

Abstract
Puerto Rico is a US territory and a popular destination for Latino immigrants in the Caribbean. Even with few language and cultural barriers, however, many Latino immigrants in Puerto Rico are uninsured. Using data from the 2014–19 Puerto Rico Community Survey, we examined inequities in health insurance coverage for non–Puerto Rican Latinos ages 18–64 living in Puerto Rico according to citizenship status and Latino subgroup (Dominican, Cuban, Mexican, and other Latino). After controlling for potential confounders, we found that noncitizen Dominicans had a significantly lower probability of having any health insurance (57.2 percent) and having any private insurance (31.5 percent). Regardless of similarities in culture and language, Latino immigrants on the island, particularly Dominicans, experience major health insurance coverage inequities. Considering that Puerto Rico’s immigration system is regulated by US federal statute, both federal and local policy makers should acknowledge and focus on reducing these immigrant disparities in health insurance coverage.
Given the location of the US territory of Puerto Rico in the Caribbean, it has historically been a prime destination for immigration from Latin America. About 3 percent of Puerto Rico’s population is foreign born,1 with 60 percent of immigrants coming from the Dominican Republic and 12 percent from Cuba.2 Moreover, among the approximately 100,000 Dominicans living there, it has been estimated that nearly 30,000 are undocumented immigrants.3 Despite significant migration to Puerto Rico, US border and immigrant health research has largely overlooked the island.
Background And Context
As a US territory, Puerto Rico is subject to US federal immigration policies. However, its 99 percent Latino population4 provides a unique environment for non–Puerto Rican Latino immigrants. Similar to most Latin American countries, Puerto Rico has a history as a long-standing Spanish colony with mixed Indigenous, African, and European influences embedded into its culture.5 The shared history, Latin culture, and Spanish language facilitate Latino immigrants’ assimilation into Puerto Rican culture.6,7 Despite a minor increase in deportations on the island since the implementation of the Trump administration’s anti-immigrant policies in 2017, Immigration and Customs Enforcement (ICE) activity is relatively low compared with the US mainland.7,8 Nevertheless, even with few language and cultural barriers, many Latino immigrants in Puerto Rico live in poverty;9,10 have low levels of education;3,9 take on unskilled or low-paying jobs;3,9,11 and experience microaggressions, marginalization, and ethnic discrimination.3,12 All of these can lead to heightened risk for poor population health outcomes.13
Among US mainland Latino immigrants, noncitizen and undocumented status is associated with poor health care access and use.14,15 Poor health outcomes for immigrants on the main-land have, in part, been attributed to disparities in access to health insurance.16 However, these outcomes might not be translatable to Puerto Rico because of the unique structure of its public insurance delivery system. The funding for Puerto Rico Medicaid comes via an annual federal block grant, as determined by Congress,17 that traditionally uses a 55 percent federal matching rate. However, unlike states, which have no funding cap, the island’s government is responsible for covering all Medicaid costs beyond this cap. Considering that nearly half of its population relies on Medicaid,18 the block grant has historically failed to cover local spending needs and increasing Medicaid costs.
Puerto Rico also uses the local Puerto Rico poverty level to determine income-based eligibility for Medicaid.19–22 Medicaid eligibility extends to any individual or family with an income at or below 133 percent of the Puerto Rico poverty level, which, for a family of four, represents an annual salary of approximately $11,316, or about 43 percent of the federal poverty level.20 Although local efforts propose a future significant long-term increase in Medicaid eligibility, they rely heavily on federal approval and funding. As part of the federal budget plan for fiscal year 2022, the Biden administration has proposed to eliminate the block grant cap for Puerto Rico and other US territories and provide a matching rate similar to that provided to the states.23
MEDICAID ELIGIBILITY FOR IMMIGRANTS
For citizens and legal residents of Puerto Rico who are eligible, applying for Medicaid merely requires proof of US citizenship or lawful residence in Puerto Rico for at least five years.24 This process is further simplified for groups with certain federal protections, such as Cubans, who up until 2017 were exempt from the five-year waiting period via the Cuban Adjustment Act of 1966.24–26 All Cubans who reached US territory automatically received a protected status, allowing them to apply for legal residence and be eligible for public benefits. Because this was exclusive to Cubans, undocumented Latinos in Puerto Rico from other subgroups were not protected or allowed the same eligibility criteria for public insurance before 2017.
In Puerto Rico private insurance is primarily employer based, and it can be inaccessible for people with low incomes or low-skill employment. Furthermore, Puerto Rican residents do not receive the tax credits or subsidies offered to residents of the states via the Affordable Care Act (ACA) to purchase private insurance through Marketplaces.27 Thus, regardless of having lawful residence, low-income immigrants might still face barriers to obtaining health insurance.
PUBLIC HEALTH DISASTERS AND EMERGENCIES
Puerto Rico has faced multiple major public health disasters and emergencies since 2017, including Hurricanes Irma and Maria, major earthquakes, and the COVID-19 pandemic. Many Puerto Ricans lost their jobs after Hurricane Maria, and the island’s unemployment rate has been magnified after the COVID-19 shutdowns of nonessential businesses.28–31 These events left many without health insurance or the ability to pay for health care.32 Devastating and often unpredictable public health emergencies like these are likely to exacerbate health disparities for Latino immigrants on the island and make undocumented immigrants even more vulnerable to negative health outcomes. Health care inequities can present greater health risks for immigrants, which is especially salient given Puerto Rico’s struggling economy and ongoing efforts to recover from recent catastrophes.
When investigating US border and immigrant health, researchers, program implementers, and federal and local policy makers must consider the border realities beyond the US mainland. To that end, there is very limited research on border health in Puerto Rico.9,33 Although early qualitative work described immigrant experiences in Puerto Rico, particularly for undocumented Dominicans,6,12 there has not been, to our knowledge, a population-level study on health insurance coverage among Latino immigrants in Puerto Rico.
