is, therefore, important to revise the minimum wage structure so that workers can live in decent housing, get healthcare when they are sick, and buy adequate nutritious food.9
The study also revealed that most of the RMG workers irrespective of their gender visit drug sellers at local pharmacies for seeking healthcare. This is not surprising since the drug sellers are popular informal healthcare providers among the poor and disadvantaged communities in Bangladesh. They prescribe drugs based on the symptoms of illness and do not take extra money for the consultation, but build relationships and do make a profit by selling the medicines.27, 28 The workers only visit qualified healthcare providers such as Bachelor of Medicine, Bachelor of Surgery doctors when the illness conditions do not improve after taking the drugs prescribed by the drug sellers. However by the time they visit the qualified healthcare providers, most often the illness conditions deteriorate. In order to avoid such negative consequences, it is important to educate the workers through organizing health campaigns in the workplace and in their communities, disseminate adequate information and highlight the need of consulting qualified providers early on to avoid aggravating their health status for any health related issues and prevent spending further. The study also found that female RMG workers visit Upazila health complexes more frequently than the male workers for different illnesses. While it was not possible for us to explore why female RMG workers used these facilities more frequently than the males, it is possible that since the user free is very minimal in these facilities, more females preferred to visit there than males.29
An important finding of this study is that health insurance related knowledge was found to be very low among the study respondents. Only 10.5% of the survey respondents reported that they know about health insurance. A recent study conducted by Ahmed et al. in selected garments factories found that employer‐sponsored health insurance (ESHI) scheme increased healthcare utilization of medically trained providers and reduce out‐of‐pocket expenditure among insured RMG workers compared with uninsured RMG workers in Bangladesh.30 The study recommended that educational interventions can be provided to RMG workers to improve their healthcare‐seeking behaviors and increase their utilization of ESHI‐designated scheme. Our findings also suggest that affordable health insurance policy can be made available to the garments workers by the factory owners which would likely improve their formal healthcare utilization and reduce out‐of‐pocket expenditure.
The study revealed that the RMG workers have good knowledge about their health rights. However, often times they do not enjoy those rights properly. Bangladesh has enacted a new Labor Law in 2006 and the government amended it in 2013 to ensure that it complies with the ILO standards.4 Various acts of the Law bring benefits to the workers involved in the private sector such as the benefit of provident fund, group insurance scheme for companies employing 200 or more workers, maternity benefit expansion from 12 to 16 weeks and others. However, certain loopholes of the law were also documented such as government control over Labor unions’ access to foreign funding, lack of accountability of employers and others.4, 31 Unless these issues are addressed immediately, labor rights of workers cannot be achieved in the RMG sector in Bangladesh.
Several limitations of the study should be noted. We collected data from 486 garments workers in the survey from eight different factories located in three areas of Dhaka. Bangladesh has more than 4000 RMG factories and there are an estimated 4 million workers working in the factories.1 Therefore, the study sample represents only a small proportion of the entire workforce and cannot be generalized to represent the entire sector. The study was cross‐sectional in nature and therefore the observed association between different illnesses of the workers and their socio‐demographic characteristics and other work related information fail to establish causality.32 We also collected data on Fridays. Given that Friday is the only weekly holiday for the RMG workers; they remain busy with their household chores. However, we tried to minimize this limitation by spending more time in interviewing the respondents when they were engaged with performing household activities.
5. CONCLUSIONS
In conclusion, the study showed that prolonged working hours combined with an absence of health insurance plan and poor accessibility to health and legal services make the RMG workers vulnerable to poor health, economic insecurities and impacts adversely on their well‐being. In order to address the overall health and well‐being of the garments workers, it is imperative to lay out a blueprint for a safe and healthy workplace, which may in the long run increase the productivity of the garments industry.
DISCLOSURE
Ethical approval: Ethical approval (2018‐025‐IR) of the study was obtained from the Institutional Review Board (IRB) of BRAC JPGSPH, BRAC University. Field research assistants were adequately trained on how to maintain ethical norms while conducting the interviews and data protection. Informed consent: During data collection, written informed consent was obtained from each respondent prior to interview. Written permission was also taken for audio recording of interviews. Conflict of interest: The authors declare no conflict of interest.
AUTHOR CONTRIBUTIONS
M.T.H., S.M.H, and S.F.R conceived and designed the study. A.A., M.U.C., and K.F.I drafted the survey questionnaire and qualitative guidelines. A.A and M.U.C. analyzed the data. M.T.H, A.A., and M.U.C. prepared the first draft. K.F.I, S.M.H., R.P., S.J.A., M.L.A., and S.F.R. critically reviewed the manuscript for important intellectual content.
ACKNOWLEDGEMENTS
This study was conducted as part of the project “ERMG” in Bangladesh currently being implemented by BRAC UDP. The ERMG project was funded by PORTICUS. We also acknowledge the support of Maria Ahmed of BRAC UDP in drafting the survey questionnaire and data collection process.
Hasan MT, Amin A, Chowdhury MU, et al. Health sufferings, healthcare seeking behavior, awareness about health insurance, and health related rights of ready made garments workers in Bangladesh: Findings from a cross‐sectional study. J Occup Health. 2021;63:e12256. 10.1002/1348-9585.12256
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1.BGMEA . Bangladesh garment manufacturer and exporters association (BGMEA): towards a sustainable garment industry. 2020. Available from http://www.BGMEA.com.bd/
- 2.Khan SI, Khan A. Social and physical problems of readymade garment art workers for having fire accident in Bangladesh. Arts Soc Sci J. 2019;10:434. 10.4172/2151-6200.1000434 [DOI] [Google Scholar]
- 3.Morshed MM. A study on labour rights implementation in readymade garment (RMG) industry in Bangladesh: bridging the gap between theory and practice. University of Wollongong Thesis Collection. 2007. Available from https://ro.uow.edu.au/theses/40/
- 4.Ferdous SR, Asaduzzaman MD, Islam MA, Haque ME, Siraj SAB. The RMG sector: prospects and challenges and role of different stakeholders. Dhaka, Bangladesh: National Human Rights Commission; 2015. [Google Scholar]
- 5.Rahman MA, Rahman MM. Sickness and treatment: a situation analysis among the garments workers. Anwer Khan Mod Med Coll J. 2013;4(1):10‐14. 10.3329/akmmcj.v4i1.13678 [DOI] [Google Scholar]
- 6.Chowdhury MM, Ahmed R, Yasmin M. Prospects and problems of RMG industry: a study on Bangladesh. Res J Finance Account. 2014;5(7). Available from https://www.iiste.org/Journals/index.php/RJFA [Google Scholar]
- 7.Chowdhury DS. Women's rights and voice in the ready‐made garments sector of Bangladesh: evidence from theory and practice. Journal of International Women's Studies. 2017;18(2):118‐133. Available from https://vc.bridgew.edu/jiws/vol18/iss2/8/ [Google Scholar]
- 8.Begum F, Ali RN, Hossain MA, Shahid SB. Harassment of women garment workers in Bangladesh. J Bangladesh Agricul Univ. 2010;8(2):291‐296. 10.3329/jbau.v8i2.7940 [DOI] [Google Scholar]
- 9.Emran SN, Kyriacou J & Rogan S. Made in poverty: the true price of fashion. Oxfam Australia; 2019. Available from https://whatshemakes.oxfam.org.au/wp‐content/uploads/2019/02/Made‐in‐Poverty‐the‐True‐Price‐of‐Fashion.‐Oxfam‐Australia..pdf
- 10.Samaddar KK. Occupational health and safety management in RMG sector of Bangladesh. Int J Sci Technol Res. 2016;5(12). Available from https://www.semanticscholar.org/paper/Occupational‐Health‐And‐Safety‐Management‐In‐RMG‐Of‐Samaddar/80c9400a9b2763b09000df6575e944b39482634a [Google Scholar]
- 11.Farhana K, Syduzzaman M, Munir MS. Present status of workers in the ready‐made garments industries in Bangladesh. Eur Sci J. 2015;11(7). Available from http://eujournal.org/index.php/esj/article/view/5341 [Google Scholar]
- 12.[12]Bangladesh Bureau of Statistics (BBS) . Population and housing census ‐. 2011. Bangladesh Bureau of Statistics, Statistics Division, Ministry of Planning, Government of the People’s Republic of Bangladesh. 2012. Available from www.bbs.gov.bd
- 13.Patra P. Sample size in clinical research, the number we need. Int J Med Sci Public Health. 2012;1(1):5‐9. [Google Scholar]
- 14.Vingard E. Chapter 5.6: Major public health problems — musculoskeletal disorders. Scand J Public Health. 2006;34(67_suppl):104‐112. 10.1080/14034950600677113 [DOI] [PubMed] [Google Scholar]
- 15.Mayo clinic . Headache: Mayo foundation for medical education and research; 2020. Available from https://www.mayoclinic.org/symptoms/headache/basics/definition/sym‐20050800.