In this study we examined how the intersection of citizenship and Latino subgroup identity is linked to health insurance coverage inequities. Using data from the 2014–19 Puerto Rico Community Survey, we determined how reports of having any health insurance, private insurance, and public insurance varied among US-born citizens, foreign-born citizens, and foreign-born noncitizens of the major non–Puerto Rican Latino subgroups on the island (Dominicans, Cubans, Mexicans, and other Latinos). Through our work, we aim to inform policies and programs to improve access to insurance for non–Puerto Rican Latino immigrants on the island, who are largely understudied and overlooked for health policy and public health interventions.
Study Data And Methods
DATA
We pooled data from the 2014–19 waves of the Puerto Rico Community Survey,34 which is an annual, cross-sectional household survey conducted by the Census Bureau that collects representative islandwide data on population demographics and economic and social characteristics. The survey samples approximately 36,000 housing units annually,35 with an average annual response rate of about 57 percent during the survey periods.36 Puerto Rico Community Survey data are publicly available.
MEASURES
For the outcome variables, the Puerto Rico Community Survey ascertains whether participants reported having any health insurance coverage, any private health insurance coverage, or any public health insurance coverage at the time of the interview. Our sample excluded any respondents younger than age sixty-five who were covered under Medicare because of a disability (n = 360). We combined the survey’s citizenship and birthplace variables as “born a US citizen,” “foreign-born citizen,” and “foreign-born noncitizen.” Per the Census Bureau’s definition, “foreign born” was used to identify anyone who was not a US citizen at birth.37 The “foreign-born citizen” group was composed mainly of naturalized citizens.
All Puerto Ricans are US citizens at birth, so they lack representation within the foreign-born categories. Because one of our study objectives was to detect within-group differences in health insurance by nativity and citizenship status, respondents who self-identified as Puerto Rican were excluded from the sample. We condensed the Puerto Rico Community Survey measure of Latino ethnicity to classify respondents into the following major non–Puerto Rican Latino sub-groups on the island: Dominican (63.3 percent of the sample); Cuban (10.5 percent); Mexican (8.5 percent); and other Latino (17.7 percent), mostly Colombian (4.4 percent) and Venezuelan (3.0 percent). For this study, respondents labeled as “born a US citizen” included those who culturally identified as an alternative Latino subgroup (that is, Dominican, Cuban, Mexican, or other non–Puerto Rican Latino group) yet were born in Puerto Rico or the US mainland. All regression models controlled for survey year, sex, age, marital status, educational attainment, employment status, and family income. Family income was reported as a percentage of the federal poverty level, as the Puerto Rico Community Survey does not capture Puerto Rico poverty level.
STATISTICAL ANALYSES
The study sample consisted of non–Puerto Rican Latino adults ages 18–64 residing in Puerto Rico at the time of the interview (n = 3,665). All non-Latinos, including Spaniards, were excluded from the analyses. Weighted descriptive statistics are presented by Latino subgroup, and Pearson chi-square tests were used to determine whether each characteristic varied significantly by subgroup. Probit regressions were run separately for each of the three outcomes (any health insurance, private insurance, and public health insurance) to determine whether citizenship status and Latino subgroup were associated with the outcomes after all covariates were controlled for. Results are reported as marginal effects for ease of interpretation, but we provide detailed multivariable regression tables in online appendix exhibits A1–A3.38
As a result of minor differences in the probabilities of having health insurance between respondents born as US citizens and those who were foreign-born citizens in the initial models across all Latino groups, and noting the clear disparity between citizens and noncitizens, particularly among Dominicans, we combined the citizen categories and compared them with noncitizens for both Dominicans and all other Latinos. Because the disparity between Dominicans and the other Latino categories was evident in the first regression, we aggregated Cubans, Mexicans, and other Latinos for statistical power and simplicity of interpretation in the second regression. An additional probit regression was used to compare the marginal effects of being insured between Dominicans and all other Latinos by citizenship status. All analyses were conducted using Stata/IC, version 16.0, and accounted for the Puerto Rico Community Survey complex survey sampling design using replicate weights.
LIMITATIONS
This study had limitations that should be considered. First, the Census Bureau does not collect data on legal residency, so we were limited to citizenship status as an indicator. This is further limited because citizenship is a self-reported measure in the Puerto Rico Community Survey, and we must consider the possibility of underreporting as a result of anti-immigrant actions and rhetoric. Second, a large portion of respondents (n = 736) indicated “other” for their race or a mixed race of “White” and “Black.” Given the “noise” of this variable, we were unable to account for race in our analyses. It is important to note that race could be a predictive sociodemographic factor for health insurance coverage, as observed on the US mainland.39,40 Third, the Puerto Rico Community Survey data contain only sociodemographic characteristics, which restricted our analyses from including other predisposing, enabling, or need factors, such as preexisting health conditions.41 Finally, because of a limited sample size, we analyzed employment as a dichotomous variable, and therefore could not measure the association between occupation type and participants’ likelihood of obtaining health insurance, specifically employer-based coverage. We present occupation type by Latino subgroup in appendix exhibit A6.38
Study Results
Exhibit 1 presents sample characteristics by Latino subgroup. Among all of the subgroups, Cubans had the highest proportion of having any insurance (90.8 percent) and any private insurance (68.8 percent), whereas Mexicans and Dominicans had the highest proportion of having any public insurance (36.0 percent and 35.3 percent, respectively). Overall, Dominicans had the highest proportion of uninsurance (36.1 percent). Most respondents were foreign-born noncitizens (48.8 percent), with 60.9 percent of Dominicans and 38.2 percent of other Latinos reporting this status. A greater proportion of Cubans were foreign-born citizens (57.7 percent), whereas Mexicans were mainly US-born citizens (74.5 percent). Cubans made up the oldest group, with 61.3 percent of respondents ages 51–64. Across all groups, most respondents were married and employed at the time of interview. Dominicans had a larger proportion of respondents with a high school education or less (61.1 percent), whereas most Cubans, Mexicans, and other Latinos had at least some college education (75.8 percent, 61.4 percent, and 70.4 percent, respectively).
EXHIBIT 1.
Weighted descriptive statistics of survey respondents in Puerto Rico, by Latino subgroup, 2014–19
| Total (N = 3,665) |
Dominican (n = 2,319) |
Cuban (n = 384) |
Mexican (n = 313) |
Other Latino (n = 649) |
p value | |
|---|---|---|---|---|---|---|
| Health insurance coveragea | ||||||
| Any insurance | 72.00% | 63.87% | 90.75% | 87.44% | 81.91% | <0.001 |
| Any private insurance | 41.86 | 30.08 | 68.78 | 52.98 | 62.84 | <0.001 |
| Any public insurance | 31.74 | 35.30 | 24.78 | 36.00 | 20.36 | <0.001 |
| Citizenship/nativity | <0.001 | |||||
| Born a US citizen | 19.30 | 8.71 | 19.99 | 74.49 | 25.49 | |
| Foreign-born citizen | 31.87 | 30.37 | 57.74 | 8.14 | 36.28 | |
| Foreign-born noncitizen | 48.83 | 60.92 | 22.27 | 17.37 | 38.23 | |
| Sex | 0.046 | |||||
| Male | 45.29 | 43.78 | 53.05 | 45.34 | 46.32 | |
| Female | 54.71 | 56.22 | 46.95 | 54.66 | 53.68 | |
| Age, years | <0.001 | |||||
| 18–30 | 18.89 | 20.05 | 7.91 | 25.22 | 17.28 | |
| 31–50 | 45.35 | 45.73 | 30.78 | 52.22 | 48.31 | |
| 51–64 | 35.76 | 34.22 | 61.31 | 22.56 | 34.41 | |
| Marital status | <0.001 | |||||
| Married | 45.74 | 41.55 | 53.15 | 48.85 | 54.93 | |
| Previously married | 21.73 | 22.99 | 22.09 | 19.10 | 18.46 | |
| Never married | 32.53 | 35.46 | 24.76 | 32.05 | 26.61 | |
| Educational attainment | <0.001 | |||||
| High school or less | 49.75 | 61.09 | 24.17 | 38.63 | 29.59 | |
| At least some college | 50.25 | 38.91 | 75.83 | 61.37 | 70.41 | |
| Employment | <0.01 | |||||
| Employed | 62.64 | 62.34 | 71.13 | 57.22 | 62.03 | |
| Currently not employed | 37.36 | 37.66 | 28.87 | 42.78 | 37.97 | |
| Income as percent of federal poverty levelb | <0.001 | |||||
| >200% | 30.85 | 19.56 | 62.21 | 37.20 | 50.28 | |
| 100%–200% | 28.60 | 32.04 | 19.64 | 28.31 | 21.37 | |
| <100% | 40.55 | 48.40 | 18.15 | 34.49 | 28.35 |
SOURCE Authors’ analysis of data from the Puerto Rico Community Survey, 2014–19. NOTES Values are shown in column percentages. The sum of shares for the insurance categories does not equal 100 percent, as some respondents had both private and public insurance. Significance was determined using Pearson chi-square tests comparing sample characteristics and Latino subgroups.
Each insurance category is independent of one another, and values reported represent the percentage of respondents with that given insurance; separate tests were run for each health insurance coverage category.
Reported as percent of federal poverty level because the survey does not capture Puerto Rico poverty level.
Most respondents (40.6 percent) were living below 100 percent of the federal poverty level. Among the Latino subgroups, Dominicans (48.4 percent) had a higher proportion living at this income level. Cubans, Mexicans, and other Latinos had a higher proportion living above 200 percent of the federal poverty level (62.2 percent, 37.2 percent, and 50.3 percent, respectively). In a separate analysis (see appendix exhibit A4),38 we found that 28.5 percent of Dominicans, 11.5 percent of Cubans, 18.5 percent of Mexicans, and 17.2 percent of other Latinos had incomes lower than 50 percent of the federal poverty level, which is the rough equivalent of the Puerto Rico Medicaid eligibility threshold (133 percent of the Puerto Rico poverty level). Each of the covariates significantly differed by Latino subgroup (p < 0.05).
As shown in exhibit 2, Cubans, Mexicans, and other Latinos—regardless of citizenship status and nativity—were significantly more likely to have any insurance and to have any private insurance compared with Dominicans of the same citizenship status and nativity. Furthermore, the magnitude of these marginal effects varied by citizenship status. For example, Cubans born as US citizens had a 10.3 percent higher probability of having any insurance compared with Dominicans born as US citizens, whereas Cuban foreign-born citizens had an 11.4 percent greater probability of having any insurance compared with Dominican foreign-born citizens. This disparity between Cubans and Dominicans was further exacerbated for noncitizens, with noncitizen Cubans being 18.1 percent more likely to have any insurance than noncitizen Dominicans. This pattern, however, was not consistent for public insurance. After statistical adjustment, Dominicans were significantly more likely to have any public insurance compared with other Latinos, regardless of citizenship and nativity. Although there was no significant difference between Dominicans and Cubans or Mexicans in having any public insurance, we must consider the limitation that the sample of Cubans and Mexicans with public insurance was small (n = 86 and n = 107, respectively).
EXHIBIT 2.
Marginal effects of citizenship and nativity on having health insurance in Puerto Rico, by Latino subgroup, 2014–19
| Any insurance | Any private insurance | Any public insurance | |
|---|---|---|---|
| CUBANS | |||
| Born a US citizen | 10.26**** | 12.38**** | −0.06 |
| Foreign-born citizen | 11.43**** | 12.40**** | −0.06 |
| Foreign-born noncitizen | 18.06**** | 11.86**** | −0.05 |
| MEXICANS | |||
| Born a US citizen | 8.03*** | 9.53*** | −0.75 |
| Foreign-born citizen | 8.89*** | 9.56*** | −0.73 |
| Foreign-born noncitizen | 13.53*** | 9.07*** | −0.64 |
| OTHER LATINOS | |||
| Born a US citizen | 5.58*** | 14.66**** | −10.00*** |
| Foreign-born citizen | 6.15*** | 14.68**** | −9.58*** |
| Foreign-born noncitizen | 9.02*** | 14.14**** | −8.15*** |
SOURCE Authors’ analysis of data from the Puerto Rico Community Survey, 2014–19. NOTES Sample size is in exhibit 1. Marginal effects are shown as percentages, with Dominicans as the reference group. All models were adjusted for survey year, sex, age, marital status, education, employment status, and income level. Each citizenship/nativity category is compared with the same category of the reference group.