- 16.Dinarello CA, Porat R. Chapter 15: Fever. In: Jameson JL, Fauci AS, Kasper DL, eds. Harrison's Principles of Internal Medicine, 20th edn. New York, NY: McGraw‐Hill; 2018:1‐2. [Google Scholar]
- 17.Healthline . What’s causing your abdominal pain and how to treat it. Healthline Media; 2020. Available from https://www.healthline.com/health/abdominal–pain
- 18.UN‐Habitat . Slums. United Nations Human Settlements Programme (UN‐HABITAT). n.d. Available from https://mirror.unhabitat.org/documents/media_centre/sowcr2006/SOWCR%205.pdf
- 19.Ahmed S, Siddique AK, Iqbal A, et al. Causes for hospitalizations at upazila health complexes in Bangladesh. J Health Popul Nutr. 2010;28(4):399‐404. 10.3329/jhpn.v28i4.6047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Shazzad MN, Ahmed S, Haq SA, et al. Musculoskeletal symptoms and disorders among 350 garment workers in Bangladesh: a cross‐sectional pilot study. Int J Rheum Dis. 2018;21(12):2063‐2070. 10.1111/1756-185X.13423 [DOI] [PubMed] [Google Scholar]
- 21.Nunes IL, Work‐Related Bush PM. musculoskeletal disorders assessment and prevention. In Ergonomics ‐ A Systems Approach, Isabel L. Nunes, IntechOpen 2012, doi: 10.5772/37229. Available from: https://www.intechopen.com/books/ergonomics‐a‐systems‐approach/work‐related‐musculoskeletal‐disorders‐assessment‐and‐prevention [DOI]
- 22.Saha TK, Dasgupta A, Butt A, Chattopadhyay O. Health status of workers engaged in the small‐scale garment industry: how healthy are they? Ind J Commun Med. 2010;35(1):179‐182. 10.4103/0970-0218.62584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Khan AR, Khan MJ. Musculoskeletal symptoms among female garments worker: working environment. J Exerc Sports Orthopedics. 2018;5(2):1‐7 10.15226/2374-6904/5/2/00173 [DOI] [Google Scholar]
- 24.Coury HG, Aparecida I, Alem M, Oishi J. Influence of gender on work‐related musculoskeletal disorders in repetitive tasks. Int J Ind Ergon. 2002;29(1):33‐39. [Google Scholar]
- 25.Latif MB, Irin A, Ferdaus J. Socio‐economic and health status of slum dwellers of the Kalyanpur slum in Dhaka city. Bangladesh J Sci Res. 2016;29(1):73‐83. 10.3329/bjsr.v29i1.29760 [DOI] [Google Scholar]
- 26.Mannan MA. Burden of disease on the urban poor: a study of morbidity and utilization of healthcare among slum dwellers in Dhaka city. 2017. Available from https://www.think‐asia.org/handle/11540/7953
- 27.Sudhinaraset M, Ingram M, Lofthouse HK, Montagu D. What is the role of informal healthcare providers in developing countries? a systematic review. PLoS One. 2013;8(2):e54978. 10.1371/journal.pone.0054978 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.World Health Organization. Regional Office for the Western Pacific. Bangladesh health system review . Manila: WHO Regional Office for the Western Pacific; 2015. Available from https://apps.who.int/iris/handle/10665/208214 [Google Scholar]
- 29.Hospitals and Clinics Section, Directorate General of Health Service . User fees: hospital user fees. Available from http://hospitaldghs.gov.bd/hospital–user–fees/
- 30.Ahmed S, Sarker AR, Sultana M, et al. Do employer‐sponsored health insurance schemes affect the utilization of medically trained providers and out‐of‐pocket payments among ready‐made garment workers? a case–control study in Bangladesh. BMJ Open. 2019;10:e030298. 10.1136/bmjopen-2019-030298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sharma V. Imperfect work conditions in Bangladesh RMG sector. Int J Law Manag. 2015;57(1):28‐37. 10.1108/IJLMA-07-2013-0034. [DOI] [Google Scholar]
- 32.Gordis L. Epidemiology, 5th edn. Philadelphia, PA: Saunders/Elsevier; 2014. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.