p < 0.01
p < 0.001
Exhibit 3 shows the predictive margins of having any health insurance, any private insurance, and any public insurance, using a condensed form of the Latino subgroups by citizenship: noncitizen Dominicans, noncitizen other Latinos, citizen Dominicans, and citizen other Latinos. Among noncitizen Dominicans, there was a 57.2 percent probability (95% confidence interval: 54.0, 60.4) of having any insurance, 31.5 percent probability (95% CI: 28.7, 34.3) of having any private insurance, and 26.9 percent probability (95% CI: 24.4, 29.5) of having any public insurance. Among noncitizen other Latinos, there was a 71.6 percent probability (95% CI: 66.0, 77.3) of having any insurance, 48.6 percent probability (95% CI: 43.7, 53.6) of having any private insurance, and 23.9 percent probability (95% CI: 18.6, 29.2) of having any public insurance. Citizen Dominicans had higher probabilities of having any and private insurance than their noncitizen counterparts, with an 80.8 percent probability (95% CI: 77.5, 84.0) of having any insurance, 43.6 percent probability (95% CI: 39.7, 47.5) of having any private insurance, and 39.5 percent probability (95% CI: 36.5, 42.6) of having any public insurance. Other Latino citizens had the highest any insurance and private insurance proportions, with an 88.0 percent probability (95% CI: 85.5, 90.6) of having any insurance, 52.5 percent probability (95% CI: 49.2, 55.8) of having any private insurance, and 35.9 percent probability (95% CI: 32.5, 39.2) of having any public insurance. For having any public health insurance, noncitizen other Latinos were the only group whose probability of having any public insurance was not significantly different from that of noncitizen Dominicans (p = 0.314).
EXHIBIT 3. Predictive margins of having any health insurance, any private insurance, and any public insurance in Puerto Rico, by Latino subgroup and US citizen status, 2014–19.
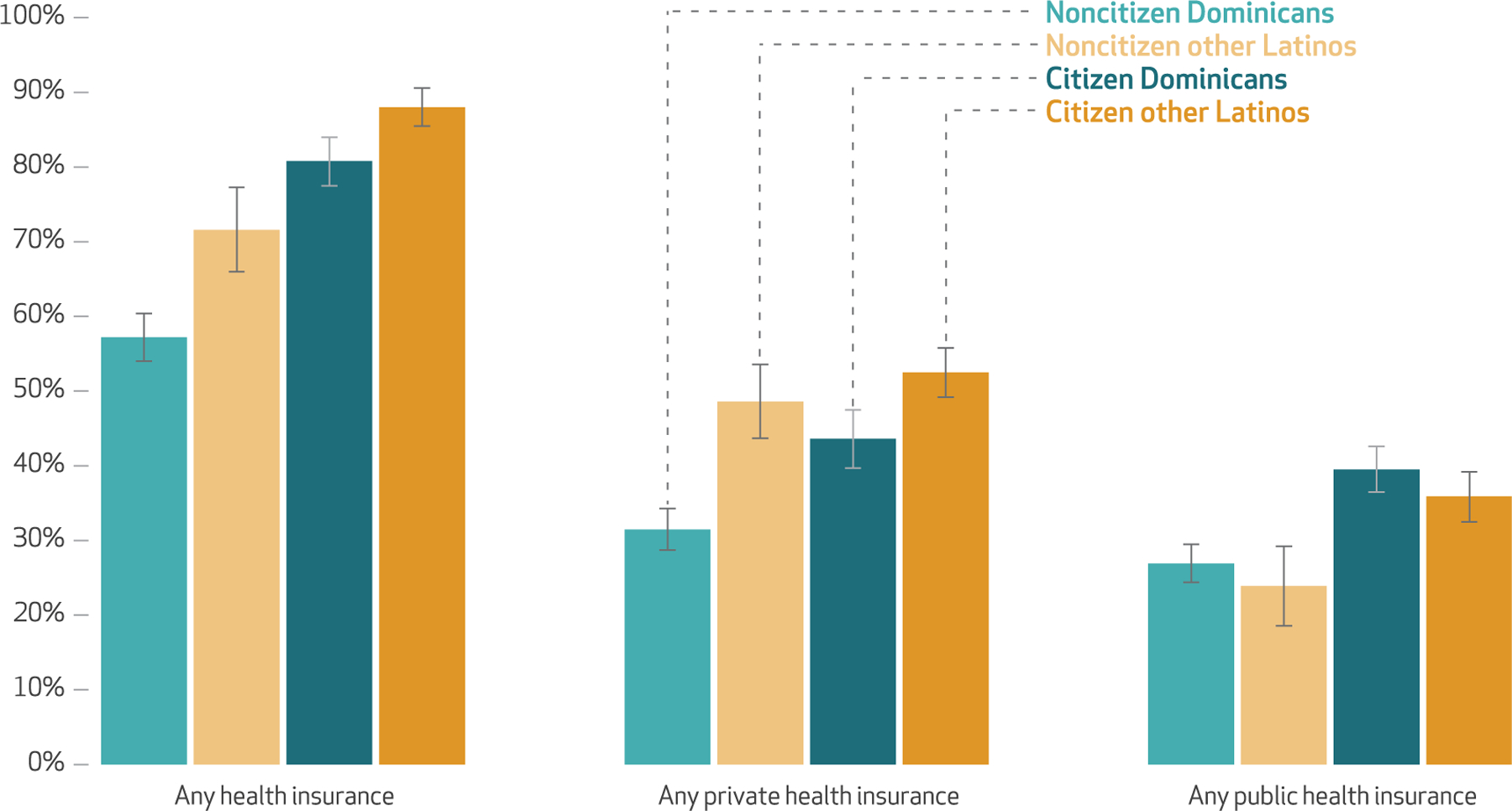
SOURCE Authors’ analysis of data from the Puerto Rico Community Survey, 2014–19. NOTES Marginal effects are shown as percentages; the error bars represent 95% confidence intervals. All models were adjusted for survey year, sex, age, marital status, education, employment status, and income level.
Discussion
Despite the favorable cultural and linguistic context in Puerto Rico for Latino immigrants, they face social and health insurance inequities. These challenges apply especially to Dominican immigrants. Furthermore, during the period we examined, citizenship played a protective role for within-Latino-group differences in having any health insurance: Citizens had a significantly higher probability of being insured than noncitizens. As a consequence, noncitizen Dominicans in Puerto Rico were the most vulnerable group for lacking health insurance. Previous work has shown how Dominican immigrants in Puerto Rico are more likely to have lower educational attainment, limited employment opportunities, increased poverty, and worse living conditions3,6,9–12 compared with other Latino immigrant groups. These factors, combined with the lack of health insurance observed in our study, can exacerbate health inequities and contribute to poor community health.8
Although citizen Dominicans had the highest probability of having public insurance, noncitizen Dominicans living under the Puerto Rico poverty level threshold remain ineligible for governmental assistance if their residence or citizenship status is undefined or unauthorized. Furthermore, despite the large relative number of Dominicans with public insurance, there is still a substantial share without insurance. Alternatively, access to private health insurance relies on certain types of employment or the ability to pay for insurance premiums out of pocket. Although most Latinos in Puerto Rico are employed, a large portion of Dominican immigrants are informally employed through low-skill labor,11 whereas other Latinos, such as Cubans, tend to be employed in higher-skill jobs that come with employee benefits, as shown in online appendix exhibit A6.38 Because informal employers might be less willing to invest in employee health insurance,42 this could contribute to the disparate coverage rates among Dominicans compared with other Latino subgroups.
In Puerto Rico many Dominicans remain noncitizens, with about 30 percent estimated to be undocumented.3 For other Latino immigrant subgroups, certain federal and local protections make them eligible for citizenship and governmental assistance programs such as Medicaid. Until 2017 Cubans were protected under the federal “wet-foot, dry-foot” policy, or Cuban Adjustment Act, which allowed any noncitizen Cubans seeking asylum the right to stay and apply for expedited legal residence in Puerto Rico and, eventually, for US citizenship.25 However, these protections rarely extend to Dominicans, even though the Dominican workforce contributes billions of dollars to the Puerto Rican economy.43 Although most Dominicans have migrated in search of better job opportunities after political tensions, a debt crisis, and high poverty rates in the Dominican Republic,44 they are not considered asylum seekers by the US government and hence do not receive special protections.45 Although Dominican migrants in the 1970s were considered “privileged” or “elite,” with a majority being highly educated professionals, the debt crisis has led to a greater migration into the US of low-income and poorly educated people escaping economic hardship.46
In our study most Dominicans were foreign-born noncitizens with lower levels of income and educational attainment compared with the other Latino subgroups. In contrast, not only were most Cubans, Mexicans, and other Latinos in Puerto Rico US citizens, but they also had higher levels of educational attainment and employment, which are known protective factors for access to health insurance.47,48 We must also consider the different employment profiles of these Latino subgroups. Cubans, Mexicans, and other Latinos, such as Colombians, residing in Puerto Rico are more often professionally employed,49,50 with many being in administrative positions (for example, managers), as shown in online appendix exhibit A6.38 Certain local protections also extend to Latinos who migrate to Puerto Rico with the purpose of investing in business. These immigrants receive investor visas that can be renewed indefinitely so long as they provide evidence that theirbusinessescontinuetobeactive.51 However, this policy favors Latino immigrants who arrive with higher educational attainment and other sociodemographic advantages.
In this study we observed significant inequities in insurance coverage among non–Puerto Rican Latinos on the island. Particular attention should be given to Dominican groups in Puerto Rico, especially noncitizens, considering their higher odds for uninsurance compared with other Latino subgroups. Because Puerto Rico is subject to US federal immigration policies, both federal and local policy makers should consider addressing the potential barriers for noncitizen Dominicans to qualify for legal residence or government programs such as Medicaid. The need for federal reform of the US immigration system affects both the US mainland and Puerto Rico. Thus, the Biden administration’s proposal to “fix” the path to citizenship52 should consider Puerto Rico’s border context, where the Latin culture and Spanish language ease Latino immigrants’ social assimilation, yet major disparities still exist in individual-level factors such as health insurance. In addition, a restructuring of the poorly resourced Medicaid program in Puerto Rico requires accountability and political will from local and federal policy makers to redirect efforts and funding toward health care to expand public insurance eligibility.17
In recent years immigrant health has gained attention from local lawmakers. For example, the Puerto Rico Senate’s SP 1313 bill sought to forbid discrimination against immigrants of any status in obtaining vaccination and emergency care services.53 In 2015 the local Senate’s Committee on Health and Nutrition passed SR 1081, in which they proposed an investigation into the accessibility of health services for immigrants, regardless of their legal authorization status, and the needs and barriers the immigrant community faces.54 However, the follow-up of this initiative remains unclear.
By demonstrating major gaps in insurance coverage according to Latino subgroup and citizenship status, our findings could help inform new political efforts. Local policy makers and program planners should consider reinforcing the few existing programs that offer health care services to undocumented immigrants in Puerto Rico, such as the Migrant Health Center55 and HealthproMed,56 which are two federally qualified health centers that provide primary health care to low-income immigrants regardless of legal authorization status and insurance coverage. However, considering that centers such as these have limited financial and structural resources,57 there is a need to direct more public funds toward these centers, which serve as safety-net facilities for many immigrants. Local policy makers should also collaborate with community-based organizations, public health agencies, and private partners to develop programs aimed at increasing health insurance coverage and access to care for noncitizen Dominicans.
Conclusion
Despite similarities in culture and language, Latino immigrants in Puerto Rico, especially Dominicans, experience significant health insurance inequities. With the island’s current fragile economic status, recent public health disasters, and the ongoing COVID-19 pandemic, it is critical to address factors affecting health care access, such as health insurance, for this vulnerable group. Local and federal policy makers could use the findings from this study to engage in discussions about health insurance and care disparities for immigrants in Puerto Rico, and the findings can inform population health initiatives targeted for immigrants on the island. With this study, we aim to bring attention to a heavily understudied population and contribute to the scarce literature regarding immigrant health care in Puerto Rico.
Supplementary Material
Acknowledgments
Funding for this work was provided through Grant No. R01MD013866 and Grant No. R01MD014146 from the National Institute on Minority Health and Health Disparities, National Institutes of Health, to Alexander Ortega.
Contributor Information
Alexandra C. Rivera-González, Department of Health Management and Policy, Drexel University Dornsife School of Public Health, in Philadelphia, Pennsylvania.
Jim P. Stimpson, Department of Health Management and Policy, Drexel University Dornsife School of Public Health.
Dylan H. Roby, Department of Health Policy and Management at the University of Maryland School of Public Health, in College Park, Maryland; an adjunct associate professor in the Fielding School of Public Health, University of California Los Angeles (UCLA), in Los Angeles, California; and a faculty associate in the UCLA Center for Health Policy Research.
Glorisa Canino, Department of Pediatrics and director of the Behavioral Sciences Research Institute in the School of Medicine, University of Puerto Rico, in Rio Piedras, Puerto Rico..
Jonathan Purtle, Department of Health Management and Policy, Drexel University Dornsife School of Public Health..
Scarlett L. Bellamy, Department of Epidemiology and Biostatistics, Drexel University Dornsife School of Public Health.
Alexander N. Ortega, Department of Health Management and Policy, Drexel University Dornsife School of Public Health.
NOTES
- 1.Census Bureau. Public Use Microdata, American Community Survey: 2019: ACS 5-year estimates data profiles [Internet] Washington (DC): Census Bureau; 2020. Table DP02PR, Selected social characteristics in Puerto Rico; [cited2021 Jun 2]. Available from: https://data.census.gov/cedsci/table?q=foreign%20born%20puerto%20rico&tid=ACSDP5Y2019.DP02PR [Google Scholar]
- 2.Census Bureau. Public Use Microdata, American Community Survey: 2019: ACS 5-year estimates data profiles [Internet] Washington (DC): Census Bureau; 2020. Table B05006PR, Place of birth for the foreign-born population in Puerto Rico; [cited2021 Jun 2]. Available from: https://data.census.gov/cedsci/table?q=B05006PR%20&tid=ACSDT5Y2019.B05006PR [Google Scholar]
- 3.Minority Rights Group International . Puerto Rico: Dominicans [Internet] London: MRG; 2015June19[cited2021 May 19]. Available from: https://minorityrights.org/minorities/dominicans/ [Google Scholar]
- 4.Census Bureau. Public Use Microdata, American Community Survey: 2019: ACS 5-year estimates data profiles [Internet] Washington (DC): Census Bureau; 2020. Table DP05, ACS demographic and housing estimates, Puerto Rico; [cited2021 Jun 2]. Available from: https://data.census.gov/cedsci/table?q=dp05%20puerto%20rico&tid=ACSDP5Y2019.DP05 [Google Scholar]
- 5.Van Atten S Puerto Rican culture: national identity, gender roles, and religion [Internet] New York (NY): Hachette Book Group; 2013March20[cited2021 May 19]. Available from: https://www.hachettebookgroup.com/travel/arts-culture/puertorican-culture-national-identity-gender-roles-religion/ [Google Scholar]
- 6.Duany J Dominican migration to Puerto Rico: a transnational perspective. Centro J 2005;17(1): 242–69. [Google Scholar]
- 7.Alford NS. Police violence against Dominicans in Puerto Rico suggests systemic problem. Guardian [serial on the Internet].2019October10[cited2021 May 19]. Available from: https://www.theguardian.com/world/2019/oct/10/police-violence-against-dominicans-in-puerto-rico-suggests-systemic-problem
- 8.Torres M How Trump’s anti-immigrant policies separate families in Puerto Rico Centro de Periodismo Investigativo; [serial on the Internet].2019January16[cited2021 May 19]. Available from: https://periodismoinvestigativo.com/2019/01/how-trumps-anti-immigrant-policies-separate-families-in-puerto-rico/ [Google Scholar]
- 9.Tamez M, Ríos-Bedoya CF, Rodríguez-Orengo JF, Tucker KL, Mattei J. Sociodemographic and lifestyle factors, and health conditions of Dominican adults living in Puerto Rico. J Immigr Minor Health 2018;20(5):1085–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Corpus E Migrants rebuild their lives in Puerto Rico despite challenges [Internet] Los Angeles (CA): USC Annenberg Media; 2019September30[cited2021 May 19]. Available from: https://www.uscannenbergmedia.com/2019/09/30/migrants-rebuild-their-lives-in-puerto-rico-despite-challenges/ [Google Scholar]
- 11.Persad K Dominican immigrants in Puerto Rico find success as business owners [Internet] Phoenix (AZ): Arizona State University, Walter Cronkite School of Journalism and Mass Communication; 2012October29[cited2021 May 19]. Available from: https://cronkite.asu.edu/projects/buffett/Puertorico/bizowners.html [Google Scholar]
- 12.Bishop M The other border: unauthorized immigration to Puerto Rico [Internet] New York (NY: ): Latino USA; 2015January2[cited2021 May 19]. Available from: https://www.latinousa.org/2015/01/02/border-unauthorized-immigration-Puerto-rico/ [Google Scholar]
- 13.Derose KP, Escarce JJ, Lurie N. Immigrants and health care: sources of vulnerability. Health Aff (Millwood) 2007;26(5):1258–68. [DOI] [PubMed] [Google Scholar]
- 14.Carrasquillo O, Carrasquillo AI, Shea S. Health insurance coverage of immigrants living in the United States: differences by citizenship status and country of origin. Am J Public Health 2000;90(6):917–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ku L, Matani S. Left out: immigrants’ access to health care and insurance. Health Aff (Millwood) 2001;20(1): 247–56. [DOI] [PubMed] [Google Scholar]
- 16.Stimpson JP, Wilson FA. Medicaid expansion improved health insurance coverage for immigrants, but disparities persist. Health Aff (Millwood) 2018;37(10):1656–62. [DOI] [PubMed] [Google Scholar]
- 17.Park E How states would fare under Medicaid block grants or per capita caps: lessons from Puerto Rico [Internet] New York (NY): Common-wealth Fund; 2021January6[cited2021 May 19]. Available from: https://www.commonwealthfund.org/publications/issue-briefs/2021/jan/how-states-fare-medicaid-block-grants-per-capita-caps-puerto-rico [Google Scholar]
- 18.Census Bureau. Public Use Microdata, American Community Survey: 2019: ACS 5-year estimates data profiles [Internet] Washington (DC): Census Bureau; 2020Table S2704, ACS demographic and housing estimates, Puerto Rico; [cited2021 Jun 9]. Available from: https://data.census.gov/cedsci/table?q=health%20insurance%20puerto%20rico&tid=ACSST5Y2019.S2704 [Google Scholar]
- 19.Patron M Puerto Rico’s exodus of doctors adds health care strain to dire financial crisis. NBC News [serial on the Internet].2017August8[cited2021 May 19]. Available from: https://www.nbcnews.com/news/latino/puerto-rico-s-exodus-doctors-adds-health-care-strain-diren783776
- 20.Medicaid and CHIP Payment and Access Commission. Fact sheet: Medicaid and CHIP in Puerto Rico [Internet] Washington (DC): MACPAC; 2021February[cited2021 May 19]. Available from: https://www.macpac.gov/wp-content/uploads/2020/08/Medicaid-and-CHIP-in-Puerto-Rico.pdf [Google Scholar]
- 21.Puerto Rico Department of Health. Puerto Rico Medicaid state plan [Internet] San Juan: The Department; 2019May[cited2021 May 19]. Available from: https://www.medicaid.pr.gov/pdf/stateplan/08_SPA_Attach1.pdf [Google Scholar]
- 22.Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. 2020 poverty guidelines [Internet] Washington (DC): ASPE; 2020January21[cited2021 May 19]. Available from: https://aspe.hhs.gov/2020-poverty-guidelines [Google Scholar]
- 23.Office of Management and Budget. Budget of the US government: fiscal year 2022 [Internet] Washington (DC): White House; 2021May28[cited2021 Jun 10]. Available for download from: https://www.whitehouse.gov/omb/budget [Google Scholar]
- 24.Department of Health, Medicaid Program. Frequently asked questions [Internet] San Juan: The Department; 2021[cited2021 Jun 7]. Available from: https://www.medicaid.pr.gov/Home/FAQS/#p2 [Google Scholar]
- 25.US Citizenship and Immigration Services. Residencia permanente para naturales o ciudadanos Cubanos [Internet] Washington (DC): US Citizenship and Immigration Services; 2020June16[cited2021 May 19]. Spanish. Available from: https://www.uscis.gov/es/residencia-permanente-tarjeta-verde/categorias-de-elegibilidad-a-la-residencia-permanente/residencia-permanente-para-naturales-o-ciudadanos-cubanos [Google Scholar]
- 26.Florido A End of “wet-foot, dry-foot” means Cubans can join ranks of “undocumented.” National Public Radio [serial on the Internet].2017January15[cited2021 May 19]. Available from: https://www.npr.org/sections/codeswitch/2017/01/15/509895837/end-of-wet-foot-dry-foot-means-cubans-can-join-ranks-of-the-undocumented
- 27.Kelto A In Puerto Rico, health overhaul gets an incomplete. National Public Radio [serial on the Internet].2015February7[cited2021 May 19]. Available from: https://www.npr.org/sections/health-shots/2015/02/07/384060725/in-puerto-rico-health-overhaul-gets-an-incomplete
- 28.Rodríguez-Díaz CE. Maria in Puerto Rico: natural disaster in a colonial archipelago. Am J Public Health 2018;108(1):30–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Robles F Months after Puerto Rico earthquakes, thousands are still living outside. New York Times [serial on the Internet].2020March1[last updated 2021 Apr 8; cited2021 May 19]. Available from: https://www.nytimes.com/2020/03/01/us/puerto-rico-earthquakes-fema.html
- 30.Perez Semanaz S The impact of the Covid-19 pandemic in Puerto Rico [Internet] Washington (DC): American University; 2020November1[cited2021 May 19]. Available from: https://www.american.edu/cas/news/catalyst/covid-19-in-puerto-rico.cfm [Google Scholar]
- 31.Rosa A, Robles F. Pandemic plunges Puerto Rico into yet another dire emergency. New York Times [serial on the Internet].2020July8[last updated 2021 Apr 8; 2021 May 19]. Available from: https://www.nytimes.com/2020/07/08/us/coronavirus-puerto-rico-economy-unemployment.html
- 32.Seervai S How Hurricane Maria worsened Puerto Rico’s health care crisis [Internet] New York (NY): Commonwealth Fund; 2017December18[cited2021 May 19]. Available from: https://www.commonwealthfund.org/publications/other-publication/2017/dec/how-hurricane-maria-worsened-puerto-ricos-health-care [Google Scholar]
- 33.Colón-Burgos JF, Colón-Jordan HM, Reyes-Ortiz VE, Marin-Centeno HA, Rios-Mota R. Disparities and barriers encountered by immigrant Dominican mothers accessing prenatal care services in Puerto Rico. J Immigr Minor Health 2014;16(4): 646–51. [DOI] [PubMed] [Google Scholar]
- 34.Ruggles S, Flood S, Foster S, Goeken R, Pacas J, Schouweiler M, et al. IPUMS USA, version 11.0 [Internet] Minneapolis (MN): IPUMS; 2021[cited2021 May 19]. Available from: https://ipums.org/projects/ipums-usa [Google Scholar]
- 35.Census Bureau. American Community Survey: design and methodology [Internet] Washington (DC): Census Bureau; 2014January30[cited2021 May 19]. Available from: https://www2.census.gov/programs-surveys/acs/methodology/design_and_methodology/acs_design_methodology_report_2014.pdf [Google Scholar]
- 36.Census Bureau. American Community Survey: sample size, Puerto Rico [Internet] Washington (DC): Census Bureau; 2020[cited2021 May 19]. Available from: https://www.census.gov/acs/www/methodology/sample-size-and-data-quality/sample-size/index.php [Google Scholar]
- 37.Census Bureau. About foreign born [Internet] Washington (DC): Census Bureau; 2020October16[cited2021 May 19]. Available from: https://www.census.gov/topics/population/foreign-born/about.html [Google Scholar]
- 38.To access the appendix, click on the Details tab of the article online.
- 39.Artiga S, Orgera K, Damico A. Changes in health coverage by race and ethnicity since the ACA, 2010–2018 [Internet] San Francisco (CA): Henry J. Kaiser Family Foundation; 2020March5[cited2021 May 19]. Available from: https://www.kff.org/racial-equity-and-health-policy/issue-brief/changes-in-health-coverage-by-race-and-ethnicity-since-the-aca-2010-2018/ [Google Scholar]
- 40.Buchmueller TC, Levy HG. The ACA’s impact on racial and ethnic disparities in health insurance coverage and access to care. Health Aff (Millwood) 2020;39(3):395–402. [DOI] [PubMed] [Google Scholar]
- 41.Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav 1995;36(1):1–10. [PubMed] [Google Scholar]
- 42.Bitran R Universal health coverage and the challenge of informal employment: lessons from developing countries [Internet] Washington (DC): World Bank, Human Development Network; 2014January[cited2021 May 19]. (HNP Discussion Paper No. 87077). Available from: http://documents1.worldbank.org/curated/en/698041468180275003/pdf/870770REVISED00mal0Employment0FINAL.pdf [Google Scholar]
- 43.Notiséis 360. Fuerza laboral dominicana aporta $1,700 millones a la economía de Puerto Rico. WIPR [serial on the Internet].2020March11[cited2021 May 19]. Spanish. Available from: https://wipr.pr/fuerza-laboral-dominicana-aporta-1700-millones-a-la-economia-de-puerto-rico/
- 44.Organization for Economic Cooperation and Development. The Dominican Republic’s migration landscape. In: Interrelations between public policies, migration, and development in the Dominican Republic [Internet] Paris: OECD; 2017June22[cited2021 May 19]. Available from: https://www.oecdilibrary.org/sites/97892642768266-en/index.html?itemId=/content/component/9789264276826-6-en [Google Scholar]
- 45.Cita MR. US asylum eligibility: citizenship in the Dominican Republic. Harv CR-CLL Rev 2015;50(1): 255–87. [Google Scholar]
- 46.Zong J, Batalova J. Dominican immigrants in the United States [Internet] Washington (DC): Migration Policy Institute; 2018April11[cited2021 May 19]. Available from: https://www.migrationpolicy.org/article/dominican-immigrants-united-states-2016 [Google Scholar]
- 47.Goldman D, Smith JP. The increasing value of education to health. Soc Sci Med 2011;72(10):1728–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Antonisse L, Garfield R. The relationship between work and health: findings from a literature review [Internet] San Francisco (CA): Henry J. Kaiser Family Foundation; 2018August7[cited2021 May 19]. Available from: https://www.kff.org/medicaid/issue-brief/the-relationship-between-work-and-health-findings-from-a-literature-review/ [Google Scholar]
- 49.Melo JC. Mexicanos impulsan economía en Puerto Rico. Metro [serial on the Internet].2015December19[cited2021 May 19]. Spanish. Available from: https://www.metro.pr/pr/economia/2015/12/19/mexicanos-impulsan-economia-puerto-rico.html
- 50.Banuchi R Colombianos celebran en Puerto Rico su independencia. Primera Hora [serial on the Internet].2014July20[cited2021 May 19]. Spanish. Available from: https://www.primerahora.com/noticias/puerto-rico/notas/colombianos-celebran-en-puerto-rico-su-independencia/
- 51.Sotheby’s International Realty. EB5: Immigrant investor program: United States Citizenship & Immigration Services [Internet] San Juan (PR): Sotheby’s International Realty; 2014August18[cited2021 May 19]. Available from: http://puertoricotaxincentives.com/eb5-immigrant-investor-program/ [Google Scholar]
- 52.Shear MD. Biden’s immigration plan would offer path to citizenship for millions. New York Times [serial on the Internet].2021March8[last updated 2021 May 18; cited2021 May 19]. Available from: https://www.nytimes.com/live/2021/02/18/us/joe-biden-news
- 53.SP 1313, Puerto Rico Senate, 17th Legislative Assembly, 5th Ordinary Session; 2015.
- 54.SR 1081, Puerto Rico Senate, 17th Legislative Assembly, 5th Ordinary Session; 2015.
- 55.Migrant Health Center. Servicios [Internet] Mayagüez: Migrant Health Center; 2021[cited2021 May 19]. Spanish. Available from: http://migrantspr.com/espanol/#servicios [Google Scholar]
- 56.Resumen de Salud. Ofrecerán servicios médicos a dominicanos en Puerto Rico [Internet]. Santo Domingo: Resumen de Salud; 2019. December 22 [cited 2021 May 19]. Spanish. Available from: https://www.resumendesalud.net/40-clinicas-y-hospitales/18455-ofreceran-servicios-medicos-a-dominicanos-en-puerto-rico [Google Scholar]
- 57.Torres M Community health centers were lifesavers after the hurricane, but government didn’t count on them [Internet] San Juan: Centro de Periodismo Investigativo; 2019June13[cited2021 May 19]. Available from: https://periodismoinvestigativo.com/2019/06/community-health-centers-were-lifesavers-after-the-hurricane-but-government-didnt-count-on-them/ [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.